Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
|
|
|
- Colin Newman
- 5 years ago
- Views:
Transcription
1
2 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell function Insulin resistance Impaired glucose tolerance Ominous octet T2DM Ongoing hyperglycemia DEATH Ongoing, worsening macrovascular and microvascular complications Hypertension Endothelial dysfunction Hyperinsulinemia HDL-C, Triglycerides Eye, nerve, and kidney damage Atherosclerosis Myocardial infarction Cardiovascular event Blindness Chronic renal failure Amputation Disability HDL-C = high density lipoprotein-cholesterol; T2DM = type 2 diabetes mellitus.
3
4 Relative Risk A1C and Microvascular Complications: DCCT Retinopathy Nephropathy Neuropathy Microalbuminuria DCCT Research Group. N Engl J Med. 1993;329:977. Skyler J. Endocrinol Metab Clin North Am. 1996;25:243. A1C (%) A1C = glycated hemoglobin; DCCT = Diabetes Control and Complications Trial.


5 UKPDS: Benefits of Glycemic Control Every 1% decrease in A1C led to significant reductions in diabetes-related complications 14% 21% 37% 43% Risk of myocardial infarction Risk of diabetesrelated death Risk of microvascular complications Risk of amputation or PVD Death Decrease was statistically significant for all comparisons shown UKPDS: United Kingdom Prospective Diabetes Study Stratton IM et al. BMJ. 2000;321:


6 UKPDS: Follow-up A1C Mean A1C levels for patients originally assigned to receive either sulfonylurea insulin or conventional therapy are shown Clinical data were not available in years 6 through 10 (when questionnaires were used) UKPDS: United Kingdom Prospective Diabetes Study Holman R et al NEJM, 2008;359:


7 UKPDS: Follow-up All-cause mortality A similar long-term benefit in terms of reduced mortality risk was observed for patients who received initial intensive treatment UKPDS: United Kingdom Prospective Diabetes Study Holman R et al NEJM, 2008;359:



8 Myocardial Infarction Hazard Ratio UKPDS 10-year follow-up (fatal or non-fatal myocardial infarction or sudden death) Intensive (metformin) vs. conventional glucose control Conventional Intensive Δ Holman R et al NEJM, 2008;359:

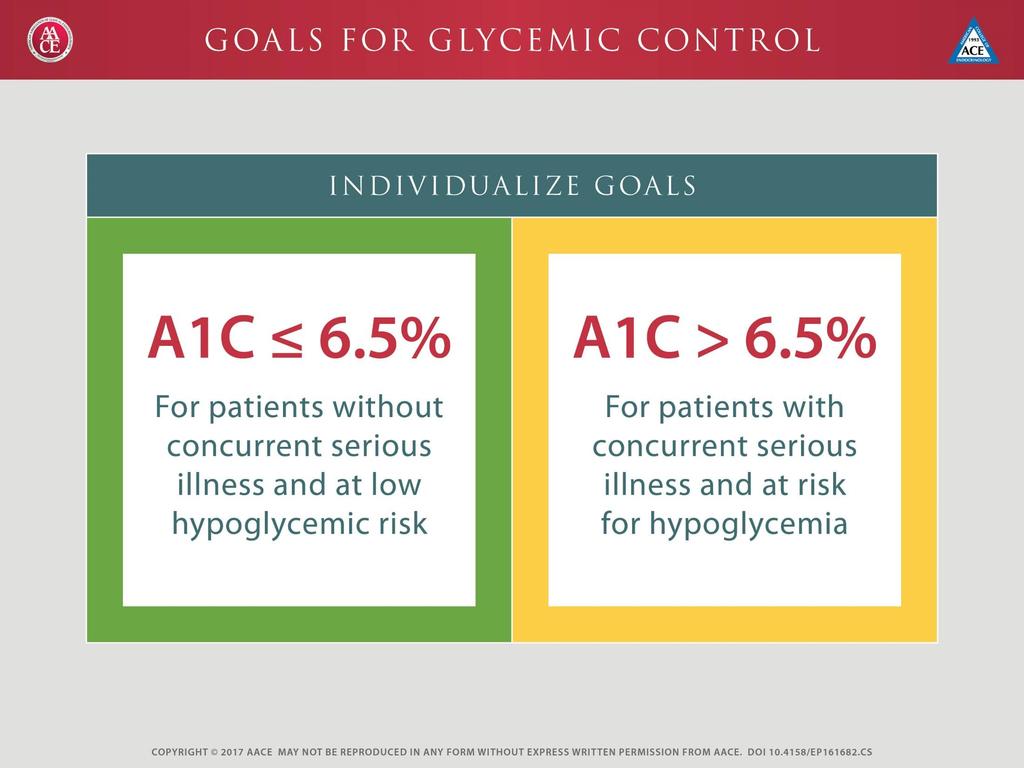
9 Glycemic Management of Type 2 Diabetes: Treatment Goals Lowering A1C Preventing Hypoglycemia Individualized Algorithm
10 Risk of Hypoglycemia Plays a significant role in choice of agents in AACE algorithm For patients at highest risk of hypoglycemia, may consider close evaluation of agents chosen as well as therapeutic goal Patients with type 2 diabetes at highest risk of low blood glucose include those with: Diabetes duration >15 years Advanced macrovascular disease Hypoglycemia unawareness Limited life expectancy Severe comorbidities Garvey et al. Endocr. Pract. 2016;22 (Suppl 3); AACE/ACE Diabetes Algorithm Endocr. Pract. 2015;21 (Suppl 1); AACE/ACE Obesity Algorithm Part 2
11

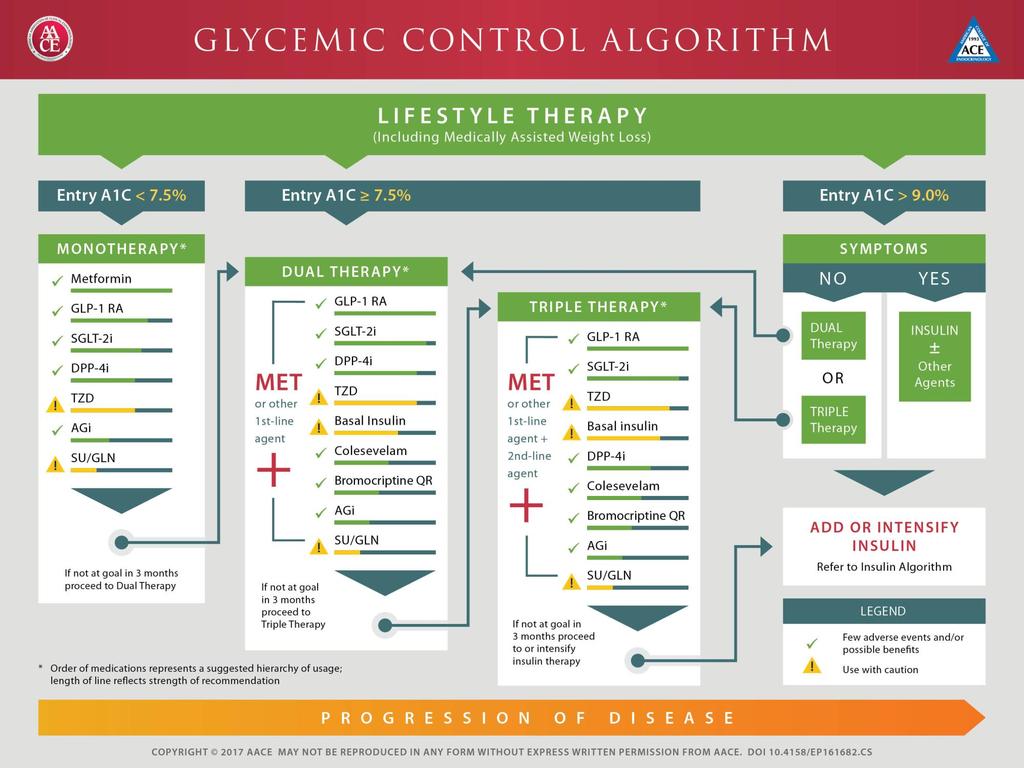
12 Algorithm To Achieve Glycemic Goals Baseline A1C 6.5% - 7.5% Monotherapy may be effective in this range Metformin first choice for monotherapy if no contraindications Consider DPP-4 if PP and FPG, GLP-1 if PP, TZD if metabolic syndrome or NAFLD, AGI if PP Do not recommend secretagogue (SU or glinide) in this range due to risk of hypoglycemia; short-lived effect If monotherapy is unsuccessful, move on to dual oral rx; often need to augment reduction in PP BG to get to goal in this A1C range DPP-4=dipeptidyl peptidase-4; PP=post-prandial; FPG=fasting plasma glucose; GLP- 1 = glucagon-like peptide-1; TZD=thiazolidinedione; NAFLD=non-alcoholic fatty liver disease; AGI=alpha-glucosidase inhibitor; SU=sulfonylurea; A1C=glycated hemoglobin; SGLT-2=sodium glucose transport-2 AACE/ACE Comprehensive Type 2 Diabetes Management Algorithm Endocr Pract.2017,doi: /EP CS. Inzucchi S et al. Diabetes Care 2015;38:

13 Algorithm To Achieve Glycemic Goals Baseline A1C 7.6% - 9.0% Dual therapy with metformin provides superior glycemic control over metformin alone. If dual oral rx is unsuccessful, consider triple therapy If triple oral rx fails to achieve A1C goal, initiate insulin GLP-1 RA = glucagon-like peptide-1 receptor agonist DPP4-i=dipeptidyl peptidase 4 inhibitor TZD=thiazolidinedione SGLT-2=sodium glucose cotransporter 2 inhibitor QR=quick-release AG-i=alpha-glucosidase inhibitor SU=sulfonylurea GLN=glinide AACE/ACE Comprehensive Type 2 Diabetes Management Algorithm Endocr Pract.2017,doi: /EP CS. Inzucchi S et al. Diabetes Care 2015;38:

14 Algorithm to Achieve Glycemic Goals Baseline A1C > 9.0% If patient is asymptomatic with recent onset of disease and drug naïve, may consider starting with dual or triple oral regimens If symptomatic, start insulin Once A1C has improved to <7.5%, consider initiation of dual oral therapy with tapering and possible discontinuation of insulin rx AACE/ACE Comprehensive Type 2 Diabetes Management Algorithm Endocr Pract.2017,doi: /EP CS.

15 Current Antihyperglycemic Medications Insulin Replacement Therapy Glinides Restore postprandial insulin patterns Sulfonylureas Generalized insulin secretagogue TZDs Reduce peripheral insulin resistance Biguanide Reduce hepatic insulin resistance GLP-1 Analogs Stimulate cells, suppress glucagon 12 Groups with Different Mechanisms of Action SGLT-2 Inhibitors Block renal glucose reabsorption DPP-4 Inhibitors Restore GLP-1 Level Amylin Analog Suppress glucagon -Glucosidase Inhibitors Delay CHO absorption Dr. Phil Levy Colesevelam Bile acid sequestrant Bromocriptine Hypothalamic pituitary reset
16

17 Primary Risk Factors for CVD: Treatment Goals Hyperglycemia FPG / preprandial glucose PPG A1C mg/dl <180 mg/dl <7%, or lowest possible without unacceptable hypoglycemia Hypertension Blood pressure <140/80 mmhg, or further lowering if tolerated by patients Dyslipidemia LDL HDL Triglycerides <100 mg/dl, patients with diabetes <70 mg/dl, very high risk patients with diabetes and CVD >40 mg/dl, men; >50 mg/dl, women <150 mg/dl A1C = glycated hemoglobin; CVD = cardiovascular disease; FPG = fasting plasma glucose; HDL = high density lipoprotein; LDL = low density lipoprotein; PPG = postprandial plasma glucose. AACE Algorithm 2016 American Diabetes Association, Diabetes Care 2016;39 (Suppl 1).
18 The Steno-2 Study: Synergy in Care Treating Glucose, Blood Pressure, and Lipids A follow-up study, conducted 21 years after the original trial, found a median gain of 7.9 years of life in Steno-2 patients originally provided with intensive treatment. CABG = coronary artery bypass graft; PCI = percutaneous coronary intervention. Gæde P, et al. Diabetologia. 2016;59: Gæde P, et al. NEMJ. 2003;348(5):
Welcome and Introduction
 Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Update on Oral Agents for T2DM and Obesity
 Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved,
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Update on Oral Agents for T2DM and Obesity
 AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
AACE 2016 To AACE Update on Oral Agents for T2DM and Obesity This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus Type 2 Evidence-Based Drivers
 This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
This module is supported by an unrestricted educational grant by Aventis Pharmaceuticals Education Center. Copyright 2003 1 Diabetes Mellitus Type 2 Evidence-Based Drivers Driver One: Reducing blood glucose
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Application of the Diabetes Algorithm to Patients
 Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
Objectives 2/13/2013. Figuring out the dose. Sub Optimal Glycemic Control: Moving to the Appropriate Treatment
 Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Sub Optimal Glycemic Control: Moving to the Appropriate Treatment Judy Thomas, MSN, FNP-BC Holt and Walton, Rheumatology and Endocrinology Objectives Upon completion of this session you will be better
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM. Sherwin D Souza, MD, FACE
 AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
AACE/ACE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM Sherwin D Soza, MD, FACE Prediabetes Treatment Algorithm T2DM = type 2 diabetes mellits BP = blood pressre CVD = cardiovasclar disease
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 ( ) 가천의대길병원내분비대사내과
 가천의대길병원내분비대사내과") 효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
효과적인경구혈당강하제의조합은? 대한당뇨병학회제 17 차연수강좌 (2011.10.30.) 가천의대길병원내분비대사내과 박이병 내용 배경 경구혈당강하제의병합이왜필요한가? (WHY?) 경구혈당강하제의병합은언제시작하나? (WHEN?) 경구혈당강하제의병합은어떻게하는것이좋은가?(HOW) 맺음말 배경 : drugs for treating diabetes In 1995 :
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Combination treatment for T2DM
 Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Combination treatment for T2DM Date of approval: December 2016 SAGLB.DIA.16.08.0657 Abbreviations ADA: American Diabetes Association CVD: Cardiovascular disease DPP-4: Dipeptidyl Peptidase-4 EASD: European
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Treatment of Type 2 Diabetes: What Have We Learned? AACE Diabetes Algorithm. ADOPT Trial 6/13/2012
 Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
Treatment of Type 2 Diabetes: What Have We Learned? Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering needed, patientspecific
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Diabetes Mellitus in Older Adults. Presenter Disclosure Information
 Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus in Older Adults Medha Munshi, M.D. Joslin Diabetes Center Beth Israel Deaconess Medical Center Harvard Medical School Presenter Disclosure Information Medha Munshi Research grant from
Diabetes Mellitus: Overview and Guidelines
 Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Fixed dose combination for Trusted Diabetes Control Lobna Farag Eltooy Head of Internal Medicine Department Assiut University
 Fixed dose combination for Trusted Diabetes Control By Lobna Farag Eltooy Head of Internal Medicine Department 1 Assiut University 3/18/2018 3/18/2018 3/18/2018 Diabetes Complications with Increasing HbA1c
Fixed dose combination for Trusted Diabetes Control By Lobna Farag Eltooy Head of Internal Medicine Department 1 Assiut University 3/18/2018 3/18/2018 3/18/2018 Diabetes Complications with Increasing HbA1c
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Diabetes Overview. How Food is Digested
 Diabetes Overview You are The Teacher, The Coach and the Fan Pathophysiology of Diabetes Complications Know the Numbers Treatment Can Good Control Make a Difference? Can Tight Control Be too Tight? How
Diabetes Overview You are The Teacher, The Coach and the Fan Pathophysiology of Diabetes Complications Know the Numbers Treatment Can Good Control Make a Difference? Can Tight Control Be too Tight? How
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type 2 Diabetes
 Draft Comparative Effectiveness Review Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type Diabetes Prepared for: Agency for Healthcare Research and Quality U.S. Department
Draft Comparative Effectiveness Review Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type Diabetes Prepared for: Agency for Healthcare Research and Quality U.S. Department
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy
 Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Old oral antidiabetic agents in the armamentarium of diabetes mellitus treatment: Safety and efficacy Melpomeni Peppa Assistant Professor of Endocrinology 2 nd Dept of Internal Medicine-Propaedeutic, Athens
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Type 2 Diabetes. Treat to: limit complications maintain quality of life Improve survival
 Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Type 2 Diabetes Treat to: limit complications maintain quality of life Improve survival 1 Criteria for the diagnosis of diabetes 1. HbA1C 6.5% (rounded to 50mmol/mol). 2. FPG 7.0 mmol/l. 3. 2-h plasma
Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion
 Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion Om P. Ganda, MD; Kirit Tolia, MD, FACE Postcardiac Follow-up in a 66-Year-Old Man Slide 1. Dr. Ganda: Now we will present a case
Clinical Approach to Achieving Treatment Targets: Case Vignette Discussion Om P. Ganda, MD; Kirit Tolia, MD, FACE Postcardiac Follow-up in a 66-Year-Old Man Slide 1. Dr. Ganda: Now we will present a case
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
9/29/14. Disclosures. Nothing to disclose
 Disclosures Nothing to disclose 1 Pharmacist Objectives 1. Select individualized glucose goals for patients with type 2 diabetes 2. List advantages and disadvantages of various classes of medications used
Disclosures Nothing to disclose 1 Pharmacist Objectives 1. Select individualized glucose goals for patients with type 2 diabetes 2. List advantages and disadvantages of various classes of medications used
Current Controversies in Diabetes Control
 Current Controversies in Diabetes Control Dara P. Schuster, MD, FACE ADA, AACE/ACE, and ACP Guidelines: Treatment Goals for A1C, FPG, and PPG Parameter Normal 1,2 Level ADA 3 Goal AACE/ACE 2 Goal ACP 4
Current Controversies in Diabetes Control Dara P. Schuster, MD, FACE ADA, AACE/ACE, and ACP Guidelines: Treatment Goals for A1C, FPG, and PPG Parameter Normal 1,2 Level ADA 3 Goal AACE/ACE 2 Goal ACP 4
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease
 The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Presented By: Creative Educational Concepts, Inc. Lexington, KY
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
Glycemic control A combination of life style interaction and the use of drugs
 Multifactorial management to reduce cardiovascular risk in patients with diabetes mellitus Glycemic control A combination of life style interaction and the use of drugs Eberhard Standl Munich Diabetes
Multifactorial management to reduce cardiovascular risk in patients with diabetes mellitus Glycemic control A combination of life style interaction and the use of drugs Eberhard Standl Munich Diabetes
1. Pharmacokinetics. When is steady state achieved? Steady-state was reached after 4 to 5 days of once-daily dosing with Sulisent 100 mg to 300mg.
 1. Pharmacokinetics How is Sulisent metabolized? Sulisent has a novel mechanism of action that targets the kidneys and allows for excess glucose excretion resulting in urinary calorie loss. Sulisent is
1. Pharmacokinetics How is Sulisent metabolized? Sulisent has a novel mechanism of action that targets the kidneys and allows for excess glucose excretion resulting in urinary calorie loss. Sulisent is
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
5/18/2011. Diabetes: Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Diabetes: 2011 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Pre Test Questions 1. There is evidence that lowering A1c reduces the risk of both micro- and macrovascular disease. A. True
Diabetes: 2011 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Pre Test Questions 1. There is evidence that lowering A1c reduces the risk of both micro- and macrovascular disease. A. True
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION
 OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
AACE/ACE Consensus Statement
 AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic
AACE/ACE Consensus Statement Statement by an American Association of Clinical Endocrinologists/ American College of Endocrinology Consensus Panel on Type 2 Diabetes Mellitus: An Algorithm for Glycemic