PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI. Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
|
|
|
- Mildred Reed
- 5 years ago
- Views:
Transcription



1 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
2 Disclosure Dr Massimo Boemi has been granted as speaker by: Eli Lilly, Novo-Nordisk, Sanofi, Boehringer-Ingelheim, Jannsen, MSD, Astra Zeneca, Novartis, Sigma-Tau Dr Massimo Boemi has been granted as partecipant in boards/consultant by: Eli Lilly, Novo-Nordisk, Boehringer-Ingelheim, Jannsen, Astra Zeneca Dr Massimo Boemi Unit received financial support/sponsorship by: Eli-Lilly, Sigma-Tau
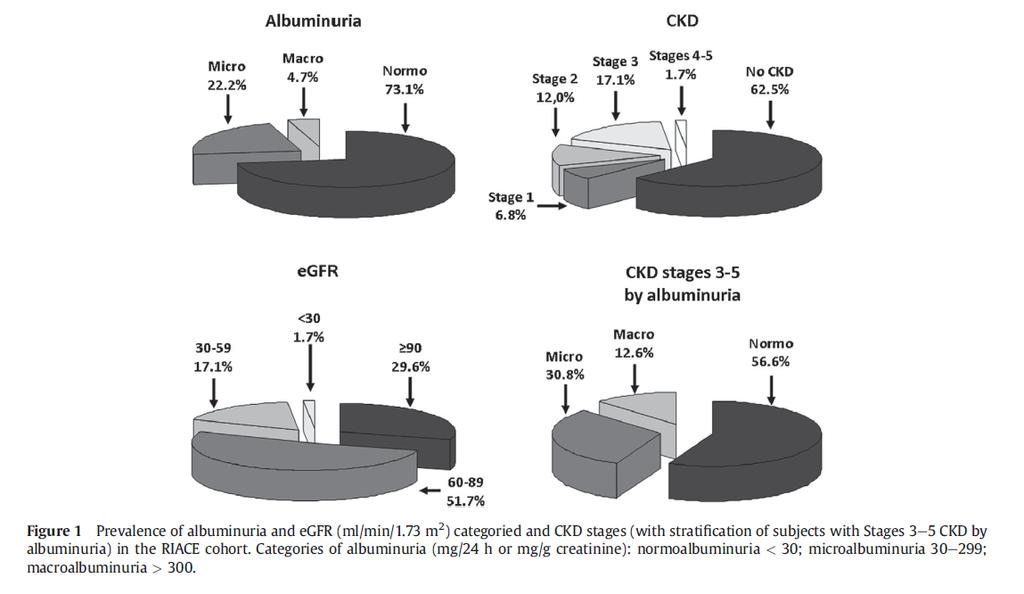
3 Renal dysfunction is common in patients with T2DM The RIACE Study: 15,773 patients with T2DM 17.1% 1.7% No CKD CKD stage 1 CKD stage 2 CKD stage 3 CKD stages 4/5 12.0% 6.7% 62.5% Approximately 40% of patients with T2DM show signs of CKD (stages 1-5) Approximately 20% of patients with T2DM show signs of renal failure (egfr <60 ml/min/1.73 m 2 ) Penno G et al. J Hypertens 29: , 2011
4 Renal dysfunction is common in patients with T2DM The RIACE Study: 15,773 patients with T2DM Albuminuria Normal Mild (micro) Severe (macro) egfr ml/min/ 1.73 m 2 MDRD > Stage 0 (no CKD) 62.5% Stage 3/5 NON albuminuric CKD phenotype 10.6% Stage albuminuric phenotype Stage 2 Stages 3/5 Stage albuminuric 3 CKD phenotype Stage % 8.2% Penno G et al. J Hypertens 29: , 2011
 Patel A et al.")
5 HbA 1 c Media (%) Standard Intensivo Δ 0.67% (95% CI ); p< Follow-up (Mesi) Patel A et al., N Engl J Med 2008; 358(24):
6
7 Methods: microvascular and renal outcomes Composite microvascular outcomes (secondary outcomes): initiation of retinal photocoagulation, vitreous hemorrhage, diabetes-related blindness, incident or worsening nephropathy* *incident or worsening nephropathy was defined as: Progression to macroalbuminuria (UACR >300 mg/g) or Doubling of serum creatinine accompanied by egfr (MDRD) 45 ml/min/1.73m 2 or Initiation of renal replacement therapy or Death due to renal disease Prespecified Renal Endpoints in the statistical analysis plan - Incident or worsening nephropathy (individual components); - Incident or worsening nephropathy or CV death (composite) - doubling of serum creatinine, initiation of renal replacement therapy, or death due to renal disease (composite) - incident albuminuria (UACR 30 mg/g) in patients with normoalbuminuria at baseline - egfr (CKD-EPI) over time UACR, urine albumin-to-creatinine ratio; egfr, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration. Christoph Wanner et al. published online June 14, 2016, at NEJM.org 7
8
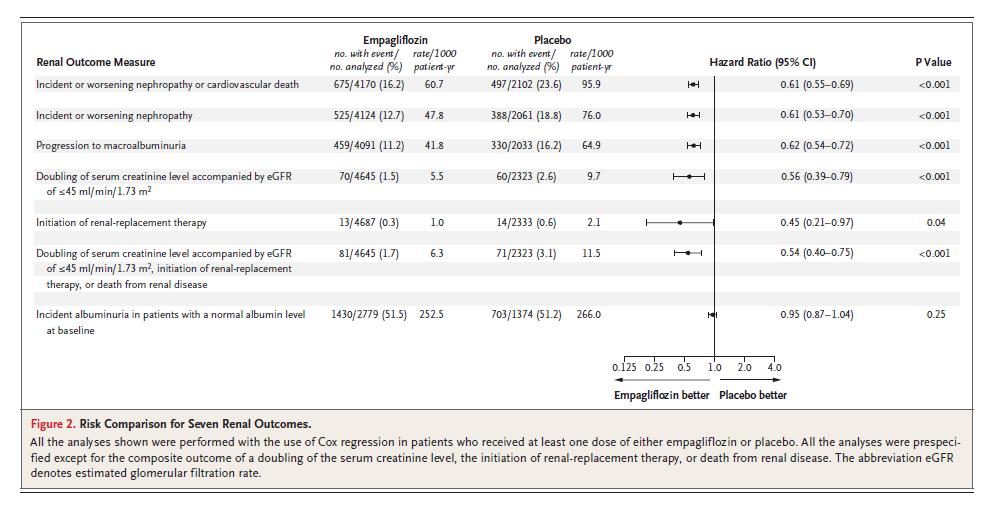
9 Incident or worsening nephropathy Doubling of serum creatinine, initiation of renal replacement therapy, or death due to renal disease
10
11
12 Adjusted mean change from baseline in UACR (% [95% C1]) Post-hoc analysis of data from a randomised, placebocontrolled, double blinded Phase 3 trial in patients with T2DM, CK3D and albuminuria 104 weeks in duration Patients received dapagliflozin 5 mg (n=53) or 10 mg (n=56) or placebo (n=57) 120 Placebo DAPA 5 mg DAPA 10 mg 80 Week 104 UACR ( 19.0, 111.9) 26.4 ( 55.0, 20.5) 43.9 ( 64.3, 12.0) Number of Patients per Time Point Placebo DAPA 5 mg DAPA 10 mg Baseline UACR mg/g mg/g mg/g
13 Difference vs placebo (% [95% CI]) The UACR reduction by dapagliflozin is independent of changes in blood pressure, HbA 1C and egfr 1 20 Placebo-corrected percentage change in albuminuria adjusted for changes in HbA 1C, SBP, DBP and egfr DAPA 5 mg (n = 20) DAPA 10 mg(n = 29) NOT including covariates for ΔHbA1c, ΔSBP, ΔDBP and ΔeGFR Including covariates for ΔHbA1c, ΔSBP, ΔDBP and ΔeGFR The UACR reduction remains after adjustments for changes in blood pressure, HbA1c and egfr indicating direct renal effect independent of changes in these variables 1
14
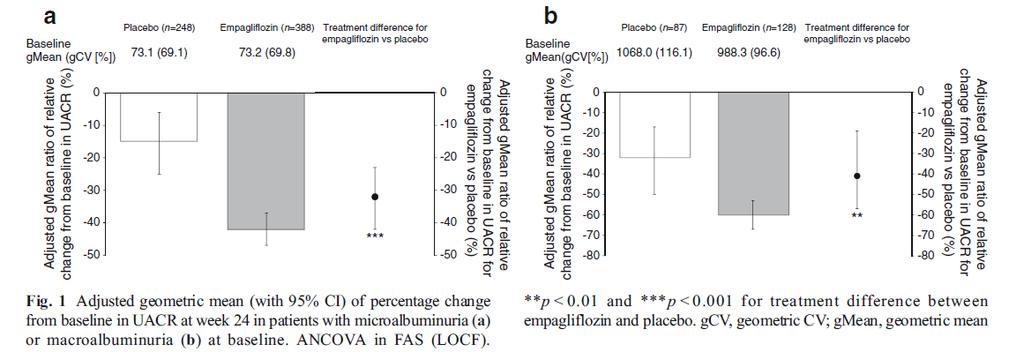
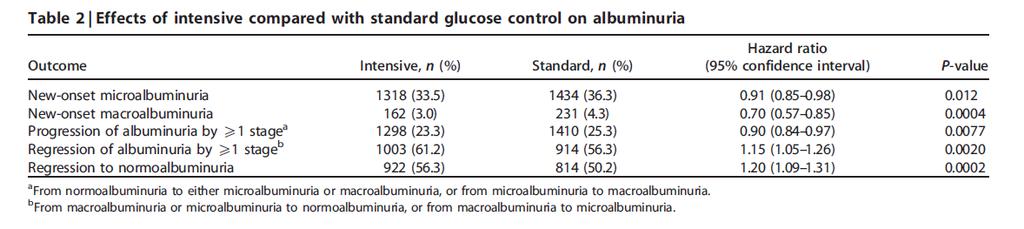
15 MICRO MACRO
16
17
18 9340 patients Double blinded 2-week placebo run-in Placebo run-in Liraglutide mg OD + standard of care Placebo + standard of care Safety follow-up Safety follow-up 2 weeks Duration years 30 days Screening Randomisation (1:1) End of treatment Key inclusion criteria T2DM, HbA 1c 7.0% Antidiabetic drug naïve; OADs and/or basal/premix insulin Age 50 years and established CV disease or chronic renal failure or Age 60 years and risk factors for CV disease Key exclusion criteria T1DM Use of GLP-1RAs, DPP-4i, pramlintide, or rapid-acting insulin Familial or personal history of MEN-2 or MTC
19 Baseline renal function Liraglutide (N=4668) Placebo (N=4672) Normal renal function (egfr 90 ml/min/1.73 m 2 ) 1620 (34.7) 1655 (35.4) Mild impairment (egfr ml/min/1.73 m 2 ) 1932 (41.4) 1975 (42.3) Moderate impairment (egfr ml/min/1.73 m 2 ) 999 (21.4) 935 (20.0) Severe impairment (egfr <30 ml/min/1.73 m 2 ) 117 (2.5) 107 (2.3) Liraglutide Placebo Microalbuminuria 26.4% 26.6% Macroalbuminuria 10.0% 11.0% egfr <60 ml/min/1.73 m % 22.3% Full analysis set. Data are number of patients (percentage of either liraglutide-treated or placebo-treated group). Percentage data refer to proportion of patients egfr, estimated glomerular filtration rate. Marso SP et al. N Engl J Med DOI: /NEJMoa
20 HbA 1c (%) HbA 1c (mmol/mol) HbA 1c P la c e b o L ir a g lu t id e ETD at month 36: -0.40% 95% CI (-0.45 ; -0.34) E O T Time from randomisation (months) Number of patients at each visit Liraglutide Placebo Data are estimated mean values from randomisation to EOT. CI, confidence interval; EOT, end of trial; ETD, estimated treatment difference; HbA 1c, glycosylated haemoglobin. Marso SP et al. N Engl J Med DOI: /NEJMoa

21 Presentation title Date 21

22 Microvascular event definitions *and egfr 45 ml/min/1.73 m 2 per MDRD egfr: estimated glomerular filtration rate; MDRD, modification of diet in renal disease. Presented at 52 nd EASD Annual Meeting, 14 September 2016, Munich, Germany
23 Patients with an event (%) LEADER: Time to first renal event Macroalbuminuria, doubling of serum creatinine*, ESRD, renal death Placebo -22% Liraglutide HR: % CI (0.67 ; 0.92) p= Patients at risk Liraglutide Placebo Time since randomisation (months) *and egfr 45 ml/min/1.73 m 2 per MDRD. The cumulative incidences were estimated with the use of the Kaplan Meier method, and the HRs with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months because less than 10% of the patients had an observation time beyond 54 months CI: confidence interval; ESRD: end-stage renal disease; HR: hazard ratio Presented at 52 nd EASD Annual Meeting, 14 September 2016, Munich, Germany
24 Patients with an event (%) LEADER: Time to new onset of persistent macroalbuminuria 6 Placebo 4-26% Liraglutide 2 HR: % CI (0.60 ; 0.91) p= Patients at risk Time since randomisation (months) Liraglutide Placebo Full analysis set. EAC-confirmed index events from randomisation to follow-up. The cumulative incidences were estimated with the use of the Kaplan Meier method, and the HRs with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months because less than 10% of the patients had an observation time beyond 54 months. Macroalbuminuria was defined as urine albumin >300 mg/g creatinine CI, confidence interval; EAC, event adjudication committee; HR, hazard ratio Presented at ASN Kidney Week, 19 November 2016, Chicago, USA
25 LEADER: Time to first microvascular endpoints Hazard ratio (95% CI) Liraglutide Placebo N % N % Number of patients Microvascular endpoint 0.84 (0.73 ; 0.97) Nephropathy 0.78 (0.67 ; 0.92) New onset of persistent macroalbuminuria* 0.74 (0.60 ; 0.91) Persistent doubling of serum creatinine 0.89 (0.67 ; 1.19) Need for continuous renal replacement therapy 0.87 (0.61 ; 1.24) Death due to renal disease 1.59 (0.52 ; 4.87) Hazard ratio (95% CI) Favours liraglutide Favours placebo Full analysis set. EAC-confirmed microvascular events, including events with onset between date of randomisation and date of follow-up. Cox proportional-hazard model adjusted for treatment. Development of diabetes-related blindness was not analysed as an individual component as only one event was observed *New onset of persistent macroalbuminuria: urine albumin 300 mg/g creatinine. Persistent doubling of serum creatinine level and egfr 45 ml/min/1.73m 2 per MDRD CI, confidence interval; EAC, event adjudication committee; egfr, estimated glomerular filtration rate; MDRD, modification of diet in renal disease Presented at ASN Kidney Week, 19 November 2016, Chicago, USA
26 LEADER: Urinary albumin creatinine ratio at 3 years Estimated treatment ratio (95% CI) Total 0.81 (0.76 ; 0.86) Without renal impairment (egfr-mdrd 90) Mild renal impairment (egfr-mdrd 60 to <90) Moderate renal impairment (egfr-mdrd 30 to <60) Severe renal impairment (egfr-mdrd <30) 0.78 (0.70 ; 0.87) 0.80 (0.73 ; 0.89) 0.82 (0.72 ; 0.95) 0.83 (0.55 ; 1.26) Estimated treatment ratio (95% CI) Favours Liraglutide Favours Placebo CI: confidence interval; egfr: estimated glomerular filtration rate; MDRD, modification of diet in renal disease Presented at 52 nd EASD Annual Meeting, 14 September 2016, Munich, Germany.
27 egfr (ml/min/1.73 m 2 ) LEADER: Change in egfr (MDRD) Liraglutide Placebo 1,5 1,3 1,0 0,8 Ratio to baseline at Month 36 ETR: % CI (1.00 ; 1.03) p= ,5 0,3 0,89 0, ,0 Liraglutide Placebo Time since randomisation (months) Number of patients at each visit Liraglutide Placebo Full analysis set. Estimated means ± standard error. Change from baseline to last assessment analysed using a linear mixed model for log-transformed assessment accounting for repeated measures. Analyses truncated at 48 months as <10% of patients had an observation time beyond 48 months. CI, confidence interval; egfr, estimated glomerular filtration rate; ETR, estimated treatment ratio; MDRD, modification of diet in renal disease Presented at ASN Kidney Week, 19 November 2016, Chicago, USA
28
29 Randomisation (1:1:1:1) 3297 subjects with T2D Semaglutide 1.0 mg Semaglutide 0.5 mg Placebo 1.0 mg Placebo 0.5 mg Trial information Randomised, double-blind, placebo-controlled, four-armed parallel-group trial Additional glucose-lowering medication could be added to achieve glycaemic control at the discretion of investigator Dose escalation * 4 8 weeks Treatment maintenance weeks Treatment duration 104 weeks Follow-up 5 weeks Inclusion criteria HbA 1c 7.0% Previously on 0 2 OADs, basal or pre-mix insulin ± 0 2 OADs Age 50 years with established CVD (prior cardio-, cerebro- or peripheral vascular disease, chronic heart failure [NYHA class II III]), or CKD stage 3 or worse or Age 60 years with at least one cardiovascular risk factor Key endpoints Primary: time to first occurrence of death from cardiovascular causes, non-fatal myocardial infarction or non-fatal stroke Secondary: time to first occurrence of revascularisation, unstable angina requiring hospitalisation, hospitalisation for heart failure, all-cause death, non-fatal MI or non-fatal stroke; time to each individual component
30 Baseline characteristics Semaglutide 0.5 mg Semaglutide 1.0 mg Placebo 0.5 mg Placebo 1.0 mg (n=826) (n=822) (n=824) (n=825) (N=3297) Age (years) 64.6 (7.3) 64.7 (7.1) 64.8 (7.6) 64.4 (7.5) 64.6 (7.4) Sex (N, %) Male 495 (59.9) 518 (63.0) 482 (58.5) 507 (61.5) 2002 (60.7) Body weight (kg) * 91.8 (20.3) 92.9 (21.1) 91.8 (20.4) 91.9 (20.8) 92.1 (20.6) Type 2 diabetes, mean (SD) Diabetes duration (years) 14.3 (8.2) 14.1 (8.2) 14.0 (8.5) 13.2 (7.4) 13.9 (8.1) Glycated haemoglobin (%) 8.7 (1.4) 8.7 (1.5) 8.7 (1.5) 8.7 (1.5) 8.7 (1.5) Cardiovascular risk factors Systolic blood pressure (mmhg) * (18.0) (17.0) (16.2) (17.5) (17.2) Total Diastolic blood pressure (mmhg) * 77.1 (9.8) 76.9 (10.2) 77.5 (9.9) 76.7 (10.2) 77.0 (10.0) LDL cholesterol (mg/dl) 81.6 (47.1) 83.3 (41.2) 80.9 (48.1) 83.6 (45.9) 82.3 (45.6) Never smoked 390 (47.2) 364 (44.3) 391 (47.5) 348 (42.2) 1493 (45.3) Table 1. * Means and standard deviations. Geometric means and coefficients of variation. Number of patients (N) and percentage (%). LDL, low-density lipoprotein; SD, standard deviation. Marso et al. NEJM [in press] 30
31 HbA1c (%) HbA1c (mmol/mol) Change from baseline (%) Overall mean at baseline: 8.7% 9,0 72,1 0,0 Semaglutide 0.5 mg Semaglutide 1.0 mg Placebo 0.5 mg Placebo 1.0 mg 8,5 67,1-0,5-0,4-0,4 8,0 7,5 62,1 57,1-1,0-1,1-1,4-1,5 7,0 52,1 6,5 47, ,0 42, ,0 ETD: 1.05* [ 1.19; 0.91] ETD: 0.66* [ 0.80; 0.52] Weeks since randomisation Semaglutide 0.5 mg Semaglutide 1.0 mg Placebo 0.5 mg Placebo 1.0 mg Figure 2A. Data are estimated mean plus or minus standard error of the mean based on in-trial data for scheduled visits from the full analysis set, analysed by a mixed model for repeated measures with treatment group (semaglutide 0.5 and 1.0 mg and comparable placebo doses) and stratification (9 levels) as fixed factors and the corresponding baseline value as fixed factors and the corresponding baseline value as a covariate, all nested within visit. *Indicates significance (p-value <0.0001). CI, confidence interval; ETD, estimated treatment difference. Marso et al. NEJM [in press]
32 Microvascular outcomes Semaglutide No. (%) Incidence rate per 100 PYR No. (%) Placebo Incidence rate per 100 PYR Retinopathy complications 50 (3.0) (1.8) ; Need for retinal photocoagulation 38 (2.3) (1.2) ; Vitreous haemorrhage 16 (1.0) (0.4) ; Need for treatment with intravitreal agent Onset of diabetes-related blindness HR (95% CI) 16 (1.0) (0.8) ; (0.3) (0.1) ; New or worsening nephropathy 62 (3.8) (6.1) ; Persistent macroalbuminuria 44 (2.7) (4.9) ; Persistent doubling of serum creatinine level and creatinine clearance per MDRD <45 ml/min/1.73m2 Need for continuous renal-replacement therapy 18 (1.1) (0.8) ; P value 11 (0.7) (0.7) ; Supplementary Table 9. The primary composite outcome in the time-to-event analysis consisted of the first occurrence of either death from cardiovascular causes, non-fatal myocardial infarction or non-fatal stroke. The expanded composite outcome included death from cardiovascular causes, non-fatal myocardial infarction, non-fatal stroke, revascularisation (coronary and peripheral), hospitalisation for unstable angina or heart failure. CI, confidence interval; HR, hazard ratio; PYR, patient years of risk time (time from randomisation until first event or censoring). 32 Marso et al. NEJM [in press]
33 Patients with an event (%) New or worsening nephropathy 8 6 HR, 0.64 (95% CI, 0.46; 0.88) Events: 62 Semaglutide; 100 Placebo P=0.005 Placebo, 6.1% 4 Semaglutide, 3.8% Weeks since randomisation 109 Number of patients at risk Semaglutide Placebo Supplementary Figure 5B. Kaplan Meier plot for time from randomisation to first EAC-confirmed new or worsening nephropathy using in-trial data from subjects in the full analysis set. HR is from a proportional hazard model. CI, confidence interval; EAC, (external) event adjudication committee; HR, hazard ratio. 33 Marso et al. NEJM [in press]
34


35
36 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Grazie della vostra attenzione
37
38
39
40
41 The RIACE (Renal Insufficiency and Cardiovascular Events) study 15,773 patients with type 2 diabetes from Italy Stages of Diabetic nephropathy Normo 73,1% Micro 22,2% Macro 4,7% egfr strata (ml/min/1.73 m 2 ) 90 29,6% ,7% ,1% <30 1,7% MDRD NKF s KDOQI CKD stages No CKD 62,5% Stage 1 90* Stage * Stage Stages 4, 5 6,7% 12,0% 17,1% 1,7% <30 * Plus kidney damage Penno G et al. J Hypertens 29: , 2011
42
43
44
45 Baseline characteristics Liraglutide (N=4668) Placebo (N=4672) Male sex, N (%) 3011 (64.5) 2992 (64.0) Age, years 64.2 ± ± 7.2 Diabetes duration, years 12.8 ± ± 8.1 Geographic region Europe 1639 (35.1) 1657 (35.5) North America 1401 (30.0) 1446 (31.0) Asia 360 (7.7) 351 (7.5) Rest of the world 1268 (27.2) 1218 (26.1) HbA 1c, % 8.7 ± ± 1.5 BMI, kg/m ± ± 6.3 Body weight, kg 91.9 ± ± 20.8 Systolic blood pressure, mmhg ± ± 17.7 Diastolic blood pressure, mmhg 77.2 ± ± 10.1 Heart failure*, N (%) NYHA I,II,III. 835 (17.9) 832 (17.8) Full analysis set. Data are means ± standard deviations or number of patients (percentage of either liraglutide-treated or placebo-treated group). Percentage data refer to proportion of patients. *Heart failure includes NYHA class I, II and III. BMI, body mass index; HbA 1c, glycosylated haemoglobin; NYHA, New York Heart Association. Marso SP et al. N Engl J Med DOI: /NEJMoa
46 Primary outcome: Subgroup analyses Subgroup Hazard ratio (95% CI) p-value for interaction No. of patients Liraglutide Placebo no. of events/no. of patients (%) Primary analysis 0.87 (0.78 ; 0.97) /4668 (13.0) 694/4672 (14.9) Renal function 0.01 <60 ml/min/1.73 m (0.57 ; 0.85) /1116 (15.4) 223/1042 (21.4) >/=60 ml/min/1.73 m (0.83 ; 1.07) /3552 (12.3) 471/3630 (13.0) Renal function 0.93 <30 ml/min/1.73 m (0.51 ; 1.54) /117 (21.4) 26/107 (24.3) >/=30 ml/min/1.73 m (0.77 ; 0.97) /4551 (12.8) 668/4565 (14.6) Hazard ratio (95% CI) Favours Liraglutide Favours Placebo Prespecified Cox proportional-hazard regression analyses were performed for subgroups of patients with respect to the primary outcome (first occurrence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke). P values signify tests of homogeneity for between -group differences with no adjustment for multiple testing. The percentages of patients with a first primary outcome between the randomization date and the date of las t follow-up are shown. Renal function was assessed by means of the estimated glomerular filtration rate, as calculated by the Modification of Diet in Renal Disease equ ation. CI, confidence interval. Marso SP et al. N Engl J Med In press.
47
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare
 Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
Gli endpoint micro-vascolari nei trial di outcome cardiovascolare Giorgio Sesti University Magna Graecia of Catanzaro ITALY Potenziali conflitti di interesse Il Prof Giorgio Sesti dichiara di aver ricevuto
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Current Updates & Challenges In Managing Diabetes in CVD
 Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Current Updates & Challenges In Managing Diabetes in CVD Preventive Cardiovascular Conference 2016 Instituit Jantung Negara 12 th November 2016 Nor Azmi Kamaruddin Diabetes Clinic Department of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
LEADER and EMPA-REG. John Buse, MD, PhD. University of North Carolina School of Medicine Chapel Hill, NC, USA. Duality of Interest Declaration
 1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital Agenda Association between Cardiovascular Disease and Type 2 Diabetes Importance of HbA1c Management esp. High risk patients
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Endocrinologist Sweetgrass Endocrinology
 Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
Endocrinologist Sweetgrass Endocrinology Sanders, Cummings Ask Justice Department to Investigate Insulin Prices The Department of Justice and the FTC are asked to investigate whether Lilly, Novo Nordisk,
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Supplementary Online Content
 Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
Supplementary Online Content Afkarian M, Zelnick L, Hall YN, et al. Clinical manifestations of kidney disease among US adults with diabetes, 1988-2014. JAMA. doi:10.1001/jama.2016.10924 emethods efigure
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Kidney and heart: dangerous liaisons. Luis M. RUILOPE (Madrid, Spain)
") Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Kidney and heart: dangerous liaisons Luis M. RUILOPE (Madrid, Spain) Type 2 diabetes and renal disease: impact on cardiovascular outcomes The "heavyweights" of modifiable CVD risk factors Hypertension
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei
 University of Groningen Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Data Analysis Plan for assessing clinical efficacy and safety of ER niacin/laropiprant in the HPS2-THRIVE trial
 Data Analysis Plan for assessing clinical efficacy and safety of ER niacin/laropiprant in the HPS2-THRIVE trial 1 Background This Data Analysis Plan describes the strategy, rationale and statistical methods
Data Analysis Plan for assessing clinical efficacy and safety of ER niacin/laropiprant in the HPS2-THRIVE trial 1 Background This Data Analysis Plan describes the strategy, rationale and statistical methods
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
Bardoxolone Methyl Prevents egfr Decline in Patients with Chronic Kidney Disease Stage 4 and Type 2 Diabetes Post-hoc Analyses from BEACON
 Bardoxolone Methyl Prevents egfr Decline in Patients with Chronic Kidney Disease Stage 4 and Type 2 Diabetes Post-hoc Analyses from BEACON Christoph Wanner, MD; George Bakris, MD; Geoffrey A. Block, MD;
Bardoxolone Methyl Prevents egfr Decline in Patients with Chronic Kidney Disease Stage 4 and Type 2 Diabetes Post-hoc Analyses from BEACON Christoph Wanner, MD; George Bakris, MD; Geoffrey A. Block, MD;
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Rawshani Aidin, Rawshani Araz, Franzén S, et al. Risk factors,
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Rawshani Aidin, Rawshani Araz, Franzén S, et al. Risk factors,
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Cardiovascular Diabetology. Open Access ORIGINAL INVESTIGATION. C. R. L. Cardoso 1, N. C. Leite 1, C. B. M. Moram 2 and G. F.
 https://doi.org/10.1186/s12933-018-0677-0 Cardiovascular Diabetology ORIGINAL INVESTIGATION Open Access Long term visit to visit glycemic variability as predictor of micro and macrovascular complications
https://doi.org/10.1186/s12933-018-0677-0 Cardiovascular Diabetology ORIGINAL INVESTIGATION Open Access Long term visit to visit glycemic variability as predictor of micro and macrovascular complications
21 st Pan Arab Conference on diabetes March Intercontinental City Stars Hotel Cairo
 21 st Pan Arab Conference on diabetes March 21-24 2017 Intercontinental City Stars Hotel Cairo PACD21 2017 We are delighted to present you with the highlights this year from yet again a very successful
21 st Pan Arab Conference on diabetes March 21-24 2017 Intercontinental City Stars Hotel Cairo PACD21 2017 We are delighted to present you with the highlights this year from yet again a very successful
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Nuove opportunità terapeutiche nel Diabete Mellito
 Nuove opportunità terapeutiche nel Diabete Mellito Raffaele Napoli UOSD Medicina Interna ad indirizzo Diabetologico Dipartimento di Scienze Mediche Traslazionali, Università Federico II di Napoli 1 Potenziali
Nuove opportunità terapeutiche nel Diabete Mellito Raffaele Napoli UOSD Medicina Interna ad indirizzo Diabetologico Dipartimento di Scienze Mediche Traslazionali, Università Federico II di Napoli 1 Potenziali
JARDIAMET. (empagliflozin and metformin hydrochloride) 5 mg/500 mg, 5 mg/850 mg, 5 mg/1000 mg, 12.5 mg/500 mg, 12.5 mg/850 mg, 12.
 5 mg/500 mg, 5 mg/850 mg, 5 mg/1000 mg, 12.5 mg/500 mg, 12.5 mg/850 mg, 12.") JARDIAMET (empagliflozin and metformin hydrochloride) 5 mg/500 mg, 5 mg/850 mg, 5 mg/1000 mg, 12.5 mg/500 mg, 12.5 mg/850 mg, 12.5 mg/1000 mg NAME OF THE MEDICINE JARDIAMET contains two oral antihyperglycaemic
JARDIAMET (empagliflozin and metformin hydrochloride) 5 mg/500 mg, 5 mg/850 mg, 5 mg/1000 mg, 12.5 mg/500 mg, 12.5 mg/850 mg, 12.5 mg/1000 mg NAME OF THE MEDICINE JARDIAMET contains two oral antihyperglycaemic
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Updates from the ADA Annual Meeting. The LEADER and DEVOTE Trials
 18/09/2017 1 Updates from the ADA Annual Meeting The LEADER and DEVOTE Trials Richard Pratley, M.D. Samuel Crockett Chair in Diabetes Research Director, Florida Hospital Diabetes Institute Senior Scientist
18/09/2017 1 Updates from the ADA Annual Meeting The LEADER and DEVOTE Trials Richard Pratley, M.D. Samuel Crockett Chair in Diabetes Research Director, Florida Hospital Diabetes Institute Senior Scientist
Introduction, Study Rationale & Design
 Introduction, Study Rationale & Design John Buse, MD, PhD Verne S. Caviness Distinguished Professor Chief, Division of Endocrinology Director, NC Translational and Clinical Sciences Institute Executive
Introduction, Study Rationale & Design John Buse, MD, PhD Verne S. Caviness Distinguished Professor Chief, Division of Endocrinology Director, NC Translational and Clinical Sciences Institute Executive
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Du gusts is megl che one. Edoardo Mannucci
 Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Prevention of complications: are we winning or losing the battle. Naveed Sattar Professor of Metabolic Medicine
 Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Prevention of complications: are we winning or losing the battle Naveed Sattar Professor of Metabolic Medicine Duality of Interest Declaration Consultant or speaker for: Amgen, AstraZeneca, Boehringer
Heart Failure Management in T2 DM A Practical Approach. David Fitchett MD St Michael s Hospital Toronto
 Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Heart Failure Management in T2 DM A Practical Approach David Fitchett MD St Michael s Hospital Toronto Faculty: Faculty Disclosure David Fitchett MD,, FRCP(C) Associate Professor of Medicine, University
Supplementary Table 1. Patient demographics and baseline characteristics (treated patients).
.") Supplementary Table 1. Patient demographics and baseline characteristics (treated patients). Placebo (n=188) 10 mg (n=186) 25 mg (n=189) Total (n=563) Gender, n (%) Male 75 (40) 97 (52) 84 (44) 256 (45)
Supplementary Table 1. Patient demographics and baseline characteristics (treated patients). Placebo (n=188) 10 mg (n=186) 25 mg (n=189) Total (n=563) Gender, n (%) Male 75 (40) 97 (52) 84 (44) 256 (45)
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Faculty. Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY
 Faculty Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY 2 Disclosures Robert S. Busch, MD, FACE serves as a speaker for Astra Zeneca,
Faculty Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY 2 Disclosures Robert S. Busch, MD, FACE serves as a speaker for Astra Zeneca,
How to apply novel outcome data. to clinical practice. Preventing Cardiovascular Disease in Patients with T2DM
 Preventing Cardiovascular Disease in Patients with T2DM How to apply novel outcome data with GLP-1 RA to clinical practice Lars Rydén Department of Medicine K2 Karolinska Institutet Stockholm, Sweden Ljubljana
Preventing Cardiovascular Disease in Patients with T2DM How to apply novel outcome data with GLP-1 RA to clinical practice Lars Rydén Department of Medicine K2 Karolinska Institutet Stockholm, Sweden Ljubljana
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA
 Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
Actualités en diabétologie Quoi de neuf en 2016? S. Aouiche Service de diabétologie CHU Mustapha Alger.Pr BOUDIBA Deux médicaments valent mieux qu un dans le traitement du patient diabétique Jochen.SEUFERT
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Evaluation of Chronic Kidney Disease KDIGO. Paul E de Jong University Medical Center Groningen The Netherlands
 Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
SGLT-2 INHIBITORS: CVD REDUCTION THROUGH DIURESIS
 SGLT-2 INHIBITORS: CVD REDUCTION THROUGH DIURESIS Dr. Kirtida Acharya National chair, Diabetes Kenya Consultant Endocrinologist/Diabetologist, MP Shah Hospital KCS Symposium, 30 th June, 2017 Sarova Whitesands,
SGLT-2 INHIBITORS: CVD REDUCTION THROUGH DIURESIS Dr. Kirtida Acharya National chair, Diabetes Kenya Consultant Endocrinologist/Diabetologist, MP Shah Hospital KCS Symposium, 30 th June, 2017 Sarova Whitesands,
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes?
 Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Have you seen a patient like Elaine *?
 (linagliptin) 5mg tablets Have you seen a patient like Elaine *? *Hypothetical patient profile Elaine * : 60 years old Housewife *Hypothetical patient profile ELAINE*: T2D Patient with early signs of kidney
(linagliptin) 5mg tablets Have you seen a patient like Elaine *? *Hypothetical patient profile Elaine * : 60 years old Housewife *Hypothetical patient profile ELAINE*: T2D Patient with early signs of kidney
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
7 th Munich Vascular Conference
 7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
7 th Munich Vascular Conference Secondary prevention of major cardiovascular events in patients with CHD or PAD - What can we learn from EUCLID and COMPASS, evaluating Clopidogrel, Ticagrelor and Univ.-Prof.
Effect of SGLT-2 Inhibitors on the Heart. Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic
 Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
Effect of SGLT-2 Inhibitors on the Heart Robert Zimmerman MD Vice Chairman Endocrinology Director Diabetes Center Cleveland Clinic Disclosures Speaker - Johnson and Johnson - Merck Research - Merck - Novo
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
E.Ritz Heidelberg (Germany)
") Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale
 Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale Dichiarazione esplicita di trasparenza delle fonti di finanziamento e dei
Farmaci innovativi e terapie di associazione: quali opportunità? Giuseppe Penno Dipartimento di Medicina Clinica e Sperimentale Dichiarazione esplicita di trasparenza delle fonti di finanziamento e dei
Diabete mellito e complicanze cardiovascolari: dimensione del problema, bisogni ed evoluzioni terapeutiche
 ROADSHOW DIABETOLOGIA DIABETE MELLITO E COMPLICANZE CARDIOVASCOLARI Milano, 5 dicembre 2018 Diabete mellito e complicanze cardiovascolari: dimensione del problema, bisogni ed evoluzioni terapeutiche Stefano
ROADSHOW DIABETOLOGIA DIABETE MELLITO E COMPLICANZE CARDIOVASCOLARI Milano, 5 dicembre 2018 Diabete mellito e complicanze cardiovascolari: dimensione del problema, bisogni ed evoluzioni terapeutiche Stefano
Rationale: Objectives: Indication: Diabetes Mellitus, Type 2 Study Investigators/Centers: 300 physicians in 292 clinics Research Methods: Data Source:
 GSK Medicine: N/A Study No.: 112255 Title: A Korean, multi-center, nation-wide, cross-sectional, epidemiology study to identify prevalence of diabetic nephropathy in hypertensive patients with type 2 diabetes
GSK Medicine: N/A Study No.: 112255 Title: A Korean, multi-center, nation-wide, cross-sectional, epidemiology study to identify prevalence of diabetic nephropathy in hypertensive patients with type 2 diabetes
Personalising treatment of diabetic complications with a focus on A potential role for the gut microbiota in diabetic kidney complications
 Personalising treatment of diabetic complications with a focus on A potential role for the gut microbiota in diabetic kidney complications Peter Rossing MD DMSc University of Copenhagen Steno Diabetes
Personalising treatment of diabetic complications with a focus on A potential role for the gut microbiota in diabetic kidney complications Peter Rossing MD DMSc University of Copenhagen Steno Diabetes
Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative.
 Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative. Authors: Pamela Piscitelli 1, Francesca Viazzi 2 ; Paola Fioretto
Supplementary Information for: Predictors of chronic kidney disease in type 1 diabetes: a longitudinal study from the AMD Annals initiative. Authors: Pamela Piscitelli 1, Francesca Viazzi 2 ; Paola Fioretto
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Translating GLP-1 trial outcomes to cardiology practice
 Translating GLP-1 trial outcomes to cardiology practice Which patients will benefit? Lars Rydén Senior Professor Department of Medicine K2 Karolinska Institutet Stockholm, Sweden Munich August 27, 2018
Translating GLP-1 trial outcomes to cardiology practice Which patients will benefit? Lars Rydén Senior Professor Department of Medicine K2 Karolinska Institutet Stockholm, Sweden Munich August 27, 2018
SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney?
 SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney? Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center Groningen The Netherlands Disclosures:
SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney? Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center Groningen The Netherlands Disclosures: