Supplementary Online Content
|
|
|
- Brenda Robbins
- 5 years ago
- Views:
Transcription
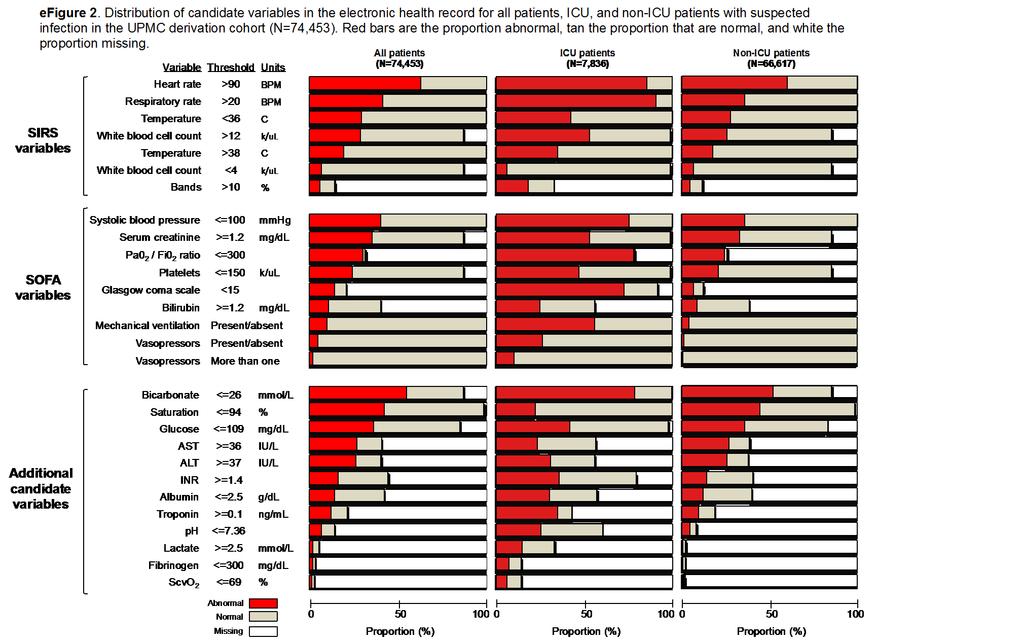
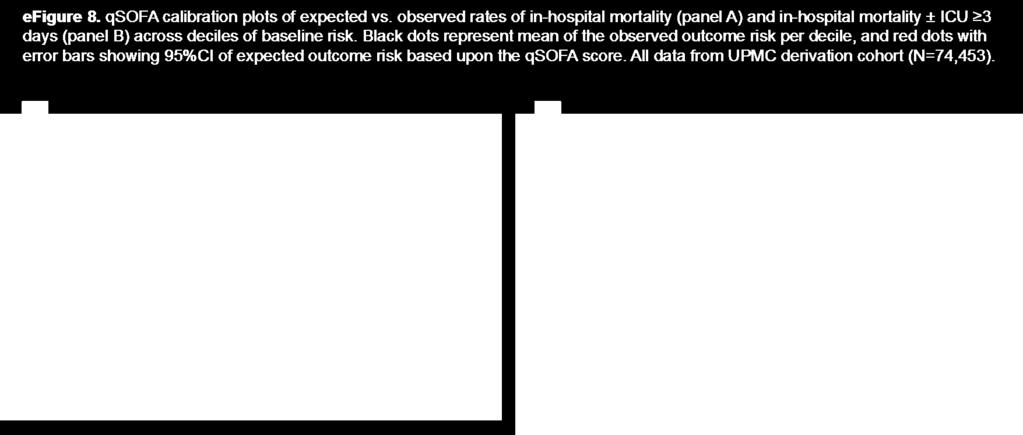
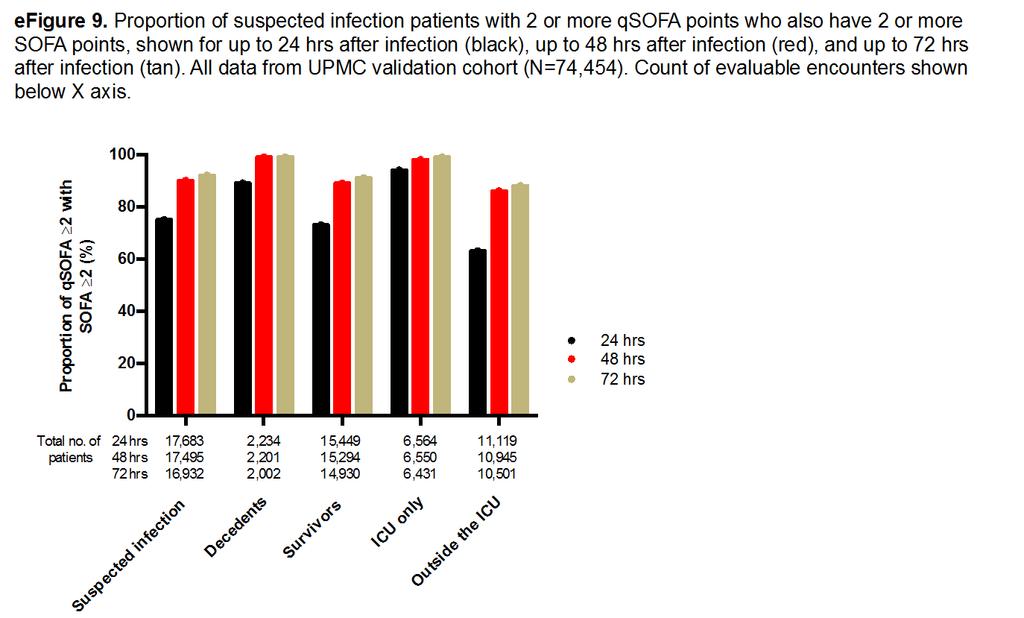
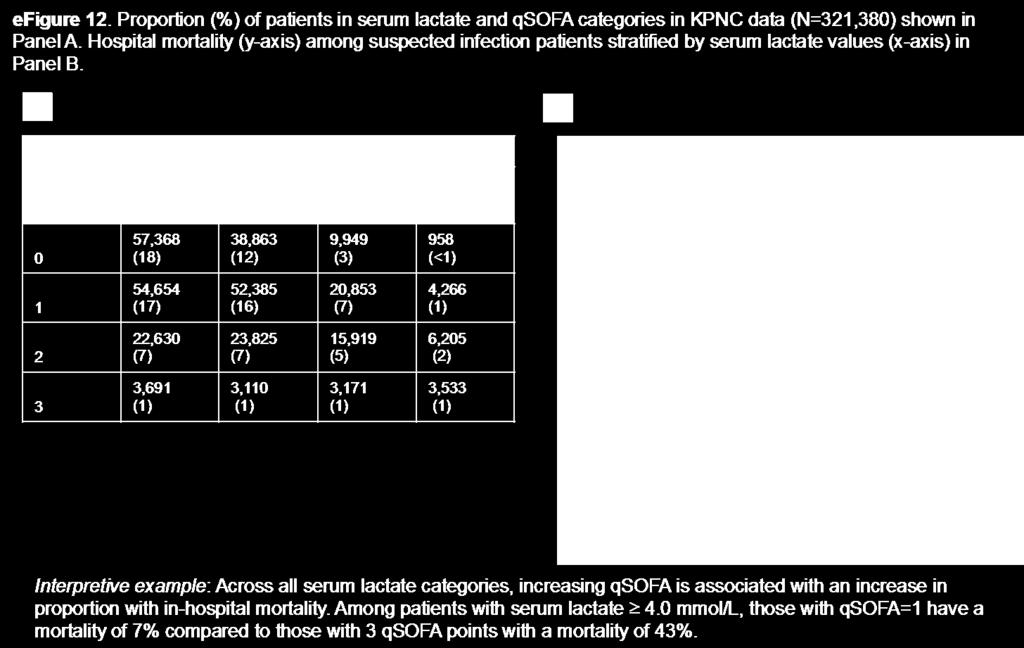
1 Supplementary Online Content Seymour CW, Liu V, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. doi: /jama eappendix. Discussion of Supplementary Methods efigure 1. Distribution of Baseline Risk of In-Hospital Mortality (± ICU Stay of 3 Days) Across Deciles efigure 2. Distribution of Candidate Variables in the Electronic Health Record for All Patients, ICU, and Non-ICU Patients With Suspected Infection in the UPMC Derivation Cohort (N=74,453) efigure 3. Proportion of Patients With In-Hospital Mortality Across the Range of SIRS, SOFA, LODS, and qsofa in the UPMC Validation Cohort (N=74,454) efigure 4. AUROC for In-Hospital Mortality for SIRS, SOFA, LODS, and qsofa in the UPMC Validation Cohort (N=74,454) and External Datasets efigure 5. Fold Change in In-Hospital Mortality (± ICU Stay of 3 Days) Comparing Encounters by Different Criteria in the UPMC Validation Cohort (N=74,454) efigure 6. AUROC for In-Hospital Mortality (± ICU Stay of 3 Days) for SIRS, SOFA, LODS, and qsofa in the UPMC Validation Cohort (N=74,454) efigure 7. Distribution of qsofa in External Datasets and Crude Rates of In-Hospital Mortality by qsofa efigure 8. Calibration of qsofa Score for In-Hospital Mortality (± ICU Stay of 3 Days) efigure 9. Proportion of Encounters With 2 or More qsofa Points Who Also Have 2 or More SOFA Points Over Different Time Intervals After Onset of Suspected Infection in the UPMC Validation Cohort (N=74,454), Ranging From 24 to 72 Hours efigure 10. AUROC for qsofa With and Without Serum Lactate 2.0 mmol/l and Fold Change in In- Hospital Mortality Comparing Encounters Classified by qsofa Model With and Without Lactate efigure 11. Crude In-Hospital Mortality Rates for Each qsofa Score Over the Distribution of Baseline Risk Comparing, Including Patients qsofa=1 Who Do and Do Not Have Serum Lactate 2.0 mmol/l efigure 12. Crude In-Hospital Mortality Rate Stratified by Serum Lactate and qsofa etable 1. Characteristics of Patients in External Datasets etable 2. AUROC Values for In-Hospital Mortality for SIRS, SOFA, LODS, and qsofa With Pairwise Comparisons and Tests of Inference etable 3. Classification of Decedents and Survivors With Suspected Infection by SIRS, SOFA, LODS and qsofa etable 4. Sensitivity Analyses of qsofa This supplementary material has been provided by the authors to give readers additional information about their work.
2 eappendix. Discussion of Supplementary Methods (A) Description of methods to identify infection We identified suspected infection by clinicians in the electronic health record using two concurrent events: 1) order for administration of antibiotics and 2) order for body fluid culture. These two events needed to occur in a specific time epoch with two options as described below. We used this algorithm in the derivation cohort (UPMC) and external cohorts (VA, KPNC). We identified only the first episode of suspected infection for each encounter. The specific date/time of suspected infection ( time zero ) was whichever of these two events that occurred first. In option 1, the body fluid culture was drawn first, and the antibiotic administration must occur within 72 hrs. In option 2, the antibiotic dose occurs first, and the body fluid culture must occur within 24 hrs. We excluded all antibiotic doses administered as a single dose or in the operating room. We excluded antibiotics administered without an accompanying body fluid culture. We included fluid cultures form a variety of sites: abdomen, bronchoalveolar lavage, blood, bone, cerebral spinal fluid, catheters/devices, pleural space, skin/tissue, stool, urinary tract. Culture types included bacterial, fungal, viral, parasitic, and testing for C diff. toxin. In external datasets without electronic health records, the presence of infection was identified as previously described in these retrospective cohorts. In ALERTS, research coordinators screened hospitalized patients of more than 48 hrs who received antibiotics for the presence of Center for Disease Control criteria for hospital-acquired infection. 1 In KCEMS, prehospital records were linked to discharge diagnoses with present-on-admission indicators. We identified infected patients in this cohort using the Angus implementation of infection (with explicit severe sepsis codes), as validated in prior work. 2,3 (B) Sensitivity analyses We assessed the predictive validity (AUROC) of the qsofa model after testing a variety of assumptions. These included various subsets, strategies to account for missing data, different epochs of time for qsofa variables, and alternative outcomes.
3 UPMC sensitivity analyses: 1) Multiple imputation. Multiple imputation procedure Missing data was common in our database (Figure 3). In our sensitivity analysis, we assumed that missing data was conditional on observed covariates, and was missing at random. We used a flexible multivariable imputation procedure of multiple chained regression equations (multiple imputation by chained equations, i.e. MICE) which generated values for all missing data using the observed data for all patients. 4 We included the all covariates and our primary outcome in the imputation procedure. We modeled variables using logistic, multinomial, or ordinal regression as appropriate. MICE may still lead to bias in the setting of missingness > 50%, but this bias is generally less than that resulting from complete case analysis (which assumes missing completely at random). 5 The imputation procedure created 11 independent datasets. For continuous, non-normal variables with upper and lower bounds (Glasgow coma scale score), we used predictive mean matching. 5 Analysis after multiple imputation We assessed the AUROC for the primary outcome (hospital mortality) in the independent imputed datasets. We report the median (range) of these measures across our imputed validation sets for three reasons: 1) the normality assumption of these statistics is uncertain, 2) they are generally bounded by 0 and 1, and 3) they are unlikely to have a symmetric distribution. 5 2) Altered mentation defined as GCS <15 Because GCS may not always be measured, we used any alteration in mentation (GCS<15) instead of GCS 13 in the qsofa model. 3) Restricted cohorts We assessed the predictive validity among cohorts with more specificity for infection. These included patients with presumed infection those suspected infection who received 2 doses of antibiotics within a 96 hr period. This signifies the patient received a course of antibiotics. If the patient was discharged or died prior to 96 hrs, they were deemed to have presumed infection. We also identified patients with positive blood cultures from microbiology record in the electronic health record. These were termed confirmed bacteremia. 4) Excluded: DNR, DNI, or CMO Because patients with code status limitations may not have clinical assessments as often as those who are full code, and thus may not have qsofa measured, we excluded those patients with either do-not-resuscitate, do-not-intubate, or comfortmeasures-only status at the time of suspected infection. 5) Added: serum lactate We explored how adding serum lactate to the qsofa model would change the AUROC. We dichotomized infection patients whether serum lactate (arterial or venous) >=2.0 mmol/l in the time window around infection (48 hrs before, 24 hrs after). We gave 1 point for elevated serum lactate, and the qsofa model had a range of 0 to 4 points. We chose not to use assessments of net reclassification as no validated risk threshold are used in the care of septic patients for clinical decision making. 6 There are also known limitations of using the incremental discrimination improvement as a metric. 7 6) Excluded: antibiotics administered 24 hrs after culture We defined suspected infection using a dyad of body fluid culture and antibiotic administration. If the culture came first, the median time to antibiotic dosing was 3.1 hours [IQR: 1.3, 13.1 hours]. We tested if the predictive validity of qsofa was robust to excluding encounters in which the time after body fluid culture to antibiotics was 24 hrs. 7) Time window: restricting to 24 hrs after onset of infection Although debated, some clinicians may not review the electronic health record prior to suspected infection for organ dysfunction criteria. They may only look at proximate data or wait for organ dysfunction to develop in the future. To address
4 the concern that a 48 hour look back window would bias our findings, we tested the predictive validity of qsofa using only the 24 hrs forward in time after the onset of infection. KPNC sensitivity analyses 1) Restricted cohorts We assessed two restricted cohorts at KPNC. The first tested the predictive validity of qsofa only among patients at hospital who had >50% of GCS documented (N=88,062). This was 27% of the KPNC cohort. Second, we tested qsofa in presumed infection patients using the same procedure as UPMC. 2) Altered mentation defined using LAPS2 We used an alternative method to identify altered mentation in the electronic health record. The LAPS2 is a validated method (Medical Care, 2008, Escobar et al.) that provides a measure of altered mentation using natural language processing, specifically for patients in whom GCS is missing. For this analysis, as a result, the altered mentation variable had no missingness. 3) Excluded: DNR, DNI, or CMO at the time of infection Similar to UPMC, we excluded encounters deemed to be DNR, DNI, or CMO at the time of infection. 4) Adding serum lactate level We conducted extensive sensitivity analyses when adding serum lactate to qsofa - as described in the Methods of the main paper. Serum lactate was measured in more than 50% of suspected infection patients at KPNC as a result of a system wide quality improvement program. We tested a variety of serum lactate thresholds (2.0 mmol/l, 3.0 mmol/l, and 4.0 mmol/l), and show results for 2.0 mmol/l given use of this threshold in prior consensus statements. 8 We also tested how qsofa would improve if serum lactate modeled as a continuous variable was added to the model. Results were similar for other thresholds. 5) Time windows We used a time window of 48 hrs before to 24 hrs after for primary qsofa analyses. We chose this window as it captures the breadth of clinical data available to the physician prescribing antibiotics/obtaining cultures who is considering criteria for sepsis. We use a lag period of 24 hrs after infection, as important lab values may not populate in the electronic health record in real time. To explore different windows, we narrowed the time window to 3 hrs before until 3 hrs after infection suspected, and 12 hours before to 12 hours after, and repeated analyses. VA sensitivity analyses 1) Restricted cohorts We used the same parameterization of presumed infection in the VA data and repeated analyses. 2) Outcome We used hospital mortality as one of the outcomes in our predictive validity analyses. This outcome may suffer from discharge bias. 9,10 We used fixed time point mortality (30 days) and repeated analyses. 3) Serum lactate We added serum lactate to the qsofa model using a threshold of 2.0 mmol/l. Because the VA model did not have GCS, the serum lactate qsofa model had a range of 0 to 3 points.
5
6
7
8
9
10
11
12

13
14

15
16
17 etable 1. Characteristics of Patients With Suspected Infection in External Datasets* Variable KPNC (N=321,380) VA (N=377,325) ALERTS (N=1,186) KCEMS (N=6,508) Infection type & Presumed 312, ,950 1,186. Confirmed bacteremia 29,243 55, Age, mean (SD) years 66 (19) 67 (12) 66 (15) 72 (16) Male gender, no. (%) 144,347 (45) 363,131 (96) 636 (54) 2,890 (44) Race or ethnicity, no. (%) White 212,825 (66)... Black 30,009 (9)... Other 78,546 (24)... Weighted Charlson sum, mean (SD) 1.3 (1.3) 2.4 (2.3) 2.4 (1.4) 1.8 (1.6) Surgery prior to infection suspected, no. (%) 25,429 (8) 143,726 (38) 705 (60) ^. Onset of infection within 48 hours of admission, no. (%) 260,387 (81) 253,992 (67) 0 (0) 6,508 (100) Unit location at the time infection suspected, no. (%) ED 239,526 (75) 0 (0) 0 (0) 6,508 (100) Ward 23,358 (7) 310,324 (82) 727 (61) 0 (0) ICU 7,031 (2) 73,264 (19) 300 (25) 0 (0) PACU or Procedure unit 31,208 (10) 0 (0) 0 (0) 0 (0) Step-down unit 2,257 (1) 0 (0) 0 (0) 0 (0) Other or missing 18,000 (6) 0 (0) 159 (13) 0 (0) Max. SIRS day of infection suspected, mean (SD) ** 2.3 (1.0). 1.6 (1.3). median [IQR] 2 [2-3]. 2 [1-3]. Max. SOFA score day of infection suspected, mean (SD) *** 1.9 (2.4) 1.3 (1.7).. median [IQR] 1 [0-3] 1 [0-2].. Lactate measured on day of infection suspected, no. (%) 183,037 (57) 25,250 (7).. Lactate 2.0 mmol/l, no. (%) of measured 64,854 (20) 9,323 (37).. ICU admission, no. (%) 71,362 (22) 110,815 (29) 300 (25) 3,066 (47) Hospital length of stay, median [IQR] days 4 [2-6] 7 [4-12] 25 [16-28] 4 [2-7] Hospital mortality, no. (%) 16,092 (5) 22,593 (6) 210 (18) 700 (11) * KPNC and VA data derived from electronic health records, ALERTS from a prospective cohort study of hospital acquired infections, and KCEMS from an administrative database of out-of-hospital records & Infection type specified as suspected, presumed, or confirmed bacteremia as described in the emethods.( Restricted cohorts ). ** SIRS criteria range from 0 to 4, where 1 point is given for perturbations of the following variables, respiratory rate, white blood cell count/bands, heart rate, or temperature. 29 Maximum SIRS reported from day infection suspected. *** SOFA (sepsis-related organ failure assessment) score ranges from 0 to 24, where 0 to 4 points are assigned for one of six organ dysfunctions: hematologic, hepatic, respiratory, neurologic, cardiac, and renal. 11 A greater score corresponds to greater severity. Maximum score reported from day infection suspected. Abbreviations: ED = emergency department; ICU = intensive care unit; IQR = interquartile; range no. = number; PACU = post-acute care unit; SD = standard deviation; SIRS = systemic inflammatory response syndrome; SOFA = sepsis related organ function assessment
18 etable 2. Area Under the Receiver Operating Characteristic Curve for In-Hospital Mortality of Candidate Criteria (SIRS, SOFA, LODS, qsofa) Among Suspected Infection Encounters in the UPMC Validation Cohort (N=74,454). Criteria ICU (N=7,932) Comparison P value Outside the ICU (N=66,522) Comparison P value Baseline model 0.58 (0.57, 0.60) (0.68, 0.70).. SIRS 0.64 (0.62, 0.66) SOFA 0.74 (0.73, 0.76) LODS 0.75 (0.73, 0.76) qsofa * 0.66 (0.64, 0.68) vs SOFA: <0.01 vs SOFA: <0.01 vs. qsofa: (0.75, 0.77) vs. qsofa: <0.01 vs. LODS: <0.01 vs. LODS: <0.01 vs SIRS: <0.01 vs SIRS: <0.01 vs. LODS: (0.78, 0.80) vs. LODS: <0.01 vs. qsofa: <0.01 vs. qsofa: <0.01 vs SIRS: <0.01 vs SIRS: <0.01 vs. SOFA: (0.80, 0.82) vs. SOFA: <0.01 vs. qsofa: <0.01 vs. qsofa: 0.72 vs SIRS: 0.01 vs SIRS: <0.01 vs. SOFA: < (0.80, 0.82) vs. SOFA: <0.01 vs. LODS: <0.01 vs. LODS: 0.72 All auroc values correspond to a model that includes the criteria plus baseline variables (age, gender, race/ethnicity, co-morbidity). *AUROC for in-hospital mortality for qsofa in UPMC derivation cohort was 0.67 (95%CI: 0.66, 0.69) among ICU encounters (N=7,836) and 0.81 (95%CI: 0.80, 0.82) among non-icu encounters (N=66,617).
19 etable 3. Classification of Decedents and Survivors With Suspected Infection by SIRS, SOFA, LODS and qsofa in Different Hospital Locations at Different Thresholds in the UPMC Validation Cohort (N=74,454) Model Threshold Population Sample size No. deaths (%) No. survivors (%) Proportion of decedents with score at or above threshold (%, 95%CI) Proportion of survivors with score below threshold (%, 95%CI) SIRS criteria 2 All 74,454 3,175 (4) 71,279 (96) 75 (74, 77) 60 (59, 60) ICU 7,932 1,289 (16) 6,643 (84) 91 (89, 92) 17 (16, 18) Non-ICU 66,522 1,886 (3) 64,636 (97) 64 (62, 67) 65 (64, 65) SOFA score 2 All 74,454 3,175 (4) 71,279 (96) 80 (79, 81) 61 (61, 62) ICU 7,932 1,289 (16) 6,643 (84) 98 (97, 99) 10 (10, 11) Non-ICU 66,522 1,886 (3) 64,636 (97) 68 (66, 70) 67 (66, 67) SOFA score 3 All 74,454 3,175 (4) 71,279 (96) 72 (70, 73) 75 (75, 76) ICU 7,932 1,289 (16) 6,643 (84) 96 (95, 97) 19 (18, 20) Non-ICU 66,522 1,886 (3) 64,636 (97) 55 (53, 57) 81 (81, 82) Logistic organ dysfunction score 2 All 74,454 3,175 (4) 71,279 (96) 85 (83, 86) 64 (63, 64) ICU 7,932 1,289 (16) 6,643 (84) 98 (97, 99) 14 (13, 15) Non-ICU 66,522 1,886 (3) 64,636 (97) 75 (73, 78) 69 (68, 69) Logistic organ dysfunction score 3 All 74,454 3,175 (4) 71,279 (96) 79 (77, 80) 70 (70, 70) ICU 7,932 1,289 (16) 6,643 (84) 96 (95, 97) 19 (18, 20) Non-ICU 66,522 1,886 (3) 64,636 (97) 66 (64, 69) 75 (75, 76) qsofa 1 All 74,454 3,175 (4) 71,279 (96) 92 (91, 93) 43 (43, 44) ICU 7,932 1,289 (16) 6,643 (84) 99 (99, 99) 3 (2, 3) Non-ICU 66,522 1,886 (3) 64,636 (97) 86 (85, 88) 47 (47, 48) qsofa 2 All 74,454 3,175 (4) 71,279 (96) 70 (69, 72) 78 (78, 79) ICU 7,932 1,289 (16) 6,643 (84) 92 (91, 94) 19 (18, 20) Non-ICU 66,522 1,886 (3) 64,636 (97) 55 (53, 57) 84 (84, 85) Abbreviations: ICU intensive care unit; qsofa quick sepsis-related organ failure assessment; SIRS systemic inflammatory response syndrome; SOFA sepsis-related organ failure assessment
20 etable 4. Sensitivity Analyses of the Predictive Validity of qsofa After Testing Various Assumptions and A Priori Subgroups in UPMC Validation Cohort (N=74,454), KPNC (N=321,380), and VA Data (N=377,125) Sensitivity analysis or subgroup No. patients AUC (95% CI) for qsofa above baseline UPMC Validation cohort, primary model 74, (0.82, 0.83) Multiple imputation ^ 74, (0.82, 0.84) Altered mentation defined as GCS<15 74, (0.81, 0.84) Restricted: presumed infection 56, (0.79, 0.80) Restricted: confirmed bacteremia 3, (0.74, 0.78) Excluded: DNR/DNI/CMO at time of infection 72, (0.81, 0.85) Excluded: antibiotics administered 24 hrs after culture 67, (0.83, 0.86) Added: serum lactate 2.0 mmol/l 74, (0.83, 0.85) Time window: 24 hrs after time of infection 74, (0.83, 0.84) KPNC Full cohort, primary model 321, (0.78, 0.78) Restricted: hospitals with >50% GCS documentation 88, (0.78, 0.79) Restricted: presumed infection 312, (0.78, 0.79) Altered mentation defined using LAPS2 321, (0.78, 0.79) Excluded: DNR/DNI/CMO at time of infection 309, (0.78, 0.79) Added: serum lactate 2.0 mmol/l 321, (0.79, 0.80) Added: serum lactate 3.0 mmol/l 321, (0.79, 0.81) Added: serum lactate 4.0 mmol/l 321, (0.79, 0.81) Time window: 3 hrs before to 3 hrs after 321, (0.77, 0.78) Time window: 12 hrs before to 12 hrs after 321, (0.78, 0.79) VA * Full cohort, primary model 377, (0.78, 0.79) Restricted: presumed infection 247, (0.79, 0.79) Outcome: 30 day mortality 377, (0.78, 0.78) Added: serum lactate 2.0 mmol/l 377, (0.80, 0.80) Abbreviations: AUC area under the receiver operating characteristic curve, CI confidence interval, CMO comfort measures only, DNR do not resuscitate, DNI do not intubate, GCS Glasgow coma scale score, LAPS2 - laboratory-based acute physiology score-2.0 ^ Reporting the mean AUC and range (min, max) across 11 imputed datasets * External validation cohort at VA did not have GCS values and qsofa is a modified two variable model (systolic blood pressures and respiratory rate only), with range 0 to 2 points
21 ereferences 1. Hagel S, Ludewig K, Frosinski J, et al. [Effectiveness of a hospital-wide educational programme for infection control to reduce the rate of health-care associated infections and related sepsis (ALERTS)--methods and interim results]. Dtsch Med Wochenschr. 2013;138(34-35): Iwashyna TJ, Odden, A., Rohde, J., Bonham, C., Kuhn, L., Malani, P., Chen, L., Flanders, S. Identifying patients with severe sepsis using administrative claims: patient-level validation of the Angus implementation of the International Consensus Conference Definition of severe sepsis. Med Care. 2014; 52 (6): Seymour CW, Rea TD, Kahn JM, Walkey A, Yealy DM, Angus DC. Severe Sepsis in Prehospital Emergency Care: Analysis of Incidence, Care, and Outcome. Am J Resp Crit Care Med. 2012; 186 (12): van Buuren S, Boshuizen HC, Knook DL. Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med. 1999;18(6): Marshall A, Altman DG, Royston P, Holder RL. Comparison of techniques for handling missing covariate data within prognostic modelling studies: a simulation study. BMC Med Res Methodol. 19;10(1):7. 6. Pencina MJ, D'Agostino RB, Sr., Steyerberg EW. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat Med. J2011;30(1): Kerr KF, McClelland, R.L., Brown, E.R., Lumley T. Evaluating the incremental value of new biomarkers with integrated discrimination improvement. Am J Epidemiol. 2011;174 (3): Cecconi M, De Backer D, Antonelli M, et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12): Reineck LA, Pike F, Le TQ, Cicero BD, Iwashyna TJ, Kahn JM. Hospital Factors Associated With Discharge Bias in ICU Performance Measurement. Crit Care Med. 2014; 42(5): Vasilevskis EE, Kuzniewicz MW, Dean ML, et al. Relationship between discharge practices and intensive care unit inhospital mortality performance: evidence of a discharge bias. Med Care. 2009;47(7): Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996; 22(7): Le Gall JR, Klar J, Lemeshow S, et al. The Logistic Organ Dysfunction system. A new way to assess organ dysfunction in the intensive care unit. ICU Scoring Group. JAMA. 1996; 276(10):
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis-3: clarity or confusion
 Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Sepsis-3: clarity or confusion Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Can an otherwise
Assessment of Clinical Criteria for Sepsis For the Third International Consensus Definitions for Sepsis and Septic Shock(Sepsis-3)
") Research Original Investigation CARING FOR THE CRITICALLY ILL PATIENT Assessment of Clinical Criteria for Sepsis For the Third International Consensus Definitions for Sepsis and Septic Shock(Sepsis-3)
Research Original Investigation CARING FOR THE CRITICALLY ILL PATIENT Assessment of Clinical Criteria for Sepsis For the Third International Consensus Definitions for Sepsis and Septic Shock(Sepsis-3)
What the ED clinician needs to know about SEPSIS - 3. Anna Morgan Consultant EM Barts Health
 What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
What the ED clinician needs to know about SEPSIS - 3 Anna Morgan Consultant EM Barts Health Aims: (1) To review the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3) (2)
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign
 Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Updates On Sepsis Updates based on 2016 updates on sepsis from The International Surviving Sepsis Campaign Dr. Joseph K Erbe, DO Medical Director Hospitalist Division of Medicine Objectives 1. Review the
Sepsis 3 & Early Identification. Disclosures. Objectives 9/19/2016. David Carlbom, MD Medical Director, HMC Sepsis Program
 Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
Sepsis 3 & Early Identification David Carlbom, MD Medical Director, HMC Sepsis Program Disclosures I have no relevant financial relationships with a commercial interest and will not discuss off-label use
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
3 papers from ED. counting sepsis sepsis 3 wet or dry?
 3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
3 papers from ED counting sepsis sepsis 3 wet or dry? 5 million deaths/yr globally 24 billion USD annually in US system causes or contributes to half of US hospital deaths BP GCS RR From: The Third International
JMSCR Vol 05 Issue 06 Page June 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-45 DOI: https://dx.doi.org/.18535/jmscr/v5i6.1 A Study on Quick Sofa Score as a redictive
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-45 DOI: https://dx.doi.org/.18535/jmscr/v5i6.1 A Study on Quick Sofa Score as a redictive
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions
 Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Early Recognition and Timely Management of Sepsis Amid Changes in Definitions Tze Shien Lo, MD, FACP Chief, Infectious Disease Service Fargo VA Medical Center Professor of Medicine UND School of Medicine
Text-based Document. Implications of the Sepsis-3 Definition on Nursing Research and Practice. Authors Peach, Brian C. Downloaded 5-Jul :03:48
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Sepsis and Septic Shock: New Definitions for Adults
 PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
PL Detail-Document #320424 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER April 2016 Sepsis and Septic
Supplementary Online Content
 Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Supplementary Online Content Cooper DJ, Nichol A, Bailey M, et al. Effect of early sustained prophylactic hypothermia on neurologic outcomes among patients with severe traumatic brain injury: the POLAR
Keywords sepsis surveillance, Quick SOFA (qsofa), St John Sepsis Surveillance Agent, sepsis clinical decision support, early recognition of sepsis
, St John Sepsis Surveillance Agent, sepsis clinical decision support, early recognition of sepsis") 692034AJMXXX10.1177/1062860617692034American Journal of Medical QualityAmland and Sutariya research-article2017 Article Quick Sequential [Sepsis-Related] Organ Failure Assessment (qsofa) and St. John Sepsis
692034AJMXXX10.1177/1062860617692034American Journal of Medical QualityAmland and Sutariya research-article2017 Article Quick Sequential [Sepsis-Related] Organ Failure Assessment (qsofa) and St. John Sepsis
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Sepsis 3.0: pourquoi une nouvelle définition?
 Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
Sepsis 3.0: pourquoi une nouvelle définition? Jean-Daniel Chiche, MD PhD MICU & Dept Infection, Immunity & Inflammation Hôpital Cochin & Institut Cochin, Paris-F JAMA 2016; 315(8) WHY 1991 & 2001 Definitions:
Basics from anatomy and physiology classes Local tissue reactions
 Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
Septicaemia & SIRS Septicaemia is a life-threatening condition that arises when the physical reaction to an infection, causes damage to tissue and organs Basics from anatomy and physiology classes Local
MURDOCH RESEARCH REPOSITORY
 MURDOCH RESEARCH REPOSITORY This is the author s final version of the work, as accepted for publication following peer review but without the publisher s layout or pagination. The definitive version is
MURDOCH RESEARCH REPOSITORY This is the author s final version of the work, as accepted for publication following peer review but without the publisher s layout or pagination. The definitive version is
Supplementary Online Content
 Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Sepsis Learning Collaborative: Sepsis New Definitions
 Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
Sepsis Learning Collaborative: Sepsis New Definitions Sepsis 3, a New Definition Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Program Director and Academic Chair Department of Emergency Medicine Disclosures
No conflicts of interest to disclose
 No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
No conflicts of interest to disclose Introduction Epidemiology Surviving sepsis guidelines 2012 Updates Resuscitation protocols Map Goals Transfusion Sepsis-3 Bundle Management Questions Sepsis is a systemic,
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING
 IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
IDENTIFYING SEPSIS IN THE PREHOSPITAL SETTING Christopher Hunter, MD, PhD, FACEP Director, Health Services Department Associate Medical Director, Orange County EMS System Medical Director, Orlando Health
Appendix 1. Sensitivity analysis for ACQ: missing value analysis by multiple imputation
 Appendix 1 Sensitivity analysis for ACQ: missing value analysis by multiple imputation A sensitivity analysis was carried out on the primary outcome measure (ACQ) using multiple imputation (MI). MI is
Appendix 1 Sensitivity analysis for ACQ: missing value analysis by multiple imputation A sensitivity analysis was carried out on the primary outcome measure (ACQ) using multiple imputation (MI). MI is
Sepsi: nuove definizioni, approccio diagnostico e terapia
 GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
GIORNATA MONDIALE DELLA SEPSI DIAGNOSI E GESTIONE CLINICA DELLA SEPSI Giovedì, 13 settembre 2018 Sepsi: nuove definizioni, approccio diagnostico e terapia Nicola Petrosillo Società Italiana Terapia Antiinfettiva
NEW SEPSIS AND SEPTIC SHOCK DEFINITIONS. Giorgio Tulli e Giulio Toccafondi 2016
 NEW SEPSIS AND SEPTIC SHOCK DEFINITIONS Giorgio Tulli e Giulio Toccafondi 2016 THE STORY STARTS MORE THAN 20 YEARS AGO FIRST AND SECOND DEFINITIONS OF SEPSIS AND SEPTIC SHOCK Bone RC et al American College
NEW SEPSIS AND SEPTIC SHOCK DEFINITIONS Giorgio Tulli e Giulio Toccafondi 2016 THE STORY STARTS MORE THAN 20 YEARS AGO FIRST AND SECOND DEFINITIONS OF SEPSIS AND SEPTIC SHOCK Bone RC et al American College
Prehospital recognition of sepsis Christopher W. Seymour, MD MSc
 Prehospital recognition of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
Prehospital recognition of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
SEPSIS-3: THE NEW DEFINITIONS
 SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
SEPSIS-3: THE NEW DEFINITIONS WHAT THEY SHOULD MEAN TO YOU MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK https://www.youtube.com/watch?v=1s8l5d2xr6w IN THE
Current State of Pediatric Sepsis. Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018
 Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
Current State of Pediatric Sepsis Jason Clayton, MD PhD Pediatric Critical Care 9/19/2018 Objectives Review the history of pediatric sepsis Review the current definition of pediatric sepsis Review triage
SEPSIS & SEPTIC SHOCK
 SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
SEPSIS & SEPTIC SHOCK DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and mitigate potential bias
A BRIEF HISTORY OF SEPSIS. Euan Mackay
 A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
A BRIEF HISTORY OF SEPSIS Euan Mackay Aims History of sepsis definition Validity of new definition Hippocrates 4 th century BC Hippocrates introduced the term "σήψις the process of decay or decomposition
Supplementary Online Content
 Supplementary Online Content Toyoda N, Chikwe J, Itagaki S, Gelijns AC, Adams DH, Egorova N. Trends in infective endocarditis in California and New York State, 1998-2013. JAMA. doi:10.1001/jama.2017.4287
Supplementary Online Content Toyoda N, Chikwe J, Itagaki S, Gelijns AC, Adams DH, Egorova N. Trends in infective endocarditis in California and New York State, 1998-2013. JAMA. doi:10.1001/jama.2017.4287
Sepsis Denials. Presented by James Donaher, RHIA, CDIP, CCS, CCS-P
 Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
Sepsis Denials Presented by James Donaher, RHIA, CDIP, CCS, CCS-P Sepsis-1 2 From the first Sepsis Definition Conference in 1991 Defined sepsis as systemic response syndrome (SIRS) due to infection SIRS
New sepsis definition changes incidence of sepsis in the intensive care unit
 New sepsis definition changes incidence of sepsis in the intensive care unit James N Fullerton, Kelly Thompson, Amith Shetty, Jonathan R Iredell, Harvey Lander, John A Myburgh and Simon Finfer on behalf
New sepsis definition changes incidence of sepsis in the intensive care unit James N Fullerton, Kelly Thompson, Amith Shetty, Jonathan R Iredell, Harvey Lander, John A Myburgh and Simon Finfer on behalf
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
2017 American Medical Association. All rights reserved.
 Supplementary Online Content Borocas DA, Alvarez J, Resnick MJ, et al. Association between radiation therapy, surgery, or observation for localized prostate cancer and patient-reported outcomes after 3
Supplementary Online Content Borocas DA, Alvarez J, Resnick MJ, et al. Association between radiation therapy, surgery, or observation for localized prostate cancer and patient-reported outcomes after 3
Sepsis: What Is It Really?
 Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Sepsis: What Is It Really? Steven D. Burdette, MD, FIDSA, FACP Professor of Medicine Wright State University Boonshoft School of Medicine Director of Antimicrobial Stewardship for Premier Health and Miami
Supplementary Online Content
 Supplementary Online Content Andrews B, Semler MW, Muchemwa L, et al. Effect of an early resuscitation protocol on in-hospital mortality among adults with sepsis and hypotension: a randomized clinical
Supplementary Online Content Andrews B, Semler MW, Muchemwa L, et al. Effect of an early resuscitation protocol on in-hospital mortality among adults with sepsis and hypotension: a randomized clinical
Supplementary Online Content
 1 Supplementary Online Content 2 3 4 5 Hay AD, Little P, Harnden A, et al. Effect of oral prednisolone on symptom duration in nonasthmatic adults with acute lower respiratory tract infection: a randomized
1 Supplementary Online Content 2 3 4 5 Hay AD, Little P, Harnden A, et al. Effect of oral prednisolone on symptom duration in nonasthmatic adults with acute lower respiratory tract infection: a randomized
Supplementary Online Content
 Supplementary Online Content Berhane K, Chang C-C, McConnell R, et al. Association of changes in air quality with bronchitic symptoms in children in California, 1993-2012. JAMA. doi:10.1001/jama.2016.3444
Supplementary Online Content Berhane K, Chang C-C, McConnell R, et al. Association of changes in air quality with bronchitic symptoms in children in California, 1993-2012. JAMA. doi:10.1001/jama.2016.3444
Inflammatory Statements
 Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Inflammatory Statements Using ETCO 2 Analysis in Sepsis Syndromes George A. Ralls M.D. Orange County EMS System Sepsis Sepsis Over 750,000 cases annually Expected growth of 1.5% per year Over 215,000 deaths
Supplementary Online Content
 Supplementary Online Content Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305(15):1553-1559. eequation. Applying the
Supplementary Online Content Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305(15):1553-1559. eequation. Applying the
Sepsis and septic shock are common, pathophysiologically
 Commentary THE NEW SEPSIS DEFINITIONS: IMPLICATIONS FOR CRITICAL CARE PRACTITIONERS By Ruth M. Kleinpell, RN, PhD, Christa A. Schorr, RN, MSN, NEA-BC, and Robert A. Balk, MD Sepsis and septic shock are
Commentary THE NEW SEPSIS DEFINITIONS: IMPLICATIONS FOR CRITICAL CARE PRACTITIONERS By Ruth M. Kleinpell, RN, PhD, Christa A. Schorr, RN, MSN, NEA-BC, and Robert A. Balk, MD Sepsis and septic shock are
Systemic inflammatory response syndrome in Sepsis-3: a retrospective study
 Zhang et al. BMC Infectious Diseases (2019) 19:139 https://doi.org/10.1186/s12879-019-3790-0 RESEARCH ARTICLE Systemic inflammatory response syndrome in Sepsis-3: a retrospective study Wei Zhang 1,2*,
Zhang et al. BMC Infectious Diseases (2019) 19:139 https://doi.org/10.1186/s12879-019-3790-0 RESEARCH ARTICLE Systemic inflammatory response syndrome in Sepsis-3: a retrospective study Wei Zhang 1,2*,
Sepsis. Current Dilemmas in Diagnosing Sepsis. Chapter 2
 Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Chapter 2 Current Dilemmas in Diagnosing Derek Braun Derek Braun, Banner Health, 2901 N. Central Ave. Ste 180, Phoenix, AZ 85012 Email: derek.braun@bannerhealth.com Abbreviations: APACHE : Acute Physiology,
Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis
 The new england journal of medicine original article Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis Kirsi-Maija Kaukonen, M.D., Ph.D., Michael Bailey, Ph.D., David Pilcher,
The new england journal of medicine original article Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis Kirsi-Maija Kaukonen, M.D., Ph.D., Michael Bailey, Ph.D., David Pilcher,
Supplementary Online Content
 Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
TITLE: A Data-Driven Approach to Patient Risk Stratification for Acute Respiratory Distress Syndrome (ARDS)
") TITLE: A Data-Driven Approach to Patient Risk Stratification for Acute Respiratory Distress Syndrome (ARDS) AUTHORS: Tejas Prahlad INTRODUCTION Acute Respiratory Distress Syndrome (ARDS) is a condition
TITLE: A Data-Driven Approach to Patient Risk Stratification for Acute Respiratory Distress Syndrome (ARDS) AUTHORS: Tejas Prahlad INTRODUCTION Acute Respiratory Distress Syndrome (ARDS) is a condition
Consensus Definitions for Sepsis and Septic Shock (Sepsis-III)
") Consensus Definitions for Sepsis and Septic Shock (Sepsis-III) Advantages and Disadvantages Dr. Luis García-Castrillo Content: Reasons for new definition. Advantages of Sepsis III. Disadvantages of Sepsis
Consensus Definitions for Sepsis and Septic Shock (Sepsis-III) Advantages and Disadvantages Dr. Luis García-Castrillo Content: Reasons for new definition. Advantages of Sepsis III. Disadvantages of Sepsis
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series
 Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series Li-Wei H. Lehman, MIT Shamim Nemati, Emory University Roger G. Mark, MIT Proceedings Title: Computing
Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series Li-Wei H. Lehman, MIT Shamim Nemati, Emory University Roger G. Mark, MIT Proceedings Title: Computing
Supplementary Online Content
 Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Supplementary Online Content Dharmarajan K, Wang Y, Lin Z, et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA. doi:10.1001/jama.2017.8444 etable
Sepsis: Mitigating Denials Amid Definition Disparity
 Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Mitigating Denials Amid Definition Disparity White Paper - April 2017 Sepsis Criteria at a Glance The Society of Critical Care Medicine (SCCM) met in 2016 to update the definition of sepsis. During
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Supplementary Online Content
 Supplementary Online Content James MT, Neesh P, Hemmelgarn BR, et al. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA. doi:10.1001/jama.2017.16326
Supplementary Online Content James MT, Neesh P, Hemmelgarn BR, et al. Derivation and external validation of prediction models for advanced chronic kidney disease following acute kidney injury. JAMA. doi:10.1001/jama.2017.16326
Andrea Blotsky MDCM FRCPC General Internal Medicine, McGill University Thursday, October 15, 2015
 The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
The TIMES Project: (Time to Initiation of Antibiotic Therapy in Medical Patients Presenting to the Emergency Department with Sepsis) - Preliminary Findings Andrea Blotsky MDCM FRCPC General Internal Medicine,
Critical care resources are often provided to the too well and as well as. to the too sick. The former include the patients admitted to an ICU
 Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines
 TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
TITLE: Optimal Oxygen Saturation Range for Adults Suffering from Traumatic Brain Injury: A Review of Patient Benefit, Harms, and Guidelines DATE: 11 April 2014 CONTEXT AND POLICY ISSUES Traumatic brain
Contents. Version 1.0: 01/02/2010 Protocol# ISRCTN Page 1 of 7
 Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Contents 1. INTRODUCTION... 2 2. STUDY SYNOPSIS... 2 3. STUDY OBJECTIVES... 2 3.1. Primary Objective... 2 3.2. Secondary Objectives... 2 3.3. Assessment of Objectives... 3 3.4. Change the Primary Objective
Yun-Xia Chen 1, Jun-Yu Wang 1 and Shu-Bin Guo 1,2*
 Chen et al. Critical Care (2016) 20:167 DOI 10.1186/s13054-016-1351-0 RESEARCH Use of CRB-65 and quick Sepsis-related Organ Failure Assessment to predict site of care and mortality in pneumonia patients
Chen et al. Critical Care (2016) 20:167 DOI 10.1186/s13054-016-1351-0 RESEARCH Use of CRB-65 and quick Sepsis-related Organ Failure Assessment to predict site of care and mortality in pneumonia patients
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc
 Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
Prehospital treatment of sepsis Christopher W. Seymour, MD MSc The CRISMA Center Assistant Professor of Critical Care Medicine & Emergency Medicine University of Pittsburgh School of Medicine Disclosures
Supplementary Online Content
 Supplementary Online Content Schnabel RB, Aspelund T, Li G, et al. Validation of an atrial fibrillation risk algorithm in whites and African Americans. Arch Intern Med. 2010;170(21):1909-1917. eappendix.
Supplementary Online Content Schnabel RB, Aspelund T, Li G, et al. Validation of an atrial fibrillation risk algorithm in whites and African Americans. Arch Intern Med. 2010;170(21):1909-1917. eappendix.
Sepsis in primary care. what is good care?
 Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Sepsis in primary care @SepsisUK what is good care? Emmanuel Nsutebu Consultant Infectious Disease Physician & Clinical lead for sepsis Tropical and Infectious Disease Unit Royal Liverpool Hospital Do
Time to Treatment and Mortality during Mandated Emergency Care for Sepsis
 The new england journal of medicine Original Article Time to Treatment and Mortality during Mandated Emergency Care for Sepsis Christopher W. Seymour, M.D., Foster Gesten, M.D., Hallie C. Prescott, M.D.,
The new england journal of medicine Original Article Time to Treatment and Mortality during Mandated Emergency Care for Sepsis Christopher W. Seymour, M.D., Foster Gesten, M.D., Hallie C. Prescott, M.D.,
Chapter 17 Sensitivity Analysis and Model Validation
 Chapter 17 Sensitivity Analysis and Model Validation Justin D. Salciccioli, Yves Crutain, Matthieu Komorowski and Dominic C. Marshall Learning Objectives Appreciate that all models possess inherent limitations
Chapter 17 Sensitivity Analysis and Model Validation Justin D. Salciccioli, Yves Crutain, Matthieu Komorowski and Dominic C. Marshall Learning Objectives Appreciate that all models possess inherent limitations
Yun Tae Jung 1, Jiyeon Jeon 2, Jung Yun Park 1, Myung Jun Kim 1, Seung Hwan Lee 1 and Jae Gil Lee 1*
 Jung et al. World Journal of Emergency Surgery (2018) 13:14 https://doi.org/10.1186/s13017-018-0173-6 RESEARCH ARTICLE Open Access Addition of lactic acid levels improves the accuracy of quick sequential
Jung et al. World Journal of Emergency Surgery (2018) 13:14 https://doi.org/10.1186/s13017-018-0173-6 RESEARCH ARTICLE Open Access Addition of lactic acid levels improves the accuracy of quick sequential
Glucose tolerance status was defined as a binary trait: 0 for NGT subjects, and 1 for IFG/IGT
 ESM Methods: Modeling the OGTT Curve Glucose tolerance status was defined as a binary trait: 0 for NGT subjects, and for IFG/IGT subjects. Peak-wise classifications were based on the number of incline
ESM Methods: Modeling the OGTT Curve Glucose tolerance status was defined as a binary trait: 0 for NGT subjects, and for IFG/IGT subjects. Peak-wise classifications were based on the number of incline
Evaluation of Serum Lactate as Predictor of Morbidity and Mortality in Sepsis and Trauma Cases
 IOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS) e-issn:2278-38, p-issn:2319-7676. Volume 12, Issue 3 Ver. VII (May June 217), PP 1-5 www.iosrjournals.org Evaluation of Serum Lactate as Predictor
IOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS) e-issn:2278-38, p-issn:2319-7676. Volume 12, Issue 3 Ver. VII (May June 217), PP 1-5 www.iosrjournals.org Evaluation of Serum Lactate as Predictor
Supplementary Online Content
 Supplementary Online Content Downes KJ, Cowden C, Laskin BL, et al. Association of acute kidney injury with concomitant vancomycin and piperacillin/tazobactam treatment among hospitalized children. JAMA
Supplementary Online Content Downes KJ, Cowden C, Laskin BL, et al. Association of acute kidney injury with concomitant vancomycin and piperacillin/tazobactam treatment among hospitalized children. JAMA
What is sepsis? RECOGNITION. Sepsis I Know It When I See It 9/21/2017
 Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Sepsis I Know It When I See It September 15, 2017 Matthew Exline, MD MPH Medical Director, Medical ICU What is sepsis? I shall not today attempt further to define the kinds of material [b]ut I know it
Genetic risk prediction for CHD: will we ever get there or are we already there?
 Genetic risk prediction for CHD: will we ever get there or are we already there? Themistocles (Tim) Assimes, MD PhD Assistant Professor of Medicine Stanford University School of Medicine WHI Investigators
Genetic risk prediction for CHD: will we ever get there or are we already there? Themistocles (Tim) Assimes, MD PhD Assistant Professor of Medicine Stanford University School of Medicine WHI Investigators
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
BIOSTATISTICAL METHODS
 BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency
 BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
BIOMARKERS IN SEPSIS: DO THEY REALLY GUIDE US? Asist. Prof. M.D. Mehmet Akif KARAMERCAN Gazi University School of Medicine Depertment of Emergency Medicine 1 NO CONFLICT OF INTEREST 2 We do not fully understand
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
de Groot et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2017) 25:91 DOI /s
 25:91 DOI /s") de Groot et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2017) 25:91 DOI 10.1186/s13049-017-0436-3 ORIGINAL RESEARCH Open Access The most commonly used disease severity scores
de Groot et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2017) 25:91 DOI 10.1186/s13049-017-0436-3 ORIGINAL RESEARCH Open Access The most commonly used disease severity scores
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Supplementary Online Content
 Supplementary Online Content Pincus D, Ravi B, Wasserstein D. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. doi: 10.1001/jama.2017.17606 eappendix
Supplementary Online Content Pincus D, Ravi B, Wasserstein D. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA. doi: 10.1001/jama.2017.17606 eappendix
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Supplementary Online Content
 Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Supplementary Online Content Wolters FJ, Li L, Gutnikov SA, Mehta Z, Rothwell PM. Medical attention seeking after transient ischemic attack and minor stroke in relation to the UK Face, Arm, Speech, Time
Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series
 Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series The MIT Faculty has made this article openly available. Please share how this access benefits you.
Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series The MIT Faculty has made this article openly available. Please share how this access benefits you.
Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
 Clin Exp Emerg Med 2014;1(1):35-40 http://dx.doi.org/10.15441/ceem.14.012 Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
Clin Exp Emerg Med 2014;1(1):35-40 http://dx.doi.org/10.15441/ceem.14.012 Impact of timely antibiotic administration on outcomes in patients with severe sepsis and septic shock in the emergency department
Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials
 Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials Harm Jan de Grooth, Jean Jacques Parienti, [to be determined],
Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials Harm Jan de Grooth, Jean Jacques Parienti, [to be determined],
Supplemental Material
 Supplemental Material Supplemental Results The baseline patient characteristics for all subgroups analyzed are shown in Table S1. Tables S2-S6 demonstrate the association between ECG metrics and cardiovascular
Supplemental Material Supplemental Results The baseline patient characteristics for all subgroups analyzed are shown in Table S1. Tables S2-S6 demonstrate the association between ECG metrics and cardiovascular
BC Sepsis Network Emergency Department Sepsis Guidelines
 The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
The provincial Sepsis Clinical Expert Group developed the BC, taking into account the most up-to-date literature (references below) and expert opinion. For more information about the guidelines, and to
Supplementary Material*
 Supplementary Material* Park LS, Tate JP, Sigel K, Brown ST, Crothers K, Gibert C, et al. Association of Viral Suppression With Lower AIDS-Defining and Non AIDS-Defining Cancer Incidence in HIV-Infected
Supplementary Material* Park LS, Tate JP, Sigel K, Brown ST, Crothers K, Gibert C, et al. Association of Viral Suppression With Lower AIDS-Defining and Non AIDS-Defining Cancer Incidence in HIV-Infected
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Usefulness of Procalcitonin in the management of Infections in ICU. P Damas CHU Sart Tilman Liège
 Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
Usefulness of Procalcitonin in the management of Infections in ICU P Damas CHU Sart Tilman Liège Procalcitonin Peptide 116 AA Produced by parenchymal cells during «sepsis»: IL1, TNF, IL6 : stimulators
The Ever Changing World of Sepsis Management. Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital
 The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
The Ever Changing World of Sepsis Management Laura Evans MD MSc Medical Director of Critical Care Bellevue Hospital COI Disclosures No financial interests to disclose Learning Objectives Review the evolution
Retrospective study; only patients w/lactate > 4. Initial Lactate: Did not address
 References and Literature Grading Is Lactate Measurement in the Emergency epartment Valuable as a Predictor of Outcomes in Adult Patients with Sepsis? Reference Grade Rank omment Support for: Lokhandwala,
References and Literature Grading Is Lactate Measurement in the Emergency epartment Valuable as a Predictor of Outcomes in Adult Patients with Sepsis? Reference Grade Rank omment Support for: Lokhandwala,
SUCCESS IN SEPSIS MORTALITY REDUCTION. Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar
 SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
SUCCESS IN SEPSIS MORTALITY REDUCTION Maryanne Whitney RN MSN CNS Improvement Advisor, Cynosure Health HRET HEN AK Webinar Got Sepsis? Now What?- Alerts & Bundles Maryanne Whitney RN, MS, CNS Improvement
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Supplementary Online Content
 Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
Supplementary Online Content Larsen JR, Vedtofte L, Jakobsen MSL, et al. Effect of liraglutide treatment on prediabetes and overweight or obesity in clozapine- or olanzapine-treated patients with schizophrenia
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain