Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine
|
|
|
- Douglas August Ford
- 6 years ago
- Views:
Transcription



1 Gegia Chapter of the American Association of Clinical Endocrinologists, 2017 Annual Meeting January 28, 2017 Silvio E. Inzucchi MD Section of Endocrinology Yale School of Medicine
2 DIABETES MANAGEMENT GUIDELINES 1. Pathophysiologicallybased therapeutic options in T2DM 2. ADA-EASD Statements 3. AACE & Other Guidelines 4. Considerations in Choosing Drugs 5. A Look to the Future
3 Multiple Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption - - pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? hepatic glucose production renal glucose excretion peripheral glucose uptake Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011
4 Multiple Pathophysiologically-Based Therapies f T2DM GLP-1R agonists incretin effect DPP-4 inhibits gut A G I s carbohydrate delivery & absption Glinides Amylin mimetics - Insulin S U s pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA DA agonists? Metfmin T Z D s Bile acid sequestrants hepatic glucose production SGLT-2 inhibits renal glucose excretion - peripheral glucose uptake Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011


5 GLP-1R agonists DPP-4 inhibits incretin enhancers Insulin S U s insulin providers Metfmin insulin sensitizers T Z D s SGLT-2 inhibits glucose excreter
6 Classes Generic Names A1c Sideeffects Insulin Degludec,Glargine, Detemir, NPH, Regular, Lispro, Aspart, Glulisine No limit Hypo,weight gain, injections SU s Glyburide, Glipizide, Glimepiride 1-1.5% Hypo, weight gain Metfmin Metfmin 1-1.5% GI,lactic acidosis, B-12 deficiency TZD s Rosiglitazone,Pioglitazone 1-1.5% Weightgain, edema, HF, bone fx s,?bladder ca DPP-4 i s Sitagliptin, Saxagliptin, Alogliptin, Linagliptin 0.5-1% Urticaria,?pancreatitis GLP-1 RA s Exenatide, Liraglutide, Albiglutide, Dulaglutide, Lixisenatide SGLT2-i s Canagliflozin,Dapagliflozin, Empagliflozin 1-1.5% GI,?pancreatic disease, injections 0.5-1% Polyuria, GUinfections, DKA,?bone fxs
7 Classes Generic Names A1c Costs Insulin Degludec,Glargine, Detemir, NPH, Regular, Lispro, Aspart, Glulisine No limit variable SU s Glyburide, Glipizide, Glimepiride 1-1.5% $ Metfmin Metfmin 1-1.5% $ TZD s Rosiglitazone, Pioglitazone 1-1.5% $ - $$$ DPP-4 i s Sitagliptin, Saxagliptin, Alogliptin, Linagliptin 0.5-1% $$$$ GLP-1 RA s Exenatide, Liraglutide, Albiglutide, Dulaglutide, Lixisenatide 1-1.5% $$$$ SGLT2-i s Canagliflozin,Dapagliflozin, Empagliflozin 0.5-1% $$$$
8 Half-Century of HTN & T2DM Medications in U.S. Number of Medication Classes zz zz adrenergic neuronal blockers peripheral α-1 blockers β-blockers central α-2 agonists diuretics Biguanides Ca 2 channel blockers Angiotensin II recept blockers ACE Inhibits SGLT-2 inhibits Dopamine agonists Renin inhibits TZDs α-gis Biguanides Glinides Bile acid sequestrants DPP-4 inhibits Amylin mimetics GLP-1R Agonists insulin 2 1 vasodilats Sulfonylureas Adapted from: Inzucchi SE. Comparing and Choosing Oral Agents, in Clinical Diabetes, Fonseca VA, WB Saunders,




9











10 Type 2 DM Management Guidelines




11

12 Guideline vs. guideline Clinical Practice Guidelines statements that include recommendations intended to optimize patient care... infmed by a systematic review of evidence and an assessment of the benefits and harms of care options. multidisciplinary expert panel systematic review rate quality of evidence and strength of recommendations transparent process to minimize biases and COI s consider patient subgroups and patient preferences discuss alternative care options revised when new infmation available guideline noun guide line \ˈgīd-ˌlīn\ Definition: a rule instruction that shows tells how something should be done
13 DIABETES MANAGEMENT GUIDELINES 1. Pathophysiologicallybased therapeutic options in T2DM 2. ADA-EASD Statements 3. AACE & Other Guidelines 4. Considerations in Choosing Drugs 5. A Look to the Future
14 American Diabetes Assoc(ADA) -European Assocf the Study of Diabetes (EASD): 2006 Consensus Statement Diagnosis Lifestyle interventions metfmin No A1C 7% Yes* Add basal insulin - most effective Add sulfonylurea - least expensive Add glitazone - no hypoglycemia No A1C 7% No A1C 7% No A1C 7% Yes* Yes* Yes* Intensify insulin Add glitazone Add basal insulin Add sulfonylurea No A1C 7% Yes* No A1C 7% Yes* Add basal intensify insulin * Check A1C every 3 months until < 7% and then at least every 6 months. Although 3 al agents can be used, initiation and intensification of insulin therapy is preferred based on effectiveness and expense. Intensive insulin metfmin ± glitazone Nathan DM, et al. Diabetes Care. 2006;29:
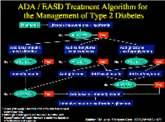
15 ADA -EASD Consensus Statement (2008) STEP 1 STEP 2 STEP 3 Tier 1: Well-validated therapies At Diagnosis: Lifestyle Metfmin Lifestyle Metfmin Basal Insulin Lifestyle Metfmin Sulfonylurea a Lifestyle Metfmin Intensive Insulin Tier 2: Less well-validated therapies Lifestyle Metfmin Pioglitazone Lifestyle Metfmin Pioglitazone Sulfonylurea a Lifestyle Metfmin GLP-1 agonist b Lifestyle Metfmin Basal Insulin Reinfce lifestyle changes at every visit and check A1C every 3 months until < 7.0%, then at least every 6 months thereafter. Change interventions whenever A1C 7.0%. a Sulfonylureas other than glibenclamide (glyburide) chlpropamide. b Insufficient clinical use to be confident regarding safety. Nathan DM, et al. Diabetes Care. 2008;31:1
16 2012 ADA-EASD Position Statement : Management of Hyperglycemia in T2DM: A Patient-Centered Approach GLUCOSE-LOWERING THERAPY Glycemic targets - HbA1c < 7.0% (mean PG mg/dl [ mmol/l]) - Pre-prandial PG <130 mg/dl (7.2 mmol/l) - Post-prandial PG <180 mg/dl (10.0 mmol/l) - Individualization is key: PG = plasma glucose Tighter targets ( %) - younger, healthier Looser targets ( %) -older, combidities, hypoglycemia prone, etc. Pharmacological options - Individualize drug choice - Minimize adverse effects, especially hypoglycemia - Patient-centered care Diabetes Care 2012;35: Diabetologia 2012;55:



17 Figure 1 Diabetes Care 2012;35: Diabetologia 2012;55:
18 Clinical Assessment of Individualized Glycemic Goals in T2DM: Fmulation of an Algithm Based on a Survey Among Leading Wldwide Diabetologists. 9.0% 8.5% Recommended HbA1c 8.0% 7.5% 7.0% 6.5% 6.0% 5.5% 5.0% Vignette 1 Vignette 2 Vignette 3 Vignette 4 Vignette 5 Vignette 6 Cahn A et al. Diabetes Care 2015;38: N=57 global diabetes experts




19 Diabetes Care 2012;35: Diabetologia 2012;55: ADA-EASD Position Statement


20
21 Figure 1. Modulating intensiveness of A1c lowering in T2DM PATIENT / DISEASE FEATURES Risks potentially associated with hypoglycemia and other drug adverse effects me stringent low Approach to the management of hyperglycemia HbA1c 7% less stringent Disease duration newly diagnosed long-standing Life expectancy long sht Usually not modifiable Imptant combidities absent few / mild severe Established vascular complications absent few / mild severe Patient attitude and expected treatment effts ly motivated, adherent, excellent self-care capacities less motivated, non-adherent, po self-care capacities Potentially modifiable Resources and suppt system Readily available limited Diabetes Care 2015;38:140-49; Diabetologia :429-42
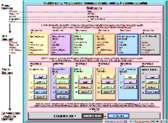
22 Monotherapy Efficacy * Hypo risk Weight Side effects Costs Dual therapy Triple therapy Efficacy * Hypo risk Weight Side effects Costs Healthy eating, weight control, increased physical activity & diabetes education Metfmin low risk neutral/loss GI / lactic acidosis low If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): Metfmin Sulfonylurea moderate risk gain hypoglycemia low Metfmin Sulfonylurea TZD Metfmin low risk gain edema, HF, fxs low Metfmin Thiazolidinedione Thiazolidinedione SU Metfmin DPP-4 inhibit intermediate low risk neutral rare Metfmin Metfmin SGLT2 inhibit intermediate low risk loss GU, dehydration Metfmin GLP-1 recept agonist low risk loss GI If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): DPP-4 Inhibit SU Metfmin SGLT-2 Inhibit SU Metfmin GLP-1 recept agonist SU Metfmin Insulin (basal) est risk gain hypoglycemia variable Metfmin Insulin (basal) TZD DPP-4-i DPP-4-i TZD TZD TZD DPP-4-i SGLT2-i SGLT2-i SGLT2-i DPP-4-i Insulin SGLT2-i 2015 ADA-EASD Position Statement on Management of Hyperglycemia in T2DM Combination injectable therapy GLP-1-RA Insulin GLP-1-RA Insulin Basal Insulin Insulin Insulin GLP-1-RA If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on al combination, move to injectables, (2) on GLP-1 RA, add basal insulin, (3) on optimally titrated basal insulin, add GLP-1-RA mealtime insulin. In refracty patients consider adding TZD SGLT2-i: Metfmin Mealtime Insulin GLP-1-RA Diabetes Care 2015;38: ; Diabetologia 2015;58:


: DPP-4 Inhibit SU Metfmin SGLT-2 Inhibit SU Metfmin GLP-1 recept agonist SU Metfmin Insulin (basal)")
23 Monotherapy Efficacy * Hypo risk Weight Side effects Metfmin Costs intolerance contraindication HbA1c 9% Dual therapy Triple therapy Efficacy * Hypo risk Weight Side effects Costs Healthy eating, weight control, increased physical activity & diabetes education Metfmin low risk neutral/loss GI / lactic acidosis low If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): Metfmin Sulfonylurea moderate risk gain hypoglycemia low Metfmin Sulfonylurea TZD Metfmin low risk gain edema, HF, fxs low Metfmin Thiazolidinedione Thiazolidinedione SU Metfmin DPP-4 inhibit intermediate low risk neutral rare Metfmin Metfmin SGLT2 inhibit intermediate low risk loss GU, dehydration Metfmin GLP-1 recept agonist low risk loss GI If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): DPP-4 Inhibit SU Metfmin SGLT-2 Inhibit SU Metfmin GLP-1 recept agonist SU Metfmin Insulin (basal) est risk gain hypoglycemia variable Metfmin Insulin (basal) TZD DPP-4-i DPP-4-i TZD TZD TZD DPP-4-i Uncontrolled hyperglycemia (catabolic features, BG mg/dl, HbA1c 10-12%) Combination injectable therapy SGLT2-i GLP-1-RA Insulin SGLT2-i GLP-1-RA Insulin Basal Insulin SGLT2-i Insulin DPP-4-i Insulin Insulin SGLT2-i GLP-1-RA If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on al combination, move to injectables, (2) on GLP-1 RA, add basal insulin, (3) on optimally titrated basal insulin, add GLP-1-RA mealtime insulin. In refracty patients consider adding TZD SGLT2-i: Metfmin Mealtime Insulin GLP-1-RA Diabetes Care 2015;38: ; Diabetologia 2015;58:



24 AMERICAN DIABETES ASSOCIATION Standards of Medical Care in Diabetes Diabetes Care 2017;40:S66 Anti-hyperglycemic therapy in T2DM: General recommendations

