Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense
|
|
|
- Carol Adams
- 5 years ago
- Views:
Transcription
1 Polypharmacy: A Rational Evidence-informed Approach with a Touch of Common Sense KEEP CALM BECAUSE LESS IS MORE James McCormack B.Sc. (Pharm), Pharm.D. Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC therapeuticseducation.org Get handout here -

2 WHY!!
3 We all need to do a better job when it comes to medications
4 POLYPHARMACY does NOT= >5 meds It means taking medications/supplements which For symptoms For prevention are not providing a complete or clinically important effect or are given at doses larger than is required to achieve that effect if one was fully informed by the best available evidence about benefits and harms one would not take them


5 BOTH COULD BE POLYPHARMACY

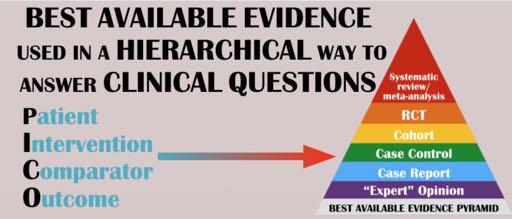
6 MY BELIEF All Health Care Providers should have their practice underpinned by the best available evidence Evidence-Based Practice (EBP)


7

8


9

10 Combine Evidence with Common Sense So rare that it s a super SHHH. MY COMMON power SENSE IS TINGLING. Common Sense So rare that it s a superpower
11 Three Approaches Dose issues Symptom issues Prevention issues
12 This simple concept can eliminate most medication problems USE VERY LOW DOSES



13 The doses in these books are all WRONG for individual patients

14 Everyone is a genetic mongrel
15 It s a dose thing more than 80% of ADRs causing admission or occurring in hospital... are dose related, an accentuation of the known pharmacological effect of the drug, and thus predictable and potentially avoidable Br J Clin Pharmacol 2004; 57:121 6

16 Unless the condition is severe or lifethreatening, drug treatment can be started at a very low dose (half or one-quarter the recommended starting dose) CMAJ DOI: /cmaj Most of the effect of a medication comes from the low starting doses AND doubling a dose never doubles the effect - in fact it sometimes has no additional effect
17 A sample of Low-Dose RCT Evidence 6.25 mg hydrochlorothiazide first marketed at 50 to 200 mg daily 6.25 mg captopril 25 mg PO TID is still a commonly recommended initial starting dose for hypertension 25 mg sildenafil (Viagra) effective dose for erectile dysfunction 25 mg sumatriptan (Imitrex) works as well as100 mg 5 mg daily fluoxetine (Prozac) similar effects to those seen at 20 mg and 40 mg daily 0.25 mg ezetimibe (Ezetrol) 1/40th of the recommended initial starting dose provides 50% of the LDL lowering effect 15 mg elemental iron daily as effective for anemia in elderly as 50 mg and 150 mg with a lower incidence of side effects 150 mg daily bupropion (Zyban) 0.5 mg BID varenicline (Champix) produces the same rate of smoking cessation at one year as 300 mg daily (1.0 mg BID) 10 mg atorvastatin produces 2/3 of the effect on cholesterol as that seen with an 80 mg (8-fold increase) dose 200 mg ibuprofen (Motrin) as effective as 400 mg for migraine headache 25 mg ranitidine (Zantac) as effective as 125 mg for heartburn relief 1.8 mg colchicine as effective as 4.8mg for acute gout with less adverse events

18 Doxepin (Sinequan) Depression - start mg - optimal 75mg -150mg up to 300mg The results support the effectiveness of low doses (25-50 mg) of doxepin to improve sleep Efficacy and Safety of Three Different Doses of Doxepin in Adults with Primary Insomnia All three doses worked better than placebo AND NO side effects over placebo J Clin Psychiatry 2001;62: Sleep 2007; 30: A recommended low dose was still times TOO HIGH
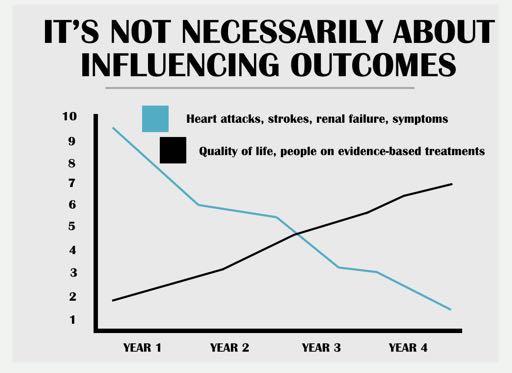
19 Approaches differ depending on outcome Every patient is an experiment - dose and effect SYMPTOMS - we can usually figure out if it is working - but it is tricky PREVENTION - one will never know if it worked Expectations

20 Symptoms
21 You primarily need to know IF it works and DID it work Safety, cost and convenience Older medications first - safety Head-to-head studies are uncommon Doses in the CPS are wrong N-of-1 studies Let the patient tell you
22 Symptom NNTs PPIs, sildenafil - NNT ~2 NSAIDs, opioids - pain NNT ~3-5 Antidepressants - severe depression - NNT ~10 Ipratropium - asthma attack - NNT ~11 Cholinesterase inhibitors - ADAS-Cog >4 - NNT ~10 Sleeping pills - improvement in sleep quality - NNT ~13 Steroids - sore throat - NNT ~3, Bell s palsy - NNT ~10 Antibiotics - acute COPD exacerbation - NNT ~5 Topical antibiotics - bacterial conjunctivitis - NNT ~7
23 But you need to know what goes on in the placebo group Response in the placebo group If a person has responded, what is the % chance it was the medication RCT Benefit 10% - NNT 10 RCT Benefit 20% - NNT 5 0% ~100% ~100% 10% ~50% ~66% 20% ~33% ~50% 30% ~25% ~40% 40% ~20% ~33%
24 The Placebo Group Effect not the placebo effect and these are ballpark numbers ~0% - general anesthesia ~5% - psychosis ~10% - sildenafil, OCD ~20% - Alzheimer s meds, acetaminophen for headaches, side effects ~25% - menopausal symptoms, migraine (frequency/severity) ~30% - blood pressure goal, depression, anxiety, PTSD, PPIs/H2RA, sore throat, NSAIDs of OA, inhalers for COPD ~40% - panic disorders
25 When a medication has worked, if you were a betting person you would bet that it probably wasn't because the medication worked.
26 KEEP CALM AND TAPER ON

27 Cut tablets/t he dose in half It s not as scary as you think...or is it?
28 Tapering Antidepressants Taper - approximately 25% will have a recurrence of depression over 18 months Leave them on - approximately 10% will have a recurrence of depression 15% will be harmed and 85% will benefit because they are on medications apparently unnecessarily
29 Rebound after PPI withdrawal in healthy people 120 healthy volunteers 12 weeks of placebo or 8 weeks of esomeprazole 40 mg daily and then 4 weeks of placebo Reporting dyspepsia, heartburn or acid regurg during weeks 9-12 Placebo ~ 5% PPI ~ 20% Gastroenterology 2009;137:80-7
30 PPI withdrawal in asymptomatic GERD patients 71 patients - tried to titrate dose down over 3-6 months 42% still on PPI - median reinstitution time 14 days 34% ended up on H2RA 7% on prokinetic agent 1% on both 16% no-drugs Gastroenterology 2001;121: patients on lansoprazole 30mg BID 50% ended up on rabeprazole 20mg daily 10% off all drugs 56% with erosive esophagitis failed 31% of those with endoscopic-negative failed Aliment Pharmacol Ther 2007;25:709 71

31 July 4, 2013 Withdrawal of antipsychotics - for every 4 people, you prevent 1 death and 1 study suggests that 1 in 4 will have a relapse of neuropsychiatric symptoms Antipsychotics also worsen cognition
32 Donepezil withdrawal 295 Community dwelling patients on donepezil (most >2 yrs) mean age 77, mean MMSE 9, followed 1 yr. Stopping of med worsened MSE by 1.9 pts Less effect (1.3) if severe dementia (<9 MSE) Don t give number attaining MCID (1.4) Withdrawal from study more if stopped! Death: no difference N Engl J Med 2012;366:
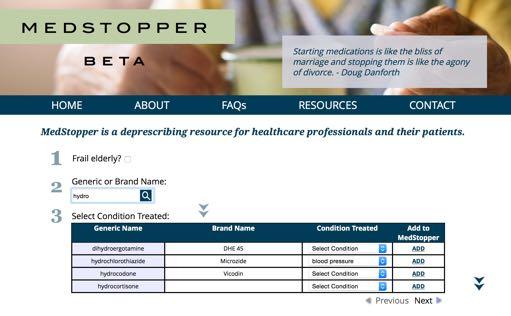
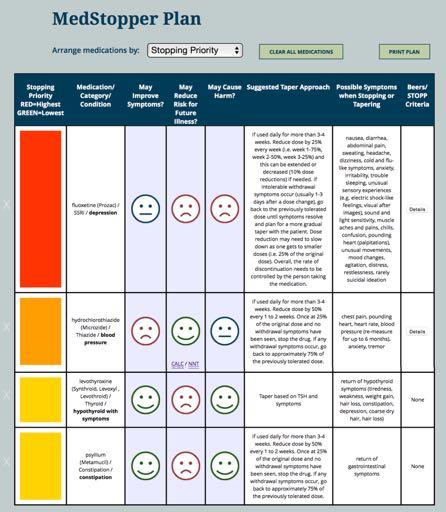
33 MEDSTOPPER medstopper.com
34 Symptom meds PPIs, NSAIDs etc Typically one should reduce the dose slowly - cut the dose in half or do something similar - change interval The dose likely wasn t right in the first place Put the onus on, and give the power to, the patient to find the right dose



35 Prevention

36 Unfortunately, depending on how their reliability is measured, up to 50% of guidelines can be considered untrustworthy. This carries serious consequences for patients safety, resource use and health economics burden. EBM 2017;22:1-3
37 Qualitative study using semi-structured interviews Many of the preferences expressed by the clinicians and lay people in this study are at odds with recommendations in guidelines BMJ 2003;327:841

38 cvdcalculator.com 1.Calculate ballpark 10-yr risk of CVD - BP, chol, diabetes 2.Make estimate of benefit based on the best available evidence 3.Gives a list of adverse effects to discuss


39 1. Calculate ballpark annual risk of stroke - based on risk factors- BP, chol, diabetes 2. Make estimate of benefit based on the best available evidence - all agents 3. Make estimate of a GI bleed
40 Optimal management of elderly pts with vascular disease (DEBATE) RCT, f/u 3.4 years 400 patients - avg age 80, all CVD Usual care (primary care) or specialized care Evidence-Based European CPG for chronic CVD it was possible and safe to institute evidence-based cardiovascular treatments and improve risk factors in patients 75 years or older in a pragmatic setting. Am Heart J 2006;152:585-92
 MEDS: ACE (+30%) & statin (+50%) ACTUAL BENEFIT - NONE IN BOTH GROUPS Mortality 18% Stroke 6% MI/coronary death 16% PREDICTED BENEFIT UKPDS risk")
41 Outcome Systolic BP: 7.8 mmhg lower Diastolic BP: 3.9 mmhg lower Glucose: 0.55 mmol/l lower Cholesterol: 0.78 mmol/l lower LDL: 0.73 mmol/l lower (45% to target) MEDS: ACE (+30%) & statin (+50%) ACTUAL BENEFIT - NONE IN BOTH GROUPS Mortality 18% Stroke 6% MI/coronary death 16% PREDICTED BENEFIT UKPDS risk engine 18% CVD risk reduced to14% NNT = 25 NNT = infinite
42 Treatment of Hypertension in Patients 80 Years of Age or Older Patients 3,845 patients with a SBP > 160 mm Hg, TC 5.3 mmol/l, 12% history of CVD, 60% were female, average age was 83, BMI 25 Treatment Indapamide (1.25 mg) - then indapamide plus perindopril (2 or 4mg) or placebo daily Duration Followed for 1.8 years Results BP differences at the end (15/6 mm Hg lower) - 74% on both drugs N Engl J Med 2008:358
43 BP elderly results Fatal or nonfatal stroke (%) Serious adverse event (%) Overall mortality (%) MI (%) Any cardiovascular event (%) Placebo Inda/perin Relative risk reduction Absolute risk reduction Number needed to treat P= NSS No mention of adverse effects
44 All the TARGET dose evidence Drug High/low dose Duration (years) Absolute Benefits Absolute Harms Enalapril 4x 0.5 None 8% Lisinopril 7-15x 4 4/6% 3/7% Carvedilol 4x 0.5 None 10% Carvedilol 8x 4 None 20% Losartan 3x 5 3% 3/7% Benefits - primarily hospitalizations Harms - hypotension, withdrawal, dose reduction

45 883 heart failure patients - age % class II, 29% class III Randomised to bisoprolol (10 mg daily) or carvedilol (25 mg BID) and slowly up-titrated patients to the RECOMMENDED doses Fraction of dose Patients on dose at end/12 weeks 0 1/8 1/4 1/2 FULL 10% 10% 25% 25% 30% Eur J Heart Fail 2011;13:670-80
46 Prevention medications do NOT make you feel better primary prevention 1-2% benefit over 5 years % do not secondary prevention 5-10% benefit over 5 years % do not lab tests false positives witch hunt evidence plus patient values - 1/3 not adherent
47 Risk reduction meds ASA, statins - you can just stop them Fibrates - please just stop them Blood pressure and diabetes drugs? dosage should be reduced by 50%, with reassessment of blood pressure at 2 weeks if the patient is still normotensive, reduce the dosage by another 50% (i.e., to 25% of the initial dose) and recheck the blood pressure in another 2 weeks
48 Use tricks to get patient interest THEIR ARGUMENTS I ve taken these for years and now you are telling me I don t need them But these are for my heart!! It s OK, I don t pay for my medications But my specialist says I need these If it isn t broken then don t fix it
49 YOUR ARGUMENTS Well your renal function/hepatic function are decreased Look what you ve been able to do for yourself You take control and figure out the dose - you teach me what works Your specialist doesn t know you like I do We can always restart if we need to
50 KEEP CALM BECAUSE LESS IS MORE KEEP CALM AND USE VERY LOW DOSES KEEP CALM AND TAPER ON
51 KEEP CALM AND DO THE RIGHT THING
Evidence and So Much More
 Evidence and So Much More James McCormack, BSc(Pharm), PharmD Professor, Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC Entire salary comes through the UBC Faculty of
Evidence and So Much More James McCormack, BSc(Pharm), PharmD Professor, Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC Entire salary comes through the UBC Faculty of
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada
, PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada") James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada My Agenda Discuss the best available evidence Put the evidence into
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada My Agenda Discuss the best available evidence Put the evidence into
Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course
 Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course An interactive course on common and new drug therapy issues from an evidence based perspective Education should not be
Welcome to the 19th Annual wow, almost 20 years Drug Therapy Decision Making Course An interactive course on common and new drug therapy issues from an evidence based perspective Education should not be
A C A D E M I C D E TA I L I N G C H O O S I N G W I S E LY C O N F E R E N C E O C T 2 1, PA M M C L E A N - V E Y S E Y B S C P H A R M D R
 PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
PPI DEPRESCRIBING Canadian Deprescribing Network (CaDeN) goals are to: Reduce harm by raising awareness and cutting risky prescriptions for seniors by 50% by 2020. Promote health by ensuring access to
Kanyini Guidelines Adherence with the Polypill (Kanyini GAP)
") Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) Disclosures Funded by the National Health and Medical Research Council of Australia. Dr Reddy s Laboratories Ltd manufactured and supplied polypills
Kanyini Guidelines Adherence with the Polypill (Kanyini GAP) Disclosures Funded by the National Health and Medical Research Council of Australia. Dr Reddy s Laboratories Ltd manufactured and supplied polypills
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY
 TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
TOP 5 DRUGS.. TO AVOID IN THE ELDERLY Debbie Kwan, BScPhm., MSc., FCSHP Canadian Geriatrics Society, April 20, 2013 Disclosure of Potential for Conflict of Interest: Financial Disclosure: None Mar 26,
BLCS 1-Clinical Overview. Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative
 BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
BLCS 1-Clinical Overview Dr. Chris Rauscher Clinical Lead Shared Care Polypharmacy Risk Reduction Initiative Fraser Health Guide To Person-Centered Medication Decisions Factors to Consider When Systematically
Pain therapeutics. Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain
 Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
Pain therapeutics Acetaminophen/NSAIDs Acute pain Osteoarthritis Migraine Acute Gout Neuropathic pain James McCormack, Pharm.D. Professor Faculty of Pharmaceutical Sciences, UBC Common types of pain killers
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Rational Medication Use in Dementia
 Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Rational Medication Use in Dementia Stephen Thielke sthielke@u.washington.edu (206) 764 2815 I have no conflicts of interest to report. I am an employee of the federal government. The opinions in this
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
What s New, What s True, and What s Poo Part 1
 What s New, What s True, and What s Poo Part 1 Tina Korowynk and Mike Kolber PEER Group What s New? What s True? What s Poo? 1 Anti-Depressants Meta-Analysis (Network): 522 RCTs (116477 pts) Mean duration
What s New, What s True, and What s Poo Part 1 Tina Korowynk and Mike Kolber PEER Group What s New? What s True? What s Poo? 1 Anti-Depressants Meta-Analysis (Network): 522 RCTs (116477 pts) Mean duration
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy
 David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
David Gardner, BSc Pharm, MSc CH&E, PharmD Professor, Department of Psychiatry & College of Pharmacy It s no dream. Sleep well without sleeping pills. Outline Baby boomers & beyond: medication use Deprescribing
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
DEPRESCRIBING IN THE ELDERLY
 DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
DEPRESCRIBING IN THE ELDERLY G E R I A T R I C S R E F R E S H E R D A Y W E D N E S D A Y, A P R I L 5 TH, 2 0 1 7 V É R O N I Q U E F R E N C H M E R K L E Y, M D, C C F P ( C O E ) B R U Y È R E C O
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Disclosures. Objectives. Cardiovascular Risk. Patient Case. JUPITER: The final frontier in statin utilization or an idea from outer space?
 Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Informed Consent, Goals and Targets
 Informed Consent, Goals and Targets Kenneth Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics Florida State University College of Medicine Objectives Understand the nature of true informed
Informed Consent, Goals and Targets Kenneth Brummel-Smith, MD Charlotte Edwards Maguire Professor of Geriatrics Florida State University College of Medicine Objectives Understand the nature of true informed
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
The who, what, why, where, and when of Clinical Practice Guidelines (CPGs)
") The who, what, why, where, and when of Clinical Practice Guidelines (CPGs) Appraisal of Guidelines for Research and Evaluation (AGREE) II DOMAIN 1. SCOPE AND PURPOSE DOMAIN 2. STAKEHOLDER INVOLVEMENT DOMAIN
The who, what, why, where, and when of Clinical Practice Guidelines (CPGs) Appraisal of Guidelines for Research and Evaluation (AGREE) II DOMAIN 1. SCOPE AND PURPOSE DOMAIN 2. STAKEHOLDER INVOLVEMENT DOMAIN
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION. Building Partnerships for Successful Aging
 MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
MEDICATION APPROPRIATENESS FOR THE AGING POPULATION Building Partnerships for Successful Aging Learning objectives Appreciate complexities involved in making appropriate clinical decisions in older adults
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada
, PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada") LESS IS MORE James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada MORE OR LESS therapeuticseducation.org medicationmythbusters.com
LESS IS MORE James McCormack BSc (Pharm), PharmD Professor Faculty of Pharmaceutical Sciences University of British Columbia Vancouver, BC, Canada MORE OR LESS therapeuticseducation.org medicationmythbusters.com
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Hypertension and Cholesterol in the Elderly
 Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Hypertension and Cholesterol in the Elderly Angela Sanford, MD Assistant Professor of Geriatrics Saint Louis University School of Medicine I have no relevant financial disclosures Cushman WC. The burden
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Brief Intervention for Smoking Cessation. National Training Programme
 Brief Intervention for Smoking Cessation National Training Programme Introduction Monitor tobacco use and prevention policies Protect people from tobacco smoke Offer help to quit tobacco use Warn about
Brief Intervention for Smoking Cessation National Training Programme Introduction Monitor tobacco use and prevention policies Protect people from tobacco smoke Offer help to quit tobacco use Warn about
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016
 2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
2016 Update in Geriatrics Elizabeth Eckstrom, MD, MPH Oregon Health & Science University Oregon Geriatrics Society October 7, 2016 I have no conflicts of interest Photos thanks to Google images This year
SESSION 5 2:20 3:35 PM
 SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 5 2:20 3:35 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
CYP2C19-Proton Pump Inhibitors
 CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
CYP2C19-Proton Pump Inhibitors Cameron Thomas, Pharm.D. PGY2 Clinical Pharmacogenetics Resident St. Jude Children s Research Hospital February 1, 2018 Objectives: CYP2C19-PPI Implementation Review the
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Polypharmacy & De-prescribing In Older Adults
 Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
Polypharmacy & De-prescribing In Older Adults Maryland Association of Osteopathic Physicians Annual Meeting September 15, 2018 Elizabeth Phung, DO Lead Clinical Associate Physician Beacham Center for Geriatric
How to CRITICALLY APPRAISE
 How to CRITICALLY APPRAISE an RCT in 10 minutes James McCormack BSc(Pharm), Pharm D Professor Faculty of Pharmaceutical Sciences, UBC Vancouver, BC, Canada medicationmythbusters.com CRITICAL APPRAISAL
How to CRITICALLY APPRAISE an RCT in 10 minutes James McCormack BSc(Pharm), Pharm D Professor Faculty of Pharmaceutical Sciences, UBC Vancouver, BC, Canada medicationmythbusters.com CRITICAL APPRAISAL
Type 2 Diabetes. Stopping Smoking. Consider referral to smoking cessation. Consider referring for weight management advice.
 Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Type 2 Diabetes Stopping Smoking Consider referral to smoking cessation BMI > 25 kg m² Set a weight loss target of a 5-10% reduction Consider referring for weight management advice Control BP to
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Smoking Cessation. Disclosures. Thank You. None
 Smoking Cessation Dr. Jamie Kellar; BSc, BScPhm, PharmD Clinician Educator Centre for Addiction and Mental Health Assistant Professor Leslie Dan Faculty of Pharmacy Disclosures None Thank You Several slides
Smoking Cessation Dr. Jamie Kellar; BSc, BScPhm, PharmD Clinician Educator Centre for Addiction and Mental Health Assistant Professor Leslie Dan Faculty of Pharmacy Disclosures None Thank You Several slides
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand
 Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Family Medicine Clerkship. Learning Prompts
 Family Medicine Clerkship Learning Prompts 9 SYSTEMS & CONDITIONS Respiratory conditions................................. 1 COPD Asthma Infectious diseases.................................... 2 Sore throat
Family Medicine Clerkship Learning Prompts 9 SYSTEMS & CONDITIONS Respiratory conditions................................. 1 COPD Asthma Infectious diseases.................................... 2 Sore throat
Vascular Diseases. Overview: Selected Slides
 Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Current Issues in Cardiovascular Risk Management. Les Toop Norman Sharpe June 2014
 Current Issues in Cardiovascular Risk Management Les Toop Norman Sharpe June 2014 Risk assessment is just the beginning of a conversation Les Toop Department of General Practice, University of Otago, Christchurch
Current Issues in Cardiovascular Risk Management Les Toop Norman Sharpe June 2014 Risk assessment is just the beginning of a conversation Les Toop Department of General Practice, University of Otago, Christchurch
A Process for Performing Medication Assessments
 A Process for Performing Medication Assessments Derek Jorgenson, BSP, PharmD, FCSHP College of Pharmacy and Nutrition University of Saskatchewan Objectives 1. Learn an overview of a medication assessment
A Process for Performing Medication Assessments Derek Jorgenson, BSP, PharmD, FCSHP College of Pharmacy and Nutrition University of Saskatchewan Objectives 1. Learn an overview of a medication assessment
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Benzodiazepines: risks, benefits or dependence
 Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Benzodiazepines: risks, benefits or dependence A re-evaluation Council Report CR 59 January 1997 Royal College of Psychiatrists, London Due for review: January 2002 1 Contents A College Statement 3 Benefits
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment
 Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Reducing the Anxiety of Pediatric Anxiety Part 2: Treatment Lisa Lloyd Giles, MD Medical Director, Behavioral Consultation, Crisis, and Community Services Primary Children s Hospital Associate Professor,
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Deconstructing Polypharmacy. Alan B. Douglass, M.D. Director
 Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
Deconstructing Polypharmacy Alan B. Douglass, M.D. Director Recognize this patient? Mrs. Brown- 82 years young Active Medical Problems Hypertension Hyperlipidemia Type 2 Diabetes Peripheral edema Osteoarthritis
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Disclosure. Overview. Objectives. Five Noteworthy Outpatient Publications. Factors Affecting Antibiotic Prescribing 7/24/2013
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Five Noteworthy Outpatient Publications R. Vandervoort, Pharm.D. Disclosure I do not have a vested interest in or affiliation with any corporate organization
47 th Annual Meeting August 2-4, 2013 Orlando, FL Five Noteworthy Outpatient Publications R. Vandervoort, Pharm.D. Disclosure I do not have a vested interest in or affiliation with any corporate organization
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Prevention of MACROvascular Complications of Diabetes
 Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
PPIs: Good or Bad? 1. Basics of PPIs. Gastric Acid Basics. Outline. Gastric Acid Basics. Proton Pump Inhibitors (PPI)
") Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Outline Quick basics on Proton Pump Inhibitors (PPIs) PPIs: Good or Bad? What are potential risks of PPI therapy? How to approach your patients American Gastroenterology Association (AGA) recommendations
Drugs that poison the elderly
 Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Drugs that poison the elderly Brent Tipping Sub-specialist Geriatrician and Specialist Physician Division of Geriatric Medicine, Department of Medicine University of the Witwatersrand To treat or not to
Drugs Categories. 4. Which suffix do alpha blocker generic drug names often end with?
 CATEGORIES: QUIZ 3 Drugs Categories 1. What drug subcategory often ends with the suffix -azosin? a. Corticosteroids b. Alpha blockers c. Calcium channel blockers d. Beta blockers e. ACE inhibitors 2. What
CATEGORIES: QUIZ 3 Drugs Categories 1. What drug subcategory often ends with the suffix -azosin? a. Corticosteroids b. Alpha blockers c. Calcium channel blockers d. Beta blockers e. ACE inhibitors 2. What
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
SMOKING CESSATION IS HARD
 POWER TO BREAK THE HOLD OF NICOTINE ADDICTION 1 SMOKING CESSATION IS HARD Most smokers try to quit 5-7 times before they are successful. 2 Why is it so hard to quit? Typical withdrawal symptoms from stopping
POWER TO BREAK THE HOLD OF NICOTINE ADDICTION 1 SMOKING CESSATION IS HARD Most smokers try to quit 5-7 times before they are successful. 2 Why is it so hard to quit? Typical withdrawal symptoms from stopping
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
CARDIAC REHABILITATION PROGRAMME:- MEDICATION
 CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
CARDIAC REHABILITATION PROGRAMME:- MEDICATION AIM OF THIS SESSION Understand the reasons for taking your medications, Discuss the common side effects associated with these medications - knowing when to
To Take or Not To Take?
 To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests
To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests