Clinical Case Presentation. Dana Assis, MD
|
|
|
- Stephen Hector Russell
- 6 years ago
- Views:
Transcription
1 Clinical Case Presentation Dana Assis, MD
2 Clinical Presentation 63 year old male with medical history AIDS (CD4 11, VL 62K), Hep C cirrhosis (never treated), DM II c/b diabetic retinopathy, HTN, CKD III, former IVDU. Presents to clinic with up trending creatinine (previous baseline Cr since 2014), hematuria, and nephrotic range proteinuria.
3 ROS negative for weight loss/gain, cough, shortness of breath, chest pain, nausea, vomiting, diarrhea, abdominal pain, joint pains, fevers, chills, rashes. ROS positive LE swelling three years, foamy urine 8 months. PMHx:. AIDs dx 1995, on ARV since 1996, stopped taking for 3 years, then restarted one year ago. Following with hepatology for possible hepatitis C treatment Social: IVDU x 20 years, No etoh, Puerto Rico FHx: DM, HTN, no Renal/Rheum disease Meds: Novolog, epzicom, norvir, prezista, darunavir, losartan, amlodipine, aspirin, mvi
4 Physical Exam BP 162/71 P 61 O2 100% RA Gen NAD CV s1s2 diastolic murmur rusb Pulm cta bl Abd soft nd nt Ext b/l 2+ pitting edema extending to shins
5 Laboratory Findings


6 Basic Metabolic Panel

7 Urine 4/2015 Up 471 Ucr 81 10/2015 Up 488 Ucr 101 Umicroalbumin 2598 mg/l Urine cytology negative for malignant cells, positive for red blood cells


8 HIV VL 62,500 copies/ml Hep BcAb reactive sag NR K/L 3.86 Kappa free 803 Lambda free 208 IgG lambda band identified IgG 2900 IgA 318 IgM 154 RF Negative C3 104 C4 27 TC 142 TG 148 LDL 76 HDL 36 Albumin 2.4 Hb 9.9 ANCA negative ANA negative Anti GBM negative
9 Imaging Renal ultrasound normal renal sonogram both kidneys measuring 10-11cm in length. No evidence of renal calculi. No hydronephrosis. No renal mass. Bladder outline normal with splenomegaly Cirrhotic morphology of liver portal hypertension with splenomegaly no ascites
10 Differential Diagnosis Diabetic Nephropathy HIV associated Nephropathy / ICD MPGN Hep C Amyloidosis
11 Renal Pathology Biopsy Diffuse nodular glomerulosclerosis, consistent with diabetic nephropathy Interstitial inflammatory cell infiltrate diffuse and mild Negative congo red stain for amyloid Interstitial fibrosis/tubular atropthy (20-30%) Global glomerulosclerosis 2/49 Moderate arteriolar hyalinosis Marked thickened glomerular basement membranes No evidence of immune complex mediated GN, HIV or Hep C infection associated GN or monoclonal associated disease.
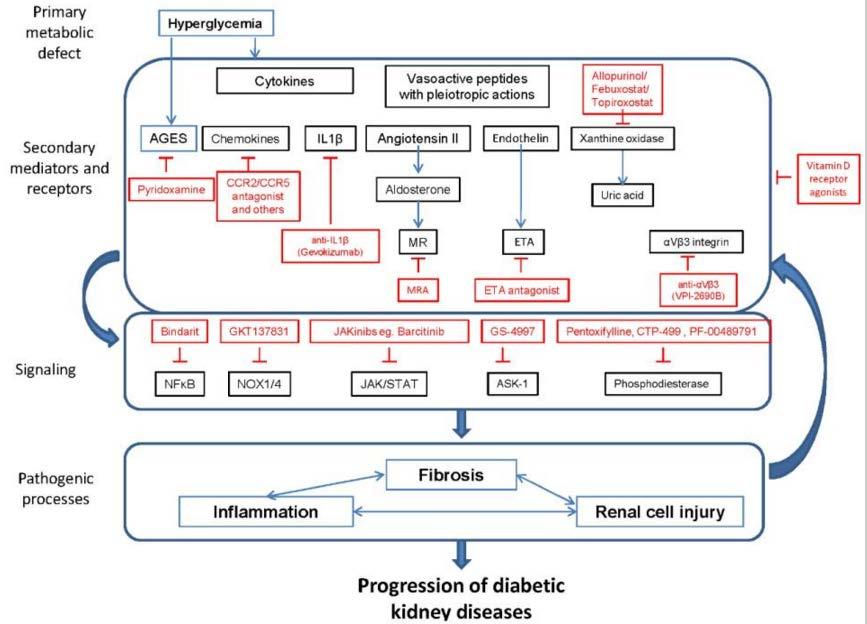
12 Diabetic Nephropathy Targeting Signaling Pathways Nephrotic syndrome Angiopoietin like 4
13

14 Complexity Podocyte Foot Process
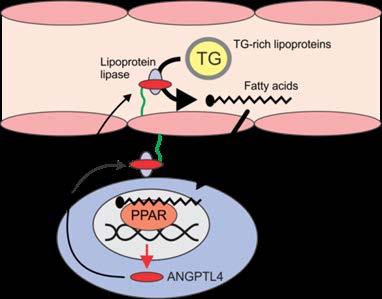
15 Angiopoietin like protein 4
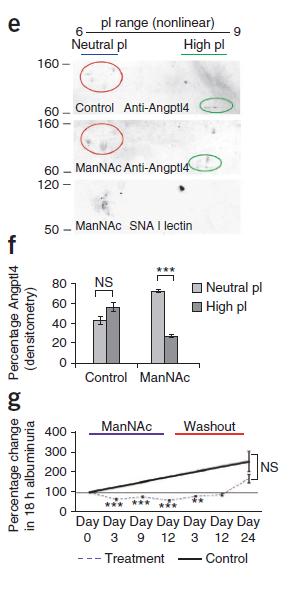
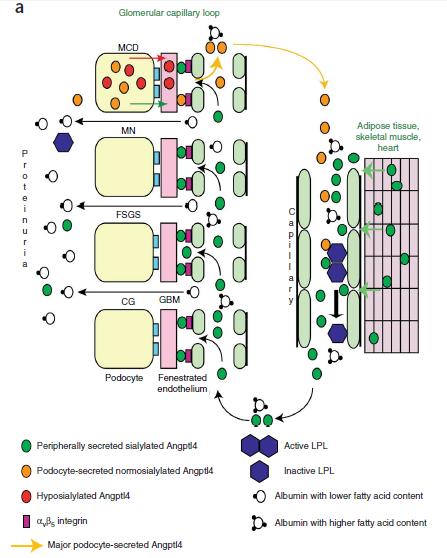
16 Angiopoietin-like-protein 4 Podocyte phenotype Loss of glomerular basement membrane (GBM) charge and foot process effacement Two types of Angptl4 Hyposialylated form secreted from podocytes Sialylated form secreted from skeletal muscle, heart, and adipose tissue.
17
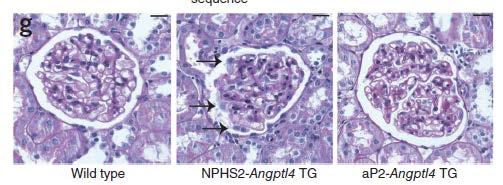
18 Article Highlights Angptl4 is upregulated in serum and podocytes of patients and mouse/rat models of MCD Transgenic NPHS2-angptl4 rats versus ap2 Sialylation of Angptl4
19
20 γ2 Nephrotoxic Serum (NTS) Phosphate Buffered Saline (PBS) Lipopolysaccharide (LPS) Rat Model
21 Increased proteinuria = increase mrna expression Angptl4 Seen in mouse model MCD
22 Transgenic Rat Model

23 Relationship between Angptl4 overexpression and proteinuria
24
25
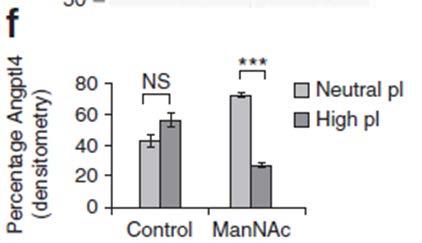
26 Summary Slide Transgenic expression of Angptl4 from podocyte reproduced key feature of MCD Absence of proteinuria in ap2-angptl4 transgenic rats localized prodution of Angptl4 by podocytes in proteinuric disease Treatment with sialic acid precursor N-acetyl-Dmannosamine (ManNAc) converts high pi glomerular Angptl4 to neutral Angptl4 in vivo and reduces albuminuria and proteinuria
27
28 Study Highlights Mechanism between proteinuria and hyperlipidemia in nephrotic syndrome In this study high serum levels of angptl4 (presumably normosialylated based on neutral isoelectric point) in other glomerular diseases as well Systemic feed back loop role of circulating Angptl4
29
30
31 Plasma ANGPTL4 Volunteer v Untreated Patients * P < 0.05 ** P <0.01 *** P <0.001

32
33

34 PAN hypertg present throughout proteinuria and persisted despite normalization proteinuria
35 Angplt4 Adipose versus NPHS2 rats
36 Hypertriglyceridemia was absent in Angptl4 mice despite these mice having significant P<0.001 proteinuria
37 Origins of circulating Angplt4 Mild upregulation in GM subsided day 9 No glomerular upregulation
38

39 Test effect of raising plasma FFA levels on nephrotic syndrome
40 High circulating Angplt4 levels reduce proteinuria
41 Angplt4 interaction with αγβ5 integrin Recombinant normosialylated rat Angplt4 (mimics circulating Angptl4 in nephrotic state) protect cultured endothelial cells from oxidative stress Hyposialylated Angplt4 (key mediator of proteinuria that secreted by podocytes in MCD) increased effects of oxidative stress
42
43
44
45 Study Highlights Explore effect of Angptl4 on DN Streptozotocin induced diabetic model Urinary level of angptl4 and relationship with albuminuria
46 Summary Angplt4 plays a role in nephrotic syndrome Connection between albuminuria and hypertriglyceridemia Role in DN
47 The End Happy Birthday Apra and Mansi
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
GRAND ROUNDS
 GRAND ROUNDS 5.14.13 CASE 64 y.o AAF with h/o HTN, DM, HLD, MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria Per patient systolic BP
GRAND ROUNDS 5.14.13 CASE 64 y.o AAF with h/o HTN, DM, HLD, MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria Per patient systolic BP
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Supplementary Information Titles
 Journal: Nature Medicine Supplementary Information Titles Article Title: Podocyte secreted Angiopoietin-like mediates proteinuria in glucocorticoid sensitive nephrotic syndrome Corresponding Author: Sumant
Journal: Nature Medicine Supplementary Information Titles Article Title: Podocyte secreted Angiopoietin-like mediates proteinuria in glucocorticoid sensitive nephrotic syndrome Corresponding Author: Sumant
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Foamy Urine and Sickled Cells. Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA
 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Hasan Fattah 4/30/2013
 Hasan Fattah 4/30/2013 49 yo hispanic male, ho HIV(CD4 229), currently on HAART, course c/b AIDS, Presents with two days ho fever, SOB, blood tinged sputum, and visible hematuria. ROS: no skin rash, joint
Hasan Fattah 4/30/2013 49 yo hispanic male, ho HIV(CD4 229), currently on HAART, course c/b AIDS, Presents with two days ho fever, SOB, blood tinged sputum, and visible hematuria. ROS: no skin rash, joint
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. HIV and the Kidney. Leah Haseley, MD. Presentation prepared by: LH NW AETC ECHO June 2012
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
NORTHWEST AIDS EDUCATION AND TRAINING CENTER HIV and the Kidney Leah Haseley, MD Presentation prepared by: LH NW AETC ECHO June 2012 Etiology of renal disease in HIV 1985- The virus 1995- The antivirals
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Mouse Models of Diabetic Nephropathy. Mount Sinai / Jefferson / Einstein / Minnesota Erwin Böttinger, PI Kumar Sharma, Co-PI
 Mouse Models of Diabetic Nephropathy Mount Sinai / Jefferson / Einstein / Minnesota Erwin Böttinger, PI Kumar Sharma, Co-PI Group Members Mount Sinai: Phenotyping, Molecular Pathology & Validation Erwin
Mouse Models of Diabetic Nephropathy Mount Sinai / Jefferson / Einstein / Minnesota Erwin Böttinger, PI Kumar Sharma, Co-PI Group Members Mount Sinai: Phenotyping, Molecular Pathology & Validation Erwin
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy. Patohistological Aspects
 HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
Enterprise Interest Nothing to declare Minimal change disease (MCD) related new electron microscopy findings in a patient on Levothyroxine sodium (LT) for hypothyroidism: A case report Dr. Ali Al-Omari
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
ANNEX FORM TO EXAMINE THE CAUSES OF ESRD I IDENTIFICATION. 1 Record number (patient chart) Name. 1.1 Date of birth / / 1.2 Sex:
 Name. 1.1 Date of birth / / 1.2 Sex:") Supplementary Material from Prevalence of clinically validated primary causes of end-stage renal disease (ESRD) in a State Capital in Northeastern Brazil ANNEX FORM TO EXAMINE THE CAUSES OF ESRD I IDENTIFICATION
Supplementary Material from Prevalence of clinically validated primary causes of end-stage renal disease (ESRD) in a State Capital in Northeastern Brazil ANNEX FORM TO EXAMINE THE CAUSES OF ESRD I IDENTIFICATION
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1
 Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
Management and treatment of glomerular diseases KDIGO Controversies Conference Part 1 Dr.M.Matinfar Assistant Professor of Internal Medicine & Nephrology IUMS -IKRC GENERAL PRINCIPLES IN THE MANAGEMENT
TOO MUCH OF A GOOD THING. Mitra Barahimi, MD, PGY-1 University of Washington Internal Medicine Residency Lauren Beste, MD, MSc Jeremiah Alexander, MD
 TOO MUCH OF A GOOD THING Mitra Barahimi, MD, PGY-1 University of Washington Internal Medicine Residency Lauren Beste, MD, MSc Jeremiah Alexander, MD Collaborators Lauren Beste, MD, MSc Jeremiah Alexander,
TOO MUCH OF A GOOD THING Mitra Barahimi, MD, PGY-1 University of Washington Internal Medicine Residency Lauren Beste, MD, MSc Jeremiah Alexander, MD Collaborators Lauren Beste, MD, MSc Jeremiah Alexander,
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
6/24/2009. Representative photo
 Advances in Internal Medicine UCSF CME June 24 th, 2009 Discussant: Dr. Harry Hollander A 62 year old woman presents with dyspnea on exertion and abdominal swelling. HPI Previously unlimited exercise tolerance,
Advances in Internal Medicine UCSF CME June 24 th, 2009 Discussant: Dr. Harry Hollander A 62 year old woman presents with dyspnea on exertion and abdominal swelling. HPI Previously unlimited exercise tolerance,
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH
 ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
ENAL VEIN ROMBOSIS WHAT WAS IT? DR.JANANI SANKAR UNIT DR. KEDARI NAGARJUNA, DNB P KKCTH RESENTING COMPLAINTS: u 9 ¾ yrs, boy u Fever, Loose stools 10 days back u Right sided Abdominal pain+ NVESTIGATIONS
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Multiple Myeloma Advances for clinical pathologists & histopathologists
 Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Diabetes on Renal Biopsy-Current Appraisal
 Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016
Diabetes on Renal Biopsy-Current Appraisal Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology, retired Washington University School of Medicine St. Louis, MO BNS 2016
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Proteinuria (Protein in the Urine) Basics
 Basics") Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
Proteinuria (Protein in the Urine) Basics OVERVIEW Proteinuria is the medical term for protein in the urine Urinary protein is detected by urine dipstick analysis, urinary protein: creatinine ratio (UP:C
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
For more information about how to cite these materials visit
 Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Frank Brosius, M.D, 2011 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Nephrotic Syndrome. Department of pediatrics The first affiliated hospital Sun Yat Sen University. Yue Zhihui ( 岳智慧 )
") Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia. Jess Hwang 11/8/12
 58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
Cardiorenal and Renocardiac Syndrome
 And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
And Renocardiac Syndrome A Vicious Cycle Cardiorenal and Renocardiac Syndrome Type 1 (acute) Acute HF results in acute kidney injury Type 2 Chronic cardiac dysfunction (eg, chronic HF) causes progressive
renoprotection therapy goals 208, 209
 Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Subject Index Aldosterone, plasminogen activator inhibitor-1 induction 163, 164, 168 Aminopeptidases angiotensin II processing 64 66, 214 diabetic expression 214, 215 Angiotensin I intrarenal compartmentalization
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Quantitative protein estimation of Urine
 Quantitative protein estimation of Urine 1 In a healthy renal and urinary tract system, the urine contains no protein or only trace amounts. The presence of increased amounts of protein in the urine can
Quantitative protein estimation of Urine 1 In a healthy renal and urinary tract system, the urine contains no protein or only trace amounts. The presence of increased amounts of protein in the urine can
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Case Presentation. 60 yo. AA male with h/o HIV/AIDS (Cd 4 count-89/ml, VL-undetectable) Whether he is a candidate for Renal Transplant?
 Whether he is a candidate for Renal Transplant?") Case Sonika Puri Case Presentation ESRD; on Hemodialysis since 07/2011 60 yo. AA male with h/o HIV/AIDS (Cd 4 count-89/ml, VL-undetectable) Whether he is a candidate for Renal Transplant? --Etiology of
Case Sonika Puri Case Presentation ESRD; on Hemodialysis since 07/2011 60 yo. AA male with h/o HIV/AIDS (Cd 4 count-89/ml, VL-undetectable) Whether he is a candidate for Renal Transplant? --Etiology of
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
AGING KIDNEY IN HIV DISEASE
 AGING KIDNEY IN HIV DISEASE Michael G. Shlipak, MD, MPH Professor of Medicine, Epidemiology and Biostatistics, UCSF Chief, General Internal Medicine, San Francisco VA Medical Center Kidney, Aging and HIV
AGING KIDNEY IN HIV DISEASE Michael G. Shlipak, MD, MPH Professor of Medicine, Epidemiology and Biostatistics, UCSF Chief, General Internal Medicine, San Francisco VA Medical Center Kidney, Aging and HIV
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018
 GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months
GLOMERULONEPHRITIS CLINICAL APPROACH TO GLOMERULAR DISEASE ACOI 2018 Disclosures Nothing to declare Case 1 44 yo Caucasian woman admitted from PCP with dyspnea and HTN Has not felt well for 3-4 months