New Strategies for Cardiovascular Risk reduction in Diabetes
|
|
|
- Emory Stevens
- 5 years ago
- Views:
Transcription
, MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC")
1 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology
2 % event as first CV event HF was the one of the first manifestation of T2D-related CV disease Cohort study of patients (n=1.9 million) with T2D and incidence of CV disease 16.2% 14.1% 11.5% 10.3% 4.2% PAD HF* NFMI CVA CV death *Heart failure post MI was not included in this definition of HF In this large cohort, PAD and HF were the two most common first presentations of T2D-related CV disease Yet, myocardial infarction and stroke continue to be chosen as primary outcomes of major type 2 diabetes trials, as part of the MACE endpoint This suggests that future studies should assess CV events that occur earlier in patients with T2D such as HF and PAD CV, cardiovascular; CVA, cerebrovascular accident; HF, heart failure; NFMI, nonfatal myocardial infarction; PAD, peripheral arterial disease; T2D, type 2 diabetes. Shah AD, et al. Lancet Diabetes Endocrinol. 2015;3: , Appendix.

3 Proportion surviving The presence of HF in patients with diabetes is associated with an increased risk of death Diabetes, without heart failure (n=69,083) P < ,803 adults 65 years and older in fee-for-service Medicare without a prior HF claim were followed for 5 years Incident HF was determined using DRG codes 0.25 Diabetes with incident heart failure (n=46,720) Survival was significantly lower in those who developed HF compared with those without HF Years HF, heart failure; DRG, diagnosis related group Bertoni AG, et al. Diabetes Care. 2004;27:
4 Incidence of hhf Type 2 diabetes is a potent, independent risk factor for heart failure Four year follow up of a cohort with and without T2D (n=45,227) and either established CVD or CV risk factors 10% 9.4% 8% 6% 5.9% OR (adjusted*) 1.33 (95% CI, ). 4% 2% T2D No T2D 0% Diabetes mellitus was associated with a 33% greater risk of hospitalization for heart failure hhf, hospitalization for heart failure Cavender Circulation. 2015;132: * sex, age, geographic region, cardiovascular risk factors; ischemic event, renal dysfunction, known vascular disease, congestive heart failure, atrial fibrillation, and medications (statins, aspirin, blood pressure treatment, antihyperglycemic agent).


5 Left ventricular dysfunction is an early complication of T2 diabetes 68% of patients with T2D had evidence of LV dysfunction 5 years after T2D diagnosis Normal LV function N=124 32% 16% 27% Diastolic LVD N=61 Systolic LVD N=106 This suggests the earliest defect in the diabetic heart is diastolic dysfunction Systolic and diastolic LVD N=95 25% Patients had no evidence of inducible ischemia by stress testing at baseline LV, left ventricular; LVD, LV dysfunction Faden Diabetes and Clinical Research 2013; Seferović PM, Paulus WJ. Eur Heart J. 2015;36: , 1727a-1727c
6 Older glucose-lowering agents have not definitively shown positive effects on major CV events Trial ACE (N=6522) 1 Acarbose versus placebo + CV prevention therapy TOSCA.IT (N=3,028) 2 PIO versus SU as add-on to MET ACCORD (N=10,251) 4 HbA 1c <6.0% versus HbA 1c % (MET, SU, TZD, insulin) VADT (N=1791) 5 HbA 1c 1.5% versus the standard group (MET or GLIM, ROSI, insulin) DEVOTE (N=7367) 6 IGlar versus IDeg Outcome 5P-MACE: CV death, NF-MI, NF-stroke, hua, hhf All-cause death, NF-MI, silent MI, NF-stroke, urgent coronary revascularization HR (95% CI) 0.96 (0.74, 1.26) ADVANCE (N=11,140) 3 3P-MACE: CV death, NF-MI, HbA 1c 6.5% versus HbA 1c >6.5% (gliclazide + any other agent) NF-stroke 0.94 (0.84, 1.06) 3P-MACE: CV death, NF-MI, NF-stroke 7P-MACE: CV death, MI, stroke, HF, surgery for vascular disease, inoperable CHD, amputation for ischemic gangrene 3P-MACE: CV death, NF-MI, NF-stroke (0.86, 1.11) 0.90 (0.78, 1.04) 0.88 (0.74, 1.05) 0.91 (0.78, 1.06) CI, confidence interval; CV, cardiovascular; GLIM, glimepiride; HR, hazard ratio; MACE, major adverse cardiovascular event; hhf, hospitalization for heart failure; HF, heart failure; hua, hospitalization for unstable angina; MET, metformin; NF, non-fatal; PIO, pioglitazone; ROSI, rosiglitazone; SU, sulfonylurea; TZD, thiazolidinedione 1. Holman RR, et al. Lancet Diabetes Endocrinol 2017; doi: /S (17) ; 2. Vaccaro O, et al. Lancet Diabetes Endocrinol 2017;5: ; 3. ADVANCE Collaborative Group. N Engl J Med 2008;358: ; 4. The ACCORD Study Group. N Engl J Med 2008;358: ; 5. Duckworth W, et al. N Engl J Med 2009;360: ; 6. Marso SP, et al. N Engl J Med 2017;377:
7 Incidence of primary endpoint events (%) Incidence of primary endpoint events (%) Patients with events (%) while DPP-4 inhibitors were largely CV neutral Saxagliptin (SAVOR trial) 1 Alogliptin (EXAMINE trial) 2 Sitagliptin (TECOS trial) 3 Primary endpoint: Composite of CV death, myocardial infarction, or ischemic stroke Primary endpoint: Composite of CV death, nonfatal myocardial infarction, or nonfatal stroke Primary endpoint: Composite of CV death, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for unstable angina Hazard ratio: 1.0 (95% CI: 0.89, 1.12) P<0.001 for noninferiority P=0.99 for superiority Placebo (n=8212) Saxagliptin (n=8280) Hazard ratio: 0.96 (upper boundary of the one-sided repeated CI: 1.16) P<0.001 for noninferiority P=0.32 for superiority Hazard ratio: 0.98 (95% CI: 0.89, 1.08) P=0.65 Placebo (n=7339) Sitagliptin (n=7332) 5 5 Placebo (n=2679) Alogliptin (n=2701) Months Months Months CI, confidence interval; CV, cardiovascular; CVOT, cardiovascular outcomes trial; DPP-4, dipeptidyl peptidase-4 1. Adapted from Scirica B, et al. N Engl J Med 2013;369: ; 2. Adapted from White W, et al. N Engl J Med 2013;369: ; 3. Adapted from Green JB, et al. N Engl J Med 2015;373:
8 CVOTs with GLP-1 RAs in patients with type 2 diabetes demonstrated heterogeneous results Trial Outcome HR (95% CI) ELIXA (N=6068) 1 Lixisenatide vs placebo Time to first occurrence of CV death, nonfatal MI, nonfatal stroke, or hospitalization for unstable angina 1.02 (0.89, 1.17) EXSCEL (N=14,752) 2 Exenatide vs placebo 3P-MACE: CV death, NF-MI, NF-stroke 0.91 (0.83, 1.00) LEADER (N=9340) 3 Liraglutide vs placebo SUSTAIN-6 (N=3297) 4 Semaglutide vs placebo 3P-MACE: CV death, NF-MI, NF-stroke 3P-MACE: CV death, NF-MI, NF-stroke 0.87 (0.78, 0.97) 0.74 (0.58, 0.95) CI, confidence interval; CV, cardiovascular; CVOT, cardiovascular outcomes trial; GLP-1 RA, glucagon-like peptide-1 receptor agonist; HR, hazard ratio; MI, myocardial infarction; NF, nonfatal; 3P-MACE. 3 point major adverse cardiac event 1. Pfeffer MA, et al. N Engl J Med 2015;373: ; 2. Holman RR, et al. N Engl J Med 2017;377: ; 3. Marso SP, et al. N Engl J Med 2016;375: ; 4. Marso SP, et al. N Engl J Med 2016;375:
9 The impact of GLDs on heart failure has also been heterogeneous and may depend on the class Class Study Impact on HF Insulin SU (2 nd generation) TZD Review of diabetes registry from Kaiser Permanente Northwest Registry (n=8063) 1 Analysis of UK General Practice Research Database (n=91,521) 2 Meta-analysis of patients with prediabetes and diabetes (n=20,191) 3 2 fold increase* HR (p=0.01 and p< 0.001)** RR 1.72 [ ] (p=0.002) DPP4 Meta-analysis of RCT with DPP4s 4 OR 1.19 [ ] (p=0.015) GLP-1 Meta-analysis of four CV outcome studies HR 0.93 [ ] with GLP-1 receptor antagonists 5 (p=0.20) GLD, glucose lowering drugs; HR, hazard ratio; RR relative risk; RCT randomized clinical trials; HF, heart failure; SU, sulfonylurea; TZD, thiazolidinedione *when insulin was added; ** compared to metformin monotherapy 1. Nichols Diabetes Metab Res Rev. 2005;21:51-57; 2.Tzoulaki et al. BMJ2009;339:b4731; 3. Lago et al. Lancet 2007; 370: ; 4. Monami et al. Nutr Meta Cardiovasc Dis 2014;24: ; 5. Bethel et al, Lancet Diabetes Endocrinology 2018;6:105-13
10 CV outcomes data for SGLT2 inhibitors are building Two SGLT2 studies demonstrate a reduction in both MACE and heart failure endpoints EMPA-REG OUTCOME CANVAS Outcome HR (95% CI) Outcome HR (95% CI) MACE (3-point) 0.86 (0.74, 0.99) MACE (3-point) 0.86 (0.75, 0.97) hhf 0.65 (0.50, 0.85) hhf 0.67 (0.52, 0.87) Favors empagliflozin Favors placebo Demonstrated a significant reduction in CV events in patients receiving empagliflozin Established CVD: 99% Favors canagliflozin Favors placebo Demonstrated a significant reduction in CV events in patients receiving canagliflozin Established CVD: 66% MACE, major adverse cardiovascular event (CV death, nonfatal MI and nonfatal stroke); MI, myocardial infarction; hhf hospitalization for heart failure. Zinman B, et al. N Engl J Med 2015;373: ; Neal B, et al. N Engl J Med :644-57
11 Patients with event (%) Patients with event (%) Hypothesis about HF prevention have emerged from SGLT2i trials EMPA-REG OUTCOME 1 hospitalisation for HF* Placebo CANVAS 2 hospitalisation for HF* Placebo 4 HR=0.65 (95% CI: ) P= HR=0.67 (95% CI: ) 3 Empagliflozin 3 Canagliflozin Month These hypothesis generating exploratory analyses* will need to be confirmed in future trials *hhf is an exploratory end point in both studies. In the EMPA-REG OUTCOME protocol it was considered an exploratory end point. In CANVAS, after the MACE end point, the hierarchical testing started with all-cause mortality. This did not meet statistical significance thus no additional testing was done. Therefore the HF end point is considered exploratory Month CI, confidence interval; CV, cardiovascular; HF, heart failure; hhf, hospitalisation for heart failure; HR, hazard ratio; MACE, major adverse cardiovascular events; SGLT2, sodium-glucose cotransporter-2; T2D, type 2 diabetes. 1. Zinman B, et al. N Engl J Med. 2015;373: Neal B, et al. N Engl J Med. 2017;377:
12 While EMPA-REG and CANVAS suggest CV risk can be reduced, these results were seen in T2D patients who predominantly had established CV disease EMPA-REG OUTCOME 1 (N=7,020) >99% of patients had ecvd CANVAS 2 (N=10,142) 65.6% of patients had ecvd >99% of T2D patients in the EMPA-REG OUTCOME trial and 65.6% of the T2D patients in the CANVAS trials already had established CV disease i.e. had a previous CV event (MI, stroke) or documented atherosclerosis (coronary artery stenosis, peripheral arterial stenosis) 1,2 CV, cardiovascular; ecvd, established CV disease; MI, myocardial infarction; SGLT2, sodium glucose co-transporter 2; T2D, type 2 diabetes. 1. Zinman B, et al. N Engl J Med 2015;373: ; 2. Neal B, et al. N Engl J Med 2017;377:



13 The CVD-REAL Study Lower Rates of Hospitalization for Heart Failure and All- Cause Death in New Users of SGLT-2 Inhibitors versus Other Glucose Lowering Drugs: The CVD-REAL Study Real World Data from 6 Countries (US, UK, Germany, Sweden, Denmark, Norway) > 300,000 patients
14 Proportion of Exposure Time (%) CONTRIBUTION OF SGLT-2 INHIBITORS TO ALL-CAUSE DEATH AND HHF IN CVD REAL Toulis et al, JCEM, Feb EMPA 6.7% EMPA 5.3% EMPA 8.3% 80 DAPA 19.3% 60 DAPA 51.0% 40 CANA 75.4% DAPA 90.1% 20 CANA 42.3% Toulis et al, JCEM, Feb All countries combined US only European countries combined US, Norway, Sweden, Denmark, UK, Germany CANA 1.5
15 In CVD-REAL, a real-world study, SGLT2 inhibitors were associated with reductions in CV outcomes as well as hhf compared to oglds All-cause death and hhf for SGLT2 inhibitors vs oglds 1 Outcome N No. of events HR (95% CI) All-cause death hhf All-cause death or hhf 215, , , (0.41, 0.57) 0.61 (0.51, 0.73) 0.54 (0.48, 0.60) 13% of patients had established CVD* Compared to oglds, SGLT2 inhibitors were associated with a 39% reduction in hhf Favours SGLT2 inhibitor Favours ogld *Previous event of myocardial infarction, stroke, unstable angina, heart failure or atrial fibrillation. CI, confidence interval; CVD, cardiovascular disease; hhf, hospitalisation for heart failure; HR, hazard ratio; ogld, other glucose-lowering drug. SGLT2, sodium-glucose cotransporter-2. Kosiborod M, et al. Circulation. 2017;136:
16 Dapagliflozin versus DPP-4 inhibitors was associated with reductions in CV endpoints and death in a population with a broad cardiovascular risk profile MACE and all-cause mortality for dapagliflozin vs DPP-4 inhibitors 2 23% of patients had established Outcome MACE All-cause mortality HR (95% CI) hhf 0.62 (0.50, 0.77) 0.79 (0.67, 0.94) 0.59 (0.49, 0.72) CVD Compared to DPP4i, Dapagliflozin was associated with a 38% reduction in hhf Favors dapagliflozin Favors DPP-4 inhibitors CI, confidence interval; CV, cardiovascular; CVD, cardiovascular disease; DPP-4, dipeptidyl peptidase-4; hhf, hospitalization for heart failure; HR, hazard ratio; MACE, major adverse cardiac event; SGLT2, sodium glucose co-transporter 2; ogld, other glucose-lowering drug. 1. Persson F, et al. Diabetes Obes Metab 2018;20:








17 The CVD-REAL 2 Study (Asia Data) Lower Risk of Cardiovascular Events and Death Associated with Initiation of SGLT-2 Inhibitors versus Other Glucose Lowering Drugs Real World Data from 6 Countries (S. Korea, Japan, Singapore, Australia, Canada, Israel) > 400,000 Patients

18 Use of SGLT-2i: Proportion of Exposure Time *In South Korea and Japan; In Japan only.

19 Subgroup Analyses Outcomes With and Without CVD at Baseline ITT, adjusted analysis
20 Summary of CVD-REAL 1 & CVD-REAL 2 results All-Cause Death 51% HR: %CI (0.41,0.57) P<0.001 Hospitalization for HF 39% HR: %CI (0.51,0.73) P<0.001 All-Cause Death or Hospitalization for HF 46% HR: %CI (0.48,0.60) P<0.001 All-Cause Death Hospitalization of HF Myocardial Infarction Stroke 49% 36% 19% 32% HR: %CI (0.37,0.70) P<0.001 HR: %CI (0.50,0.82) P<0.001 HR: %CI (0.74,0.88) P<0.001 HR: %CI (0.55,0.84) P<0.001 Kosiborod M et al. Circulation Jul 18;136(3):
: Age 55 years (men), 60 years (women) AND 1 additional risk factors: Dyslipidemia Hypertension Peripheral")
 Composite endpoint of CV death, MI, stroke (MACE) Add on to background CV and GLD per treating physician Event-driven duration, with planned median duration ~4.")

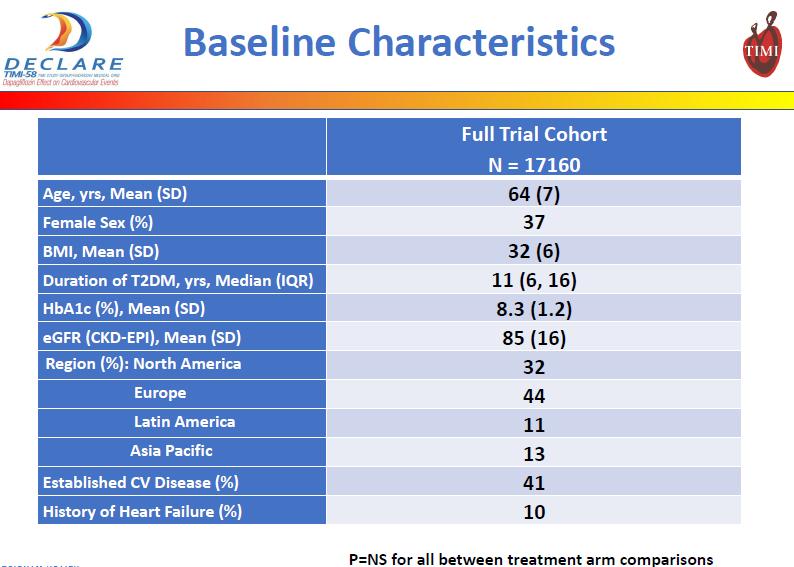
21 Co-Primary Endpoints DECLARE-TIMI58 TRIAL: THE LARGEST (N=17,160) OUTCOME TRIAL IN SGLT-2 INHIBITORS Established CV disease n=~7,000 (40%): Age 40 years AND 1 additional diagnoses: Ischemic heart disease Cerebrovascular disease Multiple risk factors n=~10,000 (60%): Age 55 years (men), 60 years (women) AND 1 additional risk factors: Dyslipidemia Hypertension Peripheral arterial disease Tobacco use Composite endpoint of T2D, 40 years plus: Placebo Hospitalization for heart failure or CV death Multiple ( 2) risk factors OR Established CVD Dapagliflozin (10 mg per day) Composite endpoint of CV death, MI, stroke (MACE) Add on to background CV and GLD per treating physician Event-driven duration, with planned median duration ~4.5 years Prior to the first interim analysis, the secondary endpoint of hhf was elevated to a composite primary endpoint of hhf and CV death Therefore DECLARE will provide a comprehensive assessment of the impact of dapagliflozin on common and important diabetesrelated CV events Raz I, et al. Presented at the 77th Scientific Sessions of the American Diabetes Association, June 9-13, 2017, San Diego, CA
22 Outcomes Primary safety outcome Non inferiority for 3-pt MACE (CV death, MI or ischaemic stroke) Co-primary efficacy outcomes Composite of CV death or hospitalization for heart failure 3-pt MACE Secondary outcomes Renal composite (40% fall in egfr, ESRD or renal or CV death) All-cause mortality

23 DECLARE Study Population China + HONG KONG ~300 subjects
24
25
26
27
28
29
30
31
32
33

34
35 Differences and similarities between SGLT2 inhibitor CVOT DECLARE-TIMI 58 EMPA-REG CANVAS Intervention Dapaglifloxin / PBO Empagliflozin / PBO Canagliflozin / PBO Patient number 17,160 7,020 10,142 HbA1c <12.0% 7.0%-10.0% 7.0%-10.5% Established CVD Yes Yes Yes Multiple risk factors without established CVD Yes No Yes Renal function CrCl >60 ml/min egfr 30 ml/min/1.73m 2 egfr 30 ml/min/1.73m 2 Primary endpoint(s) Co-primary: MACE hhf or CV death Target number of events 1, Estimated follow-up ~4.5 years 3.1 years 5.7 years MACE MACE


")
36 2018 American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD) Consensus Report
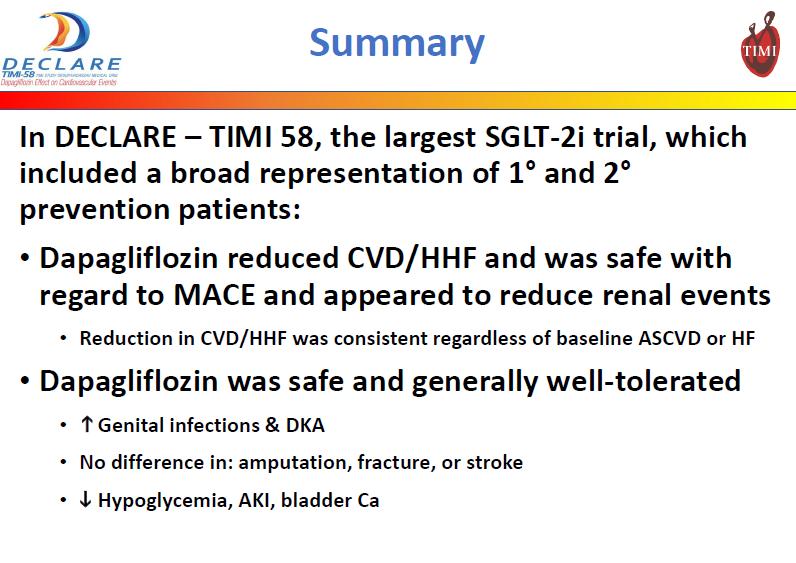
37 Heart failure: Preventable and Treatable CV complication of Diabetes Diabetes is an independent risk factor for heart failure (HF) HF is an early complication of T2D with significant morbidity and mortality When choosing an antidiabetic therapy, the impact on HF merits consideration Exploratory analyses of RCTs suggest that SGLT2 inhibitors reduce hhf in those with prior CVD DECLARE-TIMI 58 results and CVD REAL 1 & 2 suggest that this extends to those without prior CVD (mainly for dapagliflozin)
38 Summary The pattern of complications of diabetes is changing Improvements in some classical complications; emergence of newer complications RCTs show CVD benefits for SGLT2i and GLP1 agonists Findings predominantly in secondary prevention Real world evidence for SGLT2i suggests: Benefits are seen outside clinical trials Benefits extend to primary prevention Benefits extend to Asian populations DECLARE extends SGLT2i RCT benefits to primary prevention

39 Recent evidence on individualizing cardio-protective therapy in DM For people with prior CVD Strong evidence of benefit for SGLT2i Evidence of modest benefit for liraglutide Suggestive evidence of benefit of exenatide All people with T2DM & prior CVD should be considered for an SGLT2i or GLP1 agonist For people without prior CVD DECLARE and CVD REAL indicate benefit of SGLT2i (mainly dapagliflozin) SGLT2i becoming the preferred second line agent
40 Thank You
41 A number of possible mechanisms of CV benefit with SGTL2 inhibitors have been put forward Improved endothelial function Reduced sodium load Reduced tissue sodium accumulation Evidence supporting potential mechanisms is sparse Reduction in blood pressure Decreased systemic glucose load There has been considerable discussion about three potential mechanisms Improvements in hemodynamics Super-fuel hypothesis Decreased glucose trafficking and metabolism Super fuel hypothesis Increased haemotocrit Improved oxygen delivery CV, cardiovascular; SGLT2, sodium-glucose cotransporter-2. Mudaliar S, et al. Diabetes Care. 2016;39:
42 The super-fuel hypothesis suggests that SGLT2 inhibitors shift fuel metabolism to a more efficient source Improvements in Myocardial energy substrate metabolism Myocardial contractility Cardiac efficiency by shifting to a more energy-efficient fuel: ketone bodies instead of fatty acids/glucose By shifting fuel utilisation away from lipids and glucose (which are less energy efficient) toward ketone bodies that produce ATP energy more efficiently than glucose or FFA, SGLT2 inhibitors improve myocardial fuel metabolism, myocardial contractility, and cardiac efficiency SGLT2, sodium-glucose cotransporter-2. Mudaliar S, et al. Diabetes Care. 2016;39:
43 Haematocrit (%) Red cell mass change from baseline (%) SGLT2 inhibitor-associated increased haematocrit and red blood cell mass may increase tissue oxygen delivery Pooled data from 17 randomised trials in patients with T2DM 1 Increased red blood cell mass (~6%) was observed following treatment with dapagliflozin 2 Changes in hematocrit with empagliflozin n=3695 [VALUE] % n=3806 [VALUE] % n=4782 [VALUE] % P: -1.2 (-3.2 to +1.3) D: +6.6 (+1.0 to +9.3) H: -6.5 (-16.1 to +3.8) -2 Placebo EMPA 10 mg EMPA 25 mg -40 Placebo Dapagliflozin Hydrochlorothiazide EMPA, empagliflozin; SGLT2, sodium-glucose cotransporter Kohler S. Clin Ther. 2016;38: Lambers-Heerspink HJ, et al. Diabetes Obes Metab. 2013;15:
44 Primary End Points Heart failure hospitalization is well characterized in DECLARE TIMI-58 Hospitalization for HF is prespecified in a primary endpoint as part of a composite with CV death Adjudication criteria for hhf are defined from study start Baseline LV-function data are collected where available and blood samples for biomarkers like NT-proBNP are collected Composite end point of CV death, MI, stroke (MACE) Composite end point of Hospitalization for heart failure or CV death CV, cardiovascular; hhf, hospitalization for heart failure; LV, left ventricular; NT-proBNP, N-terminal pro b-type natriuretic peptide. 1. Raz I, et al. Diabetes Obes Metab Wiviott SD, et al. Am Heart J
45 CANVAS vs EMPAR-REG OUTCOME - Effect on MI and stroke??
46 DECLARE has the largest number of T2D patients without prior CVD among the SGLT2i CV outcomes studies to date In the T2D patient population, most patients do not have established CV disease 1 EMPA-REG OUTCOME 2 (N=7,020) <1% CANVAS 3 (N=10,142) 34.4% (n=3,486) DECLARE 4 (N=17,160) 59.4% (n=10,189) CV, cardiovascular; CVD, CV disease; SGLT2i, sodium glucose co-transporter 2 inhibitor; T2D, type 2 diabetes 1. Einarson TR, et al. Cardiovasc Diabetol 2018;17:83; 2. Zinman B, et al. N Engl J Med 2015;373: ; 3. Neal B, et al. N Engl J Med 2017;377: ; 4. Raz I, et al. Diabetes Obes Metab 2018;20:
47
48
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
La lezione dei trials di safety cardiovascolare. Edoardo Mannucci
 La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
La lezione dei trials di safety cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician
 Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Heart Failure Management in T2 DM A Practical Approach. David Fitchett MD St Michael s Hospital Toronto
 Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Effect of SGLT-2 Inhibitors on the Heart. Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic
 Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD
 HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD Author affiliations: Department of Cardiology, Hôpital Saint Joseph, Paris, France Address for correspondence: Michel Komajda,
HEART FAILURE AND DIABETES MELLITUS: DANGEROUS LIASONS MICHEL KOMAJDA, MD Author affiliations: Department of Cardiology, Hôpital Saint Joseph, Paris, France Address for correspondence: Michel Komajda,
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus
 Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus Mikhail Kosiborod, MD Professor of Medicine (Cardiology) Saint Luke s Mid America Heart Institute University of
Emergence of the New Classes of Compounds for Managing Heart Disease in Diabetes Mellitus Mikhail Kosiborod, MD Professor of Medicine (Cardiology) Saint Luke s Mid America Heart Institute University of
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Review of FDA Guidance on Cardiovascular Outcomes for Diabetes Medication Trials and Application to Clinical Management
 Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Katherine S. O Neal Pharm.D., MBA, BCACP, CDE, BC-ADM, AE-C Associate Professor The University of Oklahoma Health Sciences Center College of Pharmacy Department of Internal Medicine Oklahoma City, OK Member,
Sodium-glucose cotransporter 2 inhibitors and death and heart failure in type 2 diabetes
 Editorial Page 1 of 5 Sodium-glucose cotransporter 2 inhibitors and death and heart failure in type 2 diabetes Hidekatsu Yanai Department of Internal Medicine, National Center for Global Health and Medicine
Editorial Page 1 of 5 Sodium-glucose cotransporter 2 inhibitors and death and heart failure in type 2 diabetes Hidekatsu Yanai Department of Internal Medicine, National Center for Global Health and Medicine
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
Congestive Heart Failure: The Complication that Gets No Respect Richard J. Katz, MD Saturday, February 18, :30 a.m. 10:15 a.m.
 Congestive Heart Failure: The Complication that Gets No Respect Richard J. Katz, MD Saturday, February 18, 2017 9:30 a.m. 10:15 a.m. The prevalence of the combination of diabetes and both systolic and
Congestive Heart Failure: The Complication that Gets No Respect Richard J. Katz, MD Saturday, February 18, 2017 9:30 a.m. 10:15 a.m. The prevalence of the combination of diabetes and both systolic and
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Lower Risk of Death With SGLT2 Inhibitors in Observational Studies: Real or Bias? Diabetes Care 2018;41:6 10
 6 Diabetes Care Volume 41, January 2018 PERSPECTIVES IN CARE Lower Risk of Death With SGLT2 Inhibitors in Observational Studies: Real or Bias? Diabetes Care 2018;41:6 10 https://doi.org/10.2337/dc17-1223
6 Diabetes Care Volume 41, January 2018 PERSPECTIVES IN CARE Lower Risk of Death With SGLT2 Inhibitors in Observational Studies: Real or Bias? Diabetes Care 2018;41:6 10 https://doi.org/10.2337/dc17-1223
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Disclosures. Objectives. Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials 8/28/2017
 Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Bryan Cardiology Conference DM2 & Cardiovascular Outcome Trials Shannon Wakeley MD Complete Endocrinology 9/2/2017 Disclosures Speakers Bureau: Astra Zeneca, Sanofi, Abbvie, Boehringer-Ingelheim, Medtronic,
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS?
 MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS? Ralph A. DeFronzo, M.D. Professor of Medicine Chief, Diabetes Division University of Texas Health Science Center San Antonio, Texas
MANAGING THE HYPERGLYCEMIA OF DIABETES: SHOULD CVOTs IMPACT MEDICATIONS? Ralph A. DeFronzo, M.D. Professor of Medicine Chief, Diabetes Division University of Texas Health Science Center San Antonio, Texas
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus
 Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Nevada Academy of Family Physicians 29 th Annual Summer CME Meeting August 3 5, 2018 An Update on Guidelines and Evidence of the Treatment of Type 2 Diabetes Mellitus Presented by: James D. Honeycutt,
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale
 Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale Dichiarazione esplicita di trasparenza delle fonti di finanziamento e dei
Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale Dichiarazione esplicita di trasparenza delle fonti di finanziamento e dei
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
Current Updates & Challenges In Managing Diabetes in CVD
 Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Diabetes Drugs and Cardiac Disease. Disclosures
 Diabetes Drugs and Cardiac Disease Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Disclosures None 1 Written Comments As I have said every
Diabetes Drugs and Cardiac Disease Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco robert.rushakoff@ucsf.edu Disclosures None 1 Written Comments As I have said every
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Cardiovascular Consequences of Diabetes Mellitus
 Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know. Hani Sabbour MD FACC FHRS
 Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Cardiovascular outcome studies with glucagon-like peptide 1 receptor agonists what will REWIND add?
 Editorial Page 1 of 5 Cardiovascular outcome studies with glucagon-like peptide 1 receptor agonists what will REWIND add? Keith C. Ferdinand, Indrajeet Mahata Department of Medicine, Tulane School of Medicine,
Editorial Page 1 of 5 Cardiovascular outcome studies with glucagon-like peptide 1 receptor agonists what will REWIND add? Keith C. Ferdinand, Indrajeet Mahata Department of Medicine, Tulane School of Medicine,
DISCLOSURES. Learning objectives NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Investigator Initiated Trial Support:
 NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
Glucose Lowering Medications and CV Risk Reduction: A New Era Jane EB Reusch MD ADA President for Medicine and Science
 Glucose Lowering Medications and CV Risk Reduction: A New Era Jane EB Reusch MD ADA President for Medicine and Science Professor of Medicine, Division of Endocrinology, Metabolism and Diabetes and Associate
Glucose Lowering Medications and CV Risk Reduction: A New Era Jane EB Reusch MD ADA President for Medicine and Science Professor of Medicine, Division of Endocrinology, Metabolism and Diabetes and Associate
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
New Therapies for Type 2 Diabetes
 New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New Therapies for Type 2 Diabetes
 New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
New for Type 2 Diabetes Joshua J. Joseph, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio State University Wexner Medical Center Financial Disclosures: None
Class Update: Sodium-glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Dapagliflozin and Outcomes in Patients with Peripheral Artery Disease: Insights from DECLARE-TIMI 58
 Dapagliflozin and Outcomes in Patients with Peripheral Artery Disease: Insights from DECLARE-TIMI 58 Marc P. Bonaca MD MPH for the DECLARE TIMI 58 Investigators American College of Cardiology March 2019
Dapagliflozin and Outcomes in Patients with Peripheral Artery Disease: Insights from DECLARE-TIMI 58 Marc P. Bonaca MD MPH for the DECLARE TIMI 58 Investigators American College of Cardiology March 2019
Class Update: Sodium glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Endocrinologist Sweetgrass Endocrinology
 Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
SGLT2 and cardiovascular events: Why did EMPA-REG Outcomes surprise and what were the likely mechanisms? David Preiss, 3 John J McMurray 1
 SGLT2 and cardiovascular events: Why did EMPA-REG Outcomes surprise and what were the likely mechanisms? Naveed Sattar, 1 James McLaren, 1 Søren L Kristensen, 2 David Preiss, 3 John J McMurray 1 1 Institute
SGLT2 and cardiovascular events: Why did EMPA-REG Outcomes surprise and what were the likely mechanisms? Naveed Sattar, 1 James McLaren, 1 Søren L Kristensen, 2 David Preiss, 3 John J McMurray 1 1 Institute
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA
 Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
Diabetes and Heart Failure: Challenges and Opportunities
 AHA Get With The Guidelines-Heart Failure Webinar Diabetes and Heart Failure: Challenges and Opportunities Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA
AHA Get With The Guidelines-Heart Failure Webinar Diabetes and Heart Failure: Challenges and Opportunities Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
THE EVOLUTION OF CLINICAL TRIALS IN T2DM: FROM TARGETING A1C TO TARGETING CARDIOVASCULAR OUTCOMES
 Learning Objectives 1) Evaluate the interrelationship between diabetes, glycemic control, and cardiovascular disease. 2) Examine the evolution of type 2 diabetes (T2DM) drug development and factors leading
Learning Objectives 1) Evaluate the interrelationship between diabetes, glycemic control, and cardiovascular disease. 2) Examine the evolution of type 2 diabetes (T2DM) drug development and factors leading
Educational Objectives
 Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
Educational Objectives Recognize the rationale for cardiovascular outcome trials (CVOTs) in T2DM and review data from recent CVOTs of anti hyperglycemic agents Examine alignment of managed care T2DM treatment
SGLT2 Inhibition and cardiovascular events: why did EMPA-REG Outcomes surprise and what were the likely mechanisms?
 Diabetologia (2016) 59:1333 1339 DOI 10.1007/s00125-016-3956-x REVIEW SGLT2 Inhibition and cardiovascular events: why did EMPA-REG Outcomes surprise and what were the likely mechanisms? Naveed Sattar 1
Diabetologia (2016) 59:1333 1339 DOI 10.1007/s00125-016-3956-x REVIEW SGLT2 Inhibition and cardiovascular events: why did EMPA-REG Outcomes surprise and what were the likely mechanisms? Naveed Sattar 1
Impatto dei farmaci antidiabetici sullo scompenso cardiaco
 Impatto dei farmaci antidiabetici sullo scompenso cardiaco Riccardo Candido S.S.D. Gestione Rete Diabetologica Aziendale Azienda Sanitaria Universitaria Integrata di Triste Il sottoscritto Riccardo Candido
Impatto dei farmaci antidiabetici sullo scompenso cardiaco Riccardo Candido S.S.D. Gestione Rete Diabetologica Aziendale Azienda Sanitaria Universitaria Integrata di Triste Il sottoscritto Riccardo Candido
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Drug Class Monograph
 Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center