INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
|
|
|
- Neal Fields
- 5 years ago
- Views:
Transcription
1 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
2 OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT DIFFERENT KINDS OF INSULIN PREPARATIONS DIFFER AS TO SOURCE, STRENGTH, AND DURATION OF ACTION STATE THE IMPORTANCE OF ACCURATE TIMING OF INSULIN ADMINISTRATION DESCRIBE TREATMENT OPTIONS AVAILABLE
3 WHO IS HERE TODAY? PLEASE RAISE YOUR HAND IF YOU ARE : 1. PHYSICIAN 2. NURSE PRACTITIONER 3. NURSE 4. PHYSICIAN ASSISTANT 5. PHARMACIST 6. DIABETES EDUCATOR 7. DIETITIAN 8. ADMINISTRATOR 9. OTHER 3
 Indirect (disability, work loss, premature death): $69 billion 4 http://www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf")
4 NATIONAL DIABETES STATISTICS REPORT, million people or 9.3% of the U.S. population have diabetes Diagnosed: 21 million Undiagnosed: 8.1 million Estimated diabetes costs in the U.S. (2012) Total (direct and indirect): $245 billion Direct medical costs: $176 billion (2.3 x higher than people without diabetes) Indirect (disability, work loss, premature death): $69 billion 4
5 Obesity Trends* Among U.S. Adults BRFSS, 1990, 2000, 2010 (*BMI 30, or about 30 lbs. overweight for 5 4 person) No Data <10% 10% 14% 15% 19% 20% 24% 25% 29% 30%

6 Diabetes Among U.S. Adults 1990, 2000, No Data < 4% 4% 7.9% 8% 11.9% 12% 15.9% 16%

7 Population (%) Population (%) INCREASE IN DIABETES PARALLELS THE INCREASE IN OBESITY IN THE UNITED STATES Obesity* Diabetes % increase % increase *BMI 30 kg/m 2. CDC. National diabetes statistics report, Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, Mokdad AH, et al. JAMA. 1999;282: ; Mokdad AH, et al. Diabetes Care. 2000;23: ; Flegal KM, et al. JAMA. 2016;315:

8 BURDEN OF DIABETES

9 PREVALENCE OF DIABETES IN HOSPITALS IS HIGH AND INCREASING Number of discharges with diabetes as firstlisted diagnosis: 635,000 Average length of stay: 4.6 days How many patients discharged from your hospital have diabetes? 9 Accessed August 5, 2014

10 SHARP HEALTHCARE PERCENT OF ACUTE INPATIENT DIABETICS CY 2010 TO 2017
11 DEFINITION OF DIABETES Metabolic alteration in the way the body uses food for growth and energy Type 1: autoimmune process beta cell destruction, lack of insulin production Type 2: resistance to insulin aided transport of glucose into muscle and adipose tissue; overproduction of glucose by the liver GDM (gestational diabetes): glucose intolerance that develops during pregnancy
12 ROLE OF INSULIN ANABOLIC HORMONE FACILITATES STORAGE OF NUTRIENTS GLUCOSE GLYCOGEN IN LIVER AMINO ACIDS PROTEIN IN MUSCLES FATTY ACIDS TRIGLYCERIDES IN FAT PREVENTS HEPATIC BREAKDOWN OF GLYCOGEN (GLYCOGENOSIS)

13 INSULIN ACTS LIKE A KEY
14 INSULIN DEFICIENCY

15 WHAT HAPPENS WHEN INSULIN IS INSUFFICIENT? CELLULAR STARVATION CATABOLIC PROCESS RELEASE OF NUTRIENTS GLUCOSE GLYCOGEN IN THE LIVER AMINO ACIDS PROTEIN IN THE MUSCLES FATTY ACIDS TRIGLYCERIDES IN THE FAT
16 HISTORY OF INSULIN IN THE U.S The introduction of insulin began with pancreatic extract, first used to treat humans in 1922 (bovine insulin) by Banting and Best, and different preparations became available over the following decades Human insulin was developed in the laboratory in 1978 and approved for therapeutic use in 1982, as a U100 insulin Concentrated insulin was introduced in 1980, and recent years have seen the production of many concentrated insulin preparations including U200 and U Insulin analogues were introduced in 1998, with the approval of insulin lispro (Eli Lilly and Company, Indianapolis, IN), followed in 2000 by insulin glargine, which was developed as a peak less insulin. Analogue insulin is available in two main forms, rapid acting and long acting, as well as premixed combinations.
17 UNDERSTANDING INSULIN SENSITIVITY AND DIABETES Diabetes is a disorder in the way the body uses glucose, a sugar that serves as fuel for the body. When blood glucose levels rise, the pancreas normally make the hormone insulin, which signals cells to take sugar from the blood. Fat cells store excess glucose in the form of lipids (fats). In the most common form of diabetes, type 2, cells lose their sensitivity to insulin.

18 INSULIN RESISTANCE REDUCTION IN BIOLOGICAL RESPONSE TO INSULIN ASSOCIATED WITH BOTH GENETICS AND LIFESTYLE LACK OF EXERCISE, HIGH CALORIC DIET AND STRESSFUL LIFESTYLE - OBESITY INCREASED RISK OF CARDIOVASCULAR DISEASE NOT LIMITED TO TYPE 2 DIABETES DIABESITY
19 INSULIN RESISTANCE As the diabetes population gets heavier, daily doses of more than 100 units are more common. An increasing number of patients have severe insulin resistance and require large doses of insulin. Managing patients with severe insulin resistance is challenging because it is difficult to achieve good glycemic control using conventional treatment approaches Patients with severe insulin resistance require >2 units/kg of body weight or 200 units/day of insulin. Insulin can cause weight gain, which further contributes to worsening insulin resistance. Large total daily dose requirements of standard U-100 insulin can be painful to administer and the onset and duration of insulin activity can be altered with high-volume doses.
20 PHYSIOLOGIC INSULIN SECRETION: DESIGNING AN INSULIN REGIMEN Insulin (µu/ml) Basal Insulin 150 Breakfast Lunch Dinner Glucose (mg/dl) A.M. P.M. Basal Glucose Time of Day
 Normal Secretory Pattern of Insulin Basal insulin Breakfast Lunch Dinner")
21 Insulin MAINTAINING PHYSIOLOGIC INSULIN DELIVERY IN THE HOSPITAL: BASAL BOLUS Correctional insulin Mealtime insulin (bolus) Normal Secretory Pattern of Insulin Basal insulin Breakfast Lunch Dinner Bedtime
22 INSULIN OPTIONS FOR BASAL INSULIN (CONTROLLING BG IN FASTING STATE) ANALOGS DETEMIR GLARGINE HUMAN NPH HUMULIN R U-500 OPTIONS FOR NUTRITIONAL INSULIN (CONTROLLING BG WHEN THERE IS CALORIC INTAKE) ANALOGS ASPART GLULISINE LISPRO HUMAN REGULAR Analogs cost about $270 per 10 ml vial, while Regular Human insulins such as Novolin and Humulin run about $120 per 10 ml vial.
23 PHYSIOLOGIC MULTIPLE INJECTION REGIMENS THE BASAL-BOLUS INSULIN CONCEPT BASAL INSULIN CONTROLS GLUCOSE PRODUCTION BETWEEN MEALS AND OVERNIGHT NEAR-CONSTANT LEVELS USUALLY ~50% OF DAILY NEEDS BOLUS INSULIN (MEALTIME OR PRANDIAL) LIMITS HYPERGLYCEMIA AFTER MEALS IMMEDIATE RISE AND SHARP PEAK AT 1 HOUR POST MEAL 10% TO 20% OF TOTAL DAILY INSULIN REQUIREMENT AT EACH MEAL

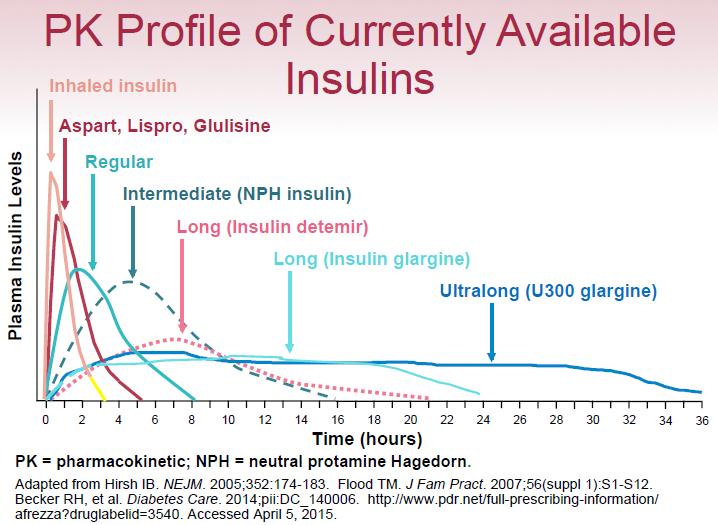
24 INSULIN ACTIONS
25 SUBCUTANEOUS INSULIN ADMINISTRATION Scheduled Sliding Scale Insulin only uses this component Basal Nutritional Correctional Total daily insulin needs Longacting insulin Rapid-acting insulin Trence DL, et al. J Clin Endocrinol Metab. 2003;88: Moghissi ES, et al. Endocr Pract. 2009;15: Moghissi ES. Curr Med Res Opin. 2010;26: Clement S, et al. Diabetes Care. 2004;27:
. 2013;41(2):45 53.")
26 GLUCOCORTICOIDS AND GLYCEMIC CONTROL Administration of glucocorticoids Adversely affects carbohydrate metabolism Worsens glycemic control in patients with diabetes Disproportionately affects postprandial glycemia Low Wang CC, Draznin B. Hosp Pract (1995). 2013;41(2):

27 INSULIN SUBCUTANEOUS POWER PLANS INSULIN SENSITIVITY: SENSITIVE: LEAN, ELDERLY, MALNOURISHED, RENAL IMPAIRMENT, TOTAL DAILY DOSE (TDD) <20 UNITS/DAY AVERAGE: TDD UNITS/DAY RESISTANT: OBESE, RECEIVING CORTICOSTEROIDS, EXPERIENCING SEVERE INFECTION, TDD > 40 UNITS/DAY ENHANCED: HIGH DOSE CORTICOSTEROIDS, BLOOD GLUCOSE TARGETS NOT MET BY THE RESISTANT SCALE


28 STRIKING THE RIGHT BALANCE Hyperglycemia Hypoglycemia
 SUCH AS REDNESS, SWELLING, AND ITCHING CAN HAPPEN.")
29 INSULIN INJECTION SITES BE SURE TO USE A DIFFERENT INJECTION SITE EACH TIME AND DO NOT OVERUSE ANY SITE. REACTIONS AT THE INJECTION SITE (LOCAL ALLERGIC REACTION) SUCH AS REDNESS, SWELLING, AND ITCHING CAN HAPPEN. DO NOT INJECT INSULIN INTO A SKIN AREA THAT IS RED, SWOLLEN, OR ITCHY.
30 REAL LIFE RESULTS OF INSULIN RESISTANCE INSULIN MORE INSULIN COMPLICATIONS COMPLICATIONS WITH HIGH DOSES OF INSULIN WEIGHT GAIN FLUID RETENTION INCREASED RISK OF HYPOGLYCEMIA EXPENSIVE MULTIPLE INJECTIONS DAILY ADHERENCE DIFFICULTIES PAIN LARGE VOLUME OF INJECTION UNPREDICTABLE ABSORPTION

31 NON INSULIN MEDICATIONS FOR TYPE 2 ~MORE APPLICABLE IN THE OBESE ALTERNATIVE TREATMENTS OF TYPE 2 DIABETES: Metformin GLP 1 TZD DPP4 GLP 1 TZD DPP4 GLP1 TZD s SGLT2 METFORMIN DECREASES GLUCOSE PRODUCTION BY THE LIVER. FIRST LINE MED FOR TYPE 2 GLP 1 GUT, LIVER, PANCREAS - INCREASES SATIETY LEVELS BY SLOWING DOWN GASTRIC EMPTYING, INCREASES INSULIN RELEASE WITH FOOD, SUPPRESSES GLUCAGON SGLT 2 DECREASES GLUCOSE REABSORPTION IN THE KIDNEY (LOWERS RENAL THRESHOLD) TZD MUSCLE INCREASES INSULIN SENSITIVITY TZD s DPP4 GUT, PROLONGS ACTION OF GUT HORMONES, INCREASES INSULIN SECRETION, DELAYS GASTRIC EMPTYING. GLP1



32 ARE WE CONFUSED YET
33 WHY ARE CONCENTRATED INSULINS NEEDED? INSULIN THERAPY PLAYS A CRITICAL ROLE IN THE TREATMENT OF TYPE 1 AND TYPE 2 DIABETES MELLITUS AND WE ARE LOOKING FOR THE PERFECT SUBSTITUTE TO ENDOGENOUS PHYSIOLOGIC INSULIN PRODUCTION.. DESIRE TO FIND A BASAL INSULIN WITH 24-HOUR COVERAGE WITH FLATTER AND LESS VARIABLE INSULIN EXPOSURE PROFILE DESIRE TO LIMIT OR ELIMINATE THE RISK OF HYPOGLYCEMIA PROVIDE CLINICALLY NECESSARY HIGH DOSES OF INSULIN IN LOW VOLUME INJECTIONS FOR INSULIN RESISTANT PATIENTS
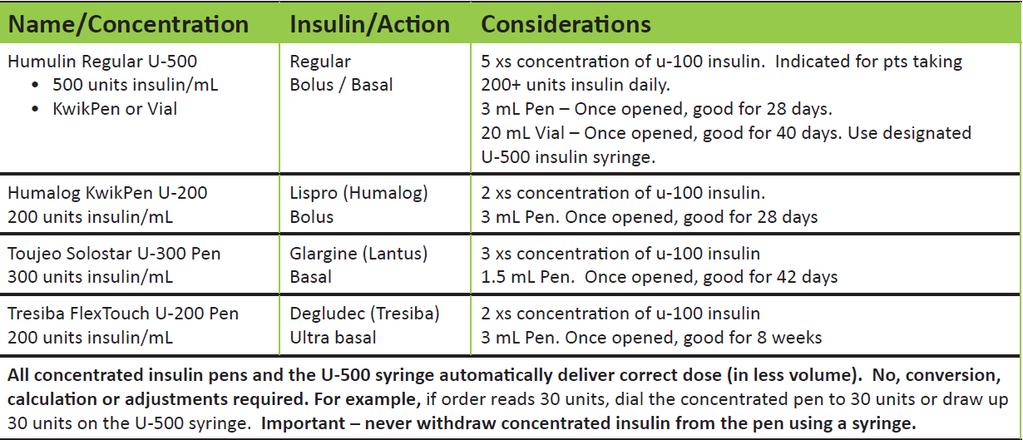
34 CONCENTRATED INSULIN

35 PROS AND CONS OF CONCENTRATED BASAL INSULIN THERAPY GLYCEMIC CONTROL WITH DEGLUDEC U200 AND GLARGINE U300 IS SIMILAR TO INSULIN GLARGINE U100 AND NOCTURNAL HYPOGLYCEMIA IS REDUCED NEWER CONCENTRATED BASAL INSULINS MAY OFFER AN ADVANTAGE IN TERMS OF REDUCED INTRAINDIVIDUAL VARIABILITY REDUCES THE INJECTION BURDEN IN INDIVIDUALS REQUIRING HIGH-DOSE AND LARGE VOLUME INSULIN THERAPY.
 3X Concentration of glargine u-100 insulin Cost : $300-$400 for 3 pens (450 units per 1.")
36 INSULIN GLARGINE U300 (TOUJEO ) SERUM INSULIN AND GIR PROFILE 60% of Gla-100 Exposed within the 1 st 12 hours Favorable basal insulin action providing sustained glucose lowering effect without increasing the risk for hypoglycemia Duration of Action is >30 hrs, Does not cause weight gain (-0.8%) 3X Concentration of glargine u-100 insulin Cost : $300-$400 for 3 pens (450 units per 1.5mL) Comes in a 1.5ml pen, once opened is good for 42 days Automatically delivers correct dose in less volume No Conversion calculation or adjustments required

37 TRESIBA FLEXTOUCH U-200 PEN Favorable basal insulin action providing sustained glucose lowering effect without increasing the risk for hypoglycemia Duration of Action is 42hrs, Does not cause weight gain (-1.3%) 2X Concentration of u-100 insulin Cost : $500 for 3 pens (600units per 3mL) Comes in a 3ml pen, once opened is good for 8 weeks Automatically delivers correct dose in less volume No Conversion calculation or adjustments required
 THIS CONCENTRATED INSULIN IS ESPECIALLY USEFUL FOR THE TREATMENT OF INSULIN")
38 U-500 INSULIN U-500R INSULIN HAS BEEN THE ONLY CONCENTRATED INSULIN AVAILABLE FOR USE SINCE THE 1950S HUMULIN-R U500 HAS A SIMILAR ONSET BUT LONGER DURATION OF ACTION COMPARED WITH U100 REGULAR INSULIN HUMULIN R U-500 CONTAINS 500 UNITS OF INSULIN IN EACH MILLILITER (5 TIMES MORE CONCENTRATED THAN HUMULIN R U-100) THIS CONCENTRATED INSULIN IS ESPECIALLY USEFUL FOR THE TREATMENT OF INSULIN RESISTANT PATIENTS WHO REQUIRE DAILY DOSES OF MORE THAN 200 UNITS PER DAY EXTREME CAUTION MUST BE OBSERVED IN THE MEASUREMENT OF DOSAGE BECAUSE INADVERTENT OVERDOSE MAY RESULT IN SERIOUS ADVERSE REACTION OR LIFE-THREATENING HYPOGLYCEMIA TO REDUCE THE RISK OF DOSING ERRORS THE ACTUAL DOSE FIELD SHOULD REFLECT BOTH UNITS AND VOLUME (IE.150 UNITS, 0.3ML) IN THE MAR COMES IN 3ML PEN (GOOD FOR 28 DAYS WHEN OPENED) AND 20 ML VIAL GOOD FOR 40 DAYS DOES CAUSE WEIGHT GAIN +4.9KG COST 6 MLS OF 500/ML (3) HUMULIN R U-500 KWIKPEN $ OR $1, FOR 20ML VIAL



39 COMPARISON OF U-100 ML SYRINGE WITH HUMULIN R U-100 AND HUMULIN R U-500 DOSE 39

40 SAFETY MEASURES REQUIRED WITH RU-500 Standardized CPOE, with alerts to Pharmacist and Diabetes Educator Pharmacy home dose verification of R U- 500 insulin on admission Caution: Patients home dose may need to be significantly reduced due to dietary restrictions in the hospital The only syringe approved for use with U-500 insulin Pharmacy dispenses pre filled Volumetric syringe to the unit Discuss discharge dose based on expected dietary intake in the home setting 40


41 INSULIN PUMP IS USEFUL FOR OBESE PATIENTS TO REDUCE THE TOTAL DAILY DOSE (TDD)
42
43 POST-ACTIVITY QUESTION #1 PLEASE MATCH THE INSULIN FORMULATION WITH THE PROPER BRAND NAME INSULIN: 1) Glargine U300 a) Tresiba 2) Degludec U200 b) Humulin R 3) Regular U500 c) Humalog U200 kwikpen 4) Insulin Lispro U200 d) Toujeo
44 POST-ACTIVITY QUESTION #2 WHAT ARE THE COMMON RESULT(S) WHEN INSULIN RESISTANT PATIENTS HAVE TO USE LARGE VOLUMES OF INSULIN? a) UNPREDICTABLE ABSORPTION b) INCREASE PAIN c) LESS DISCOMFORT AT SITE OF INJECTION d) INSULIN LEAKAGE FROM INJECTION SITE e) A, B AND D
45 POST-ACTIVITY QUESTION #3 WHAT IS A COMMON REASON FOR USING CONCENTRATED INSULIN FORMULATION? a) INSULIN ABSORPTION HAS BECOME UNPREDICTABLE b) REDUCTION IN DAILY INJECTIONS c) REDUCED VOLUME OF INJECTION d) ALL THE ABOVE
46 POST-ACTIVITY QUESTION #4 WHAT ARE SOME OF THE FACTORS THAT LEAD TO INSULIN RESISTANCE? a) OBESITY b) GENETICS, STRESS AND LIFESTYLE c) LACK OF EXERCISE d) REFINED CARBS e) ALL THE ABOVE
47 POST-ACTIVITY QUESTION #5 INSULIN RESISTANCE IS A CONDITION DEFINED BY? a) INCREASED LEVELS OF INSULIN b) IMPAIRED CELLULAR RESPONSE c) INABILITY TO FACILITATE ENTRY OF GLUCOSE INTO THE CELL d) ALL THE ABOVE
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance
 in severe insulin resistance") Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance Jodie S. Gee, Pharm.D., BCACP, CDE Clinical Pharmacy Specialist-Ambulatory Care Harris Health System Objectives To be
Safe use of insulin regular concentrated (500 units/ml) in severe insulin resistance Jodie S. Gee, Pharm.D., BCACP, CDE Clinical Pharmacy Specialist-Ambulatory Care Harris Health System Objectives To be
Diabetes Head to Toe May 31, 2017
 Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Innovations in Insulin Joanne Reid RN CDE jmreid@gbhs.on.ca Danielle Benedict RPh Outline Setting the stage Insulin as pancreas replacement therapy Commonly used insulins New insulins Case Studies Dosing
Insulin Prior Authorization with optional Quantity Limit Program Summary
 Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Insulin Prior Authorization with optional Quantity Limit Program Summary 1-13,16-19, 20 FDA LABELED INDICATIONS Rapid-Acting Insulins Humalog (insulin lispro) NovoLog (insulin aspart) Apidra (insulin glulisine)
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
INSULIN 101: When, How and What
 INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
INSULIN 101: When, How and What Alice YY Cheng @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Tips and Tricks for Starting and Adjusting Insulin. MC MacSween The Moncton Hospital
 Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Tips and Tricks for Starting and Adjusting Insulin MC MacSween The Moncton Hospital Progression of type 2 diabetes Beta cell apoptosis Natural History of Type 2 Diabetes The Burden of Treatment Failure
Newer Insulins. Boca Raton Regional Hospital 15th Annual Internal Medicine Conference
 Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
Newer Insulins Boca Raton Regional Hospital 15th Annual Internal Medicine Conference Luigi F. Meneghini, MD, MBA Professor of Internal Medicine, UT Southwestern Medical Center Executive Director, Global
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins. Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP
 These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
These Aren t Your Average Rookies: A Primer on New and Emerging Insulins Alissa R. Segal, Pharm.D, CDE, CDTC, FCCP Disclosures Eli Lilly & Company: Advisory board member Boehringer Ingelheim: Advisory
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy
 Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Update on New Basal Insulins and Combinations: Starting, Titrating and Adding to Therapy Jerry Meece, BPharm, CDE, FACA, FAADE Director of Clinical Services Plaza Pharmacy and Wellness Center Gainesville,
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
INSULIN OVERVIEW. Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro min. 3-5 hrs min.
 INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
INSULIN OVERVIEW Type Brand Name Onset Peak Duration Role in glucose management Page Rapid-Acting lispro Humalog 15-30 min 30-90 min 3-5 hrs aspart glulisine Short-Acting Regular insulin NovoLog Apidra
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI
 Trial Treatment Protocols. Askiel Bruno, MD, MS Protocol PI") Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
Stroke Hyperglycemia Insulin Network Effort (SHINE) Trial Treatment Protocols Askiel Bruno, MD, MS Protocol PI SHINE Synopsis Acute ischemic stroke
DEMYSTIFYING INSULIN THERAPY
 DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
DEMYSTIFYING INSULIN THERAPY ASHLYN SMITH, PA-C ENDOCRINOLOGY ASSOCIATES SCOTTSDALE, AZ SECRETARY, AMERICAN SOCIETY OF ENDOCRINE PHYSICIAN ASSISTANTS ARIZONA STATE ASSOCIATION OF PHYSICIAN ASSISTANTS SPRING
Basal-Bolus Insulin Therapy. Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January
 Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
Basal-Bolus Insulin Therapy Veronica Brady, PhD, FNP-BC, BC-ADM, CDE ECHO January 18 2018 Terminology No longer using the term diabetic. Diabetes does not define people. People with diabetes are individuals
8/13/2016. Insulin Basics. Rapid-Acting Insulin Analogs. Current Insulin Products and Pens. Basal Insulin Analogs. History of Insulin Therapy
 Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Insulin Basics Anabolic hormone involved in metabolism Following carbohydrate ingestion insulin release is stimulated Suppresses hepatic glucose production Stimulates peripheral glucose uptake Commercially-available
Mixed Insulins Pick Me
 Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Mixed Insulins Pick Me Alvin Goo, PharmD Clinical Associate Professor University of Washington School of Pharmacy and Department of Family Medicine Objectives Critically evaluate the evidence comparing
Providing Stability to an Unstable Disease
 Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
Basal Insulin Therapy Providing Stability to an Unstable Disease Thomas A. Hughes, M.D. Professor of Medicine - Retired Division of Endocrinology, Metabolism, and Diabetes University of Tennessee Health
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Starting and Helping People with Type 2 Diabetes on Insulin
 Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Starting and Helping People with Type 2 Diabetes on Insulin Elaine Cooke, BSc(Pharm), RPh, CDE Pharmacist and Certified Diabetes Educator Maple Ridge, BC Objectives After attending this session, participants
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Related Disclosures
 Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Diabetes Related Disclosures Speakers Bureau Amylin Boehringer Ingelheim Eli Lilly Takeda Classification of Diabetes Diabetes Care January 2011 vol. 34 no. Supplement 1 S11-S61 Type 1 Diabetes Mellitus
Inpatient Glycemic Management:
 Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
Disclosure to Participants Conflict of Interest (COI) and Financial Relationship Disclosures: Dr. Seley attended Advisory Board Meeting: Alliance (Boehringer-Ingelheim/Lilly) Bayer Diabetes Care Sanofi
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION
 INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
INSULIN INITIATION AND INTENSIFICATION WITH A FOCUS ON HYPOGLYCEMIA REDUCTION Jaiwant Rangi, MD, FACE Nov 10 th 2018 DISCLOSURES Speaker Novo Nordisk Sanofi-Aventis Boheringer Ingleheim Merck Abbvie Abbott
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
ANNUAL MEETING 2 #FSHP2017
 FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
FSHP Disclosure Strategies for Glycemic Management in the Inpatient Setting: Guidelines vs. Reality Melissa Marshall, PharmD, BCPS Jeffrey Ruff, PharmD We do not have (nor does any immediate family member
9/16/2013. No Conflict of Interest to Disclose
 Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Catie Prinzing MSN, APRN, Clinical Nurse Specialist September 27, 2013 No Conflict of Interest to Disclose List key concepts to determining patient insulin doses during transitions in care Identify 5 points
Current Trends in Diagnosis and Management of Gestational Diabetes
 Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
Current Trends in Diagnosis and Management of Gestational Diabetes Shreela Mishra, MD Assistant Clinical Professor UCSF Fresno Medical Education Program 2/2/2019 Disclosures No disclosures 2/2/19 Objectives
associated with serious complications, but reduce occurrences with preventive measures
 Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Wk 9. Management of Clients with Diabetes Mellitus 1. Diabetes Mellitus body s inability to metabolize carbohydrates, fats, proteins hyperglycemia associated with serious complications, but reduce occurrences
Learning Objectives. Are you ready for more insulin formulations?
 Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
Are you ready for more insulin formulations? Shara Elrod, PharmD, BCACP, BCGP Learning Objectives Review pharmacology and dosing of new insulin formulations Compare and contrast new insulin formulations
INJECTABLE THERAPIES IN DIABETES. Barbara Ann McKee Diabetes Specialist Nurse
 INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
INJECTABLE THERAPIES IN DIABETES Barbara Ann McKee Diabetes Specialist Nurse 1 Aims of the session Describe the different injectable agents for diabetes and when they would be used. Describe some common
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
4/2/2018. Human U-500 insulin Learning Objectives. Dr. Ken Cathcart FACE
 Human U-500 insulin 2018 Dr. Ken Cathcart FACE Learning Objectives Participants will be able to identify when it is appropriate to use U500 insulin Participants will be able to state how to determine a
Human U-500 insulin 2018 Dr. Ken Cathcart FACE Learning Objectives Participants will be able to identify when it is appropriate to use U500 insulin Participants will be able to state how to determine a
Objectives. Navigating New Insulins. Disclosures. Diabetes: The Stats. Normal Insulin Release Individuals without diabetes. History of Insulin 5/23/17
 Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
Objectives Compare and contrast currently available products. Navigating New s Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center Determine the factors
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Insulin Regimens: Hitting Glycemia Targets
 Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
Insulin Regimens: Hitting Glycemia Targets Grant Kelley MD March 1 st, 2018 Faculty Disclosure: Financial relationships with commercial interests None Overview Mortality and Morbidity Insulin and Insulin
INSULIN THERAY دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد
 INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
INSULIN THERAY DIABETES1 IN TYPE دکتر رحیم وکیلی استاد غدد ومتابولیسم کودکان دانشگاه علوم پزشکی مشهد Goals of management Manage symptoms Prevent acute and late complications Improve quality of life Avoid
Management of Gestational Diabetes
 Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Management of Gestational Diabetes A Diabetes risk assessment should be ascertained at the First prenatal visit. Low Risk: Early blood glucose screening is NOT routinely required if most of the following
Insulin Management. By Susan Henry Diabetes Specialist Nurse
 Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Insulin Management By Susan Henry Diabetes Specialist Nurse The Discovery of Insulin - 1921 - Banting & Best University Of Toronto Discovered hormone insulin in pancreatic extract of dog - Marjorie the
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption),
,") Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς
 Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Αναγκαιότητα και τρόπος ρύθμισης του διαβήτη στους νοσηλευόμενους ασθενείς Αναστασία Θανοπούλου Επίκουρη Καθηγήτρια Β Παθολογικής Κλινικής Πανεπιστημίου Αθηνών Διαβητολογικό Κέντρο, Ιπποκράτειο Νοσοκομείο
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES
 PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
PHARMACISTS INTERACTIVE EDUCATION CASE STUDIES Disclaimer: The information in this document is not a substitute for clinical judgment in the care of a particular patient. CADTH is not liable for any damages
Nph insulin conversion to lantus
 Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
Nph insulin conversion to lantus Search 26-2-2003 RESPONSE FROM AVENTIS. We appreciate the opportunity to respond to Dr. Grajower s request for information regarding Lantus ( insulin glargine [rdna origin.
DIABETES EDUCATION FOR HEALTH CARE SERIES
 American Association of Diabetes Educators Provider is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation. DIABETES EDUCATION
American Association of Diabetes Educators Provider is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation. DIABETES EDUCATION
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary
 Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Number 14 Effective Health Care Comparative Effectiveness, Safety, and Indications of Insulin Analogues in Premixed Formulations for Adults With Type 2 Diabetes Executive Summary Background and Key Questions
Type I Type II Insulin Resistance
 Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Insulin An aqueous hormonal solution made in the pancreas. Affects metabolism by allowing glucose to leave the blood and enter the body cells, preventing hyperglycemia. It is measured in units, e.g. 100
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Evidence for Basal Bolus Insulin Versus Slide Scale Insulin
 Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
Curr Emerg Hosp Med Rep (2014) 2:26 34 DOI 10.1007/s40138-013-0032-4 DIABETES AND METABOLIC DISEASE (W FORD, SECTION EDITOR) Evidence for Basal Bolus Insulin Versus Slide Scale Insulin Sameer Badlani William
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
There have been important changes in diabetes care which may not be covered in undergraduate textbooks.
 Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Diabetes Clinical update There have been important changes in diabetes care which may not be covered in undergraduate textbooks. Changes in the diagnosis of diabetes a) HbA1C Since 2011, World Health Organisation
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes
 Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Transition of Care in Hospitalized Patients with Hyperglycemia and Diabetes Critically ill patients in the ICU Hospital Non-ICU Settings Home Guillermo E Umpierrez, MD, FACP, FACE Professor of Medicine
Position Statement of ADA / EASD 2012
 Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Management of Hyperglycemia in Type2 Diabetes: A Patient- Centered Approach Position Statement of ADA / EASD 2012 Cause of : Type 2 diabetes Cardiovascular disorders Blindness End-stage renal failure Amputations
Guide to Starting and Adjusting Insulin for Type 2 Diabetes*
 Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Guide to Starting and Adjusting Insulin for Type 2 Diabetes* www.cadth.ca * Adapted from Guide to Starting and Adjusting Insulin for Type 2 Diabetes, 2008 International Diabetes Center, Minneapolis, MN.
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
Basal Bolus Insulin Therapy Frequently Asked Questions
 1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
1. What is Basal Bolus Insulin Therapy (BBIT)? 2. What evidence supports the use of subcutaneous Basal Bolus Insulin Therapy? 3. Does Basal Bolus Insulin Therapy apply to all patients? 4. What s wrong
Initiation and Adjustment of Insulin Regimens for Type 2 Diabetes
 Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
Types of Insulin Rapid-acting insulin: lispro (Humalog), aspart (NovoRapid), glulisine (Apidra) Regular short-acting insulin: Humulin R, Novolin ge Toronto, Hypurin Regular Basal insulin: NPH (Humulin
4/16/2018. Flexible Intensive Insulin Therapy (FIIT) in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures
 in People with Type 2 Diabetes: A Viable Option. Disclosures. Outline. No financial disclosures") Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
Flexible Intensive Insulin Therapy (FIIT) in People with Type Diabetes: A Viable Option Kim Bisanz, MFCS, RDN, LDN, CDE Minnesota Academy of Nutrition & Dietetics Annual Meeting April 19, 18 18 MFMER slide-1
5/15/2018 DISCLOSURE OBJECTIVES. FLORIDA HOSPITAL ORLANDO Not for profit organization Acute care medical center 1,368 licensed beds BACKGROUND
 DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
DISCLOSURE PHARMACIST DIRECTED MANAGEMENT OF GLUCOCORTICOID INDUCED HYPERGLYCEMIA AT A LARGE COMMUNITY HOSPITAL Jill Zaccardelli, PharmD PGY1 Pharmacy Resident Florida Hospital Orlando Jill.Zaccardelli@flhosp.org
Rebecca Newberry APRN MS CDE
 Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Disclosure 1/16/2017. Michael R. Brennan D.O., M.S., F.A.C.E Director Beaumont Endocrine Center Chief of Endocrine Beaumont Grosse Pointe 1/16/2017 2
 Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
Therapy For Diabetes Michigan Association of Osteopathic Family Physicians Mid-Winter Family Medicine Update Shanty Creek Resort, MI January 19-22nd 2017 Michael R. Brennan D.O., M.S., F.A.C.E Director
A Children s Bedtime Story
 A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
A Children s Bedtime Story Setting: University Medical Center, Big Town, USA Scenario: 0500, last admission of the night, 10 previous admissions, all tucked in for the night Patient: 75 year old male with
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Converting lantus to humalog 75 25
 P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
P ford residence southampton, ny Converting lantus to humalog 75 25 This page includes the following topics and synonyms: Insulin Dosing in Type 2 Diabetes, Insulin Dosing in Type II Diabetes. Thiazide
MANAGEMENT OF TYPE 1 DIABETES MELLITUS
 MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
MANAGEMENT OF TYPE 1 DIABETES MELLITUS INVESTIGATIONS AND TREATMENT MANSI NAIK VII SEMESTER INVESTIGATIONS FASTING BLOOD SUGAR PLASMA GLUCOSE HEMOGLOBIN A 1c SYMPTOMS OF TYPE 1 DIABETES MELLITUS Polyuria
Lantus levemir conversion
 Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Lantus levemir conversion Search Learn about starting insulin-naïve patients with type 2 diabetes on Levemir. Read Important Safety & Prescribing Info on the HCP Website. Lantus and Levemir have a variety
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Conversion from lantus to tresiba
 Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
Conversion from lantus to tresiba Search dosages for Diabetes Type 2 and Diabetes Type 1; plus renal, liver and. Forecast your health care. Every time you have a symptom or are diagnosed of a condition,
How they work and when to take them. Diabetes Medications
 How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
How they work and when to take them Diabetes Medications BIGUANIDES Metformin Actions Slows down the release of glucose from the liver. Helps the bodies cells become more sensitive to insulin. Pros Weight
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC)
") BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
BEDFORDSHIRE AND LUTON JOINT PRESCRIBING COMMITTEE (JPC) June 2017 Review: June 2020 (earlier if required see recommendations) Bulletin 255: Insulin aspart New Formulation - Fiasp JPC Recommendations:
Self-Monitoring Blood Glucose (SMBG) Frequency & Pattern Tool
 Frequency & Pattern Tool") Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Self-Monitoring Blood Glucose () Pattern Recommendation: Basal Insulin Only (To Target) NPH or long-acting analogue, typically given at. at least as often as is being given. Optional, less frequent can
Management of Diabetes New Concepts New Devices New Medications. Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth
 Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
Management of Diabetes New Concepts New Devices New Medications Richard J. Comi, MD Professor of Medicine Geisel School of Medicine at Dartmouth Objectives: At the end of this lecture, the learner will
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Disclosures. Learning Objectives 4/26/2017
 Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
Implementation of a quality improvement initiative to ensure the safe transition from prior-to-admission concentrated insulins to a formulary insulin regimen ERICA J. RHEIN, PHARMD PGY1 PHARMACY PRACTICE
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
BEST 4 Diabetes. Optimisation of insulin module
 BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
BEST 4 Diabetes Optimisation of insulin module Confidence and competence Where would you rate yourself? Why do all of our patient not achieve optimal blood glucose control? Insulin Therapy Goals and Purpose
Diabetes in Pregnancy
 Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Diabetes in Pregnancy Ebony Boyce Carter, MD, MPH Division of Maternal Fetal Medicine Washington University School of Medicine Disclosures I have no financial disclosures to report. Objectives Review the
Learning Objectives. Perioperative SWEET Success
 Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
Perioperative SWEET Success PERIOPERATIVE SWEET SUCCESS PRESENTED BY: KENDRA MARTIN, RN, BSN, CDE JENNIFER SIMPSON, RN, BC-ADM, MSN, CNS Disclosure to Participants Notice of Requirements For Successful
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Diabetes: What is the scope of the problem?
 Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
Diabetes: What is the scope of the problem? Elizabeth R. Seaquist MD Division of Endocrinology and Diabetes Department of Medicine Director, General Clinical Research Center Pennock Family Chair in Diabetes
LET S TALK INSULIN THE BASICS
 LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
LET S TALK INSULIN THE BASICS AUTHOR S DISCLOSURES Contracted for program development for Lifescan Canada Speaker for Lifescan, Lilly, BI, Consultant for Lilly, Janssen, Novo Nordisk, Lifescan Canada OBJECTIVES
HAP PA-HEN Achieving More Together
 HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
HAP PA-HEN Achieving More Together Managing Hyperglycemia in the Hospital: Strategies for Safe and Effective Care Pennsylvania Patient Safety Authority Managing Hyperglycemia in the Hospital: Strategies
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free