By now you re probably sick of the relentless attack of the alien melanocytes DAILY in your practice. Melanocytic conundrums
|
|
|
- Abel Green
- 5 years ago
- Views:
Transcription



1 Melanocytic conundrums Ron Rapini MD, Chernosky Chair, Dept Derm Professor of Pathology Univ Texas Medical School at Houston MD Anderson Cancer Center Conflict of interest statement: None - I have no stock in grocery stores that sell Rapini By now you re probably sick of the relentless attack of the alien melanocytes DAILY in your practice 1


2 Melanocytes come from the neural crest born to wander wunderlust If you think about it, there are not too many tumors 1 mm in size which regularly metastasize Main goal of the dermatopathologist should be to be helpful; even though often we don t know for sure what all these melanocytic neoplasms are 2
 Morphological diagnosis, whether of birds, fish, plants, or pathological processes in human")
3 "Be kinder than necessary, for everyone you meet is fighting some kind of battle." Plastic surgeon: I am sorry; I just need a definitive diagnosis so I can know what to do... (complaining about report atypical melanocytic proliferation atypical nevus favored over melanoma ) Morphological diagnosis, whether of birds, fish, plants, or pathological processes in human beings, is 100% subjective Ackerman AB. Discordance among expert pathologists in diagnosis of melanocytic neoplasms. Hum. Pathol. 1996; 27;

4 Really, H&E stain is primitive approach of using pink and blue dyes to predict complex biological behavior Future probably lies with more sophisticated methods like FISH, CGH, etc, but many feel that these do not yet give definitive diagnoses in some cases We, the H&E Olympians attempt to predict biologic behavior from pink and blue splotches What is the predicated biologic behavior of this person? Predictive clues? 1. Texas shirt 2. Orange color 3. Shorts 4. Weird hat 5. Beer in hand 6. Socks pulled up 7. Long hair 4
5 Homerun hitters vs Base hitters Homerun hitter dermpaths (one diagnosis melanoma - most of the time) are either really really right or really really wrong Base hitter dermpaths (differential all the time) are almost always right, but often not much help The ART of pathology is to be a homerun hitter as much as possible but to go for the base hit when necessary Five dermatopathologists have seen this slide Three think that it is benign and two favor malignancy They can have their opinion, but definitive answer may be unknown Vague terms ( The favorite plant of radiologists and pathologists is the hedge ) Consistent with Suggestive of Near the margin Narrow margin Approximates the margin 5
6 Clues Ackerman published several books on various clues in dermpath Our diagnoses and predictions are based upon various clues or other findings Not all clues are valid: I prefer not to use algorithms for that reason (blind alley if rely too heavily on just one finding) I prefer to look at multiple findings in tandem Our criteria may be wrong, but at least we have criteria Better than using feeling in your gut Not all criteria have equal sensitivity and specificity Use multiple criteria So let s start with a lawsuit! Happened to me when 30 years out of medical school and 25 years doing dermpath The celebration: my first Dear Dr Rapini letter received 6

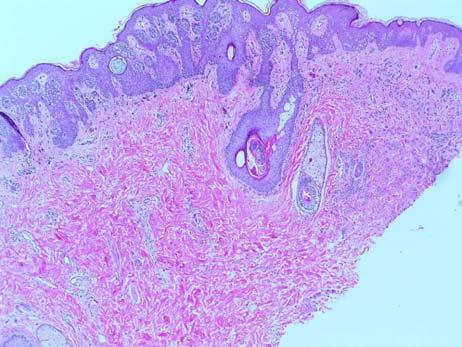
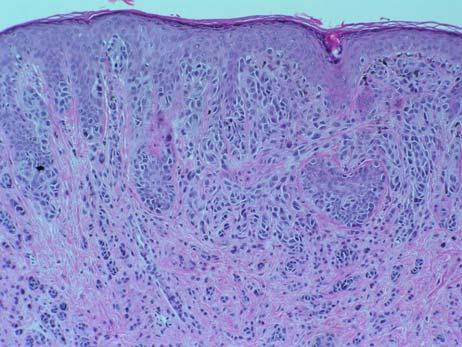
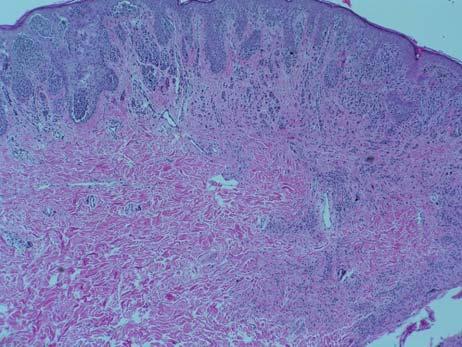
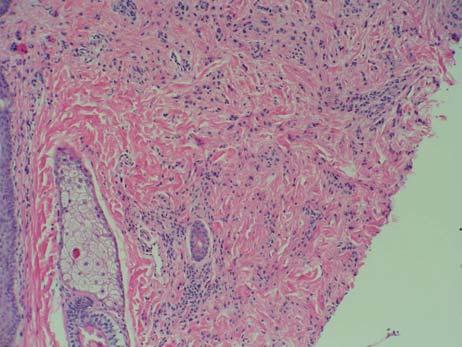
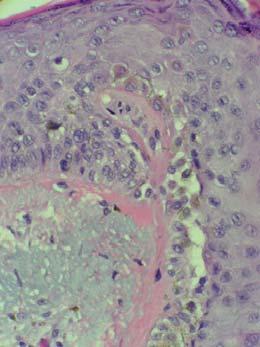
7 19 year old construction worker, shoulder 7


8 8

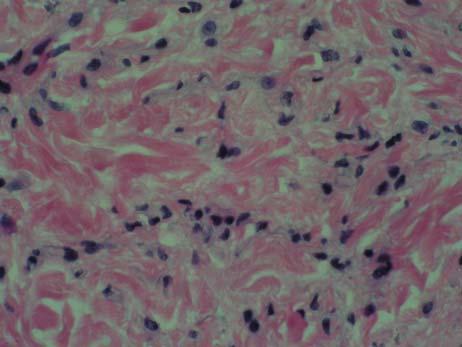
9 9


10 Dysplastic nevus with severe atypia I stated the features: Atypical epithelioid cells in superficial portion, with junctional mitoses, pagetoid Congenital features, banal single filing Clefts, Spitz nevus features, maturation No ulceration, nearly no inflammation 10
11 Dysplastic nevus with severe atypia My concluding statement: Does not meet enough criteria for melanoma If this WERE a melanoma, depth would be no greater than 0.5 mm Melanocytes extend more deeply than that but those appear benign Conservative re-excision recommended Patient went to plastic surgeon and had re-excision He decided to take 3 mm margins Tissue only showed scar Patient never had local recurrence Nothing happened until 5 years later when he developed the node in neck Lawsuit said: 2002: You misread tissue as a BENIGN dysplastic nevus with SEVERE atypia. You recommended excision of margins. 2007: Mass in lymph node on neck 11
12 They sued four parties 1. Ron Rapini MD, read original 2. Pathologist who read the re-excision as negative (he was right) 3. Path Lab that employed that 2 nd pathologist 4. Lab Corp that contracted with that lab Dermatologist wrote in chart: seriousness of the diagnosis explained to patient, before sending him to plastic surgeon After the metastasis occurred with no local recurrence, another dermatologist wrote obviously the lesion metastasized before Dr Rapini ever read the slides Slides reviewed elsewhere after metastasis known Nevoid malignant melanoma Considerable atypia in upper portion but pronounced maturation Sufficient atypia in upper portion to point to melanoma Overall pattern deceptive, however Nevoid portion extends to deep margin at 1.5 mm (level IV) (I had only measured the atypical portion at 0.5 mm) 12
13 Patient alive, had large node removed, no further recurrence yet after 2 yrs Plaintiff dermpath expert and oncologist: Case should have been sent out for consult and definitive diagnosis Patient was denied the sentinel lymph node biopsy and interferon which would have made a difference Margins would have been wider. Mediator said (in private) We attorneys just go out and hire whores, because they are more predictable and controllable Final result: All four original parties were dismissed So... I can talk about it 13
14 They then sued a 5 th party, the university, which paid them $60K Attorney for university said that this is a teenager case, and don t like child cases: cannot predict what jury will do If 80 year old, then would not have settled Preventive tactics Biopsy everything Call everything malignant Hedge all the time and don t give specific answer Clinical correlation needed Re-excision needed Order unnecessary preventive tests and consult others frequently Add sentence: Melanoma was considered, and was not favored, but cannot be completely excluded Masterful hedging? Worthless? 14
15 Takes more guts to call something benign rather than malignant Only bad things happen to the pathologist and the patient if the malignant lesion was called benign If benign called malignant, no one will know, they will remain happy there was no recurrence, and likely no one will sue for over treatment Hence, we have... Sebaceous adenomas in the setting of Muir-Torre syndrome are all sebaceous carcinoma Proliferating pilar cysts are all SCC If you live in paranoia... Your diagnoses become less specific More atypia, more malignancy LONGER notes, longer reports Personally, I still do things pretty much the same way 15
16 Internal or External Consultations help protect you But they are overrated Bandwagon opinion of the group Often everyone just hedges If someone does NOT hedge, how do you know they are right? Keep a record (in house, use initials?) I testified in this lawsuit: Pathologist diagnosis on solitary single papule: histiocytic proliferation re-excision recommended What would you do if you were the plastic surgeon? Histiocytic disorder re-excision recommended Plastic surgeon did nothing Lesion metastasizes (turns out the histiocytes were melanocytes) Patient sues plastic surgeon, not pathologist 16
17 Histiocytic disorder re-excision recommended Plastic surgeon testifies he did not reexcise because this pathologist ALWAYS says re-excision recommended, so it has no meaning Pathologist testifies: Yes, I do say on ALL skin biopsy reports with incomplete margins, re-excision recommended Case goes to court, jury finds doctor not at fault Histiocytic proliferation - case lessons Re-excision recommended is pathologist putting the onus on the clinician Clinician almost obligated to do it, but if you don t, should write explanation of why not in the chart Make sure patient is informed, give copy of pathology report, and document 17
18 OK, with that introduction (and with the knowledge that lawyers are lurking, we are ready to discuss: DYSPLASTIC NEVI! First of all we cannot agree on what to call it Dysplastic nevus (DN) Nevus with architectural disorder (NAD, NWAD) Clark s nevus Active nevus Atypical nevus Atypical mole And we have invented many other terms for the grey zone lesions MELTUMP mel tumor uncertain malig potential SAMPUS superficial atyp mel prolif uncertain signif SIMP sun-induced mel prolif AMP Atyp mel prolif AST Atyp Spitz tumor 18
19 The concept of dysplastic nevus is very controversial: induces spasms in many dermatopathologists Ackerman AB. Histopathology Sep;13(3): What naevus is dysplastic, a syndrome and the commonest precursor of malignant melanoma? A riddle and an answer. Dysplastic nevus = Clark s nevus = active nevus 5% or 50% of population criteria vary! More significant if +FH melanoma, multiple atypical nevi Most common nevus in man - Ackerman Growth industry for derm - Clark Dysplastic nevus NIH consensus conference (JAMA 1992): Clinician should call them atypical moles, pathologist should call them nevus with architectural disorder and should grade the cytology mild, moderate, severe 19
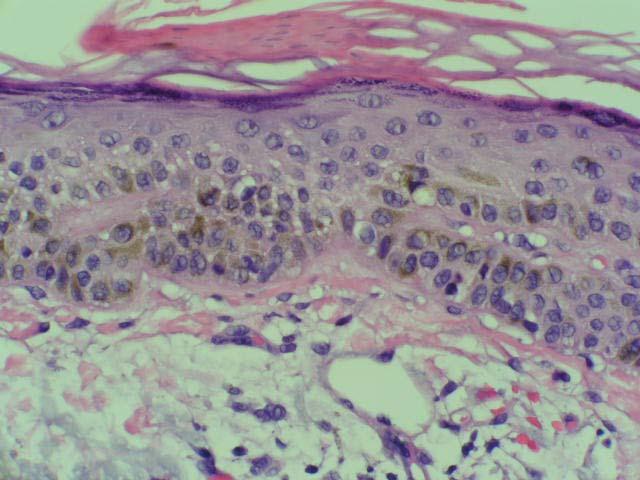
 (Ackerman s favorite was asymmetry, I think, but flat dysplastic nevi don t have enough dermal component to evaluate that) Pagetoid melanocytes (Ackerman calls")
20 My 3 favorite things to distinguish melanoma from dysplastic nevus (but exceptions to all of this) 1. More pagetoid 2. More atypia 3. More lymphocytes ( smart bombs ) (Ackerman s favorite was asymmetry, I think, but flat dysplastic nevi don t have enough dermal component to evaluate that) Pagetoid melanocytes (Ackerman calls scatter ) Melanoma Spitz nevus, pigmented spindle cell nevus Congenital nevi in neonates Acral nevi Irritated nevi (especially centrally) Keratinocyte processing artifact 20
21 Lymphocytes in benign nevi Halo nevus Spitz nevus Traumatized nevus Demodex mites and other stimuli Lots of things in pathology have plenty of cytologic atypia and are still benign It has been said that you MUST have cytologic atypia to call something dysplastic nevus Ackeman complained that most of them have NO cytologic atypia, hence the term nevus with architectural disorder Grading dysplasia in dysplastic nevi NIH consensus conference 1992 recommended grading cytology despite lack of concordance I grade only cytology as mild, moderate, severe Cockerell in Dallas does not grade at all, but points out which ones need re-excision MDACC grades both cytology and architecture Barrett: Only mild or severe, never moderate 21
22 Lack of concordance on grading dysplasia Piepkorn (J Cutan Pathol 6:542, 1992) found only 38% agreement Important to know threshold of your particular dermatopathologist Dysplastic nevus grading is a mess Need to know who is reading the biopsy and their habits to know what it all means. Lab A: won t grade them at all, but will let you know which ones they are worried about and should be excised. Lab B grades them only as SEVERE or MILD, but never MODERATE because that is too vague. Lab C will grade both the CYTOLOGY and the ARCHITECTURE into 3 grades, double-grading them 22
23 Duke, Univ Chicago, MD Anderson Grade BOTH cytology AND architecture because the authors of paper on that migrated to those places Shea CR, Vollmer RT, Prieto VG. Hum Pathol. 1999;30: Correlating architectural disorder and cytologic atypia in Clark (dysplastic) melanocytic nevi. may provide additional information for clinical management Shea et al grading architectural disorder Circumscription Asymmetry Nest cohesiveness Suprabasal melanocytes Confluence Single cell proliferation Immunostains for problem: melanoma versus nevus? K-67: Less than 5% = nevus, more than 10% = melanoma (problem that lymphocytes will often stain so some use a double labelling technique with panmel) HMB-45: Stratified staining (nevus is negative deeper in dermis) 23
24 Shaving OK in dysplastic nevi? Cosmetic result can be superior Take 2 mm superficial margin and make sure you get under the lesion Check for pigment at base after shave Better to have shave of 11 mm macule than 6 mm punch biopsy My margin recommendation: Mild atypia don t re-excise Severe atypia always re-excise Moderate atypia jump ball Tallon B, Snow J (New Zealand). Am J Dermatopathol Epub ahead of print.low Clinically Significant Rate of Recurrence in Benign Nevi. The rate of recurrence requiring re-excision is very low at 0.3%. This suggests that few cases of clinical recurrence are re-excised. Re-excision of benign nevi including mild and moderately dysplastic nevi may not be necessary. 24

 Four lessons with this case,")
25 Lentigo, DN? Dysplastic nevus? No, lentigo maligna (melanoma in situ!) Four lessons with this case, with general rules 25
26 Lessons from this case 1. If lesion recurs beyond scar, consider more worrisome, and less likely just recurrence recurrent nevi mostly IN the scar, arising from deeper component Lessons from this case 2. If you think it is dysplastic nevus, but it is present on sundamaged skin of older individual, consider an upgrade to LM Lessons from this case 3. If it is growing or changing, pay attention Listen to the patient; if they are worried then maybe you should be worried (though SKs, lots of B9 things grow) Lawyers are all around 26

27 Lessons from this case 4. Mostly OK to shave dark macules even though some say everything should be punched and shaved to adipose Better to shave entire large macule than to just punch part of it AAD guidelines of care say it is sometimes ok and advantageous to shave suspected melanomas The light brown unimpressive melanoma Not to cause paranoia, but..incidence of melanoma increasing dramatically along with increased liability concerns If the patient is worried, consider being worried yourself When in doubt, cut it out If the patient says it is growing or changing, pay attention Lentigo maligna NO 2 mm punch 27

28 Lentigo maligna = melanoma in situ of sundamaged skin We think it is a different subset because it stays in situ for centuries If you miss it, chances are next year it will still be in situ Only 5% become invasive? unlike melanoma in situ of covered sites? Lentigo maligna = melanoma in situ of sundamaged skin Atrophic epidermis Severe solar elastosis Older age Can be subtle!! MART-1, MITF SOX10 helps? 28



29 Starburst giant cells as a clue for LM Lisa Cohen 29




30 Starburst giant cells as a clue for LM Lisa Cohen Lentigo maligna of the subtle type this one was missed S Lentigo maligna of the subtle type this one was missed MART-1, S

31 Lentigo maligna is defined as (1) subset of melanoma in situ (2) on sundamaged skin Problem is: what is sundamaged? Worthwhile to subclassify? Atrophy of epidermis NOT necessary! Lentigo maligna melanoma means invasive but LM is a melanoma too (in situ) terminology problem R/O lentigo maligna - NOT MDACC Dysplastic nevus? 31


32 Mostly I accept some architectural disorder in congenital nevi without calling them dysplastic My skincolored mole regrew after it was shaved 32


33 Recurrent melanocytic nevus Kornberg & Ackerman: Pseudomelanoma Arch Dermatol 111:1588, % have pagetoid cells Heavily pigmented junctional melanocytes usually directly overlying a scar 10-30% of shaved nevi recur or persist Recurrent nevus 33
 DYSPLASTIC nevi?")

34 Recurrent nevus Do you think some recurrent nevi can be called recurrent (persistent) DYSPLASTIC nevi? For me, mostly no Jentigo? Lentiginous junctional nevus? Tiny speck nevi do you require DNs to be at least 6 mm? 34

35 Halo nevus Do you think MOST halo nevi are DYSPLASTIC nevi? Most halo nevi are on the trunk where many dysplastic nevi occur They do tend to have the architectural features of DN Nevi of special sites or sitespecific nevi (groin, genitals, breast, etc) I just call most of them dysplastic nevus and don t use site-specific or special site 35

36 Nevus spilus = speckled lentiginous nevus Jean Bolognia thinks of nevus spilus (speckled lentiginous nevus) as a garden and within the garden you can have lots of things beside just background lentigo with benign nevi Within the garden you can have dysplastic nevus, Spitz nevus, blue nevus, anything VERY rare for nevus spilus to become malignant SPARK NEVUS Features of Spitz + Clark = Spark I find the term useful sometimes Ko CJ, McNiff JM, Glusac EJ. J Cutan Pathol : Melanocytic nevi with features of Spitz nevi and Clark's/dysplastic nevi ("Spark's" nevi). 36


37 Pigmented lichenoid keratosis COMMON cause of consultation When pigment not prominent, clinically thought to be BCC Probably mostly are lentigo, seborrheic keratosis or pigmented actinic keratosis that becomes inflamed Are these regressed melanomas? 37

38 What to call it BLK benign lichenoid keratosis, but they are not all benign, some are precancer LK I like PigLK If lots of pigment just vacuolar degen made melanin incontinence, vs regressed melanocytic neoplasm? LAK if precancer, atypia Pigmented AK Mistaken for lentigo, LM, SK clinically and pathologically BUT, has atypical budding keratinocytes, parakeratosis May extend down follicle, but so can LM Melanocytes tend to have dusky or vacuolated cytoplasm 38


39 Pigmented AK Parakeratosis helpful in my opinion but some of my colleagues say PigAK does not require parakeratosis MART-1 helpful or does it cause overdiagnosis of lentigo maligna? 39


40 40

41 41
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Toby Maurer, MD University of California, San Francisco. Lifetime risk of an American developing melanoma
 Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Distinguishing Pigmented Skin Lesions and Melanoma Toby Maurer, MD University of California, San Francisco Epidemiology of Melanoma Lifetime risk of an American developing melanoma 1935: 1 in 1500 1980:
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 12, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 12, 2012 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
VACAVILLE DERMATOLOGY
 Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
Connecting the Dots on those Spots NANDAN V. KAMATH, M.D. VACAVILLE DERMATOLOGY Sources All of the photos were taken with permission from the Dermnet NZ website - Dermnet New Zealand after communicating
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB. Friday, February 13, :30 am 11:00 am
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSION PATHOLOGY OF THE SKIN LAB Friday, February 13, 2009 9:30 am 11:00 am FACULTY COPY GOALS: Describe the basic clinical and morphologic features of various
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Management of Atypical Pigmented Lesions
 Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Management of Atypical Pigmented Lesions Jennifer A. Stein MD, PhD Associate Director, Pigmented Lesion Section Ronald O. Perelman Department of Dermatology NYU Langone Medical Center July 29, 2017 1-4
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Lichenoid Tissue Reaction in Malignant Melanoma A Potential Diagnostic Pitfall
 natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
natomic Pathology / LICHENOID TISSUE RECTION IN MLIGNNT MELNOM Lichenoid Tissue Reaction in Malignant Melanoma Potential Diagnostic Pitfall CPT Scott R. Dalton, MC, US, 1,3 Capt Matt. aptista, USF, MC,
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Atypical Nevi When to Re-excise. Catherine Barry, DO Dermatopathologist
 Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Atypical Nevi When to Re-excise Catherine Barry, DO Dermatopathologist Why talk about skin cancer? Because it s the most common type of cancer! Non-melanoma Skin Cancers Basal Cell Carcinoma Squamous Cell
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Histopathology: skin pathology
 Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Histopathology: skin pathology These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual information
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
5/21/2018. Disclosures. Consulting: Myriad Genetics SciBase. Superficial Atypical Melanocytic Proliferations. SSM, LMM and (some of) their Simulants
 their Simulants") Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial
 Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Dermatology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI Memorial Cutaneous Oncology for the PCP Deanna G. Brown, MD, FAAD Susong Dermatology Consulting Staff at CHI
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
What is melanoma? Melanoma dealing with the diagnosis. What is melanoma?
 Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Melanoma is a form of cancer which develops from that part of the skin which produces its colour. It grows from the cell which produces the brown pigment in our skin: the melanocyte. Often the melanoma
Learning Objectives. Tanning. The Skin. Classic Features. Sun Reactive Skin Type Classification. Skin Cancers: Preventing, Screening and Treating
 Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Learning Objectives Skin Cancers: Preventing, Screening and Treating Robert A. Baldor, MD, FAAFP Professor, Family Medicine & Community Health University of Massachusetts Medical School Distinguish the
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Actinic keratosis (AK): Dr Sarma s simple guide
: Dr Sarma s simple guide") Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Actinic keratosis (AK): Dr Sarma s simple guide Actinic keratosis is a very common lesion that you will see in your day-to-day practice. First, let me explain the name Actinic keratosis. It means keratosis
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited. Timothy H. McCalmont, MD University of California, San Francisco
 Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited Timothy H. McCalmont, MD, San Francisco I. IS IT BENIGN OR IS IT MALIGNANT? One of the commonest determinations we make as
Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited Timothy H. McCalmont, MD, San Francisco I. IS IT BENIGN OR IS IT MALIGNANT? One of the commonest determinations we make as
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Regression 2/3/18. Histologically regression is characterized: melanosis fibrosis combination of both. Distribution: partial or focal!
 Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Regression Margaret Oliviero MSN, ARNP Harold S. Rabinovitz MD Histologically regression is characterized: melanosis fibrosis combination of both Distribution: partial or focal! Dermatoscopic terminology
Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Morphologic characteristics of nevi associated with melanoma: a clinical, dermatoscopic and histopathologic analysis Temeida Alendar 1, Harald Kittler
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
EARLY ONLINE RELEASE
 EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
EARLY ONLINE RELEASE Note: This article was posted on the Archives Web site as an Early Online Release. Early Online Release articles have been peer reviewed, copyedited, and reviewed by the authors. Additional
Regeneron and Sanofi are financial supporters of The Skin Cancer Foundation and collaborated in the development of this article. US-ONC /2018
 A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
A D E E P E R L O O K When detected early, most cases of local cutaneous squamous cell carcinoma are easily treated and usually cured. But when they become more advanced, this second most common form of
Histopathology of Melanoma
 THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
THE YALE JOURNAL OF BIOLOGY AND MEDICINE 48, 409-416 (1975) Histopathology of Melanoma G. J. WALKER SMITH Department ofpathology, Yale University School ofmedicine, 333 Cedar Street, New Haven, Connecticut
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,500 108,000 1.7 M Open access books available International authors and editors Downloads Our
Identifying Benign and Malignant Skin Lesions. No Disclosures. Common Benign Lesions. Benign Lesions 2/25/2018. Stucco Keratoses.
 Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Dermatology in Primary Care Identifying Benign and Malignant Skin Lesions Christy Quire Baker, APRN, FNP-BC, DCNP Dermatology Certified Nurse Practitioner No Disclosures Common Benign Lesions Seborrheic
Guy Perrot (Ги Перро)
") НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
НАУЧНО-ПРАКТИЧЕСКАЯ КОНФЕРЕНЦИЯ (МАСТЕР-КЛАСС) «ПРАКТИЧЕСКИЕ АСПЕКТЫ ДИАГНОСТИКИ И ЛЕЧЕНИЯ МЕЛАНОМЫ КОЖИ» DIAGNOSTIC AND PITFALLS IN MELANOMA Guy Perrot (Ги Перро) MD PHD pathologist, University Hospital
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Mole mapping and monitoring. Dr Stephen Hayes. Associate Specialist in Dermatology, University Hospital Southampton
 Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Mole mapping and monitoring Dr Stephen Hayes Associate Specialist in Dermatology, University Hospital Southampton Outline of presentation The melanoma epidemic Benefits of early detection Risks of the
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Diagnosis of Lentigo Maligna Melanoma. Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ
 Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
Diagnosis of Lentigo Maligna Melanoma Steven Q. Wang, M.D. Memorial Sloan-Kettering Cancer Center Basking Ridge, NJ Conflict of Interest: None Topics Epidemiology and Natural History Clinical and Histologic
 Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Page 1 of 15 Title Authored By Course No Contact Hours 2 Skin Cancer the Real Picture for Early Detection and Treatment Cheryl Sommer RN, MSN, ARNP SC120604 Purpose The purpose of this course is to provide
Cancer Reporting for Dermatologists. Florida Department of Health Florida Cancer Data System. March 9, Agenda
 Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Cancer Reporting for Dermatologists Florida Department of Health Florida Cancer Data System March 9, 2011 Agenda Welcome Introductions Cancer Reporting in Florida BETA Participation Expectations Review
Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio. Glen M. Bowen, MD Huntsman Cancer Institute University of Utah
 Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio Glen M. Bowen, MD Huntsman Cancer Institute University of Utah I. Objectives: a. Review the terminology of LM/LMM b. Understand the relative
Lentigo Maligna: Striking a Balance With the Risk-Benefit Ratio Glen M. Bowen, MD Huntsman Cancer Institute University of Utah I. Objectives: a. Review the terminology of LM/LMM b. Understand the relative
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
SKIN CANCER. Most common cancer diagnosis 40% of all cancers
 SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
SKIN CANCER Most common cancer diagnosis 40% of all cancers OBJECTIVES Review common and uncommon cancers of the skin. Special emphasis on melanoma and dysplastic nevus Review pathology/tnm/staging, which
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT
 LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
LUMPS AND BUMPS: AN ORGANIZED APPROACH TO DIAGNOSIS AND MANAGEMENT Tammy P. Than, M.S., O.D., F.A.A.O. The University of Alabama at Birmingham / School of Optometry 1716 University Blvd. Birmingham, AL
Cutaneous Malignancies: A Primer COPYRIGHT. Marissa Heller, M.D.
 Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Cutaneous Malignancies: A Primer Marissa Heller, M.D. Associate Director of Dermatologic Surgery Department of Dermatology Beth Israel Deaconess Medical Center December 10, 2016 Skin Cancer Non-melanoma
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma and Dermoscopy. Disclosure Statement: ABCDE's of melanoma. Co-President, Usatine Media
 Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
Melanoma and Dermoscopy Richard P. Usatine, MD, FAAFP Professor, Family and Community Medicine Professor, Dermatology and Cutaneous Surgery Medical Director, University Skin Clinic University of Texas
SEBACEOUS NEOPLASMS. Dr. Prachi Saraogi Clinical Fellow in Dermatology
 SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
SEBACEOUS NEOPLASMS Dr. Prachi Saraogi Clinical Fellow in Dermatology Sebaceous neoplasms Sebaceous adenoma (Benign) Sebaceous carcinoma (Malignant) SEBACEOUS ADENOMA Benign tumours composed of incompletely
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation. Dermatopathology Specialists Needed. Changing Trends
 Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
S everal morphological features are frequently used in the
 1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
LENTIGO SIMPLEX. Epidemiology
 LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
LENTIGO SIMPLEX Epidemiology The frequency of lentigo simplex in children and adults has not been determined. There does not appear to be a racial or gender predilection. Lentigo simplex is the most common
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations
 F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
F006 Imaging in Dermatology Melanocytic Neoplasia Clinical-Confocal-Pathological-Correlations Melissa Gill, MD SkinMedical Research and Diagnostics Dobbs Ferry, NY, USA Department of Pathology SUNY Downstate
PATHOLOGY OF THE SKIN 2. Tumours of the skin
 PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
PATHOLOGY OF THE SKIN 2. Tumours of the skin Máirín E. McMenamin MB MRCPI FRCPath Dip (Dermatopathol) RCPath St. James s Hospital and University of Dublin, Trinity College Tumour (Neoplasia) Benign or
Common Benign Lesions and Skin Cancers. 22nd May 2015 Dr Mark Foley
 Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Common Benign Lesions and Skin Cancers 22nd May 2015 Dr Mark Foley Thank you for downloading this file. This intended to supplement the presentation given at the NZ Wound Care Conference, it is not intended
Skin Cancer A Personal Approach. Dr Matthew Strack Dunedin New Zealand
 Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Skin Cancer A Personal Approach Dr Matthew Strack Dunedin New Zealand Outline Dermoscopy Instruments and setup Photochemosurgery Clinical Aim: Leave with 2-3 ideas JLE Benign Junctional Nevus Management
Know who is at risk: LOOK! for ABCDs, rapidly changing lesions, do a biopsy when indicated
 Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Lindy P. Fox, MD Assistant Professor Director, Hospital Consultation Service Department of Dermatology University of California, San Francisco Applies to adults without history of malignancy or premalignant
Acquired melanocytic nevi in Egyptian patients: A clinicopathological study
 Acta Dermatovenerol APA Acta Dermatovenerologica Alpina, Pannonica et Adriatica ;:- doi:.8/v---8 Acquired melanocytic nevi in Egyptian patients: A clinicopathological study Mohamed A. El-Khalawany Abstract
Acta Dermatovenerol APA Acta Dermatovenerologica Alpina, Pannonica et Adriatica ;:- doi:.8/v---8 Acquired melanocytic nevi in Egyptian patients: A clinicopathological study Mohamed A. El-Khalawany Abstract
6/17/2018. Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things. Bad?
 Dermoscopy of Brown(ish) Things. Bad?") Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Breaking Bad (Part 1) Dermoscopy of Brown(ish) Things Jennie T. Clarke, MD ssociate Professor of Dermatology University of Utah School of Medicine Bad? 1 Brown(ish) Things Bad Melanoma Pigmented basal
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783
 Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783 Pie Chart Participants N=74 Benign: 48 N=74 Blue naevus: 38 Intradermal: 12 DPN: 10 Compound 3 Clonal: 3; Spitz 2; Special Site: 1; Congenital:
Case RAC7783. M46. Ear. Mole. r/o MM.?Blue naevus RAC7783 Pie Chart Participants N=74 Benign: 48 N=74 Blue naevus: 38 Intradermal: 12 DPN: 10 Compound 3 Clonal: 3; Spitz 2; Special Site: 1; Congenital:
Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions
 Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions Symon D Oyly Cotton Ela Claridge School of Computer Science, The University of Birmingham Birmingham B15 2TT, UK Per Hall
Assisting diagnosis of melanoma through the noninvasive biopsy of skin lesions Symon D Oyly Cotton Ela Claridge School of Computer Science, The University of Birmingham Birmingham B15 2TT, UK Per Hall
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Pathology. Skin Tumor. Bayan N. Mohammad 15/10/2015. Mohammad al-orjani. Page 0 of 23
 #7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
#7 35 Pathology Skin Tumor Bayan N. Mohammad 15/10/2015 Mohammad al-orjani Page 0 of 23 بسم هللا الرحمن الرحيم GREETINGS This lecture is about skin tumors, all the slides are included and every slide will
Atypical Histologic Features in Melanocytic Nevi
 The American Journal of Dermatopathology 22(5): 391 396, 2000 2000 Lippincott Williams & Wilkins, Inc., Philadelphia Atypical Histologic Features in Melanocytic Nevi Carmelo Urso, M.D. The atypical histologic
The American Journal of Dermatopathology 22(5): 391 396, 2000 2000 Lippincott Williams & Wilkins, Inc., Philadelphia Atypical Histologic Features in Melanocytic Nevi Carmelo Urso, M.D. The atypical histologic
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
Mimics from TEXAS. Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas
 Mimics from TEXAS Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas *Conflict of interest - Elsevier *I do not own stores that
Mimics from TEXAS Ron Rapini MD Chernosky Chair Dept Dermatology Professor of Pathology Univ of Texas and MD Anderson Cancer Cntr Houston, Texas *Conflict of interest - Elsevier *I do not own stores that
BAP-oma & BEYOND MICHAEL A NOWAK, MD
 BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
BAP-oma & BEYOND MICHAEL A NOWAK, MD CONFLICTS No conflicts with the content of this lecture BAP-oma Wiesner 2011: Families with multiple tan dome-shaped papules of head, neck, trunk, and extremities.
Melanoma. Consultation on draft guideline - stakeholder comments. Comments to be submitted before 5pm on Friday 13 March 2015
 Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
Please note: Please fill in both the stakeholder organisation and name of commentator fields. We cannot accept forms with attachments such as research articles, letters or leaflets. Stakeholder organisation(s)
None. Conflicts of Interest: Good News! NEJM 2011
 Napa Dermatoathology Meeting 2018: Medicolegal Issues in Dermpath Whitney A. High, MD, JD, MEng whitney.high@ucdenver.edu Professor of Dermatology & Pathology Vice-Chairman, Dermatology Director of Dermatopathology
Napa Dermatoathology Meeting 2018: Medicolegal Issues in Dermpath Whitney A. High, MD, JD, MEng whitney.high@ucdenver.edu Professor of Dermatology & Pathology Vice-Chairman, Dermatology Director of Dermatopathology
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
So, we already talked about that recognition is the key to optimal treatment and outcome.
 Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
K Blessing, J J H Grant, D S A Sanders, M M Kennedy, A Husain, P Coburn
 J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands