만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
|
|
|
- Ilene Rogers
- 5 years ago
- Views:
Transcription
1 만성콩팥병환자에서의혈압관리 분당서울대병원신장내과 안신영
2 Contents Introduction Lifestyle and Pharmacological Tx CKD ND ptswithout diabetes CKD ND ptswith diabetes In elderly ptswith CKD ND 2013 대한고혈압학회진료지침 JNC 8th
 and hypertension (HTN) Strong")
 Each can cause and")
3 Introduction Chronic kidney disease (CKD) and hypertension (HTN) Strong association btw CKD and high blood pressure (BP) Each can cause and aggravate the other



4 Introduction BP control in CKD patients Fundamental to the care of patients with CKD Slow progression to ESRD Reduce cardiovascular morbidity and mortality
5 KDIGO 2012 guideline The 2012 KDIGO clinical practice guideline aims to provide guidance on BP management and treatment for all non-dialysisdependent CKD patients and kidney transplant recipients. Populations of interest Adults with CKD ND (non-dialysis-dependent) without diabetes Adults with CKD ND with diabetes Adults with CKD ND who have received a kidney transplant Children with CKD ND Elderly with CKD ND


6 Relationship among categories for albuminuria and proteinuria
7 Introduction The strength of recommendation Level 1 ( We recommend ) Most patients should receive the recommended course of action Level 2 ( We suggest ) Different choices will be appropriate for different patients Each patient needs help to arrive at a management decision consistent with her or his values and preferences Not Graded Typically to provide guidance based on common sense or where the topic dose not allow adequate application of evidence


8 Introduction The quality of the supporting evidence
9 - Lifestyle and pharmacological treatment General strategies (not graded) 환자의나이, 동반질환, 만성신부전진행의가능성등을고려하여 혈압의목표를개별화하고적절한약제를선택한다. 주기적으로기립성어지럼증등의증상및저혈압발생여부에대해서평가한다. 고령, 자율신경기능장애를동반한당뇨환자의경우기립성저혈압의고위험군


10 - Lifestyle and pharmacological treatment 생활습관개선 건강체중유지 = BMI (1D) 저염식이 : < 2 g/day of Na or < 5 g/day of NaCl (1C)
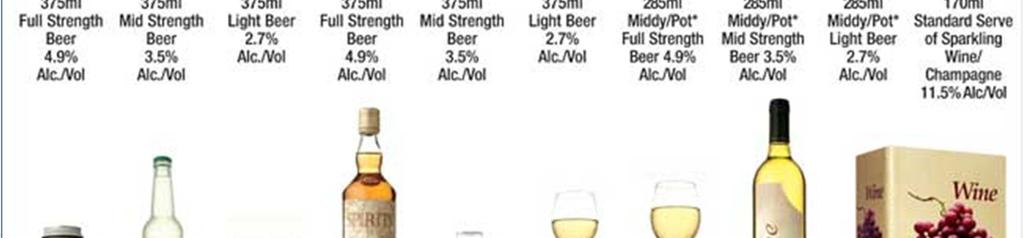
11 - Lifestyle and pharmacological treatment 생활습관개선 : 운동 : 30 minutes & 5 times/week (1D) 음주 : 남성 < 2 standard drinks/day, 여성 < 1 standard drinks/day (2D) Standard drinks : g of alcohol (in different countries) 10g of alcohol = 100ml of wine, 285ml of full strength beer, 425ml of light beer


12
13 - Lifestyle and pharmacological treatment 고혈압약제 RAAS blockers : ACEi or ARB 적응증 : CKD with urinary albumin excretion 주의사항 : hyperkalemia, decreased GFR Risk factors - Renal atery stenosis - Volume depletion - NSAIDs or COX-2 inhibitor 등과병행사용
14 Case - F/65, DM for 10yrs - 24h urine protein 535 mg/day, BP : 140/90 mmhg, scr 1.0 mg/dl - Start ARB scr 1.3 mg/dl(2wks later) -?? ARB exerts desired action (intraglomerular pr ) Accept 20-30% increase in scr within 2wks of initiation Repeat scr 2-4 wks Stabilization : continue scr > 30% : dose by 50% & exclude hypovolemia, NSAIDs scr > 50% : stop ARB or ACEi & study of renal artery stenosis
15 - Lifestyle and pharmacological treatment Diruetics 만성콩팥병환자에서혈압상승의주된요인 : salt and water retention Thiazide Since 1950s Salt and water excretion 부종이있는 CKD 환자에서 1 or 2 번째항고혈압약제로많이사용 ACEior ARB 와함께처방 : hyperkalemia 의위험을낮춤 Loop diuretics Thiazide 보다는 short-term 으로사용 CKD stage 4-5 환자에서부종조절시 thiazide 보다많이사용
16 - Lifestyle and pharmacological treatment Beta blockers In CKD : Accumulation of beta-blockers or active metabolites exacerbate concentration-dependent side effects : bradycardia ex) atenolol, bisoprolol (not carvedilol, propranolol, metoprolol) 적응증 CKD with heart failure : endorsed usage of beta-blocker CKD without heart failure : no evidence on direct efficacy to mortality
17 - Lifestyle and pharmacological treatment Calcium channel blocker 3 subclasses Dihydropyridines - amlodipine, nifedipine, lercanidipine : more selective for vascular smooth muscle (vasodilatation) Non-dihydropyridine benzothiazepines diltiazem Phenylalkylamines verapamil Do not acculmate in patients with impaired kidney functions Exception of nicardipine and nimodipine in elderly patients with CKD
18 - Lifestyle and pharmacological treatment Calcium channel blocker 적응증 Widely used in HTN, angina, supra-ventricular tachycardia Consideration Dihydropyridine : urinary albumin excretion 증가된환자에서사용하지않도록 Non-dihydropyridines ( 특히 ACEi/ARB 같이쓰지않는경우 ) beta-blocker (atenolol or bisoprolol 등 ) 과같이사용할경우 bradycardia 에주의 신장이식을받은환자에서 CNI, sirolimus 의 blood level 을높일수있으므로주의가 필요함
19 - In CKD ND patients without diabetes Urine albumin excretion < 30 mg/day (protein excretion < 150 mg/day) Office BP > 140 mmhg systolic or > 90 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 140/90 mmhg (1B) Rationale High BP is a risk factor for CVD and development and progression of CKD Lowering BP in the general population reduces cardiovascular risk Lowering BP in CKD patients reduces the rate of CKD progression CKD is a major risk factor for CVD
20 - In CKD ND patients without diabetes Urine albumin excretion 30~300 mg/day (protein excretion 150~500 mg/day) Office BP > 130 mmhg systolic or > 80 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 130/80 mmhg (2D) ARB or ACEi(2D) Urine albumin excretion > 300 mg/day (protein excretion > 500 mg/day) Office BP > 130 mmhg systolic or > 80 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 130/80 mmhg (2C) ARB or ACEi(1B)
21 - In CKD ND patients without diabetes Rationale Microalbuminuriaand macroalbuminuria are major risk factors for CVD and CKD progression RCTs suggest that a BP 130/80 mmhg may reduce progression of CKD in patients with albuminuria
22 -In CKD ND patients with diabetes Urine albumin excretion < 30 mg/day (protein excretion < 150 mg/day) Office BP > 140 mmhg systolic or > 90 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 140/90 mmhg (1B) Rationale RCTs and observational studies have been consistent in suggesting that lowering BP so that it is consistently < 140/90 mmhg will prevent major cardiovascular events. Lowering BP to these levels is also likely to reduce the risk of progressive CKD The evidence for the benefit of further lowering of the BP target is mixed
23 -In CKD ND patients with diabetes Urine albumin excretion > 30 mg/day (protein excretion > 150 mg/day) Office BP > 130 mmhg systolic or > 80 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 130/80 mmhg (2D) Rationale Observational studies :The level of urine albumin predicts the risk of adverse cardiovascular and kidney outcomes BP lowering reduces the rate of urinary albumin excretion, which may lead to a reduced risk of both kidney and cardiovascular events ARB or ACEi(2D)
24 -In CKD ND patients with diabetes Urine albumin excretion > 300 mg/day Office BP > 130 mmhg systolic or > 80 mmhg diastolic Treated with BP-lowering drugs to maintain a BP 130/80 mmhg ARB or ACEi(1B)
25 -In elderly patients with CKD ND Elderly : 65 years of age Tailor BP treatment considering age, co-morbidities and other therapies, with gradual escalation of treatment Close attention to adverse events related to BP treatment, including electrolyte disorders, acute deterioration in kidney function, orthostatic hypotension and drug side effects (Not Graded)
26 2013 대한고혈압학회진료지침 만성콩팥병과고혈압 혈압조절의목표는당뇨병의동반여부와무관함 목표혈압 알부민뇨없는만성콩팥병 : < 140/90 mmhg 알부빈뇨동반시 : < 130/80 mmhg 알부민뇨가동반되었을때 : 우선적으로 ACEi/ARB 제재를사용
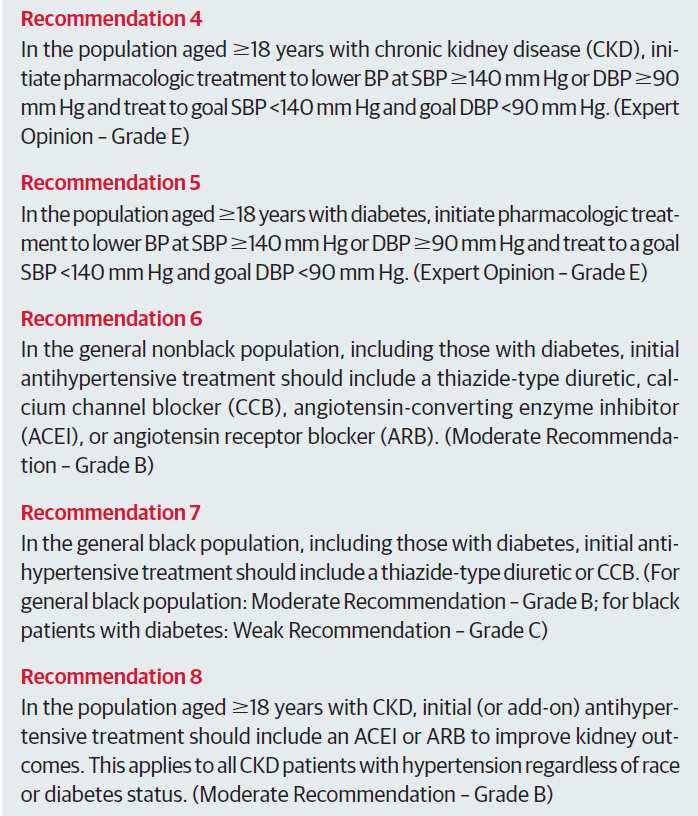
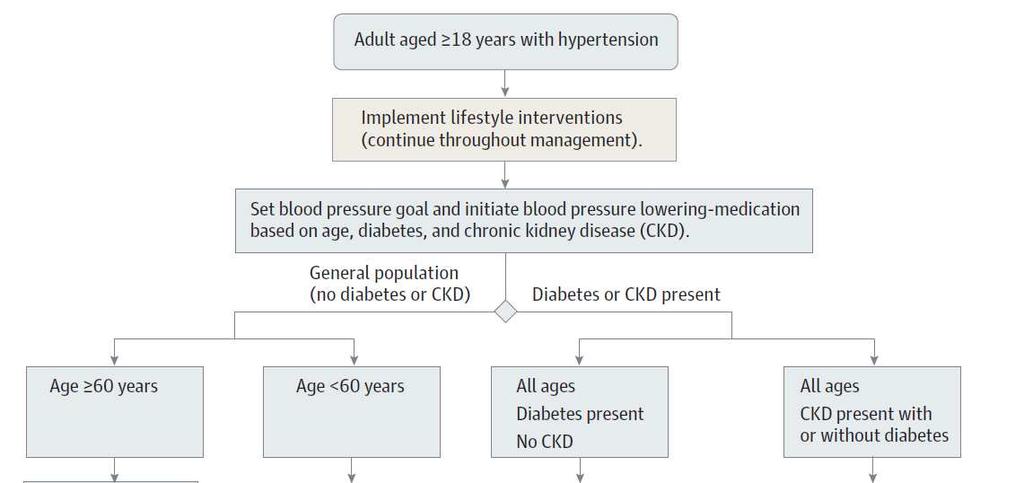
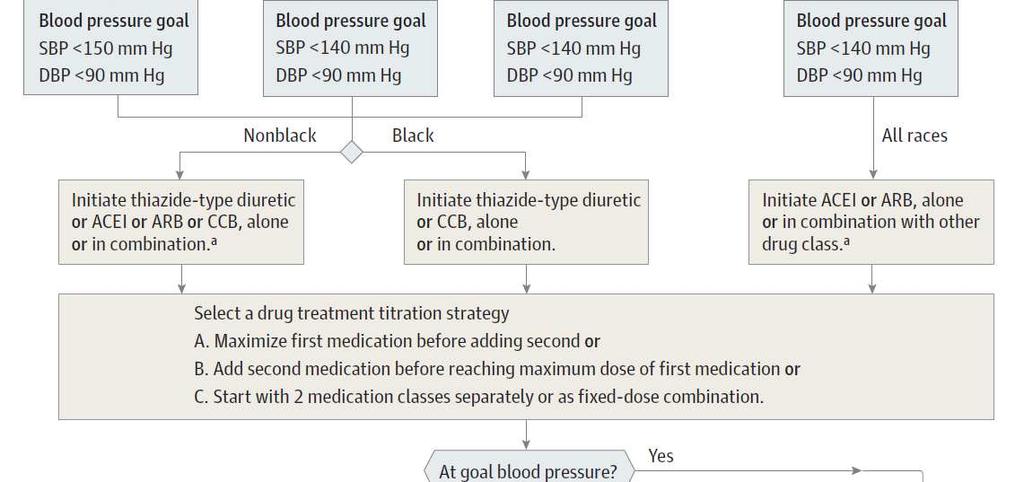
27 JNC 8th
28
29 Summary Albuminuria A1 (UACR <30mg/g) A2 (UACR mg/g) A3 (UACR > 300 mg/g) Non diabetes 140/90 (1B) 130/80 (2D) 130/80 (2C) Diabetes 140/90 (1B) 130/80 (2D) 130/80 (2D) Elderly Tailor BP treatment (Not Graded) CKD ND and urine albumin excretion mg/day : ARB or ACEi (2D) CKD ND and urine albumin excretion > 300 mg/day : ARB or ACEi (1B)
30 감사합니다.
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
4/3/2018 PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES
 PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES To identify Blood pressure (BP) medications which are used to manage
PHARMACOLOGICAL MANAGEMENT OF HYPERTENSION IN THE PATIENT WITH CKD TONI A. HARPS, APRN-CNS, MSN NEPHROLOGY WHY THIS TOPIC/OBJECTIVES To identify Blood pressure (BP) medications which are used to manage
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
HypertensionTreatment Guidelines. Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC
 HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
HypertensionTreatment Guidelines Michaelene Urban APRN, MSN, ACNS-BC, ANP-BC Objectives: Review the definition of the different stages of HTN. Review the current guidelines for treatment of HTN. Provided
What in the World is Functional Medicine?
 What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
What in the World is Functional Medicine? An Introduction to a Systems Based Approach of Chronic Disease Meneah R Haworth, FNP-C Disclosure v I am a student of the Institute for Functional Medicine. They
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Network Hypertension Algorithm
 Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Network Hypertension Algorithm Content Review and Approval: This document is subject to review, revision, and (re)approval by the Clinical Integration and Oversight Committee (CIOC) annually and following
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Antihypertensives. Diagnostic category
 Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Measurement of blood pressure At first assessment, take both arms then choose the one with the higher reading. Beware of orthostatic hypotension. Measure BP in sitting position, and repeat after patient
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
β adrenergic blockade, a renal perspective Prof S O McLigeyo
 β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
β adrenergic blockade, a renal perspective Prof S O McLigeyo Carvedilol Third generation β blocker (both β 1 and β 2 ) Possesses α 1 adrenergic blocking properties. β: α blocking ratio 7:1 to 3:1 Antioxidant
ACEIs / ARBs NDHP dihydropyridine ( DHP ) ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )
 ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )") 005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Byvalson. (nebivolol, valsartan) New Product Slideshow
 New Product Slideshow") Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
Byvalson (nebivolol, valsartan) New Product Slideshow Introduction Brand name: Byvalson Generic name: Nebivolol, valsartan Pharmacological class: Beta-blocker + angiotensin II receptor blocker (ARB) Strength
ANTI- HYPERTENSIVE AGENTS
 CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
CLINICAL ANTI- HYPERTENSIVE AGENTS Jacqueline van Schoor, MPharm, BSc (Hons) Amayeza Info Centre Hypertension represents a major public health concern. It affects about a billion people worldwide and is
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Dr Narender Goel MD (Internal Medicine and Nephrology) Financial Disclosure: None, Conflict of Interest: None
 Financial Disclosure: None, Conflict of Interest: None") Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Dr Narender Goel MD (Internal Medicine and Nephrology) drnarendergoel@gmail.com Financial Disclosure: None, Conflict of Interest: None 12 th December 2013, New York Visit us at: http://kidneyscience.info/
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Antihypertensive drugs SUMMARY Made by: Lama Shatat
 Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Antihypertensive drugs SUMMARY Made by: Lama Shatat Diuretic Thiazide diuretics The loop diuretics Potassium-sparing Diuretics *Hydrochlorothiazide *Chlorthalidone *Furosemide *Torsemide *Bumetanide Aldosterone
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Cardiovascular Pharmacotherapy in Special Population: Cardio-Nephrology
 49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
49 th Annual Scientific Meeting The Heart Association of Thailand under the Royal Patronage of H.M. the King Cardiology on the move 24-25 March 2017 @Sheraton, HuaHin Cardiovascular Pharmacotherapy in
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Combining Antihypertensives in People with Diabetes
 Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Combining ntihypertensives in People with Diabetes The majority of people with diabetes will develop hypertension and this subsequently increases the risk of microvascular and macrovascular complications.
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Chapter 7: Blood pressure management in elderly persons with CKD ND Kidney International Supplements (2012) 2, ; doi: /kisup.2012.
 2, ; doi: /kisup.2012.") http://www.kidney-international.org chapter 7 & 2012 KDIGO Chapter 7: Blood pressure management in elderly persons with CKD ND Kidney International Supplements (2012) 2, 377 381; doi:10.1038/kisup.2012.57
http://www.kidney-international.org chapter 7 & 2012 KDIGO Chapter 7: Blood pressure management in elderly persons with CKD ND Kidney International Supplements (2012) 2, 377 381; doi:10.1038/kisup.2012.57
Prof. Ramzy H. El Mawardy. Cairo Egypt 2009
 Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
Prof. Ramzy H. El Mawardy Ain Shams University Cairo Egypt 2009 Burden of HRN is increasing worldwide = 7 billion individuals. BP control is still poor = 60.70%. Global risk assessment is essential in
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
Section 3, Lecture 2
 59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
59-291 Section 3, Lecture 2 Diuretics: -increase in Na + excretion (naturesis) Thiazide and Related diuretics -decreased PVR due to decreases muscle contraction -an economical and effective treatment -protect
Outpatient Management of Chronic Kidney Disease for the Internist
 Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
Outpatient Management of Chronic Kidney Disease for the Internist Annual Meeting of Maryland Chapter of the American College of Physicians February 3, 2018 MARY (TESSIE) BEHRENS, MD, FACP, FASN, FNKF MID-ATLANTIC
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Diabetes in Renal Patients. Contents. Understanding Diabetic Nephropathy
 Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Diabetes in Renal Patients Contents Understanding Diabetic Nephropathy What effect does CKD have on a patient s diabetic control? Diabetic Drugs in CKD and Dialysis Patients Hyper and Hypoglycaemia in
Antihypertensives. Antihypertensive Classes. RAAS Inhibitors. Renin-Angiotensin Cascade. Angiotensin Receptors. Approaches to Hypertension Treatment
 Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
Approaches to Hypertension Treatment Antihypertensives Inhibit Sympathetic impulses Inhibit contractility Inhibit heart rate Inhibit vasoconstriction Inhibit smooth muscle function Inhibit RAAS Inhibit
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP
 HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
HYPERTENSION IN EMERGENCY MEDICINE Michael Jay Bresler, M.D., FACEP What is normal blood pressure? Prehypertension 130-139/80-90 Compared with normal BP Double the risk for developing hypertension. Lifestyle
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Long-Term Care Updates
 Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Long-Term Care Updates January 2016 By Yunuo (Enora) Wu, PharmD Chronic kidney disease (CKD) is defined as kidney damage (including structural or functional abnormalities) or glomerular filtration rate
Applying clinical guidelines treating and managing CKD
 Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Applying clinical guidelines treating and managing CKD Develop patient treatment plan according to level of severity. Source: Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Hypertension Management - Summary
 Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Who should have blood pressure assessed? Hypertension Management - Summary All patients over the age of 40 years, every 1-3 years in order to determine their cardiovascular risk (ie. Framingham Risk Score)
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Treatment of Hypertension
 This Clinical Resource gives subscribers additional insight related to the Recommendations published in January 2018 ~ Resource #340101 Treatment of Hypertension In 2013, the JNC 8 panel released recommendations
This Clinical Resource gives subscribers additional insight related to the Recommendations published in January 2018 ~ Resource #340101 Treatment of Hypertension In 2013, the JNC 8 panel released recommendations
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Antihypertensive drugs: I. Thiazide and other diuretics:
 Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
Clinical assessment of hypertensive patient: You have to take history regarding the presence of other risk factors for CAb like diabetes mellitus, smoking, etc. Take history whether the patient takes medications
2014 HYPERTENSION GUIDELINES
 2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
2014 HYPERTENSION GUIDELINES Eileen M. Twomey, Pharm.D., BCPS 1 Learning Objectives Describe specific blood pressure thresholds at which antihypertensive therapy should be initiated and blood pressure
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Dr (Prof.) N P Singh
 N P Singh") Dr (Prof.) N P Singh MD, FAMS, FACP, FRCP Edin, MBA, FISN, FICP Former-Director Prof. Medicine, MAMC, Delhi Medical Advisor Director, Medicine & Allied Specialities Senior Consultant in Internal Medicine
Dr (Prof.) N P Singh MD, FAMS, FACP, FRCP Edin, MBA, FISN, FICP Former-Director Prof. Medicine, MAMC, Delhi Medical Advisor Director, Medicine & Allied Specialities Senior Consultant in Internal Medicine
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic