Controlling Hypertension in Primary Care: Hitting a moving target?
|
|
|
- Quentin Rodgers
- 5 years ago
- Views:
Transcription

1 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine No Conflicts of Interest
2 Controlling Hypertension in Primary Care: Hitting a moving target? Objectives Review why hypertension is the most important topic in medicine and the great job that primary care is doing Be familiar with the shifting and conflicting guidelines: JNC 7, JNC 8 now AHA/ACC 2017 vs AAFP/ACP 2017 vs. other international groups vs NCQA (clinical quality) metrics Appreciate the critical role of how the blood pressure is measured in interpreting the guidelines Be relieved by the lack of controversy in drug regimens Recognize and intervene on resistant hypertension
3 Hypertension is the most important topic in medicine.
4 Prevalence of Hypertension in the United States* 100% Hypertension Prevalence 80% 60% 40% 20% 6% 16% 31% 48% 65% 78% 0% Age *Based on NHANES data. Hypertension is defined as blood pressure 140/90 mmhg or antihypertensive treatment. Low reliability due to large relative error. Fields et al. Hypertension. 2004:44;
5 Benefits of Lowering BP Average Percent Reduction Stroke incidence 35 40% Myocardial infarction 20 25% Heart failure 50%
6 Global Disability Adjusted Life Years (DAYLs) Attributable to the 25 Leading Risk Factors 2010 Risk Factor 2010 Rank DALYs (95% UI) in thousands High blood pressure 1 173,556 ( Tobacco smoking, including exposure to secondhand smoke 2 156,838 (136, ) Household air pollution from solid fuels 3 108,084 (84, ,983) Diet low in fruit 4 104,095 (81, ,169) Alcohol use 5 97,237 (87, ) High body-mass index 6 93,609 (77, ,600) High fasting plasma glucose level 7 89,012 (77, ,390) Childhood underweight 8 77,316 (64,497-91,943) Expo sure to amblent particulate-matter pollution 9 76,163 (68,086-85,171) Physical inactivity or low level of activity 10 69,318 (58,646-80,182) Murray, Christopher J, et. al, New England Journal of Medicine, 2013
 32% Microvascular Complications 32% *P <0.05 compared to tight glucose control * 37% * Tight BP Control (Average 144/82 mmhg) Bakris GL, et al. Am J Kidney Dis.")
7 Diabetes: Tight Glucose vs Tight BP Control and CV Outcomes in UKPDS % Reduction In Relative Risk Stroke 5% 44% * Any Diabetic Endpoint 12% 24% * DM Deaths 10% Tight Glucose Control (Goal <6.0 mmol/l or 108 mg/dl) 32% Microvascular Complications 32% *P <0.05 compared to tight glucose control * 37% * Tight BP Control (Average 144/82 mmhg) Bakris GL, et al. Am J Kidney Dis. 2000;36(3): Reprinted by permission, Harcourt Inc.

8 Hypertension Control Horrible-Isn t it? Less than ½ of persons with hypertension are controlled 70% of people who start BP drugs stop within 5 years..

9 Blood Pressure Control Over Time Chobanian, N Engl J Med 2009;361:
10 The percentages are shown (mean and 95% confidence intervals) for hypertension prevalence, awareness, treatment, control, and proportion of treated patients controlled (control/treated) among adults 18 years of age in NHANES 1999 to 2012 at 2-year increments. Egan B M et al. Circulation. 2014;130: Copyright American Heart Association, Inc. All rights reserved.
11 Another database showing Hypertensives are mostly adherent 625,000 patients with prescription refill records available from insurer Adherent (>80%) 74.6% Moderate (60-79%) 15.3% Poor (<60%) 9.9% Pittman DG, et al Am J Managed Care 2010

12 Harris Health October 2018
13 Controlling Hypertension in Primary Care: Hitting a moving target? - Be familiar with the shifting and conflicting guidelines: JNC 7, JNC 8 now AHA/ACC 2017 vs AAFP/ACP 2017 vs. other international groups vs NCQA (clinical quality) metrics





14
15 Hypertension Treatment Effect Mirrors Observational Data Incidence of cardiovascular disease Systolic blood pressure (mmhg)





")
16 National Heart, Lung, and Blood Institute National High Blood Pressure Education Program U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)
17 JNC BP Classifications: DBP Stage 4 DBP (mm Hg) Hypertensive Consider therapy Severe Severe Severe Moderate Moderate Moderate Mild Mild Mild Stage 3 Stage 3 Stage 2 Stage 2 Stage 1 Stage 1 Stage 2 Stage Normal Normal Normal Normal Optimal Optimal Highnormal Highnormal Highnormal Highnormal Prehypertension Normal JNC I JNC II JNC III JNC IV JNC V JNC VI JNC 7 JNC I. JAMA. 1977;237: JNC II. Arch Intern Med. 1980;140: JNC III. Arch Intern Med. 1984;144: JNC IV. Arch Intern Med. 1988;148: JNC V. Arch Intern Med. 1993;153: JNC VI. Arch Intern Med. 1997;157: Chobanian AV et al. JAMA. 2003;289:

18 Hypertension. 1999;34:
19 JNC BP Classifications: SBP SBP (mm Hg) No recommendations for SBP in JNC I or JNC II ISH Border - line ISH Border - line Normal Stage 2 Stage 1 Stage 4 Stage 3 Stage 3 Stage 2 Stage 2 Stage 1 Stage 1 Highnormal Highnormal Normal Normal Optimal Optimal Prehypertension Normal JNC I JNC II JNC III JNC IV JNC V JNC VI JNC 7 JNC I. JAMA. 1977;237: JNC II. Arch Intern Med. 1980;140: JNC III. Arch Intern Med. 1984;144: JNC IV. Arch Intern Med. 1988;148: JNC V. Arch Intern Med. 1993;153: JNC VI. Arch Intern Med. 1997;157: Chobanian AV et al. JAMA. 2003;289:
20 Goals of Therapy JNC 8 majority report: over age 60: DM, cad, Ckd 150/90 mm/hg 140/90 mm/hg JNC 8 minority report: over age 60: 140/90 mm/hg
21 2010 Accord BP Diabetics 120mmHg vs. 140mmHg Negative 2013 SPS3 Post subcortical <130 mmhg vs < 140 mmhg Negative stroke 2015 SPRINT high risk 120mmHG vs. 140mmHG Stopped early!! not DM or CVA Benefit
22 Sprint Trial Major inclusion criteria Age > 50 SBP (tx or un tx) At least one of : Clinical CVD except CVA CKD egfr Framingham 10yr CVD risk > 15% Age >75 Major exclusion criteria Stroke DM CHF(sx or EF<35%) proteinuria >1 g/d CKD egfr <20 ADHERENCE CONCERNS SBP achieved: mmhg NNT event 61 NNT to Prevent one death 90





23 AHA/ACC 2017 vs everyone else
24 AHA 2017
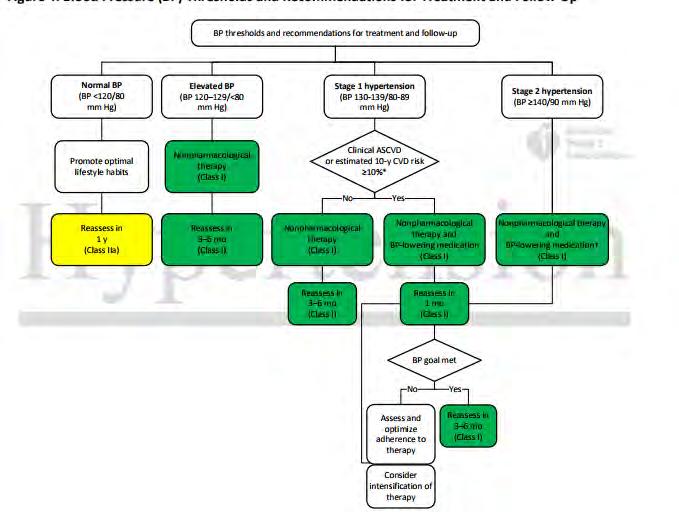
25 Changes in BP Categories from JNC 7 to the 2017 ACC/AHA HTN Guideline SBP DBP JNC ACC/AHA <120 and <80 Normal BP Normal BP and <80 Prehypertension Elevated BP or Prehypertension Stage 1 hypertension or Stage 1 hypertension Stage 2 hypertension 160 or 100 Stage 2 hypertension Stage 2 hypertension The 2017 ACC/AHA guideline definition of hypertension: SBP 130 mm Hg or DBP 80 mm Hg
26
27
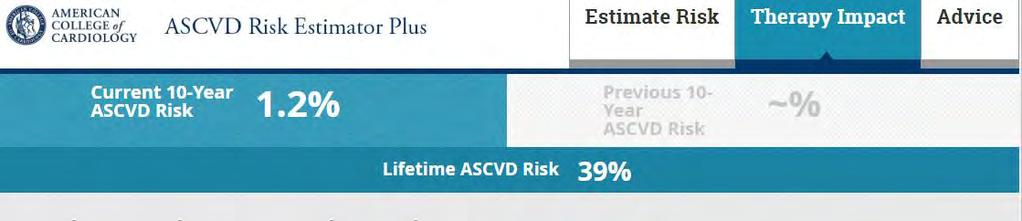
28
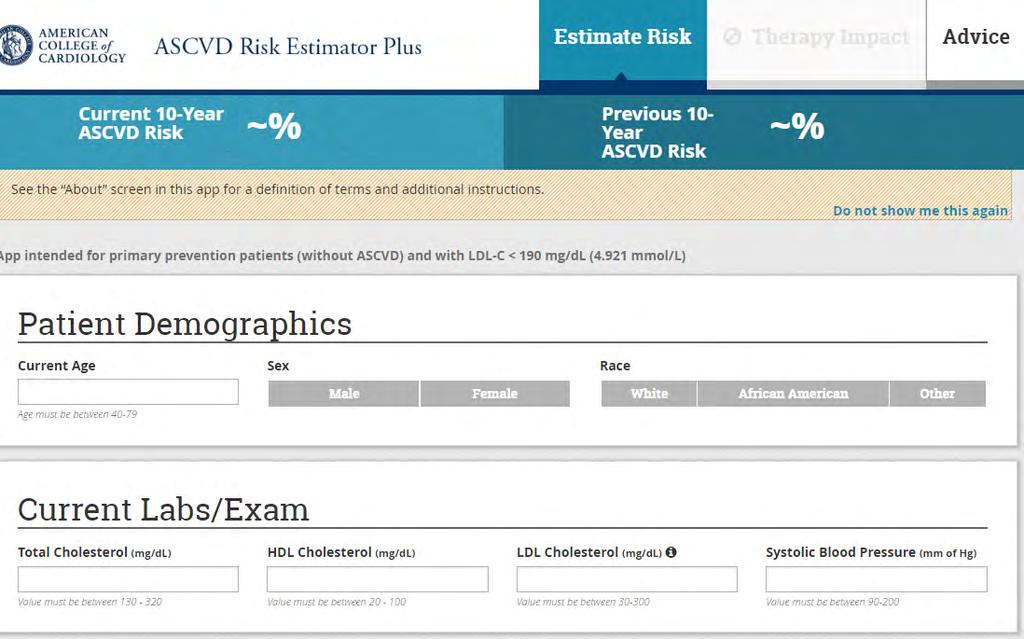
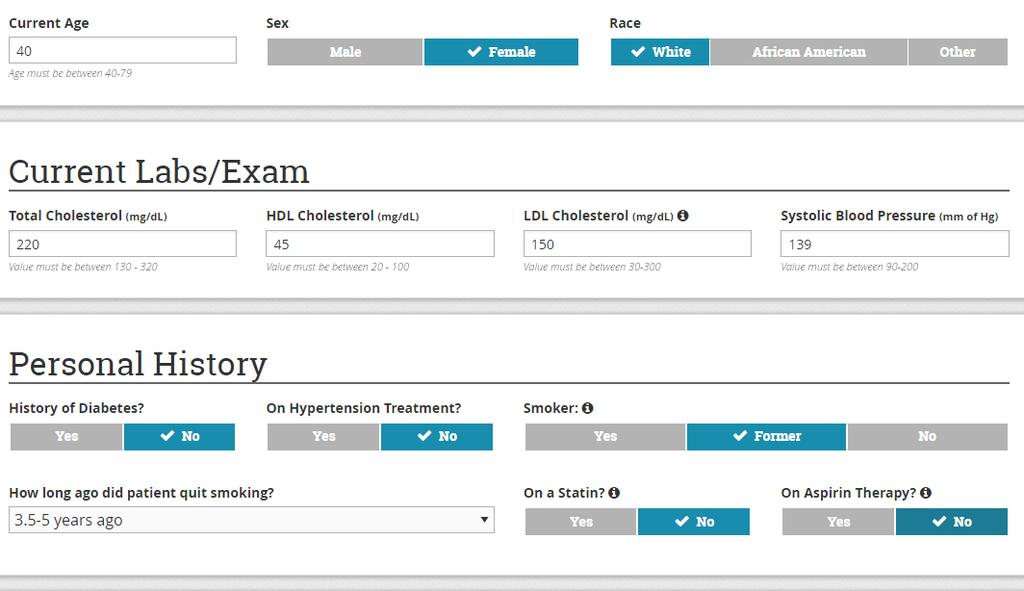
29 If same patient was 60WF 10 yr risk 4.8% If 40 WM 10 yr risk 1.8% If 40 BM 10 yr risk 10.0% If 60 WM,BM,BF 10 yr risk >10% You have to use the calculator, guesstimates difficult


30 Prevalence of Hypertension 2017 ACC/AHA and JNC 7 Guidelines Prevalence of hypertension, % Number of US adults with hypertension, millions 13.7% 31.1, M Muntner et. al., Journal of the American College of Cardiology 2017, Nov 6 Muntner, et. al., Circulation 2017 Nov 13
31 JNC 8 AHA/ACC 2017 ESC/ESH 2018 ACP/AAFP 2017 Threshold for starting by age >60 150/90 < /90 all ages 140/90 130/80 High risk < /90 >80 160/90 >60 150/no rec strong >60 CVA/TIA consider 140 (weak) >60 high risk consider 140 (weak Target for on treatment BP >60 150/90 <60 140/90 <130/ to 130 but not <120 > >60 < 150 >60 CVA/TIA consider 140mmHG (weak) >60 High risk consider 140 mmhg (weak)


32 Hitting the target How do you measure the BP you are acting on?
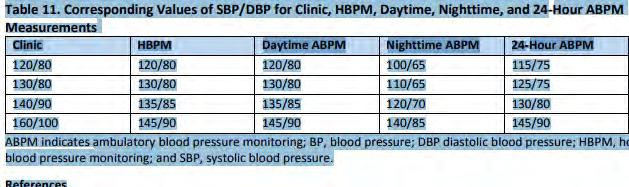
33 BP Measurement Techniques Method In-office Brief Description Two readings, 5 minutes apart, sitting in chair. Confirm elevated reading in contralateral arm. Ambulatory BP monitoring Indicated for evaluation of white-coat HTN. Absence of 10 20% BP decrease during sleep may indicate increased CVD risk. Self-measurement In Office automated unobserved May help improve adherence to therapy and evaluate white-coat HTN. Pt alone in room
34 If mean office visit SBP 140mmHG control about 50% frequency 68% 95% 99.7% mean Number of standard deviations either side of mean
35 AHA 2017
36 Sprint Maybe much ado about nothing? 1) Sprint used unobserved Automated Office BP (AOBP) - pt seated alone in room for 5 minutes - only after 5 minutes of rest, would take 3 measurement 1 minute apart unobserved AOBP averages SBP 16mmHG lower than regular office BP often similar to day ABPM 2) Intervention achieved SBP mmhg = about current 140 3) Control group had target of 140mmHG, could have baseline medications reduced to get there actual SBP controls mmhg = if individual at 140, = 166 Kjeldsen & Mancia European Heart J 2016


37 What BPs are we being graded on?


38 Definition of Hypertension Control in Clinical Practice NCQA/ HEDIS Enrolled for 1 year or more Have a hypertension code in 1st 6 months of year Age BP at last visit in chart used Control: < 140 and < 90 mmhg at sampled visit Sennett C, Managed Care 2000
39 NCQA HEDIS 2019 < 140/90 on last visit in evaluation period or remote BP devices electronically submitted HEDIS / w dm 140/ w/o dm 150/90

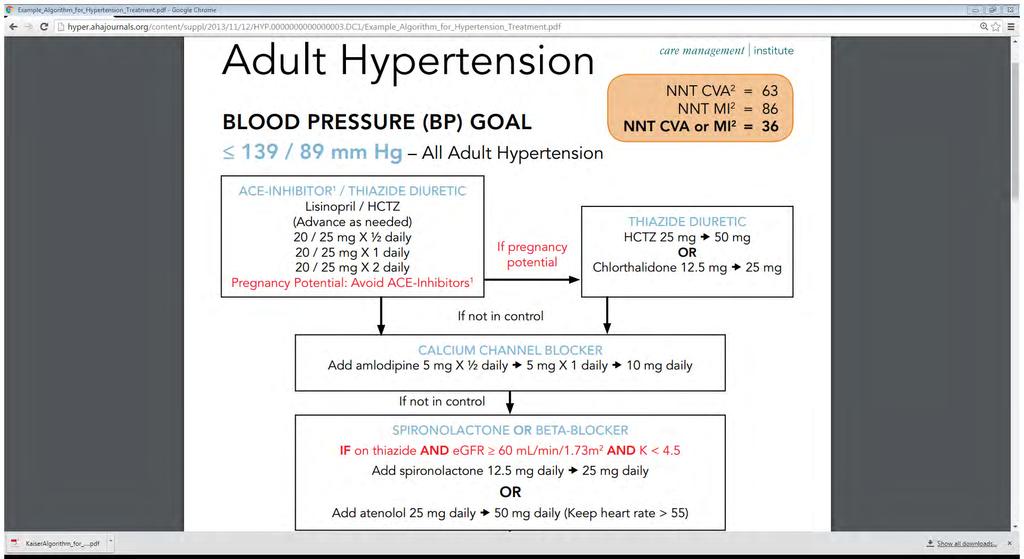
40 BP Drugs now the easy part - It will likely take more than one drug, tell patients this right from start - If it is really high start 2 drugs - Multidrug combination pills maybe good - If the blood pressure is high on subsequent visits- titrate the medication!!!! Clinical Inertia: not lack of access or non-adherence is biggest reason for lack of control
41 Order of BP medication use: 1 st (Ace or ARB) or CCB or Diuretic For DM (Ace or ARB ) For African Origin no DM: CCB or Diuretic 2 nd (Ace or ARB) and CCB or (ACE or ARB) and Diuretic 3 rd (Ace or ARB) and CCB and Diuretic 4 th spironolactone Only then, the other classes Sometimes other classes needed for other conditions or contraindications
42 NO ENALAPRIL Use Lisinopril Few B blockers NO Atenolol The REAL Dose of HCTZ is 50mg Chlorthalidone may be coming to Harris Health
43
44 What if the patient s Blood Pressure does not respond? RESISTANT HYPERTENSION
45 Definitions Resistant Hypertension: office blood pressure that remains elevated despite optimal doses of 3 classes of medication including diuretic if tolerated or controlled on 4 medicines Pseudo-resistant Hypertension: seems to meet definition but on further evaluation pt is -Non-adherent - Controlled on 24 hour ABPM - not really on optimal medications, - only uncontrolled on poor office measurement True resistant: not pseudo- resistant Apparent Resistant Hypertension: seems to meet definition but pseudo-resistant not ruled out
46 Apparent Resistant Hypertension Drilling down on the medical regimen: Source Result Persell NHANES Any diuretic 86% 2011 Study BP, drug names loop 30% not dosage thiazide like 59%(HCTZ 93%) 539 patients uncontrolled > 3 aldo antagonists 3.0% or controlled > 4 drugs Hanselin Drug insurance data base Any diuretic 93% 2011 drug names, dose, No BPs loop 19% 140,000/5million hypertensives on thiazide like 80% (HCTZ 94%) > 4 drugs Chlorthalidone 3%, aldo antagonist 5.9% HCTZ mean dose 21.1 mg Fontil National Ambulatory Medical Care Survey Any diuretic 77% drug names, no dosages, office BP loop 23 % 1567 pts w uncontrolled > 3 or controlled thiazide like 56% (HCTZ 96%) > 4 drugs Chlorthalidone 1.2% aldo antagonists 3.9% Grigoryan Primary care patients uncontrolled Any Diuretic 91% 2013 > 3 drugs, n=34 loop 15% Drug names, doses, ABPM, thiazide like 84% (HCTZ electronic adherence monitor Chlorthalidone 0% aldo antagonists 0% > ½ max dose ace/arb/ccb HCTZ 24/26 at 25mg QD
47 Resistant Hypertension Uncommon if Appropriate Drugs used In a network of 200 practices across the Southeast with 468,000 treated hypertensives those uncontrolled on 3 or more drugs at acceptable dose: 4.7% Egan B, Zhao Y, Li J et al
48 Houston TX On a very detailed drill down using ABPM and electronic bottle cap monitoring: of Apparent resistant hypertenvsives (N=69) 22% normal ABPM 29% non adherent Essentially no one optimally treated, mostly HCTZ 25,no Chlorthalidone, no spironolactone Grigoryan L, Pavlik VN, Hyman DJ J Am Soc Hypertens 2013
49 Patients with severe BP elevations referred to resistant hypertension clinics or for device therapy have very high levels of non-adherence when measured by blood or urine samples
50 Diuretics are the key to controlling difficult to control hypertension The dose of HCTZ is 50mg!!!!!! Chlorthalidone if you can get it- 25 mg Spironolactone 25 to 50 mg is 4 th drug Eplerenone is alternative
51 What is real prevalence of resistant hypertension? A network of 200 practices across the Southeast 468,000 treated hypertensives - uncontrolled on 3 or more drugs at acceptable dose Semi Apparent Resistant Hypertension 4.7% Egan B, Zhao Y, Li J et al
52 Diuretics are the key to controlling difficult to control hypertension The dose of HCTZ is 50mg!!!!!! Chlorthalidone if you can get it- 25 mg Spironolactone 25 to 50 mg is 4 th drug Eplerenone is alternative
53 Conclusions Hypertension is the most important topic in Medicine! You don t have to accept the 2017 AHA/ACC guideline A well measured in office 140/90 is good criteria for starting 130/80 maybe indicated is some high risk patients 130/80 maybe reasonable target if well tolerated It is very fair that we will still be graded on 140/90 If someone actually fits SPRINT criteria, and wants to do it- go for it! but remember it is an average SBP 121mm, not always less than 120mmHG
54 Conclusions continued.. Measurement counts- follow the literature -follow your office practicethe closer to Automated Office BP method the better Do drugs! ACE(ARB) CCB diuretics Hctz 50 aldactone 4 th Resistant hypertension: check adherence. Rare referral for 2 nd hypertension

55 Hypertension is the most important topic in medicine!!! Please do not let any differences in guidelines lead us to nihilism and inaction!!!
56
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice
 Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
Hypertension Guidelines: Lessons for Primary Care. Paul A James MD Professor and Chair Department of Family Medicine University of Washington
 Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων
 Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων Εύα Καρπάνου Δ/ντρια Αντιυπερτασικού Ιατρείου Α ΚΚ Ωνάσειου ΚΚ Θεσσαλονίκη, 14/2/13 Η µελέτη δεν υποστηρίχθηκε από φαρµακευτικές εταιρείες
Στόχοι αρτηριακής πίεσης σε ειδικούς πληθυσµούς και επιλογή φαρµάκων Εύα Καρπάνου Δ/ντρια Αντιυπερτασικού Ιατρείου Α ΚΚ Ωνάσειου ΚΚ Θεσσαλονίκη, 14/2/13 Η µελέτη δεν υποστηρίχθηκε από φαρµακευτικές εταιρείες
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Best Practices in Cardiac Care: Getting with the Guidelines
 Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Osama Sanad (MD) Prof. of Cardiology Benha University 2016
 Prof. of Cardiology Benha University 2016") Osama Sanad (MD) Prof. of Cardiology Benha University 2016 Back in time. 1912 Back in time. 1912 No body knows that hypertension is a lethal disease Hypertension in 1940s Among anti-hypertensives mentioned
Osama Sanad (MD) Prof. of Cardiology Benha University 2016 Back in time. 1912 Back in time. 1912 No body knows that hypertension is a lethal disease Hypertension in 1940s Among anti-hypertensives mentioned
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
JNC-8. (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines
 An Update on Hypertension Guidelines") JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
JNC-8 (Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure- 8) An Update on Hypertension Guidelines Derrick Sorweide, DO Assistant Professor of Family Medicine,
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB
 Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB Increasing stroke numbers in New Zealand an 'epidemic' says leading AUT
Management of Hypertension for Stroke Prevention in New Zealand: Can We Do Better? Walter van der Merwe Nephrologist Waitemata DHB Increasing stroke numbers in New Zealand an 'epidemic' says leading AUT
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Hypertension Guidelines Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center
 Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Hypertension Guidelines 2016 Michael A. Weber, MD Division of Cardiovascular Medicine State University of New York Downstate Medical Center Speaker Disclosures I disclose that I am a Consultant for: Ablative
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card