Changing Diabetes: The time is now!
|
|
|
- Angelica Greene
- 5 years ago
- Views:
Transcription

1 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison ARNP,CDE GHG Endocrinology 1
2 The problem Every 33 seconds someone dies from CAD ( one woman dies every 62 seconds) 21 million Americans have diabetes 1 in 3 Americans born in 2000 will have diabetes in their lifetime By million people worldwide may have T2DM 18% of people over the age of 65 have diabetes 2



3 Escalating Epidemic of Type 2 Diabetes Overweight rates are fueling the diabetes epidemic 1,2 References: 1. CDC Data and trends; 2. CDC Prevalence data. 3
4 High blood sugar & Obesity Having hyperglycemia produces many symptoms that that mirror the metabolic problems of having too much fat. ENDOTHELIAL DYSFUNTION OXIDATIVE STRESS VASCULAR INFLAMMATION ABNORMAL CLOTTING METABOLIC ABNORMALITIES HYPERTENSION ABNORMAL LIPIDS 4
5 Coronary Heart Disease Incidence by HbA1c Levels in Type 2 Diabetes Incidence (%) in 3.5 Years Low < 6% CHD Mortality Middle 6% 7.9% HbA1c Tertile High > 7.9% Incidence (%) in 3.5 Years All CHD Events Low < 6% Middle 6% 7.9% HbA1c Tertile High > 7.9% P < 0.01 vs lowest tertile; P < 0.05 vs lowest tertile. N = 1298 men and women. Patients years old with or without type 2 diabetes at baseline. Reprinted with permission from Kuusisto J et al. Diabetes. 1994;43:
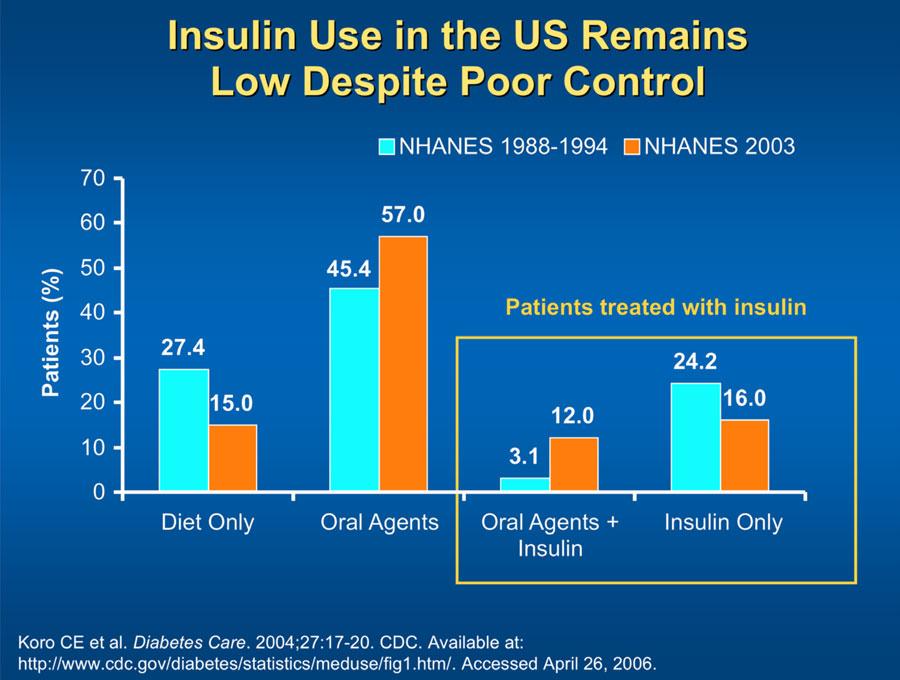
6 A1C Goals Unmet in Majority of Patients With Diabetes % have A1C >10% A1C (%) 64.2% of patients with type 2 diabetes have A1C 7% % have A1C >9% 37.2% have A1C >8% ADA recommended target (<7%) 3 ACE recommended target (<6.5%) 4 Upper limit of normal range (6%) 1. Data from Saydah SH, et al. JAMA. 2004; 291: Calculated from Koro CE, et al. Diabetes Care. 2004; 27: Data from ADA. Diabetes Care. 2003; 26(suppl 1):S33-S50 4. Data from ACE. Endocrine Practice Average Glucose A1C eag (mg/dl) A1c eag

 Biguanides: hepatic glucose output TZD: insulin sensitivity Alpha-glucosidase inhibitors: Slow the absorption of dietary starches SFU: insulin")
7 Standard of Care Diet- refer to dietitian Exercise- daily Hypertension control Hyperlipidemia control Quit smoking ASA Home glucose monitoring Education- see a CDE! Traditional Treatment Options for Diabetes Increased Beta-Cell Workload (Insulin Resistance) Diminished Beta-Cell Response (Insulin (Insulin Deficiency) Deficiency) Biguanides: hepatic glucose output TZD: insulin sensitivity Alpha-glucosidase inhibitors: Slow the absorption of dietary starches SFU: insulin secretion Meglitinides: insulin secretion Insulin: Exogenous replacement Adapted from 2005 International Diabetes Center, Minneapolis, MN All rights reserved 7



8 Effects of Oral Therapies on A1c DRUG A1c % reduction Sulfonylureas Biguanide (metformin) a-glucosidase Inhibitors DPP-4 inhibitors 0.8 Pramlintide Exenatide Thiazolidinedione 1.5 AACE Med Guidelines Clinic Practice for Management of Diabetes Mellitus
9 Thiazolidinediones- Pioglitazone, Rosiglitiazone Should they be used? Warning: can cause or exacerbate CHF in some patients. Is not recommended in pt with symptomatic heart failure, or pt with established Class III or IV heart failure. Pioglitazone- Proactive A1c lower in pioglitazone group (6.9%) 5.3% lowering of LDL, 8.9% higher HDL, 13.2% lower triglycerides 10% lowering of the primary endpoint in the active group, not statistically significant. 16% reduction in secondary endpoints Heart failure and edema were increased 9


10 INCRETINS Gut hormones that enhance insulin secretion in response to food. Glucose dependent GLP-1 secreted from L cells of the intestine Incretin Effect 10

11 Byetta Exenatide (GLP-1 analogue) Injected bid Lowers fasting and pp bg, A1c level Slows gastric emptying, weight loss T2DM not controlled with oral hypoglycemics 11
12 Improvement in CV Risk Factors With 3.5 y of Exenatide Parameter Triglycerides (mg/dl) Baseline (Mean ± SD) 225±142 Δ Baseline (Mean ± SE) -44.4± % CI to Total cholesterol (mg/dl) 184± ± to -4.6 HDL-C (mg/dl) 39±10 8.5± to 9.7 LDL-C (mg/dl) 114± ± to -6.1 Systolic blood pressure (mmhg) 129±13-3.5± to -1.0 Diastolic blood pressure (mmhg) 79±8-3.3± to y y completers, N = 151 Kendall D, et al. Diabetes. 2007:56(Suppl1):A149 Amylin Is Co-Secreted With Insulin 30 Meal Meal Meal Insulin Amylin Plasma Amylin (pm) Plasma Insulin (pm) 5 7 am 12 noon 5 pm Midnight Time (24 h) 0 Healthy adults; n = 6 Data from Kruger D, et al. Diabetes Educ 1999; 25:
13 Amylin Is Deficient in Diabetes 20 Meal Plasma Amylin (pm) Without Diabetes Late Stage Type Time After Sustacal Meal (min) Type 1 Without diabetes; n = 27 Late-stage type 2; n = 12 Type 1; n = 190 Data from Kruger D, et al. Diabetes Educ 1999; 25: Pramlinitide (Symlin) Synthetic amylin Injected before meals with insulin Lowers primarily pp bg Decreases A1c and weight Nausea is a side effect T1 and T2 DM not controlled with insulin 13
14 Pramlintide Clinical Effects TYPE 1 DIABETES COMBINED PIVOTALS Placebo + Insulin 30 or 60 μg Pramlintide TID or QID + Insulin Δ A1C (%) Δ Insulin Use (%) Δ Weight (kg) 0 Week 4 Week 13 Week 26 8 Week 4 Week 13 Week 26 1 Week 4 Week 13 Week ITT; Mean (SE); P<0.05, P<0.01, P<0.0001; Placebo + insulin, N = 538, Baseline A1C = 9.0% ; Pramlintide + insulin, N = 716, Baseline A1C = 8.9% Pramlintide Acetate Prescribing Information, 2005; Data on file, Amylin Pharmaceuticals, Inc. Data from: Whitehouse FW, et al. Diabetes Care 2002; 25: ; Ratner R, et al. Diabetic Med 2004; 21: Pramlintide Clinical Effects TYPE 2 DIABETES COMBINED PIVOTALS Placebo + Insulin 120 μg Pramlintide BID + Insulin Δ A1C (%) Δ Insulin Use (%) Δ Weight (kg) 0 Week 4 Week 13 Week 26 8 Week 4 Week 13 Week 26 1 Week 4 Week 13 Week ITT; Mean (SE); P<0.01, P< Placebo + insulin, N = 284, Baseline A1C = 9.3%; Pramlintide + insulin, N = 292, Baseline A1C = 9.1% Pramlintide Acetate Prescribing Information, Data on file, Amylin Pharmaceuticals, Inc. Data from: Hollander P, et al. Diabetes Care 2003;26: ; Ratner RE, et al. Diabetes Technol Ther 2002; 4:
15 S e c t i o n 12, 12.2 Mechanism of Action of Sitagliptin Glucose Ingestion of food Release of active incretins GI tract GLP-1 and GIP JANUVIA (DPP-4 inhibitor) Inactive GLP-1 X DPP-4 enzyme Inactive GIP Pancreas Beta cells Alpha cells dependent Insulin (GLP-1and GIP) Glucosedependent Glucagon (GLP-1) Glucose uptake by peripheral tissue Hepatic glucose production Incretin hormones GLP-1 and GIP are released by the intestine throughout the day, and their levels in response to a meal. Blood glucose in fasting and postprandial states Concentrations of the active intact hormones are increased by JANUVIA (sitagliptin phosphate), thereby increasing and prolonging the actions of these hormones. S e c t i o n 14.1 Reduction of A1C : 2 Monotherapy Studies of JANUVIA at 18 Weeks Baseline A1C (%) Change in A1C, % Inclusion Criteria: 7% 10% Pooled Analysis Overall <8 8 <9 9 n=769 n=411 n= n= The magnitude of A1C lowering by strata varied by study. Reductions are placebo-subtracted. P<0.001 overall and for treatment by subgroup interactions. Combined number of patients on JANUVIA or placebo. Aschner et al. Diabetes 2006; 55:A462 15
16 16
17 Using insulin would be ideal if it could imitate the natural process. MacLeod & Campbell 1925 Insulin Insulin may be anti inflammatory Insulin suppresses NFkB binding activity Reactive oxygen species ICAM PAI-1 Lipolysis and FFA formation 17

")

18 Plasm a insuli n levels Action Profiles of Injectable Insulin Analogues Aspart, glulisine, lispro 4 6 hours Regular 6 8 hours NPH hours Ultralente hours (No longer avail) Glargine 24 hours Detemir (6-24 hrs) Hours 18
19 19


20 We have come a long way! A Revolution in Diabetes Management 20


21 Insulin pumps Who s an insulin pump candidate? 4 or more daily injections Blood glucose testing 4+ times daily Family and patient interested in pump & able to manage pump therapy Failure to achieve target A1C goal Frequent Hypoglycemia Erratic eating/lifestyle patterns Frequent DKA Blackett PR: Insulin Pump Treatment for Recurrent Ketoacidosis in Adolescence; Diabetes Care;1995;18:


22 Continuous glucose sensor 68 y/o with HbA1c 8.5 % Tests twice a day: am and pm Never has had blood glucose above 123mg/dl 22

23 CareLink Download The patient is always the one in control. You may spend about minutes with your patient face to face 4-5 x year Which leaves the patient in control 1435 minutes EVERY DAY! Teamwork is the ability to work together toward a common vision. It is the fuel that allows common people to attain uncommon results 23
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
DIABETES. Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes. November 2013
 DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
DIABETES Mary Bruskewitz APNP, MS, BC-ADM Clinical Nurse Specialist Diabetes November 2013 mbruskewitz@outlook.com Objectives Part 1 Overview of Endocrine Physiology Pathophysiology of Diabetes Diabetes
Pancreatic b-cell Dysfunction in Type 2 Diabetes ZIAD KAHWASH, M.D. Insulin resistance: Defects in Insulin Signaling
 Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Plasma insulin (mu/ml) ZIAD KAHWASH, M.D. resistance: Defects in Signaling Increased glucose production Glucose Insufficient glucose disposal X Liver glucagon insulin Pancreas Peripheral tissues (skeletal
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT STATEGIES IN DIABETES MELLITUS DIABETES. Recommendations for Adults CURRENT STRATEGIES IN DIABETES MELLITUS. Diabetes Mellitus: U.S.
 CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Diabetes Oral Agents Pharmacology. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Diabetes Oral Agents Pharmacology University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 Learning Objectives Understand the role of the utilization of free
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Julie White, MS Administrative Director Boston University School of Medicine Continuing Medical Education
 MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
MENTOR QI Diabetes Performance Improvement Initiative, Getting Patients to Goal in Glycemic Control: Current Data Julie White, MS Administrative Director Boston University School of Medicine Continuing
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption),
,") Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
Normal Fuel Metabolism Five phases of fuel homeostasis have been described A. Phase I is the fed state (0 to 3.9 hours after meal/food consumption), in which blood glucose predominantly originates from
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact DIABETES
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact DIABETES
A New Therapeutic Strategey for Type II Diabetes: Update 2008
 Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
Update on Diabetes Mellitus
 Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
Update on Diabetes Mellitus Treatment: Targeting the Incretin System Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose control Amylin Incretin Hormones New therapies
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Understanding Diabetes and Insulin Delivery Systems
 Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Page 1 This program has been supported by an educational grant from Sanofi Aventis Scott K. Stolte, Pharm.D. Associate Dean, Academic Affairs Bernard J. Dunn School of Pharmacy Shenandoah University Winchester,
Type II Diabetes Improving Blood Sugar Control. Geneva Clark Briggs, Pharm.D., BCPS
 Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
Type II Diabetes Improving Blood Sugar Control Geneva Clark Briggs, Pharm.D., BCPS Overview Importance of glucose control State of control Review available therapies Helping patients achieve control The
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
CURRENT ISSUES IN DIABETES MANAGEMENT
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2011 BMI
Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) (908)
 (908)") News Release FOR IMMEDIATE RELEASE Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) 423-6537 (908) 423-5185 Tracy Ogden (267) 305-0960 FDA Approves Once-Daily JANUVIA, the First and Only DPP-4
News Release FOR IMMEDIATE RELEASE Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) 423-6537 (908) 423-5185 Tracy Ogden (267) 305-0960 FDA Approves Once-Daily JANUVIA, the First and Only DPP-4
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Merck & Co, Inc. Announced Approval of JANUVIA TM (INN: sitagliptin), a new oral treatment of diabetes, by the US FDA
, a new oral treatment of diabetes, by the US FDA") October 23, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Phone: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Phone: +81-3-6272-1001 Merck & Co, Inc. Announced Approval of JANUVIA
October 23, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Phone: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Phone: +81-3-6272-1001 Merck & Co, Inc. Announced Approval of JANUVIA
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Metabolic Syndrome: What s so big about BIG?
 Tuesday, 10:00 11:30, A2 Objectives: Notes: Metabolic Syndrome: What s so big about BIG? Patrice Conrad pbconrad1@att.net 1. Identify advances in clinical assessment and management of selected healthcare
Tuesday, 10:00 11:30, A2 Objectives: Notes: Metabolic Syndrome: What s so big about BIG? Patrice Conrad pbconrad1@att.net 1. Identify advances in clinical assessment and management of selected healthcare
Pramlintide & Weight. Diane M Karl MD. The Endocrine Clinic & Oregon Health & Science University Portland, Oregon
 Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Pramlintide & Weight Diane M Karl MD The Endocrine Clinic & Oregon Health & Science University Portland, Oregon Conflict of Interest Speakers Bureau: Amylin Pharmaceuticals Consultant: sanofi-aventis Grant
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control
 Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
Glyceamic control is indicated by 1. Fasting blood sugar less than 126 mg/dl 2. Random blood sugar 3. HbA1c less than 6.5 % Good glycaemic control can prevent many of early type 1 DM(in DCCT trail ). UK
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
Enrique Caballero, MD Director, Latino Diabetes Initiative Joslin Diabetes Center Harvard Medical School
 New Diabetes Treatments Embryonic Stem Cells (ESC) Ectoderm Mesoderm Enrique Caballero, MD Director, Latino Diabetes Initiative Joslin Diabetes Center Harvard Medical School ESC Endoderm Pancreas Islet
New Diabetes Treatments Embryonic Stem Cells (ESC) Ectoderm Mesoderm Enrique Caballero, MD Director, Latino Diabetes Initiative Joslin Diabetes Center Harvard Medical School ESC Endoderm Pancreas Islet
Rebecca Newberry APRN MS CDE
 Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
Current Diabetes Medications Nursing Implications and Applications Rebecca Newberry APRN MS CDE Methodist Center for Diabetes and Nutritional Health Disclosures Objectives Speakers Bureaus/Consulting Board
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
I. General Considerations
 1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
1 2 3 I. General Considerations A. Type I ( Juvenile Onset or IDDM) IDDM results from autoimmune destruction of beta cells inability to secrete insulin --> ketone formation --> DKA 4 Diabetic Ketoacidosis
CE on SUNDAY Miami, FL May 31, 2009
 CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
CE on SUNDAY Miami, FL May 31, 2009 Date: Sunday, May 31, 2009 Time: 1:15 PM 2:15 PM Location: Doubletree Miami Mart/Airport Hotel Title: Speaker(s): Understanding Diabetes and Insulin Delivery Systems
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
American Diabetes Association 65 th Annual Scientific Sessions. Investor Reception June 12, 2005
 American Diabetes Association 65 th Annual Scientific Sessions Investor Reception June 12, 2005 Safe Harbor Statement > This presentation contains forward-looking statements about Amylin. Our actual results
American Diabetes Association 65 th Annual Scientific Sessions Investor Reception June 12, 2005 Safe Harbor Statement > This presentation contains forward-looking statements about Amylin. Our actual results
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Type 2 DM in Adolescents: Use of GLP-1 RA. Objectives. Scope of Problem: Obesity. Background. Pathophysiology of T2DM
 Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Helpful Hints for Taking Care of Your Diabetes. Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center
 Helpful Hints for Taking Care of Your Diabetes Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center Objectives How big of a problem is diabetes? What is diabetes? How is
Helpful Hints for Taking Care of Your Diabetes Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center Objectives How big of a problem is diabetes? What is diabetes? How is
22 Emerging Therapies for
 22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
22 Emerging Therapies for Treatment of Type 2 Diabetes Siddharth N Shah Abstract: The prevalence of Diabetes is progressively increasing world-wide and the growth of the disease in our country is phenomenal.
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Addressing Addressing Challenges in Type 2 Challenges in Type 2 Diabetes Diabetes Speaker:
 Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Oral and Injectable Medication Options for Diabetes Treatment
 Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Oral and Injectable Medication Options for Diabetes Treatment Presented by: Dr. Daphne E. Smith, Pharm.D., CDE Clinical Assistant Professor/Clinical Pharmacist-University of Illinois at Chicago College
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Drugs used in Diabetes. Dr Andrew Smith
 Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Drugs used in Diabetes Dr Andrew Smith Plan Introduction Insulin Sensitising Drugs: Metformin Glitazones Insulin Secretagogues: Sulphonylureas Meglitinides Others: Acarbose Incretins Amylin Analogues Damaglifozin
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION
 SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
SIMPLICITY IN T2DM MANAGEMENT WITH DPP4 INHIBITORS: SPECIAL POPULATION DR ROSE ZHAO-WEI TING ( 丁昭慧醫生 ) MBBS (HK), MRCP (UK), FHKCP, FHKAM (MEDICINE) Specialist in Endocrinology, Diabetes and Metabolism
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Treating Type 2 Diabetes with Bariatric Surgery. Goal of Treating T2DM. Remission of T2DM with Bariatric
 Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
Treating Type 2 Diabetes with Bariatric Surgery Number (in Millions) of Persons with Diagnosed Diabetes, United States, 198 25 The number of Americans with diabetes increased from 5.6 to 15.8 million Guilherme
No disclosures. Diabetes Test Topics. Case #1. Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan
 Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan No disclosures Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March
Diabetes Family Medicine Board Review: Improving Clinical Care Across the Lifespan No disclosures Sarah Kim, MD Assistant Clinical Professor of Clinical Medicine, UCSF Division of Endocrinology, SFGH March