Medical Therapy: Indications
|
|
|
- Baldwin Montgomery
- 5 years ago
- Views:
Transcription
1
2 Medical Therapy: Indications Severe complications of hypercortisolism Pre-treatment before pituitary surgery Post-treatment after unsuccessful surgery Bridging therapy before, during and after pituitary radiation Primary medical therapy (contraindications for surgery or refusal of surgery)

3 Potential Targets for Medical Therapy in Cushing s Disease Pituitary gland CRH Pasireotide Cabergoline Adrenal glands Ketoconazole Metyrapone Mitotane LCI699 ACTH Cortisol Mifepristone Glucocorticoid receptors
4 The use of pasireotide: rationale Limited number of effective medical therapies available and none licenced for CD Pasireotide Somatostatin analogue targeting multiple somatostatin receptor subtypes 1 Highest affinity for sst 5, the most prevalent somatostatin receptor subtype on ACTH-secreting pituitary adenomas 2 Inhibits ACTH production in corticotroph adenomas in vitro 3 Phase 2, 15-day study demonstrated promising clinical efficacy 4 1. Bruns C et al. Eur J Endocrinol 2002;146: Hofland LJ et al. Endocr Rev 2003;24: Hofland LJ et al. Eur J Endocrinol 2005;152: Boscaro M et al. J Clin Endocrinol Metab 2009;94:


5 B2305: Largest Cushing s Disease Trial Colao A et al. N Engl J Med 2012;366: countries, 62 sites 329 patients screened 162 patients randomized Argentina, Belgium, Brazil, Canada, China, Denmark, Finland, France, Germany, Source: xxxxxxxxx Greece, Israel, Italy, Mexico, Poland, Portugal, Spain, Turkey, United States
6 Study Design Core study Extension Primary efficacy (Normalization of UFC without dose up-titration before 6 months) n= μg BID (unblinded)* Screening Washout of other meds Pasireotide 600 μg sc BID Pasireotide 900 μg sc BID n= μg bid 1200 μg BID (unblinded)* 900 µg BID dose titration per investigator Optional extension phase Month 1 Day 1 Month 3 Month 6 Month 12 Screening Double blind Partially blind Open label *For patients who had a mean baseline UFC 2x ULN with a 3-month UFC >2x ULN OR For patients who had a mean baseline UFC 1.5 2x ULN with a 3-month UFC above their baseline UFC Colao A et al. N Engl J Med 2012;366:
7 Baseline Demographics by Randomized Dose Overall n= µg BID n= µg BID n=80 Mean age, (years) Female, n (%) 126 (77.8) 62 (75.6) 64 (80.0) Time since diagnosis (months) Cushing s disease status Persistent/recurrent, n (%) 135 (83.3) 67 (81.7) 68 (85.0) De novo, n (%) 27 (16.7) 15 (18.3) 12 (15.0) Previous surgery, n (%) 128 (79.0) 64 (78.0) 64 (80.0) Previous medication, n (%) 78 (48.1) 36 (43.9) 42 (52.5) Previous pituitary irradiation, n (%) 7 (4.3) 3 (3.7) 4 (5.0) Colao A et al. N Engl J Med 2012;366:
8 Baseline UFC by randomized dose ~8xULN Baseline UFC, nmol/24h 600 µg bid (n=77) 900 µg bid (n=76) Overall (n=153) 1015 Mean Mean UFC (nmol/24h) ~5xULN SD Median Min Max ULN: 145 nmol/24h µg bid 900 µg bid Colao A et al. N Engl J Med 2012;366:
9 Distribution of baseline UFC At baseline, 78% of patients had moderate to very severe hypercortisolism Proportion of patients (%) % 5% 13% 11% 34% 32% 16% 50% Missing >10xULN >5x to 10xULN >2x to 5xULN 0 15% 18% 600 μg bid 900 μg bid 1.5 to 2xULN Colao A et al. N Engl J Med 2012;366:
10 Patient disposition 329 patients screened Overall, n (%) N= μg bid, n (%) N= μg bid, n (%) N=80 Disposition Completed month (66.0) 54 (65.9) 53 (66.3) Completed month (48.1) 39 (47.6) 39 (48.8) Reason for discontinuation Unsatisfactory therapeutic effect 41 (25.3) 19 (23.2) 22 (27.5) Adverse event(s) 28 (17.3) 13 (15.9) 15 (18.8) Subject withdrew consent 24 (14.8) 13 (15.9) 11 (13.8) Protocol deviation 4 (2.5) 4 (4.9) 0 Colao A et al. N Engl J Med 2012;366:
11 Reasons for patient discontinuation Protocol deviation Withdrawal of consent Patient discontinuations (n) Lack of efficacy Adverse event months 3 6 months 6 12 months Patients who discontinued (n) Patients ongoing (n) Colao A et al. N Engl J Med 2012;366:
12 Change in UFC from Baseline to Month 6 in the 103 patients with baseline and month-6 UFC measurements µg BID 900 µg BID * Baseline UFC Month 6 UFC Month 6 UFC ULN UFC (nmol/24 h) ULN Median percentage UFC change from baseline was 47.9% in both groups Reference line is the upper limit of normal UFC, which is 145 nmol/24 h (52.5 µg/24 h) Colao A et al. N Engl J Med 2012;366:
13 Mean UFC Levels Showed a Rapid and Robust Reduction That Was Maintained Over Time Mean UFC ± SE (nmol/24 h) n = ULN: 145 nmol/24 h (52.5 µg) 600 µg BID 900 µg BID Similar trends seen for: Serum cortisol Salivary cortisol Month Statistically significant (p<0.001) decrease from baseline to month 6 and month 12 for both dose groups Colao A et al. N Engl J Med 2012;366:
14 Primary Efficacy Results 600 µg BID (n=82) 900 µg BID (n=80) Overall (n=162) 6 months *Response, n (%) [95% CI] 12 (14.6) [7.0, 22.3] 21 (26.3) [16.6, 35.9] 33 (20.4) [14.2, 26.6] 12 months Fully controlled, n (%) 11 (13.4) 20 (25.0) 31 (19.1) *Note: Responder was a patient with UFC ULN who did not require uptitration Fully controlled: UFC ULN The predetermined criterion for the primary efficacy endpoint was that the lower bound of the 95% CI had to be >15% for at least one of the dose groups; this was met for the 900 µg group Colao A et al. N Engl J Med 2012;366:
15 Response Rates at Month µg BID (n=82) 900 µg BID (n=80) Fully controlled 13 (15.9%) 23 (28.8%) Partially controlled 15 (18.3%) 10 (12.5%) Uncontrolled 54 (65.9%) 47 (58.8%) 34% 41% Fully controlled: UFC ULN; partially controlled: UFC >ULN, but had 50% reduction from baseline; Uncontrolled: UFC >ULN and <50% reduction from baseline At month 6, 41.3% of patients treated with 900 µg BID were controlled or partially controlled Colao A et al. N Engl J Med 2012;366:
16 Which is the real potential of disease control of pasireotide? Is the dose of 900 µg more efficacious than the dose of 600 µg twice a day in term of chance of hormone control?
17 Early prediction of uncontrolled patients at months 6 and 12 Within 1 2 months, patients who will remain uncontrolled can be identified Early nonresponders Month 6 response Month 12 response UC FC PC UC FC PC UC Months 1 + 2, n (%) 72 (100.0) 4 (5.6) 2 (2.8) 66 (91.7) 6 (8.3) 2 (2.8) 64 (88.9) Months , n (%) 63 (100.0) 2 (3.2) 1 (1.6) 60 (95.2) 5 (7.9) 1 (1.6) 57 (90.5) Colao A et al. N Engl J Med 2012;366: Fully controlled (FC): UFC ULN Partially controlled (PC): UFC >ULN but had 50% reduction from baseline Uncontrolled (UC): UFC >ULN and <50% reduction from baseline, or missing values
18 Baseline UFC level and response at month 6 Higher rate of UFC normalization with lower baseline UFC 600 µg bid (n=82) Baseline UFC shown as fold elevations above ULN >5x >2x to 5x >1.5 to 2x 4/39 1/22 1/12 7/26 10/ µg bid (n=80) 7/ Patients achieving normal UFC at month 6 (%) Colao A et al. N Engl J Med 2012;366:
19 What to do with patients partially controlled by pasireotide? Withdrawal? Combination with another drug? Criteria? Which drug?
20 Mean UFC ± SE (nmol/24 h) Significant Decrease in Blood Pressure Systolic blood pressure (SBP) Month and UFC Mean UFC Mean SBP B Diastolic blood pressure (DBP) Mean UFC Mean DBP B Colao A et al. N Engl J Med 2012;366: Mean BP ± SE (mmhg) Significant (p=0.03) change from baseline to month 12 was observed for: SBP 6.1 mmhg (95% CI: 9.8, 2.4) DBP 3.7 mmhg (95% CI: 6.2, 1.2) Note: Changes in anti-hypertensive medicines were allowed
21 Significant Decrease in Weight and UFC Significant (p<0.0001) decrease in weight of 6.7 kg from baseline to month 12 (95% CI: 8.0, 5.4) Mean UFC ± SE (µg/24 h) Mean UFC Mean weight Mean weight ± SE (kg) 0 B Month Colao A et al. N Engl J Med 2012;366:
22 Significant Decrease in BMI and UFC Significant decrease in BMI of 2.5 kg/m 2 from baseline to month 12 (95%CI: 3.0, 2.0) Mean UFC ± SE (µg/24 h) Mean UFC Mean BMI Mean BMI ± SE (kg/m 2 ) 0 B Month Colao A et al. N Engl J Med 2012;366:
23 Significant Decrease in LDL-cholesterol and UFC Significant (p<0.001) decrease in LDL-cholesterol of 0.4 mmol/l from baseline to month 12 (95% CI: 0.6, 0.2) Mean UFC ± SE (µg/24 h) B Month Colao A et al. N Engl J Med 2012;366: Mean UFC Mean LDL-cholesterol Mean LDL-cholesterol ± SE (mmol/l)
24 Significant Improvement in HRQoL and UFC Measured via Cushing QoL Significant (11.1 points) improvement from baseline to month 12 (95% CI: 6.8, 15.5) Mean UFC ± SE (µg/24 h) Mean UFC Mean HRQoL Mean HRQoL score 0 B Month Colao A et al. N Engl J Med 2012;366:
25 Improvements in Signs of Cushing s Disease After 12 months of treatment, a high proportion of patients still enrolled also had improvements in the signs of Cushing s disease Proportion of patients with improvement (%) 600 µg BID 900 µg BID Facial rubor Striae Bruising Supraclavicular fat pads Dorsal fat pads Muscle strength Colao A et al. N Engl J Med 2012;366:


26 Improvements in Signs and Symptoms as Mean UFC Decreased: Clinical Case Baseline, 900 µg BID Month 15,* 900 µg BID UFC: 417 nmol/24 h Weight: 76 kg SBP: 122 mmhg UFC: 54.5 nmol/24 h Weight : 55 kg SBP: 110 mmhg * Photograph taken at month 12; Courtesy of Dr Feng Gu, China
27 Improvement in Tumor Volume Following Treatment With Pasireotide sc BID Tumor volume was assessed by MRI at baseline, month 6 and 12 At baseline 75 patients (46%) had a measureable pituitary tumor Median tumor volume was 0.24 cm 3 in the 600 μg group (n=36) and 0.20 cm 3 in the 900 μg group (n=39) Colao A et al. N Engl J Med 2012;366:

28 Change in Tumor Volume From Baseline % mean change (95% CI) from baseline ,3 n = Colao A et al. N Engl J Med 2012;366: Study B2305 n = n = Month 6 Month µg 900 µg n = 18
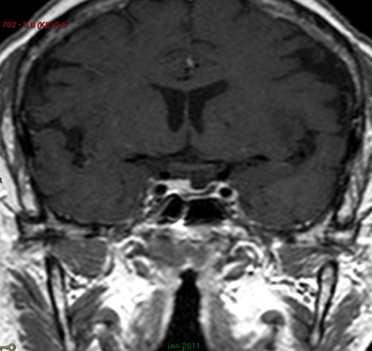
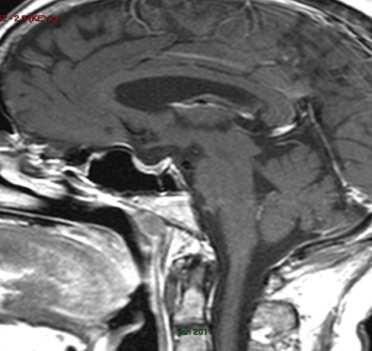
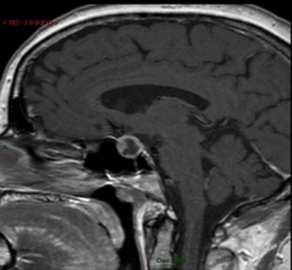
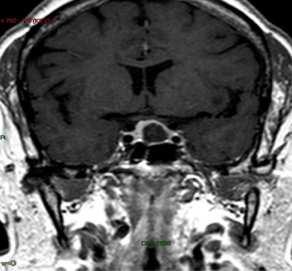
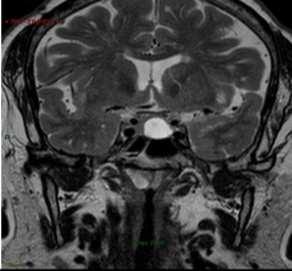
29 Significant Decrease in Tumor Volume Baseline 24 months pasireotide Shimon. Pituitary Dec;15(4):608-13
30 Why this difference in tumor shrinkage with the two different dose of pasireotide?
31 Sustained reductions in UFC were observed through to month patients entered a 12-month extension phase 1,2 Mean decreases in UFC were maintained up to 24 months 1 Mean UFC (nmol/24h) Pasireotide 600 µg bid Pasireotide 900 µg bid ULN (145 nmol/24h) Reductions in serum cortisol and plasma ACTH, as well as improvements in signs and symptoms, were sustained 1 Core study (months) Extension phase (months) 1 Bertherat J et al. EndocrRev 2012;33:abst SUN-734; 2 Bertherat J et al. EndocrRev 2012;33:abst SUN-735
32 Control of UFC was observed up to Patients with UFC ULN (%) month µg bid 900 µg bid 34.5% of patients who entered the extension phase had UFC ULN at month 24 0 Month Responders (n) Core study (month) Extension phase (month)
33 Safety summary at the month-12 cut-off Treatment duration was up to 38 months (mean 10.8) 600 µg bid (n=82) 900 µg bid (n=80) Overall (n=162) Adverse events (AEs), n (%) 80 (97.6) 79 (98.8) 159 (98.1) Drug-related AEs 79 (96.3) 76 (95.0) 155 (95.7) Discontinued due to AEs 13 (15.9) 15 (18.8) 28 (17.3) Grade 3 or 4 AEs 39 (47.6) 40 (50.0) 79 (48.8) AEs of special interest, n (%) 79 (96.3) 77 (96.3) 156 (96.3) Serious adverse events (SAEs), n (%) 19 (23.2) 21 (26.3) 40 (24.7) Drug-related SAEs 7 (8.5) 12 (15.0) 19 (11.7) Discontinued due to SAEs 3 (3.7) 5 (6.3) 8 (4.9) Deaths during treatment, n (%)* Colao A et al. N Engl J Med 2012;366:
34 Most common AEs at 12 months Overall (N=162) AE All grades n (%) Grades 3 or 4 n (%) Hyperglycemia related 118 (72.8) 40 (24.7) Diarrhea related 95 (58.6) 5 (3.1) Nausea related 85 (52.5) 4 (2.5) Gallbladder and biliary related 54 (33.3) 4 (2.5) Liver chemistry related 26 (16.0) 7 (4.3) Bradycardia related 23 (14.2) 3 (1.9) Hypocortisolism related 13 (8.0) 4 (2.5) QT prolongation related 13 (8.0) 4 (2.5) Hypothyroidism related 7 (4.3) 0 Colao A et al. N Engl J Med 2012;366: Grading (1 4) of AEs follows the US HHS Common Terminology Criteria for Adverse Events (CTCAE) Common AE terms were pooled, for example, all terms relating to elevations in blood glucose or terms relating to diarrhea
35 Hypocortisolism is a risk of any effective treatment for Cushing s disease No standard definition of hypocortisolism; AEs were determined by the investigator Among the patients with UFC ULN, 13 patients had hypocortisolism-related AEs, reported as: Adrenal insufficiency (n=9) Blood cortisol decreased (n=1) UFC decreased (n=2) Hypocortisolism Secondary adrenocortical insufficiency (n=1) Patients responded to a reduction in pasireotide dose and/or short-term exogenous steroid treatment ULN, upper limit of normal
36 Gallbladder changes from baseline Changes from baseline to last assessment, n (%) Baseline Normal Sludge Gallstones Biliary duct dilatation Missing ultrasound Normal (n=137) 83 (60.6) 9 (6.6) 27 (19.7) 0 18 (13.1) Most cases were asymptomatic Six patients underwent cholecystectomy Comparable to other somatostatin analogues in Caucasians
37 Liver biochemistry As with other somatostatin analogues, there was a mild, transient elevation in liver enzyme levels (~30% of patients) In most patients, enzyme levels decreased to baseline during continued pasireotide treatment Six patients discontinued because of elevated liver enzymes There were no cases of concomitant elevations of AST/ALT >3xULN and bilirubin >ULN (accepted regulatory marker for severe liver injury) ALT, alanine aminotransferase; AST, aspartate aminotransferase
38 Adverse events suspected to be study drug related at month 24 Treatment duration was up to 42 months (mean 27.1) CTCAE grades 3 & 4 Overall (n=162) All grades Diarrhea 4 (2.5) 90 (55.6) Nausea 4 (2.5) 78 (48.1) Hyperglycemia 19 (11.7) 63 (38.9) Cholelithiasis 2 (1.2) 51 (31.5) Safety profile at month 24 was similar to that at month 12 Abdominal pain 3 ( (20.4) Diabetes mellitus 14 (8.6) 33 (20.4) Fatigue 3 (1.9) 21 (13.0) HbA 1c elevation 1 (0.6) 17 (10.5) Type 2 diabetes mellitus 7 (4.3) 15 (9.3) GGT elevation 5 (3.1) 15 (9.3) ALT elevation 3 (1.9) 15 (9.3) Headache 1 (0.6) 14 (8.6) Influenza 0 14 (8.6) Bertherat J et al. Endocr Rev 2012;33:abst SUN-735 No new safety issues observed Grading (1 4) of AEs follows the US HHS Common Terminology Criteria for Adverse Events (CTCAE) 2009: Grade 3 = severe AE; grade 4 = life-threatening or disabling AE GGT, γ-glutamyltransferase; HbA 1c, glycosylated hemoglobin
39 Changes in glycemia Mean fasting plasma glucose (mg/dl) Baseline Day 15 Month 3 Month 6 Month µg bid(n=82) 900 µg bid(n=80) µg bid(n=82) 900 µg bid(n=80) Mean HbA 1c (%) Baseline Month 2 Month 6 Month 12
40 Time to first hyperglycemia-related AE µg bid(n=82) 900 µg bid(n=80) Proportion of patients with events Number of events Kaplan-Meier median 600 µg bid µg bid Log-rankPvalue = Time (months)
41 Changes in antidiabetic medication At the month-12 cut-off, antidiabetic medication was initiated in 74 of 162 patients 41% of patients (53/129) not receiving glucose-lowering medication at baseline initiated 1 antidiabetic medication 64% of patients (21/33) receiving antidiabetic medication at baseline received 1 additional agent Among patients in whom glucose-lowering therapy was initiated during the study, reductions in mean fasting plasma glucose were observed to mg/dl (9.2 to 6.7 mmol/l) in the 600 μg group to mg/dl (8.9 to 7.4 mmol/l) in the 900 μg group
42 Changes from baseline in diabetes status Changes from baseline to last assessment, n (%) Baseline Normal Pre-diabetic Diabetic Missing Normal (n=67) 14 (21) 29 (43) 23 (34) 1 (1.5) Pre-diabetic (n=39) 1 (3) 9 (23) 28 (72) 1 (3) Diabetic (n=55) 1 (2) 6 (11) 47 (85) 1 (2) Missing (n=1) 1 (100) Patients with pre-diabetes had a higher risk of developing diabetes
43 Glycemia remained stable to month Mean fasting plasma glucose levels (mg/dl) Time (months) Pasireotide 600 μg Pasireotide 900 μg Mean HbA 1c (%) Time (months)
44 Role of somatostatin in glucose metabolism Somatostatin is an inhibitor of both insulin and glucagon secretion 1 Binds with high affinity to the five somatostatin receptor subtypes 2 sst 2 and sst 5 are the predominantly expressed subtypes in human pancreatic islet cells 3 Inhibition of insulin is mediated mainly by sst 2 and sst 5 in humans 4,5 Inhibition of glucagon is mediated almost entirely by sst 2 6,7 Pasireotide is a multireceptor-targeted somatostatin analogue with high binding affinity for sst 1 3 and sst 5 1 Hauge-Evans AC et al. Diabetes 2009;58: ; 2 Patel YC. Front Neuroendocrinol 1999;20: ; 3 Kumar U et al. Diabetes 1999;48:77 85; 4 Fagan SP et al.surgery 1998;124: ; 5 Zambre Y et al. BiochemPharmacol 1999;57: ; 6 Singh V et al. JClinEndocrinolMetab 2007;92: ; 7 Singh V et al. Endocrinology 2007;148:
45 Role of somatostatin in glucose homeostasis Somatostatin is an inhibitor of both insulin and glucagon secretion a Somatostatin Receptors sst 2 sst 5 sst expression in human pancreatic β-cells b sst expression in human pancreatic α-cells b Receptor binding affinity Pasireotide c Octreotide c Inhibition of insulin d,e Inhibition of glucagon f a Hauge-Evans AC, et al. Diabetes. 2009;58(2): ; b Kumar U, et al. Diabetes. 1999;48(1):77-85; c Adapted from Bruns C, et al. Eur J Endocrinol. 2002;146(5): ; d Zambre Y, et al. Biochem Pharmacol. 1999;57(10): ; e Singh V, et al. J Clin Endocrinol Metab. 2007;92(2): ; f Patel YC. Front Neuroendocrinol. 1999;20(3):
46 Evaluating the underlying mechanism of pasireotide-related hyperglycemia Two studies have been conducted to assess the mechanism(s) responsible for pasireotide-related hyperglycemia SOM230B2216: Double-blind, randomized, single-center trial in healthy male volunteers evaluating the mechanism responsible for pasireotide-related hyperglycemia SOM230B2124: Randomized, open-label, single-center study evaluating the effects of the co-administration of antihyperglycemicagents and pasireotide, compared with pasireotide alone, on glucose metabolism in healthy male volunteers
47 SOM230B2216: Study design Mechanistic study Pasireotide 600 µg bid sc Days 3 10 (n=19) Healthy male volunteers (n=45) BASELINE Pasireotide 900 µg bid sc Days 3 10 (n=19) Pasireotide 1200 µg bid sc* Days 3 10 (n=7) Screening Days 1 3 Baseline tests Day 1: OGTT Day 2: HCT Day 3: HECT Day 3 (begin pasireotide dosing) Days 8 10 End-of-study tests Day 8: OGTT Day 9: HCT Day 10: HECT Henry RR et al. ENDO 2011;abst P3-274 *1200 µg bid sc arm was closed due to AEs of nausea and vomiting OGTT, oral glucose tolerance test; HECT, hyperinsulinemic-euglycemic clamp test; HGCT, hyperglycemic clamp test
48 Mechanistic investigations of glucose metabolism Oral glucose tolerance test (OGTT) Standard test to confirm normal glycemia and measure parameters of glucose absorption and insulin secretion Measures blood glucose for 3 hours after a drink of a liquid containing 75 g of glucose Two-step hyperglycemic clamp test (HCT) Quantifies insulin secretion Followed by an arginine (5 g iv) test for assessing acute, maximal insulin response Two-step hyperinsulinemic euglycemic clamp test (HECT) Measures tissue insulin sensitivity (or resistance)
49 OGTT: Pasireotide increases postprandial plasma glucose Glucose AUC min and AUC 0 180min significantly higher at day 8 than at baseline (P<0.001) in both dose groups µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 8 Mean plasma glucose (mmol/l) Time post-ogtt (min) Henry RR et al. ENDO 2011;abst P3-274
50 OGTT: Pasireotide decreases postprandial plasma insulin Insulin AUC 0 30min, AUC min and AUC 0 180min significantly lower at day 8 than at baseline (P<0.001) in both dose groups Mean plasma insulin (pmol/l) Time post-ogtt (min) 600 µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 8 Henry RR et al. ENDO 2011;abst P3-274
51 OGTT: Pasireotide decreases postprandial plasma glucagon Glucagon AUC 0 30min, AUC min and AUC 0 180min significantly lower at day 8 than at baseline (P 0.01) in both dose groups µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 8 Mean plasma glucagon (pmol/l) Time post-ogtt (min) Henry RR et al. ENDO 2011;abst P3-274
52 OGTT: Pasireotide decreases postprandial GLP-1 and GIP Mean plasma GLP-1 (pmol/l) µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day Time post-ogtt (min) GLP-1 AUC 0 30min and AUC 0 180min significantly lower at day 8 than at baseline in the 600 µg group AUC 0 30min, AUC min and AUC 0 180min significantly lower at day 8 than at baseline in the 900 µg group Mean plasma GIP (pmol/l) µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 8 GIP AUC 0 30min, AUC min and AUC 0 180min significantly lower at day 8 than at baseline in both dose groups Time post-ogtt (min) Henry RR et al. ENDO 2011;abst P3-274 GIP, glucose-dependent insulinotropic polypeptide; GLP-1, glucagon-like peptide-1
53 HCT: Pasireotide decreases plasma insulin with minimal changes in plasma glucagon Mean plasma insulin (nmol/l) µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 9 Insulin Decreases in AUC 0 10min, AUC min and AUC 0 180min between baseline and day 9 were significant in both dose groups (P<0.001) Time post-hct (min) Mean plasma glucagon (pmol/l) µg bid, baseline 600 µg bid, day µg bid, baseline 900 µg bid, day 9 Glucagon Minimal effect of pasireotide on glucagon secretion Time post-hct (min) Henry RR et al. ENDO 2011;abst P3-274
54 HECT: Pasireotide does not affect insulin sensitivity Mean glucose disposal rate (mg/kg/min) 5 0 Baseline Day 10 Baseline Day mu/m 2 /min 120 mu/m 2 /min Pasireotide 600 µg bid Pasireotide 900 µg bid The mechanisms of hyperglycemia associated with pasireotide 15 are related to: Decreases in insulin secretion, as observed following OGTT and HCT 10 Significantly decreased incretin response, as observed following OGTT and HGCT Pasireotide does not affect insulin sensitivity Henry RR et al. ENDO 2011;abst P3-274
55 SOM230B2124: Study design Management of hyperglycemia Pasireotide 600 µg sc bid alone (n=18) Healthy male volunteers (n=90) Baseline Randomization 1:1:1:1:1 Start of treatment period (day 1) + metformin500 mg IR pobid (n=18) + nateglinide 60 mg po tid (n=18) + vildagliptin 50 mg po bid (n=18) End of treatment period (day 7) Safety follow-up (day 21) Safety follow-up (day 35) + liraglutide 0.6 mg sc qd (n=18) OGTT on day 1, prior to drug administration OGTT on day 1, after drug administration OGTT on day 7, after last drug administration Henry RR et al. ENDO 2011;abst P3-274
56 Changes in glucose levels during OGTT 16 All baseline All after 1 st pasireotide dose After 7 days of pasireotide alone After 7 days of pasireotide + metformin (biguanide) After 7 days of pasireotide + nateglinide (insulin secretagogue) After 7 days of pasireotide + vildagliptin (DPP-4 inhibitor) After 7 days of pasireotide + liraglutide (GLP-1 agonist) 14 Mean plasma glucose (mmol/l) Henry RR et al. ENDO 2011;abst P Time (min) DPP-4, dipeptidyl peptidase-4; GLP-1, glucagon-like peptide-1
57 AUC 0 4h of plasma glucose Plasma glucose decreased after 7 days of treatment, compared with pasireotide alone: 29% with liraglutide (geometric mean ratio 0.71; 90% CI 0.66, 0.76) 15% with vildagliptin (geometric mean ratio 0.85; 90% CI 0.79, 0.91) 10% with nateglinide (geometric mean ratio 0.90; 90% CI 0.83, 0.96) 2% with metformin (geometric mean ratio 0.98; 90% CI 0.91, 1.05) Henry RR et al. ENDO 2011;abst P3-274
58 Changes in insulin levels during OGTT 500 All baseline All after 1 st pasireotide dose After 7 days of pasireotide alone After 7 days of pasireotide + metformin After 7 days of pasireotide + nateglinide After 7 days of pasireotide + vildagliptin After 7 days of pasireotide + liraglutide 400 Mean plasma insulin (pmol/l) Henry RR et al. ENDO 2011;abst P Time (min)
59 AUC 0 4h of serum insulin Serum insulin increases after 7 days of treatment, compared with pasireotide alone: 71% with vildagliptin (geometric mean ratio 1.71; 90% CI 1.33, 2.19) GLP-1 agonists and DPP-4 inhibitors appear to be the most effective 34% with drugs liraglutide for ameliorating hyperglycemia associated with pasireotide treatment (geometric mean ratio 1.34; 90% CI 1.03, 1.73) 6% with metformin (geometric mean ratio 1.06; 90% CI 0.82, 1.36) 3% with nateglinide (geometric mean ratio 1.03; 90% CI 0.80, 1.32) Henry RR et al. ENDO 2011;abst P3-274
60 Changes in glucagon levels during OGTT All baseline All after 1 st pasireotide dose After 7 days of pasireotide alone After 7 days of pasireotide + metformin After 7 days of pasireotide + nateglinide After 7 days of pasireotide + vildagliptin After 7 days of pasireotide + liraglutide Mean plasma glucagon (pmol/l) Henry RR et al. ENDO 2011;abst P Time (h)
61 SOM230B2124: Safety/tolerability Adverse events occurring more frequently than with pasireotide alone Liraglutide Nateglinide Metfomin Vildagliptin Decreased appetite (38.9%) Nausea (72.2%) Nausea (83.3%) Diarrhea (77.8%) Abdominal pain (72.2%) Vomiting (27.8%) Dizziness (50.0%) Injection site pain (22.2%) Fatigue (22.2%) Headache (27.8%) Cholestasis SAE (5.6%) Fatigue (33.3%) Hypoglycemia (66.7%) Nausea (61.1%) Abdominal pain (44.4%) Decreased appetite (27.8%) Abdominal distension (22.2%) Overall, AEs were consistent with the safety profile of pasireotide and the antidiabetic drugs used Henry RR et al. ENDO 2011;abst P3-274
62 Summary: Pasireotide safety profile Safety of pasireotide was similar to that of other somatostatin analogues, except for the degree of hyperglycemia Most frequently reported AEs were gastrointestinal 11.7% of patients had 1 serious AE suspected to be study drug related As expected with an effective treatment for Cushing s disease, some patients (8%) experienced hypocortisolism Responded to dose reduction and/or temporary corticosteroid substitution 72.8% of patients had at least one hyperglycemia-related AE 6% of patients discontinued treatment because of a hyperglycemiarelated AE during the core study No new safety issues were identified up to the 24-month data cut-off No deaths were reported during the entire study Colao A et al. N Engl J Med 2012;366:
63 Summary: Mechanism and management of hyperglycemia The mechanisms of hyperglycemia seen with pasireotide sc at doses of 600 and 900 μg bid are related to: Decreases in insulin secretion, as observed following OGTT and HGCT Significantly decreased incretin response, as observed following OGTT and HGCT Pasireotide does not affect insulin sensitivity GLP-1 agonists and DPP-4 inhibitors appear to be the most effective drugs for ameliorating hyperglycemia associated with pasireotide treatment Despite a lack of efficacy in healthy volunteers, metformin may provide clinical benefit in patients with Cushing s disease who often present with underlying insulin resistance and β-cell dysfunction Hyperglycemia during treatment with pasireotide may be effectively managed by early intervention and regular (self-) monitoring of blood glucose levels Henry RR et al. ENDO 2011;abst P3-274
64 Hyperglycemia Key Message Flow to Address Customer Information Need Physicians Questions Who is more likely to develop hyperglycemia? Key Messages Patients with prediabetes and diabetes mellitus at baseline had a greater risk for increased glucose and HbA 1c levels When is it likely to occur? Why does it happen? What steps do I need to take to manage it? *Following current treatment guidelines Hyperglycemia may appear shortly after treatment initiation Pasireotide reduces insulin secretion without affecting insulin sensitivity Correct management of hyperglycemia should include:* Regular monitoring of blood glucose levels Proactive approach of an antidiabetic treatment initiation or adjustment Primary medical therapy might include* DPP-IV inhibitors (eg, vildagliptin) GLP-1 agonists (eg, liraglutide) Insulin secretagogues (eg, nateglinide) secondary option
65 Combination Therapy 17 patients Ketoconazole 200 mg TID Feelders et al. N Engl J Med. 2010;362: Stepwise Medical Treatment Pasireotide 250 µg TID Pasireotide 100 µg TID 0 Cabergoline 1.5 mg QOD Time, d Stepwise Medical Treatment B2402 STUDY 80
66 Combination Therapy Disease control with pasireotide alone or in combination in 88% of patients with Cushing s disease Feelders et al. N Engl J Med. 2010;362:
67 Future?
68 SOM230G2304: Evaluating the efficacy and safety of pasireotide LAR in patients with Cushing s disease Global, multicenter, randomized, double-blind, Phase III study Target enrollment is ~148 patients; recruitment is under way Screening RANDOMIZATION Pasireotide LAR 10 mg/28 days im dose reduction for safety* LAR 30 mg/28 days im LAR 10 mg/28 days im LAR 40 mg/28 days im Primary efficacy dose titration per investigator (if 5 mg not tolerated, patient will discontinue) Pasireotide LAR 30 mg/28 days im LAR 30 mg/28 days im Month 1 Day 1 Month 4 Month 7 Month 9 Month 12 Screening Double blind Partial blind Ligueros-Saylan M et al. Endocr Abstr 2012;29:abst P *One dose level reduction permitted during the first 7 months (30 to 10 or 10 to 5 mg) im, intramuscular injection
69 CSOM230B Pasireotide in combination with cabergoline SOM 900 µg bid + Cab 1 mg qd 1,2 SOM 900 µg bid + Cab 0.5 mg qd 1,2 8 weeks SOM 900 µg bid 1, 2 8 weeks SOM 600 µg bid1, 2, 3 8 weeks 8 weeks 1. Patients not achieving normal UFC at the end of each treatment period will have the dose of the medication up-titrated to the next level 2. Patients losing biochemical control at any time point will have the dose of the study medication up-titrated to the next level 3. Patients that cannot have the dose up-titrated to 900 µg because of safety reasons, e.g. increased blood glucose levels, will be treated with the combination SOM 600 µg and cabergoline at increasing doses. Patients who cannot tolerate 600 µg bid will have the dose down-titrated to 300 µg bid
70 Thanks
Sponsor Novartis. Generic Drug Name Pasireotide. Therapeutic Area of Trial Cushing s disease. Protocol Number CSOM230B2208E1
 Sponsor Novartis Generic Drug Name Pasireotide Therapeutic Area of Trial Cushing s disease Protocol Number CSOM230B2208E1 Title Extension to a multicenter, open-label study to assess the safety and efficacy
Sponsor Novartis Generic Drug Name Pasireotide Therapeutic Area of Trial Cushing s disease Protocol Number CSOM230B2208E1 Title Extension to a multicenter, open-label study to assess the safety and efficacy
ADVANCES IN MANAGING CUSHING S DISEASE. Rosario Pivonello Department of Clinical Medicine and Surgery, Federico II University, Naples, Italy
 ADVANCES IN MANAGING CUSHING S DISEASE Rosario Pivonello Department of Clinical Medicine and Surgery, Federico II University, Naples, Italy Patients with persistent Cushing s disease have higher morbidity
ADVANCES IN MANAGING CUSHING S DISEASE Rosario Pivonello Department of Clinical Medicine and Surgery, Federico II University, Naples, Italy Patients with persistent Cushing s disease have higher morbidity
Sponsor Novartis. Generic Drug Name Vildagliptin/Metformin. Therapeutic Area of Trial Type 2 diabetes. Approved Indication Type 2 diabetes
 Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY
 Case Report MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY Murray B. Gordon, MD, FACE; Kellie L. Spiller, MS ABSTRACT Submitted for publication July
Case Report MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY Murray B. Gordon, MD, FACE; Kellie L. Spiller, MS ABSTRACT Submitted for publication July
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide)
") Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Sponsor / Company: Sanofi Drug substance(s): Insulin Glargine (HOE901) Insulin Glulisine (HMR1964)
: Insulin Glargine (HOE901) Insulin Glulisine (HMR1964)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT
 I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia Sezione di Endocrinologia, Università Federico II di Napoli, Italy 1 Treatment
I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia Sezione di Endocrinologia, Università Federico II di Napoli, Italy 1 Treatment
A 12-Month Phase 3 Study of Pasireotide in Cushing s Disease
 T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article A 12- Phase 3 Study of Pasireotide in Cushing s Disease Annamaria Colao, M.D., Ph.D., Stephan Petersenn, M.D., John Newell-Price,
T h e n e w e ngl a nd j o u r na l o f m e dic i n e original article A 12- Phase 3 Study of Pasireotide in Cushing s Disease Annamaria Colao, M.D., Ph.D., Stephan Petersenn, M.D., John Newell-Price,
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Supplementary Online Content
 Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease
 Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease Information Reader Box (IRB) to be inserted on inside front cover for documents
Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease Information Reader Box (IRB) to be inserted on inside front cover for documents
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Treating Type 2 Diabetes with Bariatric Surgery. Goal of Treating T2DM. Remission of T2DM with Bariatric
 Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
23-Aug-2011 Lixisenatide (AVE0010) - EFC6014 Version number: 1 (electronic 1.0)
 - EFC6014 Version number: 1 (electronic 1.0)") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top of metformin
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top of metformin
Prospective, Open Label, Phase 3 Study of Levoketoconazole in Cushing Syndrome (SONICS): Primary Safety and Efficacy Results
: Primary Safety and Efficacy Results") Prospective, Open Label, Phase 3 Study of Levoketoconazole in Cushing Syndrome (SONICS): Primary Safety and Efficacy Results Eliza B. Geer Maria Fleseriu, 1 Rosario Pivonello, 2 Atanaska Elenkova, 3 Roberto
Prospective, Open Label, Phase 3 Study of Levoketoconazole in Cushing Syndrome (SONICS): Primary Safety and Efficacy Results Eliza B. Geer Maria Fleseriu, 1 Rosario Pivonello, 2 Atanaska Elenkova, 3 Roberto
Managing Acromegaly: Review of Two Cases
 Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Long-term treatment of Cushing s disease with pasireotide: 5-year results from an open-label extension study of a Phase III trial
 Endocrine (2017) 57:156 165 DOI 10.1007/s12020-017-1316-3 ORIGINAL ARTICLE Long-term treatment of Cushing s disease with pasireotide: 5-year results from an open-label extension study of a Phase III trial
Endocrine (2017) 57:156 165 DOI 10.1007/s12020-017-1316-3 ORIGINAL ARTICLE Long-term treatment of Cushing s disease with pasireotide: 5-year results from an open-label extension study of a Phase III trial
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line
 for acromegaly first and second line") Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
SYNOPSIS. Administration: subcutaneous injection Batch number(s):
:") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, 2-arm parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, 2-arm parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top
Galvus the most comprehensively studied DPP-4 inhibitor
 Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
SYNOPSIS 2/198 CSR_BDY-EFC5825-EN-E02. Name of company: TABULAR FORMAT (For National Authority Use only)
") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, fixed-dose (rimonabant 20 mg) multicenter study of long-term glycemic control with rimonabant in treatment-naïve
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, fixed-dose (rimonabant 20 mg) multicenter study of long-term glycemic control with rimonabant in treatment-naïve
EFFECTIVE MEDICAL THERAPY FOR CUSHING DISEASE CAN INCREASE THE SUSCEPTIBILITY TO RELATIVE HYPOCORTISOLISM
 Case Report EFFECTIVE MEDICAL THERAPY FOR CUSHING DISEASE CAN INCREASE THE SUSCEPTIBILITY TO RELATIVE HYPOCORTISOLISM Kevin C.J. Yuen, MD, FRCP (UK), FACE; Jennifer U. Mercado, ARNP; Kelley Moloney, ARNP;
Case Report EFFECTIVE MEDICAL THERAPY FOR CUSHING DISEASE CAN INCREASE THE SUSCEPTIBILITY TO RELATIVE HYPOCORTISOLISM Kevin C.J. Yuen, MD, FRCP (UK), FACE; Jennifer U. Mercado, ARNP; Kelley Moloney, ARNP;
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Signifor 0.3 mg solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One ampoule of 1 ml contains 0.3 mg pasireotide
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Signifor 0.3 mg solution for injection 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One ampoule of 1 ml contains 0.3 mg pasireotide
To cite this version: HAL Id: inserm
 Pasireotide can induce sustained decreases in urinary cortisol and provide clinical benefit in patients with Cushing s disease: results from an open-ended, open-label extension trial Jochen Schopohl, Feng
Pasireotide can induce sustained decreases in urinary cortisol and provide clinical benefit in patients with Cushing s disease: results from an open-ended, open-label extension trial Jochen Schopohl, Feng
AECOM, Bronx, NY; 2 Incyte Corporation, Wilmington, DE; 3 dgd Research, San Antonio, TX; 4 Profil Institute, San Diego, CA
 INCB013739, a Selective Inhibitor of 11β-Hydroxysteroid Dehydrogenase Type 1 (11βHSD1), Improves Insulin Sensitivity and Lowers Plasma Cholesterol Over 28 Days in Patients with Type 2 Diabetes Mellitus
INCB013739, a Selective Inhibitor of 11β-Hydroxysteroid Dehydrogenase Type 1 (11βHSD1), Improves Insulin Sensitivity and Lowers Plasma Cholesterol Over 28 Days in Patients with Type 2 Diabetes Mellitus
Clinical Trial Synopsis TL-OPI-525, NCT#
 Clinical Trial Synopsis, NCT#00762736 Title of Study: A Phase II, Double-Blind, Randomized, Placebo-Controlled, Proof-of-Concept Study of the Efficacy, Safety, and Tolerability of Pioglitazone HCl (ACTOS
Clinical Trial Synopsis, NCT#00762736 Title of Study: A Phase II, Double-Blind, Randomized, Placebo-Controlled, Proof-of-Concept Study of the Efficacy, Safety, and Tolerability of Pioglitazone HCl (ACTOS
Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes
 Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
Adv Ther (2013) 30(2):81 101. DOI 10.1007/s12325-013-0009-4 REVIEW Mechanisms and Clinical Efficacy of Lixisenatide for the Management of Type 2 Diabetes Michael Horowitz Christopher K. Rayner Karen L.
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Role of incretins in the treatment of type 2 diabetes
 Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
Role of incretins in the treatment of type 2 diabetes Jens Juul Holst Department of Medical Physiology Panum Institute University of Copenhagen Denmark Diabetes & Obesity Spanish Society of Internal Medicine
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Discussion & Conclusion
 Discussion & Conclusion 7. Discussion DPP-4 inhibitors augment the effects of incretin hormones by prolonging their half-life and represent a new therapeutic approach for the treatment of type 2 diabetes
Discussion & Conclusion 7. Discussion DPP-4 inhibitors augment the effects of incretin hormones by prolonging their half-life and represent a new therapeutic approach for the treatment of type 2 diabetes
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
SYNOPSIS OF RESEARCH REPORT (PROTOCOL BC20779)
") TITLE OF THE STUDY / REPORT No. / DATE OF REPORT INVESTIGATORS / CENTERS AND COUNTRIES Clinical Study Report Protocol BC20779: Multicenter, double-blind, randomized, placebo-controlled, dose ranging phase
TITLE OF THE STUDY / REPORT No. / DATE OF REPORT INVESTIGATORS / CENTERS AND COUNTRIES Clinical Study Report Protocol BC20779: Multicenter, double-blind, randomized, placebo-controlled, dose ranging phase
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function
 Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
Effect of macronutrients and mixed meals on incretin hormone secretion and islet cell function Background. Following meal ingestion, several hormones are released from the gastrointestinal tract. Some
Le incretine: un passo avanti. Francesco Dotta
 Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
SELECTED ABSTRACTS AND POSTER PRESENTATIONS
 SELECTED ABSTRACTS AND POSTER PRESENTATIONS The following summaries are based on abstracts and posters presented at the American Diabetes Association s 65th Annual Scientific Sessions held in San Diego,
SELECTED ABSTRACTS AND POSTER PRESENTATIONS The following summaries are based on abstracts and posters presented at the American Diabetes Association s 65th Annual Scientific Sessions held in San Diego,
The enteroinsular axis in the pathogenesis of prediabetes and diabetes in humans
 The enteroinsular axis in the pathogenesis of prediabetes and diabetes in humans Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Seoul National University College of Medicine Plasma glucose
The enteroinsular axis in the pathogenesis of prediabetes and diabetes in humans Young Min Cho, MD, PhD Division of Endocrinology and Metabolism Seoul National University College of Medicine Plasma glucose
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Signifor 0.3 mg solution for injection Signifor 0.6 mg solution for injection Signifor 0.9 mg solution for injection 2. QUALITATIVE
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Signifor 0.3 mg solution for injection Signifor 0.6 mg solution for injection Signifor 0.9 mg solution for injection 2. QUALITATIVE
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Study Code: Date: 27 July 2007
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Int. J. Pharm. Sci. Rev. Res., 22(2), Sep Oct 2013; nᵒ 21,
, Sep Oct 2013; nᵒ 21,") Research Article A Comparative Study to Evaluate the Efficacy and Safety of Vildagliptin as an Add-on Therapy to a Low-Dose Metformin vs an Uptitration of Metformin in Type 2 DM Patients Basavaraj Bhandare*
Research Article A Comparative Study to Evaluate the Efficacy and Safety of Vildagliptin as an Add-on Therapy to a Low-Dose Metformin vs an Uptitration of Metformin in Type 2 DM Patients Basavaraj Bhandare*
Data from an epidemiologic analysis of
 CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
CLINICAL TRIAL RESULTS OF GLP-1 RELATED AGENTS: THE EARLY EVIDENCE Lawrence Blonde, MD, FACP, FACE ABSTRACT Although it is well known that lowering A 1c (also known as glycated hemoglobin) is associated
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Scope. History. History. Incretins. Incretin-based Therapy and DPP-4 Inhibitors
 Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Plasma Glucose (mg/dl) Plasma Insulin (pmol/l) Incretin-based Therapy and Inhibitors Scope Mechanism of action ผศ.ดร.นพ.ว ระเดช พ ศประเสร ฐ สาขาว ชาโภชนว ทยาคล น ก ภาคว ชาอาย รศาสตร คณะแพทยศาสตร มหาว ทยาล
Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors. Richard E. Pratley and Matthew Gilbert
 REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
REVIEW Targeting Incretins in Type 2 Diabetes: Role of GLP-1 Receptor Agonists and DPP-4 Inhibitors Richard E. Pratley and Matthew Gilbert Diabetes and Metabolism Translational Medicine Unit, University
Efficacy/pharmacodynamics: 85 Safety: 89
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor/Company: Sanofi Drug substance:
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor/Company: Sanofi Drug substance:
To assess the safety and tolerability in each treatment group.
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Case Report Monitoring Patient Improvement Parameters following Pasireotide Treatment in Cushing s Disease
 Case Reports in Endocrinology Volume 2013, Article ID 735489, 5 pages http://dx.doi.org/10.1155/2013/735489 Case Report Monitoring Patient Improvement Parameters following Pasireotide Treatment in Cushing
Case Reports in Endocrinology Volume 2013, Article ID 735489, 5 pages http://dx.doi.org/10.1155/2013/735489 Case Report Monitoring Patient Improvement Parameters following Pasireotide Treatment in Cushing
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
New York State Medicaid Prescriber Education Program
 New York State Medicaid Prescriber Education Program Metformin as a first-line medication Treating type 2 diabetes mellitus Key messages 1) Metformin should be used as a first-line medication in almost
New York State Medicaid Prescriber Education Program Metformin as a first-line medication Treating type 2 diabetes mellitus Key messages 1) Metformin should be used as a first-line medication in almost
Drug Class Monograph
 Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
PROCEEDINGS CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES * Vivian A. Fonseca, MD, FRCP ABSTRACT
 CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
CLINICAL RESEARCH AND EXPERIENCE WITH INCRETIN-BASED THERAPIES Vivian A. Fonseca, MD, FRCP ABSTRACT Despite proven lifestyle recommendations and the availability of a range of oral antidiabetic agents,
In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo Shin Choi 2, and Seung Eun Lee 2. Departments of Surgery, Dongguk University College of Medicine 2
 Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Clinical Trial Synopsis TL-OPI-518, NCT#
 Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016
 Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016 Scholar: Review the literature in an evidenced based manner to determine the difference in our clinical setting. Advocate: Develop a better
Ahmed Al Nahari Pediatric Endocrinology Fellow March 11,2016 Scholar: Review the literature in an evidenced based manner to determine the difference in our clinical setting. Advocate: Develop a better
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Xultophy 100/3.6. (insulin degludec, liraglutide) New Product Slideshow
 New Product Slideshow") Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
PRODUCT MONOGRAPH SIGNIFOR LAR. Pasireotide for Injectable Suspension
 PRODUCT MONOGRAPH Pr SIGNIFOR LAR Pasireotide for Injectable Suspension 10 mg, 20 mg, 30 mg, 40 mg, and 60 mg pasireotide (as pasireotide pamoate) per vial SOMATOSTATIN AND ANALOGUES Novartis Pharmaceuticals
PRODUCT MONOGRAPH Pr SIGNIFOR LAR Pasireotide for Injectable Suspension 10 mg, 20 mg, 30 mg, 40 mg, and 60 mg pasireotide (as pasireotide pamoate) per vial SOMATOSTATIN AND ANALOGUES Novartis Pharmaceuticals
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Sponsor Novartis. Generic Drug Name. Valsartan and amlodipine Trial Indication(s) Hypertension Protocol Number CVAA489A2306 Protocol Title
 Hypertension Protocol Number CVAA489A2306 Protocol Title") Sponsor Novartis Generic Drug Name Valsartan and amlodipine Trial Indication(s) Hypertension Protocol Number CVAA489A2306 Protocol Title A randomized, double-blind, multi-center, active-controlled, parallel
Sponsor Novartis Generic Drug Name Valsartan and amlodipine Trial Indication(s) Hypertension Protocol Number CVAA489A2306 Protocol Title A randomized, double-blind, multi-center, active-controlled, parallel
These results are supplied for informational purposes only.
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption),
,") Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
A randomised controlled clinical trial in type 2 diabetes comparing semaglutide to placebo and liraglutide
 A randomised controlled clinical trial in type 2 diabetes comparing semaglutide to placebo and liraglutide This trial was conducted in Europe,Asia and Africa. Study participants were randomised evenly
A randomised controlled clinical trial in type 2 diabetes comparing semaglutide to placebo and liraglutide This trial was conducted in Europe,Asia and Africa. Study participants were randomised evenly
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
SYNOPSIS. Number of subjects: Planned: 22 Randomized: 23 Treated: 23. Evaluated: Pharmacodynamic: 22 Safety: 23 Pharmacokinetics: 22
 SYNOPSIS Title of the study: A randomized, cross-over, open, euglycemic clamp study on the relative bioavailability and activity of 0.6 U/kg insulin glargine and 20 µg lixisenatide, given as on-site mix
SYNOPSIS Title of the study: A randomized, cross-over, open, euglycemic clamp study on the relative bioavailability and activity of 0.6 U/kg insulin glargine and 20 µg lixisenatide, given as on-site mix
Pharmacotherapy IV: Liraglutide for Chronic Weight Management SARAH CAWSEY MD, FRCPC 2 ND ANNUAL OBESITY UPDATE SEPTEMBER 22, 2018
 Pharmacotherapy IV: Liraglutide for Chronic Weight Management SARAH CAWSEY MD, FRCPC 2 ND ANNUAL OBESITY UPDATE SEPTEMBER 22, 2018 Disclosures Faculty Assistant Clinical Professor, Department of Medicine,
Pharmacotherapy IV: Liraglutide for Chronic Weight Management SARAH CAWSEY MD, FRCPC 2 ND ANNUAL OBESITY UPDATE SEPTEMBER 22, 2018 Disclosures Faculty Assistant Clinical Professor, Department of Medicine,
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist