Postgastrectomy Syndromes
|
|
|
- Brook Chapman
- 5 years ago
- Views:
Transcription
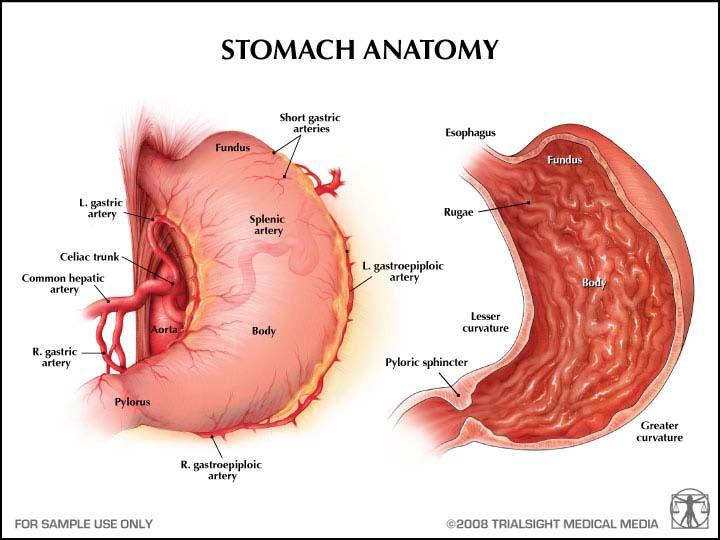
1 Postgastrectomy Syndromes
2
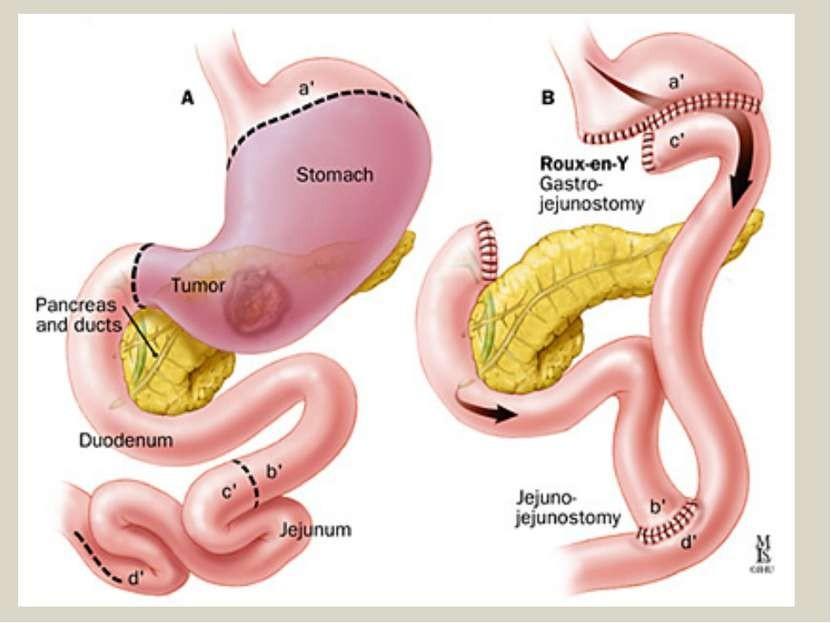
3 Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer disease, cancer, or weight loss (bariatric). The surgical procedures include Billroth-I, Billroth-II, and Roux-en-Y gastric bypass.

 for")
4 History of gastrectomy 1881 Theodor Billroth first to successfully resected the distal stomach Patient had distal gastric cancer Continuity re-established by gastroduodenostomy (Billroth I) Patient recovered, but died 4 months later with abdominal carcinomatosis 1885 Billroth performs successful distal gastrectomy & gastrojejunostomy (Billroth II) for gastric cancer

5 Billroth I Billroth II
6
7 Postgastrectomy syndromes include small capacity dumping syndrome bile gastritis afferent loop syndrome efferent loop syndrome anemia metabolic bone disease.
8 Dumping syndrome is the effect of altered gastric reservoir function, abnormal postoperative gastric motor function, and/or pyloric emptying mechanism. Clinically significant dumping syndrome occurs in approximately 10% of patients after any type of gastric surgery and in up to 50% of patients after laparoscopic Roux-en-Y gastric bypass. Dumping syndrome can be separated into early and late forms, depending on the occurrence of symptoms in relation to the time elapsed after a meal.
9 Both forms occur because of the rapid delivery of large amounts of osmotically active solids and liquids to the duodenum. This is a direct result of alterations in the storage function of the stomach and/or pyloric emptying mechanism.
10
11 Early dumping Rapid emptying of gastric contents into the small intestine or colon may result in high amplitude propagated contractions and increased propulsive motility, thereby contributing to the diarrhea seen in persons with the dumping syndrome. Symptoms of early dumping syndrome occur minutes after a meal. Symptoms are believed to result from accelerated gastric emptying of hyperosmolar contents into the small bowel. This leads to fluid shifts from the intravascular compartment into the bowel lumen, resulting in rapid small bowel distention and an increase in the frequency of bowel contractions.
12 Early dumping Bowel distention may be responsible for GI symptoms, such as crampy abdominal pain, bloating, and diarrhea. Intravascular volume contraction due to osmotic fluid shifts is perhaps responsible for the vasomotor symptoms, such as tachycardia and lightheadedness.
13 Early dumping Early dumping systemic symptoms : Desire to lie down Rapid, strong heartbeat Fatigue Faintness Syncope Sweating Headache Flushing Early dumping abdominal symptoms : Epigastric fullness Diarrhea Nausea Abdominal spasm Borborygmi (rumbling or gurgling noise made by the movement of fluid and gas in the intestines).
14 Late dumping Late dumping occurs 1-3 hours after a meal. The pathogenesis is thought to be related to the early development of hyperinsulinemic (reactive) hypoglycemia. Rapid delivery of a meal to the small intestine results in an initial high concentration of carbohydrates in the proximal small bowel and rapid absorption of glucose. This is countered by a hyperinsulinemic response. The high insulin levels stay for longer period and are responsible for the subsequent hypoglycemia. Intrajejunal glucose induces a higher insulin release than does the intravenous infusion of glucose.
15 Late dumping symptoms are as follows: Perspiration Shakiness Difficulty to concentrate Decreased consciousness Hunger
16 Approach Considerations Signs and symptoms can be elicited with the glucose challenge test (50 g oral glucose). A positive result from a hydrogen breath test after ingestion of glucose is also 100% sensitive. A gastric emptying study may be helpful to document rapid gastric emptying. An endoscopy or a barium study can be helpful in discerning the anatomy.
17 Diet Dietary prohibitions and instructions are very important in the management of dumping syndrome. Note the following: Daily energy intake is divided into 6 meals. Fluid intake during and with meals is restricted. Avoiding liquids for at least half an hour after a meal is helpful. Simple sugars are best avoided. Milk and milk products are generally not tolerated and should be avoided. Because carbohydrate intake is restricted, protein and fat intake should be increased to fulfill energy needs. Most patients have relatively mild symptoms and respond well to dietary manipulations. In some patients with postprandial hypotension, lying supine for 30 minutes after meals may delay gastric emptying and also increase venous return, thereby minimizing the chances of syncope.
18 Medical Care: Octreotide. Somatostatin and its synthetic analogue octreotide have been used with short-term success in patients with dumping syndrome, but the long-term efficacy of octreotide is much less favorable. They exert a strong inhibitory effect on the release of insulin and several gut-derived hormones. The effectiveness of octreotide in controlling the symptoms of both early and late dumping has been demonstrated in several randomized control trials. The usual initial dose of octreotide is 50 mcg administered subcutaneously 30 minutes prior to each meal. The dose may be increased if smaller doses are not effective; however, higher doses are seldom effective if the smaller doses do not work.
19 Medical Care: Octreotide. The mechanisms of action of octreotide in dumping syndrome are as follows: Delay in the accelerated initial gastric emptying Delay in small intestinal transit time Inhibition of enteral hormone release Induction of a fasting intestinal pattern Inhibition of insulin release Splanchnic vasoconstriction Inhibition of postprandial vasodilation
20 Surgical Care Several surgical procedures have been designed to rectify the symptoms of dumping: surgical narrowing of the gastrojejunal stoma conversion of Billroth II anastomosis to Billroth I gastroduodenostomy jejunal interposition ( isoperistaltic loop, reversed 10- cm jejunal segments ) conversion to Roux-en-Y gastrojejunostomy pyloric reconstruction.
21 Summary of remedial operations For patients with prior pyloroplasty, pyloric reconstruction should be the initial remedial operation. For patients with Billroth I and Billroth II gastrectomies, Roux-en-Y reconstruction is the simplest and most effective therapy. For patients who already have a Roux-en-Y reconstruction, a 10-cm antiperistaltic jejunal loop should be interposed.
22 Conclusion Dumping syndrome is a common postsurgical complication after gastric surgery. The symptoms of dumping produce considerable morbidity. Fortunately, the indications for gastric surgery are declining, although the need for gastric surgery in emergency cases has not changed. Initially, patients with this condition should be treated medically with dietary modifications and octreotide. Close attention should be given to the patient's nutritional status. If medical management fails to provide adequate symptom relief, remedial surgery should be offered with the understanding that even surgical intervention may not be successful.
23 Afferent loop syndrome (ALS) Afferent loop syndrome (ALS) is a purely mechanical complication that infrequently occurs following the construction of a gastrojejunostomy. Creation of an anastomosis between the stomach and jejunum leaves a segment of the small bowel, most commonly consisting of duodenum and proximal jejunum, lying upstream from the gastrojejunostomy. This limb of intestine transfers bile, pancreatic juices, and other proximal intestinal secretions toward the gastrojejunostomy and is thus termed the afferent loop.

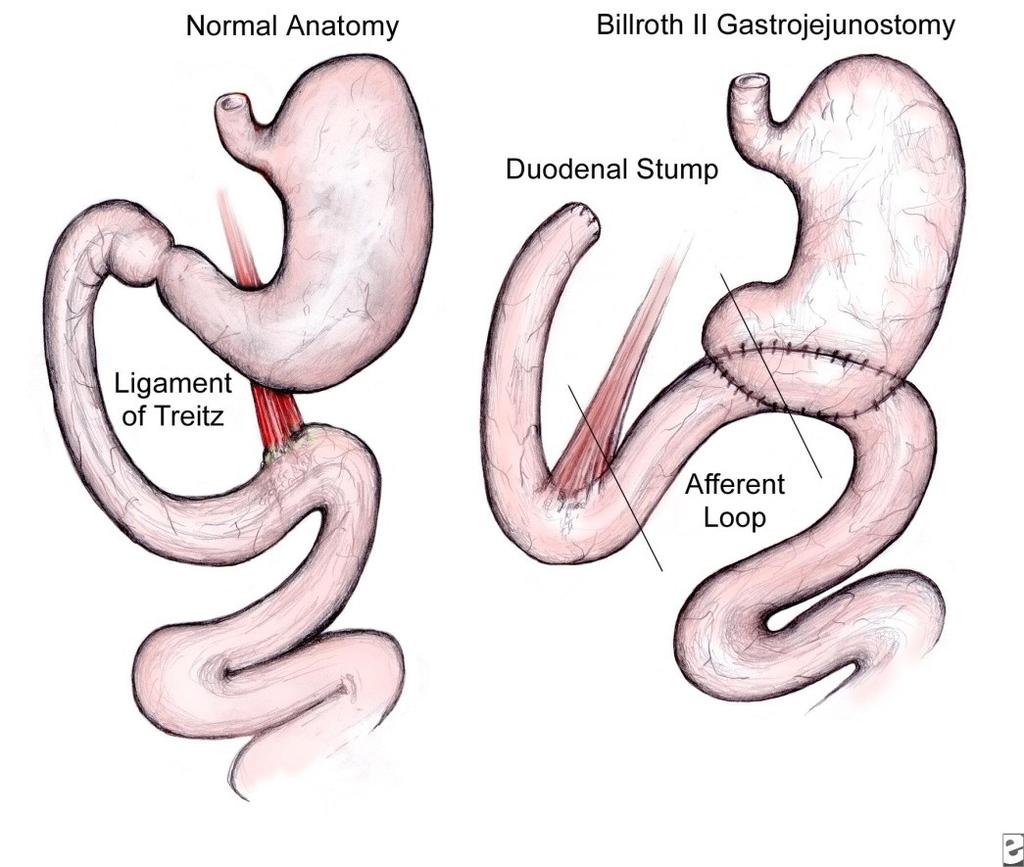
24 Types of reconstractions after Billroth II gastric resection
25
26 Symptoms Symptoms associated with ALS are caused by increased intraluminal pressure and distention due to accumulation of enteric secretions in a partially or completely obstructed afferent limb. ALS is one of the main causes of duodenal stump blowout in the early postoperative period and is also an etiology for postoperative obstructive jaundice, ascending cholangitis, and pancreatitis due to transmission of high pressures back into the biliopancreatic ductal system. High luminal pressures and distention increase bowel wall tension in the afferent loop and can lead to ischemia and gangrene with subsequent perforation and peritonitis.
27 Secondarily, prolonged stasis and pooling of secretions with partial obstruction facilitate bacterial overgrowth in the afferent loop. [2] Bacteria deconjugate bile acids, which can lead to steatorrhea, malnutrition, and vitamin B-12 deficiency leading to megaloblastic anemia. The severity at presentation mainly depends on the degree and duration of obstruction. The pathophysiology and signs and symptoms associated with ALS result from partial or complete obstruction of the afferent loop. Patients with ALS may present with an acute, completely obstructed form or with a chronic, partially obstructed form. The syndrome can manifest at any time from the first postoperative day to many years after surgery.
28 Etiology of ALS Each of the following postoperative conditions can cause ALS in a patient with a gastrojejunostomy: Compression of the afferent loop by postoperative adhesions Internal hernia (eg, through a mesocolic defect) Volvulus of the intestinal segment Enteroenteral or enterogastric intussusception Kinking of the afferent limb at the gastrojejunostomy
29 Patients have an increased chance of developing ALS if one or more of the following conditions is met: The jejunal portion of the afferent limb is longer than 30-40cm in length. The gastrojejunostomy is placed in an antecolic position instead of a retrocolic position. Mesocolic defects are not properly closed after construction of a retrocolic gastrojejunostomy.
30 Physical Examination Physical examination can reveal one or more of the following findings: An ill-defined mass in the right upper abdominal quadrant may be present in one-third of patients with acute ALS. Localized midepigastric or right upper abdominal quadrant tenderness Peritonitis and/or a rigid abdomen if necrosis or perforation of the bowel wall has occurred Jaundice Signs of pancreatitis (upper abdominal pain radiating to the flank or back)
31 Surgical treatment Billroth I gastroduodenostomy This procedure creates a direct anastomosis between the stomach and duodenum. It is the most physiologic procedure and is therefore the operation of choice. Several factors may preclude its use, including previous subtotal gastrectomy or extensive scarring around the duodenum. In these situations, the surgeon may be unable to gain enough mobility on the stomach and duodenum to create an anastomosis without excessive tension. Roux-en-Y gastrojejunostomy Jejunal segment interposition (between the gastric remnant and duodenum to create a modified Billroth I type anastomosis) Resection of the redundant portion of the afferent jejunal loop
Chronic abdominal pain after RYGB A management guide
 OBES 21 st October 2017 Chronic abdominal pain after RYGB A management guide Dr Chun-Hai Tan MBBS, Masters of Medicine (Surgery), FRCS (Edinburgh) Consultant Surgeon Metabolic & Bariatric Surgery, Minimally
OBES 21 st October 2017 Chronic abdominal pain after RYGB A management guide Dr Chun-Hai Tan MBBS, Masters of Medicine (Surgery), FRCS (Edinburgh) Consultant Surgeon Metabolic & Bariatric Surgery, Minimally
OPERATIVE TREATMENT OF ULCER DISEASE
 Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 8 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Imaging findings in complications of bariatric surgery.
 Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
Imaging findings in complications of bariatric surgery. Poster No.: C-1791 Congress: ECR 2012 Type: Educational Exhibit Authors: A. Fernandez Alfonso, G. Anguita Martinez, D. C. Olivares Morello, C. García
Use of the Henley loop for postvagotomy diarrhea
 Use of the Henley loop for postvagotomy diarrhea Sharon Grundfest, M.D. Caldwell B. Esselstyn, Jr., M.D. Department of General Surgery D. Roy Ferguson, M.D. Department of Gastroenterology Postvagotomy
Use of the Henley loop for postvagotomy diarrhea Sharon Grundfest, M.D. Caldwell B. Esselstyn, Jr., M.D. Department of General Surgery D. Roy Ferguson, M.D. Department of Gastroenterology Postvagotomy
Commonly Performed Bariatric Procedures in Singapore. Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital
 Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Commonly Performed Bariatric Procedures in Singapore Lin Jinlin Associate Consultant General, Upper GI and Bariatric Surgery Changi General Hospital Scope 1. Introduction 2. Principles of bariatric surgery
Laparoscopic Gastric Bypass Information
 1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
1441 Constitution Boulevard, Salinas, CA 93906 (831) 783-2556 www.natividad.com/weight-loss (Roux-en-Y Gastric Bypass) What is gastric bypass surgery? Gastric bypass surgery, a type of bariatric surgery
Adipocytes, Obesity, Bariatric Surgery and its Complications
 Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Adipocytes, Obesity, Bariatric Surgery and its Complications Daniel C. Morris, MD, FACEP, FAHA Senior Staff Physician Department of Emergency Medicine Objectives Basic science of adipocyte Adipocyte tissue
Postgastrectomy and Postvagotomy Syndromes
 H. D. Becker W.F. Caspary Postgastrectomy and Postvagotomy Syndromes With 84 Figures (Mainly in Two Colors) Springer-Verlag Berlin Heidelberg New York 1980 Professor Dr. med. H. D. Becker KlInik und PolIklImk
H. D. Becker W.F. Caspary Postgastrectomy and Postvagotomy Syndromes With 84 Figures (Mainly in Two Colors) Springer-Verlag Berlin Heidelberg New York 1980 Professor Dr. med. H. D. Becker KlInik und PolIklImk
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor
 Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Gastrointestinal Surgery for Severe Obesity 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
SIBO
 SIBO What is it? Small Intestinal Bowel Overgrowth A chronic bacterial infection of the small intestine Caused by bad bacteria such as E Coli and Clostridium migrating to the small intestine There is not
SIBO What is it? Small Intestinal Bowel Overgrowth A chronic bacterial infection of the small intestine Caused by bad bacteria such as E Coli and Clostridium migrating to the small intestine There is not
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS
 Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
Bariatric Surgery: How complex is this? Pradeep Pallati, MD, FACS, FASMBS Nothing to Disclose Types of Bariatric Surgery Restrictive Malabsorptive Combination Restrictive and Malabsorptive Newer Endoluminal
SURGICAL MANAGEMENT OF MORBID OBESITY
 Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Greenfield, Lazar J., Mulholland, Michael W., Oldham, Keith T., Zelenock, Gerald B., Lillemoe, Keith D. Surgery: Scientific Principles & Practice,
Malabsorption: etiology, pathogenesis and evaluation
 Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Gut involvement in PoTS an overview
 Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Gut involvement in PoTS an overview Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology Case Hx * 28 year old lady presents with a long hx of constipation
Small-Bowel and colon Transit. Mahsa Sh.Nezami October 2016
 Small-Bowel and colon Transit Mahsa Sh.Nezami October 2016 Dyspeptic symptoms related to dysmotility originating from the small bowel or colon usually include : Abdominal pain Diarrhea Constipation However,
Small-Bowel and colon Transit Mahsa Sh.Nezami October 2016 Dyspeptic symptoms related to dysmotility originating from the small bowel or colon usually include : Abdominal pain Diarrhea Constipation However,
Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, ,
 IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP
 Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
Gut complications in autonomic dysfunction Qasim Aziz, PhD, FRCP Centre for Neuroscience and Trauma Wingate Institute of Neurogastroenterology GI involvement in autonomic dysfunction Conditions Diabetes
Home Total Parenteral Nutrition for Adults
 Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Home Total Parenteral Nutrition for Adults Policy Number: Original Effective Date: MM.08.007 05/21/1999 Line(s) of Business: Current Effective Date: PPO, HMO, QUEST Integration 05/27/2016 Section: Home
Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications
 Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications Poster No.: C-1323 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Tincey, A. N. Tavare, A.
Managing obesity and the gastric bypass: understanding anatomy and major postoperative complications Poster No.: C-1323 Congress: ECR 2015 Type: Educational Exhibit Authors: S. Tincey, A. N. Tavare, A.
Complications and management of upper GI 高雄醫學大學附設醫院胃腸及一般外科謝建勳
 Complications and management of upper GI surgery 高雄醫學大學附設醫院胃腸及一般外科謝建勳 Introduction-1 Any surgical intervention, elective or acute, laparoscopic or open, may lead to postoperative complications. Depends
Complications and management of upper GI surgery 高雄醫學大學附設醫院胃腸及一般外科謝建勳 Introduction-1 Any surgical intervention, elective or acute, laparoscopic or open, may lead to postoperative complications. Depends
Case Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery.
 Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE!
 : A MANAGEMENT CHALLENGE!") SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
SHORT GUT SYNDROME (SGS) : A MANAGEMENT CHALLENGE! Muhammad Saaiq DEPARTMENT OF SURGERY,PIMS, ISLAMABAD. Surgical Grand Round, Pakistan Institute of Medical Sciences (PIMS), Islamabad. September 23, 2005.
REFLUX ALKALINE GASTRITIS* SYRACUSE, NEW YORK
 VOL. 115, No. 2 REFLUX ALKALINE GASTRITIS* By SEUK KY KIM, M.D.,t LLOYD S. ROGERS, M.D.,t and ROBERT E. HEITZMAN, M.D. SYRACUSE, NEW YORK E ARLY physiologists thought that gastric acid was partly controlled
VOL. 115, No. 2 REFLUX ALKALINE GASTRITIS* By SEUK KY KIM, M.D.,t LLOYD S. ROGERS, M.D.,t and ROBERT E. HEITZMAN, M.D. SYRACUSE, NEW YORK E ARLY physiologists thought that gastric acid was partly controlled
STOMACH and DUODENUM DISEASE
 STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
STOMACH and DUODENUM DISEASE STOMACH ANATOMY In the living and upright posture, the stomach is a j-shaped. It has two surfaces, two curvatures and two openings. Esophagus Fundus cardia Pylorus B o d y
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Tornado Roux-en-Y anastomosis in laparoscopy-assisted distal gastrectomy
 Gastric Cancer (2008) 11: 181 185 DOI 10.1007/s10120-008-0474-7 Technical note 2008 by International and Japanese Gastric Cancer Associations Tornado Roux-en-Y anastomosis in laparoscopy-assisted distal
Gastric Cancer (2008) 11: 181 185 DOI 10.1007/s10120-008-0474-7 Technical note 2008 by International and Japanese Gastric Cancer Associations Tornado Roux-en-Y anastomosis in laparoscopy-assisted distal
Internal hernias after laparoscopic Roux-en-Y gastric bypass
 The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
Viriato Fiallo, MD Ursula McMillian, MD
 Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Viriato Fiallo, MD Ursula McMillian, MD Objectives Define obesity and effects on society and healthcare Define bariatric surgery Discuss recent medical management versus surgery research Evaluate different
Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row.
 Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row. Poster No.: C-2184 Congress: ECR 2012 Type: Educational Exhibit Authors: M. M. Mendigana Ramos, A. Burguete, A. Sáez de
Gastrectomy procedure and its complications: Findings at TC multi-detector 64 row. Poster No.: C-2184 Congress: ECR 2012 Type: Educational Exhibit Authors: M. M. Mendigana Ramos, A. Burguete, A. Sáez de
Lecture Goals. Body Mass Index. Obesity Definitions. Bariatric Surgery What the PCP Needs to Know 11/17/2009. Indications for bariatric Surgeries
 Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
Bariatric Surgery What the PCP Needs to Know Mouna Abouamara Assistant Professor Internal Medicine James H Quillen College Of Medicine Lecture Goals Indications for bariatric Surgeries Different types
PARENTERAL NUTRITION THERAPY
 UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
UnitedHealthcare Benefits of Texas, Inc. 1. UnitedHealthcare of Oklahoma, Inc. 2. UnitedHealthcare of Oregon, Inc. UnitedHealthcare of Washington, Inc. UnitedHealthcare West BENEFIT INTERPRETATION POLICY
Afferent loop syndrome (bilious vomiting following partial gastrectomy)
") University of Nebraska Medical Center DigitalCommons@UNMC MD Theses College of Medicine 5-1-1969 Afferent loop syndrome (bilious vomiting following partial gastrectomy) Kelly Burt University of Nebraska
University of Nebraska Medical Center DigitalCommons@UNMC MD Theses College of Medicine 5-1-1969 Afferent loop syndrome (bilious vomiting following partial gastrectomy) Kelly Burt University of Nebraska
NOTES: The Digestive System (Ch 14, part 2)
") NOTES: The Digestive System (Ch 14, part 2) PANCREAS Structure of the pancreas: The pancreas produces PANCREATIC JUICE that is then secreted into a pancreatic duct. The PANCREATIC DUCT leads to the The
NOTES: The Digestive System (Ch 14, part 2) PANCREAS Structure of the pancreas: The pancreas produces PANCREATIC JUICE that is then secreted into a pancreatic duct. The PANCREATIC DUCT leads to the The
A rare case of intestinal obstruction due to internal hernia. Dr. Jayanth 3 rd year PG Dept. Of General Surgery
 A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated
Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know
 Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know Valerie J. Halpin Legacy Weight and Diabetes Institute November 3, 2017 Surgical Overview Indications Contraindications
Bariatric Surgery: Patient Selection, Complications, What the Internist Should Know Valerie J. Halpin Legacy Weight and Diabetes Institute November 3, 2017 Surgical Overview Indications Contraindications
Abdominal Imaging. Afferent loop obstruction after gastric cancer surgery: helical CT findings
 Abdom Imaging 28:624 630 (2003) DOI: 10.1007/s00261-002-0070-y Abdominal Imaging Springer-Verlag New York Inc. 2003 Afferent loop obstruction after gastric cancer surgery: helical CT findings H.-C. Kim,
Abdom Imaging 28:624 630 (2003) DOI: 10.1007/s00261-002-0070-y Abdominal Imaging Springer-Verlag New York Inc. 2003 Afferent loop obstruction after gastric cancer surgery: helical CT findings H.-C. Kim,
Bariatric Surgery Risk Education Packet Walter J. Chlysta MD, FACS
 Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
Date: Patient Name: Height: Weight: Ideal Body Weight: Excess Weight: Realistic Gastric Bypass Weight Goal (77 % Excess weight loss): Realistic Sleeve Gastrectomy Weight Goal (70 % Excess weight loss):
Gastric Bypass Surgery
 Gastric Bypass Surgery Introduction Obesity is associated with many diseases such as diabetes, high blood pressure, heart problems, and degeneration of the joints. These diseases and the obesity itself
Gastric Bypass Surgery Introduction Obesity is associated with many diseases such as diabetes, high blood pressure, heart problems, and degeneration of the joints. These diseases and the obesity itself
Here are some types of gastric bypass surgery:
 Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Gastric Bypass- Definition By Mayo Clinic staff Weight-loss (bariatric) surgeries change your digestive system, often limiting the amount of food you can eat. These surgeries help you lose weight and can
Small bowel atresia. Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families
 Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Great Ormond Street Hospital for Children NHS Foundation Trust: Information for Families Small bowel atresia This information sheet from Great Ormond Street Hospital explains the causes, symptoms and treatment
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
ADVANCE AT YOUR OWN PACE
 ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
ADVANCE AT YOUR OWN PACE Welcome and Introductions Obesity and Its Impact on Health Surgeon Introduction Surgical Weight Loss Options AGENDA OSVALDO ANEZ, MD 28 years of experience Performed approximately
Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
 OBES SURG (2012) 22:855 862 DOI 10.1007/s11695-011-0519-6 CLINICAL REPORT Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
OBES SURG (2012) 22:855 862 DOI 10.1007/s11695-011-0519-6 CLINICAL REPORT Classification and Management of Leaks after Gastric Bypass for Patients with Morbid Obesity: A Prospective Study of 60 Patients
Clinical Case Presentation. Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006
 Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
Clinical Case Presentation Jared B. Smith, M.D. Surgical Grand Rounds, August 21, 2006 Clinical History CC: Can t swallow anything HPI: 50 y.o. male from western Colorado, greater than 2 years of emesis
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015
 ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
ADULT RETROGRADE INTUSSUSCEPTION Brian Tiu Richmond University Medical Center September 3, 2015 CASE PRESENTATION 41 yo woman presented one day hx abdominal pain, worsening nausea/vomiting denied flatus/bm
Safety of Laparoscopic Vs Open Bariatric Surgery. Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat
 Safety of Laparoscopic Vs Open Bariatric Surgery 1 Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat Surgical Treatment of Obesity 2 Bariatrics is the branch of
Safety of Laparoscopic Vs Open Bariatric Surgery 1 Dr. Kishore Nadkarni Director Nadkarni Group of Hospitals Killa Pardi, Vapi, Valsad, Surat Surgical Treatment of Obesity 2 Bariatrics is the branch of
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
BARIATRIC SURGERY. Weight Loss Surgery. A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female
 BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
BARIATRIC SURGERY Weight Loss Surgery A variety of surgical procedures to reduce weight performed on people who have obesity. Therapy Male & Female About Bariatric surgery Bariatric surgery offers a treatment
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine
 Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none none Reserved for pts: Complications from GERD Refractory esophagitis** Stricture Barrett s Persistent reflux
Catherine Kerschen DO, FACOI Michigan State University College of Osteopathic Medicine none none Reserved for pts: Complications from GERD Refractory esophagitis** Stricture Barrett s Persistent reflux
Imaging features of the complications of bariatric surgery
 Imaging features of the complications of bariatric surgery Poster No.: C-2173 Congress: ECR 2014 Type: Authors: Educational Exhibit M. Lahkim 1, J. Lucas 2, A. HAMEG 3, P. Lacombe 4 ; 1 Rabat/MA, 2 Neuilly/Seine/FR,
Imaging features of the complications of bariatric surgery Poster No.: C-2173 Congress: ECR 2014 Type: Authors: Educational Exhibit M. Lahkim 1, J. Lucas 2, A. HAMEG 3, P. Lacombe 4 ; 1 Rabat/MA, 2 Neuilly/Seine/FR,
Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor
 Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
Sleeve Plus Options Disclosure Medtronic - Speaker/ Research Grant/ Robotics Advisory Board Gore - Education Grant/ Speaker Teleflex - Consultant Da Vinci - Proctor Mederi - Speaker Novadaq - Advisory
University of Buea. Faculty of Health Sciences. Programme in Medicine
 Faculty of Health Sciences University of Buea Wednesday, 28 th January 2009 Time: 8 00-10 00 Programme in Medicine MED 303 (Gastrointestinal Physiology) EXAMS (2008-2009) Identify the letter of the choice
Faculty of Health Sciences University of Buea Wednesday, 28 th January 2009 Time: 8 00-10 00 Programme in Medicine MED 303 (Gastrointestinal Physiology) EXAMS (2008-2009) Identify the letter of the choice
Motility Conference Ghrelin
 Motility Conference Ghrelin Emori Bizer, M.D. Division of Gastroenterology/Hepatology November 21, 2007 Ghrelin: Basics Hormone produced by the A-like A endocrine cells in the oxyntic mucosa (stomach body
Motility Conference Ghrelin Emori Bizer, M.D. Division of Gastroenterology/Hepatology November 21, 2007 Ghrelin: Basics Hormone produced by the A-like A endocrine cells in the oxyntic mucosa (stomach body
Imaging Following Mini-Gastric Bypass and Sleeve Gastrectomy: what every radiologists need to know
 Imaging Following Mini-Gastric Bypass and Sleeve Gastrectomy: what every radiologists need to know Poster No.: C-1264 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Yazgan, S. BALCI, T. Sahin,
Imaging Following Mini-Gastric Bypass and Sleeve Gastrectomy: what every radiologists need to know Poster No.: C-1264 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Yazgan, S. BALCI, T. Sahin,
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications
 A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
A Bariatric Patient in my Waiting Room: Choosing the Right Patient for the Right Operation: Bariatric Surgery Indications Shahzeer Karmali MD FRCSC FACS Associate Professor Surgery University of Alberta
Policy Specific Section: April 14, 1970 June 28, 2013
 Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Medical Policy Bariatric Surgery Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Surgery Original Policy Date: Effective Date: April 14, 1970 June 28, 2013 Definitions
Amyloidosis & the GI Tract
 Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Amyloidosis & the GI Tract John O. Clarke, M.D. Director, Esophageal Program Clinical Associate Professor of Medicine Stanford University john.clarke@stanford.edu 2017 Topics to cover 1) Patterns of GI
Despicable Diarrhea. Darlene G. Kelly, MD, PhD Associate Professor of Medicine Medical Director HPN Program Mayo Clinic Rochester, Minnesota
 Despicable Diarrhea Darlene G. Kelly, MD, PhD Associate Professor of Medicine Medical Director HPN Program Mayo Clinic Rochester, Minnesota Conflict of Interest Statement Commercial Interests None Off
Despicable Diarrhea Darlene G. Kelly, MD, PhD Associate Professor of Medicine Medical Director HPN Program Mayo Clinic Rochester, Minnesota Conflict of Interest Statement Commercial Interests None Off
Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives
 Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives page 2 This booklet has been written to provide information about the surgical procedures
Department of Hepatobiliary and Pancreatic Surgery About Pancreatic Surgery A guide for patients and relatives page 2 This booklet has been written to provide information about the surgical procedures
Digestion and Absorption
 Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
VOMITING. Tan Lay Zye
 VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
VOMITING Tan Lay Zye Vomiting is a common symptom. It is a complex reflex behavioural response involving forceful expulsion of the stomach contents through oral cavity. Contents Emetic reflex Causes of
Gastrointestinal obstruction Dr Iain Lawrie
 Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
Gastrointestinal obstruction Dr Iain Lawrie Consultant and Honorary Clinical Senior Lecturer in Palliative Medicine The Pennine Acute Hospitals NHS Trust / The University of Manchester iain.lawrie@pat.nhs.uk
The Bariatric and Heartburn Center of Northeast Ohio
 The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
The Bariatric and Heartburn Center of Northeast Ohio A message from Dr. Chlysta: Walter J. Chlysta MD, FACS, FASMBS 1900 23 rd Street, Suite 403 Cuyahoga Falls, OH 44223 Phone 330-926-3443 Fax 330-255-5092
LEARNING OBJECTIVES. Obesity. Obesity. Consequences of Malnutrition in Obesity: Undernutrition Concurrent with Overnutriton. Obesity.
 @PhD_Leigh #BariatricSurgery #Nutrition LEARNING OBJECTIVES Consequences of Malnutrition in : Undernutrition Concurrent with Overnutriton Leigh A. Frame, PhD, MHS Program Director in Integrative Medicine,
@PhD_Leigh #BariatricSurgery #Nutrition LEARNING OBJECTIVES Consequences of Malnutrition in : Undernutrition Concurrent with Overnutriton Leigh A. Frame, PhD, MHS Program Director in Integrative Medicine,
INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE
 INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor
INFORMED CONSENT FOR LAPAROSCOPIC ROUX-EN-Y GASTRIC BYPASS SURGICAL PROCEDURE It is very important to Venice Metabolic and Bariatric Surgery that you understand and consent to the treatment your doctor
Complications after laparoscopic gastric bypass for morbid obesity. Background LGBP. Eirik Hornes Halvorsen, MD, PhD Oslo
 Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
RADIATION INDUCED SMALL BOWEL DISEASE. Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology
 RADIATION INDUCED SMALL BOWEL DISEASE Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology INTRODUCTION Radiation therapy is not regularly indicated in the treatment of small bowel disease. Reasons are complex
RADIATION INDUCED SMALL BOWEL DISEASE Dr Mnguni Supervisor: Dr Lohlun Radiation Oncology INTRODUCTION Radiation therapy is not regularly indicated in the treatment of small bowel disease. Reasons are complex
Short Bowel Syndrome: Medical management
 Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Short Bowel Syndrome: Medical management La Sindrome dell'intestino Corto in età pediatrica Brescia 18 marzo 2011 Jon A.Vanderhoof, M.D. Division of Pediatric GI Harvard Medical School Children s Hospital,
Bariatric Surgery. Policy Number: Last Review: 12/2018 Origination: 10/1988 Next Review: 12/2019
 Bariatric Surgery Policy Number: 7.01.47 Last Review: 12/2018 Origination: 10/1988 Next Review: 12/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for bariatric surgery
Bariatric Surgery Policy Number: 7.01.47 Last Review: 12/2018 Origination: 10/1988 Next Review: 12/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for bariatric surgery
Afferent Loop Syndrome After Subtotal Gastrectomy With Billroth-II Reconstruction: Etiology and Treatment
 Int Surg 2016;101:194 200 DOI: 10.9738/INTSURG-D-15-00137.1 Afferent Loop Syndrome After Subtotal Gastrectomy With Billroth-II Reconstruction: Etiology and Treatment Sung-Heun Kim 1, Jong-Young Oh 2, Ki-Han
Int Surg 2016;101:194 200 DOI: 10.9738/INTSURG-D-15-00137.1 Afferent Loop Syndrome After Subtotal Gastrectomy With Billroth-II Reconstruction: Etiology and Treatment Sung-Heun Kim 1, Jong-Young Oh 2, Ki-Han
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Nutrition Management in GI Diseases
 Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Nutrition Management in GI Diseases Aryono Hendarto MD Nutrition & Metabolic Diseases Division Department of Child Health Cipto Mangunkusumo Hospital University of Indonesia 1 Patient s Care 1. Drugs 2.
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Note: Page numbers of article titles are in boldface type. A Abdominal pain, enteral therapy in acute pancreatitis and, 812 Abscess(es), pancreatic, nutritional support for, 814 815 Acute Physiology and
Bariatric Surgery MM /11/2001. HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient; Inpatient
 of Service: Outpatient; Inpatient") Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Bariatric Surgery Policy Number: Original Effective Date: MM.06.003 09/11/2001 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 05/01/2012 Section: Surgery Place(s) of Service: Outpatient;
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
A Guide to Gastrointestinal Motility Disorders
 A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord André Smout Jan Tack A Guide to Gastrointestinal Motility Disorders Albert J. Bredenoord Gastroenterology and Hepatology Academic Medical
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
University of Groningen. The Roux-en-Y syndrome Mijle, Hubertus Cornelis Joseph van der
 University of Groningen The Roux-en-Y syndrome Mijle, Hubertus Cornelis Joseph van der IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen The Roux-en-Y syndrome Mijle, Hubertus Cornelis Joseph van der IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
Simple Versus Double Jejunal Pouch for Reconstruction after Total Gastrectomy
 Simple Versus Double Jejunal Pouch for Reconstruction after Total Gastrectomy Maria A. Gioffre Florio, MD, Marcello Bartolotta, MD, Joseph C. Miceli, MD, Giuseppa Giacobbe, MD, Francesco P. Saitta, MD,
Simple Versus Double Jejunal Pouch for Reconstruction after Total Gastrectomy Maria A. Gioffre Florio, MD, Marcello Bartolotta, MD, Joseph C. Miceli, MD, Giuseppa Giacobbe, MD, Francesco P. Saitta, MD,
See Policy CPT CODE section below for any prior authorization requirements
 Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
Effective Date: 9/1/2018 Section: SUR Policy No: 139 Medical Officer 9/1/2018 Date Technology Assessment Committee Approved Date: 3/04; 3/05; 3/06; 4/12; 4/16 Medical Policy Committee Approved Date: 11/08;
Post surgical Gastroenterology problems. Dr Derek Luo Gastroenterologist Counties Manukau Health Macmurray Centre CME 19/3/2014
 + Post surgical Gastroenterology problems Dr Derek Luo Gastroenterologist Counties Manukau Health Macmurray Centre CME 19/3/2014 + Outline 1. Consequences of bowel resection 2. Post cholecystectomy Syndrome
+ Post surgical Gastroenterology problems Dr Derek Luo Gastroenterologist Counties Manukau Health Macmurray Centre CME 19/3/2014 + Outline 1. Consequences of bowel resection 2. Post cholecystectomy Syndrome
Chapter 20 The Digestive System Exam Study Questions
 Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil
 Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
Nutritional Management in Enterocutaneous fistula Dr Deepak Govil MS, PhD (GI Surgery) Senior Consultant Surgical Gastroenterology Indraprastha Apollo Hospital New Delhi What is enterocutaneous fistula
University of Groningen. Dumping syndrome after esophageal, gastric or bariatric surgery van Beek, A.P.; Emous, M.; Laville, Maurice; Tack, Johannes
 University of Groningen Dumping syndrome after esophageal, gastric or bariatric surgery van Beek, A.P.; Emous, M.; Laville, Maurice; Tack, Johannes Published in: Obesity Reviews DOI: 10.1111/obr.12467
University of Groningen Dumping syndrome after esophageal, gastric or bariatric surgery van Beek, A.P.; Emous, M.; Laville, Maurice; Tack, Johannes Published in: Obesity Reviews DOI: 10.1111/obr.12467
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
GASTROINTESTINAL SYSTEM
 GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
GASTROINTESTINAL SYSTEM Topographic Anatomy of the Abdomen Surface Landmarks Xiphoid process T9/T10 Inferior costal margin L2/L3 Iliac Crest L4 level ASIS L5/S1 level Pubic symphysis level of greater trochanter
Bariatric Surgery. Overview of Procedural Options
 Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Bariatric Surgery Overview of Procedural Options The Obesity Epidemic In 1991, NO state had an obesity rate above 20% 1 As of 2010, more than two-thirds of states (38) now have adult obesity rates above
Removal of a lap band and revision to an alternative bariatric procedure in one procedure.
 How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
How to Discuss the Case with Insurance Plan Medical Director, Letter of Medical Necessity, and Increasing the Chance of Letters of Medical Necessity are a well-known requirement when requesting authorization
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Ingestion Digestion- Absorption- Elimination
 DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
GI Complications in heds and HSD
 GI Complications in heds and HSD Qasim Aziz PhD, FRCP Professor in Neurogastroenterology Neurogastroenterology Group GUT = Gastrointestinal (GI) tract Oesophagus / gullet Gastro-oesophageal junction Stomach
GI Complications in heds and HSD Qasim Aziz PhD, FRCP Professor in Neurogastroenterology Neurogastroenterology Group GUT = Gastrointestinal (GI) tract Oesophagus / gullet Gastro-oesophageal junction Stomach
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal