Assistant Professor: Dr.Samer Al-Sawalhi (M.R.C.S.I)(M.D)
|
|
|
- Dustin Wilkins
- 5 years ago
- Views:
Transcription
1 Assistant Professor: Dr.Samer Al-Sawalhi (M.R.C.S.I)(M.D)
2
3
4
5
6
7
8
9
10 The incidence of pancreatic ca is 10: population per year *The disease is a disease of ageing. Male=Female *Approximately 80-90% of pancreatic cancer a rise from the ductules (Adenoca) *80% of pancreatic ca patients at first presentation have a tumor dvanced unresectable. *40% will exibit local spread. *50% demonestrate distant metastasis
11 *Tobacco smoking (3-4) folds. *Chronic pancreatitis *5-8% of pancreatic ca are familial
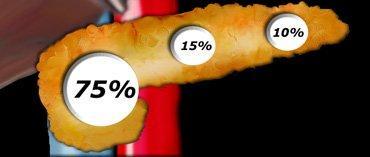
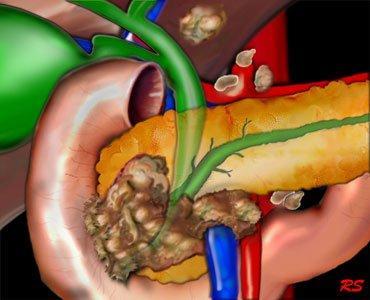
12 * > 85% of cases ductal cell adenocarcinoma. * 2/3 of pancreatic a denocarcinoma occur at head of pancreases. * 15-20% arise in the body and tail. * 20% diffusely involved the entire pancreas. *The importance of the pathology is that some tumors have a prolonged natural history,for instance, the cystadenocarcinoma,while those with an ampullary tumor or neuroendocrine have an increased survival after resection.
13
14
15 --* The most frequent symptoms are non-specific: 1- Epigastric pain & discomfort 75% Transmission of painful sensation (T5-T11)sympathetic celiac ganglia 2-Anorexia 3-Weight loss 4- Jaundice *Mild initial symptoms are dismissed both by doctor and patient *Jaundice is the commonest sign & symptoms which bring the attention of the patient *85% painless jaundice associated with nausea& epigastric discomfort. *Change in bowel habit is rare
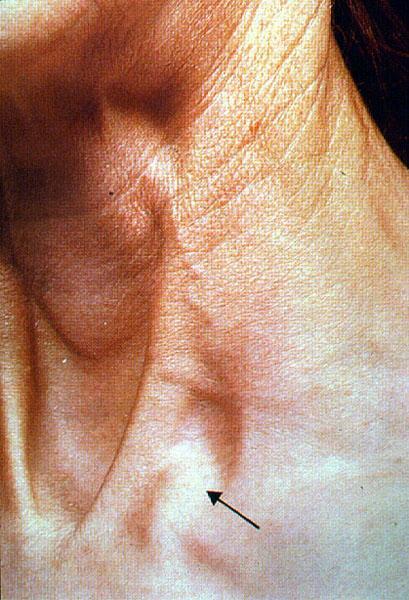
16 There is frequent evidence of weight loss Palpable liver palpable G.B (Courvoisier's law). Obstructed palpable G.B found in 1/4-1/2 of cases at presentation and it s presence doesn t implicate nonresectability. Metastatic L.N in neck(trosier s sign). Other signs of intra-abdominal malignancy should be looked for with care, such as a mass, ascites,& tumor deposits in the pelvic
17

18

19

20
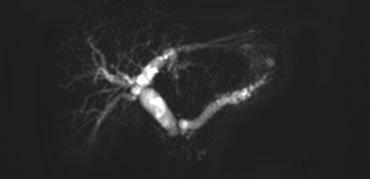
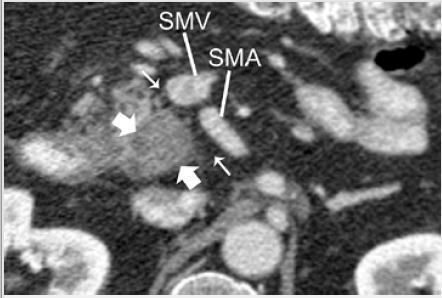
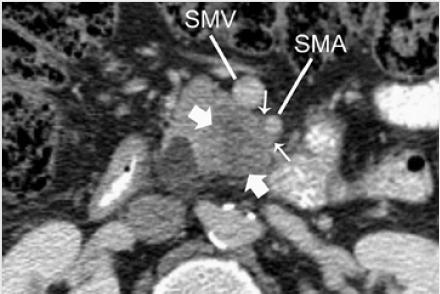
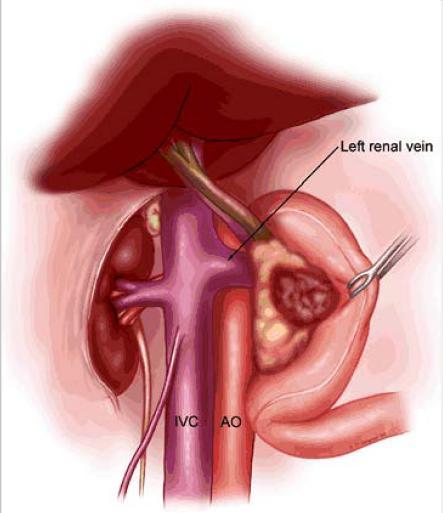
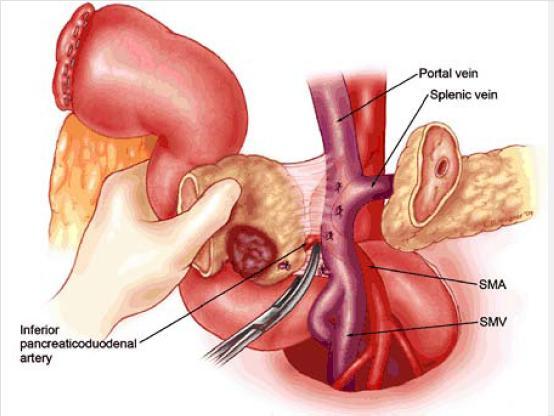
21 * Blood tests Ca 19-9 * Ultrasound: look for C.B.D Head of pancreas *Contrast enhanced spiral C-T scan(pancreatic protocol) * ERCP (DX & TX) *Endoscopic U/S: Assess the relationship between tumor and major vessels(sma, SMV,Portal vein) -Determine the location of the tumor

22


23
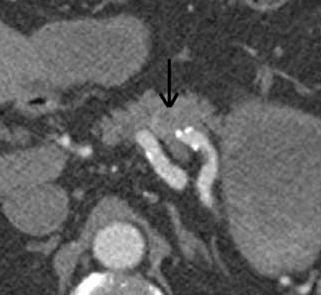
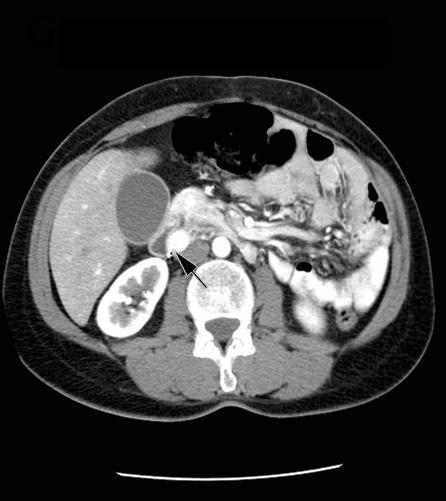
24 *Finding in C-T scan suggest unresectable tumor: 1-Presence of extra-pancreatic disease 2-Tumor extension to SMA or Celiac plexus. 3-No fat plane between the tumor and these structures 4-Occlusion of SMV-Portal vein junction

25
26
27
28

29
30
31 *90-95% of patients are unsuitable for resection because of either local spread to SMV & SMA, Para-aortic L.N or mesentric L.N or liver mets (Percutaneous True-cut biposy must be taken) *Assesement of operability and resectability Inoperable case----- palliative treatment should be offered 1-Jaundice is relieved by stent(metallic) 2-15% duodenal obstruction--- surgical bypass in early stage (gastrojejunostomy) Late phase stenting because prolonged delayed gastric emptying post surgery *PTC once ERCP or Stenting contraindicated *Neurolytic celiac plexus block to treat refratory pain (3-6) months
32 **The role of CTX in the management of pancreatic cancer remains ill defined *< 3% of pancreatic tumor (lymphoma) CTX in beneficial therapy. *In case of adenocarcinoma F.U or Gemcitabine produce a remission 15-25% * No long-term cures have been described *Neo-adjuvant or adjuvant RTX to reduce rate of local recurrence.
33 Assessment of patients general condition. Decision to a abort jaundice pre-op or not depend on: 1-If period of jaundice is short(2 weeks) it s safe to proceed to operation 2-If period of jaundice is prolonged--- stent *The clotting time should be carefully checked pre-operatively & adequate hydration must be insured
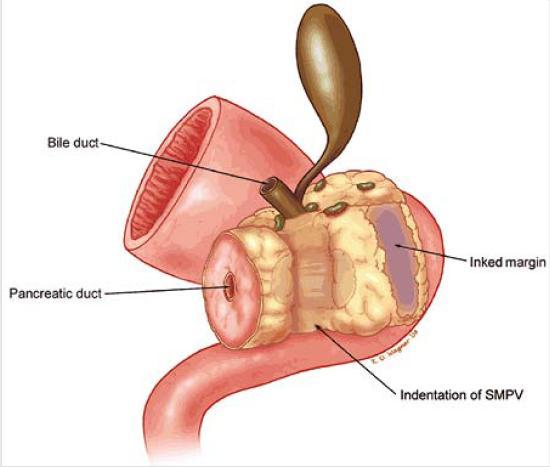
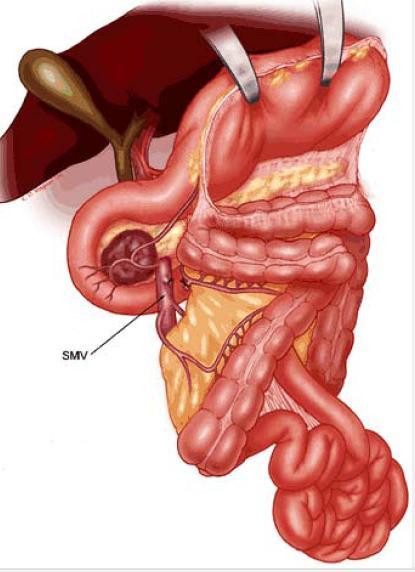
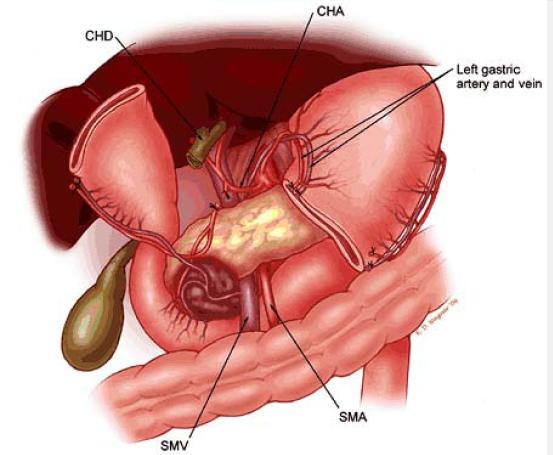
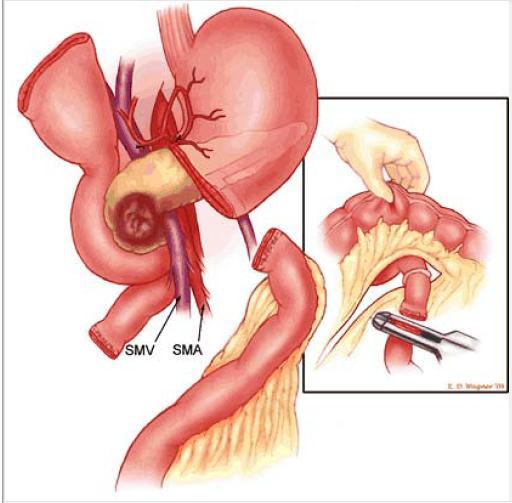
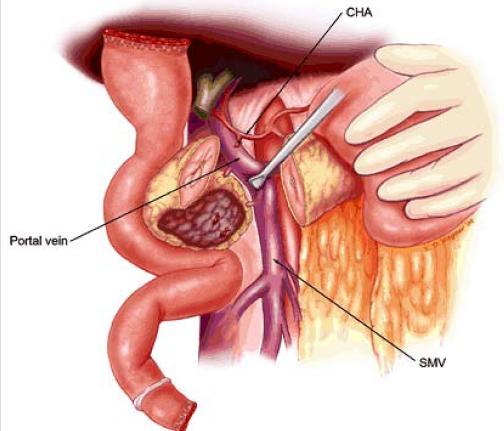
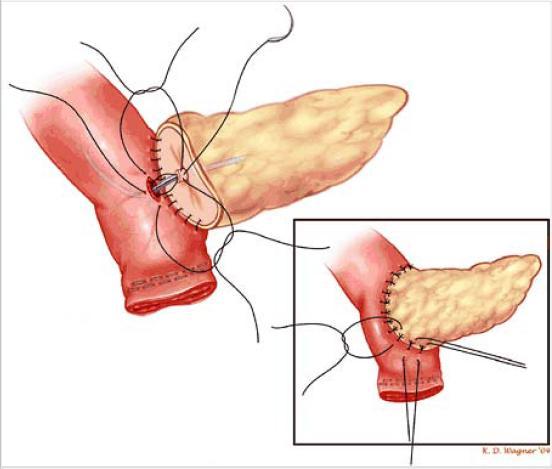
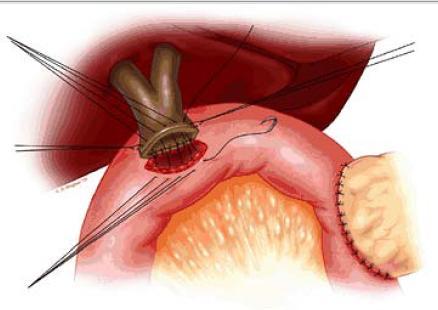
34 If a cystic tumor is encountered, no matter how large, most of these can be removed surgically with a reasonable chance of cure. *Patients with duct cell cancer which <4 cm in diameter not encasing SMV,A,Portal vein without metastsis surgical resection. *PPPR-pyloric preserving pancreatico dudenectomy with local lymphadenectomy (Whipple Procedure) Mortality rate(3-5%) Morbidity remains high with 40% complications: 1-Anastamotic leak (10%) 2-Infection-abscess 3-Dumping syndrome Post-op Adjuvant RTX and CTX with resection has not been elucidated
35
36
37
38
39
40
41
42
43
44
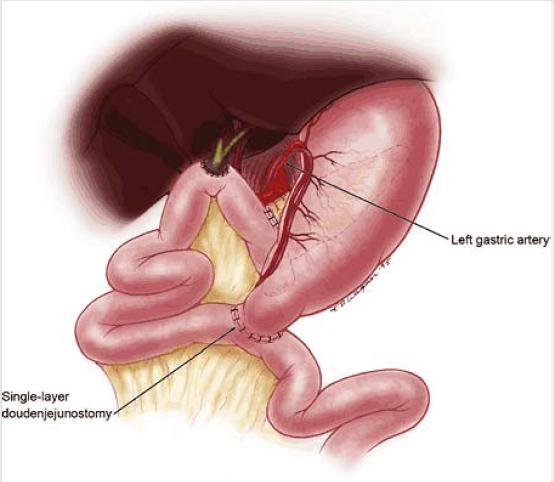
45 1- Delayed gastric emptying is found to be twice 2-Nutritional advantages 3-Decrease post-op duming syndrome and bile reflux gastritis
46 The overall median survival for patients with pancreatic cancer is 20weeks *5 year survival 5%
47
 produce insulin. 3-δ-cells (5%) produce VIP 4- PP cells (10-35%).")
48 * The islets of langerhans occupying 2% of pancreatic mass. *The islets of langerhans contain three types of cells: 1- α-cells (5-20%) produce glucagon. 2-β-cells (50-80%) produce insulin. 3-δ-cells (5%) produce VIP 4- PP cells (10-35%). *B- cells is the most prevalent *Tumors of these endocrine cell comprise 1% of all pancreatic tumors

49
50 **MEN syndrome may be assosciated with tumors in other endocrine glands specially anterior pituitary, the parathyroid and adrenal cortex *NET may secrete hormones which give rise to the following types: Insulinoma. Gastrinomas. Glucagonoma. Somatostatinoma. CCKoma. Acth ectopic Carcinoid syndrome (5HT)
51 *The most common islet cell tumor * (5-10%) accompany the MEN1 syndrome. * Most are benign *Attacks of hypoglycemia occur at irregular interval. Symptoms: Epigastric discomfort,nervousseness(odd behaviour) Trembling Sweating Dizziness
52 *Whipple triad: 1-Signs &symptoms of hypoglycemia induced by fasting 2-Blood glucose <45 mg/dl 3-Ameliorate the symptoms by administration of glucose. *Increase serum insulin>6 I.U/dl *Increase c-peptide
53 It has been founded equally distributed a cross the head, body and tail of pancreas *2/3 are located to the left of SMA. - Intra-op U/S with palpation of the pancreas -Endoscopic U/S -C-T scan -Selective angiography(rich in vascularity) -Selective arterial ca injection with hepatic venous sampling (APUD) sensitivity 90%
54
55
56 Extirpation of the tumor Intra-op U/S to localize the tumor Enuculation (Procedure of choice)
57 *ZES produces excessive amount of gastrin thereby stimulating gastric acid secretion& causing ulcer diathesis. *Highly suspected if the patient had P.U.D or G.E.RD in association with diarrhea. *80-90% of gastrinoma located in gastrinoma triangle. Duodenum is the primary site (45-60%) of the patients. 70% of duodenal gastrinoma located in the 1st part
58 75-80% are sporadic 20% are inherited associated with MEN1 60% are malignant L.Ns, liver & distant mets are common *Intractable P.U.D at very young age group. *Virulent P.U.D occurs in unusual sites like jejunum, unexplained diarrhea, coexistent parathyroid disease or family history
59 2/3 of patients with MEN1 have pancreatic neuroendocrine tumors. Symptoms: abdominal pain, secretary diarrhea relieved by N-G suction, reflux& dysphagia 90% of gastrinomas express receptors for somatostatin Therefore,somatostatin receptor scintigraphy (test of choice ) to localize the tumor
60
61 Surgical resection Octereotide Curability post surgery 30%
62 *Glucagon acts primarily to counter regulate insulin in glucose homeostasis. *Glucagon cleared by liver *Target organs for the effects of glucagon are the liver and adipose tissue. *Glucanoma are usually malignant ( body and tail) * If glucagon level >1000pg/ml diagnostic *Also increase the level of chromogranin
63 *Glucagonoma syndrome: -Diabetic mellitus -Migrating skin rash Necrolytic migratory erythema) -Hypoaminoacidemia -Malnutrition **Those patients are at high risk for development D.V.T give them prophylactic
64 To localize the tumor; 1-C-T scan 2-Somatostatin receptor scintigraphy Pre-op RX: Somatostatin analouge & nutrition supplementation
65 *Rare tumour *Neuro-endocrine tumour of D-cells *Located in the pancreas or duodenum. *> 50% have L.Ns & liver metastasis at time of diagnosis *Associated with somatostatinoma syndrome: 1-D.M 2-Cholelithiasis 3-Diarrhea with or without steatorrhea Pre-op check plasma levels of somatostatin Rx Pancreatico-dudenectomy
66 *Rare tumor * Neuroendocrine *Called Verner-Morrison s syndrome (WDHA)----watery diarrhea,hypokalemia,achlorhydriaalkalosis,flushing. *Symptoms: Ix: Elevated fasting level of VIP with secretory diarrhea>700 ml/day *Localization of the tumor by C-T scan somatostatin scintigraphy Rx---Volume resuscitating Rx of hypokalemia Octreotide Complete surgical resection
67 *Are common in F>M *5 th & 6 th decades of life *Most of them asymptomatic
68 *1-2% *Homogenous apperance *Can be radiological differentiated from malignant(serous cystadenocarcinoma) *2/3 located in body and tail *Honeycomb like cysts <2 cm *Central satellite scar(sunburst calcification) By EUS

69
70 If asymptomatic cyst <5 cm---- repeat imaging IN 3 MONTHS Rx EUS or C-T guided aspiration

71

72 * Premalignant disease * F=M *< 2% of pancreatic neoplasm. The spectrum of disease presentation ranging from the completely benign mucin producing tumour to those having insitu adenocarcinoma or invasive adenocarcinoma. *Symptoms & signs:obstructive jaundice,pancreatitis,abdominal pain, heavy mucin secretion, may present as diarrhea **mucous emanates from ampulla *K-ras (non-specific marker for the disease) Rx surgical resection(frozen section ve margin) 10% of IPMN harbor another malignancy like CRC
 protruding from the patulous orifice")
73 Figure 3. Endoscopic image of the duodenal papilla shows mucus ( ) protruding from the patulous orifice (arrows). Lim J H et al. Radiographics 2001;21: by Radiological Society of North America
74
75 Thank you
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Endocrine Tumors of the Gastrointestinal System. F. V. Nowak Ohio University March 22, 2005
 Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
CT 101 :Pancreas and Spleen
 CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
CT 101 :Pancreas and Spleen Shikha Khullar,, MD, MPH Division of Radiology University of South Alabama The Pancreas Normal Pancreas 3 Phase Pancreatic CT Non contrast Arterial phase : 30-35 35 second
