Preoperative octreotide treatment in newly diagnosed acromegalic. patients with macroadenomas increases cure short-term postoperative
|
|
|
- Marianna Haynes
- 5 years ago
- Views:
Transcription
1 J Clin Endocrin Metab. First published ahead of print May 20, 2008 as doi: /jc Preoperative octreotide treatment in newly diagnosed acromegalic patients with macroadenomas increases cure short-term postoperative rates: a prospective, randomized trial. Sven M. Carlsen a,b, Morten Lund-Johansen c,d, Thomas Schreiner e, Sylvi Aanderud f, Øivind Johannesen g, Johan Svartberg h,i, John G. Cooper j, John K. Hald k, Stine L. Fougner e,l, Jens Bollerslev e,l, on behalf of the POTA study group. a Department of Laboratory Medicine, Childrens and Womens Health, Norwegian University for Science and Technology, Trondheim, b Department of Endocrinology, St. Olavs Hospital, Trondheim, c Department of Neurosurgery, Haukeland University Hospital, Bergen, d Neurosurgery Unit, Institute of Surgical Sciences, University of Bergen, Bergen, e Endocrinology Unit, Department of Medicine, Rikshospitalet- Radiumhospitalet Medical Center, Oslo, f Endocrinology Unit, Department of Medicine, Haukeland University Hospital and Institute of Medicine, University of Bergen, g Endocrinology Unit, Department of Medicine, Aker University Hospital, Oslo, h Endocrinology Unit, Department of Medicine, University Hospital of North Norway, i Institute of Clinical Medicine, University of Tromsø, j Endocrinology Unit, Department of Medicine, Stavanger University Hospital, Stavanger, k Department of Radiology, Rikshospitalet-Radiumhospitalet Medical Center, Oslo,, and l Research Institute for Internal Medicine, University of Oslo, Oslo, Norway. Abbrevated title: Preoperative octreotide treatment and cure Key terms: Acromegaly, preoperative medical treatment, surgical cure Page 1 of 19 Copyright (C) 2008 by The Endocrine Society
2 Total number of words: 3473 Total number of tables: 3 Total number of figures: 1 Corresponding author: Sven M. Carlsen, Department of Endocrinology, St. Olavs Hospital, University Hospital of Trondheim, 7006 Trondheim, Norway. sven.carlsen@ntnu.no Reprint request: Sven M. Carlsen, Department of Endocrinology, St. Olavs Hospital, University Hospital of Trondheim, 7006 Trondheim, Norway. sven.carlsen@ntnu.no Disclosure: MLJ, TS, SA, ØJ, JS, JGC, and JKH have nothing to declare. SLF has received a research grant and lecture fees from Novartis. JB has received lecture fees from Novartis. SMC has received lecture fees from Novartis and Pfizer. Page 2 of 19
3 Summary Context: Surgery is the primary treatment of acromegaly. However it often fails to cure the patient. New strategies that improve surgical outcome are needed. Objective: To investigate whether six months preoperative treatment with octreotide improves the surgical outcome in newly diagnosed acromegalic patients. Patients: During a five year period ( ) all newly diagnosed acromegalic patients between 18 and 80 years of age in Norway were screened and invited to participate in the study. Sixty-two patients were included in the Preoperative Octreotide Treatment of Acromegaly (POTA) study. Research design and methods: After a baseline evaluation patients were randomized directly to transsphenoidal surgery (n=30) or to pre-treatment with octreotide (n=32) 20 mg im. every 28 th day for six months prior to transsphenoidal surgery. Cure was evaluated three months postoperatively primarily by Insulin like Growth Factor-1 levels (IGF-1). Results: According to the IGF-1 criteria 14 out of 31 (45%) pretreated patients vs. 7 out of 30 (23%) patients with direct surgery were cured by surgery (p=0.11). In patients with microadenomas ( 10 mm) 1 out of 5 (20%) pretreated vs. 3 out of 5 (60%) with direct surgery were cured (p=0.52). In patients with macroadenomas 13 out of 26 (50%) pretreated vs. 4 out of 25 (16%) with direct surgery were cured (p=0.017). Conclusion: Six months preoperative octreotide treatment might improve surgical cure rate in newly diagnosed acromegalic patients with macroadenomas. These results have to be confirmed in future studies. Page 3 of 19
4 Introduction: In the majority (98%) of cases, acromegaly is caused by a growth hormone (GH) producing pituitary adenoma. Retrospective cohort studies suggest that mortality in acromegaly is at least doubled compared to the general population (1-3). Morbidity and mortality are associated with elevated levels of growth hormone (GH) and Insulin-like Growth Factor-1 (IGF-1) (1,2,4). The aim of treatment is to relieve symptoms, control tumour growth and ensure biochemical cure. Neurosurgery is the accepted first-line treatment of acromegaly. Outcome predictors include tumour size, extrasellar extension, dural invasion, pre-treatment GH levels and the experience of the neurosurgeon (5,6). The best reported cure rates for micro- and macroadenomas are 80-90% and 50-60%, respectively (5-7), whereas overall cure rates as low as 18% (39% in microadenomas and 12% in macroadenomas) have been reported (8). It is possible that studies with low cure rates remain unpublished. Medical treatment of acromegaly with somatostatin analogues (SSA) can lead to normalized GH and IGF-1 levels (9) and relief of symptoms (10). SSA treatment may cause shrinkage of GH-secreting pituitary adenomas (9,11). Theoretically, this could improve the likelihood of a radical resection, particularly in macroadenomas. Furthermore, it has been suggested that SSA treatment softens the tumour parenchyma and thereby facilitates tumour removal (12,13). Finally, it has been reported that SSA pre-treatment leads to a shortening of postoperative hospital stay (14). Previous studies addressing preoperative SSA treatment and subsequent surgical cure rates are conflicting, reporting a benefit (12,14,15),or no difference between groups (13,16.17). Most of these studies were retrospective in design. Between 1999 and 2004, we included patients in the randomized Preoperative Octreotide Treatment of Acromegaly (POTA) study to investigate whether six months Page 4 of 19
5 pre-treatment with the SSA octreotide would improve the surgical cure rate of newly diagnosed acromegalic patients. Material and methods: Study population: In Norway all pituitary surgery is performed by one dedicated neurosurgeon at each of the five university hospitals. All five neurosurgical departments participated in the POTA study. All acromegalic patients in Norway diagnosed between September 1 th 1999 and October 31 th 2004 were invited to participate in the study. Inclusion criteria were: a) newly diagnosed, previously untreated patients with GH nadir > 2.5 mcg/l during a standard 75 gram 2 hour oral glucose tolerance test (OGTT), b) pituitary adenoma verified by a pituitary MRI scan, and c) age between 18 and 80 years. Exclusion criteria were; a) immediate surgery indicated by clinical criteria, b) pregnancy, c) contraindications to MRI scan, and d) patients judged not suitable to participate in the study for other reasons such as personality disorders and alcohol abuse. Power calculations indicated that 31 patients had to be included in each group in order to have an 80% probability of demonstrating an increase in overall cure rate from 40% to 75%. Eighty-three consecutive patients with previously undiagnosed acromegaly were identified during the inclusion period of five years and two months. Twenty-one of these were not included due to contraindications, unwillingness to participate or because the diagnosis of acromegaly was established after surgery. The present study presents data from the 62 (75% of eligible) included in the POTA study. Written informed consent was obtained from each patient before inclusion and the declaration of Helsinki was followed throughout the study. The study was approved by the Committee for Medical Research Ethics in each of the five health regions in Norway, and The Norwegian Medicines Agency. Page 5 of 19
6 Investigations: The diagnosis of acromegaly was made in each participating center based on a GH nadir > 2.5 mcg/l during a two hour 75 g OGTT which was performed according to the WHO procedure. Samples for GH measurements were drawn at baseline and every half hour for 2 hours. The presence of a pituitary adenoma was confirmed by a pituitary MRI scan (T1-weighted coronal and/or sagittal and/or axial scans, 3-5 mm slice thickness at 1.5T). Fasting serum samples for IGF-1 analysis were drawn at baseline and three months postoperatively and stored at -70 o C until assayed. The samples were analyzed after the last patient had completed the study schedule, as single measurements in one run using an ELISA kit from R&D. The upper limit of normal (ULN) was set as the age adjusted 95 percentile by regression based on 40 samples run in parallel with a commercial kit from CisBio with given reference interval (18). The intra- and interassay coefficient of variation were 3.8 % and 7.2 %, accordingly. In two patients, sera from the postoperative evaluation were missing and the locally measured IGF-1 values against local ULN were used instead. GH analyses were performed consecutively by standard laboratory procedures at each of the participating study centers. In Norway GH-values are given in miu/l. We chose to use a conservative conversion factor of 2.0 for conversion between mcg/l and miu/l. MRI scans were examined retrospectively in a blinded fashion by two physicians (JKH & SLF), one being an experienced neuroradiologist. Adenomas measuring ten mm or less on MRI in the largest dimension were classified as microadenomas, and larger tumors as macroadenomas. No distinction between enclosed, suprasellar and invasive macroadenomas was made as this was not predefined in the protocol. The longest anterior-posterior, vertical and transverse diameters were measured, and tumor volume calculated by the formula height width length 0.5 (19). Page 6 of 19
7 Treatment: After a baseline evaluation, patients were randomized separately for each study center in blocks of four directly to transsphenoidal surgery (direct surgery group, n = 30) or to six months of preoperative treatment with octreotide (pre-treatment group, n = 32). Randomization was completely balanced between the two study groups at the three centers that included an equal number of patients. One more patient was randomized to pre-treatment with octreotide at each of the two remaining study centers that included an odd number of patients. To reduce the risk of gastrointestinal adverse effects in the pre-treatment group, octreotide was initiated at a dose of 50 µg sc. tid for the first week and 100 µg sc. tid for the second week. From the third week on, the patients received octreotide LAR 20 mg im. every 28 th day for six months. They underwent transsphenoidal surgery within 28 days of the last injection. If surgery was delayed, an extra octreotide LAR injection was given before surgery. Hence, all patients in the pre-treatment group underwent surgery with therapeutic levels of the study medication. All patients were operated by standard microneurosurgical technique via the transsphenoidal route. During surgery, the consistency of the adenoma was graded as soft, mixed or firm, and the neurosurgeon evaluated the operative result as radical vs. subtotal resection. Peri- and postoperative surgical complications and duration of postoperative hospital stay were registered. If indicated, octreotide could be administered after the three months postoperative evaluation. Aims of the study: The aim of the study was to investigate whether six months treatment with the somatostatin analogue octreotide prior to transsphenoidal surgery in newly diagnosed acromegalic patients would improve the outcome, using cure rate at evaluation three Page 7 of 19
8 months postoperatively as the primary endpoint. Secondary endpoints included postoperative hospital stay duration and complication rates. Definition of cure: Cure was evaluated three months postoperatively primarily by fasting IGF-1 age adjusted ULN (20,21). In addition, a GH nadir 1.0 mcg/l during an OGTT was used. Statistics: All statistical procedures, except estimation of confidence intervals (CI), were performed with SPSS version CI s were estimated by binominal exact estimations using Stata Corp., version 9.0 (College station, Texas, USA). Data are presented as absolute numbers or means and standard deviations (SD). Two-sided Fischer`s exact test for categorical variables and two-sided t-tests for independent samples for continuous variables were used. No adjustments for multiple testing were performed. P-values < 0.05 were considered significant. Results: Baseline data: Eighty-three patients with previously undiagnosed acromegaly were identified during the inclusion period of five years and two months. With 4.5 million inhabitants in Norway this equals an incidence of acromegaly in Norway of 3.6 cases/million/year. At baseline there were significantly more males than females (p = 0.042) and lower IGF-1 levels (p = 0.004) in the pre-treatment group. However, when evaluating IGF-1 as percentage of age-adjusted ULN this difference lost its significance (p=0.056). Patient age, working status, GH nadir during an OGTT, tumor volume and ratio between micro- and macroadenomas did not differ between groups (table 1). All the included patients were Caucasians. One male patient with a microadenoma did not Page 8 of 19
9 undergo surgery because the tumor regressed during pre-treatment. He was excluded from analyses of surgical cure rates. None of the patients withdrew from the study or were lost to follow-up during the study period. MRI scans: By central blinded evaluation of baseline MRI scans, there were 11 microadenomas ( 10 mm in the largest diameter) and 51 macroadenomas. In six patients, at least one of the MRI scans was not available for central evaluation. For these patients the classification of adenoma size and estimation of tumor volume was based on local evaluation of the tumor during the study. At inclusion there were six adenomas in the direct surgery group with signs of cavernous sinus invasion. In the pre-treatment group there were four adenomas with signs of cavernous sinus invasion both before octreotide treatment and the same number after pre-treatment but prior to surgery. Primary outcome: IGF-1 Criteria: Cure, defined solely by IGF-1 ULN three months postoperatively, was established in 14 out of 31 (45%) pretreated patients versus 7 out of 30 (23%) direct surgery patients (p = 0.11) (table 2). Subdividing tumors according to initial size, 1 out of 5 pretreated patients versus 3 out of 5 direct surgery patients with microadenomas were cured (p = 0.52). In patients with macroadenomas, 13 out of 26 (50%) pretreated patients versus 4 out of 25 (16%) direct surgery patients were cured (p = 0.017). Cure was also estimated for age-adjusted cut-off levels of IGF-1 ranging from 80% to 120% of the ULN (table 3). In macroadenomas, pre-treatment significantly Page 9 of 19
10 increased cure rates evaluated by IGF-1 at cut-off levels ranging from 95% to 120% of ULN (p = ). None of the six patients with signs of cavernous sinus invasion in the direct surgery group were cured. One of four patients with signs of cavernous sinus invasion after pre-treatment with octreotide was cured. The overall cure rates according to IGF-1 levels ranged from 0 to 62 % in the participating study centers with the smaller ones performing as well as the larger one (table 2). Combined criteria: When adding a GH-nadir during OGTT 1.0 mcg/l to the cure criteria, three patients, all with macroadenomas, lost their status of being cured (GH-nadirs of 1.8, 2.9 and 3.5 mcg/l). Thus, the overall cure rate in the total study population was reduced to 35% (pre-treated) and 23% (direct surgery), respectively (p = 0.40). In macroadenomas 38% (10 out of 26 pre-treated) versus 16% (4 out of 25 direct surgery) of patients were cured when adding GH-nadir during OGTT to the cure criteria (p = 0.12). Tumor volume: In the pretreated patients both initial tumor volume (1.98 ± 1.61 ml vs ± 1.13 ml; p = 0.33) and tumor volume change during pre-treatment (-38 ± 30 % vs. -31 ± 29 %; p = 0.56) were equally distributed among cured and non-cured patients, accordingly. Also, when performing separate analyses with the macroadenomas, initial tumor volume and percent change during pre-treatment were equal (data not shown). Three months postoperatively tumor volume was 0.51 ± 0.73 ml in pretreated patients and 0.80 ± 1.45 ml in direct surgery patients (p = 0.34). Page 10 of 19
11 Secondary outcomes: Tumor consistency: In pretreated patients the tumor was classified as firm in eight and mixed in one patient. In direct surgery patients no firm and five mixed tumors were identified. The rest of the tumors were soft (p = 0.002). Data on two pretreated and one direct surgery patient were missing. Surgical complications: Immediate surgical complications were reported in four patients (2 transient liquorrhea, 1 hematoma, 1 transient diabetes insipidus) in the pretreated group vs. 2 patients (1 transient liquorrhea, 1 sinusitis) with direct surgery (p = 0.67). During the postoperative period prior to the three months postoperative evaluation further complications were seen. Persistent surgical complications were seen in three patients (1 anterior pituitary insufficiency, 1 diabetes insipidus, 1 minor bitemporal visual field deficit, 1 nose complication) in the pretreated group vs. 4 patients (1 anterior pituitary insufficiency, 1 diabetes insipidus, 1 olfactory nerve dysfunction, 1 eye muscle palsy; most probable secondary to progressive cavernous sinus growth) in the group with direct surgery (p = 0.71). Altogether, surgical complication was seen in 2 out of the 21 (10%) cured patients and in 9 out of 40 (23%) non cured patients (p = 0.30). In patients without surgical complications 8 out of 39 (21%) adenomas were classified as mixed or solid vs. 4 out of 14 (29%) mixed or solid adenomas in patients with surgical complications (p = 0.54). Data were missing in 8 patients. The postoperative hospital stay was similar between groups, being 3.7 ± 1.8 days in pretreated patients versus 3.6 ± 1.6 days in direct surgery patients (p = 0.54). Surgical resection evaluation: In all the 21 patients cured by the IGF-1 criteria cure was anticipated by the neurosurgeon. However, surgical cure were also anticipated in 27 of Page 11 of 19
12 the 37 non-cured patients. Non-cure were anticipated in 3 out of 29 pretreated patients versus 7 out of 29 direct surgery patients (p = 0.16). Data were missing on 3 patients. Discussion The present prospective, randomized study indicates that pre-treatment of newly diagnosed acromegalic patients with octreotide prior to transsphenoidal surgery leads to an increased surgical cure rate in patients with macroadenomas, whereas no benefit, or even a possible adverse effect, was seen in patients with microadenomas. Our findings are in accordance with some (12,14,15) but not all previous reports (13,16,17). In acromegaly levels of IGF-1 as well as mean daytime GH levels and GH-nadir during an OGTT can be used as criteria for cure (21). However, IGF-1 measurements correlate better than GH levels with clinical disease activity (22). And in patients with very mild disease IGF-1 is elevated while GH secretory parameters are virtually normal (23). In the present study, only stored fasting serum was available for centralised analyses. Hence, central quality control was only possible for IGF-1 measurements and not for dynamic GH measurements (24). Therefore, and in accordance with the protocol, we primarily used IGF-1 as criteria for cure. This decision was also supported by the fact that in the general population both GH and IGF-1 levels decline with increasing age, while age adjusted reference values are available for the latter only (25). The biochemical criteria for cure based on different commercial assays for GH and IGF-1 is presently a matter of debate (24,26). We set the primary endpoint ULN according to the age adjusted 95 percentile found by regression in our own laboratory. This might have induced a systematic error with respect to the ULN used. However, interassay variability was thereby reduced to a minimum, thereby optimising the evaluation of cure at a given level. The overall very low cure rate, however, might be Page 12 of 19
13 influenced by this method, but should not affect the difference between the two treatment arms. Moreover, additional analysis of cure rates according to ULN ranging from 95% to 120% of the values used in the present study all showed significant benefit in the group of pre-treated patients with macroadenomas. This way of presenting IGF-1 data is untraditional. Nevertheless, given the present discussion on the IGF-1 measurements and reference ranges, we believe this presentation is valuable in underlining that our results are relatively independent of the values for ULN used. In the present study evaluation of cure was performed three months postoperatively which is in accordance with present clinical routine in Norway. This means that the patients were evaluated at least 12 weeks, but some as long as 16 weeks after the last injection with octreotide. Pharmacokinetic studies indicate that by that time levels of octreotide are well below therapeutic levels (27,28,29). Furthermore, withdrawal and dose extension studies indicate that in the great majority of patients octreotide effects has disappeared 12 weeks after the last injection (30,31,32). All though this does not quite fit with the present guidelines demanding at least four months delay in evaluation when using a long-acting SSA (33), this essentially rules out the possibility that the observed effect three months postoperatively, is only representing a hangover effect of pre-operative octreotide treatment. Overall the cure rates observed in the POTA study were 23% in newly diagnosed acromegalic patients treated directly with transsphenoidal surgery and 45% in patients pretreated for six month with octreotide LAR and still being on treatment during the surgical procedure. In patients with macroadenomas, the cure rate tripled form 16% in direct surgery patients to 50% in octreotide pretreated patients. This effect was evenly distributed between the largest and the smaller study centers (data not shown). This is an impressive increase which is only possible when cure rates in control patients are low. And low overall cure rate in direct surgery patients (29.7%) was also Page 13 of 19
14 observed in one previous study indicating benefit of SSA pre-treatment before surgery (14). Thus, one intriguing question is whether the effect of pre-treatment with octreotide depends on the low cure rate seen in direct surgery patients in the present study. It should be emphasized that the low cure rate also reflects the strict criteria for cure used. Moreover, in a pragmatic multi-centre study like this one, overall cure rates are expected to be lower than results from a center of excellence. Low overall cure rate has recently been presented in the AcroBel study that also used strict criteria for cure (34). It is interesting to observe the absolute numbers for patients with microadenomas. The results might indicate an adverse effect of pre-treatment. However, there were too few patients with microadenomas in the study to draw firm conclusions (p = 0.52). Nevertheless, this is an important clinical question, which should be explored in future studies. Contrary to previously published observations indicating that treatment with a SSA tends to increase the softness of the adenomas this prospective randomized study showed a significant increase in the firmness of the adenomas. Hence, it is not likely that our findings depend on the open design and the possible awareness by the neurosurgeons of previous data indicating increased softness of the adenomas by SSA treatment (12). If octreotide treatment increases the firmness of the adenoma, this might affect the surgical outcome negatively. However, we found no indication of an adverse effect of firm tumor consistency on surgical cure in micro- or macroadenomas (data not shown). One possible explanation is that SSA induced changes in tumor consistency might assist in the discrimination between the adenoma and surrounding tissue, including normal pituitary tissue, and thus, facilitate surgical cure. On the other hand a change in tumor consistency might be more pronounced with more prolonged treatment with SSAs. If so, this might evolve as a relative contraindication for long-term primary Page 14 of 19
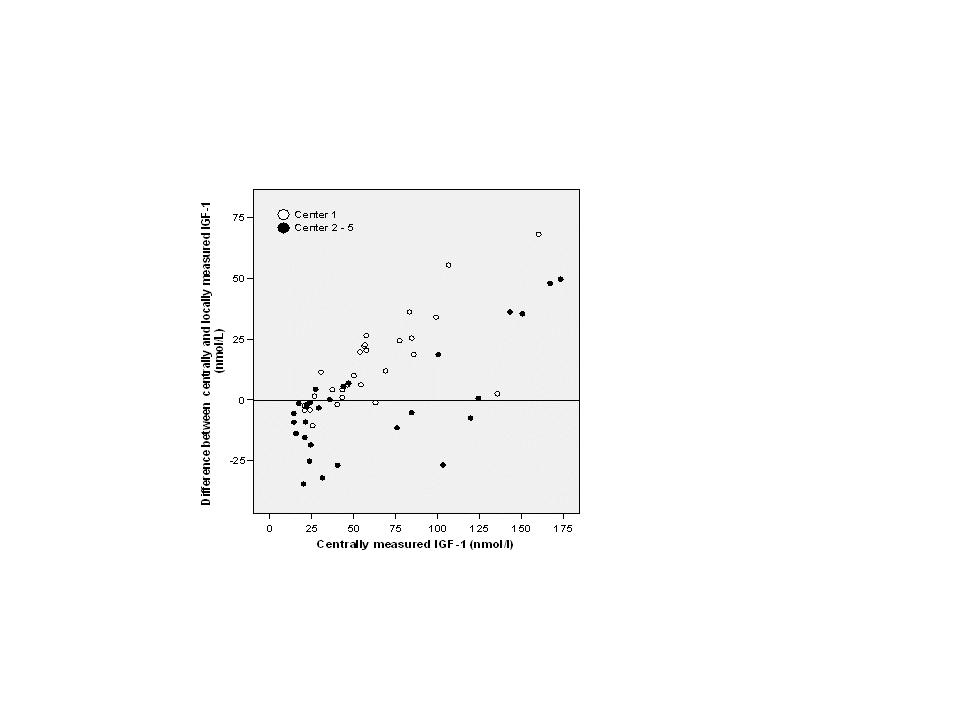
15 octreotide treatment of acromegalic patients that later might be considered for pituitary surgery. Therefore, future studies should also aim to evaluate the optimum duration of preoperative SSA treatment. In contrast with one previous report (14), pre-treatment with octreotide did not affect the duration of hospital stay. However, the standard care of pituitary surgery patients has changed markedly over the last decade which might have influenced the results. Further, we did not find any difference in surgical complication rates between the study groups. Preliminary results from our study, based on local classification of tumor size and IGF-1 measurements, were presented at the European Congress of Endocrinology in Gothenburg in September No difference between study groups was reported. The discrepancies between these preliminary results and the final results are due to reclassification of initial tumor size and cure by centralized MRI and IGF-1 evaluations. These changes were mainly related to one study center. This emphasises the importance of central quality evaluation of data and measurements in multi-centre studies. This is illustrated by the discrepancy between locally and centrally measured IGF-1 levels which supports our decision to rely primarily on a centrally measured variable (Figure 1). In conclusion, the POTA study indicates that pre-treatment with octreotide before transsphenoidal surgery improve surgical cure rates in patients with GHsecreting pituitary macroadenomas. The effect on microadenomas is inconclusive due to small numbers. Pre-treatment does not affect surgical complications or duration of hospital stay. These finding have to be confirmed by future well designed studies. Acknowledgements: Page 15 of 19
16 We thank the patients for their patience and participation throughout the study. Novartis Norway AS is recognised for their supply of study drug free of charge and their financial support to a part time study nurse. We are thankful to Kristin Godang for performing the central IGF-1 analyses and Harriet Selle for meticulous collection of patient records. Page 16 of 19
17 References 1. Beauregard C, Truong U, Hardy J, Serri O 2003 Long-term outcome and mortality after transsphenoidal adenomectomy for acromegaly. Clinical Endocrinology 58: Orme SM, McNally RJ, Cartwright RA, Belchetz PE 1998 Mortality and cancer incidence in acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. Journal of Clinical Endocrinology and Metabolism 83: Swearingen B, Barker FG II, Katznelson L, Biller BM, Grinspoon S, Klibanski A, Moayeri N, Black PM, Zervas NT 1998 Long-term mortality after transsphenoidal surgery and adjunctive therapy for acromegaly. Journal of Clinical Endocrinology and Metabolism 83: Holdaway IM, Rajasoorya RC, Gamble GD 2004 Factors influencing mortality in acromegaly. J Clin Endocrinol Metab 89: Freda PU 2003 How effective are current therapies for acromegaly? Growth Horm IGF Res Suppl A:S Nomikos P, Buchfelder M, Fahlbusch R 2005 The outcome of surgery in 668 patients with acromegaly using current criteria of biochemical 'cure'. Eur J Endocrinol. 152: Gittoes NJ, Sheppard MC, Johnson AP, Stewart PM 1999 Outcome of surgery for acromegaly--the experience of a dedicated pituitary surgeon. QJM 92: Lissett CA, Peacey SR, Laing I, Tetlow L, Davis JR, Shalet SM 1998 The outcome of surgery for acromegaly: the need for a specialist pituitary surgeon for all types of growth hormone (GH) secreting adenoma. Clin Endocrinol (Oxf) 49: Sheppard MC 2003 Primary medical therapy for acromegaly. Clin Endocrinol (Oxf) 58: Colao A, Ferone D, Marzullo P, Lombardi G 2004 Systemic complications of acromegaly: epidemiology, pathogenesis, and management. Endocr Rev 25: Melmed S, Sternberg R, Cook D, Klibanski A, Chanson P, Bonert V, Vance ML, Rhew D, Kleinberg D, Barkan A 2005 A critical analysis of pituitary tumor shrinkage during primary medical therapy in acromegaly. J Clin Endocrinol Metab 90: Stevenaert A, Beckers A 1996 Presurgical Octreotide: treatment in acromegaly. Metabolism. 45(Suppl 1): Abe T, Ludecke DK 2001 Effects of preoperative octreotide treatment on different subtypes of 90 GH-secreting pituitary adenomas and outcome in one surgical centre. Eur J Endocrinol 145: Page 17 of 19
18 14. Colao A, Ferone D, Cappabianca P, del Basso De Caro ML, Marzullo P, Monticelli A, Alfieri A, Merola B, Cali A, de Divitiis E, Lombardi G 1997 Effect of octreotide pretreatment on surgical outcome in acromegaly. J Clin Endocrinol Metab 82: Barkan AL, Lloyd RV, Chandler WF, Hatfield MK, Gebarski SS, Kelch RP, Beitins IZ 1998 Preoperative treatment of acromegaly with long-acting somatostatin analog SMS : shrinkage of invasive pituitary macroadenomas and improved surgical remission rate. J Clin Endocrinol Metab 67: Biermasz NR, van Dulken H, Roelfsema F 1999 Direct postoperative and followup results of transsphenoidal surgery in 19 acromegalic patients pretreated with octreotide compared to those in untreated matched controls. J Clin Endocrinol Metab 84: Kristof RA, Stoffel-Wagner B, Klingmuller D, Schramm J 1999 Does octreotide treatment improve the surgical results of macro-adenomas in acromegaly? A randomized study. Acta Neurochir (Wien) 141: Massart C, Poirier JY, Jard C, Pouchard M, Vigier MP 2007 Determination of serum insulin-like growth factor-i reference values for the immunometric Cisbio method on a large number of healthy subjects: Clinical utility in the follow-up of patients with treated acromegaly. Clin Chim Acta 381: Lundin P, Pedersen F 1992 Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 16: Feelders RA, Bidlingmaier M, Strasburger CJ, Janssen JA, Uitterlinden P, Hofland LJ, Lamberts SW, van der Lely AJ, de Herder WW 2005 Postoperative evaluation of patients with acromegaly: clinical significance and timing of oral glucose tolerance testing and measurement of (free) insulin-like growth factor I, acid-labile subunit, and growth hormone-binding protein levels. J Clin Endocrinol Metab 90: Barkan AL 2004 Biochemical markers of acromegaly: GH vs. IGF-I. Growth Horm IGF Res 14(Suppl A):S97-S Clemmons DR, Van Wyk JJ, Ridgway EC, Kliman B, Kjellberg RN, Underwood LE 1979 Evaluation of acromegaly by radioimmunoassay of somatomedin-c. N Engl J Med 22: Dimaraki EV, Jaffe CA, DeMott-Friberg R, Chandler WF, Barkan AL 2002 Acromegaly with apparently normal GH secretion: implications for diagnosis and follow-up. J Clin Endocrinol Metab 87: Pokrajac A, Wark G, Ellis AR, Wear J, Wieringa GE, Trainer PJ 2007 Variation in GH and IGF-I assays limits the applicability of international consensus criteria to local practice. Clin Endocrinol (Oxf) 67: Colao A, Pivonello R, Cavallo LM, Gaccione M, Auriemma RS, Esposito F, Cappabianca P, Lombardi G 2006 Age changes the diagnostic accuracy of mean Page 18 of 19
19 profile and nadir growth hormone levels after oral glucose in postoperative patients with acromegaly. Clin Endocrinol (Oxf) 65: Massart C, Poirier JY 2006 Serum insulin-like growth factor-i measurement in the follow-up of treated acromegaly: comparison of four immunoassays. Clin Chim Acta 373: Comets E, Mentré F, Grass P, Kawai R, Marbach P, Vonderscher J 2003 Population pharmacodynamic analysis of octreotide in acromegalic patients. Clin Pharmacol Ther 73: Astruc B, Marbach P, Bouterfa H, Denot C, Safari M, Vitaliti A, Sheppard M 2005 Long-acting octreotide and prolonged-release lanreotide formulations have different pharmacokinetic profiles. J Clin Pharmacol 45: Chen T, Miller TF, Prasad P, Lee J, Krauss J, Miscik K, Kalafsky G, McLeod JF 2000 Pharmacokinetics, pharmacodynamics, and safety of microencapsulated octreotide acetate in healthy subjects. J Clin Pharmacol 40: Stewart PM, Stewart SE, Clark PM, Sheppard MC 1999 Clinical and biochemical response following withdrawal of a long-acting, depot injection form of octreotide (Sandostatin-LAR). Clin Endocrinol (Oxf) 50: Turner HE, Thornton-Jones VA, Wass JA 2004 Systematic dose-extension of octreotide LAR: the importance of individual tailoring of treatment in patients with acromegaly. Clin Endocrinol (Oxf) 61: Lorcy Y, Dejager S, Chanson P; French Octreotide LAR Group 2000 Time course of GH and IGF-1 levels following withdrawal of long-acting octreotide in acromegaly. Pituitary 3: Melmed S, Casanueva F, Cavagnini F, Chanson P, Frohman LA, Gaillard R, Ghigo E, Ho K, Jaquet P, Kleinberg D, Lamberts S, Laws E, Lombardi G, Sheppard MC, Thorner M, Vance ML, Wass JA, Giustina A Consensus statement: medical management of acromegaly. Eur J Endocrinol 153: Bex M, Abs R, T'Sjoen G, Mockel J, Velkeniers B, Muermans K, Maiter D 2007 AcroBel--the Belgian registry on acromegaly: a survey of the 'real-life' outcome in 418 acromegalic subjects. Eur J Endocrinol 157: Page 19 of 19
20 Table 1. Baseline data according to treatment group Pretreatment* Direct surgery* P-value (n=32) (n=30) Age (years) 49.9 ± ± Gender (male/female) (no.) 20/12 11/ # Working status (working/sick leave) (no.) 20/12 16/ # GH nadir during OGTT (mcg/l) 19.3 ± ± IGF-1 (nmol/l) 92.1 ± ± & IGF-1 (% of ULN) 326 ± ± Tumor classification (micro/macro) (no.) 6/26 5/ # Tumor volume (cm 3 ) 1.66 ± ± * Values given as means ± SDs if otherwise not stated P-values given as independent samples t-tests used if otherwise not stated # P-values given as two-sided Pearson Chi-Square tests & This was also significantly different (p < 0.05) for both men and women ULN = Upper Limit of Normal
21 Table 2. Cure according to IGF-1 ULN and GH nadir 2.0 miu/l during OGTT three months postoperative. According to IGF-1 According to IGF-1 and GH-nadir Treatment N= Cured Not P- Cure (95% CI) N= Cured Not P- Cure (95% CI) cured value * cured value * All Pretreatment % (27-64) % (19-55) Direct surgery % (10-42) % (10-42) Microadenomas Pretreatment % (1-72) % (1-72) Direct surgery % (5-95) % (5-95) Macroadenomas Pretreatment % (30-70) % (20-59) Direct surgery % (5-36) % (5-36) All Center 1 Pretreatment % (12-62) % (12-62) Direct surgery % (2-34) % (2-34) Center 2-5 Pretreatment % (30-80) % (15-65) Direct surgery % (15-65) % (15-65) * P-value given as two-sided Fischer`s exact test for difference between treatment groups ULN = Upper Limit of Normal
22 Table 3. Cure according to IGF-1 ULN three months postoperative. All Microadenomas Macroadenomas IGF-1 as percent of ULN Treatment group Cured Not cured P-value Cured Not cured P-value Cured Not cured P-value 80 % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery % Pretreatment Direct surgery * P-value given as two-sided Fischer`s exact test for difference between treatment groups ULN = Upper Limit of Normal
23 Figure 1. Bland-Altman plot of locally and centrally measured IGF-1 levels three months postoperatively
24
Preoperative Lanreotide Treatment Improves Outcome in Patients with Acromegaly Resulting from Invasive Pituitary Macroadenoma
 The Journal of International Medical Research 2012; 40: 517 524 Preoperative Lanreotide Treatment Improves Outcome in Patients with Acromegaly Resulting from Invasive Pituitary Macroadenoma Z-Q LI 1,3,a,
The Journal of International Medical Research 2012; 40: 517 524 Preoperative Lanreotide Treatment Improves Outcome in Patients with Acromegaly Resulting from Invasive Pituitary Macroadenoma Z-Q LI 1,3,a,
Pegvisomant: an advance in clinical efficacy in acromegaly
 European Journal of Endocrinology (2003) 148 S27 S32 ISSN 0804-4643 Pegvisomant: an advance in clinical efficacy in acromegaly Paul M Stewart The University of Birmingham, Queen Elizabeth Hospital, Edgbaston,
European Journal of Endocrinology (2003) 148 S27 S32 ISSN 0804-4643 Pegvisomant: an advance in clinical efficacy in acromegaly Paul M Stewart The University of Birmingham, Queen Elizabeth Hospital, Edgbaston,
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Abstract. Introduction
 Clinical Features and Outcome of Surgery in 30 Patients with Acromegaly A. Chandna, N. Islam, A. Jabbar, L. Zuberi, N. Haque Endocrinology Section, Department of Medicine, Aga Khan University Hospital,
Clinical Features and Outcome of Surgery in 30 Patients with Acromegaly A. Chandna, N. Islam, A. Jabbar, L. Zuberi, N. Haque Endocrinology Section, Department of Medicine, Aga Khan University Hospital,
Pitfalls in early biochemical evaluation after transsphenoidal
 2017, 64 (1), 1-10 Original Advance Publication doi: 10.1507/endocrj.EJ17-0261 Pitfalls in early biochemical evaluation after transsphenoidal surgery in patients with acromegaly Hiroshi Nishioka 1), 3),
2017, 64 (1), 1-10 Original Advance Publication doi: 10.1507/endocrj.EJ17-0261 Pitfalls in early biochemical evaluation after transsphenoidal surgery in patients with acromegaly Hiroshi Nishioka 1), 3),
Research paper. *Authors with equal contribution
 HORMONES 2016, 15(2):224-234 Research paper Beneficial effect of dose escalation and surgical debulking in patients with acromegaly treated with somatostatin analogs in a Romanian tertiary care center
HORMONES 2016, 15(2):224-234 Research paper Beneficial effect of dose escalation and surgical debulking in patients with acromegaly treated with somatostatin analogs in a Romanian tertiary care center
Acromegaly: Management of the Patient Who Has Failed Surgery
 Acromegaly: Management of the Patient Who Has Failed Surgery Minnesota/Midwest Chapter of the American Association of Clinical Endocrinologists 8 th Annual Meeting October 14, 2017 Mark E. Molitch, M.D.
Acromegaly: Management of the Patient Who Has Failed Surgery Minnesota/Midwest Chapter of the American Association of Clinical Endocrinologists 8 th Annual Meeting October 14, 2017 Mark E. Molitch, M.D.
Monitoring of acromegaly: what should be performed when GH and IGF-1 levels are discrepant?
 Clinical Endocrinology (2009) 71, 166 170 doi: 10.1111/j.1365-2265.2009.03556.x CLINICAL QUESTION Monitoring of acromegaly: what should be performed when GH and IGF-1 levels are discrepant? Pamela U. Freda
Clinical Endocrinology (2009) 71, 166 170 doi: 10.1111/j.1365-2265.2009.03556.x CLINICAL QUESTION Monitoring of acromegaly: what should be performed when GH and IGF-1 levels are discrepant? Pamela U. Freda
Certain types of tumors, in the CNS and elsewhere,
 clinical article J Neurosurg 122:798 802, 2015 Percent reduction of growth hormone levels correlates closely with percent resected tumor volume in acromegaly Lucia Schwyzer, MD, Robert M. Starke, MD, John
clinical article J Neurosurg 122:798 802, 2015 Percent reduction of growth hormone levels correlates closely with percent resected tumor volume in acromegaly Lucia Schwyzer, MD, Robert M. Starke, MD, John
G Minniti 1, M-L Jaffrain-Rea 2,3, V Esposito 1,4, A Santoro 4, G Tamburrano 5 and G Cantore 1,4. Abstract. Introduction
 Evolving criteria for post-operative biochemical remission of acromegaly: can we achieve a definitive cure? An audit of surgical results on a large series and a review of the literature G Minniti 1, M-L
Evolving criteria for post-operative biochemical remission of acromegaly: can we achieve a definitive cure? An audit of surgical results on a large series and a review of the literature G Minniti 1, M-L
Remission criteria for the follow-up of patients with acromegaly
 European Journal of Endocrinology (2004) 150 465 471 ISSN 0804-4643 CLINICAL STUDY Remission criteria for the follow-up of patients with acromegaly Sevim Gullu, Hatice Keles 1, Tuncay Delibasi, Vedia Tonyukuk,
European Journal of Endocrinology (2004) 150 465 471 ISSN 0804-4643 CLINICAL STUDY Remission criteria for the follow-up of patients with acromegaly Sevim Gullu, Hatice Keles 1, Tuncay Delibasi, Vedia Tonyukuk,
Successful use of weekly pegvisomant administration in patients with acromegaly
 European Journal of Endocrinology (2009) 161 21 25 ISSN 0804-4643 CLINICAL STUDY Successful use of weekly pegvisomant administration in patients with acromegaly C E Higham, J D J Thomas 1, M Bidlingmaier
European Journal of Endocrinology (2009) 161 21 25 ISSN 0804-4643 CLINICAL STUDY Successful use of weekly pegvisomant administration in patients with acromegaly C E Higham, J D J Thomas 1, M Bidlingmaier
Pasireotide (SOM230) Demonstrates Efficacy and Safety in Patients with Acromegaly: A Randomized, Multicenter, Phase II Trial
 Demonstrates Efficacy and Safety in Patients with Acromegaly: A Randomized, Multicenter, Phase II Trial") ORIGINAL ARTICLE Endocrine Care (SOM230) Demonstrates Efficacy and Safety in Patients with Acromegaly: A Randomized, Multicenter, Phase II Trial S. Petersenn, J. Schopohl, A. Barkan, P. Mohideen, A. Colao,
ORIGINAL ARTICLE Endocrine Care (SOM230) Demonstrates Efficacy and Safety in Patients with Acromegaly: A Randomized, Multicenter, Phase II Trial S. Petersenn, J. Schopohl, A. Barkan, P. Mohideen, A. Colao,
Changing patterns of insulin-like growth factor I and glucose-suppressed growth hormone levels after pituitary surgery in patients with acromegaly
 J Neurosurg 97:287 292, 2002 Changing patterns of insulin-like growth factor I and glucose-suppressed growth hormone levels after pituitary surgery in patients with acromegaly ANA LAURA ESPINOSA-DE-LOS-MONTEROS,
J Neurosurg 97:287 292, 2002 Changing patterns of insulin-like growth factor I and glucose-suppressed growth hormone levels after pituitary surgery in patients with acromegaly ANA LAURA ESPINOSA-DE-LOS-MONTEROS,
CLINICAL REVIEW: A Critical Analysis of Pituitary Tumor Shrinkage during Primary Medical Therapy in Acromegaly
 0021-972X/05/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 90(7):4405 4410 Printed in U.S.A. Copyright 2005 by The Endocrine Society doi: 10.1210/jc.2004-2466 CLINICAL REVIEW: A Critical
0021-972X/05/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 90(7):4405 4410 Printed in U.S.A. Copyright 2005 by The Endocrine Society doi: 10.1210/jc.2004-2466 CLINICAL REVIEW: A Critical
The efficacy of medical treatment in patients with acromegaly in clinical practice
 2018, 65 (1), 33-41 Original The efficacy of medical treatment in patients with acromegaly in clinical practice Seo Young Lee 1), Jung Hee Kim 1), 2), Ji Hyun Lee 1), Yong Hwy Kim 2), 3), Hyang Jin Cha
2018, 65 (1), 33-41 Original The efficacy of medical treatment in patients with acromegaly in clinical practice Seo Young Lee 1), Jung Hee Kim 1), 2), Ji Hyun Lee 1), Yong Hwy Kim 2), 3), Hyang Jin Cha
Clinical experiences and success rates of acromegaly treatment: the single center results of 62 patients
 Evran et al. BMC Endocrine Disorders 2014, 14:97 RESEARCH ARTICLE Open Access Clinical experiences and success rates of acromegaly treatment: the single center results of 62 patients Mehtap Evran *, Murat
Evran et al. BMC Endocrine Disorders 2014, 14:97 RESEARCH ARTICLE Open Access Clinical experiences and success rates of acromegaly treatment: the single center results of 62 patients Mehtap Evran *, Murat
Neurosurg Focus 29 (4):
:") Neurosurg Focus 29 (4):E6, 2010 Endoscopic endonasal transsphenoidal surgery for growth hormone secreting pituitary adenomas Ch r i s t o p h P. Ho f s t e t t e r, M.D., Ph.D., 1 Ra a i d H. Man n a a,
Neurosurg Focus 29 (4):E6, 2010 Endoscopic endonasal transsphenoidal surgery for growth hormone secreting pituitary adenomas Ch r i s t o p h P. Ho f s t e t t e r, M.D., Ph.D., 1 Ra a i d H. Man n a a,
Cost-Effectiveness of Somatostatin Analogues for the Treatment of Acromegaly in Colombia
 Open Journal of Endocrine and Metabolic Diseases, 2012, 2, 102-106 http://dx.doi.org/10.4236/ojemd.2012.24016 Published Online November 2012 (http://www.scirp.org/journal/ojemd) Cost-Effectiveness of Somatostatin
Open Journal of Endocrine and Metabolic Diseases, 2012, 2, 102-106 http://dx.doi.org/10.4236/ojemd.2012.24016 Published Online November 2012 (http://www.scirp.org/journal/ojemd) Cost-Effectiveness of Somatostatin
Intravenous octreotide test predicts the long term outcom e of treatm ent w ith octreotide-longacting repeatable in active acrom egaly
 11 Intravenous octreotide test predicts the long term outcom e of treatm ent w ith octreotide-longacting repeatable in active acrom egaly Nienke R. Biermasz, Alberto M. Pereira, Jan W.A. Smit, Johannes
11 Intravenous octreotide test predicts the long term outcom e of treatm ent w ith octreotide-longacting repeatable in active acrom egaly Nienke R. Biermasz, Alberto M. Pereira, Jan W.A. Smit, Johannes
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide)
") Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Managing Acromegaly: Biochemical Control with SIGNIFOR LAR (pasireotide) INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of
Managing Acromegaly: Review of Two Cases
 Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Managing Acromegaly: Review of Two Cases INDICATION AND USAGE SIGNIFOR LAR (pasireotide) for injectable suspension is a somatostatin analog indicated for the treatment of patients with acromegaly who have
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line
 for acromegaly first and second line") Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
Pasireotide Long-Acting Repeatable (Signifor) for acromegaly first and second line December 2010 This technology summary is based on information available at the time of research and a limited literature
Insulin-like growth factor 1 measurement in diagnosis and management of acromegaly
 Review Article Ann Clin Biochem 2001; 38: 297±303 Insulin-like growth factor 1 measurement in diagnosis and management of acromegaly Steven R Peacey 1 and Stephen M Shalet 2 From the 1 Department of Diabetes
Review Article Ann Clin Biochem 2001; 38: 297±303 Insulin-like growth factor 1 measurement in diagnosis and management of acromegaly Steven R Peacey 1 and Stephen M Shalet 2 From the 1 Department of Diabetes
Diagnostic features and outcome of surgical therapy of acromegalic patients: Experience of the last three decades
 HORMONES 2014, 13(1):95-103 Research paper Diagnostic features and outcome of surgical therapy of acromegalic patients: Experience of the last three decades Elisa Sala, 1,2 Emanuele Ferrante, 1,2 Marco
HORMONES 2014, 13(1):95-103 Research paper Diagnostic features and outcome of surgical therapy of acromegalic patients: Experience of the last three decades Elisa Sala, 1,2 Emanuele Ferrante, 1,2 Marco
Establishing the relationship between growth hormone. Correlation between GH and IGF-1 during treatment for. acromegaly.
 CLINICAL ARTICLE J Neurosurg 126:1959 1966, 2017 Correlation between GH and IGF-1 during treatment for acromegaly Edward H. Oldfield, MD, 1 John A. Jane Jr., MD, 1 Michael O. Thorner, MBBS, DSc, 2 Carrie
CLINICAL ARTICLE J Neurosurg 126:1959 1966, 2017 Correlation between GH and IGF-1 during treatment for acromegaly Edward H. Oldfield, MD, 1 John A. Jane Jr., MD, 1 Michael O. Thorner, MBBS, DSc, 2 Carrie
Case Report. Silent growth hormone secreting pituitary adenomas: IGF-1 is not sufficient to exclude growth hormone excess. Introduction.
 Case Report Silent growth hormone secreting pituitary adenomas: IGF-1 is not sufficient to exclude growth hormone excess S Kalavalapalli 1, H Reid 2, J Kane 3, H Buckler 1, P Trainer 4 and A H Heald 1,5
Case Report Silent growth hormone secreting pituitary adenomas: IGF-1 is not sufficient to exclude growth hormone excess S Kalavalapalli 1, H Reid 2, J Kane 3, H Buckler 1, P Trainer 4 and A H Heald 1,5
Treating a Growing Problem: A Closer Look at Acromegaly. Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD
 Nicholas Tritos, MD, DSc Brooke Swearingen, MD") Treating a Growing Problem: A Closer Look at Acromegaly Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD Goal Address key challenges faced by physicians who treat acromegaly
Treating a Growing Problem: A Closer Look at Acromegaly Lisa Nachtigall, MD (Moderator) Nicholas Tritos, MD, DSc Brooke Swearingen, MD Goal Address key challenges faced by physicians who treat acromegaly
The predictive value of an acute octreotide suppression test in patients with acromegaly
 Strinović et al. Review The predictive value of an acute octreotide suppression test in patients with acromegaly Mateja Strinović¹, Jelena Marinković Radošević¹, Gorana Mirošević¹, Hrvoje Ivan Pećina²,
Strinović et al. Review The predictive value of an acute octreotide suppression test in patients with acromegaly Mateja Strinović¹, Jelena Marinković Radošević¹, Gorana Mirošević¹, Hrvoje Ivan Pećina²,
ACROMEGALY IS A rare disorder usually caused by a
 0021-972X/05/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 90(10):5627 5631 Printed in U.S.A. Copyright 2005 by The Endocrine Society doi: 10.1210/jc.2005-0531 Cotreatment of Acromegaly with
0021-972X/05/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 90(10):5627 5631 Printed in U.S.A. Copyright 2005 by The Endocrine Society doi: 10.1210/jc.2005-0531 Cotreatment of Acromegaly with
Optimalization and cost management of lanreotide-autogel therapy in acromegaly
 European Journal of Endocrinology (2007) 157 571 577 ISSN 0804-4643 CLINICAL STUDY Optimalization and cost management of lanreotide-autogel therapy in acromegaly Pascale Abrams, Orsalia Alexopoulou 1,
European Journal of Endocrinology (2007) 157 571 577 ISSN 0804-4643 CLINICAL STUDY Optimalization and cost management of lanreotide-autogel therapy in acromegaly Pascale Abrams, Orsalia Alexopoulou 1,
Beneficial effect of dose escalation of Octreotide-LAR as first-line therapy in patients with acromegaly
 European Journal of Endocrinology (2007) 157 579 587 ISSN 0804-4643 CLINICAL STUDY Beneficial effect of dose escalation of Octreotide-LAR as first-line therapy in patients with acromegaly Annamaria Colao,
European Journal of Endocrinology (2007) 157 579 587 ISSN 0804-4643 CLINICAL STUDY Beneficial effect of dose escalation of Octreotide-LAR as first-line therapy in patients with acromegaly Annamaria Colao,
Management of acromegaly in Latin America: expert panel recommendations
 Pituitary (2010) 13:168 175 DOI 10.1007/s11102-009-0206-y Management of acromegaly in Latin America: expert panel recommendations Ariel Barkan Marcello D. Bronstein Oscar D. Bruno Alejandro Cob Ana Laura
Pituitary (2010) 13:168 175 DOI 10.1007/s11102-009-0206-y Management of acromegaly in Latin America: expert panel recommendations Ariel Barkan Marcello D. Bronstein Oscar D. Bruno Alejandro Cob Ana Laura
Changes in quality of life in patients with acromegaly after surgical remission A prospective study using SF-36 questionnaire
 2017, 64 (1), 27-38 Original Changes in quality of life in patients with acromegaly after surgical remission A prospective study using SF-36 questionnaire Shingo Fujio 1), Hiroshi Arimura 2), Hirofumi
2017, 64 (1), 27-38 Original Changes in quality of life in patients with acromegaly after surgical remission A prospective study using SF-36 questionnaire Shingo Fujio 1), Hiroshi Arimura 2), Hirofumi
Ac r o m e g a ly is a chronic disorder characterized by. Pharmacological management of acromegaly: a current perspective
 Neurosurg Focus 29 (4):E14, 2010 Pharmacological management of acromegaly: a current perspective Su n i l Man j i l a, M.D., 1 Os m o n d C. Wu, B.A., 1 Fa h d R. Kh a n, M.D., M.S.E., 1 Me h r e e n M.
Neurosurg Focus 29 (4):E14, 2010 Pharmacological management of acromegaly: a current perspective Su n i l Man j i l a, M.D., 1 Os m o n d C. Wu, B.A., 1 Fa h d R. Kh a n, M.D., M.S.E., 1 Me h r e e n M.
Research Article Expression of Somatostatin Receptor 2 in Somatotropinoma Correlated with the Short-Term Efficacy of Somatostatin Analogues
 Hindawi International Endocrinology Volume 2017, Article ID 9606985, 7 pages https://doi.org/10.1155/2017/9606985 Research Article Expression of Somatostatin Receptor 2 in Somatotropinoma Correlated with
Hindawi International Endocrinology Volume 2017, Article ID 9606985, 7 pages https://doi.org/10.1155/2017/9606985 Research Article Expression of Somatostatin Receptor 2 in Somatotropinoma Correlated with
Results of surgical and somatostatin analog therapies and their combination in acromegaly: a retrospective analysis of the German Acromegaly Register
 European Journal of Endocrinology (2008) 159 525 532 ISSN 0804-4643 CLINICAL STUDY Results of surgical and somatostatin analog therapies and their combination in acromegaly: a retrospective analysis of
European Journal of Endocrinology (2008) 159 525 532 ISSN 0804-4643 CLINICAL STUDY Results of surgical and somatostatin analog therapies and their combination in acromegaly: a retrospective analysis of
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
Case report. Ilan Shimon, 1 Wolfgang Saeger, 2 Luiz Eduardo Wildemberg, 3 Monica R. Gadelha 3
 HORMONES 2017, 16(1):84-91 Case report Somatotropinomas inadequately controlled with octreotide may over-respond to pasireotide: the importance of dose adjustment to achieve long-term biochemical control
HORMONES 2017, 16(1):84-91 Case report Somatotropinomas inadequately controlled with octreotide may over-respond to pasireotide: the importance of dose adjustment to achieve long-term biochemical control
Bronstein et al. BMC Endocrine Disorders (2016) 16:16 DOI /s
 16:16 DOI /s") Bronstein et al. BMC Endocrine Disorders (2016) 16:16 DOI 10.1186/s12902-016-0096-8 RESEARCH ARTICLE Open Access Switching patients with acromegaly from octreotide to pasireotide improves biochemical control:
Bronstein et al. BMC Endocrine Disorders (2016) 16:16 DOI 10.1186/s12902-016-0096-8 RESEARCH ARTICLE Open Access Switching patients with acromegaly from octreotide to pasireotide improves biochemical control:
Summary. Introduction ORIGINAL ARTICLE
 Clinical Endocrinology (2007) 67, 282 289 doi: 10.1111/j.1365-2265.2007.02878.x ORIGINAL ARTICLE Blackwell Publishing Ltd Long-term (up to 18 years) effects on GH/IGF-1 hypersecretion and tumour size of
Clinical Endocrinology (2007) 67, 282 289 doi: 10.1111/j.1365-2265.2007.02878.x ORIGINAL ARTICLE Blackwell Publishing Ltd Long-term (up to 18 years) effects on GH/IGF-1 hypersecretion and tumour size of
Shared Care Protocol
 THE SHEFFIELD AREA PRESCRIBING COMMITTEE Shared Care Protocol for Acromegaly Devised by: The Endocrine Unit Sheffield Teaching Hospitals NHS Trust Date approved: April 2002 Review Date: On publication
THE SHEFFIELD AREA PRESCRIBING COMMITTEE Shared Care Protocol for Acromegaly Devised by: The Endocrine Unit Sheffield Teaching Hospitals NHS Trust Date approved: April 2002 Review Date: On publication
Ac r o m e g a ly is an endocrine disorder characterized. A systematic analysis of disease control in acromegaly treated with radiosurgery
 Neurosurg Focus 29 (4):E13, 2010 A systematic analysis of disease control in acromegaly treated with radiosurgery Is a a c Ya n g, M.D., Wo n Kim, M.D., An t o n i o De Sa l l e s, M.D., Ph.D., and Marvin
Neurosurg Focus 29 (4):E13, 2010 A systematic analysis of disease control in acromegaly treated with radiosurgery Is a a c Ya n g, M.D., Wo n Kim, M.D., An t o n i o De Sa l l e s, M.D., Ph.D., and Marvin
Medical Management of Functioning Pituitary Adenoma: An Update
 REVIEW ARTICLE Neurol Med Chir (Tokyo) 54, 958 965, 2014 doi: 10.2176/nmc.ra.2014-0239 Online November 29, 2014 Medical Management of Functioning Pituitary Adenoma: An Update Yutaka OKI 1,2 Departments
REVIEW ARTICLE Neurol Med Chir (Tokyo) 54, 958 965, 2014 doi: 10.2176/nmc.ra.2014-0239 Online November 29, 2014 Medical Management of Functioning Pituitary Adenoma: An Update Yutaka OKI 1,2 Departments
Insulin-like growth factor-i: marker for diagnosis of acromegaly and monitoring the efficacy of treatment
 European Journal of Endocrinology (2003) 148 S15 S20 ISSN 0804-4643 Insulin-like growth factor-i: marker for diagnosis of acromegaly and monitoring the efficacy of treatment Georg Brabant Department of
European Journal of Endocrinology (2003) 148 S15 S20 ISSN 0804-4643 Insulin-like growth factor-i: marker for diagnosis of acromegaly and monitoring the efficacy of treatment Georg Brabant Department of
Eui Hyun Kim. Department of Medicine The Graduate School, Yonsei University
 Immediate postoperative growth hormone level and early postoperative oral glucose tolerance test as predictive tools for the long-term surgical remission in acromegaly Eui Hyun Kim Department of Medicine
Immediate postoperative growth hormone level and early postoperative oral glucose tolerance test as predictive tools for the long-term surgical remission in acromegaly Eui Hyun Kim Department of Medicine
Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease
 Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease Information Reader Box (IRB) to be inserted on inside front cover for documents
Clinical Commissioning Policy Proposition: Pasireotide: An injectable medical therapy for the treatment of Cushing's disease Information Reader Box (IRB) to be inserted on inside front cover for documents
Somatostatin Analog and Estrogen Treatment in a Tall Girl
 Clin Pediatr Endocrinol 1995; 4 (2): 163-167 Copyright (C) 1995 by The Japanese Society for Pediatric Endocrinology Somatostatin Analog and Estrogen Treatment in a Tall Girl Toshiaki Tanaka, Mari Satoh,
Clin Pediatr Endocrinol 1995; 4 (2): 163-167 Copyright (C) 1995 by The Japanese Society for Pediatric Endocrinology Somatostatin Analog and Estrogen Treatment in a Tall Girl Toshiaki Tanaka, Mari Satoh,
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Pharmacy Prior Authorization Somatostatin Analogs Clinical Guideline
 Sandostatin LAR (octreotide) Signifor (pasireotide) Signifor LAR (pasireotide) Somatuline Depot (lanreotide) octreotide FDA Approved Indications: Acromegaly: Octreotide Injection is indicated to reduce
Sandostatin LAR (octreotide) Signifor (pasireotide) Signifor LAR (pasireotide) Somatuline Depot (lanreotide) octreotide FDA Approved Indications: Acromegaly: Octreotide Injection is indicated to reduce
European Journal of Endocrinology (2006) ISSN
 ISSN") European Journal of Endocrinology (2006) 154 467 477 ISSN 0804-4643 CLINICAL STUDY Efficacy of 12-month treatment with the GH receptor antagonist pegvisomant in patients with acromegaly resistant to long-term,
European Journal of Endocrinology (2006) 154 467 477 ISSN 0804-4643 CLINICAL STUDY Efficacy of 12-month treatment with the GH receptor antagonist pegvisomant in patients with acromegaly resistant to long-term,
Clinical Policy: Pasireotide (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.332 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03.01.17 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the
Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03.01.17 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the
Development of acromegaly in patients with prolactinomas
 European Journal of Endocrinology (2003) 149 17 22 ISSN 0804-4643 CLINICAL STUDY Development of acromegaly in patients with prolactinomas Marianne Andersen, Casper Hagen, Jan Frystyk 1, Henrik Daa Schroeder
European Journal of Endocrinology (2003) 149 17 22 ISSN 0804-4643 CLINICAL STUDY Development of acromegaly in patients with prolactinomas Marianne Andersen, Casper Hagen, Jan Frystyk 1, Henrik Daa Schroeder
CLINICAL REVIEW 150 Somatostatin Analogs in Acromegaly
 0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(7):3013 3018 Printed in U.S.A. Copyright 2002 by The Endocrine Society CLINICAL REVIEW 150 Somatostatin Analogs in Acromegaly
0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(7):3013 3018 Printed in U.S.A. Copyright 2002 by The Endocrine Society CLINICAL REVIEW 150 Somatostatin Analogs in Acromegaly
Metabolic Glucose Status and Pituitary Pathology Portend Therapeutic Outcomes in Acromegaly
 Metabolic Glucose Status and Pituitary Pathology Portend Therapeutic Outcomes in Acromegaly Sonia Cheng 1, Rany Al-Agha 1., Paula B. Araujo 1., Omar Serri 3, Sylvia L. Asa 2, Shereen Ezzat 1 * 1 Department
Metabolic Glucose Status and Pituitary Pathology Portend Therapeutic Outcomes in Acromegaly Sonia Cheng 1, Rany Al-Agha 1., Paula B. Araujo 1., Omar Serri 3, Sylvia L. Asa 2, Shereen Ezzat 1 * 1 Department
Effect of Sex and Assay Method on Serum Concentrations of Growth Hormone in Patients with Acromegaly and in Healthy Controls
 Papers in Press. First published January 26, 2006 as doi:10.1373/clinchem.2005.060236 Clinical Chemistry 52:3 000 000 (2006) Endocrinology and Metabolism Effect of Sex and Assay Method on Serum Concentrations
Papers in Press. First published January 26, 2006 as doi:10.1373/clinchem.2005.060236 Clinical Chemistry 52:3 000 000 (2006) Endocrinology and Metabolism Effect of Sex and Assay Method on Serum Concentrations
Ultrasonographic Assessment of Soft Tissues in Patients With Acromegaly
 Arch Rheumatol 2015;30(2):138-143 doi: 10.5606/ArchRheumatol.2015.5158 ORIGINAL ARTICLE Ultrasonographic Assessment of Soft Tissues in Patients With Acromegaly Mustafa KOÇAK, 1 Nadim CİVAN, 1 Murat KARKUCAK,
Arch Rheumatol 2015;30(2):138-143 doi: 10.5606/ArchRheumatol.2015.5158 ORIGINAL ARTICLE Ultrasonographic Assessment of Soft Tissues in Patients With Acromegaly Mustafa KOÇAK, 1 Nadim CİVAN, 1 Murat KARKUCAK,
GH Receptor Antagonist: Mechanism of Action and Clinical Utility
 Reviews in Endocrine & Metabolic Disorders 2005;6:5 13 C 2005 Springer Science + Business Media, Inc. Manufactured in The Netherlands. GH Receptor Antagonist: Mechanism of Action and Clinical Utility Sowmya
Reviews in Endocrine & Metabolic Disorders 2005;6:5 13 C 2005 Springer Science + Business Media, Inc. Manufactured in The Netherlands. GH Receptor Antagonist: Mechanism of Action and Clinical Utility Sowmya
TABLES. Table 1: Imaging. Congress of Neurological Surgeons Author (Year) Description of Study Classification Process / Evidence Class
 Description of Study Classification Process / Evidence Class") TABLES Table 1: Imaging Kremer et al (2002) 2 Study Design: Prospective followed case series. Patient Population: Fifty adult patients with NFPA Study Description: Patients underwent MRI before surgery,
TABLES Table 1: Imaging Kremer et al (2002) 2 Study Design: Prospective followed case series. Patient Population: Fifty adult patients with NFPA Study Description: Patients underwent MRI before surgery,
Disappearance of a GH secreting macro adenoma, during long-term somatostatin analogue administration and recurrence following somatostatin withdrawal
 HORMONES 2006, 5(1):57-62 Case report Disappearance of a GH secreting macro adenoma, during long-term somatostatin analogue administration and recurrence following somatostatin withdrawal S. Livadas 1,
HORMONES 2006, 5(1):57-62 Case report Disappearance of a GH secreting macro adenoma, during long-term somatostatin analogue administration and recurrence following somatostatin withdrawal S. Livadas 1,
MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY
 Case Report MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY Murray B. Gordon, MD, FACE; Kellie L. Spiller, MS ABSTRACT Submitted for publication July
Case Report MANAGEMENT OF HYPERGLYCEMIA IN A PATIENT WITH ACROMEGALY TREATED WITH PASIREOTIDE LAR: A CASE STUDY Murray B. Gordon, MD, FACE; Kellie L. Spiller, MS ABSTRACT Submitted for publication July
Transsphenoidal surgery in acromegaly investigated by intraoperative high-field magnetic resonance imaging
 European Journal of Endocrinology (2005) 153 239 248 ISSN 0804-4643 CLINICAL STUDY Transsphenoidal surgery in acromegaly investigated by intraoperative high-field magnetic resonance imaging Rudolf Fahlbusch,
European Journal of Endocrinology (2005) 153 239 248 ISSN 0804-4643 CLINICAL STUDY Transsphenoidal surgery in acromegaly investigated by intraoperative high-field magnetic resonance imaging Rudolf Fahlbusch,
sphingotest vr-hgh Risk Prediction of Incident Cardiovascular Disease
 sphingotest vr-hgh Risk Prediction of Incident Cardiovascular Disease Human Growth Hormone as Vascular Risk Biomarker sphingotec offers the vascular risk human Growth Hormone biomarker (vr-hgh) for the
sphingotest vr-hgh Risk Prediction of Incident Cardiovascular Disease Human Growth Hormone as Vascular Risk Biomarker sphingotec offers the vascular risk human Growth Hormone biomarker (vr-hgh) for the
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Health-related quality of life in acromegalic subjects: data from AcroBel, the Belgian Registry on acromegaly
 European Journal of Endocrinology (2007) 157 411 417 ISSN 0804-4643 CLINICAL STUDY Health-related quality of life in acromegalic subjects: data from AcroBel, the Belgian Registry on acromegaly Guy T Sjoen,
European Journal of Endocrinology (2007) 157 411 417 ISSN 0804-4643 CLINICAL STUDY Health-related quality of life in acromegalic subjects: data from AcroBel, the Belgian Registry on acromegaly Guy T Sjoen,
Clinical Commissioning Policy: Pegvisomant for acromegaly as a third-line treatment (adults)
") Clinical Commissioning Policy: Pegvisomant for acromegaly as a third-line treatment (adults) Reference: NHS England: 16050/P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Clinical Commissioning Policy: Pegvisomant for acromegaly as a third-line treatment (adults) Reference: NHS England: 16050/P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
General Discussion and Conclusions
 16 General Discussion and Conclusions Chapter 16 254 I. Treatm ent of acrom egaly Transsphenoidal surgery Radiotherapy Pre-surgical som atostatin analog treatm ent Som atostatin analog treatm ent Current
16 General Discussion and Conclusions Chapter 16 254 I. Treatm ent of acrom egaly Transsphenoidal surgery Radiotherapy Pre-surgical som atostatin analog treatm ent Som atostatin analog treatm ent Current
Low insulin resistance after surgery predicts poor GH suppression one year after complete resection for acromegaly: a retrospective study
 2016, 63 (5), 469-477 Original Low insulin resistance after surgery predicts poor GH suppression one year after complete resection for acromegaly: a retrospective study Naoki Edo 1), 2), Koji Morita 2),
2016, 63 (5), 469-477 Original Low insulin resistance after surgery predicts poor GH suppression one year after complete resection for acromegaly: a retrospective study Naoki Edo 1), 2), Koji Morita 2),
Preoperative Short-term Administration of Octreotide for Facilitating Transsphenoidal Removal of Invasive
 Preoperative Short-term Administration of Octreotide for Facilitating Transsphenoidal Removal of Invasive Growth Hormone-secreting Macroadenomas Eiji TACHIBANA, Kiyoshi SAITO, and Jun YOSHIDA, Nagoya University
Preoperative Short-term Administration of Octreotide for Facilitating Transsphenoidal Removal of Invasive Growth Hormone-secreting Macroadenomas Eiji TACHIBANA, Kiyoshi SAITO, and Jun YOSHIDA, Nagoya University
Comorbidities, treatment patterns and cost-of-illness of acromegaly in Sweden: a register-linkage population-based study
 Clinical Study E Lesén and others Treatment and cost-of-illness 176:2 203 212 Comorbidities, treatment patterns and cost-of-illness in Sweden: a register-linkage population-based study Eva Lesén 1, Daniel
Clinical Study E Lesén and others Treatment and cost-of-illness 176:2 203 212 Comorbidities, treatment patterns and cost-of-illness in Sweden: a register-linkage population-based study Eva Lesén 1, Daniel
Professor Ian Holdaway. Endocrinologist Auckland District Health Board
 Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Metoclopramide Domperidone. HYPER- PROLACTINAEMIA: the true and the false problems
 Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Diabetes in acromegaly, prevalence, risk factors and evolution; data from the French acromegaly
 Page 1 of 27 Accepted Preprint first posted on 4 April 2011 as Manuscript EJE-10-1050 Title: Diabetes in acromegaly, prevalence, risk factors and evolution; data from the French acromegaly registry. Authors:
Page 1 of 27 Accepted Preprint first posted on 4 April 2011 as Manuscript EJE-10-1050 Title: Diabetes in acromegaly, prevalence, risk factors and evolution; data from the French acromegaly registry. Authors:
Medical Management of Growth Hormone-Secreting Pituitary Adenomas
 Pituitary 5: 67 76, 2002 C 2003 Kluwer Academic Publishers. Manufactured in The Netherlands. Medical Management of Growth Hormone-Secreting Pituitary Adenomas Michael S. Racine and Ariel L. Barkan Division
Pituitary 5: 67 76, 2002 C 2003 Kluwer Academic Publishers. Manufactured in The Netherlands. Medical Management of Growth Hormone-Secreting Pituitary Adenomas Michael S. Racine and Ariel L. Barkan Division
Ki-67 is a predictor of acromegaly control with octreotide-lar independent of SSTR2 status
 Page 1 of 24 Accepted Preprint first posted on 7 June 2013 as Manuscript EJE-13-0349 Ki-67 is a predictor of acromegaly control with octreotide-lar independent of SSTR2 status and relates to cytokeratin
Page 1 of 24 Accepted Preprint first posted on 7 June 2013 as Manuscript EJE-13-0349 Ki-67 is a predictor of acromegaly control with octreotide-lar independent of SSTR2 status and relates to cytokeratin
Chapter 2 Acromegaly, Awareness Is Paramount for Early Diagnosis: Highlights of Diagnosis and Treatment Challenges
 Chapter 2 Acromegaly, Awareness Is Paramount for Early Diagnosis: Highlights of Diagnosis and Treatment Challenges Jessica Brzana, Christine G. Yedinak, and Maria Fleseriu Objectives To highlight clinical
Chapter 2 Acromegaly, Awareness Is Paramount for Early Diagnosis: Highlights of Diagnosis and Treatment Challenges Jessica Brzana, Christine G. Yedinak, and Maria Fleseriu Objectives To highlight clinical
Long-term follow-up of patients with elevated IGF-1 and nadir GH > 0.4 µg/l but < 1 µg/l
 original article Long-term follow-up of patients with elevated IGF-1 and nadir GH > 0.4 µg/l but < 1 µg/l Pedro Weslley Rosario 1, Maria Regina Calsolari 1 ABSTRACT Objective: To report the results of
original article Long-term follow-up of patients with elevated IGF-1 and nadir GH > 0.4 µg/l but < 1 µg/l Pedro Weslley Rosario 1, Maria Regina Calsolari 1 ABSTRACT Objective: To report the results of
ACCORDING TO CONSENSUS criteria, acromegaly is
 0021-972X/06/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 91(10):3891 3896 Printed in U.S.A. Copyright 2006 by The Endocrine Society doi: 10.1210/jc.2006-0676 Quality of Life in Treated
0021-972X/06/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 91(10):3891 3896 Printed in U.S.A. Copyright 2006 by The Endocrine Society doi: 10.1210/jc.2006-0676 Quality of Life in Treated
SAGIT : clinician-reported outcome instrument for managing acromegaly in clinical practice development and results from a pilot study
 Pituitary (2016) 19:39 49 DOI 10.1007/s11102-015-0681-2 SAGIT : clinician-reported outcome instrument for managing acromegaly in clinical practice development and results from a pilot study Andrea Giustina
Pituitary (2016) 19:39 49 DOI 10.1007/s11102-015-0681-2 SAGIT : clinician-reported outcome instrument for managing acromegaly in clinical practice development and results from a pilot study Andrea Giustina
/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(1): Copyright 2002 by The Endocrine Society
: Copyright 2002 by The Endocrine Society") 0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(1):99 104 Printed in U.S.A. Copyright 2002 by The Endocrine Society Efficacy of the New Long-Acting Formulation of ( Autogel)
0013-7227/02/$15.00/0 The Journal of Clinical Endocrinology & Metabolism 87(1):99 104 Printed in U.S.A. Copyright 2002 by The Endocrine Society Efficacy of the New Long-Acting Formulation of ( Autogel)
Change in Somatostatinergic Tone of Acromegalic Patients according to the Size of Growth Hormone-Producing Pituitary Tumors
 ORIGINAL ARTICLE Endocrinology, Nutrition & Metabolism http://dx.doi.org/1.3346/jkms.213.28.12.1774 J Korean Med Sci 213; 28: 1774-178 Change in Somatostatinergic Tone of Acromegalic Patients according
ORIGINAL ARTICLE Endocrinology, Nutrition & Metabolism http://dx.doi.org/1.3346/jkms.213.28.12.1774 J Korean Med Sci 213; 28: 1774-178 Change in Somatostatinergic Tone of Acromegalic Patients according
Effects of the long-acting somatostatin analogue Lanreotide Autogel on glucose tolerance and insulin resistance in acromegaly
 European Journal of Endocrinology (26) 1 73 78 ISSN 84-4643 CLINICAL STUDY Effects of the long-acting somatostatin analogue Lanreotide Autogel on glucose tolerance and insulin resistance in acromegaly
European Journal of Endocrinology (26) 1 73 78 ISSN 84-4643 CLINICAL STUDY Effects of the long-acting somatostatin analogue Lanreotide Autogel on glucose tolerance and insulin resistance in acromegaly
TREATMENT OF ACROMEGALY WITH THE GROWTH HORMONE RECEPTOR ANTAGONIST PEGVISOMANT
 TREATMENT OF ACROMEGALY WITH THE GROWTH HORMONE RECEPTOR ANTAGONIST PEGVISOMANT PETER J. TRAINER, M.D., WILLIAM M. DRAKE, M.B., LAURENCE KATZNELSON, M.D., PAMELA U. FREDA, M.D., VIVIEN HERMAN-BONERT, M.D.,
TREATMENT OF ACROMEGALY WITH THE GROWTH HORMONE RECEPTOR ANTAGONIST PEGVISOMANT PETER J. TRAINER, M.D., WILLIAM M. DRAKE, M.B., LAURENCE KATZNELSON, M.D., PAMELA U. FREDA, M.D., VIVIEN HERMAN-BONERT, M.D.,
Clinical Commissioning Policy: Pasireotide for acromegaly as thirdline treatment (adults)
") Clinical Commissioning Policy: Pasireotide for acromegaly as thirdline treatment (adults) Reference: NHS England: 16003/P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Clinical Commissioning Policy: Pasireotide for acromegaly as thirdline treatment (adults) Reference: NHS England: 16003/P NHS England INFORMATION READER BOX Directorate Medical Operations and Information
Usefulness of the Thyrotropin-Releasing Hormone Test in Pre-Clinical Acromegaly
 Tohoku J. Exp. Med., 2005, 206, 291-297 Pre-Clinical Acromegaly 291 Usefulness of the Thyrotropin-Releasing Hormone Test in Pre-Clinical Acromegaly KAZUNORI KAGEYAMA, TAKAKO MORIYAMA, SATORU SAKIHARA,
Tohoku J. Exp. Med., 2005, 206, 291-297 Pre-Clinical Acromegaly 291 Usefulness of the Thyrotropin-Releasing Hormone Test in Pre-Clinical Acromegaly KAZUNORI KAGEYAMA, TAKAKO MORIYAMA, SATORU SAKIHARA,
Clinical Policy: Pasireotide (Signifor LAR) Reference Number: CP.PHAR.332
 Reference Number: CP.PHAR.332") Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Signifor LAR) Reference Number: CP.PHAR.332 Effective Date: 03/17 Last Review Date: 02/17 Coding Implications Revision Log See Important Reminder at the end of this policy for important
Long-term results of gamma knife surgery for growth hormone producing pituitary adenoma: is the disease difficult to cure?
 J Neurosurg (Suppl) 102:119 123, 2005 Long-term results of gamma knife surgery for growth hormone producing pituitary adenoma: is the disease difficult to cure? TATSUYA KOBAYASHI, M.D., PH.D., YOSHIMASA
J Neurosurg (Suppl) 102:119 123, 2005 Long-term results of gamma knife surgery for growth hormone producing pituitary adenoma: is the disease difficult to cure? TATSUYA KOBAYASHI, M.D., PH.D., YOSHIMASA
Therapeutic trends and outcome of acromegaly: a single center experience over a 40-year period
 HORMONES 2016, 15(3):368-376 Research paper Therapeutic trends and outcome of acromegaly: a single center experience over a 40-year period Olga Karapanou, Marinella Tzanela, Marietta Christoforaki, Lida
HORMONES 2016, 15(3):368-376 Research paper Therapeutic trends and outcome of acromegaly: a single center experience over a 40-year period Olga Karapanou, Marinella Tzanela, Marietta Christoforaki, Lida
Acromegaly is a rare serious condition characterized by. Pasireotide Versus Octreotide in Acromegaly: A Headto-Head Superiority Study
 ORIGINAL ARTICLE Endocrine Care Pasireotide Versus Octreotide in Acromegaly: A Headto-Head Superiority Study A. Colao, M. D. Bronstein, P. Freda, F. Gu, C.-C. Shen, M. Gadelha, M. Fleseriu, A. J. van der
ORIGINAL ARTICLE Endocrine Care Pasireotide Versus Octreotide in Acromegaly: A Headto-Head Superiority Study A. Colao, M. D. Bronstein, P. Freda, F. Gu, C.-C. Shen, M. Gadelha, M. Fleseriu, A. J. van der
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Sandostatin, Sandostatin LAR Depot) Reference Number: CP.PHAR.40 Effective Date: 03.01.10 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log
Clinical Policy: (Sandostatin, Sandostatin LAR Depot) Reference Number: CP.PHAR.40 Effective Date: 03.01.10 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Coding Implications Revision Log
Efficacy and Safety of Cabergoline as First Line Treatment for Invasive Giant Prolactinoma
 J Korean Med Sci 2009; 24: 874-8 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.5.874 Copyright The Korean Academy of Medical Sciences Efficacy and Safety of Cabergoline as First Line for Invasive Giant Prolactinoma
J Korean Med Sci 2009; 24: 874-8 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.5.874 Copyright The Korean Academy of Medical Sciences Efficacy and Safety of Cabergoline as First Line for Invasive Giant Prolactinoma
Long-Term Octreotide Therapy in Growth Hormone Secreting Pituitary Adenomas: Evaluation with Serial MR
 Long-Term Octreotide Therapy in Growth Hormone Secreting Pituitary Adenomas: Evaluation with Serial MR P. Lundin, B. Edén Engström, F. A. Karlsson, and P. Burman PURPOSE: To compare the changes in tumor
Long-Term Octreotide Therapy in Growth Hormone Secreting Pituitary Adenomas: Evaluation with Serial MR P. Lundin, B. Edén Engström, F. A. Karlsson, and P. Burman PURPOSE: To compare the changes in tumor
Reduction in Cutis Verticis Gyrata after Transsphenoidal Pituitary Resection of Growth Hormone Secreting Adenoma
 84 Original Article THIEME Reduction in Cutis Verticis Gyrata after Transsphenoidal Pituitary Resection of Growth Hormone Secreting Adenoma Daniel Pinggera 1 Delia Anna Marsoner 1 Marcel Seiz-Rosenhagen
84 Original Article THIEME Reduction in Cutis Verticis Gyrata after Transsphenoidal Pituitary Resection of Growth Hormone Secreting Adenoma Daniel Pinggera 1 Delia Anna Marsoner 1 Marcel Seiz-Rosenhagen
Pegvisomant increases intra-abdominal fat in patients with acromegaly: a pilot study
 European Journal of Endocrinology (2008) 158 467 471 ISSN 0804-4643 CLINICAL STUDY Pegvisomant increases intra-abdominal fat in patients with acromegaly: a pilot study U Plöckinger and T Reuter Interdisziplinäres
European Journal of Endocrinology (2008) 158 467 471 ISSN 0804-4643 CLINICAL STUDY Pegvisomant increases intra-abdominal fat in patients with acromegaly: a pilot study U Plöckinger and T Reuter Interdisziplinäres
AN UNUSUAL CASE OF LYMPHOCYTIC HYPOPHYSITIS IN A YOUNG MAN PRESENTING WITH ELEVATED SERUM IGF-1. C. Chadha, E. R. Seaquist*
 AN UNUSUAL CASE OF LYMPHOCYTIC HYPOPHYSITIS IN A YOUNG MAN PRESENTING WITH ELEVATED SERUM IGF-1 C. Chadha, E. R. Seaquist* Case Report doi: 10.4183/aeb.2009.391 Division of Endocrinology and Metabolism,
AN UNUSUAL CASE OF LYMPHOCYTIC HYPOPHYSITIS IN A YOUNG MAN PRESENTING WITH ELEVATED SERUM IGF-1 C. Chadha, E. R. Seaquist* Case Report doi: 10.4183/aeb.2009.391 Division of Endocrinology and Metabolism,
# %# & ( # # # ) # ) # % # +# (,#. # # / # 0# # )# # %# % # (, 1 # ) 2! 3.. ) # # 0 46# : ;%%& < 87=!!7=!
 # ) # % # +# (,#. # # / # 0# # )# # %# % # (, 1 # ) 2! 3.. ) # # 0 46# : ;%%& < 87=!!7=!") ! # %# & ( # # # ) # ) # % # +# (,#. # # / # 0# # )# # %# % # (, 1 # ) 2! 3.. ) 4 2 3 56. 4 6# # 0 46# 7 283 898 89: ;%%& 8 779 + 4 < 87=!!7=! 8 99 + > Clinical Endocrinology (2008) 68, 343 349 doi: 10.1111/j.1365-2265.2007.03044.x
! # %# & ( # # # ) # ) # % # +# (,#. # # / # 0# # )# # %# % # (, 1 # ) 2! 3.. ) 4 2 3 56. 4 6# # 0 46# 7 283 898 89: ;%%& 8 779 + 4 < 87=!!7=! 8 99 + > Clinical Endocrinology (2008) 68, 343 349 doi: 10.1111/j.1365-2265.2007.03044.x
PITUITARY ADENOMAS. Effective Date: August, 2012
 CLINICAL PRACTICE GUIDELINE CNS-00 PITUITARY ADENOMAS Effective Date: August, 2012 The recommendations contained in this guideline are a consensus of the Alberta Provincial CNS Tumour Team synthesis of
CLINICAL PRACTICE GUIDELINE CNS-00 PITUITARY ADENOMAS Effective Date: August, 2012 The recommendations contained in this guideline are a consensus of the Alberta Provincial CNS Tumour Team synthesis of
G rowth hormone (GH) is an anabolic
 is an anabolic") 24 REVIEW Growth hormone and its disorders J Ayuk, M C Sheppard... Growth hormone (GH) is synthesised and secreted by the somatotroph cells of the anterior lobe of the pituitary gland. Its actions involve
24 REVIEW Growth hormone and its disorders J Ayuk, M C Sheppard... Growth hormone (GH) is synthesised and secreted by the somatotroph cells of the anterior lobe of the pituitary gland. Its actions involve
Acromegaly: a challenging condition to diagnose and manage. C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton
 Acromegaly: a challenging condition to diagnose and manage C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton Acromegaly: a challenging condition to diagnose and manage? Objectives: n Know the
Acromegaly: a challenging condition to diagnose and manage C. L. Chik, MD, PhD, FRCPC University of Alberta, Edmonton Acromegaly: a challenging condition to diagnose and manage? Objectives: n Know the
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.