Clinical Outcomes after Topography-based Corneal Laser Surgery with the. WaveLight Oculyzer and Topolyzer Platforms
|
|
|
- Edmund Lane
- 6 years ago
- Views:
Transcription
1 1 Clinical Outcomes after Topography-based Corneal Laser Surgery with the WaveLight Oculyzer and Topolyzer Platforms By Arthur B. Cummings, M.D. 1 and Nadia Mascharka, MSc 2 Corresponding Author: Arthur Cummings, M.D., Clinical Director, Wellington Eye Clinic, Dublin, Ireland Address: Wellington Eye Clinic, Suite 36, Beacon Hall, Beacon Court, Sandyford, Dublin 18, Ireland Telephone: Fax: abc@wellingtoneyeclinic.com Assistance with the preparation of this paper was provided by WaveLight AG. Dr. Cummings has no commercial or proprietary interest in WaveLight AG (Alcon Laboratories) or the products provided by these companies. Dr. Cummings does not serve as a consultant, reviewer, or evaluator for WaveLight AG. Nadia Mascharka is Product Manager Ophthalmology for WaveLight AG (Alcon Laboratories) and has a commercial and proprietary interest in this company. 1 Wellington Eye Clinic, Dublin, Ireland 2 WaveLight AG, Erlangen, Germany
2 2 Abstract Purpose: To explore the efficacy, safety, and predictability of topography-guided LASEK and LASIK treatments using the Allegro Oculyzer as compared to the Allegro Topolyzer platform (WaveLight AG). Methods: In this retrospective, non-comparative case series, 72 eyes were treated using Oculyzer data and 71 eyes were treated using Topolyzer data. 79 males and 64 females ranging in age from 21 to 63 years were included in the study. The 6 month post-operative UCVA and BSCVA of patients were compared to the pre-operative values. The data analysis was stratified based on the pre-operative refractions, separating patients into three categories: myopes, hyperopes, and mixed astigmats. Results: Of the pre-operative myopes in the Oculyzer group, 76% remained the same, 14% gained 1 line, and 5% gained 2 lines of visual acuity at 6 months. In the Topolyzer group, 69% remained the same, 25% gained 1 line, and 6% gained 2 lines of BSCVA. The outcomes of the pre-operative hyperopes and patients with mixed astigmatism are similarly reported. The difference in outcomes between the Oculyzer and Topolyzer cohorts in the myopes and patients with mixed astigmatism was not statistically significant. In the hyperopes, patients treated with the Oculyzer had superior UCVAs to those treated with the Topolyzer platform. Conclusions: This case series demonstrates that the Oculyzer and Topolyzer are both effective tools in topography-guided corneal laser surgery. In myopes and patients with mixed astigmatism, both systems were comparable in efficacy and safety. In the hyperopes, the resultant UCVA in the Oculyzer cohort was slightly superior.
3 3 Introduction Whether primary or secondary laser refractive surgery is contemplated, patients with symptoms such as glare, halos, and starbursts require a customized treatment. 1 The Allegretto Eye-Q system (WaveLight AG, Erlangen, Germany) provides five options for customization including: Wavefront Optimized ablation profiles Wavefront-guided ablation profiles Oculyzer (Pentacam)-guided - Scheimpflug using OcuLink software Topolyzer - Topography-guided (placido disk) using T-CAT (Topography-Guided Customized Ablation Treatment) software, or Custom-Q - Pre-determining the Q-value If the decision is made to proceed with a topography-guided treatment, surgeons can then select a treatment based on data generated by the Oculyzer or the Topolyzer. The Oculyzer and Topolyzer are diagnostic instruments that have been converted to Class 2b devices in order to use their data to modify an ablation profile. Oculink and T-CAT refer to the portal software on the laser s laptop that link the Oculyzer data via Oculink to the laser and the Topolyzer data via T-CAT to the laser. There are patients who have aberrations of too great a magnitude for accurate wavefront sensing. 2 The most common reason for an unacceptable wavefront map is that it can not be validated due to issues such as significant corneal irregularity, corneal or lens opacities, dry eye, keratoconus, or forme fruste keratoconus. 3-4 We found that, in the majority of cases where we were unable to obtain validated wavefront maps, that we were able to acquire good quality topography maps with both the Oculyzer and the Topolyzer. If a difference was found in the
4 4 quality of maps produced by these two devices, a treatment based on the best quality of validated data was used. The Oculyzer is optimally designed for use when the aberrations or irregularities are more centrally located and the Topolyzer, which captures 22,000 points of measurement with an interactive elevation map, 5 is optimally used when the irregularities are located more peripherally. The Topolyzer, a placido disk system, produces a central scotoma where the camera is located and central data must be extrapolated. On the other hand, the Oculyzer features a Scheimpflug rotating camera that scans the eye either 25 times or 50 times depending on the chosen setting. As a result, a wealth of data points is acquired for the central cornea. A wavefront-guided customized treatment assumes that most of a given patient's ocular aberrations can be corrected by reshaping the cornea. However, if a patient has normal topography but abnormal wavefront maps, a wavefront-guided treatment could actually induce aberrations in the cornea (Holland SP, Lin D. Topographically-directed PRK for irregular astigmatism following penetrating keratoplasty. Poster presented at: 2006 AAO Annual Meeting, Las Vegas, Nevada). The topography-guided ablation, which is a customized ablation that uses topography instead of a wavefront map as the basis for treatment, 6 is generally reserved for eyes in which aberrations exist at the level of the corneal surface. These eyes typically have a history of prior refractive surgery such as radial keratotomy or excimer ablations, which were decentered. The topography-guided ablation is also useful in eyes with severe corneal irregularities, which may include abrupt contour changes over a small area of the cornea caused by conditions such as dry eye syndrome, corneal scars and forme fruste keratoconus. Topography is the only measuring tool that can detect the hills and valleys produced by scarring
5 5 that block the visualization of aberrometry patterns from the retina. In addition, topographyguided procedures are also commonly used for the treatment of hyperopia, especially where angle kappa is present, as the topography-guided ablation profile automatically decenters the treatment to reduce the angle kappa. This retrospective, non-comparative case series compares the efficacy, safety, and predictability of topography-guided LASEK and LASIK treatments using the Allegro Oculyzer and the Allegro Topolyzer platforms. Materials and Methods Seventy-nine Caucasian males and 64 Caucasian females were included for analysis. The Oculyzer cohort had an age range of from 21 to 52 years, with a median age of 34 years. The Topolyzer cohort had an age range of from 26 to 63 years, with a median age of 36 years. Patients included in this analysis had pre-operative pachymetry greater than or equal to 460 microns (µm) for a LASEK procedure and greater than or equal to 500 microns for a LASIK procedure. In addition, LASEK patients were required to have an estimated post-procedure residual corneal bed of at least 380 microns. LASIK patients were required to have an estimated post-procedure residual corneal bed of at least 250 microns. Kanellopoulos, 1 in a study exploring topography-guided custom retreatments of symptomatic eyes, required that patients have enough corneal tissue to leave at least 280 µm of stromal bed after the planned retreatment, which is similar to the criteria adopted in this study. The corneal thickness and predicted stromal bed depth were based on pre-operative records and on pre-procedure pachymetry readings. Excluded ophthalmic conditions included clinically significant dry eyes, forme fruste keratoconus, and keratoconus. Patients who had collagen vascular disorders, uncontrolled diabetes, or who were pregnant were excluded from this analysis. 138 patients (96.5%)
6 6 underwent surgery as an initial refractive procedure, whereas 5 eyes (3.5%) underwent surgery as a secondary enhancement. The secondary enhancements included two cases of small optical zones, two cases of decentered optical zones, and one case of a small, decentered optical zone. All five cases had residual myopia and validated wavefront maps could not be acquired. The pre-operative evaluations of patients included refractions (manifest, cycloplegic, and wavefront), measurements of the uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), scotopic pupil size (Procyon P3000, Haag-Streit UK), and topography with both the Oculyzer and Topolyzer. The UCVA and BSCVA were evaluated under photopic conditions with a luminance level of 85 candela/m 2. Manifest refractions were performed using plus-to-blur and fogging techniques to confirm the spherical endpoint. In order to determine whether data generated by the Oculyzer or Topolyzer would drive the procedure, a number of factors were considered. For each study eye, four maps were taken using the Oculyzer and eight maps were taken using the Topolyzer as the number of maps captured by each system differs. In our experience, Oculyzer maps have been more repeatable than the Topolyzer maps, consistently measuring 100% of the cornea. Because of the greater variability we have observed with Topolyzer maps, we decided to capture eight maps and average the data. The portal software indicated that the average quality of data with the Topolyzer maps has ranged between measuring 90 to 100% of the cornea. The repeatability of the maps generated by both devices was compared and the more consistent method was used in planning the treatment. 1 When the maps were of comparable quality, if the topographical errors were more centrally located, within 3 millimeters (mm) of the central cornea, the Oculyzer platform was selected for
7 7 use in the treatment. If the corneal irregularities were situated more peripherally, outside the 3 mm central corneal zone, the Topolyzer platform was chosen for use in the treatment. The rationale for this determination was based on the design of the devices. With the Oculyzer, the beam of light rotates 360 degrees to capture the entire cornea with a higher density of points concentrated in the central cornea. In contrast, the Topolyzer is a placido disk system where a camera is used to image reflections from the corneal surface. Because the camera is positioned in the center of the topographer, there is a small area in the center of the topography map where data must be interpolated. Informed consent was obtained from the subjects after the nature of the procedure had been fully explained. The flaps in all primary cases required a diameter greater than 8.5 mm and were created using the Rondo microkeratome (WaveLight AG) or the Hansatome XP microkeratome (Bausch & Lomb). Any re-treatments were performed by re-lifting the flap. All LASEK and LASIK procedures were performed in the Wellington Eye Clinic, Dublin, Ireland by Dr. Cummings using the Allegretto Eye-Q 400 Hz excimer laser (WaveLight AG). All refractive procedures were completed from October 2006 to March The target refraction in all cases was a plano prescription with the exception of 4 eyes where was targeted in order to achieve monovision. UCVA, BSCVA, manifest refraction, and corneal topography were evaluated at 1 month, 3 months, and 6 months post-operatively. Statistical significance was accepted at the 95% confidence interval (P < 0.05).
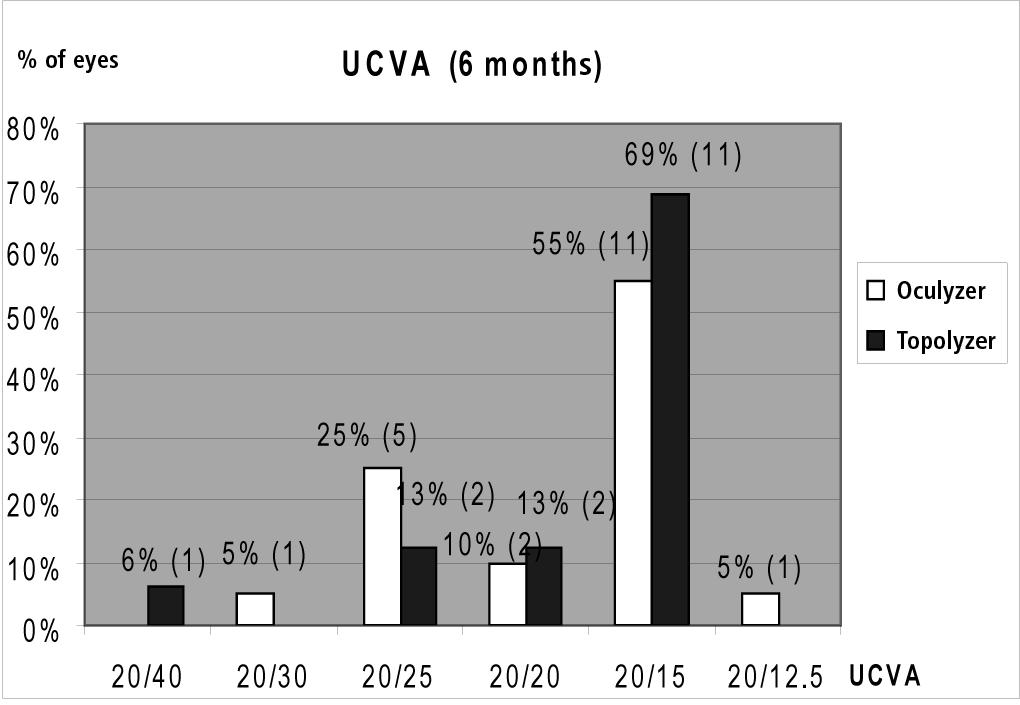
8 8 Results The results are stratified into three parts based on the patient s pre-operative refractive status: myopia, hyperopia, or mixed astigmatism. Pre-operative Myopia Group In the Oculyzer cohort, there were 21 males and 13 females, with 5 receiving LASEK and 29 receiving LASIK. In the Topolyzer cohort, there were 13 males and 14 females, with 7 receiving LASEK and 20 receiving LASIK. Two of the Oculyzer cohort and two of the Topolyzer cohort were secondary enhancements. With regards to efficacy, the UCVA results at 6 months are shown in Figure 1. In the Oculyzer group (20 patients), the majority of patients (55%, 11 patients) achieved a UCVA of 20/15 and in the Topolyzer group (16 patients), the majority of patients (69%, 11 patients) achieved a UCVA of 20/15. In the two cohorts, the difference in the lines of visual acuity lost, remaining the same, or gained was not statistically significant by the t-test (P = 0.21). Comparing the BSCVA at 6 months, in the Oculyzer group (21 patients), 5% (1 patient) had a BSCVA of 20/25, 10% (2 patients) had a BSCVA of 20/20, 76% (16 patients) had a BSCVA of 20/15, and 10% (2 patients) had a BSCVA of 20/12.5. In the Topolyzer group (16 patients), 13% (2 patients) of patients had a BSCVA of 20/20 and 88% (14 patients) had a BSCVA of 20/15.
