Vascular complications
|
|
|
- Asher Day
- 5 years ago
- Views:
Transcription

1 Vascular complications December 8, 2018
2 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships with financial sponsors: Grant / Research Support: Jannsen, Merck, Novartis, AstraZeneca, Servier, Novo Nordisk, Lilly Other Financial/Material Support: Hold a patent with BI for Linagliptin for heart failure Potential for conflict(s) of interest: Jannsen, Merck, Novartis, AstraZeneca, Servier, Novo Nordisk, Lilly and BI develops and benefits from the sale of products that might be discussed in this program.
3 Mitigating Potential Bias All the recommendations involving clinical medicine are based on evidence that is accepted within the profession. All scientific research referred to, reported, or used is in the support or justification of patient care. Recommendations conform to the generally accepted standards. Independent content validation. The presentation will mitigate potential bias by ensuring that data and recommendations are presented in a fair and balanced way. Potential bias will be mitigated by presenting a full range of products that can be used in this therapeutic area. Information of the history, development, funding, and the sponsoring organizations of the disclosure presented will be discussed.



4 Vascular protection in diabetes Dr Kim A Connelly MBBS PhD FRACP St Michaels Hospital Sunnybrook Health Sciences centre President Canadian Society of CMR Section Head: Macrovascular complications Diabetes Canada CPG Associate Professor of Medicine University of Toronto
5 Learning Objectives Upon completion of this session, participants will be equipped to: 1. Describe the vascular complications of Type II diabetes 2. Assess the impact of therapies to reduce diabetes vascular complications 3. To develop management plans to address diabetes vascular complications with the use of pharmacological therapy and healthy lifestyle interventions
6 In Canada, People with Diabetes Account For 1/3 2/5 2/3 1/2 of all heart attacks & strokes of all heart failure admissions of all nontraumatic amputations all patients starting dialysis Booth et al. ; Hux et al; and Oliver et al., Diabetes in Ontario: An ICES Practice Atlas
7 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes Recommendation 1. All individuals with diabetes should follow a comprehensive, multifaceted approach to reduce CV risk, including: A1C 7.0% implemented early in the course of diabetes [Grade C, Level 3] Systolic BP of <130 mmhg [Grade C, Level 3] and diastolic BP of <80 mmhg [Grade B, Level 1] (see Hypertension chapter) Additional vascular protective medications in the majority of adult people with diabetes (see recommendations below) [Grade A, Level 1 for those with type 2 diabetes age >40 years with albuminuria; Grade D, Consensus for those with type 1 diabetes] Achievement and maintenance of healthy weight goals [Grade D, Consensus] Healthy eating (see Nutrition Therapy Chapter for specific dietary recommendations) Regular physical activity [Grade D, Consensus] Smoking cessation [Grade C, Level 3]
8 2018 Diabetes Canada CPG The Essentials 2018 ABCDES 3 of Diabetes Care A A1C optimal glycemic control (usually 7%) B BP optimal blood pressure control (<130/80) C Cholesterol LDL <2.0 mmol/l or >50% reduction D Drugs to protect the heart A ACEi or ARB S Statin A ASA if indicated SGLT2i/GLP-1 RA with demonstrated CV benefit if type 2 DM with CVD and A1C not at target E Exercise / Healthy Eating S Screening for complications S Smoking cessation S Self-management, stress and other barriers
9 HEALTHY BEHAVIOUR INTERVENTIONS Start healthy behaviour interventions (nutritional therapy, weight management, physical activity) +/- metformin A1C <1.5% above target If not at glycemic target within 3 months, start/increase metformin If not at glycemic target AT DIAGNOSIS OF TYPE 2 DIABETES A1C 1.5% above target Start metformin immediately Consider a second concurrent antihyperglycemic agent Symptomatic hyperglycemia and/or metabolic decompensation Initiate insulin +/- metformin If not at glycemic target Clinical CVD? YES NO Start antihyperglycemic agent with demonstrated CV benefit empagliflozin (Grade A, Level 1A) liraglutide (Grade A, Level 1A) canagliflozin* (Grade C, Level 2) If not at glycemic target * Avoid in people with prior lower extremity amputation See next page 9


10 2018 Diabetes Canada CPG Chapter 8. Targets for Glycemic Control A1C Targets Adults with type 2 diabetes to reduce the risk of CKD and retinopathy if at low risk of hypoglycemia MOST ADULTS WITH TYPE 1 OR TYPE 2 DIABETES %: Functionally dependent* %: Recurrent severe hypoglycemia and/or hypoglycemia unawareness Limited life expectancy Frail elderly and/or with dementia** Avoid higher A1C to minimize risk of symptomatic hyperglycemia and acute and chronic complications End of life A1C measurement not recommended. Avoid symptomatic hyperglycemia and any hypoglycemia * Based on class of antihyperglycemic medication(s) utilized and person s characteristics ** see Diabetes in Older People chapter
11 Cardiovascular Considerations for Antihyperglycemic Agents CV considerations Class Agents Relative A1C lowering Risk of hypoglyc emia Heart failure BP effect CV superiority demonstrated as primary endpoint in RCT by 1 agent in class GLP-1 receptor agonist SGLT-2 inhibitor liraglutide, semaglutide lixisenatide, / Rare Neutral dulaglutide, exenatide empagliflozin, canagliflozin* dapagliflozin / Rare CV safety demonstrated as primary endpoint in RCT by 1 agents in class DPP-4 inhibitor Thiazolidinedione Insulin alogliptin, sitagliptin, saxagliptin, linagliptin pioglitazone, rosiglitazone glargine 100 u/ml, degludec, other basal/bolus/premixed Rare Neutral saxa Neutral Rare Neutral Yes** Neutral Neutral CV safety unknown or RCT results not yet available Agents in blue bold text showed CV superiority for MACE. Agents in black bold text showed CV safety *Increased lower extremity amputations. **Lower hypoglycemia risk with newer generation basal insulins (e.g., degludec, glargine 300 u/ml) Adapted from Mancini GB, et al. Can J Cardiol 2017; 33(3):366-77; Weight loss agent orlistat None α-glucosidase inhibitor acarbose Rare Meglitinide nateglinide, repaglinide Yes Sulfonylurea gliclazide, glimepiride, glyburide Yes
12 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes HBA1c Recommendation: In adults with type 2 diabetes with clinical CVD in whom glycemic targets are not achieved with existing antihyperglycemic medication, an antihyperglycemic agent with demonstrated CV outcome benefit should be added to reduce the risk of major CV events [Grade A, Level 1A for empagliflozin; Grade A, Level 1A for liraglutide, Grade C, Level 2 for canagliflozin]
13 B: Making the Diagnosis of Hypertension in Patients with Diabetes BP >130/80 mm Hg Confirmed on a second occasion in either the office, home or by appropriate ambulatory measurement.
14 Blood pressure Recommendation 1. Persons with diabetes mellitus should be treated to attain systolic BP of <130 mm Hg [Grade C, Level 3] and diastolic BP of <80 mm Hg [Grade B, Level 1] (these target BP levels are the same as BP treatment thresholds) 2. For persons with CVD or CKD, including albuminuria, or with CV risk factors in addition to diabetes and hypertension, an ACE inhibitor or an ARB is recommended as initial therapy [Grade A, Level 1A] 3. If target BP levels are not achieved with standard-dose monotherapy, additional antihypertensive therapy should be used. For persons in whom combination therapy with an ACE inhibitor is being considered, a dihydropyridine CCB is preferable to a thiazide/thiazide-like diuretic (Grade A).
 Tight control (mean BP 144/82 mmhg) 30 20 10 Tight BP control: 24% reduction of events (95%")
 diabetes.")
15 Patients with events (%) Hypertension in Diabetes (UKPDS) Less tight control (mean BP 154/87 mmhg) Tight control (mean BP 144/82 mmhg) Tight BP control: 24% reduction of events (95% CI 8-38) 0 UKPDS Study Group. BMJ 1998; 317: guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association Years from randomization
16 Summary of Pharmacotherapy for Hypertension in Patients with Diabetes Threshold equal or over 130/80 mmhg and Target below 130/80 mmhg Diabetes With Nephropathy, CVD or CV risk factors Without the above ACE Inhibitor or ARB 1. ACE Inhibitor or ARB or 2. Thiazide diuretic or DHP-CCB > 2-drug combinations Monitor serum potassium and creatinine carefully in patients with CKD prescribed an ACEI or ARB Combinations of an ACEI with an ARB are specifically not recommended in the absence of proteinuria More than 3 drugs may be needed to reach target values If Creatinine over 150 µmol/l or creatinine clearance below 30 ml/min ( 0.5 ml/sec), a loop diuretic should be substituted for a thiazide diuretic if control of volume is desired
17 Patients with Primary Events (%) ACE Inhibitor + CCB or Diuretic (ACCOMPLISH Study) Composite Morbidity / Mortality Endpoint Benazepril plus hydrocholorthiazide Months Benazepril plus amlodipine 21% reduction in MACE diabetes subgroup persons p=0.003 Adapted from Jamerson K, et al: N Engl J Med 2008; 359(23):
18 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes Recommendation 2. Statin therapy should be used to reduce CV risk in adults with type 1 or type 2 diabetes with any of the following features: Clinical CVD [Grade A, Level 1] Age 40 years [Grade A, Level 1 for type 2 diabetes; Grade D, Consensus for type 1 diabetes] Age <40 years and 1 of the following: Diabetes duration >15 years and age >30 years [Grade D, Consensus] Microvascular complications [Grade D, Consensus] Warrants therapy based on the presence of other risk factors according to the 2016 Canadian Cardiovascular Society Guidelines for the Diagnosis and Treatment of Dyslipidemia [Grade D, Consensus]
19 CARDS: Statins Reduced CVD in Patients with DM Colhoun HM, et al. Lancet 2004;364:685.
20 IMPROVE IT IMPROVE-IT: First large trial evaluating clinical efficacy of combination EZ/Simva vs. simvastatin (i.e., the addition of ezetimibe to statin therapy): Does lowering LDL-C with the non-statin agent ezetimibe reduce cardiac events? Is (Even) Lower (Even) Better? (estimated mean LDL-C ~50 vs. 65mg/dL) Safety of ezetimibe Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:205-12

21 CV Death, Non-fatal MI, or Non-fatal Stroke HR 0.90 CI (0.84, 0.97) p=0.003 NNT= 56 Simva 22.2% 1704 events EZ/Simva 20.4% 1544 events 7-year event rates
22 Major Pre-specified Subgroups Simva EZ/Simva Male Female Age < 65 years Age 65 years No diabetes Diabetes * Prior LLT No prior LLT LDL-C > 95 mg/dl LDL-C 95 mg/dl Ezetimibe/Simva Simva 1.3 Better Better 7-year event rates *p-interaction = 0.023, otherwise > 0.05

23
24
25 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes Recommendation ACE inhibitor or ARB, at doses that have demonstrated vascular protection, should be used to reduce CV risk in adults with type 1 or type 2 diabetes with any of the following: Clinical CVD [Grade A, Level 1] Age >55 years with an additional CV risk factor or end organ damage (albuminuria, retinopathy, left ventricular hypertrophy) [Grade A, Level 1] Microvascular complications [Grade D, Consensus]. Note: Among women with childbearing potential, ACE inhibitors, ARBs or statins should only be used if there is reliable contraception At doses that have shown vascular protection [perindopril 8 mg daily (EUROPA), ramipril 10 mg daily (HOPE), telmisartan 80 mg daily (ONTARGET)]
26 Kaplan-Meier rates Micro-HOPE (ACEi): CV Benefits 0.2 Primary Outcome (NNT 22) Placebo 0.16 All Mortality (NNT 31) Ramipril 10 mg RR = 0.75 ( ) p = RR = 0.76 ( ) p = MI (NNT 37) 0.08 Stroke (NNT 53) 0.12 CV Death (NNT 29) RR = 0.78 ( ) p = HOPE study investigators. Lancet. 2000;355: RR = 0.67 ( ) p = Duration of follow-up (days) RR = 0.63 ( ) p =

27 Unclear if RAS blockers superior to other agents in absence of HT or CV risk factors BMJ 2016;352:i438 doi: /bmj.i438
28 What About ASA for 1⁰ Prevention of CVD? Included: Six studies, n = 10,117 participants De Berardis G et al. BMJ 2009;339:b4531
29 ASA for 1⁰ Prevention in Diabetes Meta analysis of 6 studies (n = 10,117) No overall benefit for: Major CV events MI Stroke CV mortality All-cause mortality JPAD = Japanese Primary Prevention of Atherosclerosis with Aspirin for Diabetes POPADAD = Prevention of Progression of Arterial Disease and Diabetes PPP = Primary Prevention Project ETDRS = Early Treatment Diabetic Retinopathy Study PHS = Physicians Health Study WHS = Women s Health Study De Beradis G, et al. BMJ 2009; 339:b4531. Major CV events JPAD 68/1262 POPADAD 105/638 WHS 58/514 PPP 20/519 ETDRS 350/1856 Total 601/4789 Myocardial infarction JPAD 28/1262 POPADAD 90/638 WHS 36/514 PPP 5/519 ETDRS 241/1856 PHS 11/275 Total 395/5064 Stroke JPAD POPADAD WHS PPP ETDRS Total No. of events/no. in group ASA Control/placebo RR (95% CI) RR (95% CI) 12/ /638 15/514 9/519 92/ /4789 Death from CV causes JPAD 1/1262 POPADAD 43/638 PPP 10/519 ETDRS 244/1856 Total 298/4275 All-cause mortality JPAD 34/1262 POPADAD 94/638 PPP 25/519 ETDRS 340/1856 Total 493/ / /638 62/513 22/ / / / /638 24/513 10/ / / / / /638 31/513 10/512 78/ / / /638 8/ / / / /638 20/ / / Favors ASA 0.80 ( ) 0.97 ( ) 0.90 ( ) 0.90 ( ) 0.90 ( ) 0.90 ( ) 0.87 ( ) 1.10 ( ) 1.48 ( ) 0.49 ( ) 0.82 ( ) 0.40 ( ) 0.86 ( ) 0.89 ( ) 0.74 ( ) 0.46 ( ) 0.89 ( ) 1.17 ( ) 0.83 ( ) 0.10 ( ) 1.23 ( ) 1.23 ( ) 0.87 ( ) 0.94 ( ) 0.90 ( ) 0.93 ( ) 1.23 ( ) 0.91 ( ) 0.93 ( ) 2 8 Favors control/placebo
30 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes Recommendations 5. In people with established CVD, low-dose ASA therapy ( mg) should be used to prevent CV events [Grade B, Level 2] 6. ASA should not be used routinely for the primary prevention of CVD in people with diabetes [Grade A, Level 1A]. ASA may be used in the presence of additional CV risk factors [Grade D, Consensus]
31 PEGASUS TIMI 53: Background & Purpose Randomized, Double-Blind, placebo-controlled clinical trial Purpose: To test whether long-term therapy with ticagrelor added to low-dose aspirin reduces the risk of major CV events among stable patients with a history of MI. Bonaca MP., et al. NEJM. 2015;372(19):
32 CV Death, MI, or Stroke (%) Primary Endpoint: MACE ,162 patients with MI 1-3 years prior and treated with low-dose aspirin Placebo (9.0%) 8 7 Ticagrelor 90 (7.8%) Ticagrelor 60 (7.8%) Ticagrelor 90 mg HR 0.85 (95% CI ) P=0.008 Ticagrelor 60 mg HR 0.84 (95% CI ) P= Months from Randomization Bonaca MP et al. and Sabatine MS. NEJM 2015;372:
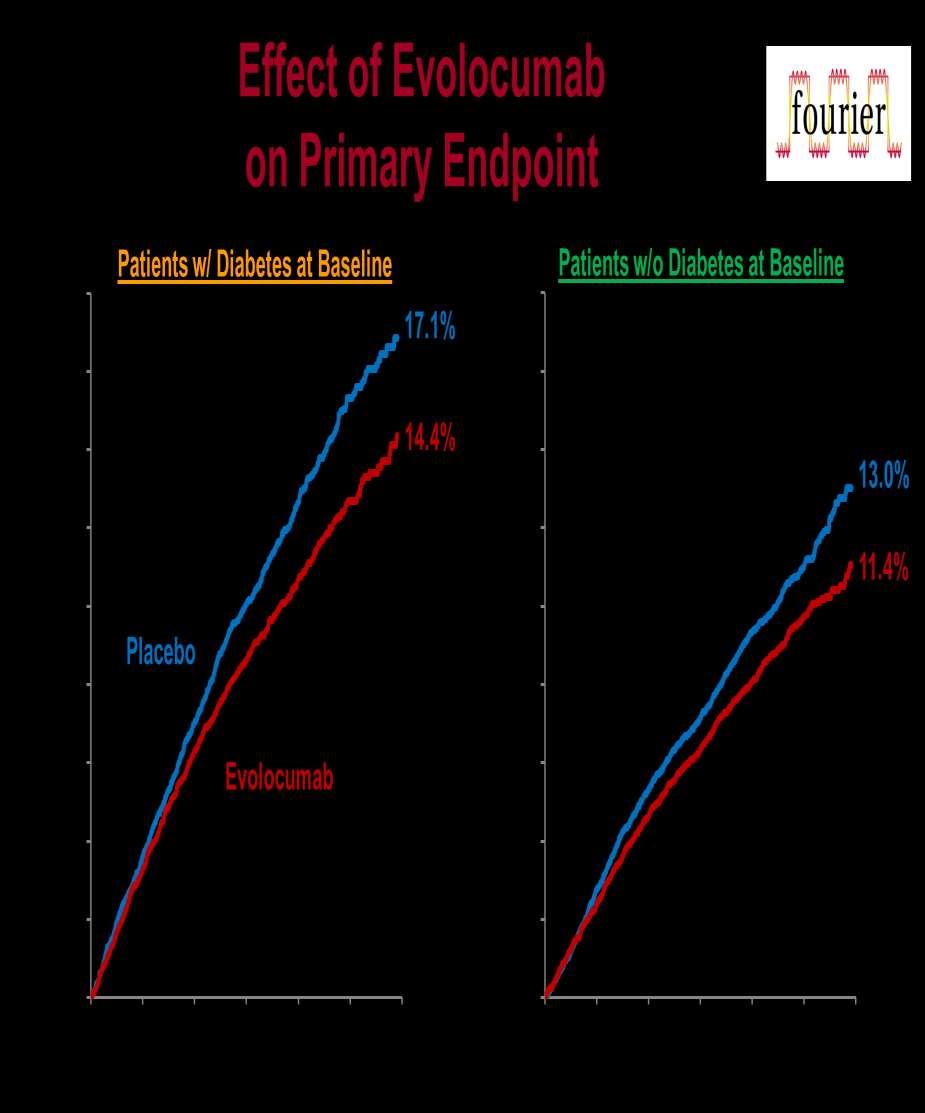
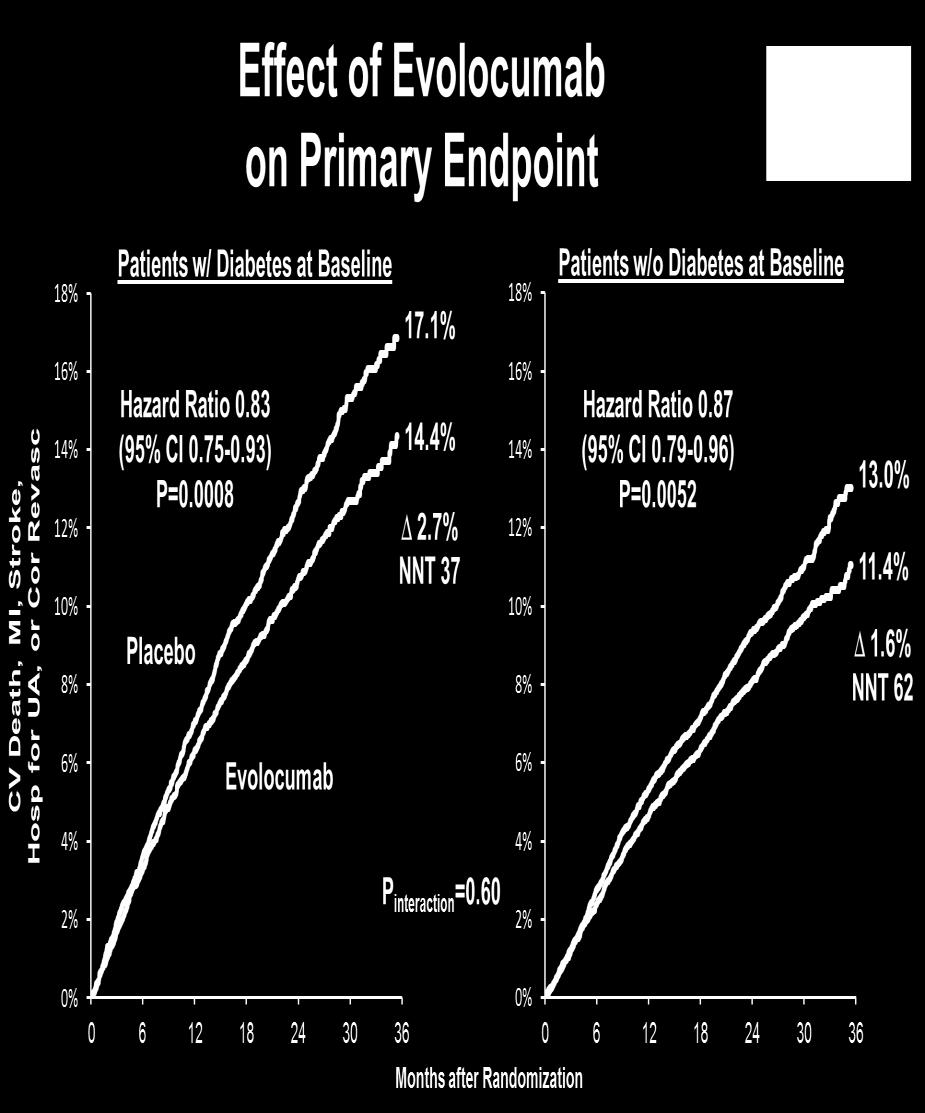
33 PEGASUS TIMI 54: Diabetes analysis (~6800 of 21000)
34 2018 Diabetes Canada CPG Chapter 23. Cardiovascular Protection in People with Diabetes Key Messages for People with Diabetes Ask your doctor about the ABCDEs to reduce your risk of heart attack and stroke: A = A1C Blood glucose control. The target is usually 7% or less B = BP Blood pressure control (less than 130/80 mm Hg) C = Cholesterol LDL-cholesterol less than 2.0 mmol/l. Your physician or nurse practitioner may advise you to start cholesterol lowering medication D = Drugs to protect your heart: These include blood pressure pills ( ACE inhibitors or ARBs), cholesterol lowering medication ( statins ), and in people with existing cardiovascular disease, certain blood glucose lowering medications. These blood glucose lowering medications can protect your heart even if your blood pressure and/or LDL-cholesterol are already at target E = Exercise /Eating Regular physical activity which includes healthy eating, and achievement and maintenance of a healthy body weight S = Stop smoking and manage stress
35 Questions?
36
37
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and Diagnosis Assess risk ANNUALLY if: Family history (First-degree
Quick Reference Guide
 2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
2018 Clinical Practice Guidelines Quick Reference Guide 416569-18 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Screening and diagnosis of type 2 diabetes in adults Assess risk factors for
Quick Reference Guide
 2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
2013 Clinical Practice Guidelines Quick Reference Guide (Updated November 2016) 416569-16 guidelines.diabetes.ca diabetes.ca 1-800-BANTING (226-8464) Copyright 2016 Canadian Diabetes Association SCREENING
Canadian Diabetes Association 2013 Clinical Practice Guidelines
 Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Canadian Diabetes Association 2013 Clinical Practice Guidelines The Essentials (Updated d November 2016) 2016 1 Faculty/Presenter Disclosure Faculty: Alan Bell MD CCFP Relationships with commercial and
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Disclaimers 22/03/2018. Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2
 Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Disclaimers Role of DPP-4 Inhibitors, GLP-1 Agonists, and SGLT-2 Inhibitors in the treatment of Diabetes Mellitus Type 2 I have not received money or gifts from medical device companies or from the pharmaceutical
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Content Development Committee
 1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
1 Content Development Committee Cardiologists: Family Physicians: Shaun Goodman, MD, MSc, FRCPC, FACC, FESC, FAHA, FCCS (Chair) Associate Head, Division of Cardiology, St. Michael s Hospital Professor,
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Medications for Type 2 Diabetes CDE Exam Preparation
 Medications for Type 2 Diabetes CDE Exam Preparation Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Agenda Medication
Medications for Type 2 Diabetes CDE Exam Preparation Medications for Type 2 Diabetes CDE Exam Preparation Wendy Graham, RD, CDE Mentor, WWD Angela Puim, RPh, CDE, CRE Preston Medical Pharmacy Agenda Medication
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY?
 MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
MANAGING DIABETES IN 2016 WHAT TO ADD, WHEN AND WHY? Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Staff Endocrinologist, St. Michael's Hospital Relationships with commercial
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks
 Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Diabetes and the Elderly: Medication Considerations When Determining Benefits and Risks Gretchen M. Ray, PharmD, PhC, BCACP, CDE Associate Professor UNM College of Pharmacy September 7 th, 2018 DISCLOSURES
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?!
 2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
2019 Update on Recent Guideline Releases for Diabetes, Hypertension, and Dyslipidemia: Can We, Please, All Just Get on the Same Page?! Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM Assistant Professor,
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC
 MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
MANAGING DIABETES IN 2017 WHAT TO ADD, WHEN AND WHY? December 8, 2017 Maria Wolfs MD MHSc FRCPC Faculty Disclosure Faculty: Maria Wolfs MD, MHSc, FRCPC Assistant Professor, University of Toronto Endocrinologist,
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Faculty/Presenter Disclosure
 DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
DIABETES UPATE 2016 Faculty/Presenter Disclosure Faculty/Presenter: tina kader Relationships with commercial interests: Grants/research support: BI; Sanofi Speaker s bureau/honoraria: eli lilly sanofi;
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
CV Risk Management in Diabetes Mellitus
 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue,
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Macrovascular Disease in Diabetes
 Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Du gusts is megl che one. Edoardo Mannucci
 Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Du gusts is megl che one Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca, Boehringer Ingelheim, Eli
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Cardiovascular Consequences of Diabetes Mellitus
 Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
Cardiovascular Consequences of Diabetes Mellitus William J. Elliott, M.D., Ph.D. 05 MAY 18 Disclosure Statement The speaker s research and educational activities have been supported in the past (but NOT
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Canadian Journal of Diabetes
 Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
What s the Goal? Individualizing Glycemic Targets. Matthew Freeby M.D. December 3 rd, 2016
 What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
What s the Goal? Individualizing Glycemic Targets Matthew Freeby M.D. December 3 rd, 2016 Diabetes Mellitus: Complications and Co-Morbid Conditions Retinopathy Between 2005-2008, 28.5% of patients with
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
The New Diabetes Standard of Care: More Than Just Glycemic Control. Copyright
 CLINICAL Viewpoint The New Diabetes Standard of Care: More Than Just Glycemic Control Advancement in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
CLINICAL Viewpoint The New Diabetes Standard of Care: More Than Just Glycemic Control Advancement in Diabetes Management: A Canadian Diabetes Steering Committee Report Copyright Not for Sale or Commercial
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
3. Cardiovascular Disease?
 Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Swiss recommendations 2016 Swiss Society of Endocrinology and Diabetology 1. Deficiency? Basal Premixed- Basal + GLP-1 RA (Xultophy ) or Basal Bolus 2. egfr < 30 ml/min? 3. Cardiovascular Disease? 4. Heart
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Update on the Canadian Diabetes Association 2008 clinical practice guidelines
 Update on the Canadian Diabetes Association 2008 clinical practice guidelines Onil K. Bhattacharyya MD PhD CCFP Elizabeth A. Estey MA Alice Y.Y. Cheng MD FRCPC Rates of diabetes are increasing in Canada,
Update on the Canadian Diabetes Association 2008 clinical practice guidelines Onil K. Bhattacharyya MD PhD CCFP Elizabeth A. Estey MA Alice Y.Y. Cheng MD FRCPC Rates of diabetes are increasing in Canada,
How to Use the ADA Type 2 Diabetes Treatment Algorithm. Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP
 How to Use the ADA Type 2 Diabetes Treatment Algorithm Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP 8 ACOFP 55th Annual Convention & Scientific Seminars ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please
How to Use the ADA Type 2 Diabetes Treatment Algorithm Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP 8 ACOFP 55th Annual Convention & Scientific Seminars ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Evaluating the Cardiovascular Benefits of Antidiabetic Medications
 Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
Evaluating the Cardiovascular Benefits of Antidiabetic Medications Target Audience: Pharmacists ACPE#: 0202-0000-18-054-L01-P Activity Type: Application-based Disclosures Stuart T. Haines has no relevant
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type 2 Diabetes
 Draft Comparative Effectiveness Review Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type Diabetes Prepared for: Agency for Healthcare Research and Quality U.S. Department
Draft Comparative Effectiveness Review Comparative Effectiveness and Safety of Diabetes Medications for Adults with Type Diabetes Prepared for: Agency for Healthcare Research and Quality U.S. Department