CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Rosnawati Yahya
|
|
|
- Luke Walsh
- 5 years ago
- Views:
Transcription
1 CHAPTER 5 Editor: Dr Rosnawati Yahya Expert Panels: Dr Rosnawati Yahya Dr Ng Kok Peng Dr Suryati Binti Yakaob Dr Mohd Zaimi Abd Wahab Dr Yee Seow Ying Dr Wong Hin Seng Contents 5. Stock and Flow of Renal Transplantation Stock and Flow Transplant Rates 5. Recipients Characteristics Demographics, Clinical and Serology Status Primary Causes of ESRF 5.3 Transplant Practices Type of Transplant Place of Transplant 5.4 Transplant Outcomes Post Transplantation Complications Biochemical Outcome Deaths and Graft Loss 5.5 Patient and Graft Survival 5.6 Cardiovascular Risk in Renal Transplant Recipients 5.7 QoL Index Score in Renal Transplant Recipients
2 List of Tables Table 5..: Stock and flow of renal transplantation, Table 5..: New transplant rate per million population (pmp), Table 5..3: Transplant prevalence rate per million population (pmp), Table 5..4: Place of transplantation, Table 5..: Renal transplant recipients characteristics, Table 5..: Primary causes of end stage renal failure, Table 5.3.: Type of renal transplantation, Table 5.3.: Biochemical data, Table 5.3.3: Immunosuppressive Medications, Table 5.3.4: Non immunosuppressive medications, Table 5.4.: Post transplant complications, Table 5.4.: Transplant patient death rate and graft loss, Table 5.4.3: Causes of death in transplant recipients, Table 5.4.4: Causes of graft failure, Table 5.5.(a): Patient survival, Table 5.5.(b): Risk factors for transplant recipient mortality Table 5.5.(a): Graft survival, Table 5.5.(b): Risk factors for transplant graft loss Table 5.5.3: Unadjusted patient survival by type of transplant, Table 5.5.4: Graft survival by type of transplant, Table 5.5.5(a): Patient survival by year of transplant (Living related transplant, 7-6)... 8 Table 5.5.5(b): Graft survival by year of transplant (Living related transplant, 7-6)... 9 Table 5.5.6(a): Patient survival by year of transplant (Commercial cadaver transplant, 7-6)... 9 Table 5.5.6(b): Graft survival by year of transplant (commercial cadaver transplant, 7-6)... Table 5.6.: Risk factors for IHD in renal transplant recipients at year Table 5.6.(a): Systolic BP, Table 5.6.(b): Diastolic BP, Table 5.6.3(a): Treatment for hypertension, Table 5.6.3(b): Distribution of systolic BP without antihypertensives, Table 5.6.3(c): Distribution of diastolic BP without antihypertensives, Table 5.6.3(d): Distribution of systolic BP on antihypertensives, Table 5.6.3(e): Distribution of diastolic BP on antihypertensives, Table 5.6.4: CKD stages, Table 5.6.5: BMI, Table 5.6.6(a): LDL, Table 5.6.6(b): Total cholesterol, Table 5.6.6(c): HDL, Table 5.7.: Cumulative distribution of QoL-Index score in relation to dialysis modality, transplant recipient patients Table 5.7.: Cumulative distribution of QoL-Index score in relation to diabetes mellitus, transplant recipient patients Table 5.7.3: Cumulative distribution of QoL-Index score in relation to gender, transplant recipient patients
3 List of Tables (cont.) Table 5.7.4: Cumulative distribution of QoL-Index score in relation to age, transplant recipient patients Table 5.7.5: Cumulative distribution of QoL-Index score in relation to year of entry, transplant recipient patients List of Figures Figure 5..: Stock and flow of renal transplantation, Figure 5..: New transplant rate, Figure 5..3: Transplant prevalence rate, Figure 5..4(a): Places of transplantation, Figure 5..4(b): Place of transplantation within Malaysia... 6 Figure 5.4.(a): Transplant recipient death rate, Figure 5.4.(b): Transplant recipient graft loss rate, Figure 5.5.(a): Patient survival, Figure 5.5.(a): Graft survival, Figure 5.5.3: Patient survival by type of transplant, Figure 5.5.4: Graft survival by type of transplants, Figure 5.5.5(a): Patient survival by year of transplant (Living related transplant, 7-6)...9 Figure 5.5.5(b): Graft survival by year of transplant (Living related transplant, 7-6)... 9 Figure 5.5.6(a): Patient survival by year of transplant (Commercial cadaver transplant, 7-6)... Figure 5.5.6(b): Graft survival by year of transplant (Commercial cadaver transplant, 7-6)... Figure 5.6.(a): Venn diagram for pre and post transplant complications (in %) at year... Figure 5.6.(b): Venn diagram for pre and post transplant complications (in %) at year 3... Figure 5.6.(c): Venn diagram for pre and post transplant complications (in %) at year 4... Figure 5.6.(d): Venn diagram for pre and post transplant complications (in %) at year 5... Figure 5.6.(e): Venn diagram for pre and post transplant complications (in %) at year 6... Figure 5.6.(a): Systolic BP, Figure 5.6.(b): Diastolic BP, Figure 5.6.4: CKD stages by year... 3 Figure 5.6.5: BMI, Figure 5.6.6(a): LDL, Figure 5.6.6(b): Total cholesterol, Figure 5.6.6(c): HDL, Figure 5.7.: Cumulative distribution of QoL-Index score in relation to dialysis modality, transplant recipient patients Figure 5.7.: Cumulative distribution of QoL-Index score in relation to diabetes mellitus, transplant recipient patients Figure 5.7.3: Cumulative distribution of QoL-Index score in relation to gender, transplant recipient patients Figure 5.7.4: Cumulative distribution of QoL-Index score in relation to age, transplant recipient patients Figure 5.7.5: Cumulative distribution of QoL-Index score in relation to year of entry, transplant recipient patients
4 5. STOCK AND FLOW The number of new transplant patients decreased from 3 in 7 to its lowest in 6 with only 8 transplant surgeries performed in 6. This substantial reduction in the number of new transplants was predominantly due to reduction in the number of transplantation performed in Kuala Lumpur and Selayang Hospital which have been the main transplant centres in Malaysia. The number of transplant performed in China has remained relatively static. However, the was an increase in the number of transplant performed in other overseas countries. It is disturbing to observe that the number of new transplants decreased by 4% with only 48 transplant performed in 6. The number of functioning renal transplants had increased by 8% from 795 in 7 to 9 in and declined steadily from onwards with 84 functioning renal transplant in 6 (Table 5..). Despite advances in immunosuppression, the rate of allograft failure remained the same with -3% of allograft loss every year. Table 5..: Stock and flow of renal transplantation, New transplant patients Died Graft failure Lost to Follow up Functioning graft at 3 st December Figure 5..: Stock and flow of renal transplantation, 7-6 New patients Functioning graft at 3st Dec,,8,6 No. of patients,4,, The incidence rate of renal transplantation had remained static in the last ten years which is between 3 to 5 per million population (Table & Figure 5..). This is extremely low in comparison to Australia and New Zealand, which reported 37 and 7 per million population in. Table 5..: New transplant rate per million population (pmp), New transplant patients New transplant rate, pmp
5 Table 5..3: Transplant prevalence rate per million population (pmp), Functioning graft at 3 st December Transplant prevalence rate, pmp The transplant prevalence rate continue to drop over the last years at 66 per million population in 7 to 59 per million population in 6 (Table & Figure 5..3). Figure 5..: New transplant rate, Rate, pmp Figure 5..3: Transplant prevalence rate, Rate, pmp New Transplant rate, pmp Transplant Prevalence rate, pmp Transplantation in local centers increased with 5 transplants performed in 6, increasing to 86 transplants in. Unfortunately, this increase was not sustained and the number of renal transplants performed in local centers had remained static in and 3, and subsequently decline to its lowest level at 48 transplants performed in 6. This is disturbing as it underscores our failure to improve rate of transplantation within the country, which is mainly due to the lack of both living as well as cadaveric donors. It was encouraging to see that the number of transplants performed in China continued to drop from 65 cases (49.6%) in 8 down to cases (. %) in 3. Unfortunately, the figure rose to 6 cases (4.8%) in 6. It is worrying to see the number of transplants performed in other overseas centres continue to increase with cases reported in 6 (Table 5..4 and Figure 5..4 (a)). The number of transplants performed in Hospital Kuala Lumpur dropped significantly from 39 transplants in 5 to only 8 transplant in 6. Similar trend was seen in Selayang Hospital from 6 transplants performed in 5 to only 9 transplants erformed in 6 The number of transplants performed in University Malaya Medical Centre is showing an encouraging improvement with 8 tranplants in to 7 transplants in 6 (Table 5..4 and Figure 5..4 (b)). Figure 5..4(a): Places of transplantation, 7-6 Local Other overseas China Unknown India Number
6 Figure 5..4(b): Place of transplantation within Malaysia HKL PPUKM Prince Court UMMC Selayang Hospital Other local Table 5..4: Place of transplantation, HKL PPUKM Prince Court Medical Centre UMMC Selayang Hospital Other local China India Other overseas Unknown Total HKL PPUKM 3.8 Prince Court Medical Centre UMMC Selayang Hospital Other local.9 China India.9. Other overseas Unknown Total
7 5. RECIPIENTS CHARACTERISTICS Over the last years, the mean age of recipients at the time of transplantation increased steadily from 37 years to 44 years. More male patients underwent renal transplantation yearly (Table 5..). For the past ten years, the proportion of diabetic patients who underwent renal transplantation decreased slowly from 8% in 6 and only % in 5, however there was a rebound in the number of diabetic patients who went for transplant in 6. Patients with hepatitis B had decreased from 7% earlier to -6% yearly in the last 3 years. The overall number of patients with hepatitis C who went for renal transplantation remained low which ranged from % to 9% yearly. In terms of underlying cause of end stage renal failure (Table 5..), the commonest cause was glomerulonephritis (GN), hypertension followed by diabetes. The proportion of transplant recipients having end stage renal disease due to unknown causes had decreased from 44% in 6 to 5% in 6. Table 5..: Renal transplant recipients characteristics, New Transplant Patients Age at transplant (years), Mean Age at transplant (years), SD % Male % Diabetic (co-morbid/ primary renal disease) % HBsAg positive % Anti-HCV positive Table 5..: Primary causes of end stage renal failure, New transplant patients Glomerulonephritis Diabetes Mellitus Hypertension Obstructive uropathy ADPKD Drugs/ toxic nephropathy Hereditary nephritis Unknown Others New transplant patients Glomerulonephritis Diabetes Mellitus Hypertension Obstructive uropathy ADPKD Drugs/ toxic nephropathy Hereditary nephritis 3 3 Unknown Others
8 5.3 TRANSPLANT PRACTICES 5.3. Type of renal transplantation The proportion of commercial transplantation had reduced in time from 44. % in 7 to 39 % in 6. This was predominantly due to the marked decline in commercial cadaveric transplantation (39.8% in 7 to 4 % in 3). However, since 4, the percentage of commercial cadaveric transplantation has slowly increased to.% in 6. There number of commercial living transplantation fluctuated from 4.4 % in 7, peaked at 6.6 % in gradually decline then but slowly increase and peaked at 6.8 % in 6. Local cadaveric transplantation made up % of transplants (9 recipients) in 6, which was the lowest ever seen in the last ten years. Local living donor transplantation had shown an initial rise from 36 transplants in 7, peaked at 63 transplants (67.3%) in 3. Unfortunately, this rise was not sustained and the number of local living donor transplants dropped to 35 (3.3%) recipients in 4 and 3 (7.4%) in 5. In 6, there was a rise in number of local living donor transplants, 4 recipients (5% out of all renal transplantations). The year 7 marked the first time where there were more local transplants (55%) compared to overseas commercial transplants (45%). Since then, the proportion of local transplants continued to rise which peaked in 3 with 86.9% of the total transplantation performed locally. However, then onwards proportion declined slowly with 79.% in 4, 75% in 5 and 6% in 6. The declined in numbers were mainly due to lower number of renal transplant operations in 4-5 for various technical reasons. Table 5.3.: Type of renal transplantation, Commercial cadaver Commercial live donor Live donor (genetically related) Live donor (emotionally related) Cadaver Total Commercial cadaver Commercial live donor Live donor (genetically related) Live donor (emotionally related) Cadaver Total *Commercial Cadaver (China, India, other oversea) *Commercial live donor (living unrelated) *Cadaver (local) 8
9 5.3. Biochemical data Table 5.3. summarised the biochemical data for all the transplant recipients from to 6. Table 5.3.: Biochemical data, -6 Biochemical parameter Summary Creatinine, umol/l n Mean SD Median Minimum 36 9 Maximum Hb, g/dl n Mean SD Median Minimum Maximum Albumin, g/l n Mean SD Median Minimum 9 9 Maximum Calcium, mmol/l n Mean SD..... Median Minimum Maximum Phosphate, mmol/l n Mean..... SD Median..... Minimum Maximum Alkaline phosphate (ALP), U/L n Mean SD Median Minimum Maximum ALT, U/L n Mean SD Median Minimum Maximum Total cholesterol, mmol/l n Mean SD Median Minimum Maximum LDL cholesterol, mmol/l n Mean SD Median Minimum
10 Table 5.3.: Biochemical data, -6 (cont ) Biochemical parameter Summary Maximum HDL cholesterol, mmol/l n Mean SD Median Minimum Maximum Systolic blood pressure, mmhg n Mean SD Median Minimum Maximum 45 9 Diastolic blood pressure, mmhg n Mean SD Median Minimum Maximum Immunosuppression medications Majority of patients were on combination immunosuppression with very small numbers on single immunosuppression drugs either prednisolone predominantly, followed by calcineurin inhibitors, antiproliferative agents and proliferation signal inhibitor (PSI). Calcineurin-inhibitor based therapy remained the mainstay immunosuppressive therapy with 86% of patients receiving it in 6. Cyclosporin was the most widely used calcineurin inhibitors until 3. However, there was a gradual decline in cyclosporine usage with 5% in to 36% in 6 which coincided with the increasing use of tacrolimus, of which 39% in to 45% in 4 and 5% in 6. The usage of anti-proliferative agents had shown similar trend over the last 5 years. The used of azathioprine continue to decline from 5% in to % in 5 and remain static in 6. The use of mycophenolic acid fluctuated between 6 to 68% from to 6. (Figure 5.3.3) The use of proliferation signal inhibitor (PSI) has increased slowly in time from 6% in to 9% in 6. Table 5.3.3: Immunosuppressive Medications, -6 Medication data All (i) Immunosuppressive drug(s) treatment Prednisolone Cyclosporin A Single drug treatment Tacrolimus (FK56) Azathioprine MPA PSI 4 4 Others
11 Combined drug treatment Medication data All (i) Immunosuppressive drug(s) treatment Prednisolone Cyclosporin A Tacrolimus (FK56) Azathioprine MPA PSI Others Non immunosuppression medications In terms of non-immunosuppressive medications, calcium channel blockers are the most commonly used antihypertensive as a single or combination agent contributing to 65% of usage. This is followed by beta blockers with 4% of patients on it either alone or in combination with other medications in 6. The use of ACE inhibitors or angiotensin receptor blocker or both showed % increment over the last 5 years; 35% of patients were on ACE inhibitors or angiotensin II receptor blockers (AIIRB) or both in and this has increased to 4 % in 4 and 45% in 6. The usage of alpha blockers either as single drug or in combination has been consistently low as there may be an associated risk of heart failure with usage of the drug. Despite CAD related death is high amongst recipients, the usage of anti-lipid remains very low. Table 5.3.4: Non immunosuppressive medications, -6 Single drug treatment Medication data All Non Immunosuppressive drug(s) treatment Alpha blocker Beta blocker Calcium channel blocker ACE inhibitor ARBs Anti-lipid 3 Other antihypertensive Combined drug treatment Medication data All Non Immunosuppressive drug(s) treatment Alpha blocker Beta blocker Calcium channel blocker ACE inhibitor ARBs Anti-lipid Other antihypertensive 3 6 6
12 5.4 TRANSPLANT OUTCOMES 5.4. Post transplant complications Hypertension remained as the most common comorbidity seen in the kidney transplant recipients pre and post-transplantation with 53% and 33% respectively. Only % of the patients had diabetes pre-transplant. 6% either developed diabetes post operatively or had existing diabetes as a comorbid after the transplant. Future data should focus on the development of NODAT and try to explain the discrepancy between the drop in proportion of patients with diabetes pre and post-operatively. In terms of cardiovascular and cerebrovascular disease, 3% had either or both prior to transplant and another % developed these complications post transplanted. This should raise concerns with regards to the detection of cardiovascular diseases as the proportion diagnosed were small given that cardiovascular event was the third most common cause of death in our transplant recipients. Cancer remains uncommon both before and after transplantation. Table 5.4.: Post transplant complications, -6 All patients Diabetes (either as primary renal disease or comorbid) Cancer Pre transplant Cardiovascular disease + cerebrovascular disorder Hypertension All patients Diabetes (either as primary renal disease or comorbid) Cancer n % 784 Post transplant n % n % n % n % Cardiovascular disease + cerebrovascular disorder Hypertension *Hypertension: BP systolic >4 and BP diastolic >9 or have either Beta blocker/ Calcium channel blocker / ACE inhibitor / ARBs/ Other antihypertensive 5.4. Deaths and graft loss In 6, 49 transplant recipients died and 54 lost their grafts. The annual rates of transplant death dropped to.7% while grafts lost remained static at 3% (Table 5.4.). The main cause of death in 6 was unknown in 9% of the transplant recipients. This was followed by infection with 8% and cardiovascular with 6% respectively. The proportion of patients who died from infection showed an improvement but the proportions of unknown causes were much higher in 6 compared to 5. Establishing the cause of death will be important to devise a better management plan for our patients. The proportion of patient who died at home, which was usually presumed to be cardiovascular related was 7%. Death due to cancers in 6 contributed to % of all deaths (Table 5.4.3).
13 Majority of the graft losses had an unknown cause with 43%. Rejection was second with 4% followed by chronic allograft nephropathy/ifta with 3% (Table 5.4.4). Determining the cause of graft loss is of utmost importance to better understand the reasons for graft failure in our population. Therefore, the need to diagnose them appropriately should be attempted whenever possible. Table 5.4.: Transplant patient death rate and graft loss, Number at risk Transplant death Transplant death rate % Graft loss Graft loss rate % Acute rejection Acute rejection rate % All losses All losses rate % *Graft loss=graft failure *All losses=death / graft loss (acute rejection happens concurrently with graft failure / death) Figure 5.4.(a): Transplant recipient death rate, 7-6 Death rate % Annual death rate Graft loss rate % Figure 5.4.(b): Transplant recipient graft loss rate, Annual graft loss rate Table 5.4.3: Causes of death in transplant recipients, Cardiovascular Died at home Infection Graft failure Cancer Liver disease Accidental death Others Unknown Total
14 Table 5.4.3: Causes of death in transplant recipients, 7-6 (cont ) Cardiovascular Died at home Infection Graft failure 4 3 Cancer Liver disease Accidental death 4 Others 3 Unknown Total Table 5.4.4: Causes of graft failure, Rejection Calcineurin toxicity 3 3 Other drug toxicity 3 Ureteric obstruction Infection 5 Vascular causes Recurrent/ de novo renal disease 3 Chronic allograft nephropathy / IFTA Technical problem Others Unknown Total Rejection Calcineurin toxicity Other drug toxicity Ureteric obstruction Infection Vascular causes Recurrent/ de novo renal disease Chronic allograft nephropathy / IFTA Technical problem Others Unknown Total PATIENT AND GRAFT SURVIVAL 5.5. Patient survival Patient survival rates from 7 6 were 96% at year, 9% at year-5 and 7% at year- post transplantation. Risk factors affecting patient survival were primary diagnosis and type of transplant. Patients with deceased donor renal transplantation had higher risk of mortality compared to living renal transplant. 4
15 Table 5.5.(a): Patient survival, 7-6 Interval % n (years) Survival SE *n=number at risk SE=standard error Figure 5.5.(a): Patient survival, 7-6 Cumulative survival Transplant patient survival, Duration in years Table 5.5.(b): Risk factors for transplant recipient mortality 7-6 Factors of transplant 7- (ref*) n 479 Hazard Ratio Age at transplant -39 (ref*) >=55 Gender Male (ref*) 57. Female Primary diagnosis Unknown primary (ref*) 77. Diabetes mellitus GN/SLE Polycystic kidney Obstructive nephropathy 6.38 Others Type of transplant Commercial cadaver (ref*) 7. Commercial live donor Living donor 3.4 Cadaver (Deceased donor) HBsAg Negative (ref*) 833. Positive NA Anti-HCV Negative (ref*) 833. Positive NA 95% CI (.946,.59) (.983,.3) (.59, 4.65) (.675,.43) (.95,.83) (.676,.6) (.49,.763) (.849, 6.36) (.3, 3.5) (.87,.674) (.677,.9) (.54, 4.84) NA NA P value NA NA 5.5. Graft survival Graft loss rates reported below was not censored for death. Graft survival rates were 9% at year-, 8% at year-5 and 57% at year- post transplantation. Older age and patients with cadaver renal transplantation had higher risk of graft loss. 5
16 Table 5.5.(a): Graft survival, 7-6 Interval % n (years) Survival SE *n=number at risk SE=standard error Figure 5.5.(a): Graft survival, 7-6 Cumulative survival Transplant graft survival, Duration in years Table 5.5.(b): Risk factors for transplant graft loss 7-6 Factors of transplant 7- (ref*) n 479 Hazard Ratio Age at transplant -39 (ref*) >= Gender Male (ref*) 57. Female 36.5 Primary diagnosis Unknown primary (ref*) 77. Diabetes mellitus GN/SLE Polycystic kidney Obstructive nephropathy Others 3.8 Type of transplant Commercial cadaver (ref*) 7. Commercial live donor 46.7 Living donor Cadaver HBsAg Negative (ref*) % CI (.39,.496) (.663, 6.3) (.5, 4.47) (.585,.78) (.98, 3.77) (.36,.879) (.86, 5.45) (.6, 5.) (.9, 3.56) (.49,.336) (.56,.8) (.4, 4.54) P value.337 <..7 Positive NA NA NA Anti-HCV Negative (ref*) 833. Positive NA NA NA
17 5.5.3 Patient survival according to type of transplant Outcomes of renal transplantation by type of transplant are shown in Table 5.5.3, Figures and Patient survival of cadaveric renal transplant was worse in comparison to live donor transplant. The patient survival of local living renal transplant was 98% and 96% at year- and year-5 respectively. In comparison, the patients who had commercial live donor renal transplant had slightly poorer survival beyond year-5 post transplant. Overall, patient survival of local cadaveric transplant is worst among all type of transplant, likely due to older age, longer dialysis vintage and more comorbidity. Table 5.5.3: Unadjusted patient survival by type of transplant, 7-6 Type of Commercial Commercial Transplant Cadaver Live Donor Live Donor Cadaver Interval (years) n % Survival SE n % Survival SE n % Survival SE n % Survival SE *n=number at risk SE=standard error Figure 5.5.3: Patient survival by type of transplant, 7-6. Transplant patient survival by Type of Transplant, 7-6 Live donor Figure 5.5.4: Graft survival by type of transplants, 7-6. Transplant graft survival by Type of Transplant, Commercial cadaver.8 Live donor Cumulative survival.6.4 Cadaver Commercial live donor Cumulative survival.6.4 Commercial cadaver Cadaver Commercial live donor Duration in years Duration in years 7
18 5.5.4 Graft survival according to type of transplant The graft survival rates reported were not censored for death. Local live donor graft survival at year-, year-3 and year-5 was 94%, 9% and 86% respectively. The graft survival of commercial live donor and commercial cadaveric transplant were similar to graft survival of local living renal transplant. Local cadaveric transplant had worst graft survival; 84% at year- and 7% at year-5 post transplant. Table 5.5.4: Graft survival by type of transplant, 7-6 Type of Commercial Commercial Transplant Cadaver Live Donor Live Donor Cadaver Interval (years) n % Survival SE n % Survival SE n % Survival SE n % Survival SE *n=number at risk SE=standard error 5.5.5: Outcome of living related renal transplantation Patient survival of local live donor renal transplant appeared to be better in those transplanted in -6 compared to those transplanted in 7-. However, graft survival (not censored for death) between these two cohorts was similar. Table 5.5.5(a): Patient survival by year of transplant (Living related transplant, 7-6) of Transplant Interval (years) n % Survival SE n % Survival SE *n=number at risk SE=standard error 8
19 Figure 5.5.5(a): Patient survival by year of transplant (Living related transplant, 7-6). Transplant patient survival by of Transplant, Figure 5.5.5(b): Graft survival by year of transplant (Living related transplant, 7-6). Transplant graft survival by of Transplant, Cumulative survival.6.4 Cumulative survival Duration in years Duration in years Table 5.5.5(b): Graft survival by year of transplant (Living related transplant, 7-6) of Transplant Interval (years) n % Survival SE n % Survival SE *n=number at risk SE=standard error Outcome of commercial cadaveric transplantation Patient survival and graft survival (not censored for death) of commercial cadaveric transplant appeared to be better in those transplanted in 7- compared to -6. However the small number of commercial renal transplants in the latter cohort may have skewed the result. Table 5.5.6(a): Patient survival by year of transplant (Commercial cadaver transplant, 7-6) of Transplant Interval (years) n % Survival SE n % Survival SE *n=number at risk SE=standard error 9
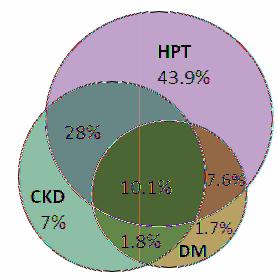
20 Figure 5.5.6(a): Patient survival by year of transplant (Commercial cadaver transplant, 7-6). Transplant patient survival by of Transplant, 7-6 Figure 5.5.6(b): Graft survival by year of transplant (Commercial cadaver transplant, 7-6). Transplant graft survival by of Transplant, 7-6 Cumulative survival Cumulative survival Duration in years Duration in years Table 5.5.6(b): Graft survival by year of transplant (commercial cadaver transplant, 7-6) of Transplant Interval (years) n % Survival SE n % Survival SE *n=number at risk SE=standard error 5.6 CARDIOVASCULAR RISK IN RENAL TRANSPLANT RECIPIENTS 5.6. Risk factors for ischaemic heart disease (IHD) In 6, 89.5% of renal transplant recipients has hypertension,.% has diabetes and 46.9% had chronic kidney disease (CKD) stage III and above. Approximately % of renal transplant recipients had all three major risk factors for cardiovascular disease. Prevalence of hypertension appeared to be increasing in the recent 5 years but prevalence of CKD showed a decreasing trend. Table 5.6.: Risk factors for IHD in renal transplant recipients at year Diabetes 7 (.7) 34 (.) 7 (.6) 4 (.5) 6 (.7) Hypertension** 594 (37.) 635 (38.4) 653 (39.8) 658 (4.) 69 (43.9) CKD 67 (.4) 48 (8.9) 3 (7.5) 47 (9.) (7.) Diabetes + Hypertension** 98 (6.) 98 (5.9) 3 (6.9) 9 (7.3) 9 (7.6) Diabetes + CKD 4 (.6) 4 (.5) 36 (.) 46 (.8) 8 (.8) CKD + Hypertension** 464 (9.) 5 (3.4) 48 (9.4) 435 (6.5) 44 (8.) Diabetes + CKD + Hypertension** (3.) 96 (.9) 7 (.6) (.8) 59 (.) **Hypertension: BP systolic > 4 and BP diastolic > 9 OR have either Beta blocker / Calcium channel blocker / ACE inhibitor / AIIRB / Other antihypertensive drugs GFR (ml/min/.73m) =.*(4-age(year ))*weight(kg) / creatinine (µmol/l) if male GFR (ml/min/.73m) =.85*(.*(4-age(year)) *weight(kg) / creatinine (µmol/l) if female CKD stage III-GFR, 3-6, CKD stage IV-GFR, 5-3, CKD stage V-GFR, <5
: Venn diagram for pre and post transplant complications (in %) at year 4 Figure 5.6.(d): Venn diagram for pre and post transplant complications (in %) at year 5 Figure 5.")
21 Figure 5.6.(a): Venn diagram for pre and post transplant complications (in %) at year Figure 5.6.(b): Venn diagram for pre and post transplant complications (in %) at year 3 Figure 5.6.(c): Venn diagram for pre and post transplant complications (in %) at year 4 Figure 5.6.(d): Venn diagram for pre and post transplant complications (in %) at year 5 Figure 5.6.(e): Venn diagram for pre and post transplant complications (in %) at year 6
22 5.6. Blood Pressure -6 Overall, blood pressure of renal transplant recipients was similar over the recent 5 years. In 6, a quarter of renal transplant recipients had systolic blood pressure of 4mmHg and % had diastolic blood pressure of 9mmHg. Table 5.6.(a): Systolic BP, < >= Percent Figure 5.6.(a): Systolic BP, -6 Systolic BP < Systolic BP -9 Systolic BP 3-39 Systolic BP 4-59 Systolic BP 6-79 Systolic BP >= Table 5.6.(b): Diastolic BP, < >= 4 Figure 5.6.(b): Diastolic BP, -6 Percent Diastolic BP <8 Diastolic BP 8-85 Diastolic BP Diastolic BP 9-99 Diastolic BP -9 Diastolic BP >= Blood pressure control The proportion of renal transplant recipients receiving treatment for hypertension was similar over the recent 5 years. Almost three-quarter of renal transplant recipients received treatment for hypertension in 6, including 3% who required two or more antihypertensive agents. However, 5% of patients had systolic blood pressure of 6mmHg and % had diastolic blood pressure of 9mmHg despite being on treatment. Table 5.6.3(a): Treatment for hypertension, -6 n % on antihypertensives drug antihypertensives antihypertensives % on antihypertensive % on % on
23 Table 5.6.3(b): Distribution of systolic BP without antihypertensives, -6 n Mean SD Median LQ UQ % Patients 6mmHg Table 5.6.3(c): Distribution of diastolic BP without antihypertensives, -6 n Mean SD Median LQ UQ % Patients 9mmHg Table 5.6.3(d): Distribution of systolic BP on antihypertensives, -6 n Mean SD Median LQ UQ % Patients 6mmHg Table 5.6.3(e): Distribution of diastolic BP on antihypertensives, -6 n Mean SD Median LQ UQ % Patients 9 mmhg Level of allograft function Prevalence of CKD in renal transplant recipients according to CKD stage over the last 5 years was similar. In 6, 4% had CKD stage III and % had CKD stage IV and above. Table 5.6.4: CKD stages, Stage Stage Stage Stage Stage Percent Figure 5.6.4: CKD stages by year CKD Stage CKD Stage CKD Stage 3 CKD Stage 4 CKD Stage
24 5.6.5 Body mass index (BMI) BMI of renal transplant recipients in the recent 5 years remains static. In 6, 8% were overweight and 5% were obese. Table 5.6.5: BMI, < > Percent Figure 5.6.5: BMI, -6 BMI < BMI -5 BMI 5-3 BMI > LDL cholesterol Overall, there appeared to be improvement in lipid profile in renal transplant recipients in 6 when compared to. In 6, 58% of renal transplant recipients had LDL.6mmol/L, % had total cholesterol >6.mmol/L and 9% had HDL <mmol/l. Table 5.6.6(a): LDL, < >= Percent Figure 5.6.6(a): LDL, -6 LDL <.6 LDL LDL >= Table 5.6.6(b): Total cholesterol, < > Figure 5.6.6(b): Total cholesterol, -6 Percent Total Cholesterol <4. Total Cholesterol Total Cholesterol Total Cholesterol Total Cholesterol >
25 Table 5.6.6(c): HDL, < > Percent Figure 5.6.6(c): HDL, -6 HDL < HDL -.3 HDL > QOL INDEX SCORE IN RENAL TRANSPLANT RECIPIENTS 833 patients who were transplanted from 7-6 were analysed for QoL index score. The overall QoL was found to be excellent with the median QoL index score of (Table & Figure 5.7.). There was no difference in the median QoL index score between diabetics and non-diabetics who underwent renal transplantation during this period (Table & Figure 5.7.). There was also no difference seen between gender (Table & Figure 5.7.3) and age (Table & Figure 5.7.4). It is worthwhile to note that those above 6 years old also enjoyed the same QoL index score () as their younger counterparts (Table & Figure 5.7.4). This trend of high QoL index score remained the same for the last ten years. Table 5.7.: Cumulative distribution of QoL-Index score in relation to dialysis modality, transplant recipient patients 7-6 Dialysis modality QoL score Number of patients 833 Centile (LQ).5 (median).75 (UQ).9.95 Table 5.7.: Cumulative distribution of QoL-Index score in relation to diabetes mellitus, transplant recipient patients 7-6 Diabetes mellitus No Yes Number of patients Centile (LQ).5 (median).75 (UQ).9.95 Figure 5.7.: Cumulative distribution of QoL-Index score in relation to dialysis modality, transplant recipient patients 7-6 Cumulative distribution of QOL by Modality, Transplant Patients Figure 5.7.: Cumulative distribution of QoL-Index score in relation to diabetes mellitus, transplant recipient patients 7-6 Cumulative distribution of QOL by DM, Transplant Patients Cumulative Distribution Cumulative Distribution QL-Index Score QL-Index Score 5 No Yes
26 Table 5.7.3: Cumulative distribution of QoL-Index score in relation to gender, transplant recipient patients 7-6 Gender Male Female Number of patients Centile (LQ).5 (median).75 (UQ).9.95 Cumulative Distribution Figure 5.7.3: Cumulative distribution of QoL-Index score in relation to gender, transplant recipient patients 7-6 Cumulative distribution of QOL by Gender, Transplant Patients QL-Index Score Male Female Table 5.7.4: Cumulative distribution of QoL-Index score in relation to age, transplant recipient patients 7-6 Age group (years) < >=6 Number of patients Centile (LQ) (median) -.75 (UQ) Figure 5.7.4: Cumulative distribution of QoL-Index score in relation to age, transplant recipient patients 7-6 Cumulative distribution of QoL-Index by Age Group, Transplant patients Figure 5.7.5: Cumulative distribution of QoL-Index score in relation to year of entry, transplant recipient patients 7-6 Cumulative distribution of QOL by of Entry, Transplant Patients Cumulative Distribution Cumulative Distribution QL-Index Score Age < Age -39 Age 4-59 Age >= QL-Index Score
27 Table 5.7.5: Cumulative distribution of QoL-Index score in relation to year of entry, transplant recipient patients 7-6 of Entry Number of patients Centile (LQ).5 (median).75 (UQ)
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Rosnawati Yahya. Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng.
 CHAPTER 5 Editor: Roswati Yahya Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng Contents 5. Stock and Flow of Rel Transplantation Stock and Flow Transplant Rates 5.2 Recipients
CHAPTER 5 Editor: Roswati Yahya Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng Contents 5. Stock and Flow of Rel Transplantation Stock and Flow Transplant Rates 5.2 Recipients
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Goh Bak Leong
 CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr (Mr) Rohan Malek Dr Wong Hin Seng Dr Fan Kin Sing Dr Rosnawati Yahya Dr S Prasad Menon Dr Tan Si
CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr (Mr) Rohan Malek Dr Wong Hin Seng Dr Fan Kin Sing Dr Rosnawati Yahya Dr S Prasad Menon Dr Tan Si
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Goh Bak Leong
 CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr Zaki Morad Mohd Zaher Dato Dr (Mr) Rohan Malek Dr Fan Kin Sing Dr Lily Mushahar Dr Lim Soo Kun Dr
CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr Zaki Morad Mohd Zaher Dato Dr (Mr) Rohan Malek Dr Fan Kin Sing Dr Lily Mushahar Dr Lim Soo Kun Dr
CHAPTER 13. Renal Transplanta on
 CHAPTER 13 Renal Transplanta on Rosnawa Yahya Hooi Lai Seong Ng Kok Peng Surya Bin Yakaob Wong Hin Seng SECTION 13.1: STOCK AND FLOW The number of new transplant pa ents decreased from 151 in 26 to its
CHAPTER 13 Renal Transplanta on Rosnawa Yahya Hooi Lai Seong Ng Kok Peng Surya Bin Yakaob Wong Hin Seng SECTION 13.1: STOCK AND FLOW The number of new transplant pa ents decreased from 151 in 26 to its
CHAPTER 14. Renal Transplantation
 15th Report of the Malaysian RENAL TRANSPLANTATION CHAPTER 14 Renal Transplantation Editor: Dr. Goh Bak Leong Expert Panel: : Dato Dr. Dato Zaki Dr. Morad Zaik Morad Mohd (Chair) Zaher (Chair) Dr. Goh
15th Report of the Malaysian RENAL TRANSPLANTATION CHAPTER 14 Renal Transplantation Editor: Dr. Goh Bak Leong Expert Panel: : Dato Dr. Dato Zaki Dr. Morad Zaik Morad Mohd (Chair) Zaher (Chair) Dr. Goh
CHAPTER 5 RENAL TRANSPLANTATION
 CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr. Goh Bak Leong Expert Panel: Dato Dr. Zaki Morad b Mohd Zaher (Chair) Dr. Goh Bak Leong (Co-Chair) Dr. Fan Kin Sing Dr. Lily Mushahar Mr. Rohan Malek Dr. S. Prasad
CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr. Goh Bak Leong Expert Panel: Dato Dr. Zaki Morad b Mohd Zaher (Chair) Dr. Goh Bak Leong (Co-Chair) Dr. Fan Kin Sing Dr. Lily Mushahar Mr. Rohan Malek Dr. S. Prasad
Chapter 12 PERITONEAL DIALYSIS
 Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
Chapter 12 PERITONEAL DIALYSIS B. Sunita A/P V. Bavanandan Anita Bhajan Manocha Lily Binti Mushahar Mohamad Zaimi Bin Abdul Wahab Sudhaharan Sivathasan PERITONEAL DIALYSIS 22nd Report of the SECTION 12.1:
CHAPTER 5. Paediatric Renal Replacement Therapy
 24th Report of the CHAPTER 5 Paediatric Renal Replacement Therapy Lee Ming Lee Lim Yam Ngo Lynster Liaw Chiew Tung Susan Pee Yap Yok Chin Wan Jazilah Wan Ismail 24th Report of the SECTION A: RRT PROVISION
24th Report of the CHAPTER 5 Paediatric Renal Replacement Therapy Lee Ming Lee Lim Yam Ngo Lynster Liaw Chiew Tung Susan Pee Yap Yok Chin Wan Jazilah Wan Ismail 24th Report of the SECTION A: RRT PROVISION
Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY. Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
 Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin SECTION A: RRT PROVISION FOR PAEDIATRIC PATIENTS This chapter presents
Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin SECTION A: RRT PROVISION FOR PAEDIATRIC PATIENTS This chapter presents
Chapter 6: Transplantation
 Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
Chapter 6: Transplantation Introduction During calendar year 2012, 17,305 kidney transplants, including kidney-alone and kidney plus at least one additional organ, were performed in the United States.
CHAPTER 3 HEART AND LUNG TRANSPLANTATION. Editors: Mr. Mohamed Ezani Hj Md. Taib Dato Dr. David Chew Soon Ping
 CHAPTER 3 Editors: Mr. Mohamed Ezani Hj Md. Taib Dato Dr. David Chew Soon Ping Expert Panel: Tan Sri Dato Dr. Yahya Awang (Chair) Mr. Mohamed Ezani Hj Md. Taib (Co-chair) Datin Dr. Aziah Ahmad Mahayiddin
CHAPTER 3 Editors: Mr. Mohamed Ezani Hj Md. Taib Dato Dr. David Chew Soon Ping Expert Panel: Tan Sri Dato Dr. Yahya Awang (Chair) Mr. Mohamed Ezani Hj Md. Taib (Co-chair) Datin Dr. Aziah Ahmad Mahayiddin
CHAPTER 12. Peritoneal Dialysis
 23rd Report of the PERITONEAL DIALYSIS CHAPTER 12 Peritoneal Dialysis Sunita Bavanandan Anita Bhajan Manocha Lily Mushahar Mohamad Zaimi Bin Abdul Wahab PERITONEAL DIALYSIS 23rd Report of the SECTION 12.1:
23rd Report of the PERITONEAL DIALYSIS CHAPTER 12 Peritoneal Dialysis Sunita Bavanandan Anita Bhajan Manocha Lily Mushahar Mohamad Zaimi Bin Abdul Wahab PERITONEAL DIALYSIS 23rd Report of the SECTION 12.1:
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures
 Supplementary Data Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures Quintiles of Systolic Blood Pressure Quintiles of Diastolic Blood Pressure Q1 Q2
Supplementary Data Supplementary Table 1. Baseline Characteristics by Quintiles of Systolic and Diastolic Blood Pressures Quintiles of Systolic Blood Pressure Quintiles of Diastolic Blood Pressure Q1 Q2
Chapter 12. End Stage Kidney Disease in Indigenous Peoples of Australia and Aotearoa/New Zealand. ANZDATA Registry 39th Annual Report
 Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
CHAPTER 6 PERITONEAL DIALYSIS
 CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Hannah Dent Kylie Hurst Stephen McDonald PERITONEAL DIALYSIS ANZDATA Registry 11 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to
CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Hannah Dent Kylie Hurst Stephen McDonald PERITONEAL DIALYSIS ANZDATA Registry 11 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to
CHAPTER 6 PERITONEAL DIALYSIS. Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst Annual Report 35th Edition
 CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst 212 Annual Report 35th Edition PERITONEAL DIALYSIS ANZDATA Registry 212 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis
CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst 212 Annual Report 35th Edition PERITONEAL DIALYSIS ANZDATA Registry 212 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
End Stage Kidney Disease Among Indigenous Peoples of Australia and New Zealand
 Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Chapter 1. Incidence of End Stage Kidney Disease. Contents:
 Chapter 1 Incidence of End Stage Kidney Disease Contents: Incidence of End Stage Kidney Disease 1-1 Stock and Flow 1-2 Incident patients 1-3 Incident Rates 1-3 Late Referral 1-7 Co-Morbidities 1-9 Primary
Chapter 1 Incidence of End Stage Kidney Disease Contents: Incidence of End Stage Kidney Disease 1-1 Stock and Flow 1-2 Incident patients 1-3 Incident Rates 1-3 Late Referral 1-7 Co-Morbidities 1-9 Primary
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
ANNUAL REPORT The Norwegian Renal Registry. (Norsk Nefrologiregister)
") ANNUAL REPORT 21 The Norwegian Renal Registry (Norsk Nefrologiregister) This report will also be available on: http://152.94.12.23/nyreforening/uremiregisteret/esdr.html Correspondence to: Overlege dr.med
ANNUAL REPORT 21 The Norwegian Renal Registry (Norsk Nefrologiregister) This report will also be available on: http://152.94.12.23/nyreforening/uremiregisteret/esdr.html Correspondence to: Overlege dr.med
Chapter 7. Australian Waiting List. ANZDATA Registry 39th Annual Report. Data to 31-Dec-2015
 Chapter 7 Australian Waiting List 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Stock and Flow The waiting list data reported here are derived from the Australian National Organ Matching System
Chapter 7 Australian Waiting List 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Stock and Flow The waiting list data reported here are derived from the Australian National Organ Matching System
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
. Time to transplant listing is dependent on. . In 2003, 9.1% of all prevalent transplant. . Patients with diabetes mellitus are less
 Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009
 Western University Scholarship@Western Electronic Thesis and Dissertation Repository June 2015 Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009 Ngan Lam The University
Western University Scholarship@Western Electronic Thesis and Dissertation Repository June 2015 Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009 Ngan Lam The University
TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA
 & TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
& TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
HAEMODIALYSIS GOVERNMENT CENTRES
 HAEMODIALYSIS IN GOVERNMENT CENTRES Stock and Flow Place of Haemodialysis and its Finance Death on Haemodialysis and Transfer to PD Government Haemodialysis Centres Haemodialysis Patient Characteristics
HAEMODIALYSIS IN GOVERNMENT CENTRES Stock and Flow Place of Haemodialysis and its Finance Death on Haemodialysis and Transfer to PD Government Haemodialysis Centres Haemodialysis Patient Characteristics
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use
 Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
Table 1 Baseline characteristics of 60 hemodialysis patients with atrial fibrillation and warfarin use Baseline characteristics Users (n = 28) Non-users (n = 32) P value Age (years) 67.8 (9.4) 68.4 (8.5)
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
REACH Risk Evaluation to Achieve Cardiovascular Health
 Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
Dyslipidemia and transplantation History: An 8-year-old boy presented with generalized edema and hypertension. A renal biopsy confirmed a diagnosis of focal segmental glomerulosclerosis (FSGS). After his
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS
 CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
Chapter 10. Cancer. ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong.
 Chapter Cancer ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong Contents: Cancer -1 Incidence of Cancer on Renal Replacement Therapy -2 Kidney Cancer
Chapter Cancer ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong Contents: Cancer -1 Incidence of Cancer on Renal Replacement Therapy -2 Kidney Cancer
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
CHAPTER 2. Prevalence of Renal Replacement Therapy for End Stage Kidney Disease
 CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per
CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per
Chapter 10. Cancer. ANZDATA Registry 39th Annual Report. Data to 31-Dec-2015
 Chapter Cancer 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Incidence of Cancer on Renal Replacement Therapy Figures.1-.6 and table.1 show the cumulative incidence of non-skin cancer in patients
Chapter Cancer 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Incidence of Cancer on Renal Replacement Therapy Figures.1-.6 and table.1 show the cumulative incidence of non-skin cancer in patients
Chapter 7: ESRD among Children, Adolescents, and Young Adults
 Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Kidney Allograft Stone after Kidney Transplantation and its Association with Graft Survival
 Original Article Kidney Allograft Stone after Kidney Transplantation and its Association with Graft Survival M. S. Rezaee-Zavareh 1,2, R. Ajudani 1, M. Ramezani Binabaj 1, F. Heydari 2, B. Einollahi 2
Original Article Kidney Allograft Stone after Kidney Transplantation and its Association with Graft Survival M. S. Rezaee-Zavareh 1,2, R. Ajudani 1, M. Ramezani Binabaj 1, F. Heydari 2, B. Einollahi 2
OUT OF DATE. Choice of calcineurin inhibitors in adult renal transplantation: Effects on transplant outcomes
 nep_734.fm Page 88 Friday, January 26, 2007 6:47 PM Blackwell Publishing AsiaMelbourne, AustraliaNEPNephrology1320-5358 2006 The Author; Journal compilation 2006 Asian Pacific Society of Nephrology? 200712S18897MiscellaneousCalcineurin
nep_734.fm Page 88 Friday, January 26, 2007 6:47 PM Blackwell Publishing AsiaMelbourne, AustraliaNEPNephrology1320-5358 2006 The Author; Journal compilation 2006 Asian Pacific Society of Nephrology? 200712S18897MiscellaneousCalcineurin
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
Chapter - 2 DIALYSIS IN MALAYSIA
 2 th Report of the Malaysian Dialysis and Transplant Registry 212 Dialysis IN Malaysia Chapter - 2 DIALYSIS IN MALAYSIA Goh Bak Leong Lim Yam Ngo Ong Loke Meng Ghazali Ahmad Lee Day Guat Dialysis IN Malaysia
2 th Report of the Malaysian Dialysis and Transplant Registry 212 Dialysis IN Malaysia Chapter - 2 DIALYSIS IN MALAYSIA Goh Bak Leong Lim Yam Ngo Ong Loke Meng Ghazali Ahmad Lee Day Guat Dialysis IN Malaysia
CHAPTER 4. Paediatric Renal Biopsies
 2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
2nd Report of the Malaysian Registry of Renal Biopsy 2008 PAEDIATRIC RENAL BIOPSIES CHAPTER 4 Paediatric Renal Biopsies Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Diltiazem use in tacrolimus-treated renal transplant recipients Kothari J, Nash M, Zaltzman J, Prasad G V R
 Diltiazem use in tacrolimus-treated renal transplant recipients Kothari J, Nash M, Zaltzman J, Prasad G V R Record Status This is a critical abstract of an economic evaluation that meets the criteria for
Diltiazem use in tacrolimus-treated renal transplant recipients Kothari J, Nash M, Zaltzman J, Prasad G V R Record Status This is a critical abstract of an economic evaluation that meets the criteria for
Clinical Outcomes of Renal Transplantation in Hepatitis C Virus Positive Recipients
 Original Research Article Clinical Outcomes of Renal Transplantation in Hepatitis C Virus Positive Recipients Surendran Sujit 1*, N. Gopalakrishnan 2 1 Assistant Professor, 2 Professor and Head Department
Original Research Article Clinical Outcomes of Renal Transplantation in Hepatitis C Virus Positive Recipients Surendran Sujit 1*, N. Gopalakrishnan 2 1 Assistant Professor, 2 Professor and Head Department
chapter seven transplantation page
 chapter seven There been times that I thought I couldn t last for long But now I think I m able to carry on It s been a long, a long time coming But I know a change gonna come, oh yes it will Sam Cooke,
chapter seven There been times that I thought I couldn t last for long But now I think I m able to carry on It s been a long, a long time coming But I know a change gonna come, oh yes it will Sam Cooke,
CHAPTER 2. Dialysis in Malaysia
 15th Report of the Malaysian Dialysis and Transplant Registry 27 DIALYSIS IN MALAYSIA CHAPTER 2 Dialysis in Malaysia Lim Yam Ngo Lim Teck Onn Lee Day Guat 4 DIALYSIS IN MALAYSIA 15th Report of the Malaysian
15th Report of the Malaysian Dialysis and Transplant Registry 27 DIALYSIS IN MALAYSIA CHAPTER 2 Dialysis in Malaysia Lim Yam Ngo Lim Teck Onn Lee Day Guat 4 DIALYSIS IN MALAYSIA 15th Report of the Malaysian
Hasan Fattah 3/19/2013
 Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 2007
 CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 27 Stephen McDonald Leonie Excell Hannah Dent NEW PATIENTS ANZDATA Registry 28 Report Figure 2.1 Annual Intake of New Patients 23-27 (Number Per Million Population)
CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 27 Stephen McDonald Leonie Excell Hannah Dent NEW PATIENTS ANZDATA Registry 28 Report Figure 2.1 Annual Intake of New Patients 23-27 (Number Per Million Population)
Renal Transplant Registry Report 2008
 Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Banks E, Crouch SR, Korda RJ, et al. Absolute risk of cardiovascular
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
KIDNEY DIALYSIS FOUNDATION ANNUAL REPORT PERITONEAL DIALYSIS PROGRAMME
 KIDNEY DIALYSIS FOUNDATION ANNUAL REPORT PERITONEAL DIALYSIS PROGRAMME 2011 Prepared by Dr Grace Medical Director With input from: Lay Kwee Chin Senior Nurse Clinician, Patient Services Theresa Soh Clinical
KIDNEY DIALYSIS FOUNDATION ANNUAL REPORT PERITONEAL DIALYSIS PROGRAMME 2011 Prepared by Dr Grace Medical Director With input from: Lay Kwee Chin Senior Nurse Clinician, Patient Services Theresa Soh Clinical
Cardiovascular Risk Reduction in Kidney Transplant Recipients
 Cardiovascular Risk Reduction in Kidney Transplant Recipients Rainer Oberbauer R.O. AUG 2010 CV Mortality in ESRD compared to the general population R.O.2/32 Modified from Foley et al. AJKD 32 (suppl3):
Cardiovascular Risk Reduction in Kidney Transplant Recipients Rainer Oberbauer R.O. AUG 2010 CV Mortality in ESRD compared to the general population R.O.2/32 Modified from Foley et al. AJKD 32 (suppl3):
CHAPTER 3. Secondary Glomerulonephritis
 CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 59 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to the MRRB from the year 2005-2010.
CHAPTER 3 Secondary Glomerulonephritis Rosnawati Yahya Liew Yew Foong 59 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to the MRRB from the year 2005-2010.
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, Jeffrey P. Harris MD, FACP
 8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
8 th Annual Congress of the Bangladesh Society of Medicine Dhaka, Bangladesh March 23-24, 2008 The Internist and the Pre-End Stage Renal Disease Patient Jeffrey P. Harris MD, FACP Country: Bangladesh Population:
CHAPTER 5. Haemodialysis. Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald
 CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Renal replacement therapy for patients with diabetes mellitus in Hong Kong
 Hong Kong J Journal Nephrol of 2001;3(2):89-96. Nephrology 2001;3(1):89-96. Y CHOY, et al R E N L REGISTRY Renal replacement therapy for patients with diabetes mellitus in Hong Kong o-ying CHOY 1, Yiu-Wing
Hong Kong J Journal Nephrol of 2001;3(2):89-96. Nephrology 2001;3(1):89-96. Y CHOY, et al R E N L REGISTRY Renal replacement therapy for patients with diabetes mellitus in Hong Kong o-ying CHOY 1, Yiu-Wing
QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room
 QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room msix PEDIATrIC ESrD 18 ž 21 ATLAS OF ESRD IN THE UNITED STATES Incident rates of ESRD in children have risen two
QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room msix PEDIATrIC ESrD 18 ž 21 ATLAS OF ESRD IN THE UNITED STATES Incident rates of ESRD in children have risen two
Nephrology. 3 rd Year Revision Session 06/05/17 Cathal Hannan
 Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
Nephrology 3 rd Year Revision Session 06/05/17 Cathal Hannan Aims Acute Kidney Injury-recognition and management Sample OSCE Station Clinically relevant renal physiology Aetiology of Chronic Kidney Disease
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Mandana Nikpour 1,2, Murray B Urowitz 1*, Dominique Ibanez 1, Paula J Harvey 3 and Dafna D Gladman 1. Abstract
 RESEARCH ARTICLE Open Access Importance of cumulative exposure to elevated cholesterol and blood pressure in development of atherosclerotic coronary artery disease in systemic lupus erythematosus: a prospective
RESEARCH ARTICLE Open Access Importance of cumulative exposure to elevated cholesterol and blood pressure in development of atherosclerotic coronary artery disease in systemic lupus erythematosus: a prospective
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Progress in Pediatric Kidney Transplantation
 Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Allocation of deceased donor kidneys. Phil Clayton NSW Renal Group 14 June 2012
 Allocation of deceased donor kidneys Phil Clayton NSW Renal Group 14 June 2012 Outline Why study kidney allocation? Equity vs utility Current Australian model Previous work in Australia US allocation research
Allocation of deceased donor kidneys Phil Clayton NSW Renal Group 14 June 2012 Outline Why study kidney allocation? Equity vs utility Current Australian model Previous work in Australia US allocation research
Objectives. Kidney Complications With Diabetes. Case 10/21/2015
 Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Objectives Kidney Complications With Diabetes Brian Boerner, MD Diabetes, Endocrinology, and Metabolism University of Nebraska Medical Center Review screening for, and management of, albuminuria Review
Effects of Lowering LDL Cholesterol on Progression of Kidney Disease
 Effects of Lowering LDL Cholesterol on Progression of Kidney Disease Richard Haynes, David Lewis, Jonathan Emberson, Christina Reith, Lawrence Agodoa, Alan Cass, Jonathan C. Craig, Dick de Zeeuw, Bo Feldt-Rasmussen,
Effects of Lowering LDL Cholesterol on Progression of Kidney Disease Richard Haynes, David Lewis, Jonathan Emberson, Christina Reith, Lawrence Agodoa, Alan Cass, Jonathan C. Craig, Dick de Zeeuw, Bo Feldt-Rasmussen,
Targeted Adverse Event (ADV)
") North American Pediatric Renal Trials Collaborative Studies Production Release 14.0 [$sitecode] User: Adverse Event: Adverse Event Date: Targeted Adverse Event (ADV) Web Version: 1.0; 2.0; 06-20-13 1.
North American Pediatric Renal Trials Collaborative Studies Production Release 14.0 [$sitecode] User: Adverse Event: Adverse Event Date: Targeted Adverse Event (ADV) Web Version: 1.0; 2.0; 06-20-13 1.
ANEMIA & HEMODIALYSIS
 ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
ANEMIA & HEMODIALYSIS The anemia of CKD is, in most patients, normocytic and normochromic, and is due primarily to reduced production of erythropoietin by the kidney and to shortened red cell survival.
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Long-term prognosis of BK virus-associated nephropathy in kidney transplant recipients
 Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Original Article Kidney Res Clin Pract 37:167-173, 2018(2) pissn: 2211-9132 eissn: 2211-9140 https://doi.org/10.23876/j.krcp.2018.37.2.167 KIDNEY RESEARCH AND CLINICAL PRACTICE Long-term prognosis of BK
Chronic Kidney Disease: Optimal and Coordinated Management
 Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
morbidity & mortality
 morbidity & mortality esrd introduction of ESRD treatment. We examine these concerns throughout the ADR, particularly in Chapter One. This year we focus on infectious complications, especially those related
morbidity & mortality esrd introduction of ESRD treatment. We examine these concerns throughout the ADR, particularly in Chapter One. This year we focus on infectious complications, especially those related
Echocardiography analysis in renal transplant recipients
 Original Research Article Echocardiography analysis in renal transplant recipients S.A.K. Noor Mohamed 1*, Edwin Fernando 2, 1 Assistant Professor, 2 Professor Department of Nephrology, Govt. Stanley Medical
Original Research Article Echocardiography analysis in renal transplant recipients S.A.K. Noor Mohamed 1*, Edwin Fernando 2, 1 Assistant Professor, 2 Professor Department of Nephrology, Govt. Stanley Medical
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
kidney OPTN/SRTR 2012 Annual Data Report:
 kidney wait list 18 deceased donation 22 live donation 24 transplant 26 donor-recipient matching 28 outcomes 3 pediatric transplant 33 Medicare data 4 transplant center maps 43 A. J. Matas1,2, J. M. Smith1,3,
kidney wait list 18 deceased donation 22 live donation 24 transplant 26 donor-recipient matching 28 outcomes 3 pediatric transplant 33 Medicare data 4 transplant center maps 43 A. J. Matas1,2, J. M. Smith1,3,
Chapter 22: Hematological Complications
 Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
GUIDELINES ON RENAL TRANSPLANTATION
 46 GUIDELINES ON RENAL TRANSPLANTATION T. Kälbe (chairman), M. Lucan, G. Nicita, R. Sells, F.J. Burgos Revilla, M. Wiesel Introduction The number of patients registered as starting end-stage renal disease
46 GUIDELINES ON RENAL TRANSPLANTATION T. Kälbe (chairman), M. Lucan, G. Nicita, R. Sells, F.J. Burgos Revilla, M. Wiesel Introduction The number of patients registered as starting end-stage renal disease
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Supplementary Online Content
 Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
Supplementary Online Content Xu X, Qin X, Li Y, et al. Efficacy of folic acid therapy on the progression of chronic kidney disease: the Renal Substudy of the China Stroke Primary Prevention Trial. JAMA
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Stephen McDonald. Matthew Jose. Kylie Hurst INDIGENOUS 12-1
 ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Reduced graft function (with or without dialysis) vs immediate graft function a comparison of long-term renal allograft survival
 vs immediate graft function a comparison of long-term renal allograft survival") Nephrol Dial Transplant (2006) 21: 2270 2274 doi:10.1093/ndt/gfl103 Advance Access publication 22 May 2006 Original Article Reduced graft function (with or without dialysis) vs immediate graft function
Nephrol Dial Transplant (2006) 21: 2270 2274 doi:10.1093/ndt/gfl103 Advance Access publication 22 May 2006 Original Article Reduced graft function (with or without dialysis) vs immediate graft function
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Status of the CKD and ESRD treatment: Growth, Care, Disparities
 Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
Status of the CKD and ESRD treatment: Growth, Care, Disparities United States Renal Data System Coordinating Center An J. Collins, MD FACP Director USRDS Coordinating Center Robert Foley, MB Co-investigator
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
2017 USRDS ANNUAL DATA REPORT KIDNEY DISEASE IN THE UNITED STATES S611
 Healthy People 2020 In this chapter, we examine data for 11 Healthy People 2020 (HP2020) objectives 10 for CKD and one for diabetes spanning 20 total indicators for which the USRDS serves as the official
Healthy People 2020 In this chapter, we examine data for 11 Healthy People 2020 (HP2020) objectives 10 for CKD and one for diabetes spanning 20 total indicators for which the USRDS serves as the official
Chapter 8: ESRD Among Children, Adolescents, and Young Adults
 Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Donation from Old Living Donors How safe is it? Safe for recipient or donor?
 Donation from Old Living Donors How safe is it? Safe for recipient or donor? Pr Lionel Rostaing Service de Néphrologie, Hémodialyse, Aphérèses et Transplantation CHU Grenoble Alpes France lrostaing@chu-grenoble.fr
Donation from Old Living Donors How safe is it? Safe for recipient or donor? Pr Lionel Rostaing Service de Néphrologie, Hémodialyse, Aphérèses et Transplantation CHU Grenoble Alpes France lrostaing@chu-grenoble.fr
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Chapter Two Renal function measures in the adolescent NHANES population
 0 Chapter Two Renal function measures in the adolescent NHANES population In youth acquire that which may restore the damage of old age; and if you are mindful that old age has wisdom for its food, you
0 Chapter Two Renal function measures in the adolescent NHANES population In youth acquire that which may restore the damage of old age; and if you are mindful that old age has wisdom for its food, you