RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
|
|
|
- Brenda Waters
- 5 years ago
- Views:
Transcription
1 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
2 HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular Glomerular Chronic Rejection
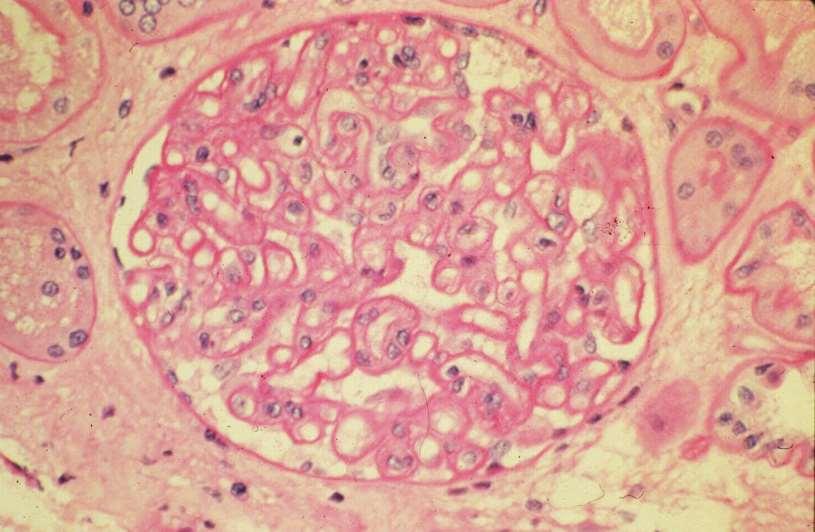
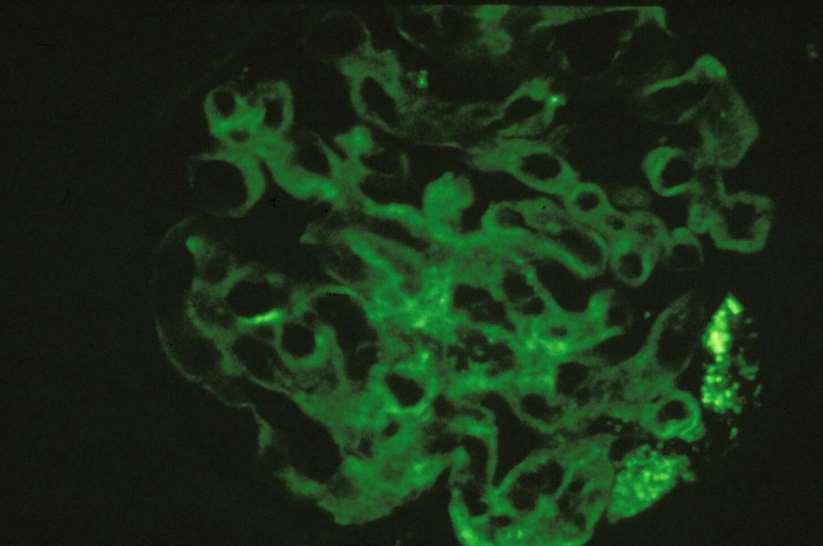
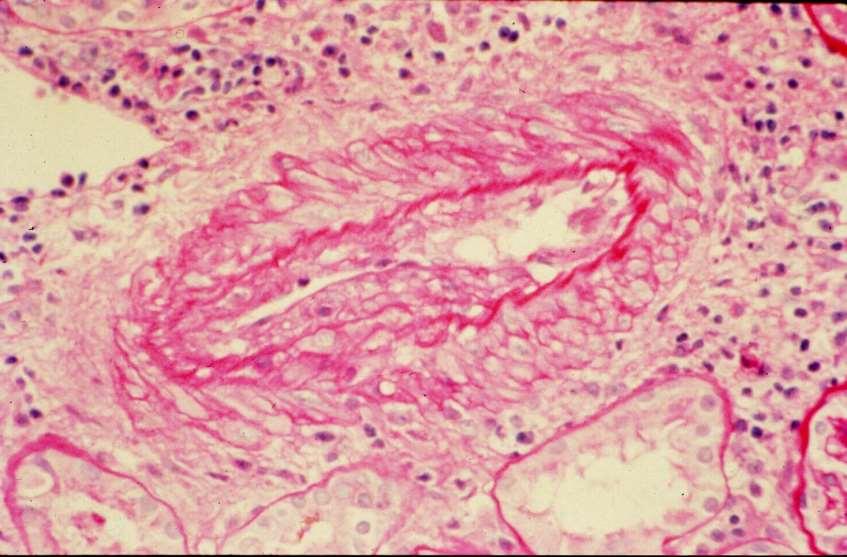
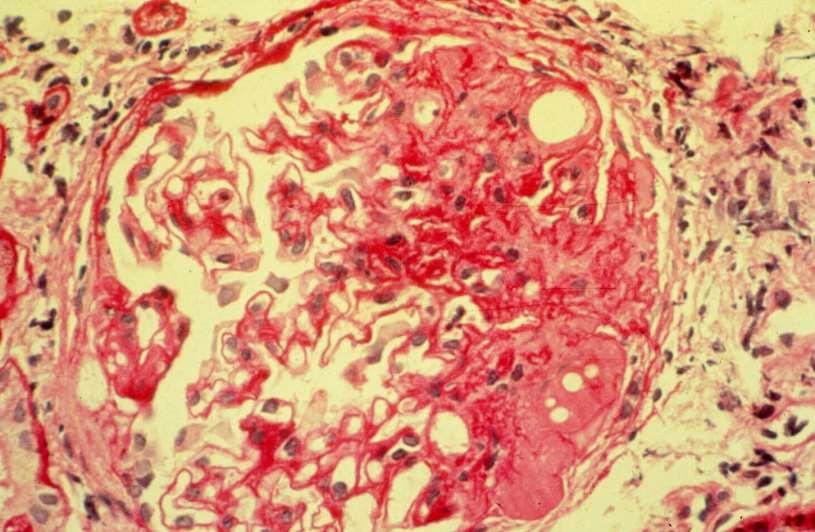
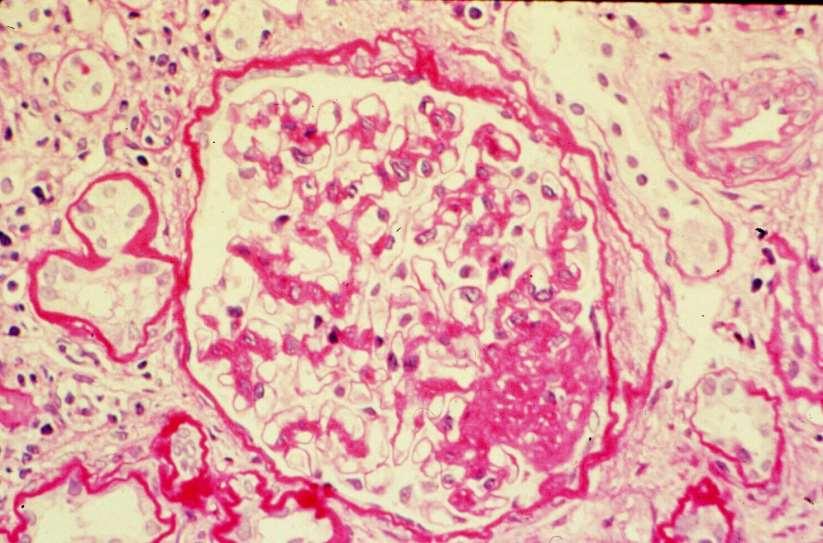
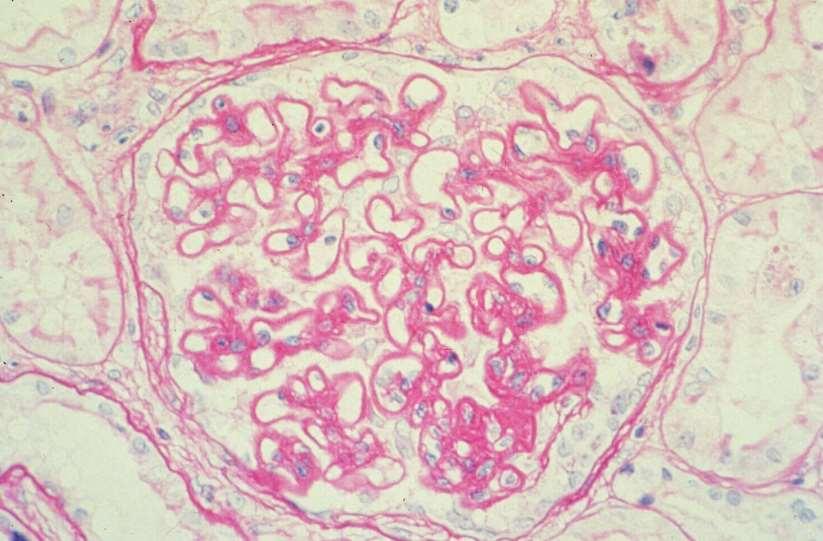
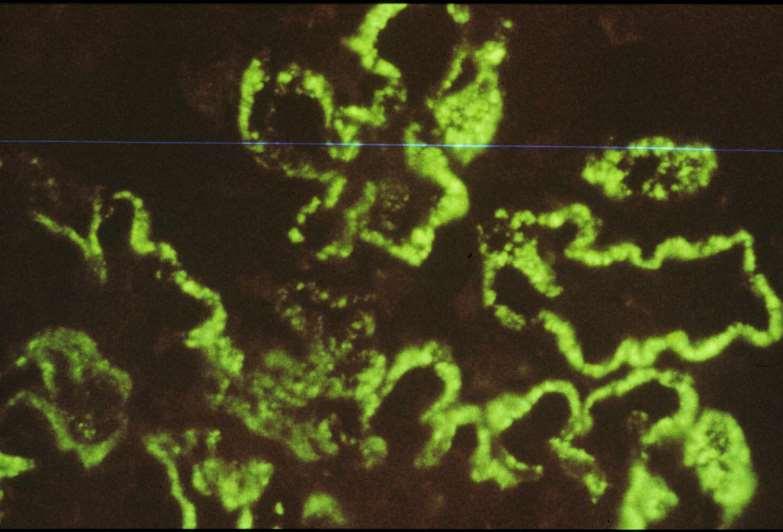
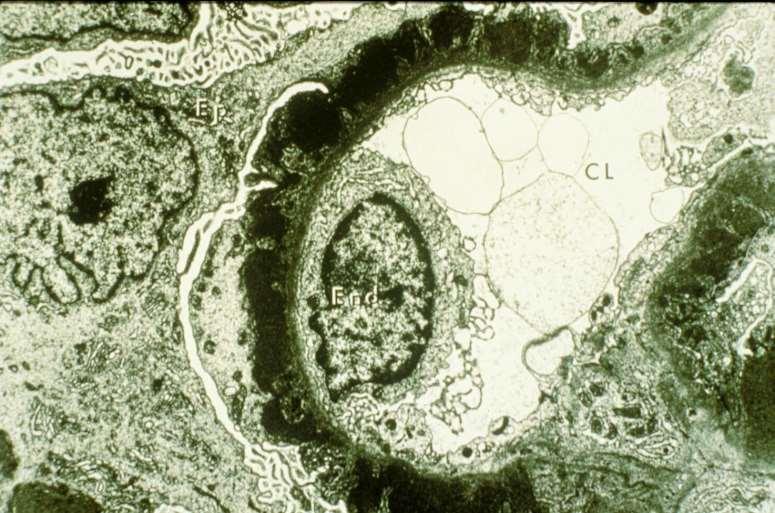
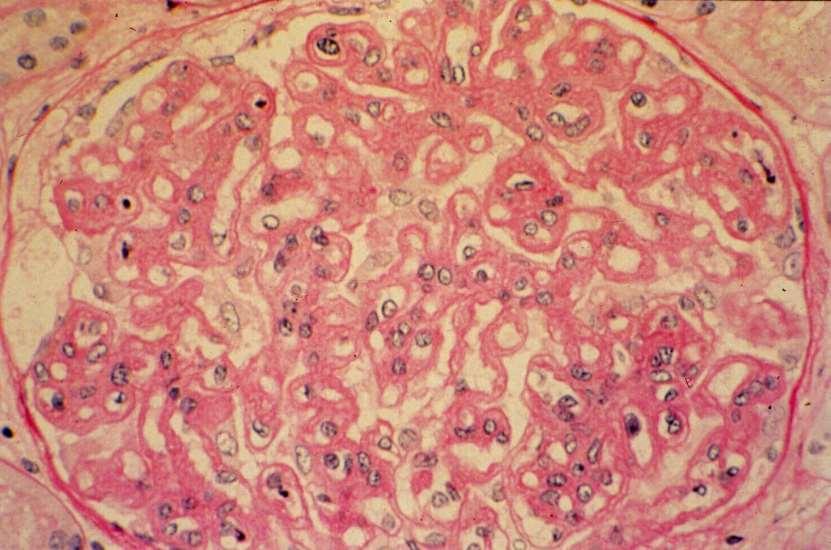
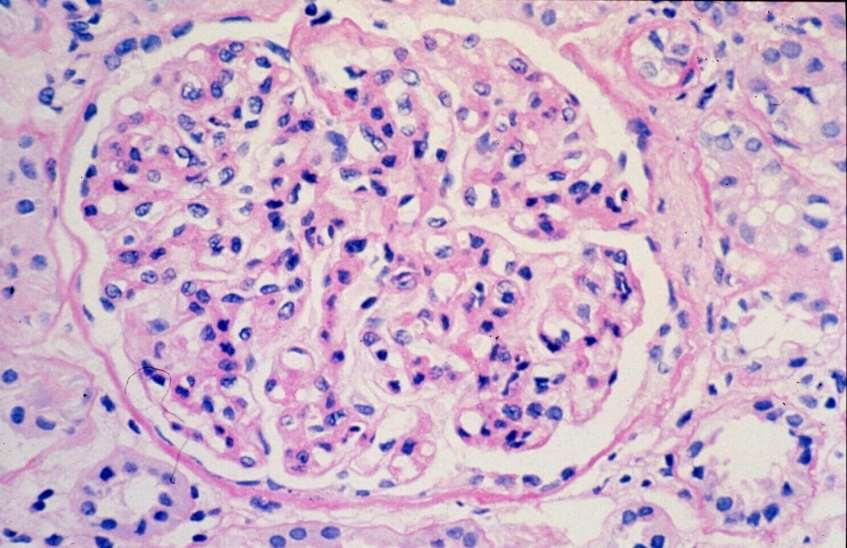
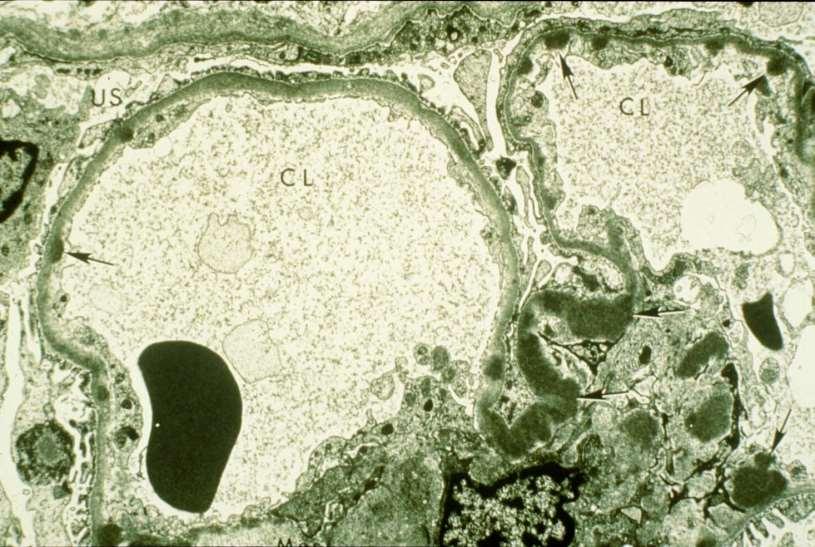
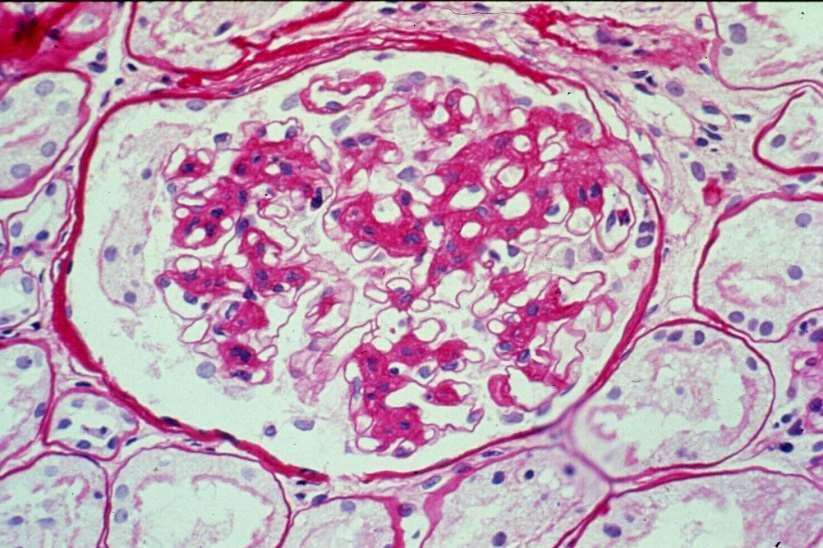
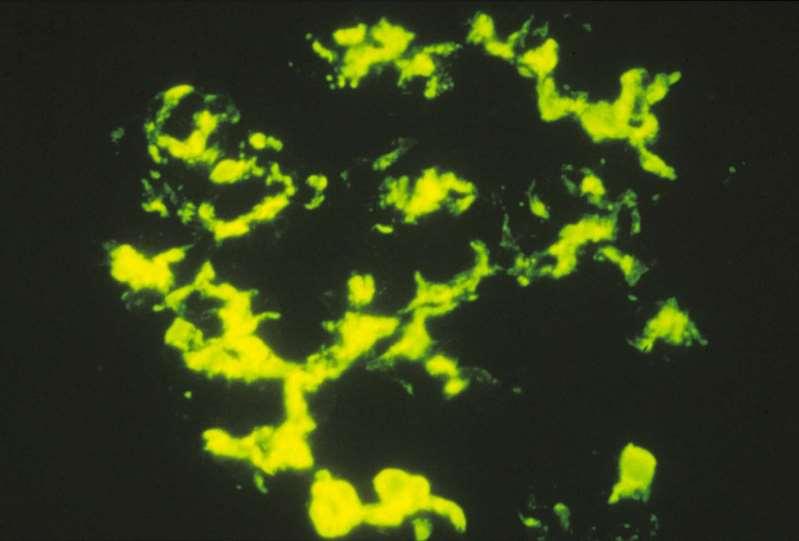
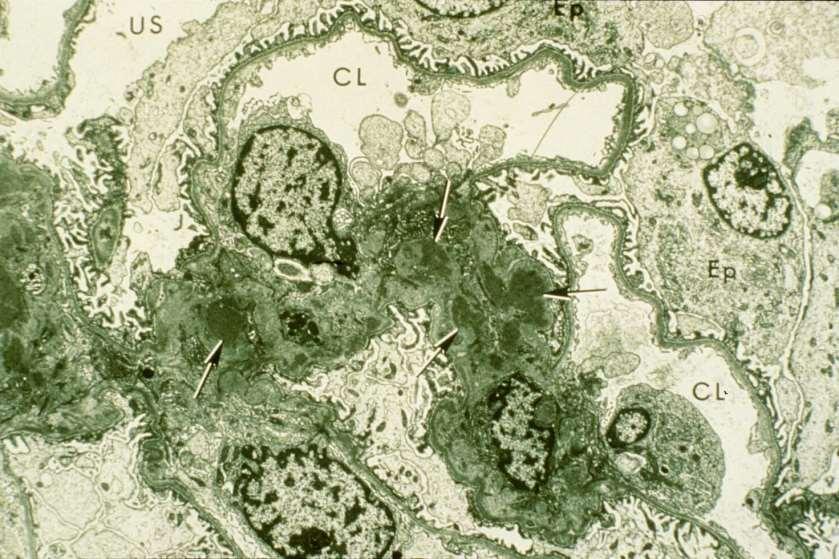
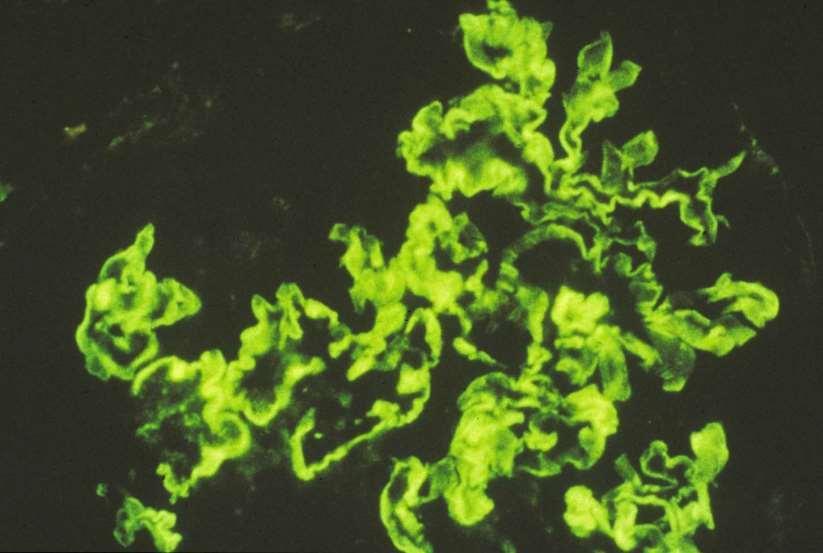
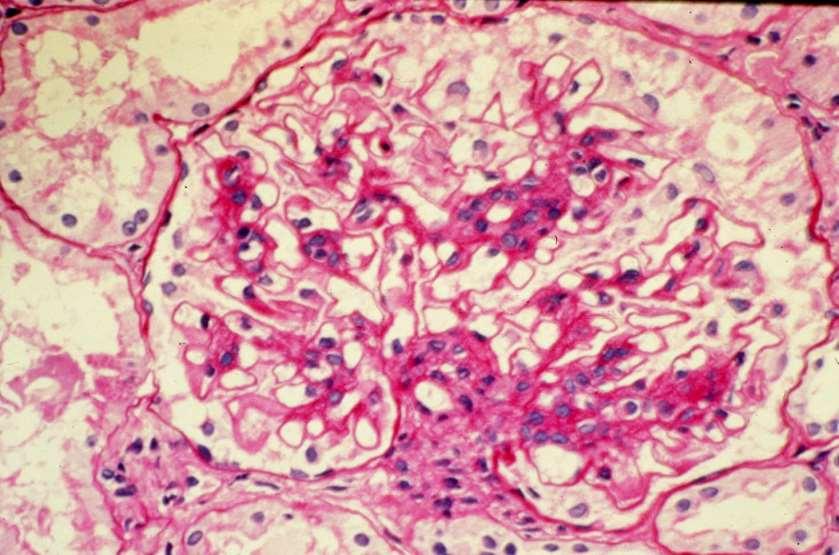
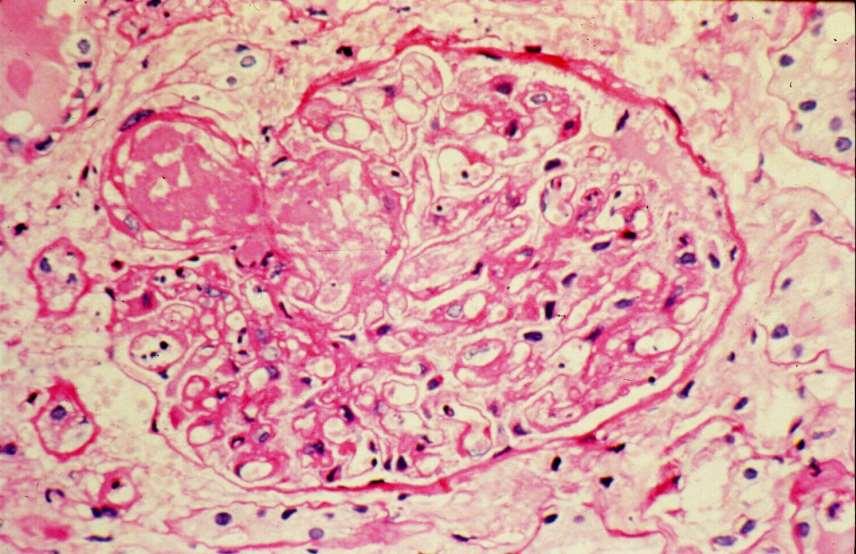
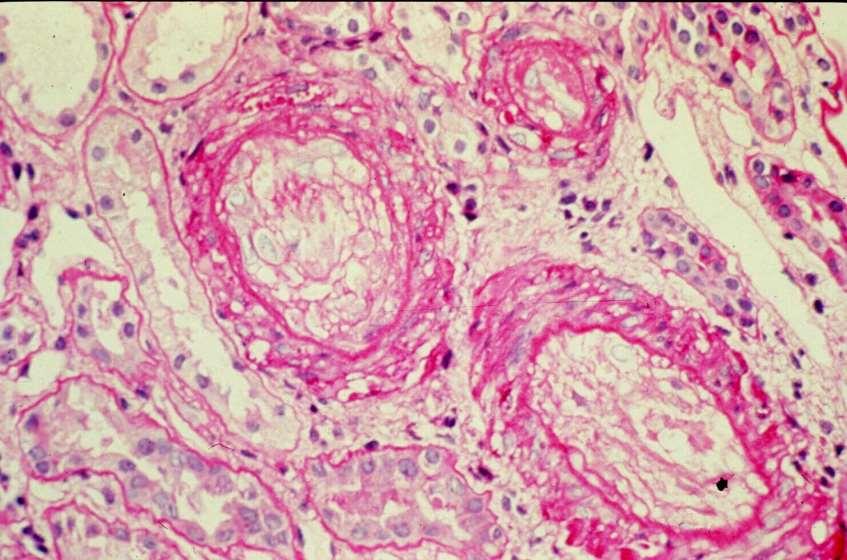
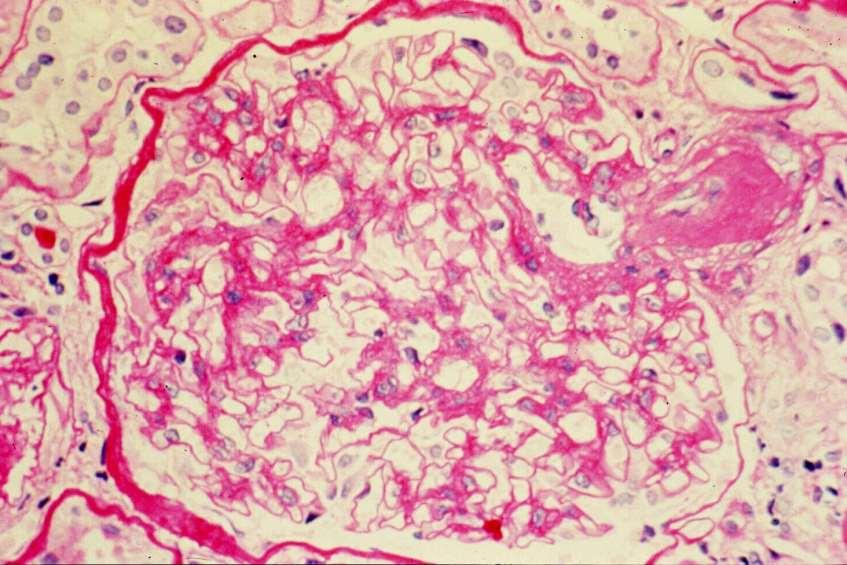
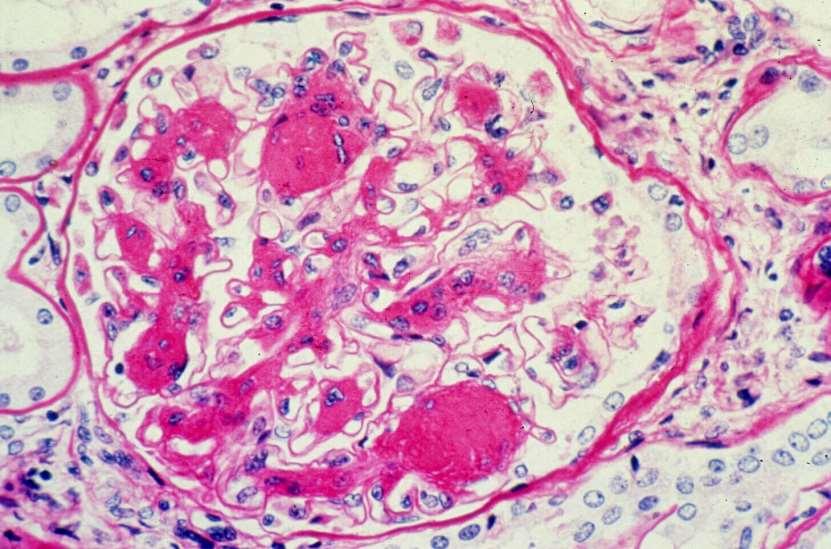
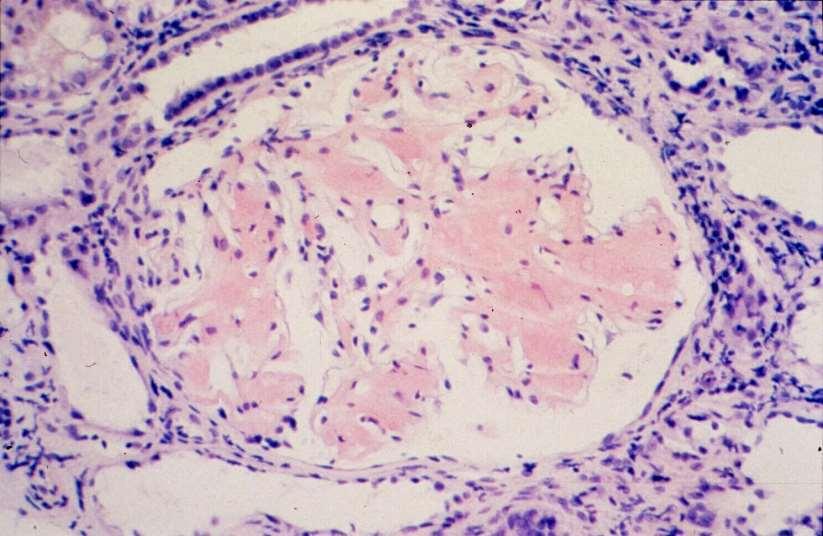
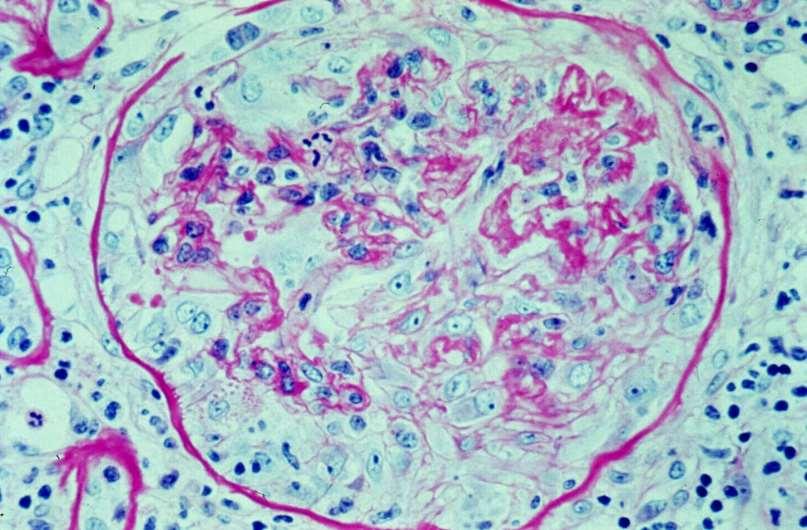
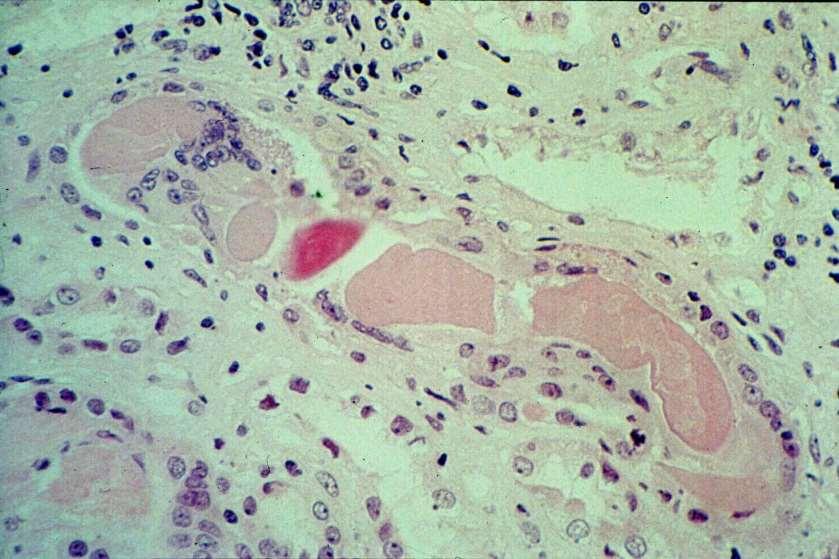
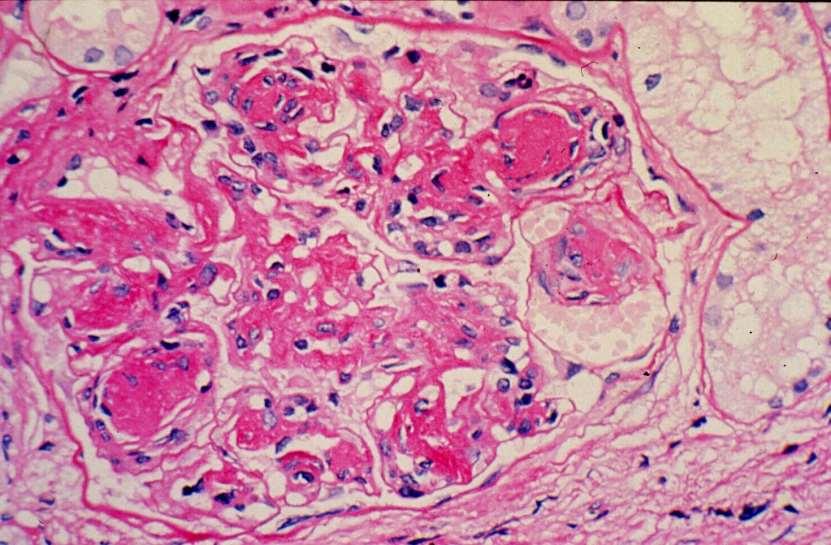
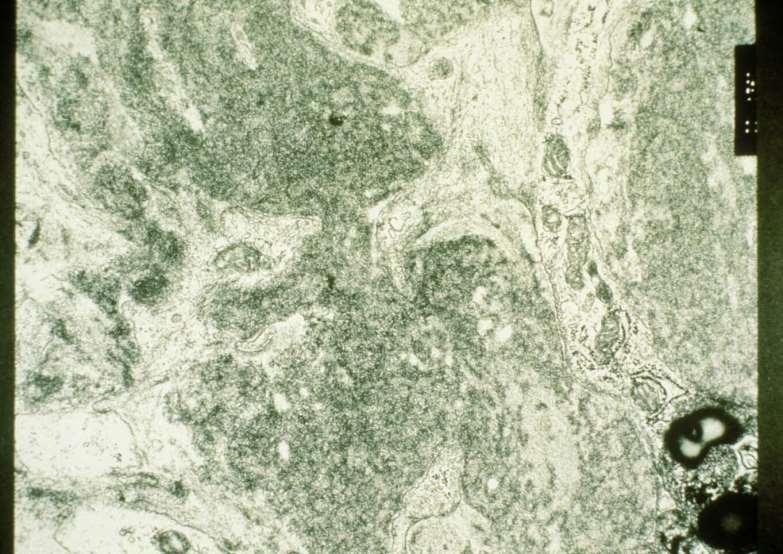
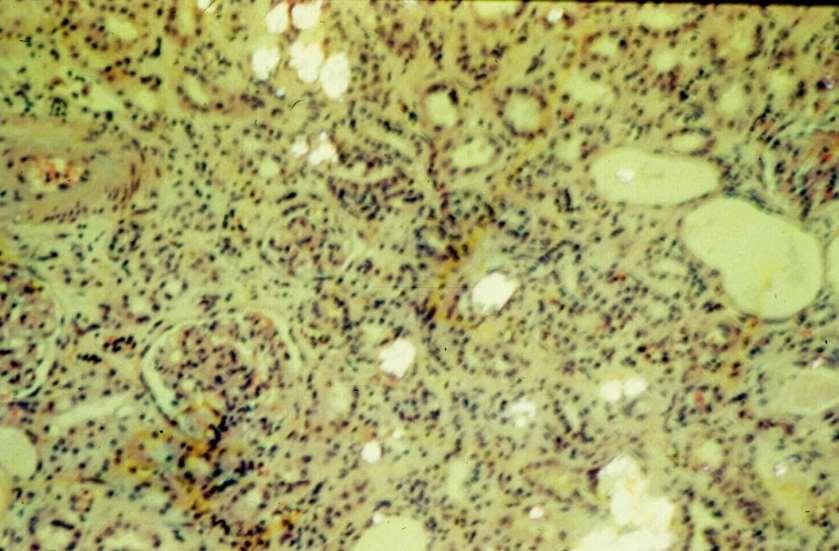
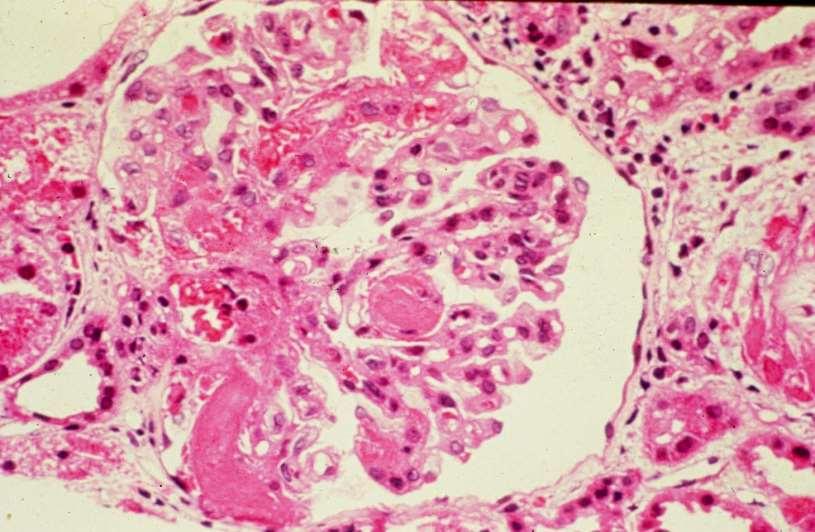
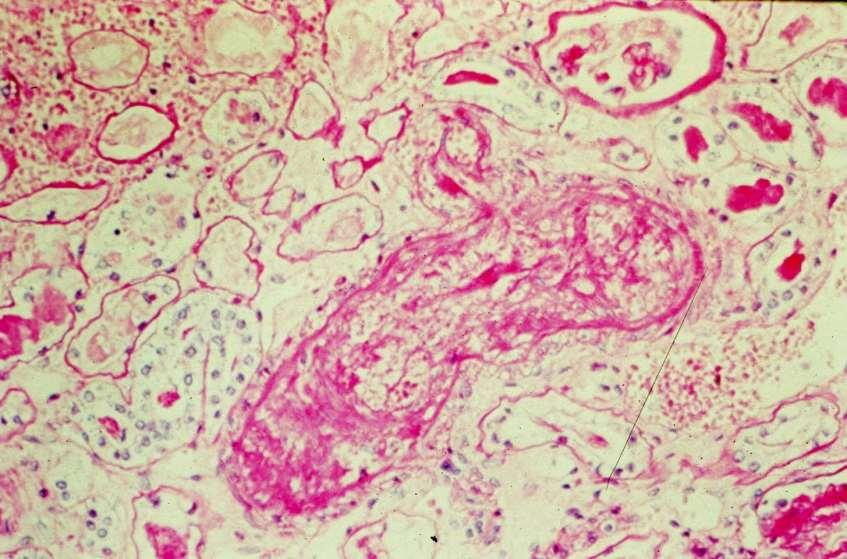
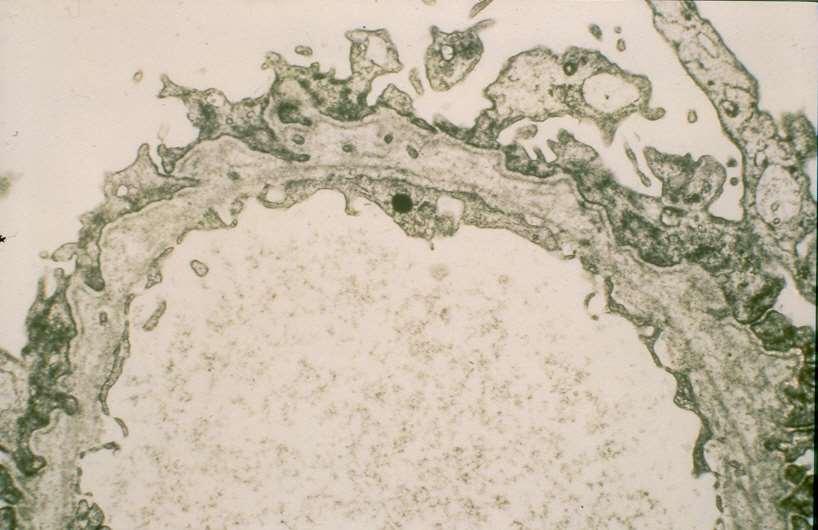
3 TRANSPLANT GLOMERULOPATHY Pathogenesis: consequence of chronic rejection; inverse relation with donor an recipient compatibility; repetitive episodes of endothelia injury Histology: endothelia and mesangial cell swelling; GBM reduplication; myointimal proliferation progressing to fibrosis leading to obliterative arteriopathy; IF- capillary wall lgm and C3; EMsubendothelial deposits, effacement of foot processes Clinical: onset of nephrotic syndrome ~ 9 mos (1-48 mos) post-tx; 2 year graft survival of 67%
4
5
6
7 TRANSPLANT GLOMERULOPATHY Pathogenesis: consequence of chronic rejection; inverse relation with donor an recipient compatibility; repetitive episodes of endothelia injury Histology: endothelia and mesangial cell swelling; GBM reduplication; myointimal proliferation progressing to fibrosis leading to obliterative arteriopathy; IF- capillary wall lgm and C3; EMsubendothelial deposits, effacement of foot processes Clinical: onset of nephrotic syndrome ~ 9 mos (1-48 mos) post-tx; 2 year graft survival of 67%
8 RECURRENCE OF DISEASE AFTER TRANSPLANTATION Mathew TM; Am J Kid Dis 12:85; Overall incidence of recurrent disease ~ 10-20% 2. Recurrent disease accounts for < 2% of graft loss 3. Most frequent cause of recurrent disease is recurrent GN 4. GN recurs in 6-9 % of transplanted patients
9 GLOMERULONEPHRITIS IN RENAL ALLOGRAFTS: RESULTS OF 18 YEARS OF TRANSPLANTATIONS Honkanen E et al; Clin Neph 21:210, 1984 Analyzed 1282 renal allograft recipients found 13 cases of allograft GN of which 4 were recurrent GN for a recurrence rate of < 1%
10 EVALUATION OF RECURRENT GLOMERULONEPHRITIS IN KIDNEY ALLOGRAFTS Morzy;cka M et al; Am J Med 72:588, 1982 In patients with glomerulonephritis as their original disease, they found a 17.9% recurrence rate of glomerular disease
11 GLOMERULAR LESIONS IN THE TRANSPLANTED KIDNEY IN CHILDREN Habib R et al; Am J Kid Dis 10:198, /436 patients 9% incidence of recurrent GN 40/120 patients 33% recurrence rate of glomerular disease in patients whose original disease was a glomerulopathy
12 PROBLEMS WITH INTERPRETATION OF DATA 1. Nature of recipient s original disease must be well documented 2. Indications for allograft biopsy usually based on an abnormality (renal dysfunction, abnormal U/A) 3. Recurrence -? Histological or clinical 4. Interpretation of biopsy differentiate recurrent changes from rejection or those already present in the grafted kidney
13 PATHOGENESIS OF RECURRENT DISEASE Nephritogenic factors: 1. Anti-GBM disease circulating anti-gbm Abs 2. Recurrent FSGS serum from patient injected into rats resulted in increased urinary protein excretion High recurrence rates in isografts and well-matched living related allografts
14 RECURRENT DISEASES OF THE ALLOGRAFT GLOMERULAR NON-GLOMERULAR PRIMARY FSGS Membranous Nephropathy MPGN I MPGN II lga Nephropathy Anti-GBM SECONDARY HSP HUS SLE DM Amyloidosis Wegener s Cryoglobulinemia (EMC) Monoclonal Gammopathy Oxalosis Fabry s Disease Cystinosis Sickle cell nephropathy Scleroderma Alport s Syndrome
15 RECURRENT FOCAL AND SEGMENTAL GLOMERULOSCLEROSIS Recurrence rate: 20% High risk group (recurrence rate of 50%) - diagnosis to ESRD < 3 years - younger patient (< 20 years of age) Once recurrence in the first graft, subsequent graft with ~ 75% rate of recurrence Histology: mesangial proliferation in the native kidney correlates with graft loss
16
17 RECURRENT FSGS Clinical most present with nephrotic range proteinuria; graft loss seen in 10-80% (highest in those with recurrence in earlier transplant); Treatment plasmapheresis, plasma exchange,mmf, high dose prograf Recommendations living related transplants are those at high risk for recurrence or those with prior history of recurrence; wait 1-2 years between transplants; counseling for LRD
18
19 RECURRENT MEMBRANOUS NEPHROPATHY Recurrence rate - ~3-7% (up to 57%); accounts for < 25% of post-transplant membranous nephropathy Clinical most present early post transplant with nephrotic range proteinuria; graft loss rare to 30% ( ± rejection); HLA-identical grafts at higher risk for recurrence Treatment no benefit with additional steroids
20
21
22
23 RECURRENT MEMBRANOUS NEPHROPATHY Recurrence rate - ~3-7% (up to 57%); accounts for < 25% of post-transplant membranous nephropathy Clinical most present early post transplant with nephrotic range proteinuria; graft loss rare to 30% ( ± rejection); HLA-identical grafts at higher risk for recurrence Treatment no benefit with additional steroids
24 RECURRENT MPGN TYPE I Recurrence rate - ~20-30% Histology- presence of subendothelial deposits and glomerular crescents may differentiate this from transplant glomerulopathy Clinical proteinuria, hematuria; serum C3 levels not helpful in diagnosis or prognosis; graft loss in 28-42% Treatment anti-platelet (ASA, dipyridamole), plasma exchange (?)
25

26
27 RECURRENT MPGN TYPE II Recurrence rate % Histology subendothelial dense deposits Clinical proteinuria, hematuria; graft loss 10-20%, up to 50% (risk factors male sex, RPGN, recurrent nephrotic syndrome) Treatment plasma exchange (?)
28
29
30 RECURRENT MPGN TYPE II Recurrence rate % Histology subendothelial dense deposits Clinical proteinuria, hematuria; graft loss 10-20%, up to 50% (risk factors male sex, RPGN, recurrent nephrotic syndrome) Treatment plasma exchange (?)
31 RECURRENT lga NEPHROPATHY Recurrence rate - ~50% (range 20-75%) Histology prominent mesangial lga staining Clinical hematuria, proteinuria; recurrence more common in LRA (83%)/HLA B35, DR4; lga rheumatoid factors may be elevated; graft loss is minimal (<10%)
32
33
34
35 RECURRENT ANTI-GBM NEPHRITIS Recurrence rate clinical recurrence (nephritis) ~25%; histologic recurrence ~50% Clinical hematuria/proteinuria; some will resolve spontaneously; graft loss is rare Recommendation: wait 6-12 months after loss of serum anti-gbm antibodies prior to transplantation
36
37 RECURRENT HENOCH-SCHOENLEIN PURPURA Recurrence rate clinical recurrence <10%; histologic recurrence (mesangial lga) ~30% Clinical hematuria/proteinuria ± purpura; those with recurrence of purpura and renal involvement had active disease within 8-18 mos of tx; graft loss may approach 40-75% if both renal and skin involved Recommendation wait at least 6-12 mos, up to 2 years after disappearance of purpura before tx
38 RECURRENT LUPUS NEPHRITIS Recurrence rate old view <1%; 5 cases documented; recent understanding 25% (Goral et al 2003) Clinical malar rash, Raynaud s, proteinuria (1-3gms), hematuria, pyuria; elevated anti-dna titers and depressed complement levels; graft loss none Treatment high dose steroids, chlorambucil, plasmapheresis Recommendation clinical and serologic quiescence prior to transplantation
39
40 RECURRENT HEMOLYTIC UREMIC SYNDROME HUS associated with viral infections, pregnancy, oral contraceptives, chemorx, CsA, malignant HTN, PSS< irradiation nephritis, severe acute vascular rejection, prograf Recurrence rate - ~25-50% Pathogenesis lack of plasma factors leading to endothelial prostacyclin synthesis; CsA effect on prostaglandin synthesis Histology microvascular thrombosis
41 RECURRENT HUS Clinical microangiopathis hemolytic anemia, thrombocytopenia, acute renal failure; graft loss 10-40% Treatment 1. Prophylactic low dose salicylate, dipyridamole 2. Acute plasma infusions, plasma exchange Recommendations avoid CsA, ALG and living related transplants
42
43
44 RECURRENT DIABETIC NEPHROPATHY Recurrence rate 100% Histology GBM thickening (2years); hyalinization of afferent and efferent arterioles (4 years); related to glycemic control (lesions not observed in renal/pancreas transplants) Clinical proteinuria; decline in renal function much faster than diabetic nephropathy in native kidneys
45
46
47 AMYLOIDOSIS 45 amyioid 45 control tx 3 yr pt survival 51% 79% 3 yr graft survival - including death 38% 45% - excluding death 53% 49% Pasternak et al Recurrence rate - ~20% (10%, 33%) Graft loss rate rare to 30%
48
49 WEGENER S GRANULOMATOSIS Few case reports Recurrence successfully treated by the use of cyclophosphamide and increase int eh steroid dose
50 I case report: WEGENER S GRANULOMATOSIS ESRD secondary to Wegener s; S/P CRA- one rejection treated with pulse steroids. One year post-tx CXR with nodular infiltrate; serum creatinine 200 to 750 μmol/l graft biopsy with focal and segmental GN with crescents (40%); ANCA 1:60 Treatment: methylprednisolone 500mg qd x 5 days (plum only); CsA added to Aza/pred x 3 weeks- no change; Switch aza to cyclophosphamide (1.5 mg/kg/d) reversed plum and renal impairment; continued on CsAcyclophos/pred; ANCA negative
51
52
53 ESSENTIAL MIXED CRYOGLOBULINEMIA Recurrence rate - ~50% Clinical renal (proteinuria, hematuria) and extrarenal (purpura, arthraigias) manifestations; cryoglobulins, rheumatoid factor and decreased C3 and C4 levels in the serum Recurrence may occur despite clinical and serologic quiescence; may lead to graft loss
54 MONOCLONAL GAMMOPATHY 1. Multiple myeloma may recur as plasmactic infiltration, tublar cast formation; fibrillar crescentic GN (graft loss) 2. Macroglobulinemic nephropathy one case report of recurrence of lgm and lambda light chain staining and diffuse mesangiocapillary changes (stable function) 3. Light chain deposition disease with or without serum nonoclonal proteins have recurred with or without effet on the allograft 4. Fibrillary GN 5.5 yrs post-tx with 17 gm proteinuria
55
56
57
58
59 OXALOSIS Inborn error in glyoxalate metabolism oxalate accumulation Recurrence rate 90% Clinical Sucdess more likely if: 1. Early tx GFR ~20 ml/min1.73 meter squared 2. Aggressive pre-op dialysis to deplete oxalate pool 3. Maintenance of high rates of urine flow; avoid allograft non-function and rejection 4. Simultaneous renal-liver transplant (enzyme replacement)

60
61
62 FABRY S DISEASE Inborn error of glycosphingolipid metabolism?? Transplanted kidney source of missing enzyme Experience disappointing; high patient mortality Dialysis preferred renal replacement therapy
63
64 CYSTINOSIS Inborn error in sulfur metabolism cystine accumulation Recurrence rate - ~10% Clinical minimal impairment in graft function; continued systemic manifestations; preferred mode of treatment of ESRD in children
65
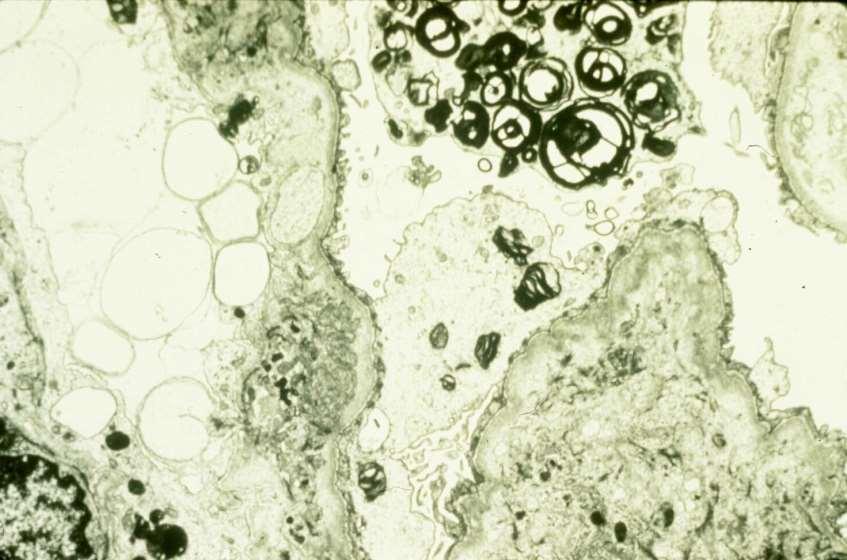
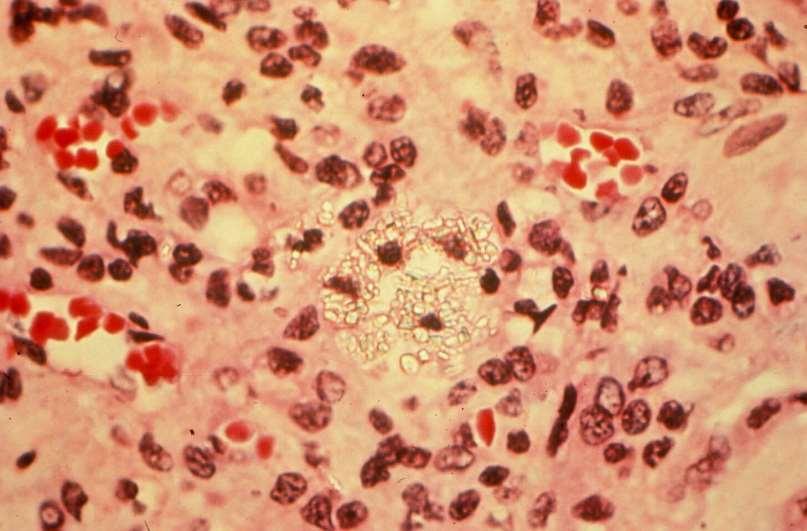
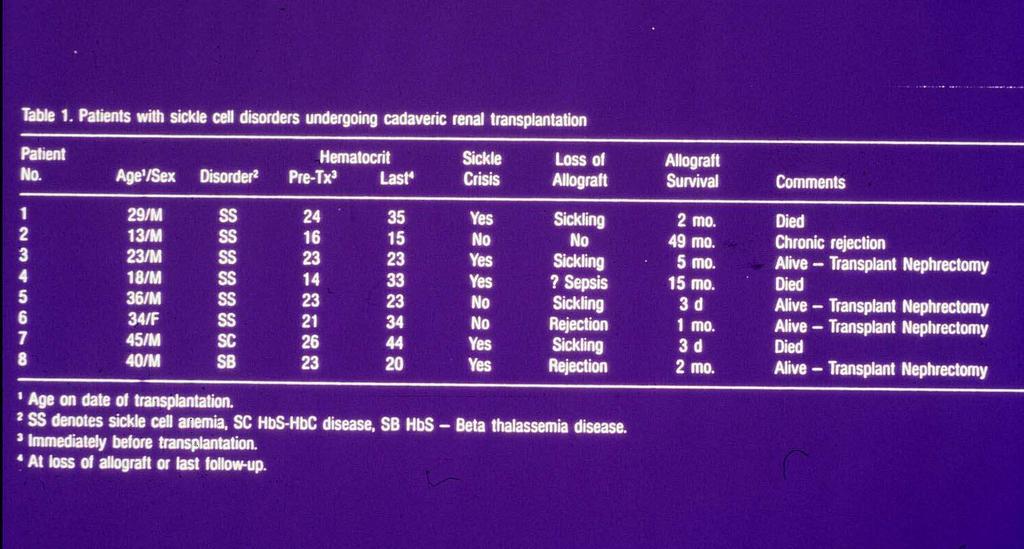
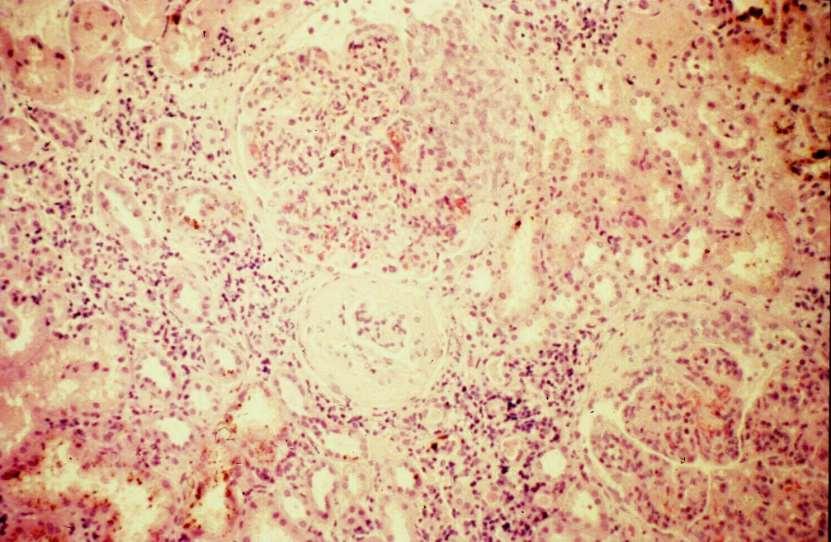
66 SICKLE CELL NEPHROPATHY University of Alabama experience disappointing with most graft loss to sickling and rejection Cumulative data (other centers) 80% 1 year graft survival Recurrence of SC nephropathy rare; one case report of prominent hemosiderosis with chronic ischemic damage, interstitial fibrosis, tubular atrophy
67
68
69 PROGRESSIVE SYSTEMIC SCLEROSIS 1. Patients who do well with dialysis or transplantation have had bilateral native nephrectomies (to control HTN) 2. Patients with recurrence (2 reports in literature) had a malignant course with onset of PSS to transplantation <1 year; anti-nuclear antibodies eluted from graft 3. Recommendation delay transplantation until clinically stable and without visceral PSS activity
70
71
72
73 ALPORT S SYNDROME Recurrence rare, only one reported case Clinical patients are at small risk to develop anti- GBM nephritis due to exposure to normal GBM antigens present in the allograft (lack a domain of type IV collagen) May have serum anti-gbm Abs, abnormal U/A, linear lgg staining, GN; crescentic GN associated with graft loss
74 CONCLUSION THE TRANSPLANTED KIDNEY IS NOT IMMUNE FROM DE NOVO OR RECURRENT RENAL DISEASE THE MAGNITUDE OF THE PROBLEM IS STILL UNDER STUDY A REGISTRY IS NOW IN PLACE TO AIDE IN OUR UNDERSTANDING
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Many patients receiving renal allografts become identified simply
 Recurrent Disease in the Transplanted Kidney Jeremy B. Levy Many patients receiving renal allografts become identified simply as recipients of kidney transplantation. All subsequent events involving changes
Recurrent Disease in the Transplanted Kidney Jeremy B. Levy Many patients receiving renal allografts become identified simply as recipients of kidney transplantation. All subsequent events involving changes
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Recurrent Diseases in the Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Recurrent Diseases in the Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History of nephrotic
Recurrent Diseases in the Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History of nephrotic
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Glomerular Diseases. Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology
 Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
Glomerular Diseases Davis Massey, MD, PhD Surgical Pathology Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Chapter 8: ESRD Among Children, Adolescents, and Young Adults
 Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Recurrent Diseases After Transplantation. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Recurrent Diseases After Transplantation Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History
Recurrent Diseases After Transplantation Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Glomerular Disease. January 16, Katharine Dahl, MD
 Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Glomerular Disease January 16, 2018 Katharine Dahl, MD kdahl@akdhc.com Glomerular Disease Nomenclature Diffuse >50% glomeruli ---- Focal
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
NEPHROTIC SYNDROME. Presents with the classic tetrad of nephrotic syndrome. Massive proteinuria (>3. 5 g/d) Hypoalbuminemia Edema Hyperlipidemia
 Hypoalbuminemia Edema Hyperlipidemia") PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
PATHOLOGY OF GLOMERULAR DISEASES Disease Etiology Pathophysiology and Clinical Presentation Urinalysis in Nephrotic Syndrome NML excretion: 150 mg/d : < 0.15 g total protein/g urine creatinine Nephrosis
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The renal biopsy is a powerful tool in the diagnostic evaluation of allograft dysfunction
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The renal biopsy is a powerful tool in the diagnostic evaluation of allograft dysfunction
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER
: 30 YEARS LATER") HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
HIV ASSOCIATED NEPHROPATHIES (HIVAN): 30 YEARS LATER Gaston Zilleruelo M.D. Professor of Pediatrics Director of Pediatric Nephrology University of Miami/Holtz Children s Hospital Worldwide 33.2 million
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
CHAPTER 3. Secondary Glomerulonephritis
 2nd Report of the Malaysian Registry of Renal Biopsy 2008 SECONDARY GLOMERULONEPHRITIS CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 41 SECONDARY GLOMERULONEPHRITIS 2nd Report
2nd Report of the Malaysian Registry of Renal Biopsy 2008 SECONDARY GLOMERULONEPHRITIS CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 41 SECONDARY GLOMERULONEPHRITIS 2nd Report
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Objectives. Glomerular Diseases. Glomerulonephritis. Microscopic Hematuria 11/6/2016. Discuss diagnosis of glomerular diseases
 Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
Glomerular Diseases in Primary Care Sadiq Ahmed, MD, FACP, FASN Associate Professor of Medicine Division of Nephrology Bone & Mineral Metabolism University of Kentucky Objectives Discuss diagnosis of glomerular
CKD in Other Organ Transplants
 CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS
 CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
CHAPTER 3. Secondary Glomerulonephritis
 CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 59 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to the MRRB from the year 2005-2010.
CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 59 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to the MRRB from the year 2005-2010.
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
1. SIGNIFICANCE 2. PREREQUISITES
 Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
Topic 13: Differential diagnosis of glomerulonephritis in children. Differential approach to treatment of glomerulonephritis in children. Thematic chapter: Differential diagnosis of the most common diseases
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND 2015
 Scottish Renal Registry Report SECTION N SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND All centres in Scotland were able to provide date of birth, sex (except centre), indication
Scottish Renal Registry Report SECTION N SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND All centres in Scotland were able to provide date of birth, sex (except centre), indication
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
RaDaR Inclusion and Exclusion Criteria
 Cohort Inclusion Criteria Exclusion Criteria Adenine Phosphoribosyltransferase Deficiency (APRT-D) APRT Deficiency APRT Deficiency confirmed Abolished APRT enzyme activity or confirmed disease-causing
Cohort Inclusion Criteria Exclusion Criteria Adenine Phosphoribosyltransferase Deficiency (APRT-D) APRT Deficiency APRT Deficiency confirmed Abolished APRT enzyme activity or confirmed disease-causing
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
NEPHRITIC SYNDROME. By Dr Mai inbiek
 NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
NEPHRITIC SYNDROME By Dr Mai inbiek Nephritic Syndrome The nephritic Syndrome is a clinical complex, usually of acute onset. Is caused by inflammatory lesions of glomeruli. Characterized by; 1) Hematuria
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney