DECLARATION OF CONFLICT OF INTEREST
|
|
|
- Sheryl Sanders
- 5 years ago
- Views:
Transcription
1 DECLARATION OF CONFLICT OF INTEREST









2 TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use aldosterone blockers? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart Failure and Hypertension Unit, Institut Lorrain du Coeur et des Vaisseaux University Henri Poincaré Nancy, France
3 TAKE HOME MESSAGES FROM RECENT HEART FAILURE CLINICAL TRIALS How to use Mineralocorticoid Receptor Antagonists (MRAs)? Faiez Zannad INSERM, U961 and Clinical Investigation Center CHU, Heart Failure and Hypertension Unit, Institut Lorrain du Coeur et des Vaisseaux University Henri Poincaré Nancy, France
4 Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from Alere, AstraZeneca, BG Medicine, Boston Scientific, Novartis, Pfizer, Resmed, Servier and Takeda.
5 MRAs in clinical practice Why? When to use? When Not to use? How? (Dosing, Safety) Which one? Class effect.
6 Aldosterone/MR antagonists beneficial across the spectrum of severity 1.00 Survival 30% RR, P < Total Mortality 15% RR, P= Spironolactone 20 Placebo 0.70 Eplerenone Placebo Months Months RALES (LVSD, CHF severe symptoms) Pitt B, Zannad F, Remme WJ, et al. N Engl J Med EPHESUS (LVSD + HF after MI) Pitt B, Remme W, Zannad F, et al. N Engl J Med. 2003
7 Probability of survival Probability of survival Aldosterone/MR antagonists beneficial across the spectrum of severity RALES 1663 NYHA class III/IV patients 95% ACE-I/10% β-blocker EMPHASIS-HF 2737 NYHA class II patients 93% ACE-I or ARB/87% β-blocker Placebo Eplerenone Placebo Spironolactone RRR (95% CI) 30 (18-40)% P < Years from randomization RRR (95% CI) 22 (5-36)% P = Years from randomization Pitt B, et al. N Engl J Med. 1999;341: Zannad F, et al. N Engl J Med. 2010;364:11-21.


8 1 year mortality (%) Opitimization of Neurohumoral blockade Systolic heart failure. Moderate to severe symptoms CONSENSUS RALES COPERNICUS NO ACE inhib. ACE inhib. Pitt B, et al. N Engl J Med. 1999;341: Packer M, et al. N Engl J Med. 2001;344: ACE inhib. ACE inhib. Aldo. antag. ACE inhib. ACE inhib. Aldo. antag. Aldo. antag Beta-blocker
9 Death at 1year (%) Opitimization of Neurohumoral blockade in systolic heart failure. Mild symptoms SOLVD-T ,6 12,4 CIBIS + MERIT-HF ,9 7,8 ACE inhib ACE inhib. ACE inhib. Beta-blocker The SOLVD Investigators. N Engl J Med ;325: CIBIS II. Lancet. 1999;353:9-13. MERIT-HF. Lancet. 1999;353: Zannad F, et al. N Engl J Med. 2011;364: EMPHASIS-HF ACE inhib. Beta-blocker 6.1 ACE inhib. Beta-blocker MRA
10 CV death or hospitalisation (%) CV death or hospitalisation (%) Which drug to add next to an ACE inhibitor and beta-blocker? CHARM-Added 2548 mainly NYHA class III patients 100% ACE-I/55% β-blocker/17% MRA EMPHASIS-HF 2737 NYHA class II patients 93% ACE-I or ARB/87% β-blocker Placebo 30 Placebo 20 Candesartan 20 Eplerenone 10 RRR 15 (4-25)% P= RRR 37 (26-46)% P< Time since randomization (years) Time since randomization (years) McMurray, et al. Lancet. 2003;362: Zannad F, et al. N Engl J Med. 2010;364:11-21.
11 Changing practice All symptomatic patients with low EF (With egfr > 30 ml/min and K <5.5 meq/l) + LBBB
12 Target population All patients with LVSD except patients with CKD (egfr < ml/min), excluded from trials and contra-indicated Patients with hyperkalemia (K+ > 5mEq/ml) Patients on potassium sparing agents or potassium supplements

13 When to initiate? CHF patients with stable conditions AHF post dischage when renal function has stabilized Acute MI + LVSD and HF as soon as possible after the 3rd day (the earlier the better)

14 EPHESUS: All-cause mortality EPHESUS Early initiation Late initiation
15 How to use? The evidence Target patient population Dosing Safety Class effect?
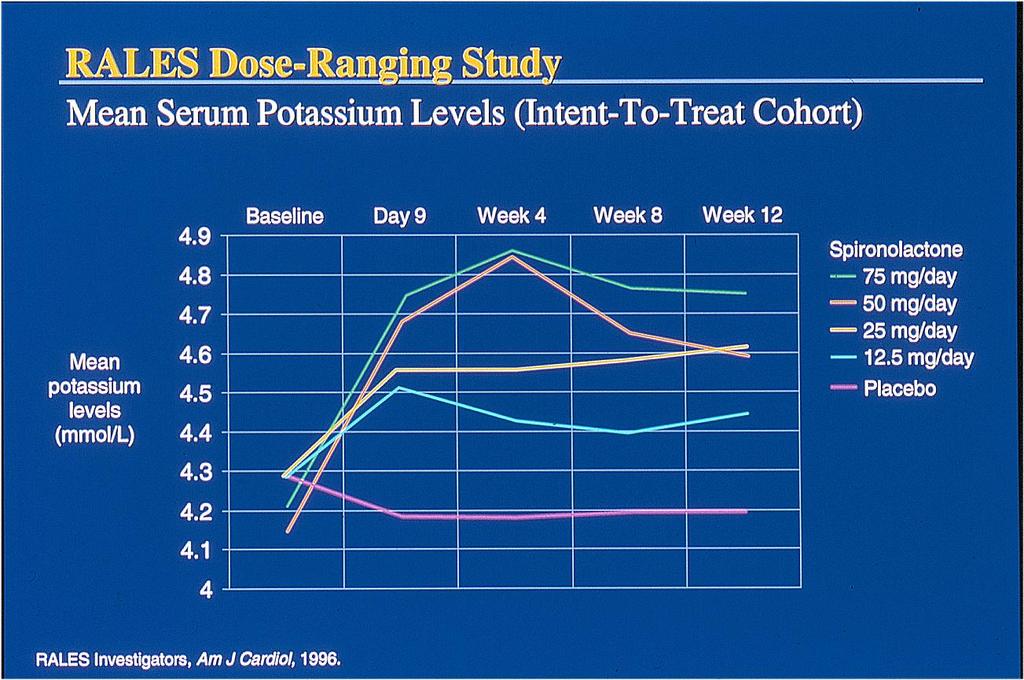
16 Dose-Finding in RALES Pmol/L 100 Nt-ANF Pcb Spironolactone (mg)
17




18 Treatment with RAAS Inhibitors Reduces Water and Sodium, but Increases Potassium Renin Inhibitors Angiotensin I ACE Inhibitors Angiotensin II ARBs Angiotensinogen K Retention Na/Water Uptake Hyperkalemia is an inherent risk in the treatment of HF with RAAS Inhibitors Mineralcorticoid Receptor AT1 Receptor Aldosterone Production Mineralocorticoid Receptor Antagonists (MRA)
19 Hyperkalemia with MRAs in Real Life HF Therapy Canada In-Hospital death from hyperkalemia before & after RALES publication Juurlink et al, NEJM 2004
20 Juurlink et al, NEJM 2004 Patients had frequently renal dysfunction Creatinine levels 1.8 to 2.0 mg per deciliter [159 to 176 μmol per liter]) RALES : 1.2 mg per deciliter (106 μmol per liter) Doses of spiro were higher than in RALES Many patients took potassium supplements or other hyerkamemic drugs Follow-up also was less vigorous than that in the clinical trial.

21 BMJ 2010;340:c1768 doi: /bmj.c1768
22 RAAS inhibition may be associated to serious adverse effects ONLY when used inappropriately In patients with or at risk of hyperkalemia or renal failure Beyond approved indications Without proper monitoring At doses exceeding the «safe» dose range
23 RAAS antagonists and Hyperkalemia How frequent? How to predict? How to prevent? How to manage?




24 Incidence (%) Incidence of hyperkalemia K+ >6.0 mmol/l Placebo Eplerenone Spironolactone P<.001 P= % 3.9% NS 2 1.7% 1.2% 2.5% 1.9% 0 RALES EPHESUS EMPHASIS-HF
25 EMPHASIS-HF Potassium Safety Outcome Patients with an adverse event leading to drug withdrawal no. (%) Eplerenone (N=1360) Placebo (N=1373) P Value Hyperkalemia (investigator reported AE) Hyperkalemia leading to drug discontinuation 109 (8) 50 (3.7) < (1.1) 12 (0.9) 0.57 Serum K+ > 5.5 mmol/l 158 (11.8) 96 (7.2) <0.001 Serum K+ > 6.0 mmol/l 33 (2.5) 25 (1.9) 0.29 Hospitalization for hyperkalemia (adjudicated) 4 (0.3) 3 (0.2) 0.85
26 CHARM Potassium Safety Study Candesartan Placebo Odds ratio CHARM Alternative CHARM Preserved CHARM Added CHARM Overall 4.0% 1.5% % 1.2% % 2.9% % 1.8% 2.9 Based on investigator s assessment of clinically important hyperkalemia Source: Desai et al, J Am Coll Cardiol 2007
27 Selected Adverse Events Rate / 100 person-years 8 7 All AEs Resulting in Discontinuation of Study Drug 6 * p < ** p = Hyperkalemia * Hypotension ** Renal Impairment * Hyperkalemia Hypotension Renal Impairment Losartan 150 mg (n=1912) Losartan 50 mg (n=1905) Konstam MA et al, Lancet 2009; 374:
28 Mineralocorticoid-antagonists and Hyperkalemia How frequent? How to predict? How to prevent? How to manage?
29 Risk Factors for Hyperkalemia Stepwise logistic regression identified 3 independent risk factors for K : Baseline K + Baseline creatinine clearance History of diabetes None was associated with a significant differential adverse effect of intervention vs. placebo for outcome
30 EMPHASIS - Cumulative rate of Worsening Renal Function (egfr> 20% decrease) without hyperkalemia (K>5.5 mmol/l) (%) HR [95% CI] = [1.044, 1.422] P = Eplerenone Placebo Months from Randomization
31 EMPHASIS Cumulative rate Hyperkalemia (K>5.5 mmol/l) With WRF without WRF (egfr> 20% decrease) (egfr> 20% decrease) 15 HR [95% CI] = [1.065, 2.094] P = Eplerenone 15 HR [95% CI] = [1.287, 2.996] P = Eplerenone Placebo 5 5 Placebo Months from Randomization Months from Randomization
32 EMPHASIS Prognostic significance of Hyperkalemia, mainly driven by assocition with worsening renal function (CV death/or HF hosp) HR CI P K>5.5 mmol/l (without egfr> 20% decrease) K>5.5 mmol/l (with egfr> 20% decrease)
33 Approach to Patients at Risk for Hyperkalemia Caused by RAAS Inhibitors 1. Estimate egfr 1. use low dose if < 60 ml/min 2. Do not use if egfr >30ml/min 2. Discontinue drugs that interfere with renal K secretion 3. Inquire about and discontinue use of herbal preparations, and NSAIDs including selective COX2 inhibitors 4. Prescribe low-potassium diet, inquire about use of salt substitutes that contain potassium 5. Prescribe thiazide or loop diuretics (loop diuretics necessary when estimated glomerular filtration rate is <30 ml/min) 6. Monitor K+ and egfr and optimise dosing
34 Mineralocorticoid-antagonists and Hyperkalemia How frequent? How to predict? How to prevent? How to manage?
35 K recommendations Do not initiate if K > 5.0 Evaluate K after initiation at 1 Week, 1 month and then every 4 months. Half the dose if K is 5.5 to 5.9 mmol/l Withhold drug if K> 6.0 mmol/l Remeasure K within 72 hours after dose reduction or drug withdrawal Restart only if K < 5.0 mmol per liter.
 4.7% absolute decrease P < 0.001 Hypokalemia (K + 3.")
36 Some potassium sparing may be beneficial? Patients 8 1.6% absolute increase Eplerenone (%) P = Placebo Serious Hyperkalemia (K meq/l) 4.7% absolute decrease P < Hypokalemia (K meq/l)
37 Conclusions on Hyperkalemia in RAAS Inhibition The fear of inducing hyperkalemia should not limit the initiation or increase in dose of ACE-Is, ARBs, DRIs and Aldosterone Blockers in patients with HF The risk of hyperkalemia is mainly driven by worsening renal function Hyperkalemia is predictable, preventable and manageable Beneficial effects of RAAS inhibition override adverse effects
38 Spironolactone or Eplerenone? The level of evidence Risk/benefit Differing pharmacokinetics Differing pharmacodynamics
39 Main features of MRA major trials Drug Dates Concomitant Beta Blockers RALES EPHESUS EMPHASIS-HF Spironolactone 1999 Eplerenone 2003 Eplerenone % 75% 86.9% N Pts ICD/CRT-D None /8.8% LVEF 25% 33% 26% NYHA III-IV NA II One year Mortality (Pcb) 27.3% 13.7% 7.1% Drug dose Spiro mg Eple mg Eple mg RR All cause death 0.70 ( ) <0.001 RR HF Hospital 0.65 ( ) < ( ) ( ) (0.62, 0.93) (0.47, 0.70) <0.0001
40 Comparative Pharmacokinetics of Eplerenone and Spironolactone Bioavailability Spironolactone ordinarily 60% 70% enhanced by food intake by almost 100% Eplerenone Unknown. Absorption approaches 100% and is not influenced by food Protein Binding >90% 50% with binding to 1 -acid glycoproteins Active Metabolites Half-life (hours) Yes sulfur-containing products Spironolactone = 1.4 Active metabolites = No 4 6
 Eplerenone monotherapy (N=1748) Maximum Potassium 6.")
41 Patients (%) Hyperkalemia in Phase III HTN Database Excluding Study-021 (Diabetics with Proteinuria) Maximum Potassium >5.5 mmol/l Verified Potassium >5.5 mmol/l Spironolactone (N=119) Eplerenone monotherapy (N=1748) Maximum Potassium 6.0 mmol/l Note: Includes studies 010, 015, 016, 017, 018, 019, 020, 021, 022, 023, 024, 026, and 049
42 Spironolactone Induces Gynecomastia in HF Patients vs. No excess Gynecomastia with Eplerenone over Placebo 15 P < Gynecomastia or Breast Pain (Males) (%) Placebo Spironolactone Pitt B et al. N Engl J Med. 1999;341:



43 Spironolactone Spironolactone The but rise not in HbA1c but not was eplerneone correlated to eplerneone raised worsened the rise in HbA1c Cortisol Cortisol Am Heart J 2010;160:
44 Ach Control Spironolactone No Ach Diabetologia (2004) 47:

45
46 Do you believe in class effect? Felis Catus Felis Catus Felis rufus Panthera leo Panthera pardus Panthera tigris
Faiez Zannad. Institut Lorrain du Coeur et des Vaisseaux. CIC - Inserm
 Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Faiez Zannad Institut Lorrain du Coeur et des Vaisseaux CIC - Inserm Disclosure Faiez Zannad Grants BG Medicine, Roche Diagnostics. Consultant/Steering committees/event committees/ Data safety Monitoring
Aldosterone Antagonism in Heart Failure: Now for all Patients?
 Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Aldosterone Antagonism in Heart Failure: Now for all Patients? Inder Anand, MD, FRCP, D Phil (Oxon.) Professor of Medicine, University of Minnesota, Director Heart Failure Program, VA Medical Center 111C
Combination of renin-angiotensinaldosterone. how to choose?
 Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Combination of renin-angiotensinaldosterone system inhibitors how to choose? Karl Swedberg Professor of Medicine Sahlgrenska Academy University of Gothenburg karl.swedberg@gu.se Disclosures Research grants
Drugs acting on the reninangiotensin-aldosterone
 Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Drugs acting on the reninangiotensin-aldosterone system John McMurray Eugene Braunwald Scholar in Cardiovascular Diseases, Brigham and Women s Hospital, Boston & Visiting Professor, Harvard Medical School
Update on pharmacological treatment of heart failure. Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy
 Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Update on pharmacological treatment of heart failure Aldo Pietro Maggioni, MD, FESC ANMCO Research Center Firenze, Italy Presenter Disclosures Dr. Maggioni : Serving in Committees of studies sponsored
Optimal blockade of the Renin- Angiotensin-Aldosterone. in chronic heart failure
 Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Optimal blockade of the Renin- Angiotensin-Aldosterone Aldosterone- (RAA)-System in chronic heart failure Jan Östergren Department of Medicine Karolinska University Hospital Stockholm, Sweden Key Issues
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials -
 Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Understanding and Development of New Therapies for Heart Failure - Lessons from Recent Clinical Trials - Clinical trials Evidence-based medicine, clinical practice Impact upon Understanding pathophysiology
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE
 Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
Position Statement on ALDOSTERONE ANTAGONIST THERAPY IN CHRONIC HEART FAILURE Over 8,000 patients have been studied in two well-designed placebo-controlled outcome-driven clinical trials to evaluate the
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
DECLARATION OF CONFLICT OF INTEREST Novel approaches in hypertension Aldosterone-synthase inhibitors. Faiez Zannad Nancy, France Disclosures Dr Zannad reports receiving Speaker/consultant honoraria from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR
 ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
ESC Guidelines for diagnosis and management of HF 2012: What s new? John Parissis, MD Athens, GR Disclosures ALARM INVESTIGATOR RESEARCH GRANTS BY ABBOTT USA AND ORION PHARMA The principal changes from
heart failure John McMurray University of Glasgow.
 A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
A to Z of RAAS blockade in heart failure John McMurray BHF Cardiovascular Research Centre University of Glasgow. RAAS inhibition in CHF ACE inhibition in patients with low LVEF CHF CONSENSUS Enalapril
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists
 I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
I know the trials in heart failure but how do I manage my patient? Dosing of neurohormones antagonists Alessandro Fucili (Ferrara, IT) Massimo F Piepoli (Piacenza, IT) Clinical Case: 82 year old woman
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd
 SMC No. (793/12) Pfizer Ltd") eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
eplerenone 25, 50mg film-coated tablets (Inspra ) SMC No. (793/12) Pfizer Ltd 08 June 2012 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises NHS Boards
Disclosures for Presenter
 A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
A Comparison of Angiotensin Receptor- Neprilysin Inhibition (ARNI) With ACE Inhibition in the Long-Term Treatment of Chronic Heart Failure With a Reduced Ejection Fraction Milton Packer, John J.V. McMurray,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care
 Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Satish K Surabhi, MD.FACC,FSCAI,RPVI Medical Director, Cardiac Cath Labs AnMed Health Heart & Vascular Care None Fig. 1. Progression of Heart Failure.With each hospitalization for acute heart failure,
Beyond ACE-inhibitors for Heart Failure. Jacob Townsend, MD NCVH Birmingham 2015
 Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Beyond ACE-inhibitors for Heart Failure Jacob Townsend, MD NCVH Birmingham 2015 % Decrease in Mortality Current Therapy HFrEF 0% Angiotensin receptor blocker ACE inhibitor Beta blocker Mineralocorticoid
Heart Failure: Combination Treatment Strategies
 Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Heart Failure: Combination Treatment Strategies M. McDonald MD, FRCP State of the Heart Symposium May 28, 2011 None Disclosures Case 69 F, prior MIs (LV ejection fraction 25%), HTN No demonstrable ischemia
Antialdosterone treatment in heart failure
 Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
Update on the Treatment of Chronic Heart Failure 2012 Antialdosterone treatment in heart failure 전남의대윤현주 Chronic Heart Failure Prognosis of Heart failure Cecil, Text book of Internal Medicine, 22 th edition
A patient with decompensated HF
 A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
A patient with decompensated HF Professor Michel KOMAJDA University Pierre & Marie Curie Pitie Salpetriere Hospital Department of Cardiology Paris (France) Declaration Of Interest 2010 Speaker : Servier,
HFpEF, Mito or Realidad?
 HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
HFpEF, Mito or Realidad? Ileana L. Piña, MD, MPH Professor of Medicine and Epidemiology/Population Health Associate Chief for Academic Affairs -- Cardiology Montefiore-Einstein Medical Center Bronx, NY
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure
 ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
ESC Guidelines for the Diagnosis and Treatment of Chronic Heart Failure - 2005 Karl Swedberg Professor of Medicine Department of Medicine Sahlgrenska University Hospital/Östra Göteborg University Göteborg
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF?
 New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
New Agents for Treating Hyperkalemia - Can They Help Us Improve Outcomes in HF? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg
ACE inhibitors: still the gold standard?
 ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
ACE inhibitors: still the gold standard? Session: Twenty-five years after CONSENSUS What have we learnt about the RAAS in heart failure? Lars Køber, MD, D.Sci Department of Cardiology Rigshospitalet University
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD
 CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
CT Academy of Family Physicians Scientific Symposium October 2012 Amit Pursnani, MD Clinical syndrome resulting from a structural or functional cardiac disorder that impairs the ability of the heart to
Influence of Baseline and Worsening Renal Function on Efficacy of Spironolactone in Patients With Severe Heart Failure
 Journal of the American College of Cardiology Vol. 60, No. 20, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.07.048
Journal of the American College of Cardiology Vol. 60, No. 20, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. http://dx.doi.org/10.1016/j.jacc.2012.07.048
Highlight Session Heart failure and cardiomyopathies Michel KOMAJDA Paris France
 Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
Highlight Session 2014 Heart failure and cardiomyopathies Michel KOMAJDA Paris France # esccongress www.escardio.org/esc2014 HEART FAILURE AND CARDIOMYOPATHIES TOPIC 1 Drug Therapy TOPIC 2 Device Therapy
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition
 New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
New Paradigms in Rx of Symptomati Heart Failure:Role of Ivabradine & Angiotensin Neprilysin Inhibition Prakash Deedwania, MD, FACC, FACP, FCCP, FAHA Professor of Medicine, UCSF School of Medicine, Director,
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists
 Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Optimizing CHF Therapy: The Role of Digoxin, Diuretics, and Aldosterone Antagonists Old Drugs for an Old Problem Jay Geoghagan, MD, FACC BHHI Primary Care Symposium February 28, 2014 None. Financial disclosures
Treating HF Patients with ARNI s Why, When and How?
 Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Treating HF Patients with ARNI s Why, When and How? 19 th Annual San Diego Heart Failure Symposium for Primary Care Physicians January 11-12, 2019 La Jolla, CA Barry Greenberg M.D. Distinguished Professor
Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece
 Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece Disclosures Grants: ALARM investigator received research grants
Medical management of LV aneurysm and subsequent cardiac remodeling: is it enough? J. Parissis Attikon University Hospital Athens, Greece Disclosures Grants: ALARM investigator received research grants
Beta-blockers in heart failure: evidence put into practice
 Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Beta-blockers in heart failure: evidence put into practice John McMurray Professor of Medical Cardiology, University of Glasgow & Consultant Cardiologist,Western Infirmary, Glasgow, UK Eugene Braunwald
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 4 2 3.5 4. 1. 1991 21 237 US prevalence*: 5. million US annual incidence: 7, Annual mortality: 22,754 5-1% depending on severity Cost:
Heart Failure Update. Michael Fu. Professor, Överläkare
 Heart Failure Update Michael Fu Professor, Överläkare Update in Diagnosis Update in Pharmacological Treatment Update in Device Therapy Heart Failure in the Elderly Put Guidelines into Clinical Practice
Heart Failure Update Michael Fu Professor, Överläkare Update in Diagnosis Update in Pharmacological Treatment Update in Device Therapy Heart Failure in the Elderly Put Guidelines into Clinical Practice
Review Article. Pharmacotherapy of Heart Failure with Reduced LVEF. Sachin Mukhedkar, Ajit Bhagwat
 Review Article Vidarbha Journal of Internal Medicine Volume 22 January 2017 Pharmacotherapy of Heart Failure with Reduced LVEF 1 2 Sachin Mukhedkar, Ajit Bhagwat ABSTRACT Heart failure with reduced ejection
Review Article Vidarbha Journal of Internal Medicine Volume 22 January 2017 Pharmacotherapy of Heart Failure with Reduced LVEF 1 2 Sachin Mukhedkar, Ajit Bhagwat ABSTRACT Heart failure with reduced ejection
ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure
 Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Patients t with acute heart failure frequently develop chronic heart failure Patients with chronic heart failure frequently decompensate acutely ESC Guidelines for the Diagnosis and A clinical response
Disclosures. Advances in Chronic Heart Failure Management 6/12/2017. Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017
 Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
Advances in Chronic Heart Failure Management Van N Selby, MD UCSF Advanced Heart Failure Program June 19, 2017 I have nothing to disclose Disclosures 1 Goal statement To review recently-approved therapies
LITERATURE REVIEW: HEART FAILURE. Chief Residents
 LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
LITERATURE REVIEW: HEART FAILURE Chief Residents Heart Failure EF 40% HFrEF Problem with contractility EF 40-50% HFmrEF EF > 50% HFpEF Problem with filling/relaxation RISK FACTORS Post MI HTN DM Obesity
Disclosures. Overview. Goal statement. Advances in Chronic Heart Failure Management 5/22/17
 Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
Disclosures Advances in Chronic Heart Failure Management I have nothing to disclose Van N Selby, MD UCSF Advanced Heart Failure Program May 22, 2017 Goal statement To review recently-approved therapies
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital
 What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
What s New in Heart Failure? Marie-France Gauthier, BSc, PharmD, ACPR Clinical Pharmacist at Montfort Hospital Disclosures I have no current or past relationships with commercial entities Learning objectives
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC
 2016: ACC / AHA and ESC") Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Updates in Heart Failure (HF) 2016: ACC / AHA and ESC Patrick McBride, MD, MPH Professor of Medicine & Family Medicine, UW School of Medicine and Public Health Special thanks to: Clyde W. Yancy, MD, MSc
Checklist for Treating Heart Failure. Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute
 Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Checklist for Treating Heart Failure Alan M. Kaneshige MD, FACC, FASE Oklahoma Heart Institute Novartis Disclosure Heart Failure (HF) a complex clinical syndrome that arises secondary to abnormalities
Akash Ghai MD, FACC February 27, No Disclosures
 Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Akash Ghai MD, FACC February 27, 2015 No Disclosures Epidemiology Lifetime risk is > 20% for American s older than 40 years old. > 650,000 new cases diagnosed each year. Incidence increases with age: 2%
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion
 Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
Behandlungsalgorithmus bei Herzinsuffizienz mit reduzierter Auswurffraktion Professor Dr. med. Roger Hullin Leiter Programm für Schwere Herzinsuffizienz, VAD & Herztransplantation Suisse Romande Klinik
n engl j med 364;1 nejm.org january 6,
 The new england journal of medicine established in 1812 january 6, 2011 vol. 364 no. 1 in Patients with Systolic Heart Failure and Mild Symptoms Faiez Zannad, M.D., Ph.D., John J.V. McMurray, M.D., Henry
The new england journal of medicine established in 1812 january 6, 2011 vol. 364 no. 1 in Patients with Systolic Heart Failure and Mild Symptoms Faiez Zannad, M.D., Ph.D., John J.V. McMurray, M.D., Henry
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC
 Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Sacubitril/Valsartan in HFrEF for All Protagonist View George Honos MD FRCPC FCCS FACC Head of Cardiology Medical Manager / CV Program CHUM Disclosure Statement Within the past two years: I have had an
Dr. Khairy Abdel Dayem. Professor of Cardiology Ain-Shams University
 Dr. Khairy Abdel Dayem Professor of Cardiology Ain-Shams University RALES Randomized Aldactone Evaluation Study 1. NEJM 1999 2. Bertram Pitt 3. 1660 Class III and IV HF patients 4. EF 35% 5. 841 placebo
Dr. Khairy Abdel Dayem Professor of Cardiology Ain-Shams University RALES Randomized Aldactone Evaluation Study 1. NEJM 1999 2. Bertram Pitt 3. 1660 Class III and IV HF patients 4. EF 35% 5. 841 placebo
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Saudi Arabia February Pr Michel KOMAJDA. Université Pierre et Marie Curie Hospital Pitié Salpétrière
 Prevention of Cardiovascular events with Ivabradine: The SHIFT Study Saudi Arabia February 2011 Pr Michel KOMAJDA Université Pierre et Marie Curie Hospital Pitié Salpétrière Paris FRANCE Declaration Of
Prevention of Cardiovascular events with Ivabradine: The SHIFT Study Saudi Arabia February 2011 Pr Michel KOMAJDA Université Pierre et Marie Curie Hospital Pitié Salpétrière Paris FRANCE Declaration Of
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than cancer") Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
Patients in US (millions) Heart Failure (HF): Scope of the Problem 1 8 6 4 2 3.5 4.8 1. 1991 21 237 US prevalence*: 5.8 million US annual incidence: 67, Annual mortality: 282,754 5-1% depending on severity
Heart Failure Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital
 Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
Heart Failure 2012 Dr Eric Klug Sunninghill, Sunward Park, CM Johannesburg Academic Hospital PRELOAD COWS Reduction in milk production INOTROPY & HEART RATE AFTERLOAD DISTRIBUTION NETWORK THE CLASSIC APPROACH
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ
 ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ Aldosterone is a mineralocorticoid hormone synthesized by the adrenal glands that has several regulatory
ΚΑΡΔΙΑΚΗ ΑΝΕΠΑΡΚΕΙΑ ΚΑΙ ΑΝΤΑΓΩΝΙΣΤΕΣ ΑΛΔΟΣΤΕΡΟΝΗΣ ΣΠΥΡΟΜΗΤΡΟΣ ΓΕΩΡΓΙΟΣ MD, FESC. E.Α Κ/Δ Γ.Ν.ΚΑΤΕΡΙΝΗΣ Aldosterone is a mineralocorticoid hormone synthesized by the adrenal glands that has several regulatory
AHA Nov 18, 2013 Late Breaking Session
 Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2013 Late Breaking Session Marc A. Pfeffer MD, PhD, on behalf of the TOPCAT Investigators TOPCAT
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2013 Late Breaking Session Marc A. Pfeffer MD, PhD, on behalf of the TOPCAT Investigators TOPCAT
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update)
") Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Chronic heart failure: management of chronic heart failure in adults in primary and secondary care (partial update) NICE guideline Apendix C The algorithms Draft for consultation, January 2010 Chronic
Heart Failure New Drugs- Updated Guidelines
 Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Heart Failure New Drugs- Updated Guidelines Eileen Handberg, PhD, ANP-BC, FAHA, FACC Professor of Medicine Division of Cardiovascular Medicine University of Florida Disclosures 1. 3 2. 6 3. 8 4. 11 Dunlay
Learning Objectives. Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis") 7:5 :5 am Update in Heart Failure SPEAKER Orly Vardeny, PharmD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Orly Vardeny, PharmD, MS: Advisory Board
7:5 :5 am Update in Heart Failure SPEAKER Orly Vardeny, PharmD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Orly Vardeny, PharmD, MS: Advisory Board
Contemporary Advanced Heart Failure Therapy
 Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
Contemporary Advanced Heart Failure Therapy Andrew Boyle, MD Professor of Medicine Medical Director of Advanced Heart Failure Thomas Jefferson University Philadelphia, PA Audience Response Question 40
The Hearth Rate modulators. How to optimise treatment
 The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
The Hearth Rate modulators How to optimise treatment Munich, ESC Congress 2012 Prof. Luigi Tavazzi GVM Care&Research E.S. Health Science Foundation Cotignola, IT Disclosure Cooperation with: Servier, Medtronic,
Outline. Classification by LVEF Conventional Therapy New Therapies. Ivabradine Sacubitril/valsartan
 New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
New Pharmacological Therapies for Heart Failure Mark Drazner, MD, MSc Clinical Chief of Cardiology Medical Director, CHF/VAD/Transplant James M. Wooten Chair in Cardiology UT Southwestern Medical Center
Heart Failure (HF): Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers
: Scope of the Problem. Temporal Trends in Age-Adjusted Survival After HF Diagnosis. More malignant than most cancers") Evidence-Based Approaches to the Management of Heart Failure: Reducing Hospitalization and Improving Patient Outcomes Eldrin F. Lewis, MD, MPH Director of Cardiovascular Clerkship Brigham and Women s Hospital
Evidence-Based Approaches to the Management of Heart Failure: Reducing Hospitalization and Improving Patient Outcomes Eldrin F. Lewis, MD, MPH Director of Cardiovascular Clerkship Brigham and Women s Hospital
Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial
 Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial Aldo P. Maggioni, MD, FESC Associazione Nazionale Medici
Effect of Aliskiren on Postdischarge Outcomes Among Non-Diabetic Patients Hospitalized for Heart Failure: Insights from the ASTRONAUT Outcomes Trial Aldo P. Maggioni, MD, FESC Associazione Nazionale Medici
Heart Failure Clinician Guide JANUARY 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2018 Introduction This evidence-based guideline summary is based on the 2018 National Heart Failure Guideline.
Scientific conclusions and detailed explanation of the scientific grounds for the differences from the PRAC recommendation
 Annex I Scientific conclusions, grounds for variation to the terms of the marketing authorisations and detailed explanation of the scientific grounds for the differences from the PRAC recommendation 1
Annex I Scientific conclusions, grounds for variation to the terms of the marketing authorisations and detailed explanation of the scientific grounds for the differences from the PRAC recommendation 1
When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist?
 When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist? Sripal Bangalore, MD, MHA, Sunil Kumar, MD, Franz H Messerli, MD,
When Conventional Heart Failure Therapy is not Enough: Angiotensin Receptor Blocker, Direct Renin Inhibitor or Aldosterone Antagonist? Sripal Bangalore, MD, MHA, Sunil Kumar, MD, Franz H Messerli, MD,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials
 AHA Nov 18, 2014 Update on Randomized Trials") Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Treatment Of Preserved Cardiac Function Heart Failure with an Aldosterone antagonist (TOPCAT) AHA Nov 18, 2014 Update on Randomized Trials Marc A. Pfeffer, MD, PhD; Brian Claggett, PhD; Susan F. Assmann,
Heart Failure Clinician Guide JANUARY 2016
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Heart Failure Clinician Guide JANUARY 2016 Introduction This evidence-based guideline summary is based on the 2016 National Heart Failure Guideline.
Congestive Heart Failure 2015
 Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
Definition Congestive Heart Failure 215 JP Mehegan/ Mercy Cardiology n Cardiac failure; Congestive heart failure; Chronic heart failure (synonyms) n When the heart is unable to pump sufficiently and at
INSPRA 25 & 50 mg TABLETS
 INSPRA 25 & 50 mg TABLETS SCHEDULING STATUS: Schedule 4 PROPRIETARY NAMES (and dosage forms): INSPRA 25 (Tablets) INSPRA 50 (Tablets) COMPOSITION: INSPRA 25: INSPRA 50: Each tablet contains 25 mg eplerenone
INSPRA 25 & 50 mg TABLETS SCHEDULING STATUS: Schedule 4 PROPRIETARY NAMES (and dosage forms): INSPRA 25 (Tablets) INSPRA 50 (Tablets) COMPOSITION: INSPRA 25: INSPRA 50: Each tablet contains 25 mg eplerenone
Combination Therapy with Aldosterone Blockade and Renin-Angiotensin Inhibitors Confers Organ Protection
 211 Review Hypertens Res Vol.29 (2006) No.4 p.211-216 Combination Therapy with Aldosterone Blockade and Renin-Angiotensin Inhibitors Confers Organ Protection Atsuhisa SATO 1), Takao SARUTA 2), and John
211 Review Hypertens Res Vol.29 (2006) No.4 p.211-216 Combination Therapy with Aldosterone Blockade and Renin-Angiotensin Inhibitors Confers Organ Protection Atsuhisa SATO 1), Takao SARUTA 2), and John
Therapeutic Targets and Interventions
 Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
Therapeutic Targets and Interventions Ali Valika, MD, FACC Advanced Heart Failure and Pulmonary Hypertension Advocate Medical Group Midwest Heart Foundation Disclosures: 1. Novartis: Speaker Honorarium
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration
![ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration](/thumbs/77/76069192.jpg "ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication Initiation and Titration") ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
ARNI (Angiotensin Receptor blocker / Neprilysin Inhibitors [Sacubutril/Valsartan]) Heart Failure Medication and Symptomatic HF despite ACEI/ARB and B-blocker therapy Bilateral renal artery stenosis Moderate/Severe
HEART FAILURE SUMMARY. and is associated with significant morbidity and mortality. the cornerstone of heart failure treatment.
 HEART FAILURE SUMMARY + Heart Failure is a condition affecting a large number of Irish people and is associated with significant morbidity and mortality. + ACE inhibitors, in combination with diuretics,
HEART FAILURE SUMMARY + Heart Failure is a condition affecting a large number of Irish people and is associated with significant morbidity and mortality. + ACE inhibitors, in combination with diuretics,
The role of angiotensin II receptor blockers in the management of heart failure
 European Heart Journal Supplements (2005) 7 (Supplement J), J10 J14 doi:10.1093/eurheartj/sui057 The role of angiotensin II receptor blockers in the management of heart failure John J.V. McMurray* Department
European Heart Journal Supplements (2005) 7 (Supplement J), J10 J14 doi:10.1093/eurheartj/sui057 The role of angiotensin II receptor blockers in the management of heart failure John J.V. McMurray* Department
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia
 Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Potassium as a Treatable Biomarker in Cardiovascular Disease: New Keys to Hyperkalemia Nicholas Wettersten, MD Associate Professor Heart Failure, Mechanical Circulatory Support and Transplant March 1 st,
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
LCZ696 A First-in-Class Angiotensin Receptor Neprilysin Inhibitor
 The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
The Angiotensin Receptor Neprilysin Inhibitor LCZ696 in Heart Failure with Preserved Ejection Fraction The Prospective comparison of ARNI with ARB on Management Of heart failure with preserved ejection
Heart Failure (HF) - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF
 - Primary Care Flow Charts. Pre diagnosis Symptoms or signs suggestive of HF") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for
 - Primary Care Flow Charts. Symptoms or signs suggestive of HF. Pre diagnosis. Refer to the Heart Failure Clinic at VHK for") Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Heart Failure (HF) - Primary Care Flow Charts Pre diagnosis Symptoms or signs suggestive of HF 12 lead ECG Normal examination and 12 lead ECG HF highly unlikely Abnormal 12 lead ECG HF Possible Arrange
Why to use digoxin in heart failure?
 Why to use digoxin in heart failure? Yves Juillière, Cardiology, ILCV, CHU Nancy-Brabois, France Digitalis purpurea Representation of the extracellular loops and the transmembrane domain regions of the
Why to use digoxin in heart failure? Yves Juillière, Cardiology, ILCV, CHU Nancy-Brabois, France Digitalis purpurea Representation of the extracellular loops and the transmembrane domain regions of the
Eplerenone and Atrial Fibrillation in Mild Systolic Heart Failure
 Journal of the American College of Cardiology Vol. 59, No. 18, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.11.063
Journal of the American College of Cardiology Vol. 59, No. 18, 2012 2012 by the American College of Cardiology Foundation ISSN 0735-1097/$36.00 Published by Elsevier Inc. doi:10.1016/j.jacc.2011.11.063
keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests
 www.bpac.org.nz keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests Why do we monitor patients taking diuretics and what do we monitor? Monitoring a person on
www.bpac.org.nz keyword: diuretics Drug monitoring Monitoring diuretics in primary care 2 March 2009 best tests Why do we monitor patients taking diuretics and what do we monitor? Monitoring a person on
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure
 Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
Managing the Yin and Yang of Hyperkalemia and MRAs in Heart Failure Barry Greenberg M.D. Distinguished Professor of Medicine Director, Advanced Heart Failure Treatement Program University of California,
2017 Summer MAOFP Update
 2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
2017 Summer MAOFP Update. Cardiology Update 2017 Landmark Trials Change Practice Guidelines David J. Strobl, DO, FNLA Heart Failure: Epidemiology More than 4 million patients affected 400,000 new cases
Mineralocorticoid receptor antagonists (MRAs) have. Original Article
 have. Original Article") Original Article Incidence, Predictors, and Outcomes Related to Hypo- and Hyperkalemia in Patients With Severe Heart Failure Treated With a Mineralocorticoid Receptor Antagonist Orly Vardeny, PharmD, MS;
Original Article Incidence, Predictors, and Outcomes Related to Hypo- and Hyperkalemia in Patients With Severe Heart Failure Treated With a Mineralocorticoid Receptor Antagonist Orly Vardeny, PharmD, MS;
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine
 Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Systolic Dysfunction Clinical /Hemodynamic Guide for Management From Neprilysin Inhibitors to Ivabradine Donna Mancini MD Choudhrie Professor of Cardiology Columbia University Speaker Disclosure Amgen
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred
 Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Implantation of a CRT-Pacemaker Rather than CRT-Defibrillator is Usually Preferred Professor John GF Cleland University of Hull Kingston-upon-Hull United Kingdom Conflict of Interest: Funding or Speakers
Heart Failure Treatments
 Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Heart Failure Treatments Past & Present www.philippelefevre.com Background Background Chronic heart failure Drugs Mechanical Electrical Background Chronic heart failure Drugs Mechanical Electrical Sudden
Congestive Heart Failure: Outpatient Management
 The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
The Chattanooga Heart Institute Cardiovascular Symposium Congestive Heart Failure: Outpatient Management E. Philip Lehman MD, MPP Disclosure No financial disclosures. Objectives Evidence-based therapy
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Management of Heart Failure in Older Adults
 Management of Heart Failure in Older Adults New Data, New Guidelines, New Challenges JOSE NATIVI, MD, MSCI Assistant Professor of Medicine Cardiovascular Director Amyloidosis Program DISCLOSURES - Advisory
Management of Heart Failure in Older Adults New Data, New Guidelines, New Challenges JOSE NATIVI, MD, MSCI Assistant Professor of Medicine Cardiovascular Director Amyloidosis Program DISCLOSURES - Advisory
Monitoring of Renal Function in Heart Failure
 Monitoring of Renal Function in Heart Failure Adriaan A. Voors, cardiologist The Netherlands Disclosures AAV received consultancy fees and/or research grants from: Alere, Bayer, Cardio3Biosciences, Celladon,
Monitoring of Renal Function in Heart Failure Adriaan A. Voors, cardiologist The Netherlands Disclosures AAV received consultancy fees and/or research grants from: Alere, Bayer, Cardio3Biosciences, Celladon,
Terapia Farmacologica della Insufficienza Cardiaca Cronica: è in arrivo una rivoluzione? Gennaro Cice
 Terapia Farmacologica della Insufficienza Cardiaca Cronica: è in arrivo una rivoluzione? Gennaro Cice Cattedra di Cardiologia Seconda Università di Napoli 60 CONGRESSO NAZIONALE SIGG NAPOLI, 25-28 NOVEMBRE
Terapia Farmacologica della Insufficienza Cardiaca Cronica: è in arrivo una rivoluzione? Gennaro Cice Cattedra di Cardiologia Seconda Università di Napoli 60 CONGRESSO NAZIONALE SIGG NAPOLI, 25-28 NOVEMBRE
From PARADIGM-HF to Clinical Practice. Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group
 From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
From PARADIGM-HF to Clinical Practice Waleed AlHabeeb, MD, MHA Associate Professor of Medicine President of the Saudi Heart Failure Group PARADIGM-HF: Inclusion Criteria Chronic HF NYHA FC II IV with LVEF
Management of chronic heart failure: update J. Parissis Attikon University Hospital
 Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Management of chronic heart failure: update 2015 J. Parissis Attikon University Hospital Disclosures: received honoraria for lectures from Servier, Pfizer, Novartis Discharges in Thousands Heart Failure
Summary/Key Points Introduction
 Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
Summary/Key Points Introduction Scope of Heart Failure (HF) o 6.5 million Americans 20 years of age have HF o 960,000 new cases of HF diagnosed annually o 5-year survival rate for HF is ~50% Classification
TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018
 Iseo 10 Novembre 2018") TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018 Carlo Lombardi Cattedra di Cardiologia Università e Spedali Civili di Brescia All-cause mortality in the European
TERAPIA DELLO SCOMPENSO DAI BETA- BLOCCANTI AGLI ARNI (ARNI SI ARNI NO) Iseo 10 Novembre 2018 Carlo Lombardi Cattedra di Cardiologia Università e Spedali Civili di Brescia All-cause mortality in the European
Heart Failure Background, recognition, diagnosis and management
 Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of heart failure
Heart Failure A Team Approach Background, recognition, diagnosis and management
 Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
Heart Failure A Team Approach Background, recognition, diagnosis and management Speaker bureau: Novartis At the conclusion of this activity, participants will be able to: Recognize signs and symptoms of
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Cardiovascular Pharmacotherapy for Heart Failure Management
 Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,
Cardiovascular Pharmacotherapy for Heart Failure Management AN UPDATE OF THE LATEST RECOMMENDATIONS AND DATA By: Debby Caraballo, PharmD, PhC, BCPS, AQ-Cardiology Balloon Fiesta Symposium, Albuquerque,