25 Figure 3. Approach to starting & adjusting insulin in T2DM # Injections 1 Basal Insulin (usually with metfmin /- other non-insulin agent) Start: 10U/day U/kg/day Adjust: 10-15% 2-4 U once-twice weekly to reach FBG target. F hypo: Determine & address cause; dose by 4 units 10-20%. Complexity low 2 Add 1 rapid insulin* injections befe largest meal If not controlled after FBG target is reached ( if dose > 0.5 U/kg/day), treat PPG excursions with meal-time insulin. (Consider initial GLP-1-RA trial.) Change to premixed insulin* twice daily mod. Start: 4U, 0.1 U/kg, 10% basal dose. If A1c<8%, consider basal by same amount. Adjust: dose by 1-2 U 10-15% oncetwice weekly until SMBG target reached. F hypo: Determine and address cause; cresponding dose by 2-4 U 10-20%. Start: Divide current basal dose into 2/3 AM, 1/3 PM 1/2 AM, 1/2 PM. Adjust: dose by 1-2 U 10-15% oncetwice weekly until SMBG target reached. F hypo: Determine and address cause; cresponding dose by 2-4 U 10-20%. 3 If not controlled, consider basalbolus. Add 2 rapid insulin* injections befe meals ('basal-bolus ) If not controlled, consider basalbolus. Start: 4U, 0.1 U/kg, 10% basal dose/meal. If A1c<8%, consider basal by same amount. Adjust: dose by 1-2 U 10-15% once-twice weekly to achieve SMBG target. F hypo: Determine and address cause; cresponding dose by 2-4 U 10-20%. Diabetes Care 2015;38:140; Diabetologia 2015; /s Flexibility me flexible less flexible



26 AMERICAN DIABETES ASSOCIATION Standards of Medical Care in Diabetes Combination injectable therapy f type 2 diabetes Diabetes Care 2017;40:S67
27 DIABETES MANAGEMENT GUIDELINES 1. Pathophysiologicallybased therapeutic options in T2DM 2. ADA-EASD Statements 3. AACE & Other Guidelines 4. Considerations in Choosing Drugs 5. A Look to the Future

28
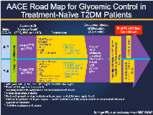
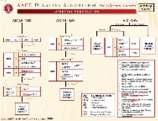
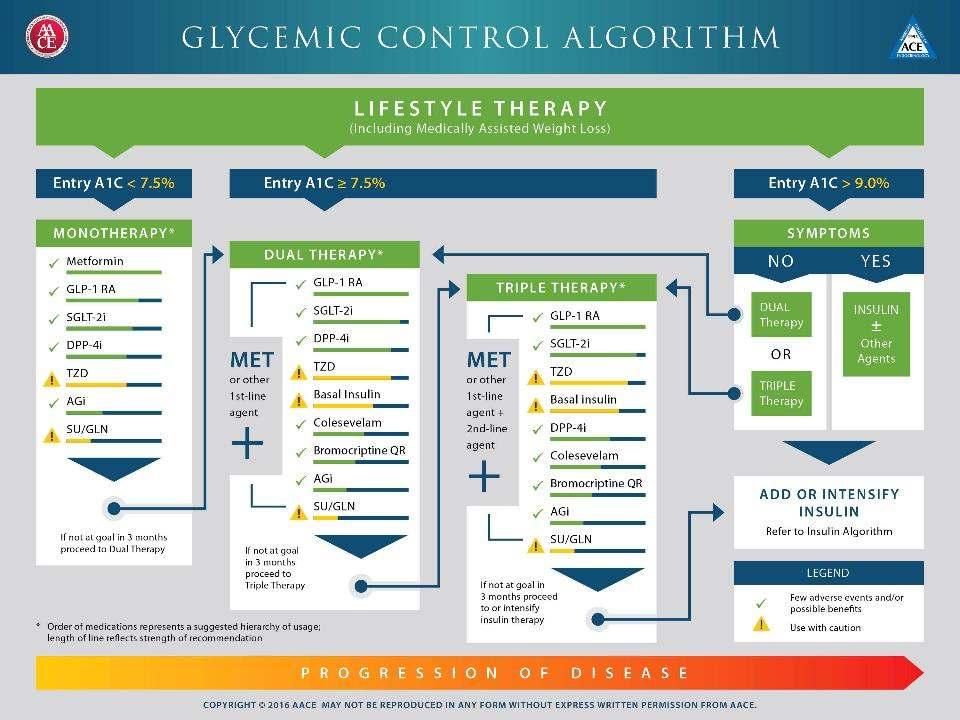
29 DM GUIDELINES: ADA-EASD vs. AACE ADA-EASD AACE Focus Glycemia Comprehensive (CV risk, weight, predm) A1c target <7.0% <6.5% Monotherapy metfmin various Combination therapy Therapeutic A1c A1c 7.5% Me narrow Me broad

30 10_FUL-v4e.pdf




31 Algithm f blood glucose lowering therapy in adults with type 2 diabetes

 failed")

32 Oral Pharmacologic Treatment of T2DM: A Clinical Practice Guideline from the American College of Physicians add als when lifestyle (has) failed monotherapy with metfmin add a second agent Qaseem A et al. Ann Intern Med 2012;156(3):

 failed monotherapy with metfmin")

33 Oral Pharmacologic Treatment of T2DM: A Clinical Practice Guideline Update from the American College of Physicians add als when lifestyle (has) failed monotherapy with metfmin add a second agent Qaseem A et al. Ann Intern Med 2017 [Epub ahead of print 3 January 2017] doi: /M
34 DIABETES MANAGEMENT GUIDELINES 1. Pathophysiologicallybased therapeutic options in T2DM 2. ADA-EASD Statements 3. AACE & Other Guidelines 4. Considerations in Choosing Drugs 5. A Look to the Future
35 6 P sof Personalizingof Diabetes Care 1. Pathophysiology Insulin resistance vs. deficiency? Stage of disease? 2. Potency Distance from A1c target? 3. Precautions 4.Pluses 5.Practicalities 6.Price Side effects, contraindications? (GI, renal, CV) Added benefits beyond glucose control? (weight, BP, CV events) Pills vs. injections? Frequency? Need f BG moniting? Branded vs. generic? Fmulary coverage?
 Sitagliptin 100mg QD Glargine 50U QD (pen) Canagliflozin")
 $733. www.goodrx.")
36 Cost f 30 days of therapy Metfmin 1000mg QD Glipizide 10mg BID Pioglitazone 45mg QD NPH 50U QD (vials) Sitagliptin 100mg QD Glargine 50U QD (pen) Canagliflozin 300mg QD Liraglutide 1.8mg QD $4. $0 $100 $200 $300 $400 $500 $600 $ X (!) $ accessed June 18, 2016, (lowest price f New Haven, CT 06510)
37 DIABETES MANAGEMENT GUIDELINES 1. Pathophysiologicallybased therapeutic options in T2DM 2. ADA-EASD Statements 3. AACE & Other Guidelines 4. Considerations in Choosing Drugs 5. A Look to the Future


38 Pre-marketing Analyses Upper CL of 95% CI <1.8 F a HR= events Post-marketing Analyses Upper CL of 95% CI <1.3 F a HR= events sponss should demonstrate that the therapy will not result in an unacceptable increase in CV risk. Courtesy, Darren McGuire, UTSW Medical Ctr, Hazard Ratio Meta-analysis strategy using Phase 2/3 data Blinded central adjudication of CVD events Inclusion of -risk subjects: advanced CVD, elderly, CKD Minimum exposure of 2 years in large CVOT Approximately 15,000 pt-yrs 1.8
39 Large CV Outcomes Trials in Diabetes (Non-Insulin) Study SAVOR EXAMINE TECOS CAROLINA CARMELINA DPP4-i saxagliptin alogliptin sitagliptin linagliptin linagliptin Comparat placebo placebo placebo sulfonylurea placebo N 16,500 5,400 14,000 6,000 8,300 Results Study LEADER ELIXA SUSTAIN 6 EXSCEL REWIND GLP1-RA liraglutide lixisenatide semaglutide exenatide LR dulaglutide Comparat placebo placebo placebo placebo placebo N 16,500 14,000 6,000 5,400 8,300 Results Study EMPA-REG CANVAS DECLARE NCT SGLT-2-i empaglifozin canagliflozin dapagliflozin ertugliflozin Comparat placebo placebo placebo placebo N , Results
40 New Clinical Trial Data Influencing Treatment Decisions in T2DM 1. EMPA-REG Outcome The SGLT2 inhibit, empagliflozin, d 3-point MACE by 14%, driven by a 38% in CV death in 7020 T2DM patients with overt CVD. Also, 35% in HF hospitalization. 2. IRIS The TZD, pioglitazone, dfatal/non-fatal stroke & MI by 24% (and 52% progression to DM) in 3895 insulin resistant patients with stroke TIA. (Suppts MACE results from 2005 s PROactivestudy.) 3. LEADER The GLP-1 RA, liraglutide, d MACE by 13% in 9340 T2DM patients at CVD risk. (22% CV death and 15% all-cause death.) 4. SUSTAIN 6 The weekly GLP-1 RA, semaglutide, d MACE by 26% in 3297 T2DM patients at CVD risk. ( 61% stroke) Zinman B et al. N Engl J Med 2015;373:2117; Kernan WN et al. N Engl J Med 2016; 374:1321; Marso SP et al. N Engl J Med 2016;375:311; Marso SP et al. N Engl J Med 2016;375:1834


: DPP-4 Inhibit SU Metfmin SGLT-2 Inhibit SU Metfmin GLP-1 recept agonist SU Metfmin Insulin (basal) est risk gain hypoglycemia variable Metfmin Insulin")
41 Monotherapy Efficacy * Hypo risk Weight Side effects Costs Dual therapy Triple therapy Efficacy * Hypo risk Weight Side effects Costs Healthy eating, weight control, increased physical activity & diabetes education Metfmin low risk neutral/loss GI / lactic acidosis low If HbA1c target not achieved after ~3 months of monotherapy, proceed to 2-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): Metfmin Sulfonylurea moderate risk gain hypoglycemia low Metfmin Sulfonylurea TZD Metfmin low risk gain edema, HF, fxs low Metfmin Thiazolidinedione Thiazolidinedione SU Metfmin DPP-4 inhibit intermediate low risk neutral rare Metfmin Metfmin SGLT2 inhibit intermediate low risk loss GU, dehydration Metfmin GLP-1 recept agonist low risk loss GI If HbA1c target not achieved after ~3 months of dual therapy, proceed to 3-drug combination (der not meant to denote any specific preference choice dependent on a variety of patient- & disease-specific facts): DPP-4 Inhibit SU Metfmin SGLT-2 Inhibit SU Metfmin GLP-1 recept agonist SU Metfmin Insulin (basal) est risk gain hypoglycemia variable Metfmin Insulin (basal) TZD DPP-4-i DPP-4-i TZD TZD TZD DPP-4-i SGLT2-i SGLT2-i SGLT2-i DPP-4-i Insulin SGLT2-i 2015 ADA-EASD Position Statement on Management of Hyperglycemia in T2DM Combination injectable therapy GLP-1-RA Insulin GLP-1-RA Insulin Basal Insulin Insulin Insulin GLP-1-RA If HbA1c target not achieved after ~3 months of triple therapy and patient (1) on al combination, move to injectables, (2) on GLP-1 RA, add basal insulin, (3) on optimally titrated basal insulin, add GLP-1-RA mealtime insulin. In refracty patients consider adding TZD SGLT2-i: Metfmin Mealtime Insulin GLP-1-RA Diabetes Care 2015;38: ; Diabetologia 2015;58:
42
 2000 (goal) mg/day HbA1c 6.8-8.")
43 Glycemia Reduction Approaches in Diabetes:A Comparative Effectiveness Study Screening T2DM on metfmin alone HbA1c >6.8% at screening < 10 years duration at randomization Metfmin run-in Titrate metfmin to 1000 (min) 2000 (goal) mg/day HbA1c % at final run-in visit Randomization n=5000 eligible subjects Sulfonylurea (glimepiride) n=1250 DPP-IV inhibit (sitagliptin) n=1250 GLP-1 analog (liraglutide) n=1250 Insulin (glargine) n=1250
44 1. Increasing T2DM prevalance& complexity of therapeutic options have led to the need f treatment guidelines. 2. These tend not to be based on -quality evidence but instead on expert opinion and/ cost concerns. 3. Most begin quite similarly ( Lifestyle then metfmin ), but differ to varying degrees on what to do next. 4. Emerging data from recent CVOT trials should lead to some modifications in guidelines -particularly in those patients with overt CVD. 5. There will also always be a need f the wise and skilled physician to choose the optimal therapeutic regimen f (and with) each patient. t
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach
 Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Insulin and Post Prandial
 Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
Insulin and Post Prandial Pr Luc Martinez PCDE Meeting Barcelona 2016 Conflicts of interest disclosure Advis consultant f Amgen Inc.; AstraZeneca Pharmaceuticals LP; GlaxoSmithKline; Ipsen; Lilly; Mayoly
SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk
 Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Treating Diabetes To Lower Cardiovascular Disease Risk
 Treating Diabetes To Lower Cardiovascular Disease Risk Anne Peters, MD Profess, USC Keck School of Medicine Direct, USC Clinical Diabetes Programs Disclosure of Financial Relationships 2015 Consultantship
Treating Diabetes To Lower Cardiovascular Disease Risk Anne Peters, MD Profess, USC Keck School of Medicine Direct, USC Clinical Diabetes Programs Disclosure of Financial Relationships 2015 Consultantship
9/12/2014. Main Pathophysiological Defect in T1DM. Main Pathophysiological Defects in T2DM. Personalizing Diabetes Care: The Alphabet Soup of Options
 9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Current Clinical Practice Guideline for Diabetes Management
 Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
Current Clinical Practice Guideline for Diabetes Management Chaicharn Deerochanawong M.D. Professor of Medicine, i Rangsit Medical University it Diabetes and Endocrinology Unit Department of Medicine Rajavithi
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
SGLT2 Inhibition in T2DM Management: Current Position and Future Promise
 SGLT2 Inhibition, Diabetes and CVD: Where Does This Fit in CV Risk Management? ESC Congress, Rome, Italy 28 August, 2016 SGLT2 Inhibition in T2DM Management: Current Position and Future Promise Silvio
SGLT2 Inhibition, Diabetes and CVD: Where Does This Fit in CV Risk Management? ESC Congress, Rome, Italy 28 August, 2016 SGLT2 Inhibition in T2DM Management: Current Position and Future Promise Silvio
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital
 Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Stephen Clement M.D. CDE Medical Director, Endocrine Services Inova Fairfax Hospital Financial Disclosures Consulting Panel for GSK on Hepatitis Vaccines Case Study BH is a 67 y/o female with T2 DM for
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Disclosures of Interest. Publications Diabetologia Key points to emphasize
 Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Disclosures of Interest No conflicts or disclosures How to Use the American Diabetes Association s Type 2 Diabetes Treatment Algorithm Rashida Downing, MD, FAAFP Primary Care Physician JenCare Medical
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
DISCLOSURES. Learning objectives NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Investigator Initiated Trial Support:
 NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
NAVIGATING THE TREATMENT OF TYPE 2 DIABETES: WHAT S NEW? Jane E-B Reusch MD Professor of Medicine, Biochemistry and Bioengineering Associate Director Center for Women s Health Research University of Colorado
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Keep Calm and Focus on the Evidence for the Management of Diabetes. Diabetes Update 2018
 Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
Keep Calm and Focus on the Evidence for the Management of Diabetes Diabetes Update 2018 Nicole C.Pezzino, PharmD, BCACP, CDE Assistant Professor, Wilkes University Pharmacist, Weis Markets Nicole.pezzino@wilkes.edu
7/8/2016. Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine
 Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Sol Jacobs MD, FACE Division of Endocrinology Emory University School of Medicine Participation in investigator initiated clinical research supported by: Merck Boehringer Ingelheim Novo Nordisk Astra Zeneca
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
LEADER and EMPA-REG. John Buse, MD, PhD. University of North Carolina School of Medicine Chapel Hill, NC, USA. Duality of Interest Declaration
 1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
1 LEADER and EMPA-REG John Buse, MD, PhD University of Nth Carolina School of Medicine Chapel Hill, NC, USA Duality of Interest Declaration I rept the following potential duality/dualities of interest
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Overview T2DM medications. Winnie Ho
 Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Overview T2DM medications Winnie Ho Diabetes in Australia 1.7 million Australians with diabetes, of these 85% have T2DM 2-fold excess risk CV death in patients with diabetes Risk factor for progression
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Canadian Journal of Diabetes
 Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
Can J Diabetes 42 (2018) S88 S103 Contents lists available at ScienceDirect Canadian Journal of Diabetes journal homepage: www.canadianjournalofdiabetes.com 2018 Clinical Practice Guidelines Pharmacologic
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
New Therapies for Diabetes Management: Hope or Headache?
 New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
New Therapies for Diabetes Management: Hope or Headache? Elizabeth Stephens, MD, FACP PMG- Endocrinology Elizabeth.Stephens@providence.org November 2018 Disclosures None 1 Objectives Discussion of 3 rd
Type 2 Diabetes Mellitus Insulin Therapy 2012
 Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
Type 2 Diabetes Mellitus Therapy 2012 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Preparations Onset Peak Duration
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Novel anti-diabetic therapies
 Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Prof. Manfredi Rizzo, MD, PhD ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of Palermo, Italy & ASSOCIATE PROFESSOR OF INTERNAL MEDICINE School of Medicine University of South
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Older Adults & Optimal Outcome. Individualizing Diabetes Management. Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC
 Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
Older Adults & Optimal Outcome Individualizing Diabetes Management Mary Moyer Janci BC-FNP BC-ADM CDE Teaching Associate Diabetes Care Center UWMC What is Diabetes? METABOLIC DISEASE Food breakdown (carbohydrates,
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Navigating the New Options for the Management of Type 2 Diabetes
 Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
Navigating the New Options for the Management of Type 2 Diabetes Clinical Associate Professor Mark Kennedy Department of General Practice, University of Melbourne Chair, Primary Care Diabetes Society of
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Making Sense of Mediations for Diabetes
 Making Sense of Mediations for Diabetes Lisa Kroon, PharmD, CDE Professor of Clinical Pharmacy UCSF School of Pharmacy Diabetes Mellitus: U.S. Impact Source: ADA; released June 10, 2014 ~1-1.5 Million
Making Sense of Mediations for Diabetes Lisa Kroon, PharmD, CDE Professor of Clinical Pharmacy UCSF School of Pharmacy Diabetes Mellitus: U.S. Impact Source: ADA; released June 10, 2014 ~1-1.5 Million
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
INSULIN THERAPY. Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital
 INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
INSULIN THERAPY Rungnapa Laortanakul, MD Maharat Nakhon Ratchasima hospital 3 Sep. 2013 Case Somsak is a 64-year-old man was diagnosed with T2DM, HT, and dyslipidemia 9 years ago. No history of hypoglycemia
7/6/ ANNUAL MEETING DIABETES - KEEPING UP WITH CHANGES TECHNICIAN OBJECTIVES PROJECTED PREVALENCE OF DIABETES IN THE UNITED STATES:
 TECHNICIAN OBJECTIVES Audience will be able to describe the differences between traditional and newer insulin products. DIABETES - KEEPING UP WITH CHANGES MARY HENCHER PHARMD, BCPS, CDE CLINICAL PHARMACIST,
TECHNICIAN OBJECTIVES Audience will be able to describe the differences between traditional and newer insulin products. DIABETES - KEEPING UP WITH CHANGES MARY HENCHER PHARMD, BCPS, CDE CLINICAL PHARMACIST,
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION
 OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
OLD AND NEW DRUGS FOR CONTROLING DIABETES THERAPEUTIC CLASSES AND MECHANISM OF ACTION Biljana Parapid, MD, PhD, FESC Belgrade University School of Medicine, Belgrade (Serbia) @biljana_parapid COI International
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c
 Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Halting the Rise, Newest Non- Insulin Options for Lowering A1c Alecia Rottinghaus, PharmD PGY-1 Pharmacy Resident Iowa City Veterans Affairs Health Care System January 29 th, 2019 Disclosures Alecia Rottinghaus
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011