Identification of subjects at high risk for cardiovascular disease
|
|
|
- Dina Hall
- 5 years ago
- Views:
Transcription



1 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April Identification of subjects at high risk for cardiovascular disease Lars Rydén Karolinska Institutet Stockholm, Sweden

2 Introductory remarks Why detect To prevent premature development of cardiovascular disease


3 Introductory remarks Is prevention of CVD possible? Impossible figure Oscar Reuterswärd Waterfall Mauritius Cornelis Escher
4 Proportionate reduction Cardiovascular Disease Prevention Impact of prevention vs. treatment - the landmark Finnish example Observed Mortality Smoking Blood pressure Cholesterol Enhanced by therapeutic success Predicted by the three factors combined -70 Vartiainen et al. BMJ 1994;309:

5 Cardiovascular Disease Prevention Impact prevention vs. treatment - CHD deaths in the Sweden ,180 fewer deaths Björk, Rosengren, Bennett, Lappas,Capewell Europ Heart J 2009; 30:1046 Risk Factors worse +11% Diabetes +8 Obesity +3 Risk Factors better - 66% Cholesterol (diet) -39 Smoking -20 Population BP fall -9 Physical activity -3 Treatments - 36% AMI -6 Secondary prevention -12 Heart failure -7 Angina ASA, CABG & PTCA -3 Hypertension -4 Primary prevention (statins) -2 Unexplained - 9%



6 Cardiovascular Disease Prevention Impact prevention vs. treatment Experiences from Beijing (50% increase ) Risk Factors worse 1820 extra deaths Cholesterol (+1.03 mmol/l) +77% Diabetes +19% Critchley, Capewell et al. Circulation 2004; 110:1236 BMI +4% Smoking +1% Treatments 370 fewer deaths
7 Cardiovascular Disease Prevention The contents - four pillars for success Epidemiological information Population based, trustworthy and updated Mortality not enough, morbidity important Risk assessement tools Considering total risk Risk engines Risk asessement tools Guidelines for cardiovascular disease prevention Comprehensive and transprofessional Regularly updated Implementated in all important respects
8 Cardiovascular Disease Prevention Four pillars for success Epidemiological information Population based, trustworthy and updated Mortality not enough, morbidity important
9 Epidemiology on Cardiovascular Disease Information from the ESC and EHN collaborating on the European Heart Health Charter
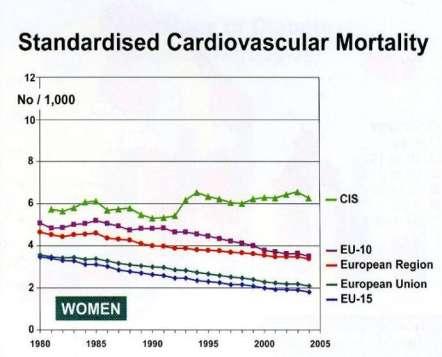
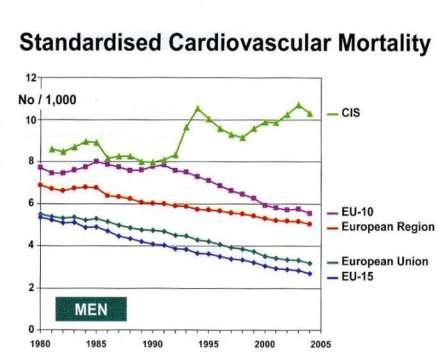
10 Epidemiology of Cardiovascular Disease Trends in mortality and morbidity

11 Epidemiology of Cardiovascular Disease Cardiovascular mortality across Europe (<65 years) CVD the major contributor to an almost 20 year difference in life expectancy across Europe
 Million with diabetes 48 and IGT 63")
12 Diabetes in Europe Actual in 2007 (IDF Diabetes Atlas 3rd edition 2006) Million with diabetes 48 and IGT 63
 Million with diabetes 56 and")
13 Diabetes in Europe Prognosis for 2026 (IDF Diabetes Atlas 3rd edition 2006) Million with diabetes 56 and IGT 71
14 Cardiovascular Disease Prevention (CVD) Four pillars for success Epidemiological information Population based, trustworthy and updated Mortality not enough, morbidity important Risk assessement tools Considering total risk Risk engines Risk asessement tools
15 Proportion Cardiovascular Disease Prevention (CVD) Three strategies Population High risk Secondary Primary Population distribution of cardiovascular (CV) risk Low risk: Covering most of those falling ill High risk: Covering a few at high risk falling ill 10-year risk WHO Technical Report Series 678, Geneva, 1982

")



16 Assessment of CV Risk Classic and Emerging Methods ID of (vulnerable) plaques MR/MSCRT Case history Length/weight Waist circumf Blood pressure ECG Stress test Echocardiogram Lab examinations Lipids Glucose

17 The Concept of Total Risk Assessment Cornerstone in Cardiovascular Disease Prevention CVD is multifactorial in origin Risk factors interact synergistically Physicians see people, not isolated risk factors Pyörälä K et al. Atherosclerosis. 1994;110:
18 10 yr risk of fatal CVD (%) Impact of combinations of risk factors year risk for fatal CVD according to SCORE Men, smoking SBP 160 mm Hg TC/HDL ratio Women, smoking SBP 160 mm Hg Men, non-smoking SBP 120 mm Hg Women, non-smoking SBP 120 mm Hg
19 Odds Ratio (99% CI) About diabetes and cardiovascular risk INTERHEART Of importance.the rapid increase in Odds Ratio by a combination of risk factors Common in diabetes (Yusuf et al. Lancet 2004; 364:937)

20 The Concept of Total Risk Assessment Why stress assessment of total CVD risk Usually multiple risk factors behind atherosclerosis causing CVD These risk factors interact, sometimes multiplicatively The aim is to reduce total risk If a target cannot be reached with one risk factor, total risk can still be reduced by trying harder with other
21 Objectives with CVD prevention 1 To assist people at low risk of CVD to maintain this state lifelong and help those at increased risk to reduce it 2 To achieve the healthy characteristics No smoking Healthy food choices Physical activity: 30 min of moderate activity/day BMI <25 kg/m 2 + avoidance of central obesity BP <140/90 mmhg Total cholesterol <5 mmol/l LDL cholesterol <3 mmol/l Blood glucose <6mmo/L
22 Objectives with CVD prevention 3 To achieve rigorous risk factor control in high risk subjects, especially in known CVD or diabetes Blood pressure under 130/80 mmhg if feasible Total cholesterol <4.5 mmol/l; option <4 mmol/l LDL cholesterol <2.5 mmol/l; option <2mmol/L Fasting blood glucose <6 mmol/l and HbA1c <6.5% 4 To consider cardioprotective drug therapy in high risk subjects especially those with atherosclerotic CVD
23 A Need to Adapt Prevention to Total Individual Cardiovascular Risk Randomized trials show that statins cause a RR reduction of 30% (outcome when applied to 2 different risk patterns) Variable Total CV risk during 10 years Absolute risk (%) 1 10 Adj RR (%) NNT (n) NNT to side effects!!! -

24 Assessment of Total CV Risk General rule according to European Guidelines Total CV risk is high or very high in subjects with: Established CVD DM Markedly elevated single risk factors - Total cholesterol 8 mmol/l, LDL cholesterol 6 mmol/l - SBP 180 mm Hg and/or DBP 110 mm Hg Pronounced family history of CVD at young age In all other subjects, total CV risk should be estimated with a risk score model. LDL, low-density lipoprotein; SBP, systolic blood pressure; DBP, diastolic BP. De Backer et al. Eur Heart J. 2003;24:
25 Identification of people at risk Risk assessement tools used in Western populations Framingham-based risk equation (USA) 1 Systematic Coronary Risk Evaluation (SCORE; Europe) 2 PREDICT (New Zealand) 3 Joint British Societies coronary risk prediction 4 HeartScore (Europe) 5 1. Wilson PWF et al. Circulation 1998;97: Conroy RM et al. Eur Heart J 2003;24: Bannink L et al. N Z Med J 2006;119:U British Cardiac Society et al. Heart 1998;80(Suppl 2): European Society of Cardiology. (Accessed 19 August 2009)


26 Assessment of Total CV Risk Framingham Heart Disease Risk Calculator Kannel WB, McGee D, Gordon T A general cardiovascular risk profile: the Framingham Study Am J Cardiol.1976;38:46
 Age 20-39 Age 40-49 Age 50-59 Age 60-69 Age 70-79 <160 0 0 0 0 0 160-199 4 3 2 1 0 200-239 7 5 3 1 0 240-279 9 6 4 2 1 >280 11 8 5 3 1 Step 5: Smoking Status Points at")
27 Assessment of Total CV Risk Framingham Heart Disease Risk Calculator Step 1: Age Years Points Step 2: Total Cholesterol TC Points (mg/dl) Age Age Age Age Age < > Step 5: Smoking Status Points at Age Nonsmoker Smoker Characteristics A rather small US population for fatal/nonfatal CHD includes: Sex and age Total & HDL cholesterol Smoking Systolic blood pressure Step 3: HDL-C HDL-C (mg/dl) Points > <40 2 Step 6: Adding Points Category: Points Age Total-C HDL-C SBP Smoking status Point Total: HDL, high-density lipoprotein. NCEP guidelines. JAMA. 2001;285: Step 4: Systolic Blood Pressure SBP Points mm Hg Untreated Treated < > Step 7: CHD Risk Point Total 10-Year Risk <0 <1% 0 1% 1 1% 2 1% 3 1% 4 1% 5 2% 6 2% 7 3% 8 4% 9 5% 10 6% 11 8% 12 10% 13 12% 14 16% 15 20% 16 25% >17 >30%

28 Assessment of Total CV Risk Framingham Heart Disease Risk Calculator: Online Access Highest risk: >20% or a history of heart disease or DM High risk: 10%-20% and 2 risk factors Moderate risk: <10% and 2 risk factors Low risk: 1 risk factor
29 Identification of people at risk Risk assessement and ethnicity Screening tools from Western populations may not be accurate in AP populations Background epidemiology of CVD and risk factors may differ affect risk calculations NCEP ATP III criteria underestimates the at-risk AP population 1 Framingham-based CV risk calculators overestimates the risk in Asian populations 2 AP: Asia-Pacific; NCEP ATP: National Cholesterol Education Programme Adult Treatment Panel 1. Tan C-E, et al. Diabetes Care 2004;27: Asia Pacific Cohort Studies Collaboration, et al. J Epidemiol Community Health 2007;61:
30 CV event (%) CV event (%) The Framingham risk engine overestimates the CVD risk in Asian populations Observed and predicted CV event rate according to deciles of predicted risk in Chinese patients Men Observed Predicted Women Bias = +276% 10 Bias = +102% Deciles of predicted risk based on Framingham equation Deciles of predicted risk based on Framingham equation CV: cardiovascular APCSC. J Epidemiol Community Health 2007;61:
31 Identification of people at risk Risk assessement and ethnicity Development of new risk assessment equations Recalibration/modification of existing equations or definitions Resources for risk factor screening are limited in many AP countries - Reliable and inexpensive risk tools are needed
 from the Framingham Study with those derived from Asian cohorts APCSC.")
32 Identification of people at risk Risk assessement in the Asian-Pacific region The Asia Pacific Cohort Studies Collaboration APCSC Objective To compare low-information equations (age, systolic blood pressure, cholesterol, smoking habits) from the Framingham Study with those derived from Asian cohorts APCSC. J Epidemiol Community Health 2007;61:
33 Identification of people at risk Risk assessement in the Asian-Pacific region Pools data from longitudinal studies with information on CVD in the Asia Pacific region Comprises data on >650,000 participants 44 separate cohort studies in mainland China, Hong Kong, Taiwan, Japan, South Korea, Singapore, Thailand, New Zealand and Australia Is one of largest databases worldwide APCSC. J Epidemiol Community Health 2007;61:
34 CV event (%) CV event (%) A new CVD equation for Asian populations Observed and predicted CV event rate according to deciles of predicted risk in Chinese patients 8 Men Observed Predicted 8 Women Bias = +11% 4 Bias = +10% Deciles of predicted risk based on other Asian equation Deciles of predicted risk based on other Asian equation APCSC. J Epidemiol Community Health 2007;61:
35 CV event (%) CV event (%) Recalibration of the Framingham risk calculator for an Asian population Observed and predicted CV event rate according to deciles of predicted risk in Chinese patients Observed Men Women 6 5 Bias = 2% 4 3 Bias = +4% Deciles of predicted risk based on the recalibrated Framingham equation Predicted Deciles of predicted risk based on the recalibrated Framingham equation APCSC. J Epidemiol Community Health 2007;61:

36 Assessment of Total CV Risk Systematic Coronary Risk Evaluation (SCORE) European Cohort Studies (n = 12) Some with multiple sub-studies Mainly population based Some figures: About 250,000 people Follow-up 3 million person years Cardiovascular fatalities >7000 Eur Heart J 2007; 28: Executive summary
 European:")


37 Assessment of Total CV Risk Systematic Coronary Risk Evaluation (SCORE) European: 10 year risk for fatal CVD; high vs. low risk populations A 10-year risk of CVD death >5% considered as a high or at least increased risk Eur Heart J 2007; 28: Executive summary
38 Assessment of Total CV Risk Systematic Coronary Risk Evaluation (SCORE) Risk estimation using SCORE qualifiers To be used with knowledge and judgement Risk overestimated with a falling and underestimated if rising CVD mortality Risk appears lower for women. This is misleading - charts show that their risk is deferred by 10 years Risk may be higher than indicated in the chart in The sedentary or obese Those with a strong family history The socially deprived Diabetes - risk x 4-5 in women and x 3 in men

39 Assessment of Total CV Risk Systematic Coronary Risk Evaluation (SCORE) Relative risk chart For younger persons who despite a low total risk may have a several times higher risk in relation to others in the same age group
40 Assessment of the Risk for Diabetes Oral Glucose Tolerance Test (OGTT) in CAD % % 8% 8% 8% 5% DM 60 27% 21% IGT IFG 40 Normal 20 % of all with OGTT 0 FPG WHO (Bartnik et al Heart 2007; 93:72) OGTT WHO 1999 criterion (FPG < 6.1 mmol/l) FPG ADA OGTT ADA 2003 criterion (FPG < 5.6 mmol/l)
 to address 10-year risk of type 2 DM (T2DM) in adults Available at:")
41 Assessment of the Risk for Diabetes FINDRISC Finnish Diabetes Risk Score (FINDRISC) to address 10-year risk of type 2 DM (T2DM) in adults Available at:
 Available at www.dtu.ox.ac.uk/index.php?")
42 Assessment of Total CV Risk in diabetes The UKPDS Risk engine Risk Engine according to United Kingdom Prospective Diabetes Study (UKPDS) Available at
43 Cardiovascular Disease Prevention The contents - four pillars for success Epidemiological information Population based, trustworthy and updated Mortality not enough, morbidity important Risk assessement tools Considering total risk Risk engines Risk asessement tools Guidelines for cardiovascular disease prevention Comprehensive and transprofessional Regularly updated Implementated in all important respects



44 From evidence to clinical practice Research Guidelines Surveys Education



45 Guidelines for CVD The European version 1994 First Joint Task Force recommendations 1998 Second Joint Task Force recommendations 2003 Third Joint Task Force guidelines 2007 Fourth Joint Task Force guidelines 2012 Fifth under way

46 Characteristics of healthy people 0 smoking 3 km of daily walking 5If high risk portions of fruit & vegetables/day <140/90 130/80 mm Hg blood pressure < mmol/l total cholesterol < mmol/l LDL-cholesterol 0 diabetes European phone number to health
47 Conclusions Prevention CVD Risk of CVD should be based on total CV risk rather Continuum than be split on primary and secondary prevention Ethnicity Family history Hyperlipidemia Hypertension Age and sex Risk calculators (ex. Framingham, SCORE UKPDS) Obesity help in assessing Metabolic total risk DM but must be adapted to Smoking syndrome local populations Prediabetes Physical inactivity DM is an independent risk factor for CVD The risk of CV events increases dramatically with concomitant risk factors Need for prevention of cardiovascular disease
48 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April Identification of subjects at high risk for cardiovascular disease Time for questions
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Cardiovascular disease - from management to prevention
 Cardiovascular disease - from management to prevention Reflections originating from the Fourth Joint European Societies Task Force on Cardiovascular Disease Prevention in Clinical Practice 2007 WHAT IS
Cardiovascular disease - from management to prevention Reflections originating from the Fourth Joint European Societies Task Force on Cardiovascular Disease Prevention in Clinical Practice 2007 WHAT IS
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention?
 well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
EuroPrevent 2010 Fatal versus total events in risk assessment models
 EuroPrevent 2010 Fatal versus total events in risk assessment models Pekka Jousilahti, MD, PhD,Research Professor National Institute for Health and Welfare, Finland Risk assessment models Estimates the
EuroPrevent 2010 Fatal versus total events in risk assessment models Pekka Jousilahti, MD, PhD,Research Professor National Institute for Health and Welfare, Finland Risk assessment models Estimates the
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk. Eberhard Standl
 Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk Eberhard Standl European Heart House Sophia Antipolis Thursday, June 17, 2010 IDF Diabetes Atlas 2009: Global Numbers Still
Epidemiology of Diabetes, Impaired Glucose Homeostasis and Cardiovascular Risk Eberhard Standl European Heart House Sophia Antipolis Thursday, June 17, 2010 IDF Diabetes Atlas 2009: Global Numbers Still
Master Class in Preventive Cardiology. The New MI Phenotype OR. Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden
 Master Class in Preventive Cardiology The New MI Phenotype OR Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden The New MI Phenotype OR Coronary disease and glucose abnormalities Klas
Master Class in Preventive Cardiology The New MI Phenotype OR Klas Malmberg MD, PhD, FESC Karolinska Institutet, Stockholm Sweden The New MI Phenotype OR Coronary disease and glucose abnormalities Klas
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Prevenzione cardiovascolare e cambiamento degli stili di vita. Gian Franco Gensini
 Prevenzione cardiovascolare e cambiamento degli stili di vita Gian Franco Gensini Main causes of death worldwide at all ages (year:: 2005) 17.5 milion Preventing Chronic Diseases A vital investiment. WHO
Prevenzione cardiovascolare e cambiamento degli stili di vita Gian Franco Gensini Main causes of death worldwide at all ages (year:: 2005) 17.5 milion Preventing Chronic Diseases A vital investiment. WHO
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
CVD Prevention, Who to Consider
 Continuing Professional Development 3rd annual McGill CME Cruise September 20 27, 2015 CVD Prevention, Who to Consider Dr. Guy Tremblay Excellence in Health Care and Lifelong Learning Global CV risk assessment..
Continuing Professional Development 3rd annual McGill CME Cruise September 20 27, 2015 CVD Prevention, Who to Consider Dr. Guy Tremblay Excellence in Health Care and Lifelong Learning Global CV risk assessment..
Economically efficient approaches to address chronic disease in developing countries
 Economically efficient approaches to address chronic disease in developing countries Thomas A. Gaziano MD MSc Division of Cardiovascular Medicine Brigham & Women s Hospital Harvard Medical School Center
Economically efficient approaches to address chronic disease in developing countries Thomas A. Gaziano MD MSc Division of Cardiovascular Medicine Brigham & Women s Hospital Harvard Medical School Center
Master class in preventive cardiology Focus on diabetes and cardiovascular disease Geneva April
 Master class in preventive cardiology Focus on diabetes and cardiovascular disease Geneva April 14 2011 Introduction Course objectives A review of available guidelines Lars Rydén Cardiology Unit Department
Master class in preventive cardiology Focus on diabetes and cardiovascular disease Geneva April 14 2011 Introduction Course objectives A review of available guidelines Lars Rydén Cardiology Unit Department
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
Population models of health impact of combination polypharmacy
 Population models of health impact of combination polypharmacy Global Summit on Combination Polypharmacy for CVD, 25 th September 2012 Dr Mark Huffman Northwestern University, Chicago Charity No: 1110067
Population models of health impact of combination polypharmacy Global Summit on Combination Polypharmacy for CVD, 25 th September 2012 Dr Mark Huffman Northwestern University, Chicago Charity No: 1110067
Professor Norman Sharpe. Heart Foundation West Coast
 Professor Norman Sharpe Heart Foundation West Coast Primary Care the Keystone to Heart Health Improvement Norman Sharpe June 2013 The heart health continuum and the keystone position The culprit disease
Professor Norman Sharpe Heart Foundation West Coast Primary Care the Keystone to Heart Health Improvement Norman Sharpe June 2013 The heart health continuum and the keystone position The culprit disease
ASSeSSing the risk of fatal cardiovascular disease
 ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
ASSeSSing the risk of fatal cardiovascular disease «Systematic Cerebrovascular and coronary Risk Evaluation» think total vascular risk Assess the risk Set the targets Act to get to goal revised; aupril
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Know Your Number Aggregate Report Single Analysis Compared to National Averages
 Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Know Your Number Aggregate Report Single Analysis Compared to National s Client: Study Population: 2242 Population: 3,000 Date Range: 04/20/07-08/08/07 Version of Report: V6.2 Page 2 Study Population Demographics
Unraveling the concealed and calculated cardiovascular risks in diabetes
 15 P B Fernando Memorial Oration 2015 Unraveling the concealed and calculated cardiovascular risks in diabetes Weerarathna T P 1 Journal of the Ceylon College of Physicians, 2016, 47, 15-19 Abstract Cardiovascular
15 P B Fernando Memorial Oration 2015 Unraveling the concealed and calculated cardiovascular risks in diabetes Weerarathna T P 1 Journal of the Ceylon College of Physicians, 2016, 47, 15-19 Abstract Cardiovascular
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Coronary interventions in patients with diabetes Lars Rydén Karolinska Institutet Stockholm, Sweden
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Diabetes, Diet and SMI: How can we make a difference?
 Diabetes, Diet and SMI: How can we make a difference? Dr. Adrian Heald Consultant in Endocrinology and Diabetes Leighton Hospital, Crewe and Macclesfield Research Fellow, Manchester University Relative
Diabetes, Diet and SMI: How can we make a difference? Dr. Adrian Heald Consultant in Endocrinology and Diabetes Leighton Hospital, Crewe and Macclesfield Research Fellow, Manchester University Relative
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Journal of the American College of Cardiology Vol. 48, No. 2, by the American College of Cardiology Foundation ISSN /06/$32.
 Journal of the American College of Cardiology Vol. 48, No. 2, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.03.043
Journal of the American College of Cardiology Vol. 48, No. 2, 2006 2006 by the American College of Cardiology Foundation ISSN 0735-1097/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2006.03.043
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient?
 Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
Northwestern University Feinberg School of Medicine Calculating the CVD Risk Score: Which Tool for Which Patient? Donald M. Lloyd-Jones, MD, ScM, FACC, FAHA Senior Associate Dean Chair, Department of Preventive
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV. GUY DE BACKER Ghent University,Belgium
 EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
40% minimum reduction from
 160 Circulatory Disease Mortality Target: Death rates in England 1993-2006 Persons under 75 Death / 100,000 population A fall of 44% over 10 years 140 120 100 80 60 40 20 141.0 84.2 Immortality guaranteed
160 Circulatory Disease Mortality Target: Death rates in England 1993-2006 Persons under 75 Death / 100,000 population A fall of 44% over 10 years 140 120 100 80 60 40 20 141.0 84.2 Immortality guaranteed
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes?
 Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Cardiovascular Risk Assessment and Management Making a Difference
 Cardiovascular Risk Assessment and Management Making a Difference Norman Sharpe March 2014 Numbers and age-standardised mortality rates from all causes, by sex, 1950 2010 Death rates halved Life expectancy
Cardiovascular Risk Assessment and Management Making a Difference Norman Sharpe March 2014 Numbers and age-standardised mortality rates from all causes, by sex, 1950 2010 Death rates halved Life expectancy
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand
 Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
Should we base treatment decisions on short-term or lifetime CVD risk? Rod Jackson University of Auckland New Zealand Presentation outline Strengths & weaknesses of short-term risk approach Strengths &
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Key causes of preventable deaths in New Zealand In a population of 10,000 New Zealanders, every year there will be about:
 Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Cardiovascular risk factor appraisal art or science?
 Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Vascular Diseases. Overview: Selected Slides
 Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
Vascular Diseases Overview: Selected Slides Total deaths and change in vascular death rates
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
DECLARATION OF CONFLICT OF INTEREST. None
 DECLARATION OF CONFLICT OF INTEREST None Dietary changes and its influence on cardiovascular diseases in Asian and European countries Problems of Eastern European countries for cardiovascular disease prevention
DECLARATION OF CONFLICT OF INTEREST None Dietary changes and its influence on cardiovascular diseases in Asian and European countries Problems of Eastern European countries for cardiovascular disease prevention
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study
 Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
Lifetime clinical and economic benefits of statin-based LDL lowering in the 20-year Followup of the West of Scotland Coronary Prevention Study Harvey White Green Lane Cardiovascular Service and Cardiovascular
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES
 CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
CARDIOVASCULAR RISK FACTORS & TARGET ORGAN DAMAGE IN GREEK HYPERTENSIVES C. Liakos, 1 G. Vyssoulis, 1 E. Karpanou, 2 S-M. Kyvelou, 1 V. Tzamou, 1 A. Michaelides, 1 A. Triantafyllou, 1 P. Spanos, 1 C. Stefanadis
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Andrejs Kalvelis 1, MD, PhD, Inga Stukena 2, MD, Guntis Bahs 3 MD, PhD & Aivars Lejnieks 4, MD, PhD ABSTRACT INTRODUCTION. Riga Stradins University
 CARDIOVASCULAR RISK FACTORS ORIGINAL ARTICLE Do We Correctly Assess the Risk of Cardiovascular Disease? Characteristics of Risk Factors for Cardiovascular Disease Depending on the Sex and Age of Patients
CARDIOVASCULAR RISK FACTORS ORIGINAL ARTICLE Do We Correctly Assess the Risk of Cardiovascular Disease? Characteristics of Risk Factors for Cardiovascular Disease Depending on the Sex and Age of Patients
5/28/2010. Pre Test Question
 Myth of Metabolic Syndrome? C. W. Spellman, DO, PhD Professor and Associate Dean Research Dir. Center Diabetes and Metabolic Disorders Department Internal Medicine, Div. Endocrinology Texas Tech University
Myth of Metabolic Syndrome? C. W. Spellman, DO, PhD Professor and Associate Dean Research Dir. Center Diabetes and Metabolic Disorders Department Internal Medicine, Div. Endocrinology Texas Tech University
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS
 BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
Discussion points. The cardiometabolic connection. Cardiometabolic Risk Management in the Primary Care Setting
 Session #5 Cardiometabolic Risk Management in the Primary Care Setting Sonja Reichert, MD MSc FCFP FACPM Betty Harvey, RNEC BScN MScN Amanda Mikalachki, RN BScN CDE S Discussion points Whom should we be
Session #5 Cardiometabolic Risk Management in the Primary Care Setting Sonja Reichert, MD MSc FCFP FACPM Betty Harvey, RNEC BScN MScN Amanda Mikalachki, RN BScN CDE S Discussion points Whom should we be
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Modelling Reduction of Coronary Heart Disease Risk among people with Diabetes
 Modelling Reduction of Coronary Heart Disease Risk among people with Diabetes Katherine Baldock Catherine Chittleborough Patrick Phillips Anne Taylor August 2007 Acknowledgements This project was made
Modelling Reduction of Coronary Heart Disease Risk among people with Diabetes Katherine Baldock Catherine Chittleborough Patrick Phillips Anne Taylor August 2007 Acknowledgements This project was made
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s
 Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Understanding new international guidelines to tackle CV Risk: A practical model John Deanfield, MD UCL, London United Kingdom s Ho Chi Minh City, Vietnam August 7, 2014 JBS 2 Risk Guidelines (2005) Based
Implementing CVD guidelines: physician and patient factors
 Implementing CVD guidelines: physician and patient factors Professor Richard Hobbs Head of Primary Care & General Practice Primary Care Clinical Sciences Building University of Birmingham, United Kingdom
Implementing CVD guidelines: physician and patient factors Professor Richard Hobbs Head of Primary Care & General Practice Primary Care Clinical Sciences Building University of Birmingham, United Kingdom
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION
 Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Prevalence of Cardiac Risk Factors among People Attending an Exhibition
 IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 3, Issue 6 Ver. IV (Nov.-Dec. 2014), PP 4-51 Prevalence of Cardiac Risk Factors among People Attending
IOSR Journal of Nursing and Health Science (IOSR-JNHS) e-issn: 2320 1959.p- ISSN: 2320 1940 Volume 3, Issue 6 Ver. IV (Nov.-Dec. 2014), PP 4-51 Prevalence of Cardiac Risk Factors among People Attending
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Case Study: Chris Arden. Peripheral Arterial Disease
 Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Case Study: Chris Arden Peripheral Arterial Disease Patient Presentation Diane is a 65-year-old retired school teacher She complains of left calf pain when walking 50 metres; the pain goes away after she
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Epidemiologic Measure of Association
 Measures of Disease Occurrence: Epidemiologic Measure of Association Basic Concepts Confidence Interval for population characteristic: Disease Exposure Present Absent Total Yes A B N 1 = A+B No C D N 2
Measures of Disease Occurrence: Epidemiologic Measure of Association Basic Concepts Confidence Interval for population characteristic: Disease Exposure Present Absent Total Yes A B N 1 = A+B No C D N 2
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Notes Indicate to the group that this patient will be the focus of today s case discussion.
 1 Indicate to the group that this patient will be the focus of today s case discussion. Read out the case authors and their disclosure information. Instructions Fill out prior to the meeting and disclose
1 Indicate to the group that this patient will be the focus of today s case discussion. Read out the case authors and their disclosure information. Instructions Fill out prior to the meeting and disclose
Hypertension Management in Diabetic Patients
 Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Hypertension Management in Diabetic Patients Park, Chang G, MD, PhD Cardiovascular Center, Guro Hospital, Korea University Medical School Contents (Treatment of 2 Cases) Type 2 Diabetes Mellitus Hypertension
Metabolic Syndrome: Why Should We Look For It?
 021-CardioCase 29/05/06 15:04 Page 21 Metabolic Syndrome: Why Should We Look For It? Dafna Rippel, MD, MHA and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Andy s fatigue Andy, 47, comes to you
021-CardioCase 29/05/06 15:04 Page 21 Metabolic Syndrome: Why Should We Look For It? Dafna Rippel, MD, MHA and Andrew Ignaszewski, MD, FRCPC CardioCase presentation Andy s fatigue Andy, 47, comes to you
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Statistical Fact Sheet Populations
 Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
CONTRIBUTING FACTORS FOR STROKE:
 CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Cardiovascular Disease in Women -Vive La Difference? Dr Homeyra Douglas Consultant Cardiologist Aintree University Hospital
 Cardiovascular Disease in Women -Vive La Difference? Dr Homeyra Douglas Consultant Cardiologist Aintree University Hospital Death By Cause - Women 2004 UK Death by Cause-Women 2004 UK -CVD is responsible
Cardiovascular Disease in Women -Vive La Difference? Dr Homeyra Douglas Consultant Cardiologist Aintree University Hospital Death By Cause - Women 2004 UK Death by Cause-Women 2004 UK -CVD is responsible
Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals
 European Heart Journal Supplements (2004) 6 (Supplement A), A12 A18 Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals University of Sydney, Sydney, NSW, Australia
European Heart Journal Supplements (2004) 6 (Supplement A), A12 A18 Reducing low-density lipoprotein cholesterol treating to target and meeting new European goals University of Sydney, Sydney, NSW, Australia
Absolute cardiovascular disease risk management
 Quick reference guide for health professionals Absolute cardiovascular disease risk management This quick reference guide is for use by health professionals for primary prevention of cardiovascular disease
Quick reference guide for health professionals Absolute cardiovascular disease risk management This quick reference guide is for use by health professionals for primary prevention of cardiovascular disease
CVD risk estimation in populations with high prevalence of MetS. Dilek Ural, 12 March 2017 Koç University, Istanbul
 CVD risk estimation in populations with high prevalence of MetS Dilek Ural, 12 March 2017 Koç University, Istanbul Understanding CV risk Likelihood of a person developing an atherosclerotic CV event over
CVD risk estimation in populations with high prevalence of MetS Dilek Ural, 12 March 2017 Koç University, Istanbul Understanding CV risk Likelihood of a person developing an atherosclerotic CV event over
Association between Raised Blood Pressure and Dysglycemia in Hong Kong Chinese
 Diabetes Care Publish Ahead of Print, published online June 12, 2008 Raised Blood Pressure and Dysglycemia Association between Raised Blood Pressure and Dysglycemia in Hong Kong Chinese Bernard My Cheung,
Diabetes Care Publish Ahead of Print, published online June 12, 2008 Raised Blood Pressure and Dysglycemia Association between Raised Blood Pressure and Dysglycemia in Hong Kong Chinese Bernard My Cheung,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Supplemental tables/figures
 Supplemental tables/figures Table S:Baseline variables included in calculation of QRISK and Framingham scores Ethnicity (European, Indian Pakistani, Bangladeshi, Black African, Black Caribbean) QRISK Age,
Supplemental tables/figures Table S:Baseline variables included in calculation of QRISK and Framingham scores Ethnicity (European, Indian Pakistani, Bangladeshi, Black African, Black Caribbean) QRISK Age,
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,