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Neuro-endocrine and pancreatic non-adenocarcinomas. Marc Engelbrecht, AMC, Amsterdam
 Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Neuro-endocrine and pancreatic non-adenocarcinomas Marc Engelbrecht, AMC, Amsterdam Pancreatic Tumors q Epithelial Exocrine q Mesenchymal Ductal Adenocarcinoma (85-95%) Metastasis Lymfoma Acinar Cell Carcinoma
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Rare GI Malignancies
 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine Outline Gastrointestinal
X-ray Corner. Imaging of The Pancreas. Pantongrag-Brown L
 X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
X-ray Corner 125 Imaging of The Pancreas Modern imaging modalities commonly used in pancreas include ultrasound (US), CT, and MRI. Pancreas is a retroperitoneal organ which makes it difficult to visualize
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas)
 (see also: biliary/pancreatic folios => pancreas)") Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Pancreas (non-endocrine) (see also: biliary/pancreatic folios => pancreas) Physiology ductal system produces bicarb, high carbonic anhydrase secretin primary stimulus duodenal enterokinase activates trypsin
Objectives. Intraoperative Consultation of the Whipple Resection Specimen. Pancreas Anatomy. Pancreatic ductal carcinoma 11/10/2014
 Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Intraoperative Consultation of the Whipple Resection Specimen Pathology Update Faculty of Medicine, University of Toronto November 15, 2014 John W. Wong, MD, FRCPC Department of Anatomical Pathology Sunnybrook
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Collecting Cancer Data: Pancreas
 Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Pancreas NAACCR 2011 2012 Webinar Series 1/5/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Endocrinology and VHL: The adrenal and the pancreas
 Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Pancreatic Pathology. Janak A. Parikh, MD, MSHS, FACS Clinical Teaching Faculty St. John Providence Hospital
 Pancreatic Pathology Janak A. Parikh, MD, MSHS, FACS Clinical Teaching Faculty St. John Providence Hospital Determination of resectability A 68 year old female presents with a biopsy proven adenoca of
Pancreatic Pathology Janak A. Parikh, MD, MSHS, FACS Clinical Teaching Faculty St. John Providence Hospital Determination of resectability A 68 year old female presents with a biopsy proven adenoca of
SOLID PANCREATIC NEOPLASMS
 SOLID PANCREAIC NEOPLASMS SCBMR, Annual Meeting October 6-10, 2012 Boston, MA Isaac R Francis, M.B; B.S. University of Michigan Ann Arbor, Michigan Over 43,000 estimated cases in US in 2010 Over 36,000
SOLID PANCREAIC NEOPLASMS SCBMR, Annual Meeting October 6-10, 2012 Boston, MA Isaac R Francis, M.B; B.S. University of Michigan Ann Arbor, Michigan Over 43,000 estimated cases in US in 2010 Over 36,000
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas
 v1 GUIDELINES Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas Pancreatic Section of the British Society of Gastroenterology, Pancreatic Society of
v1 GUIDELINES Guidelines for the management of patients with pancreatic cancer periampullary and ampullary carcinomas Pancreatic Section of the British Society of Gastroenterology, Pancreatic Society of
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreatic Cancer Early Detection, Diagnosis, and Staging
 Pancreatic Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Pancreatic Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
David Bruyette, DVM, DACVIM Medical Director
 VCAWLAspecialty.com David Bruyette, DVM, DACVIM Medical Director The pancreas is made up of endocrine and exocrine tissue. The endocrine pancreas is composed of islets of Langerhans, which make up approximately
VCAWLAspecialty.com David Bruyette, DVM, DACVIM Medical Director The pancreas is made up of endocrine and exocrine tissue. The endocrine pancreas is composed of islets of Langerhans, which make up approximately
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment
 Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Pancreatic Adenocarcinoma: Everything You Need to Know From Cross-Sectional Imaging to Treatment Andrew W. Bowman, MD PhD Assistant Professor of Radiology Mayo Clinic Florida SCBT-MR Annual Meeting Nashville,
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
DOWNLOAD PDF TUMORS OF THE PANCREAS
 Chapter 1 : Endocrine Tumors of the Pancreas NIDDK This variant of pancreatic cancer is important to recognize because it is associated with a particularly poor prognosis, and in some instances is treated
Chapter 1 : Endocrine Tumors of the Pancreas NIDDK This variant of pancreatic cancer is important to recognize because it is associated with a particularly poor prognosis, and in some instances is treated
Control of Glucose Metabolism
 Glucose Metabolism Control of Glucose Metabolism The pancreas is both an exocrine and endocrine gland. It secretes digestive enzymes into the duodenum (exocrine) and 3 specific hormones into the bloodstream
Glucose Metabolism Control of Glucose Metabolism The pancreas is both an exocrine and endocrine gland. It secretes digestive enzymes into the duodenum (exocrine) and 3 specific hormones into the bloodstream
Intraductal papillary neoplasms in the bile ducts
 Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
AN ARGUMENT FOR SURGERY FOR GASTRINOMA. Lauren Wilson R1 General Surgery
 AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
Table: CPT Codes / HCPCS Codes / ICD - 10 Codes ; Code Code Description; Information in the [brackets] below has been added for clarification
![Table: CPT Codes / HCPCS Codes / ICD - 10 Codes ; Code Code Description; Information in the [brackets] below has been added for clarification](/thumbs/83/87857670.jpg "Table: CPT Codes / HCPCS Codes / ICD - 10 Codes ; Code Code Description; Information in the [brackets] below has been added for clarification") Table: CPT Codes / HCPCS Codes / ICD - 10 Codes ; Code Code Description; Information in the [brackets] below has been added for clarification purposes. Free ebook: Machiavelli's Laboratory "Ethics taught
Table: CPT Codes / HCPCS Codes / ICD - 10 Codes ; Code Code Description; Information in the [brackets] below has been added for clarification purposes. Free ebook: Machiavelli's Laboratory "Ethics taught
Pancreaticoduodenectomy
 Pancreaticoduodenectomy A Valuable Surgery Paul Montero PGY-III September 11, 2006 Overview Brief History Perils of Early Pancreaticoduodenectomy (PD) Improvements Quality of Life after PD Widened Indications
Pancreaticoduodenectomy A Valuable Surgery Paul Montero PGY-III September 11, 2006 Overview Brief History Perils of Early Pancreaticoduodenectomy (PD) Improvements Quality of Life after PD Widened Indications
Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma
 Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma Authors: R. Revert Espí, Y. Fernandez Nuñez, I. Carbonell, D. P. Gómez valencia,
Intraductal papillary mucinous neoplasm of the bile ducts: a rare form of premalignant lesion of invasive cholangiocarcinoma Authors: R. Revert Espí, Y. Fernandez Nuñez, I. Carbonell, D. P. Gómez valencia,
Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas
 CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Team approach is essential incorporating: radiology, gastroenterology, surgery and pathology Successful performance is operator dependent
 Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Committee V Post Brushing and FNA Testing Managment Options Daniel Kurtycz, M.D. Chair Committee V Committee V - Post brushing and FNA management options Team approach is essential incorporating: radiology,
Diseases of the endocrine pancreas
 Diseases of the endocrine pancreas Lecture outline Diabetes mellitus Pancreatic neuroendocrine tumors Diabetes mellitus, introduction Hyperglycemia due to defects in insulin secretion, insulin action,
Diseases of the endocrine pancreas Lecture outline Diabetes mellitus Pancreatic neuroendocrine tumors Diabetes mellitus, introduction Hyperglycemia due to defects in insulin secretion, insulin action,
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D
 A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
Tumor markers. Chromogranin A. Analyte Information
 Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Intra-arterial chemotherapy for patients with
 Annals of the Royal College of Surgeons of England (980) vol 62 ASPECTS OF TREATMENT* ntra-arterial chemotherapy for patients with inoperable carcinoma of the pancreas Lord Smith of Marlow KBE MS PPRCS
Annals of the Royal College of Surgeons of England (980) vol 62 ASPECTS OF TREATMENT* ntra-arterial chemotherapy for patients with inoperable carcinoma of the pancreas Lord Smith of Marlow KBE MS PPRCS
53 year old Female with Hypoglycemia. Colleen Flynn, MD April 5, 2012
 53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
53 year old Female with Hypoglycemia Colleen Flynn, MD April 5, 2012 HPI 53 yo F referred to the endocrine clinic for hypoglycemia x 1 year. History of a non secreting metastatic neuroendocrine tumor diagnosed
A Rare Case of Duodenal Somatostatinoma
 www.jmscr.igmpublication.org Impact Fact cor-1.1147 ISSN (e)-2347-176x A Rare Case of Duodenal Somatostatinoma Authors Dr Jitendra T. Sankpal, Dr Spoorthy Shetty, Dr Vivek Tilwani Dr. Manjiri J. Sankpal,
www.jmscr.igmpublication.org Impact Fact cor-1.1147 ISSN (e)-2347-176x A Rare Case of Duodenal Somatostatinoma Authors Dr Jitendra T. Sankpal, Dr Spoorthy Shetty, Dr Vivek Tilwani Dr. Manjiri J. Sankpal,
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
A retrospective analysis of neuroendocrine tumour of pancreas: a single institute study
 International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
International Journal of Research in Medical Sciences Chheda YP et al. Int J Res Med Sci. 2015 Nov;3(11):3041-3045 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20150928
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
X-Plain Pancreatic Cancer Reference Summary
 X-Plain Pancreatic Cancer Reference Summary Introduction Pancreatic cancer is the 4th leading cause of cancer deaths in the U.S. About 37,000 new cases of pancreatic cancer are diagnosed each year in the
X-Plain Pancreatic Cancer Reference Summary Introduction Pancreatic cancer is the 4th leading cause of cancer deaths in the U.S. About 37,000 new cases of pancreatic cancer are diagnosed each year in the
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Stomach. R.B. Kolachalam, MD
 Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Update on pancreatic neuroendocrine tumors
 Review Article Update on pancreatic neuroendocrine tumors Logan R. McKenna, Barish H. Edil Department of Surgery, University of Colorado, Academic Office One, Aurora, CO, USA Correspondence to: Barish
Review Article Update on pancreatic neuroendocrine tumors Logan R. McKenna, Barish H. Edil Department of Surgery, University of Colorado, Academic Office One, Aurora, CO, USA Correspondence to: Barish
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Accepted Manuscript. Classical features of Zollinger-Ellison syndrome, in images. Ali Alshati, MD, Toufic Kachaamy, MD
 Accepted Manuscript Classical features of Zollinger-Ellison syndrome, in images Ali Alshati, MD, Toufic Kachaamy, MD PII: S0016-5107(19)30069-0 DOI: https://doi.org/10.1016/j.gie.2019.01.026 Reference:
Accepted Manuscript Classical features of Zollinger-Ellison syndrome, in images Ali Alshati, MD, Toufic Kachaamy, MD PII: S0016-5107(19)30069-0 DOI: https://doi.org/10.1016/j.gie.2019.01.026 Reference:
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Hepato-Pancreatico-Biliary Surgery. Dr. Ankur J. Shah. MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK)
, FRCS (UK)") Hepato-Pancreatico-Biliary Surgery Dr. Ankur J. Shah MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK) Consultant Hepato-Pancreatico-Biliary and Liver Transplant Surgeon Ansh Liver Clinic Prevention to Cure Address
Hepato-Pancreatico-Biliary Surgery Dr. Ankur J. Shah MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK) Consultant Hepato-Pancreatico-Biliary and Liver Transplant Surgeon Ansh Liver Clinic Prevention to Cure Address
Case report Osteosarcoma of long bone metastatic to the pancreas-an unusual site of
 Osteosarcoma of long bone metastatic to the pancreas-an unusual site of Dr. Santosh Kumar Singh 1, Col (Dr.) Narayanan Kannan 2, Brig (Dr) Rajnish Talwar 3, ABSTRACT Col (Dr) Arvind Kumar Tyagi 4, Dr Adarsh
Osteosarcoma of long bone metastatic to the pancreas-an unusual site of Dr. Santosh Kumar Singh 1, Col (Dr.) Narayanan Kannan 2, Brig (Dr) Rajnish Talwar 3, ABSTRACT Col (Dr) Arvind Kumar Tyagi 4, Dr Adarsh
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
21/07/2017. CS Verbeke. Non-neoplastic disease of the pancreas PATHOLOGY OF NON-NEOPLASTIC PANCREATIC DISEASES
 Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
Non-neoplastic disease of the pancreas No indication for surgical resection of non-neoplastic disease (except end-stage chronic pancreatitis) Unexpected benign disease in 5-13% of pancreatic resections
CHOLANGIOCARCINOMA (CCA)
") CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012
 Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Upper GI Malignancies Imaging Guidelines for the Management of Gastric, Oesophageal & Pancreatic Cancers 2012 Version Control This is a controlled document please destroy all previous versions on receipt
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Intro to Gallbladder & Pancreas Pathology
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Gallstones (Cholelithiasis)
Case report. Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine
 Case report Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine Past medical history 38 years old male patient No past medical or surgical history prior to presentation No medications
Case report Kováčová Martina Comenius University in Bratislava Slovakia Faculty of medicine Past medical history 38 years old male patient No past medical or surgical history prior to presentation No medications