FOOTPAD. S J Fratesi MD FRCS MMED June 2010 Quo Vadis? (where are we going?)
|
|
|
- Bertram Booker
- 5 years ago
- Views:
Transcription


1 FOOTPAD S J Fratesi MD FRCS MMED June 2010 Quo Vadis? (where are we going?)
2 8 commandments of foot care 1) Wash daily Thou shalt. 1) Inspect and lubricate daily 1) Diligent nail care 1) Proper fitting footwear 1) Regular activity and diet 1) Avoid common mistakes and be careful 7 ) Regular medical visits

3 FOOTPAD F..Foot O..Optimal O..Outcomes T.. Treatments P..People A.Algoma D.Diabetes

4
5 Ontario Diabetes database Ø burden of disease prevalence, incidence, mortality Ø process of care * screening, access, glucose control Ø outcomes of care * complications, procedures Identify DM in special populations *quality of care index
6 Burden of Diabetes vs no Diabetes Significant increase in hospital admissions for acute MI Significant increase in stroke Leading cause of new dialysis Leading cause of limb amputations
7 Burden of Disease Two million Canadians have diabetes 31% increase in prevalence over 5 years primarily due to persons living longer with DM incident (newly diagnosed) cases steady
8 Mortality and Morbidity q life expectancy with DM is about 13 years less than without DM. 12% of men with DM and 18% of women need assistance with routine activities Three year mortality after first amputation is 50 %

9 Foot Disease is the Most Common Complication of Diabetes Leading to Hospitalization (Reiber and Kosak)
10 Independent Risk Factors for PAD* Relative Risk vs the General Population Reduced Increased 4.05 Diabetes 2.55 Smoking Hypertension Total cholesterol (10 mg/dl) * PAD diagnosis based on ABI <0.90. Newman AB, et al. Circulation. 1993;88:
11 15% of diabetics will develop a foot ulcer in their lifetime amputation in the diabetic is times higher than the non-diabetic every year 1 in every 250 diabetics will undergo amputation 85% of all amputations in diabetes are preceded by an ulcer
12 60 % of diabetics with foot ulceration have neuropathy without clinically significant arterial disease 20% have ulcers primarily due to arterial disease 20 % have ulcers secondary to a combination of both neuropathy and arterial disease
13 A proactive approach should reduce the burden of this disease, improve health through prevention of complications, and reduce the financial burden Bakker (2005) states that diabetic foot problems are a threat to every individual diabetes. Worldwide there are a million amputations per year in individuals with diabetes.
14 Complications of Diabetes 30% decrease in hospital admissions for elevated blood sugar levels 75% decrease in admissions for low blood sugar levels
15 Foot care is often described as the Cinderella complication of diabetes. Prevention and ulcer treatment may be based on local custom and practice Many false perceptions about diabetic foot problems, how to recognize and treat Urgent need for a systematic review of the evidence to inform practice, to highlight the steps that can be taken to prevent amputation, and to improve care.
16 The number of individuals with diabetes in Canada documented in 2005 surpassed the levels predicted for year 2030 (Lipscombe 2007). Sixty percent of all amputations are in patients with diabetes, many of which are preventable. Northern Ontario has several cluster areas of increased diabetes and diabetes-associated complications.
17 The complication rate of diabetes is not well monitored in Canada (Harris 2003) Canadians with diabetes are not well monitored for foot conditions Globally, there is no standardization of primary foot care in diabetes.
18 There is significant variability in foot care assessment and risk classification potentially leading to inappropriate care. Thompson (2005)
19 Almost 2 million Canadians have diabetes In amputated diabetics 50% develop ulcers in the contralateral limb <2 years 50% contralateral amputation within 5 years 3 year mortality after 1st amputation..50%


20
21 Reflection Reflection as a method of learning and quality improvement (multi-professional) Reflection in Action Reflection on Action
22 Care of the foot with diabetes (Algoma) Ø Is there a problem? Ø Why does it exist? Ø What is the cause of the problem? Ø Is the problem preventable? Ø Is the problem modifiable? Ø What can be done to make it better?
23 Good Health Outcomes in Diabetes (GHOD SCORE) Process outcomes BP within 6 mo HbA1c within 6mo Lipids annually Albuminuria annually Foot exam within 1yr ( From 6 months) Eye exam within 1yr ( from 2yrs) On ACE/ARB On ASA/antiplatelet On Statins Clinical outcomes BP within 6 mo and <=130/80 mmhg HbA1c within 6 mo and <=.07 Lipids annually and LDL < 2.5
24 Where s the evidence? Lack of evidence affects the treatment of established foot ulcers Most carried out in secondary care settings Well-designed multi-center studies, with sufficient numbers of similar ulcers and appropriate randomization needed
25 Major predisposing factors Neuropathy PVD Limited joint mobility High plantar pressure Bony deformity History of previous ulceration Visual or functional impairment


26

27

28
29


30

31
32

33

34
35

36

37

38

39

40

41

42
43

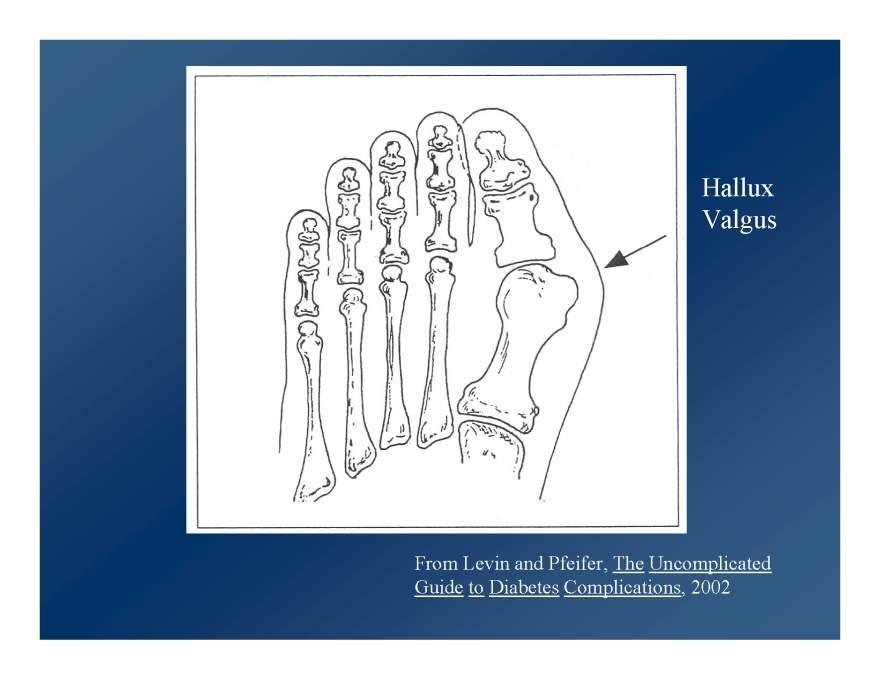
44 Common sites develop over bony prominences

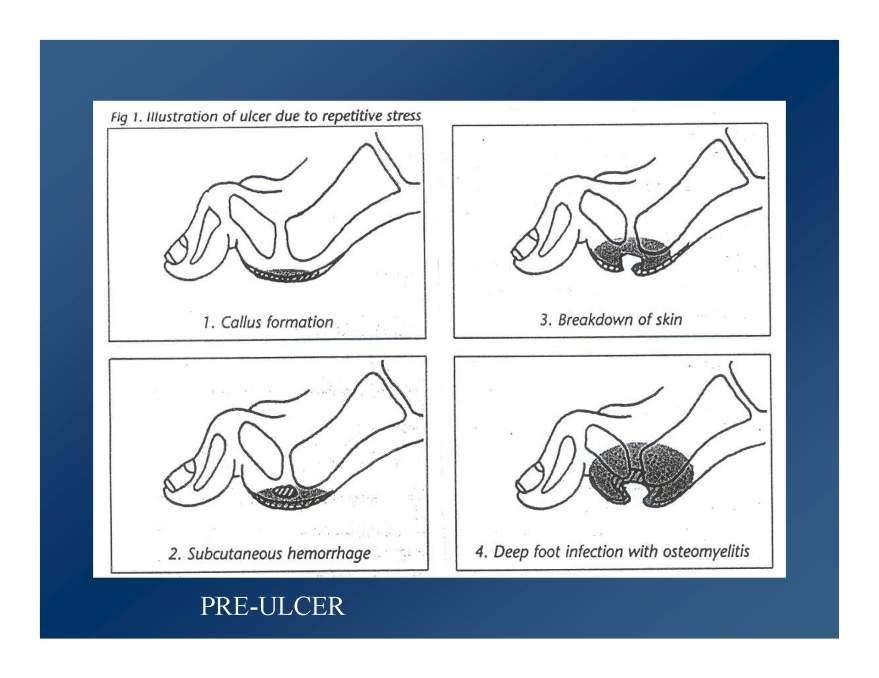
45 The process can get out of hand

46 The above is both livable and workable
47 There is strong evidence to support foot care is best done with a multidisciplinary approach The majority of amputations begin as an ulcer 85% of ulcers may be prevented.
48
49 Position statement 2005 IDF advocated for annual foot inspection, identification of the foot at risk, education of both professionals and individuals with diabetes, proper footwear as well as rapid treatment of all foot pathology.
50 Why guidelines work St Vincent Declaration (UK ) 50% reduction LEAP Program (USA) Annual exam to assess risk Intensive follow-up/education of at risk Prompt referral to multidisciplinary team
51 FOOTPAD: Foot care Optimal Outcomes and Treatment for Patients in Algoma with Diabetes Program
52 FOOTPAD initiative Establish a comprehensive, practical and evidence-based program for optimal foot care for all patients with diabetes in Algoma district. The mission statement adopted was FEET, support for life. It was hoped that a proactive approach to diabetic foot care would allow the people of Algoma access to a consistent and multidisciplinary foot care service including preventative measures and education.
53 Neuro assessment is pivotal Grade A recommendation to regular foot inspection for sensation and circulation. This is best done by testing the sensation with a monofilament or biothesiometer or tuning fork, palpation of pulses, inspection of deformity
54 Algoma district initiative The premise of FOOTPAD is that many foot related problems in diabetes are PREDICTABLE and therefore, PREVENTABLE. Early intervention in the insensate foot (PREDICTABLE) will result in less diabetic foot-related problems (PREVENTABLE). Fewer amputations will lower the burden of this health problem on our health care system. Even a trivial callus or blister should not be ignored.

55
56 FOOTPAD Patient centered Community oriented Multi-professional Standardized Seamless Evidence based Electronically supported
57
58 Basic assessment tool The basic sixty second foot exam (Armstrong 1998) with a few simple questions to answer with guidelines on clinical examination and documentation, including use of the 10 g monofilament test (Semmes-Weinstein monofilament test). This is a simple process of looking, feeling, testing and documenting as outlined in the protocol document
59
60 Advanced assessment tool A checklist assessing the presence, absence and nature of pain, pulsation and structural deformity. As well, capillary refill, skin condition and colour are described with the provided checklist
61
62 FOOTPAD was developed as both an educational tool and evidencebased program for primary foot care in diabetes. FOOTPAD was designed to show how evidence fashions best practice guidelines in diabetes
63 FOOTPAD will teach practitioners how to predict with a view to prevent. FOOTPAD is a sound, locally adaptable, evidence based guideline for foot care in diabetes. Health care professionals are encouraged to use it as best practice and as part of their continuing professional development.
64 85% of leg amputations in the diabetic preceded by a foot ulcer Major cause of a diabetic related hospital admission is a foot related problem
65 Multifactorial etiology of diabetic foot ulcer neuropathy Arterial insufficiency impaired cell immunity Non-compliance diabetic foot ulcer infection trauma


66 Diabetic ulcers


67 Diabetic neuropathy Skin abnormality,immune deficiency poor circulation Continuous/repetitive trauma Foot deformity/abnormal pressure points

68 METARSAL HEAD PROMINENCE AND ULCERATION ulceration is over the plantar surface of the metatarsal heads.


69 HAMMER-TOE DEFORMITY Claw-toe deformity with loss of function of intrinsic muscles of foot

70 CHARCOT'S FOOT Progressive neuropathy + Repetitive trauma + osteoporosis

71 Charcot's foot

72 ISCHEMIC FOOT ULCER This patient has previously had most of the toes of this foot removed because of gangrene but has failed to heal one of the amputation sites due to persistent ischemia which originated in the calf arteries.

73 ISCHEMIC FOOT ULCER
74 Diabetic ulcer risk Peripheral neuropathy Foot deformity Limited joint movement Elevated plantar pressure Prior ulcer/amputation Peripheral vascular disease Susceptibility to infection


75 Insensate foot
76 Tissue loss in the diabetic foot High foot pressure Callus/trauma ulceration Diabetic foot amputation Failure to heal infection


77 Amputations in Persons with DM
78 Footpad in holding pattern????? Footpad audit after 18 month launch
79
80
81
82
83
84 The NICE Guidelines There is level 1 evidence to support recall and regular review as part of ongoing care in the management of foot care in diabetes. As part of that review, trained personnel should establish and document risk There is level 1 evidence to support structured education in diabetes as part of foot examination and monitoring
85 EVIDENCE based medicine Only two recommendations were found based on level 1 evidence. These included the importance of a physical examination to assess risk (should be performed by a health care professional) and that all people with diabetes should receive basic foot care education. All other recommendations were based on level 4 evidence
86 Diabetes increases the risk of foot ulceration. Appropriate screening with intervention measures may reduce this risk. Screen all patients with diabetes to assign the patient to a risk category that dictates both the method and frequency of foot interventions. (Rollins 2000).
87 These interventions may reduce the risk of ulceration and possible amputation and are supported by a varying degree of evidence (Singh 2005). include education of both patient and allied health care workers optimizing glycemic control, smoking sensation possible prescription of footwear.
88 More evidence to support care of the diabetic foot in the community (primary care ) directed at ulcer prevention Recommendations based on evidence regular annual foot examination detection of feet at risk of ulceration appropriate education.
89 Initial diabetes assessment Check for foot deformity Check for pulses check for sensation (10g or vibration) Check shoes MUST BE DONE AT INITIAL ASSESSMENT THEN YEARLY Assign risk status( OOOPPS!!!!)
90 Prevention Check feet at every visit shoes/socks off Neurological examination.pinprick, reflexes, tuning fork, monofilament test* Vascular assessment.. popliteal pulse, ABI. Evaluate according to risk status
91 Risk status qpatient currently does not have an ulcer LOW - risk normal sensation, pulses, no deformity MODERATE -neuropathy or absent pulse or other risk SEVERE -neuropathy or absent pulse, deformity or previous ulcer
92 Risk assessment Nice guidelines LOW -annual assessment, education, footwear MODERATE HIGH assessment -3-6 month assessment -foot education/inspection -evaluate foot wear /circulation -1-3 months -foot assessment /circulation -intensified foot care education, specialized footwear, skin and nail care
93 Risk Identification Fundamental for effective preventive management in people diabetes The risk of ulcers or amputations is increased diabetes X 10 years male poor glucose control cardiovascular, retinal, or renal complications
94 Major predisposing factors Neuropathy PVD Limited joint mobility High plantar pressure Bony deformity History of previous ulceration Visual or functional impairment
95 Assessment of foot risk The classification of the foot into low, medium and high risk was supported by a grade C recommendation. Regular review by a foot protection team based on risk at 3, 6, and 12 monthly intervals was supported by grade C/D recommendations.
96 Five Key Risk Factors Presence or history of foot ulcers Protective sensation Structural abnormalities Circulation Self-care knowledge and behaviour Primary care can make a difference
97 Screening annual screen of everyone with diabetes for foot risk by inspection, palpation of pulses, and insensitivity to the 10g nylon monofilament is reinforced by this guideline (A). takes only minutes requires no expensive equipment doesn't matter who does it as long as it gets done.
98 Accommodative shoes Getting the right fit Major cause of trauma Ulcers often from shoes.constant pressure of 5-7 pounds per square inch over a bony prominence leads to necrosis within 7 hours
99 At risk foot at-risk individuals should receive extra foot care education and frequent review to prevent the development of ulceration. This strategy reduces morbidity and is cost- effective. (Ib)
100 Patient Education EMPOWERMENT Goal Oriented Problem Centered Offers Feedback Group Discussion Varied Presentation
101 Wagner s classification of foot ulcers Grade 0..the at risk foot Grade 1.superficial ulcer Grade 2.penetrating ulcer Grade 3 complicated by infection Grade 4.gangrene not requiring total foot amputation Grade 5 gangrene requiring leg amputation Above classification assessed in context of sufficient blood supply to heal
102 SAH Topical Wound Overview RED YELLOW BLACK assessment after proper cleansing

103 Where do you start?
104 6 simple questions Where is the infection/ulcer? How bad is it? How did it get there? What can be done to make it better? What can be done to make sure it does not recur? What are the co-morbid conditions?
105 Factors that may affect healing in the diabetic patient: Metabolic control Infection Ischemia Continuing trauma Patient education and compliance Concurrent medical problems/medication Wound environment Multidisciplinary foot care program
106 Atherosclerosis of the lower limb in the diabetic: Diabetes>20 years > 50% lose peripheral pulse Diabetics have small vessel disease plus more trifurcation disease than non-diabetics Distal revascularization has saved many diabetic limbs Smoking + diabetes = amputation


107 Wound Etiology


108 Case study 70-year-old male Previous leg ulcer Smoker claudicates Absent pulse What is your most likely diagnosis?
109 Arterial ulcer in a diabetic? OR diabetic ulcer in an arteriopath? Does it matter? Is RX same?
110 Skin breakdown due arterial causes.risk factors Diabetes Tobacco Hyperlipidemia Hypertension Obesity Cardiac disease Renal disease COPD Coagulation disorders
111 Arterial wound management objectives Keep clean Keep dry? Debride necrotic tissue Manage exudate by hydration Protect from mechanical/thermal trauma Protect from infection
112 Initial conservative measures General measures Loose weight Exercise QUIT SMOKING Pharmacologic agents.trental,adalat,asa, Ischemic bed routine
113 Investigations History Clinical examination Non-invasive arterial study(abi<.3,>.6) Arteriogram(done only if surgery is entertained)
114 Clinical assessment( Documentation of pulses/intensity Skin nutrition,ulcer, fissure,cold paronychia,temperature of foot Pallor with elevation/rubor with dependency Prolonged venous filling time

115

116

117 ANGIOGRAPHY IN DIABETES
118 Surgery Angioplasty Angioplasty/stent Bypass procedure inflow/outflow*
119 Neurological assessment of diabetic ankle reflexes vibration sensation pain sensation Diminished protective sensation to monofilament testing (10 gram / 5.07 mm Semmes-Weinstein)?

120


121 USE OF 10-GRAM MONOFILAMENT
122 Factors to enhance wound environment in diabetic patients with foot ulceration: Aggressive debridement to remove necrotic tissue and slough Control of infection Optimize oxygenation Avoidance of further trauma Ulcer dressings and topical wound therapy
123 Infections in diabetic foot ulcers: Foot infection is a common cause for diabetic hospitalization An altered immune responses may mask the clinical severity of infections. Less than 50 % with limb threatening infections have a significant fever or elevated WBC count. ice berg effect quite common
124 Infected diabetic foot ulcers: Deep tissue infections: mono-microbial infections occur in only about 20% of cases on average, deep tissue infections will grow five different bacterial species Superficial infections: milder infections have fewer bacteria: mean of 2.1 different bacterial species gram positive cocci most common bacteria but are sole pathogen in less than 50% of patients
125 Infected diabetic foot ulcers: The importance of aerobic/anaerobic culture The more serious the infection, the higher the probability of multiple organisms particularly if a deep infection Milder infections tend to have fewer organisms particularly if superficial Gm(+) cocci is the most common but is the lone ranger in<50%
126 Diabetic foot ulcers and use of antiseptics: Antiseptics are reactive chemicals that indiscriminately destroy bacteria as well as healthy granulation tissue in wounds. There is no magical, topical antiseptic that will selectively kill bacteria without harming healing cells in the wound base.
127 Wound culture techniques: surface cultures from diabetic wounds may not correlate well with deeper culture techniques Deep needle aspiration via non-infected area usually correlates with deep infections The most reliable cultures taken from biopsy or swab after the surface exudate has been removed. Important to distinguish contamination from infection Organisms usually poymicrobial

128 Wound Assessment All wounds should be probed for extent and hidden sepsis
129 Why a moist wound environment? Proven reduction in infection rate Allows natural enzymes to dissolve debris Promotes wound healing (growth factors) Helps mould wound Prevents re-injury of a dry dressing
130 Osteomyelitis in the diabetic foot Initially plain X Ray may be normal Technetium bone scans 70% reliable with lower specificity Addition of Gallium improves the sensitivity and specificity Indium WBC scanning is best scanning method but more expensive and less readily available. MRI probably best test of bone infection.

131 Osteomyelitis in diabetic foot
132 The role of foot soaks in diabetic foot care Should NOT be done a definite NO... NO Macerates tissues Increases infection Tendency to thermal injury/damage normal healthy tissue

133 A foot soak gone bad maceration
134 Diabetic foot ulcers: newer therapies Recombinant human growth factor therapy (Regranex*) Bio-engineered human skin replacements (Dermagraft*) VAC therapy (KCI) These do not replace nor are they first line strategies
135 Diabetic wound dressings Promote debridement,repair and growth Reduce the pain Absorb any exudate Maintain humidity but not mascerate Keep out the bacteria


136 HOW MUCH DOES IT COST? WHO IS GOING TO PAY?
137 Wound care management Restoration OR maintenance? Etiology, wound management, local skin care, nutrition Damage control internal factors, environmental factors behavioral factors
138 The importance of Prevention Identify the patient at risk Use of established assessment tools(braden and Norton scales) Astute skin care Minimize the aggravating factors

139

140
141

142

143

144
145
146 Wound care protocols all the standard issue discussed plus. Bioengineered tissue Growth factors

147 DERMAGRAFT* APPLICATION
148 Diabetic foot ulcers and hyperbaric oxygen therapy (HBOT): Several studies have shown increased limb salvage withthe use of hyperbaric oxygen in selected patients withinfected diabetic foot ulcers. In general, patients in these studies had deep infection with good arterial supply in whom HBOT was used as an adjunctive treatment with standard wound care therapy.
149 Assessment of the diabetic foot General / specific assessment of the patient Documentation & exploration of wound Assess the circulation Debride as necessary Xray as necessary C& S of wound Formulate treatment plan/wound care protocol Follow-up/referral as necessary
150 Initial Assessment Total Care Considerations Wound Evaluation General Health Assessment Pressure Relief Assessment Psychosocial/Environment Expectations/Goals Defined Comfort/Pain Knowledge/Education Prevention
151 Diabetic foot assessment The importance of structural deformity (Charcot, hammer or claw toe),limited joint mobility, neuropathy and impaired circulation The physical examination must include a thorough inspection, vascular assessment neuro assessment and check out the footwear
152 Management of the ulcer Debride..gets rid of the necrotic tissue/callus.allows proper assessment.increases cytokines in the wound(platelets) Off-Load the pressure.reduce friction and shear forces prescription footwear, orthotics,ortho wedge boots,silicone socks Total contact casts and removable casts
153 Ulcer management Use of antimicrobials..the importance of recognizing and treating the infected ulcer.in pt vs out patient therapy oral vs IV therapy Wound care Avoid abuse of antibiotic topical Tx Extremely important education and followup
154 Wound care protocols standard wound care management protocols Bioengineered tissue Growth factors

155 Early treatment of the diabetic foot improves function and quality of life infection control maintain health status reduce costs

156 Steps in Saving the Diabetic Foot Patient Education Identification of Risk Factors Recognition and Treatment of etiology Wound Management Augmentative Interventions
157 Patient Education Goal Oriented Problem Centred Offers Feedback Group Discussion Varied Presentation
158 Diabetic ulcer risk Peripheral neuropathy Foot deformity Limited joint movement Elevated plantar pressure Prior ulcer/amputation Peripheral vascular disease Susceptibility to infection
159 Identification of Risk Factors prior diabetic ulcer advancing age peripheral vascular disease diabetic neuropathy
160 Identification of Risk Factors Peripheral Vascular Disease Structural Deformity
161 Identification of Risk Factors Peripheral Neuropathy - motor - autonomic - sensory


162 Identification of Risk Factors Peripheral Sensory Neuropathy Autonomic Peripheral Neuropathy
163 Underlying Etiology Extrinsic Trauma Foreign Body Improper Footwear Poor Pressure Relief Surfaces Intrinsic Limited Joint Mobility Foot Deformity Foot Mechanics Neoplasm Infection Ischemia

164 Recognition and Treatment of Underlying Etiology Intrinsic Cause Foot Mechanics Limited joint mobility Foot deformity
165 Principles of Wound Management Debridement Pressure Reduction Removal of Bacterial Burden Promote Healing


166 Wound Management Pressure Reduction Remove Bacterial Burden


167 Augmentative Interventions Therapeutic Off-Loading Devices Crest Pad


168 Insoles and Orthotics Custom Footwear Off-the-Shelf Footwear

169 Diabetic Foot Ulcers are Predictable and Preventable
170 General management approach Effective care involves a partnership between patients and professionals, and all decision making should be shared Arrange recall and annual review as part of ongoing care As part of annual review, trained personnel should examine patients feet to detect risk factors for ulceration and document findings.
171 Examination of patients feet should include: testing of foot sensation using a 10 g monofilament or vibration palpation of foot pulses inspection of any foot deformity and footwear
172 Peters and Lavery (2001) provide an excellent review on the topic and conclude based on evidence that a foot risk classification will predict ulceration and amputation in diabetic feet and may function as a tool to lower extremity amputations. an increase in morbid events throughout progression through the classification system.
173 In Canada, the gold standard of diabetes care is the maintenance of proper glycosated hemoglobin levels and glucose control. The major complications of diabetes including renal failure, heart disease and ophthalmic complications receive increased attention. However, oral care and foot care have not.
174 At each review: determine risk inspect patient s feet consider need for vascular assessment evaluate and ensure the appropriate provision of intensified foot care education specialist footwear and insoles skin and nail care Ensure special arrangements for those people with disabilities or immobility
175 The high-risk group is 34 times more likely to ulcerate and 17 times more likely to have an amputation compared to the low-risk group. The high-risk group is also more likely to have a longer history of diabetes, worse glycemic control, more neuropathy, and increased plantar pressure.
176 The high risk ulcer group is also more likely to be male, alcohol users, and have other end organ diabetic complications including renal failure, retinopathy or cardiac disease. Neuropathy is the pivotal risk factor (Crawford 2007).
177 The FOOTPAD template for diabetes management was changed. All diabetes patients will be assigned a risk classification for foot disease and be reviewed by automatic recall as per the electronic medical record based on the revised template
178 Classify foot risk as: at low current risk at medium risk at high risk ulcerated foot
179 Care of people at low current risk of foot ulcers (normal sensation, palpable pulses) Annual assessment including foot care education with each person
180 Care of people at medium risk of foot ulcers (neuropathy or absent pulses or other risk factor) Arrange regular review, 3 6 monthly, by foot protection team At each review: inspect patient s feet consider need for vascular assessment evaluate footwear enhance foot care education previous foot ulcer or deformity or skin changes manage as high risk
181 Care of people at high risk of foot ulcers (neuropathy or absent pulses plus deformity or skin changes or previous ulcer) Arrange frequent review (1 3 monthly) by foot protection team
182 How can we improve????? 1)Better off loading contact casting 2)Better funding shoes/orthotics/walking boots 3)Increased community service personnel and funding 4)More aggressive vascular intervention 5)More aggressive /earlier bone intervention
183 Exciting new horizon Dr T Best surgical intervention in the the treatment of diabetic neuropathy..supported by a PSI grant..peripheral nerve decompression for the treatment of painful peripheral sensorimotor polyneuropathy in type 1 and type 2 diabetes
184 Inclusion Criteria c >18 years of age c Type 1 or 2 diabetes mellitus c Symptoms of paresthesia (including burning pain) or numbness present symmetrically in both feet, determined to be on a peripheral nerve basis c HbA1c < 7 x 2 in the past 12 months Exclusion Criteria c Other types of diabetes mellitus (gestational, drug-induced) c Causes of neuropathy than diabetes (vasculitis, HIV, renal failure, alcohol abuse) c Symptomatic lumbosacral spine disease c Symptomatic lower extremity vascular disease c Previous foot ulceration or amputation; other contradictions to surgery c History of Peripheral Arterial Disease c HbA1c >7.1 c Inability to give consent, pregnant women, prisoners, nonenglish speakers who require an interpreter

185 Smoking + diabetes = amputation
Front line management of the Diabetic Foot
 Front line management of the Diabetic Foot n o ti e b a i D + s te k o Sm = g in p Am a t u Sam Fratesi MD Smoking + diabetes = amputation Almost 2 million Canadians have diabetes In amputated diabetics
Front line management of the Diabetic Foot n o ti e b a i D + s te k o Sm = g in p Am a t u Sam Fratesi MD Smoking + diabetes = amputation Almost 2 million Canadians have diabetes In amputated diabetics
Introduction. Epidemiology Pathophysiology Classification Treatment
 Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
Diabetic Foot Introduction Epidemiology Pathophysiology Classification Treatment Epidemiology DM largest cause of neuropathy in N.A. 1 million DM patients in Canada Half don t know Foot ulcerations is
The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care
 The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care Anita Murray - Senior Podiatrist Diabetes, SCH Learning Outcomes Knowledge of the Model of Care For The Diabetic Foot
The Diabetic Foot Screen and Management Foundation Series of Modules for Primary Care Anita Murray - Senior Podiatrist Diabetes, SCH Learning Outcomes Knowledge of the Model of Care For The Diabetic Foot
Aetiology Macroangiopathy occurs mainly distally ie Popliteal artery There is arterial wall calcification Microangiopathy is less common
 DIABETIC FOOT Facts 5% of the population is diabetic 12% of diabetic admissions are with foot problems 1/3rd of diabetic foot ulcerations are neuropathic, 1/3rd are ischaemic and 1/3 are of a mixed in
DIABETIC FOOT Facts 5% of the population is diabetic 12% of diabetic admissions are with foot problems 1/3rd of diabetic foot ulcerations are neuropathic, 1/3rd are ischaemic and 1/3 are of a mixed in
Diabetic Foot Ulcers. Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C. Advanced Practice Nurse / Adult Clinical Nurse Specialist
 Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
AWMA MODULE ACCREDITATION. Module Five: The High Risk Foot (Including the Diabetic Foot)
") AWMA MODULE ACCREDITATION Module Five: The High Risk Foot (Including the Diabetic Foot) Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
AWMA MODULE ACCREDITATION Module Five: The High Risk Foot (Including the Diabetic Foot) Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
Diabetic Foot Pathophysiology. Professor Donald G. MacLellan Executive Director Health Education & Management Innovations
 Diabetic Foot Pathophysiology Professor Donald G. MacLellan Executive Director Health Education & Management Innovations AGEs & RAGEs in Diabetes AGE levels increased & RAGEs highly expressed in diabetic
Diabetic Foot Pathophysiology Professor Donald G. MacLellan Executive Director Health Education & Management Innovations AGEs & RAGEs in Diabetes AGE levels increased & RAGEs highly expressed in diabetic
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC
 High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
High Risk Podiatry in a Vascular Setting; A new paradigm in Diabetic Foot Disease? Ereena Torpey Senior Podiatrist - FMC A new paradigm? Foot ulceration 101 Assessing Perfusion a new challenge Pressure
Diabetes Foot and Skin Care. Diabetes and the feet. Foot problems: Major cause of morbidity and mortality
 Session # 11 Diabetes Foot and Skin Care Betty Harvey, RNEC BScN MScN Amanda Mikalachki, RN BScN CDE Diabetes and the feet Diabetes affects circulation and immunity. Over time, the sensory nerves in the
Session # 11 Diabetes Foot and Skin Care Betty Harvey, RNEC BScN MScN Amanda Mikalachki, RN BScN CDE Diabetes and the feet Diabetes affects circulation and immunity. Over time, the sensory nerves in the
Definitions and criteria
 Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Preventing Foot Ulcers in the Neuropathic Diabetic Foot. Glossary of Terms
 Preventing Foot Ulcers in the Neuropathic Diabetic Foot Warren Woods, Certified Orthotist, Health Sciences Centre, Rehabilitation Engineering Department What you need to know Glossary of Terms Neuropathic
Preventing Foot Ulcers in the Neuropathic Diabetic Foot Warren Woods, Certified Orthotist, Health Sciences Centre, Rehabilitation Engineering Department What you need to know Glossary of Terms Neuropathic
Helen Gelly, MD, FUHM, FCCWS
 Helen Gelly, MD, FUHM, FCCWS Diabetes mellitus is a major risk factor that impairs wound healing, making foot wounds one of the major problems of diabetes. Over 60% of lower limb amputations in the US
Helen Gelly, MD, FUHM, FCCWS Diabetes mellitus is a major risk factor that impairs wound healing, making foot wounds one of the major problems of diabetes. Over 60% of lower limb amputations in the US
Peripheral Neuropathy
 Peripheral Neuropathy Neuropathy affects 30-50% of patient population with diabetes and this prevalence tends to increase proportionally with duration of diabetes and dependant on control. Often presents
Peripheral Neuropathy Neuropathy affects 30-50% of patient population with diabetes and this prevalence tends to increase proportionally with duration of diabetes and dependant on control. Often presents
Diabetes follow-up: What are the PHO Performance Programme goals and how are they best achieved? Supporting the PHO Performance Programme
 Diabetes follow-up: What are the PHO Performance Programme goals and how are they best achieved? Supporting the PHO Performance Programme 48 BPJ Issue 39 What are the goals? The PHO Performance Programme
Diabetes follow-up: What are the PHO Performance Programme goals and how are they best achieved? Supporting the PHO Performance Programme 48 BPJ Issue 39 What are the goals? The PHO Performance Programme
Diabetic Foot Ulcers. Care for Patients in All Settings
 Diabetic Foot Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a diabetic foot ulcer. The scope of the standard
Diabetic Foot Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a diabetic foot ulcer. The scope of the standard
AGONY FEET. The. of the. Prevention and management of diabetic foot ulcers
 The AGONY of the FEET Prevention and management of diabetic foot ulcers By Margaret Falconio-West, BSN, rn, APN/CNS, CWOCN, DAPWCA Nearly 25 percent of people with diabetes will develop a diabetic foot
The AGONY of the FEET Prevention and management of diabetic foot ulcers By Margaret Falconio-West, BSN, rn, APN/CNS, CWOCN, DAPWCA Nearly 25 percent of people with diabetes will develop a diabetic foot
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists
 EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
Rapid Recovery Hyperbarics 9439 Archibald Ave. Suite 104 Rancho Cucamonga CA,
 Foot at risk Age Well By Dr LIEW NGOH CHIN Are limb amputations due to diabetes preventable? DIABETES mellitus is a major global health problem and has reached epidemic proportions in many developed and
Foot at risk Age Well By Dr LIEW NGOH CHIN Are limb amputations due to diabetes preventable? DIABETES mellitus is a major global health problem and has reached epidemic proportions in many developed and
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
Diabetic/Neuropathic Foot Ulcer Assessment Guide South West Regional Wound Care Program Last Updated June 10,
 Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline
 Certified Foot Care Nurse (CFCN) Detailed Content Outline") Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline Description Domain I: Assessment and Care Planning 010000 40 Task 1: Obtain focused
Wound, Ostomy and Continence Nursing Certification Board (WOCNCB) Certified Foot Care Nurse (CFCN) Detailed Content Outline Description Domain I: Assessment and Care Planning 010000 40 Task 1: Obtain focused
Diabetic/Neuropathic Foot Ulcer Assessment Guide South West Regional Wound Care Program Last Updated April 7,
 Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
Developed in collaboration with the Wound Care Champions, Wound Care Specialists, Enterostomal Nurses, and South West Regional Wound Care Program (SWRWCP) members from Long Term Care Homes, Hospitals,
Foot Ulcer Workshop: Prevention and Management of Diabetic Foot Ulcers. Aparna Pal, Consultant Endocrinologist, RBH Keith Hilston, Podiatrist, BHFT
 Foot Ulcer Workshop: Prevention and Management of Diabetic Foot Ulcers Aparna Pal, Consultant Endocrinologist, RBH Keith Hilston, Podiatrist, BHFT High mortality and morbidity Complex condition, longterm
Foot Ulcer Workshop: Prevention and Management of Diabetic Foot Ulcers Aparna Pal, Consultant Endocrinologist, RBH Keith Hilston, Podiatrist, BHFT High mortality and morbidity Complex condition, longterm
Diabetic Foot Services. Ketan Dhatariya Elsie Bertram Diabetes Centre Norfolk & Norwich University Hospital
 Diabetic Foot Services Ketan Dhatariya Elsie Bertram Diabetes Centre Norfolk & Norwich University Hospital Objectives 1. Background 2. Foot Screening 3. First line management ulceration 4. Management
Diabetic Foot Services Ketan Dhatariya Elsie Bertram Diabetes Centre Norfolk & Norwich University Hospital Objectives 1. Background 2. Foot Screening 3. First line management ulceration 4. Management
Service Development Tool for the Assessment of Provision of Services for Patients with Diabetes Related Foot Problems
 Division of Medicine & Community Services Service Development Tool for the Assessment of Provision of Services for Patients with Diabetes Related Foot Problems Graham Holt Advanced Practitioner / Podiatrist
Division of Medicine & Community Services Service Development Tool for the Assessment of Provision of Services for Patients with Diabetes Related Foot Problems Graham Holt Advanced Practitioner / Podiatrist
DIABETIC FOOT SCOPE OF THE PROBLEM. Hanan Gawish, Mansoura University Egypt Representative of the IWGDF
 DIABETIC FOOT SCOPE OF THE PROBLEM Hanan Gawish, Mansoura University Egypt Representative of the IWGDF Agenda Definition of DF Diabetic Foot among Diabetes complication Risk factors for amputation Risk
DIABETIC FOOT SCOPE OF THE PROBLEM Hanan Gawish, Mansoura University Egypt Representative of the IWGDF Agenda Definition of DF Diabetic Foot among Diabetes complication Risk factors for amputation Risk
Practical guidelines on the management and prevention of the diabetic foot 2011
 DIABETES/METABOLISM RESEARCH AND REVIEWS Diabetes Metab Res Rev 2012; 28(Suppl 1): 225 231. Published online in Wiley Online Library (wileyonlinelibrary.com).2253 IWGDF GUIDELINES Practical guidelines
DIABETES/METABOLISM RESEARCH AND REVIEWS Diabetes Metab Res Rev 2012; 28(Suppl 1): 225 231. Published online in Wiley Online Library (wileyonlinelibrary.com).2253 IWGDF GUIDELINES Practical guidelines
Diabetic Foot Complications
 Diabetic Foot Complications Podiatry Specialty Clinic YKHC Bethel, Alaska August 1-3, 2017 Charles C. Edwards, DPM Alaska Native Tribal Health Consortium Peripheral Neuropathy Diabetic Peripheral Neuropathy
Diabetic Foot Complications Podiatry Specialty Clinic YKHC Bethel, Alaska August 1-3, 2017 Charles C. Edwards, DPM Alaska Native Tribal Health Consortium Peripheral Neuropathy Diabetic Peripheral Neuropathy
Model of Care for the Diabetic Foot
 Model of Care for the Diabetic Foot National Clinical Programme for Diabetes Clinical Strategy and Programme Division 2018 Revision number Document drafted by National Clinical Programme for Diabetes Working
Model of Care for the Diabetic Foot National Clinical Programme for Diabetes Clinical Strategy and Programme Division 2018 Revision number Document drafted by National Clinical Programme for Diabetes Working
My Diabetic Patient Has No Pulses; What Should I Do?
 Emily Malgor, MD Assistant Professor of Surgery University of Oklahoma, Oklahoma City My Diabetic Patient Has No Pulses; What Should I Do? There are no disclosures. Background Diabetes affects 387 million
Emily Malgor, MD Assistant Professor of Surgery University of Oklahoma, Oklahoma City My Diabetic Patient Has No Pulses; What Should I Do? There are no disclosures. Background Diabetes affects 387 million
Type 2 diabetes: prevention and management of foot problems
 Type 2 diabetes: prevention and management of foot problems NICE guideline Revised version Second draft for consultation, August 2003 If you wish to comment on the recommendations, please make your comments
Type 2 diabetes: prevention and management of foot problems NICE guideline Revised version Second draft for consultation, August 2003 If you wish to comment on the recommendations, please make your comments
DIABETIC FOOT RISK CLASSIFICATION IN A TERTIARY CARE TEACHING HOSPITAL OF PESHAWAR
 ORIGINAL ARTICLE DIABETIC FOOT RISK CLASSIFICATION IN A TERTIARY CARE TEACHING HOSPITAL OF PESHAWAR Ghulam Shabbier, Said Amin, Ishaq Khattak, Sadeeq-ur-Rehman Department of Medicine Khyber Teaching Hospital
ORIGINAL ARTICLE DIABETIC FOOT RISK CLASSIFICATION IN A TERTIARY CARE TEACHING HOSPITAL OF PESHAWAR Ghulam Shabbier, Said Amin, Ishaq Khattak, Sadeeq-ur-Rehman Department of Medicine Khyber Teaching Hospital
Integumentary Physical Therapy 피부계물리치료학
 Integumentary Physical Therapy 피부계물리치료학 Dong-Ryul Lee, PT, Ph.D. Movement Impairment Specialist & Performance Enhancement Specialist Neurofeedback, Robotics & Virtual Reality Research Specialites: NeuroRehabilitation
Integumentary Physical Therapy 피부계물리치료학 Dong-Ryul Lee, PT, Ph.D. Movement Impairment Specialist & Performance Enhancement Specialist Neurofeedback, Robotics & Virtual Reality Research Specialites: NeuroRehabilitation
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Diabetes Mellitus and the Associated Complications
 Understanding and the complications relating to the disease can assist the fitter to better serve patients. and the Associated Complications Released January, 2011 Total: 25.8 million people, or 8.3% of
Understanding and the complications relating to the disease can assist the fitter to better serve patients. and the Associated Complications Released January, 2011 Total: 25.8 million people, or 8.3% of
Diabetes is a serious disease that can develop from lack of insulin production in the body or due to
 Page 1 The Diabetic Foot Definition Diabetes is a serious disease that can develop from lack of insulin production in the body or due to the inability of the body's insulin to perform its normal everyday
Page 1 The Diabetic Foot Definition Diabetes is a serious disease that can develop from lack of insulin production in the body or due to the inability of the body's insulin to perform its normal everyday
MANAGEMENT OF DIABETIC WOUNDS : HEALTH CLINIC SETTING DR NORLIZAH PAIDI FAMILY MEDICINE SPECIALIST KLINIK KESIHATAN BANDAR MAS KOTA TINGGI JOHOR
 MANAGEMENT OF DIABETIC WOUNDS : HEALTH CLINIC SETTING DR NORLIZAH PAIDI FAMILY MEDICINE SPECIALIST KLINIK KESIHATAN BANDAR MAS KOTA TINGGI JOHOR OUTLINE DEFINITION FACTORS CONTRIBUTING TO WOUND DEVELOPMENT
MANAGEMENT OF DIABETIC WOUNDS : HEALTH CLINIC SETTING DR NORLIZAH PAIDI FAMILY MEDICINE SPECIALIST KLINIK KESIHATAN BANDAR MAS KOTA TINGGI JOHOR OUTLINE DEFINITION FACTORS CONTRIBUTING TO WOUND DEVELOPMENT
10/19/2017. Shawn M Sanicola DPM, FACFAS Foot And Ankle Associates of WI. Consultant with J&J-Depuy-Synthesis
 Shawn M Sanicola DPM, FACFAS Foot And Ankle Associates of WI Consultant with J&J-Depuy-Synthesis Understand the systemic effects of diabetes on the lower extremity The significance of structural and biomechanical
Shawn M Sanicola DPM, FACFAS Foot And Ankle Associates of WI Consultant with J&J-Depuy-Synthesis Understand the systemic effects of diabetes on the lower extremity The significance of structural and biomechanical
CHAPTER.7 CARING THE DIABETIC FOOT
 CHAPTER.7 CARING THE DIABETIC FOOT Introduction Diabetes has become a global epidemic(144). The long term complications due to diabetes impose huge social and economic burden, mental and physical misery
CHAPTER.7 CARING THE DIABETIC FOOT Introduction Diabetes has become a global epidemic(144). The long term complications due to diabetes impose huge social and economic burden, mental and physical misery
Root Cause Analysis The Tools. Angie Abbott Head of Podiatry and Orthotics Torbay and Southern Devon
 Root Cause Analysis The Tools Angie Abbott Head of Podiatry and Orthotics Torbay and Southern Devon Why do RCA s? To understand if the amputation was avoidable or unavoidable Learn and improve Identify
Root Cause Analysis The Tools Angie Abbott Head of Podiatry and Orthotics Torbay and Southern Devon Why do RCA s? To understand if the amputation was avoidable or unavoidable Learn and improve Identify
Clinical assessment of diabetic foot in 5 minutes
 Clinical assessment of diabetic foot in 5 minutes Assoc. Prof. N. Tentolouris, MD 1 st Department of Propaedeutic Internal Medicine Medical School Laiko General Hospital Leading Innovative Vascular Education
Clinical assessment of diabetic foot in 5 minutes Assoc. Prof. N. Tentolouris, MD 1 st Department of Propaedeutic Internal Medicine Medical School Laiko General Hospital Leading Innovative Vascular Education
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
The Diabetic foot. diabetic. foot. the
 The Diabetic Some basic facts. Diabetes is on increase. Foot ulcers occur in 12% to 25% of people with diabetes. Diabetics who have had a ulcer are more likely to have a re occurrence. Diabetes is biggest
The Diabetic Some basic facts. Diabetes is on increase. Foot ulcers occur in 12% to 25% of people with diabetes. Diabetics who have had a ulcer are more likely to have a re occurrence. Diabetes is biggest
Management Of The Diabetic foot
 Management Of The Diabetic foot Aims, Pathways, Treatments Nikki Coates 12/1/18 Diabetic foot pathology Neuropathy Foot deformity Vascular disease Sensory neuropathy Limited Joint Mobility Smoking Autonomic
Management Of The Diabetic foot Aims, Pathways, Treatments Nikki Coates 12/1/18 Diabetic foot pathology Neuropathy Foot deformity Vascular disease Sensory neuropathy Limited Joint Mobility Smoking Autonomic
Dr. Sibbald is: Company/ Agency Lecturers. Objectives Participants will:
 Dr. R. Gary Sibbald MD, FRCPC (Med, Derm), MACP, FAAD, M.Ed. Professor Of Medicine / Public Health U. Of Toronto Director Of The International Interprofessional Wound Care Course President Of The World
Dr. R. Gary Sibbald MD, FRCPC (Med, Derm), MACP, FAAD, M.Ed. Professor Of Medicine / Public Health U. Of Toronto Director Of The International Interprofessional Wound Care Course President Of The World
Happy Feet: Feeling good about diabe.c foot screening! Family Medicine Forum 2014, Quebec City November 14, 2014
 Happy Feet: Feeling good about diabe.c foot screening! Family Medicine Forum 2014, Quebec City November 14, 2014 Dr. Michael Yan, MD, CCFP Clinical Lecturer, Department of Family Medicine, University of
Happy Feet: Feeling good about diabe.c foot screening! Family Medicine Forum 2014, Quebec City November 14, 2014 Dr. Michael Yan, MD, CCFP Clinical Lecturer, Department of Family Medicine, University of
Diabetic Foot Ulcer Treatment and Prevention
 Diabetic Foot Ulcer Treatment and Prevention Alexander Reyzelman DPM, FACFAS Associate Professor California School of Podiatric Medicine at Samuel Merritt University Diabetic Foot Ulcers One of the most
Diabetic Foot Ulcer Treatment and Prevention Alexander Reyzelman DPM, FACFAS Associate Professor California School of Podiatric Medicine at Samuel Merritt University Diabetic Foot Ulcers One of the most
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Our Vision NADA BoD Strategic Planning Session -
 Who we are NADA is a not-for-profit members-led organization established in 1995 as a result of the rising rates of diabetes among First Nations, Inuit and Métis Peoples in Canada Our Vision - 2016 NADA
Who we are NADA is a not-for-profit members-led organization established in 1995 as a result of the rising rates of diabetes among First Nations, Inuit and Métis Peoples in Canada Our Vision - 2016 NADA
Case Study 2 - Mr J. Medical history
 Case Study 2 - Mr J A 54 year-old male was referred to the podiatrist at Coast Provincial General Hospital Diabetic Clinic, for management of active foot disease. The patient s presenting complaint was
Case Study 2 - Mr J A 54 year-old male was referred to the podiatrist at Coast Provincial General Hospital Diabetic Clinic, for management of active foot disease. The patient s presenting complaint was
How can DIABETES affect my FEET? Emma Howard Specialist Podiatrist and Team Leader, Oxford Health NHS Foundation Trust
 How can DIABETES affect my FEET? By: Emma Howard Specialist Podiatrist and Team Leader, Oxford Health NHS Foundation Trust HOW CAN DIABETES AFFECT MY FEET? What is neuropathy? This leaflet explains how
How can DIABETES affect my FEET? By: Emma Howard Specialist Podiatrist and Team Leader, Oxford Health NHS Foundation Trust HOW CAN DIABETES AFFECT MY FEET? What is neuropathy? This leaflet explains how
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
The Diabetic Foot Latest Statistics
 The Diabetic Foot Latest Statistics There are 2.6 million people with diagnosed diabetes in the UK. There are predicted to be 500,000 who have the condition but are unaware of it. There are 11,859 in TH
The Diabetic Foot Latest Statistics There are 2.6 million people with diagnosed diabetes in the UK. There are predicted to be 500,000 who have the condition but are unaware of it. There are 11,859 in TH
Charcot Arthropathy of the Foot & Ankle. MTAPA Annual Meeting June 2018 Emily Harnden, MD
 Charcot Arthropathy of the Foot & Ankle MTAPA Annual Meeting June 2018 Emily Harnden, MD Background Disclosures None Learning Objectives Define the disease Recognize presenting signs/symptoms for proper
Charcot Arthropathy of the Foot & Ankle MTAPA Annual Meeting June 2018 Emily Harnden, MD Background Disclosures None Learning Objectives Define the disease Recognize presenting signs/symptoms for proper
Diabetic Feet. Juanita Muller
 Diabetic Feet Juanita Muller Mr RR 69 year old male CHARCOT ARTHROPATHY Diabetic Feet Callus Acute injury and ulceration Infection Osteomylitis Chronic ulceration Ischaemic necrosis Charcot s arthropathy
Diabetic Feet Juanita Muller Mr RR 69 year old male CHARCOT ARTHROPATHY Diabetic Feet Callus Acute injury and ulceration Infection Osteomylitis Chronic ulceration Ischaemic necrosis Charcot s arthropathy
Care of the Diabetic Patient
 Care of the Diabetic Patient Aarti Deshpande, CPO Clinic Manager Zuckerberg San Francisco General Department of Orthopaedic Surgery University of California, San Francisco March 16, 2017 Diabetes Diabetes
Care of the Diabetic Patient Aarti Deshpande, CPO Clinic Manager Zuckerberg San Francisco General Department of Orthopaedic Surgery University of California, San Francisco March 16, 2017 Diabetes Diabetes
Diabetes Foot Screening and Risk Stratification Tool
 Diabetes Foot Screening and Risk Stratification Tool Welcome to the Diabetes Foot Screening and Risk Stratification Tool This tool is based on the work of the Scottish Foot Action Group (SFAG). It has
Diabetes Foot Screening and Risk Stratification Tool Welcome to the Diabetes Foot Screening and Risk Stratification Tool This tool is based on the work of the Scottish Foot Action Group (SFAG). It has
Diabetic Foot Problems
 http://www.medicine-on-line.com Diabetic foot disease: 1/12 Diabetic Foot Problems Author: Affiliation: Rebecca Wong BN, MSc(Health Care) Prince of Wales Hospital, Hong Kong SAR Introduction Diabetes Mellitus
http://www.medicine-on-line.com Diabetic foot disease: 1/12 Diabetic Foot Problems Author: Affiliation: Rebecca Wong BN, MSc(Health Care) Prince of Wales Hospital, Hong Kong SAR Introduction Diabetes Mellitus
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
Rapid Foot Screening
 GP Symposium 2015 Workshop Rapid Foot Screening Ms Chelsea Law, Principal Podiatrist Mr Henry Lee, Podiatrist Ms Ng Jia Lin, Podiatrist Ms Polly Lim, Podiatrist Ms Wong Wan Mun, Podiatrist Mr Yeo Boon
GP Symposium 2015 Workshop Rapid Foot Screening Ms Chelsea Law, Principal Podiatrist Mr Henry Lee, Podiatrist Ms Ng Jia Lin, Podiatrist Ms Polly Lim, Podiatrist Ms Wong Wan Mun, Podiatrist Mr Yeo Boon
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME QOF indicator area: Diabetes Briefing paper Potential output: Recommendations
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE QUALITY AND OUTCOMES FRAMEWORK (QOF) INDICATOR DEVELOPMENT PROGRAMME QOF indicator area: Diabetes Briefing paper Potential output: Recommendations
NORTHEAST OHIO NEIGHBORHOOD HEALTH SERVICES, INC. PODIATRY CLINICAL GUIDELINES TABLE OF CONTENTS. Diabetes Mellitus and Podiatric Care 2
 NORTHEAST OHIO NEIGHBORHOOD HEALTH SERVICES, INC. PODIATRY 2012-2013 CLINICAL GUIDELINES TABLE OF CONTENTS CONDITION PAGE(S) Diabetes Mellitus and Podiatric Care 2 Fractures 3-4 Heel Pain (Posterior) Retrocalcaneal
NORTHEAST OHIO NEIGHBORHOOD HEALTH SERVICES, INC. PODIATRY 2012-2013 CLINICAL GUIDELINES TABLE OF CONTENTS CONDITION PAGE(S) Diabetes Mellitus and Podiatric Care 2 Fractures 3-4 Heel Pain (Posterior) Retrocalcaneal
Training Your Caregiver: Diabetes
 Diabetes, often referred to by doctors as diabetes mellitus, describes a group of metabolic diseases in which the person has high blood glucose (blood sugar), either because insulin production is inadequate,
Diabetes, often referred to by doctors as diabetes mellitus, describes a group of metabolic diseases in which the person has high blood glucose (blood sugar), either because insulin production is inadequate,
THE DIABETIC FOOT. Nicola Kilburn Diabetes Specialist Podiatrist
 THE DIABETIC FOOT Nicola Kilburn Diabetes Specialist Podiatrist Diabetic foot disease is associated with significant morbidity and mortality. Foot screening is effective in identifying an individuals risk
THE DIABETIC FOOT Nicola Kilburn Diabetes Specialist Podiatrist Diabetic foot disease is associated with significant morbidity and mortality. Foot screening is effective in identifying an individuals risk
Address: Left Leg. other: Nails: thick yellow brittle fungus abnormal thick yellow brittle fungus abnormal
 South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
Consider the possibility of pressure ulcer development
 Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Is Neuropathy the root of all evil in the diabetic foot?
 Is Neuropathy the root of all evil in the diabetic foot? Andrew J M Boulton, Manchester UK and Miami, FL Vice-President and Director of International Postgraduate Education, EASD The Global Burden of Diabetes
Is Neuropathy the root of all evil in the diabetic foot? Andrew J M Boulton, Manchester UK and Miami, FL Vice-President and Director of International Postgraduate Education, EASD The Global Burden of Diabetes
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
EDUCATION. Peripheral Artery Disease
 EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
EDUCATION Peripheral Artery Disease Peripheral Artery Disease You may have circulation problems that have to do with your blood vessels. You may feel aches, pains, cramps, numbness or muscle fatigue when
Frank K. Galbraith D.P.M. Dr. Frank Galbraith
 Frank K. Galbraith D.P.M. Dr. Frank Galbraith Ingrown Toenails Paronychia (infected toenail) Onychomycosis (fungal nails) From improper trimming, leaving nail sharp corners Curved nails Thick (Hypertrophic)
Frank K. Galbraith D.P.M. Dr. Frank Galbraith Ingrown Toenails Paronychia (infected toenail) Onychomycosis (fungal nails) From improper trimming, leaving nail sharp corners Curved nails Thick (Hypertrophic)
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Statistics on DM and DFU risk
 Disclosure NOTHING Statistics on DM and DFU risk National Institute of Diabetes Digestive & Kidney Diseases: As of September 2011 an estimated 16 million Americans are known to have diabetes, with many
Disclosure NOTHING Statistics on DM and DFU risk National Institute of Diabetes Digestive & Kidney Diseases: As of September 2011 an estimated 16 million Americans are known to have diabetes, with many
University of Huddersfield Repository
 University of Huddersfield Repository Newton, Veronica and Roberts, Peter Foot Inspection or Foot Assessment? Original Citation Newton, Veronica and Roberts, Peter (2011) Foot Inspection or Foot Assessment?
University of Huddersfield Repository Newton, Veronica and Roberts, Peter Foot Inspection or Foot Assessment? Original Citation Newton, Veronica and Roberts, Peter (2011) Foot Inspection or Foot Assessment?
Project I - Background Worksheet. Team Members: Kira Brown, Paige Fallu. Clinical problem Diabetic Foot Ulcers
 Project I - Background Worksheet Team Members: Kira Brown, Paige Fallu Clinical problem Diabetic Foot Ulcers 1) Strategic Focus based on the Strategic focus powerpoint presentation and readings a. Team
Project I - Background Worksheet Team Members: Kira Brown, Paige Fallu Clinical problem Diabetic Foot Ulcers 1) Strategic Focus based on the Strategic focus powerpoint presentation and readings a. Team
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
Assessment & Management of the Diabetic Foot
 EWMA Educational Development Programme Curriculum Development Project Education Module: Assessment & Management of the Diabetic Foot Latest review: August 2012 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
EWMA Educational Development Programme Curriculum Development Project Education Module: Assessment & Management of the Diabetic Foot Latest review: August 2012 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
Podiatry in Practice. Alan M. Singer, DPM, FACFAS
 Podiatry in Practice Alan M. Singer, DPM, FACFAS Podiatry in Practice Alan Singer, D.P.M. UNIVERSITY PODIATRY GROUP Onychomycosis Anti-fungals Onychocryptosis (Ingrown Nails) Ingrown Nails Partial Nail
Podiatry in Practice Alan M. Singer, DPM, FACFAS Podiatry in Practice Alan Singer, D.P.M. UNIVERSITY PODIATRY GROUP Onychomycosis Anti-fungals Onychocryptosis (Ingrown Nails) Ingrown Nails Partial Nail
Leg ulcer assessment and management
 Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Venous Leg Ulcers. Care for Patients in All Settings
 Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Diabetes - Foot Care
 Diabetes - Foot Care Introduction People with diabetes are more likely than others to have problems with their feet. These problems can lead to dangerous infections of the foot. Recognizing and treating
Diabetes - Foot Care Introduction People with diabetes are more likely than others to have problems with their feet. These problems can lead to dangerous infections of the foot. Recognizing and treating
ORTHOTICS COMPETENCY FRAMEWORK FOR THE PREVENTION, TREATMENT AND MANAGEMENT OF DIABETIC FOOT DISEASE - 1 -
 ORTHOTICS COMPETENCY FRAMEWORK FOR THE PREVENTION, TREATMENT AND MANAGEMENT OF DIABETIC FOOT DISEASE - 1 - THE ORTHOTICS COMPETENCY FRAMEWORK FOR THE PREVENTION, TREATMENT AND MANAGEMENT OF DIABETIC FOOT
ORTHOTICS COMPETENCY FRAMEWORK FOR THE PREVENTION, TREATMENT AND MANAGEMENT OF DIABETIC FOOT DISEASE - 1 - THE ORTHOTICS COMPETENCY FRAMEWORK FOR THE PREVENTION, TREATMENT AND MANAGEMENT OF DIABETIC FOOT
Diabetes Foot Care Clinical Pathway Healthcare Provider s Guide
 Diabetes Foot Care Clinical Pathway Healthcare Provider s Guide Diabetes, Obesity & Nutrition Strategic Clinical Network Version 1.0 Acknowledgement This healthcare provider s guide has been adapted from
Diabetes Foot Care Clinical Pathway Healthcare Provider s Guide Diabetes, Obesity & Nutrition Strategic Clinical Network Version 1.0 Acknowledgement This healthcare provider s guide has been adapted from
Appendix D: Leg Ulcer Assessment Form
 Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
Nursing Best Practice Guideline Appendix D: Ulcer Assessment Form Person Completing Assessment: Date: Client Name: Caf # CM# VON ID #: District CCAC ID # Address Telephone Home: Work: Date of Birth Y/M/D:
2008 American Medical Association and National Committee for Quality Assurance. All Rights Reserved. CPT Copyright 2007 American Medical Association
 Chronic Wound Care ASPS #1: Use of wound surface culture technique in patients with chronic skin ulcers (overuse measure) This measure may be used as an Accountability measure Clinical Performance Measure
Chronic Wound Care ASPS #1: Use of wound surface culture technique in patients with chronic skin ulcers (overuse measure) This measure may be used as an Accountability measure Clinical Performance Measure
Screening for diabetic foot complications
 Screening for diabetic foot complications Classifying risk of ulceration 4 Normal sensation, palpable pulses, no deformity Evidence of neuropathy, absence of pedal pulse(s) Evidence of neuropathy, absence
Screening for diabetic foot complications Classifying risk of ulceration 4 Normal sensation, palpable pulses, no deformity Evidence of neuropathy, absence of pedal pulse(s) Evidence of neuropathy, absence
DIABETES AND FOOTCARE
 DIABETES AND FOOTCARE Self-Care and Treatment for Healthy Feet Don t Take Your Feet for Granted Every day, you depend on your feet to keep you moving. But when you have diabetes, your feet need special
DIABETES AND FOOTCARE Self-Care and Treatment for Healthy Feet Don t Take Your Feet for Granted Every day, you depend on your feet to keep you moving. But when you have diabetes, your feet need special
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Transmetatarsal amputation in an at-risk diabetic population: a retrospective study
 The Journal of Diabetic Foot Complications Transmetatarsal amputation in an at-risk diabetic population: a retrospective study Authors: Merribeth Bruntz, DPM, MS* 1,2, Heather Young, MD 3,4, Robert W.
The Journal of Diabetic Foot Complications Transmetatarsal amputation in an at-risk diabetic population: a retrospective study Authors: Merribeth Bruntz, DPM, MS* 1,2, Heather Young, MD 3,4, Robert W.
The Diabetic Foot. Michael Anthony, DPM. 422 million diabetic million % adult population 90% Type II
 The Diabetic Foot Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center Prevalence of Diabetes 422 million diabetic 2016 382 million
The Diabetic Foot Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center Prevalence of Diabetes 422 million diabetic 2016 382 million
The Diabetic Foot. Prevalence of Diabetes United States. Prevalence of Diabetes
 The Diabetic Foot Prevalence of Diabetes Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center 422 million diabetic 2016 382 million
The Diabetic Foot Prevalence of Diabetes Michael Anthony, DPM Assistant Professor - Clinical Department of Orthopaedics The Ohio State University Wexner Medical Center 422 million diabetic 2016 382 million
AIM OF MASTERCLASS. Overview of the diabetic foot disease. Modern approach to management
 AIM OF MASTERCLASS Overview of the diabetic foot disease Modern approach to management DIABETIC FOOT DISEASE THROUGHOUT THE WORLD, THERE IS AN AMPUTATION EVERY 20 SECONDS MOST OF THESE AMPUTATIONS ARE
AIM OF MASTERCLASS Overview of the diabetic foot disease Modern approach to management DIABETIC FOOT DISEASE THROUGHOUT THE WORLD, THERE IS AN AMPUTATION EVERY 20 SECONDS MOST OF THESE AMPUTATIONS ARE
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
THE FORGOTTEN COMPLICATION M. Pfeifer
 Diabetic Neuropathy THE FORGOTTEN COMPLICATION M. Pfeifer P 1 The Burden of Diabetic Peripheral Neuropathy Most common peripheral neuropathy in the developed nations Major contributor to the hospital rate
Diabetic Neuropathy THE FORGOTTEN COMPLICATION M. Pfeifer P 1 The Burden of Diabetic Peripheral Neuropathy Most common peripheral neuropathy in the developed nations Major contributor to the hospital rate
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes
 Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Sores That Will Not Heal
 Sores That Will Not Heal Introduction Some sores have trouble healing on their own. Sores that will not heal are a common problem. Open sores that will not heal are also known as wounds or skin ulcers.
Sores That Will Not Heal Introduction Some sores have trouble healing on their own. Sores that will not heal are a common problem. Open sores that will not heal are also known as wounds or skin ulcers.