CV Risk Management in Diabetes Mellitus
|
|
|
- Owen Wiggins
- 6 years ago
- Views:
Transcription
1 CV Risk Management in Diabetes Mellitus J R Minkoff MD, FACP Endocrinology Clinical Professor of Family and Community Medicine University of California, San Francisco Mr. B 40 y/o Latino male c/o fatigue, ED, wants to talk about testosterone FH father died on insulin amputation Urine dipstick 3+ glucose Weight 250# BP 155/95 HbA1c 9.5% Fasting labs: Glucose 250 TC 250 TG 250 HDL 35 LDL 165 Bad News Leading cause of blindness, ESRD, amputation CV disease Type 2: 2x risk of cardiovascular events, death Type 1: 10 fold increase of age-adjusted risk Diabetes prevalence (CDC) increasing in the US 9.3% million people 8.1 million (27.8%) undiagnosed Over 90% type 2 DM (although type 1 also increasing)
2 More Bad News At diagnosis of type 2 DM 50% of patients have at least one complication Diabetes costs in US $245 billion per year $825 billion worldwide Good News Glucose control decreases microvascular complications In type 1 DM glucose control mitigates risk of all complications In type 2 DM: Glucose control decreases microvascular complications Early tight glucose control may improve CV complications More Good News CV complications can be decreased in patients with type 2 DM Controlling BP conveys greater benefit in DM than almost any other maneuver And in high risk individuals Statins improve outcomes ACE inhibitors improve outcomes ASA improves outcomes This can be done and has been done
3 Disclosures I have no financial interests in medical or pharmaceutical entities I do not give lectures for pharmaceutical entities nor do I have research grants associated with PhRMA References Standards of Medical Care in Diabetes 2017 Abridged for Primary Care Providers American Diabetes Association. Diabetes Care 2017;40(Suppl. 1):S1 S138. Kaiser Permanente National CLINICAL PRACTICE GUIDELINES 1/16. _adult_diabetes_guidelines1.pdf Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From the American College of Physicians. Ann Int Med. 3 JANUARY 2017 UKPDS 33: Lancet (1998) 352, UKPDS 34: Lancet (1998) 352, UKPDS 38: BMJ (1998) 317, UKPDS 39: BMJ (1998) 317, Objectives Participants will: 1) understand the need for tight glucose control to prevent microvascular complications and mitigate cardiovascular complications in diabetes 2) feel comfortable discussing the evidence for BP control in diabetes 3) know when to prescribe statins, ACE inhibitors and aspirin for patients with diabetes who have not yet had a vascular event
4 Type 1 DM In type 1 DM glucose control mitigates risk of all complications Glucose control decreases microvascular complications nephropathy Retinopathy neuropathy CV complications can be decreased Treatment for Type 1 DM is simple - Insulin Therapy The patient who knows the most lives longest. Elliot P Joslin MD Excellent evidence avoiding complications and survival directly related to glucose control. MDI or pump therapy. It s not easy Education is key In Type 1 Diabetes - Glycemic control predicts all outcomes Insulin basal prandial Corrective Glucose monitoring Diet carbohydrate counting Exercise Encouragement Monitor for complications Educate - Repeat
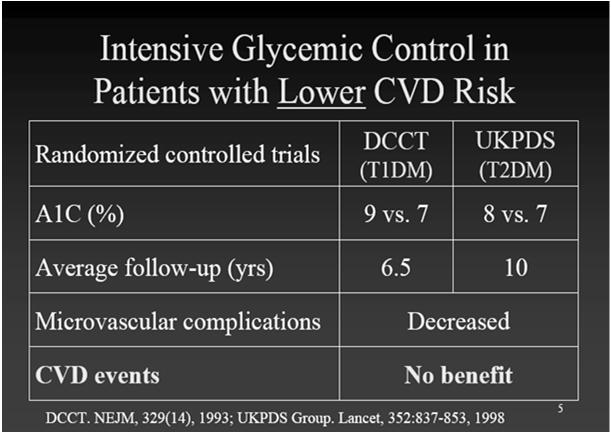
5 Type 1 DM - DCCT 1441 type 1 DM average 26 years old 7-9 years of intensive (7%) A1c or conventional (9%) A1c Intensive control decreased: retinopathy 63-76% microaluminuria 39-54% neuropathy 60% macrovascular disease 41% (NS) The Diabetes Control and Complications Trial Research Group * N Engl J Med 1993; 329:977 Side Effects of Tight Control Hypoglycemia Diet Exercise Insulin adjustment Weight gain Diet Exercise Insulin adjustment DCCT: Risk of Sustained Retinopathy Progression by HbA 1c Level and Years of Follow-up DCCT Research Group. Diabetes. 1995;44: Mean HbA 1c = 11% 10% 9% Rate Per 100 Person-Years % 7% Time During Study (yr)


6 DCCT/EDIC 10 years after DCCT, HbA1c then 8% 10 years after RCT study - DCCT was over all subjects received usual care. Despite HbA1c now equal between both groups (intensive vs control), CV outcomes were markedly different DCCT/EDIC Research Group. JAMA.2002;287:2563. Nathan DM, et al. N Engl J Med. 2005;353:2643 DCCT-EDIC: Long-Term Risk of Macrovascular Complications
7 Basement Membrane Damage Is Forever Questions about type 1 DM? But Type 2 Diabetes is Complex Some damage occurs before diagnosis - associated with insulin resistance Early glucose control: Paramount in preventing microvascular complications Likely prevents macrovascular complications Blood Pressure and Lipid control are arguably more effective than tight glucoses control in reducing cardiovascular risk and macrovascular complications
8 Anabolic Effects of Insulin FAT FFA GLU FFA GLU GLU GLU FFA MUSCLE LIVER Resistance to Insulin FAT FFA GLU FFA GLU GLU GLU FFA MUSCLE LIVER Mechanisms of Vascular Injury in Type 2 Diabetes Metabolic Syndrome Insulin resistance Dyslipidemia HDL Triglycerides Hypertension Obesity Hyperglycemia Increased Free Fatty Acids cause endothelial dysfunction and are proinflammatory Oxidative Stress is increased by multiple cardiovascular risk factors

9 Metabolic Syndrome Risk Factors Predict CVD Events : WOSCOPS Sattar et al, Circulation 2003 Patients with DM are more likely to have a greater burden of atherosclerotic risks: CAD Silent MI; atypical angina Small vessel CAD; Multivessel CAD other CV risks Hypertension Dyslipidemia Small dense LDL High TG, low HDL Increased fibrinogen, clotting factors, platelet adhesion Endothelial dysfunction Hyperglycemia Increased Risk of Cardiovascular Events Over 7 Years in Patients With Type 2 Diabetes Myocardial Infarction Stroke CV Death Nondiabetic MI (n=1,304) Diabetic MI (n=890) Nondiabetic +MI (n=69) P<0.001* Diabetic +MI (169) P<0.001* P<0.001* CV = cardiovascular; -MI = no prior myocardial infarction; +MI = prior myocardial infarction *For diabetes vs. no diabetes and prior MI vs. no prior MI Haffner SM, et al. N Engl J Med. 1998;339:
10 Prevention of Complications Regular medical care Education Monitoring Glucose (A1c, self monitoring) Goal A1c < 7% Microalbumin Photo or Dilated retinal exam Foot and monofilament testing BP control: <139/89 lower is better Lipid control ASA if needed High index of suspicion for complications Educate, Motivate, Intervene - REPEAT To improve outcomes in diabetes - Remember your ABC s Aspirin: over 50 or risk CV risk ACEi or ARB over 50, BP or microalbuinuria Blood Pressure control Cholesterol treatment: statins Diabetes (glucose) control Education (Exercise, Encouragement) Multiple risk factor intervention UK Prospective Diabetes Study 5102 newly diagosed type 2 DM age 56 An intensive glucose control policy HbA1 c 7.0 % vs 7.9 % reduces risk of any diabetes-related endpoints 12% p=0.030 microvascular endpoints 25% p=0.010 myocardial infarction 16% p=0.052
11 A1C Control Decreases Microvascular Disease Type 2 Benefits of A1C Control Incidence / 1000 p-yrs (%) Microvascular Endpt M I A1C A1C UKPDS, B Med J, UKPDS Glucose Control Study Summary The intensive glucose control policy maintained a lower HbA 1c by mean 0.9 % over a median follow up of 10 years from diagnosis of type 2 diabetes with reduction in risk of: 12% for any diabetes related endpoint p= % for microvascular endpoints p= % for myocardial infarction p= % for cataract extraction p= % for retinopathy at twelve years p= % for albuminuria at twelve years p= UKPDS: Metformin Is Associated With a Reduction in Cardiovascular Events Glibenclamide Insulin Metformin Sulfonylurea/ Insulin Conventional Mean Change in Risk* P Value Mean Change in Risk* P Value Hemoglobin A 1c Metformin Diabetes-related death 42% % 0.19 All-cause mortality 36% % 0.49 Any diabetes-related endpoint 32% % 0.46 Chlorpropamide Myocardial infarction 39% % 0.11 Stroke 41% % Years *Compared with conventional therapy based on diet/exercise in overweight patients UKPDS = United Kingdom Prospective Diabetes Study Reprinted in an adapted form from UKPDS Group. Lancet 1998;352: , with permission from Elsevier.

12
13 And yet UKPDS 10 year follow-up after RCT was completed: Although differences in HbA1c levels lost 1 year after study Between-group relative reductions in risk persisted at 10 years sulfonylurea insulin any diabetes-related end point 9% P=0.04 microvascular disease 24% P=0.001 myocardial infarction 15% P=0.01 death from any cause 13% P=0.007 Metformin group Holman RR NEJM 2008; 359: any diabetes-related end point 21%, P=0.01 myocardial infarction 33%, P=0.005 death from any cause 27%, P=0.002 Delayed Benefits in Patients Younger and Lower CVD risk DCCT Type 1 Age 44 HbA1c ~ 8% Average f/u y Microvascular Decreased Complications UKPDS Type 2 56 ~ 8% y Decreased CVD Events Decreased Decreased DCCT/EDIC NEJM 2005: 353:2643 UKPDS 80 NEJM 2008:359
14 Questions about beneficial effects of glucose control in type 1 or type 2 DM? To improve outcomes in diabetes - Remember your ABC s Aspirin: over 50 or risk CV risk ACEi or ARB over 50, BP or microalbuinuria Blood Pressure control Cholesterol treatment: statins Diabetes (glucose) control Education (Exercise, Ecouragement) UK Prospective Diabetes Study A tight blood pressure control policy 144/82 vs 154/87 mmhg reduces risk of any diabetes-related endpoint 24% p=0.005 microvascular endpoint 37% p=0.009 stroke 44% p=0.013
15 BP Goal for Diabetes - 139/89 or less major improvement in CV risk in DM patients: Study Systolic BP < 145 UKPDS <135 Advance <130 Steno-2 Diastolic BP < 80 HOTS ACCORD trial showed possibly no benefit and more side effects with Systolic < 120 So HEDIS changed BP goal to 139/89, consistent with the JNC 8. BP control is essential so is glycemic control Although benefits of improved BP control were lost 10 years after the UKPDS study Early tight glucose control resulted in persistent benefits 10 year after Education Glucose, BP and Lipid control Safety Follow-up Self-monitoring glucose Symptoms/Treatment of high or low glucose Diet Exercise Smoking cessation REPEAT Insulin administration
16 Mr. B 5 years later (now 45 years old) Followed diet and exercise recommendations and weight has plateaued No hypoglycemic symptoms Meds: metformin 1000 mg bid + NPH 24 lisinopril 20/hctz 25 mg daily Weight 225; BP 132/78 LDL 158, A1c 8.5%, normal Cr and K What else? CV risk management Control glucose Control BP Control lipids MONITOR REPEAT Diabetes tends to be progressive BP and lipid management tends to be stable Newer medications associated with decreased CV risk
17 Liraglutide (GLP-1 agonist) and CV outcomes Marso et al NEJM 375:311 type 2 DM + CV disease average 3.8 year follow-up N = 9340 CV events CV death Death Placebo 14.9% 6% 9.6% Liraglutide 13% 4.7% 8.2% NNT CANVAS and CANVAS-R trials N > 10,000 Composite CV outcome event per 1000 patientyears Renal progression Amputation Canagliflozin 26.9 Decreased Increased Placebo 31.5 DBP and A1c also NNT 22 Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes Neal B et al 2017 NEJM.DOI: /NEJMoa , SGLT 2 Inhibitor EMPAG REG study high CV risk RCT using Jardiance (empagliflozin) reduced CV related deaths by 2.2% over 3.1 years (3.7% vs 5.9%) % increased rate of genital infection NNT 45 for 3.1 years to prevent 1 death Cost: ~$ a year
 - 0.")
18 Degludec v Glargine for 2 years Marso SP 2015 NEJM, DOI: /NEJMoa w DM2, 85% with complications Age 65, duration of DM 16 years Similar A1c drop from 8.5% to 7.5% Less severe hypoglycemia, lower FBS with Degludec Non-inferiority of Degludec NNT = 120 for 2 years) - 0.8% fewer primary composite outcomes* *in the time-to-event analysis the first occurrence of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke Mechanisms of Vascular Injury in Type 2 Diabetes Metabolic Syndrome Insulin resistance Dyslipidemia HDL Triglycerides Hypertension Obesity Hyperglycemia Increased Free Fatty Acids cause endothelial dysfunction and are proinflammatory Oxidative Stress is increased by multiple cardiovascular risk factors How We EVOLVED


19 Age-adjusted Prevalence of Obesity and Diagnosed Diabetes Among US Adults Obesity (BMI 30 kg/m 2 ) No Data <14.0% 14.0% 17.9% 18.0% 21.9% 22.0% 25.9% > 26.0% Diabetes No Data <4.5% 4.5% 5.9% 6.0% 7.4% 7.5% 8.9% >9.0% CDC s Division of Diabetes Translation. United States Surveillance System available at Type 2 DM intravascular inflammation Hyperglycemia glycosylation products Lipid abnormalities Free Fatty Acids Bradykinins Cytokines Increased fibrinogen Basement Membrane Damage Is Forever early tight control
20 Addressing Intravascular Inflammation Evidence: Statins RAS control ACE inhibitors Angiotensin Receptor Blocker ASA BP control Safely lowering glucose in DM Decreasing adiposity Exercise Lack of evidence: Vitamins E, C, B12, Folate anit-inflammatory diet To improve outcomes in diabetes - Remember your ABC s Aspirin: over 50 or risk CV risk ACEi or ARB over 50, BP or microalbuminuria Blood Pressure control use ACEi Cholesterol treatment: statins Diabetes (glucose) control insulin early Education (Exercise, Encouragement) CHD Prevention Trials with Statins in Diabetic Subjects: Subgroup Analyses Study Primary Prevention AFCAPS/TexCAPS Secondary CARE 4S LIPID 4S-Extended Drug Lovastatin Pravastatin Simvastatin Pravastatin Simvastatin No CHD Risk Reduction (overall) 37% 23% 32% 25% 32% CHD Risk Reduction (diabetes) 43% 25% (p=0.05) 55% (p=0.002) 19% 42% (p=0.001) Adapted from Downs JR et al. JAMA 1998;279: ; Goldberg RB et al. Circulation 1998;98: ; Py r l K et al. Diabetes Care 1997;20: ; The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) Study Group. N Engl J Med 1998;339: ; Haffner SM et al. Arch Intern Med 1999;159:

21 4S Group. Lancet 1994;334: Simvastatin Reduced the Risk of Major Coronary Events Subgroup Analyses, Scandinavian Simvastatin Survival Study Percent Risk Reduction n= P< n=407 n=1156 n=542 n=573 n= P=0.01 P< P<0.002 P<0.002 P=0.002 Men Women Older Smokers Hypertension Diabetes Simvastatin: Heart Protection Study After allowance for noncompliance, 40 mg daily simvastatin safely reduces the risk of heart attack, of stroke, and of revascularization by about one third. 5 years of statin typically prevents these major vascular events in: 100 of every 1000 people with previous MI NNT= " " other previous CHD NNT= " " cerebrovascular disease NNT = " " other arterial disease 70 of every 1000 people with diabetes (age 40+) irrespective of cholesterol level (or age, or sex, or other treatments). Heart Protection Study Collaborative Group. Lancet 2002;360:7 22. Why give statins in diabetes despite normal LDL? Patients with DM have at least twice the CV mortality risk This can be considered secondary prevention HPS, 4S and Steno-2 Pleotropic effect even with LDL at goal
 control insulin early Education (Exercise, Encouragement) Why give ACE inhibitors in diabetic patients?")
22 To improve outcomes in diabetes - Remember your ABC s Aspirin: over 50 or risk CV risk ACEi or ARB over 50, BP or microalbuminuria Blood Pressure control use ACEi Cholesterol treatment: statins Diabetes (glucose) control insulin early Education (Exercise, Encouragement) Why give ACE inhibitors in diabetic patients? with elevated BP with microalbuminuria or higher grade proteinuria with CV risk despite normal BP? HOPE and Steno-2: NNT over 4 years to prevent CV events and death Blocking Renin-Angiotensin System forestalls progression of microalbuminuria to proteinuria to ESRD and dialysis Heart Outcomes Prevention Evaluation (HOPE) Study Effect of Ramipril on Cardiovascular Events (Myocardial Infarction, Stroke, or CVD Death) ~ 4.5 Yrs % of Patients % Risk Reduction 15.0 NNT = 21 21% Risk Reduction Placebo Ramipril Placebo Ramipril N=3,578 P N=5,719 P Diabetic Patients Nondiabetic Patients Hope Study Investigators. N Engl J Med. 2000;342:

23 CA Dezsi Additional benefits of ACE inhibitors include: maintaining levels of bradykinin, inhibiting platelet aggregation and endothelial apoptosis For Our Patients Cardiovascular Quality Means Consistency BP and lipid control each associated with better cardiac outcomes. Lower HbA1c may. Aim for excellent control and Any lowering of BP lower CV risks. Any statin lower CV risks. Lower A1c without hypoglycemia lower CV risks. Your intervention/intensification is key. Smoking cessation, ACE inhibitor, statin and ASA risk It works, but it requires everyone participate! STENO-2: Risk-Factor Targets Attained at 7.8 Years With Intensive Treatment Program p <.001 Intensive Therapy Conventional Therapy p = Patients (%) p = 0.06 Hemoglobin A 1c <6.5% Cholesterol <175 mg/dl Triglycerides <150 mg/dl Systolic Blood Pressure <130 mm Hg Diastolic Blood Pressure <80 mm Hg Reprinted from Gaede P, et al. N Engl J Med. 2003;348: Copyright 2003 Massachusetts Medical Society, All rights reserved.
24 Steno-2 Study: Multifactorial Intervention for Type 2 Diabetes: multifactorial, target-driven treatment of type 2 diabetes with microalbuminuria. Decreased CV Events Cumulative Incidence Cardiovascular Event (%) Conventional Therapy P<0.001 Intensive Therapy Years of Follow-up No. at Risk Intensive Therapy Conventional Therapy Gaede P, et al. N Engl J Med. 2008;358: Copyright 2008 Massachusetts Medical Society. All rights reserved. Steno-2 after 21.2 years of follow-up Gæde, P., Oellgaard, J., Carstensen, B. et al. Diabetologia (2016). doi: /s All patients offered intensive management after initial randomized trial - average 7.8 years. Outcomes median of 7.9 years of gain of life. 38 intensive-therapy patients vs 55 conventional-therapy patients died during follow-up (HR 0.55 [95% CI 0.36, 0.83], p = 0.005). hazard for all microvascular complications was decreased in the intensive-therapy group in the range 0.52 to 0.67, except for peripheral neuropathy (HR 1.12). Steno-2 follow-up over 2 decades: Early intensive managed type 2 DM vs usual care
25 Although initial Steno-2 trial ended at 7.8 years A total of 21 years of follow-up with additional intensive management resulted in continued, improved MORTALITY. Gaede, P et al. Diabetologia (2016). doi: /s Early Glycemic Control and Magnitude of HbA1c Reduction Predict Cardiovascular Events and Mortality: Population-Based Cohort Study of 24,752 Metformin Initiators median age 62.5 years, 55% males wi median follow-up of 2.6 years A1c attained and amount of improvement both associated with fewer MACE Svensson E et al Diabetes Care 40(6); 800 Combined outcome event (acute myocardial infarction, stroke, or death) by achieved early glycemic level. Elisabeth Svensson et al. Dia Care 2017;40: by American Diabetes Association
 by magnitude of HbA1c reduction from baseline to")
26 Adjusted HRs for combined outcome event (acute myocardial infarction, stroke, or death) by achieved HbA1c 6 months after metformin initiation. Elisabeth Svensson et al. Dia Care 2017;40: by American Diabetes Association Adjusted HRs for combined outcome event (acute myocardial infarction, stroke, or death) by magnitude of HbA1c reduction from baseline to 6 months. Elisabeth Svensson et al. Dia Care 2017;40: by American Diabetes Association NEJM 2010


27 And we did it with fewer Caths National data for cardiac caths And CABG s Use of cardioprotective medications increased 2-3 fold And we did it with generics!
28 Trend in decreasing MI s persists Solomon, M et al JACC 68(6), 666. and continues to decrease in patients with diabetes Find your patient s motivation Do not give up Escalate and intensify treatment early Using insulin and sulfonylureas: educate about hypoglycemia and celebrate success. Allow down-titration to improve self-efficacy Adding new meds: look for effect (improved glucose control and/or weight control)

29 Impact of Improvements in Cardiovascular Care on KPNC Member Mortality: From : 30.4% reduction in mortality from CVD 42.2% reduction in mortality from stroke 10.9% reduction in mortality from cancer Sidney S, Closing the Gap Between Cardiovascular and Cancer Mortality in an Integrated Health Care Delivery System, : The Kaiser Permanente Experience. Circulation 2011; 124: A13610 To improve outcomes in diabetes - Remember your ABC s Aspirin: over 50 or risk CV risk ACEi or ARB over 50, BP or microalbuminuria Blood Pressure control use ACEi Cholesterol treatment: statins Diabetes (glucose) control insulin early Education (Exercise, Encouragement) You can do it! Questions? Comments?
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Microvascular Disease in Type 1 Diabetes
 Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Microvascular Disease in Type 1 Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine The Course
Management of Cardiovascular Disease in Diabetes
 Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Management of Cardiovascular Disease in Diabetes Radha J. Sarma, MBBS, FACP. FACC. FAHA. FASE Professor of Internal Medicine Western University of Health Sciences. Director, Heart and Vascular Center Western
Diabetes and the Heart
 Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Diabetes and the Heart Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 6, 2012 Outline Screening for diabetes in patients with CAD Screening for CAD in patients with
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Update on Diabetes. Ketan Dhatariya. Why it s Not Just About Glucose Lowering Any More. Consultant in Diabetes NNUH
 Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Update on Diabetes Why it s Not Just About Glucose Lowering Any More Ketan Dhatariya Consultant in Diabetes NNUH The Story So Far.. DCCT Retinopathy Neuropathy Nephropathy Intensive glucose control in
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Macrovascular Disease in Diabetes
 Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications
 American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
American Diabetes Association Standards of Medical Care in Diabetes 2017: Focus on Complications Juan Pablo Frias, M.D., FACE President and CEO, National Research Institute, Los Angeles, CA Clinical Faculty,
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Complications of Diabetes: Screening and Prevention. Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley
 Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Complications of Diabetes: Screening and Prevention Dr Martin McIntyre Consultant Physician Royal Alexandra Hospital Paisley Diabetic Complications Microvascular: Retinopathy Nephropathy Neuropathy Macrovascular:
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Educational and behavioral interventions hitherto published
 Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,
Treatment of High-Risk Patients with Diabetes: Motivation and Teaching Intervention: A Randomized, Prospective 8-Year Follow-Up Study Rita Rachmani, Inna Slavacheski, Maya Berla, Ronni Frommer-Shapira,
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions
 Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
Diabetes and Concomitant Cardiovascular Disease: Guideline Recommendations and Future Directions Diabetes is one of the largest global health emergencies of 21 st century, with the number of people with
Vascular complications
 Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
Vascular complications December 8, 2018 Faculty Disclosure Faculty: Kim Connelly, MBBS, PhD, FRACP Associate Professor of Medicine, University of Toronto Cardiologist, St. Michael s Hospital Relationships
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Diabetes and Heart Disease. Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center
 Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Heart Disease Sarah Alexander, MD, FACC Assistant Professor of Medicine Rush University Medical Center No conflicts of interest or financial relationships to disclose. 2 What s the problem??
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Prevention of MACROvascular Complications of Diabetes
 Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
Prevention of MACROvascular Complications of Diabetes Matt Bouchonville, MD, CDE Endocrinology Division University of New Mexico School of Medicine July 12, 2018 Conflicts of Interest None Objectives 1.
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf
 Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
Reducing CVD globally through combination approaches to prevention: the polypill. Salim Yusuf Disclosure None Polypill & CVD Prevention 1. Why do we need a polypill? 2. What components in the polypill?
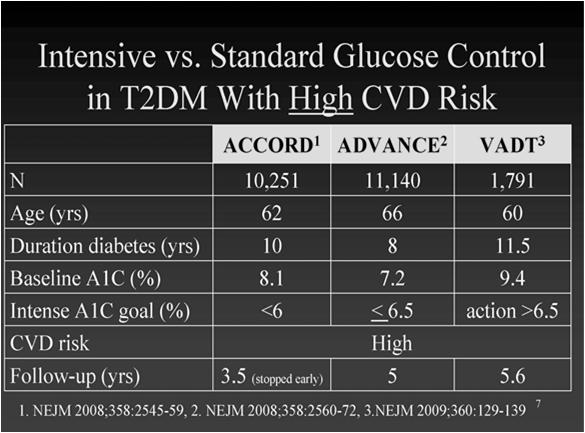
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
1/28/2014. The Metabolic Syndrome: Early History. Insulin Resistance: Early Diagnosis and Treatment to Prevent Cardiovascular Disease
 : Early Diagnosis and Treatment to Prevent Cardiovascular Disease Henry N. Ginsberg, M.D. Irving Professor of Medicine Columbia University College of Physicans and Surgeons The Metabolic Syndrome: Early
: Early Diagnosis and Treatment to Prevent Cardiovascular Disease Henry N. Ginsberg, M.D. Irving Professor of Medicine Columbia University College of Physicans and Surgeons The Metabolic Syndrome: Early
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Review. Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction
 Review Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction Diabetes mellitus is increasingly recognized as an essentially vascular
Review Hyperglycemia, dyslipidemia and hypertension in older people with diabetes: the benefits of cardiovascular risk reduction Diabetes mellitus is increasingly recognized as an essentially vascular
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Metabolic Syndrome. Shon Meek MD, PhD Mayo Clinic Florida Endocrinology
 Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Metabolic Syndrome Shon Meek MD, PhD Mayo Clinic Florida Endocrinology Disclosure No conflict of interest No financial disclosure Does This Patient Have Metabolic Syndrome? 1. Yes 2. No Does This Patient
Evidence-Based Glucose Management in Type 2 Diabetes
 Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Evidence-Based Glucose Management in Type 2 Diabetes James R. Gavin III, MD, PhD CEO and Chief Medical Officer Healing Our Village, Inc. Clinical Professor of Medicine Emory University School of Medicine
Welcome and Introduction
 Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)