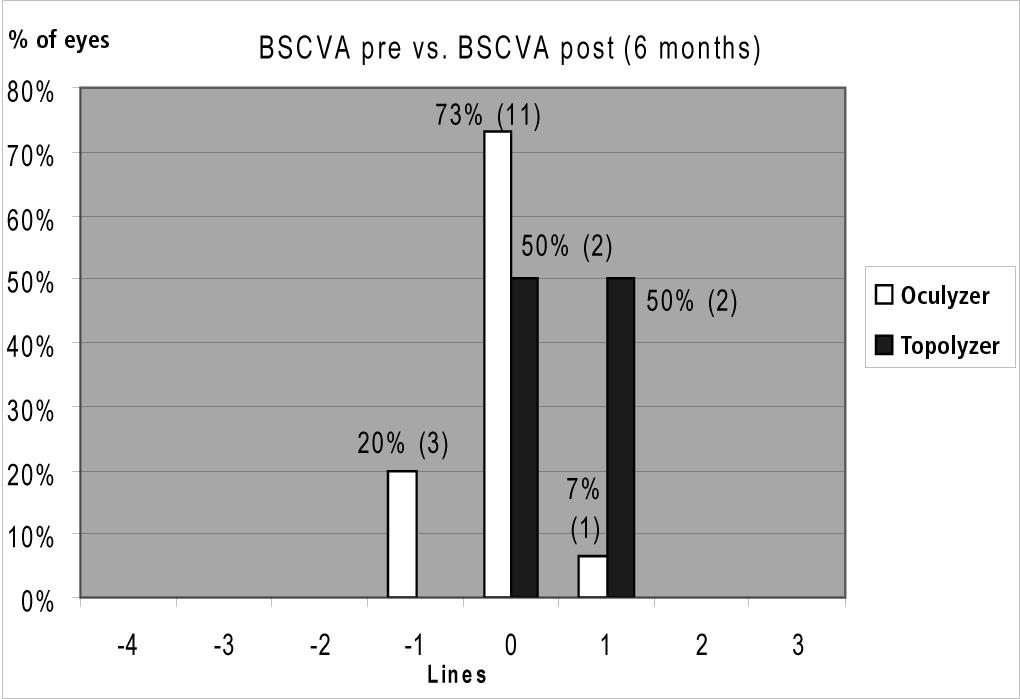
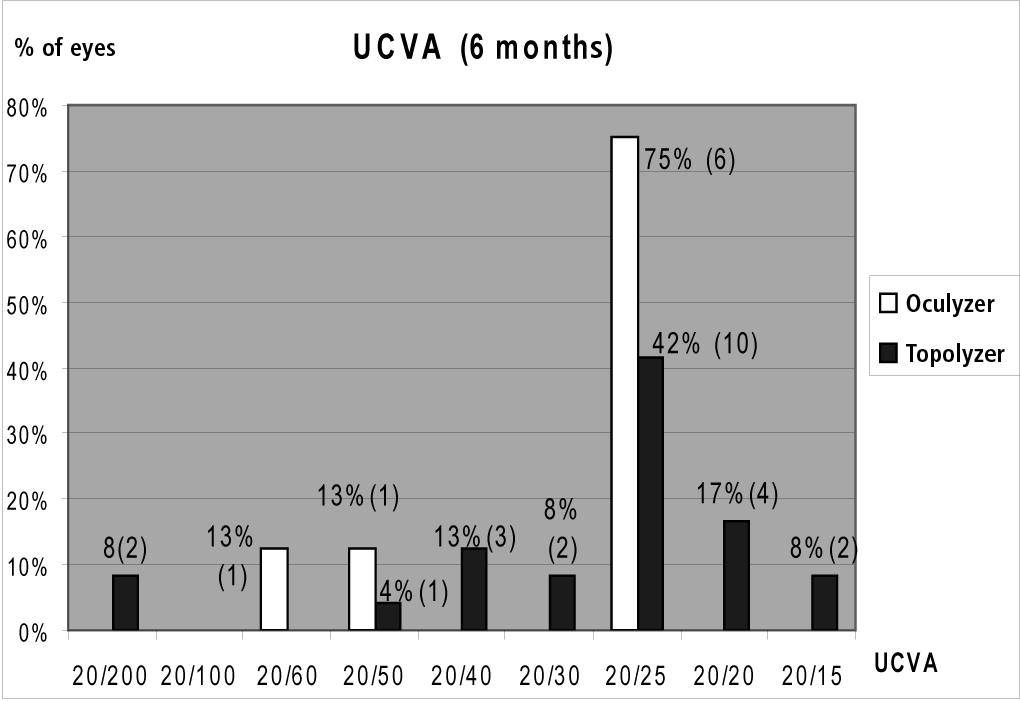
9 9 With regards to safety at 6 months, the results are shown in Figure 2. Comparing the preoperative BSCVA and the 6 month post-procedure BSCVA, in the Oculyzer group (15 patients), the majority of patients (73%, 11 patients) remained the same pre- and post-operatively. In the Topolyzer group (4 patients), 50% (2 patients) showed no change in BSCVA and 50% (2 patients) gained 1 line of visual acuity. Comparing the Oculyzer and Topolyzer groups, the difference in the number of visual acuity lines lost, remaining the same, or gained was not statistically significant by the t-test (P = 0.12). Pre-operative Hyperopia Group In the Oculyzer cohort, there were 11 males and 5 females, with all 16 patients receiving LASIK. In the Topolyzer cohort, there were 19 males and 14 females, with 1 receiving LASEK and 32 receiving LASIK. With regards to efficacy at 6 months, the results are shown in Figure 3. In the Oculyzer group (8 patients), 75% (6 patients) achieved a UCVA of 20/25. In the Topolyzer group (24 patients), 42% (10 patients) had a UCVA of 20/25 and 17% (4 patients) had a UCVA of 20/20. A comparison of lines of visual acuity lost, remaining the same, or gained in the Oculyzer and Topolyzer group revealed that the difference was not statistically significant by the t-test (P = 0.39). Examining the BSCVA post-procedure at 6 months, in the Oculyzer group (8 patients), 40% (4 patients) had a BSCVA of 20/25, 50% (5 patients) had a BSCVA of 20/20, and 10% (1 patient) had a BSCVA of 20/15. In the Topolyzer group (23 patients), 4% (1 patient) had a BSCVA of
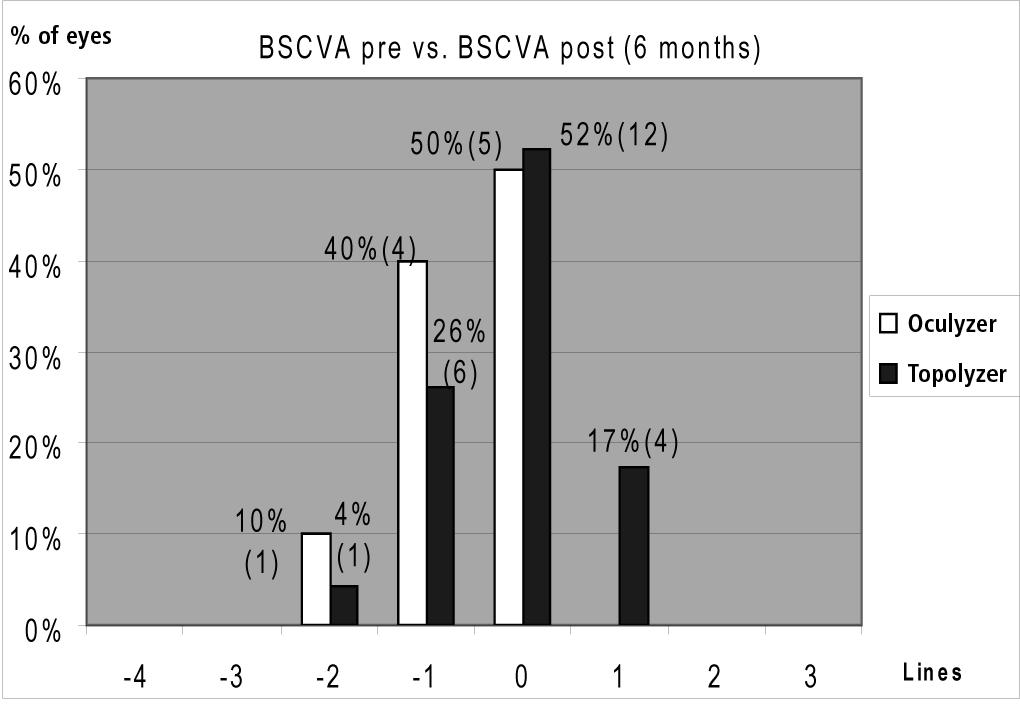
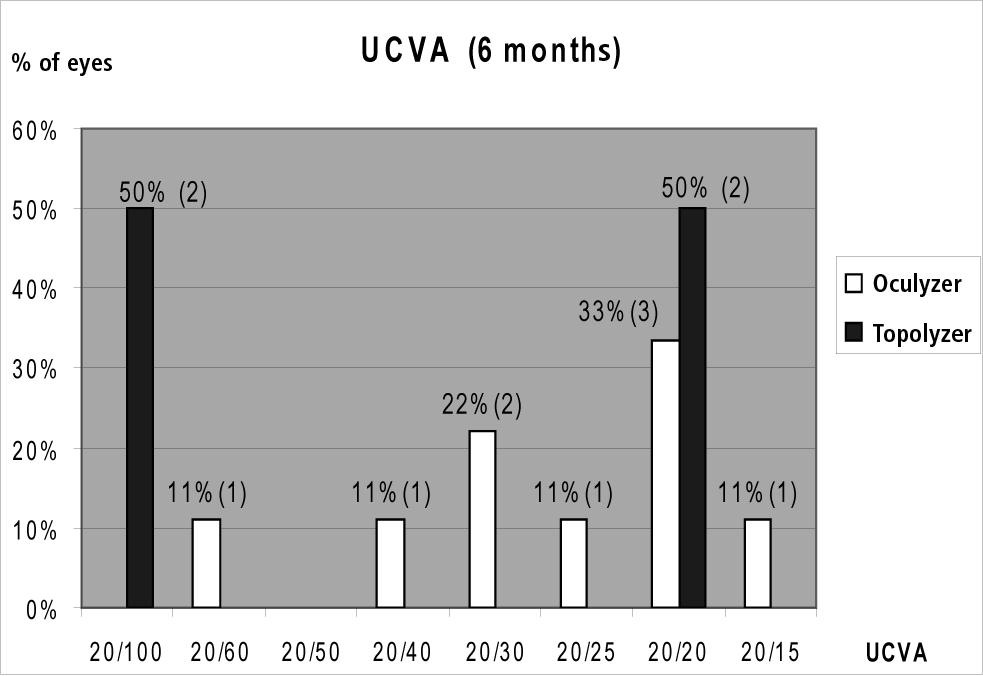
10 10 20/50, 4% (1 patient) had a BSCVA of 20/30, 26% (6 patients) had a BSCVA of 20/25, 48% (11 patients) had a BSCVA of 20/20, and 17% (4 patients) had a BSCVA of 20/15. Addressing the safety of the procedure at 6 months, the results are shown in Figure 4. In the Oculyzer group (10 patients), 40% (4 patients) lost 1 line of BSCVA and 50% (5 patients) remained the same pre- and post-operatively. In the Topolyzer group (23 patients), 26% (6 patients) lost 1 line of BSCVA, 52% (12 patients) remained the same pre- and post-operatively, and 17% (4 patients) gained 1 line of BSCVA. The difference in the number of visual acuity lines lost, remaining the same, or gained in the Oculyzer and Topolyzer groups was not statistically significant by the t-test (P = 0.07). Pre-operative Mixed Astigmatism Group In the Oculyzer cohort, there were 12 males and 10 females with 4 patients receiving LASEK and 18 patients receiving LASIK. The Topolyzer cohort consisted of 3 males and 8 females, with 3 receiving LASEK and 8 receiving LASIK. One patient in the Oculyzer cohort had a secondary enhancement. In regards to the efficacy of the procedure at 6 months, the results are shown in Figure 5. In the Oculyzer group (9 patients), 22% (2 patients) had a UCVA of 20/30 and 33% (3 patients) had a UCVA of 20/20. In the Topolyzer group (4 patients), 50% (2 patients) had a UCVA of 20/100 and 50% (2 patients) had a UCVA of 20/20. The difference in the number of visual acuity lines lost, remaining the same, or gained in the Oculyzer and Topolyzer groups was not statistically significant by the t-test (P = 0.18).
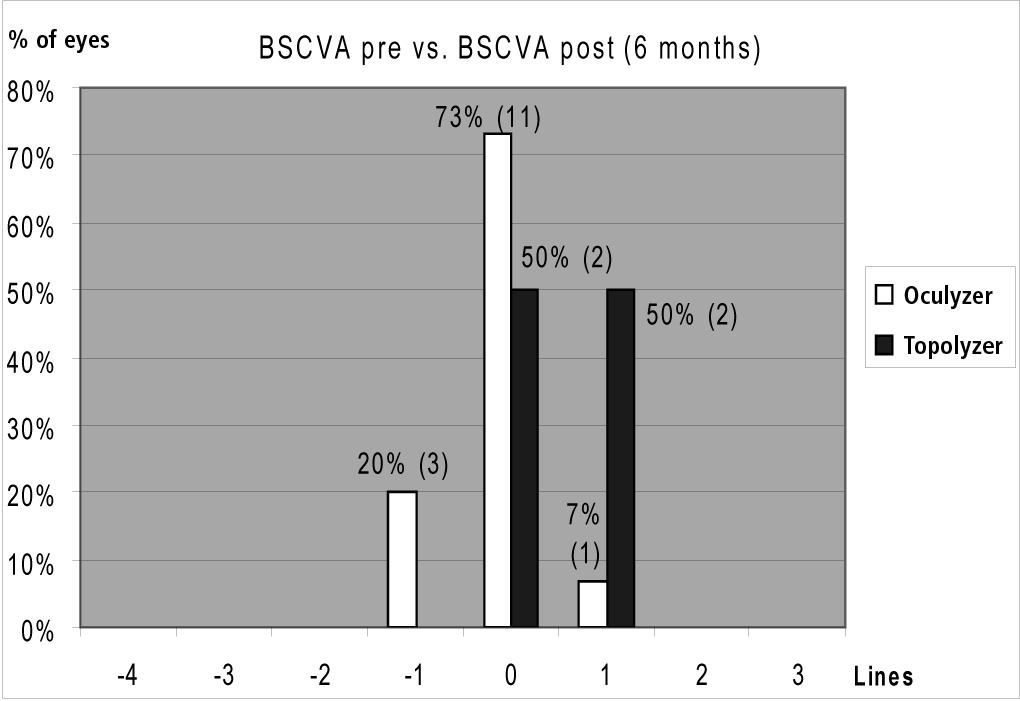
11 11 Looking at the BSCVA at 6 months, in the Oculyzer group (15 patients), 7% (1 patient) had a BSCVA of 20/50, 7% (1 patient) had a BSCVA of 20/40, 7% (1 patient) had a BSCVA of 20/30, 20% (3 patients) had a BSCVA of 20/20, and 60% (9 patients) had a BSCVA of 20/15. In the Topolyzer group (4 patients), 25% (1 patient) had a BSCVA of 20/20 and 75% (3 patients) had a BSCVA of 20/15. Exploring the safety of the procedure at 6 months, the results are shown in Figure 6. In the Oculyzer group (15 patients), 20% (3 patients) lost 1 line of BSCVA and 73% (11 patients) remained the same pre- and post-operatively. In the Topolyzer group (4 patients), 50% (2 patients) remained the same pre- and post-operatively and 50% (2 patients) gained 1 line of BSCVA. The difference in the number of visual acuity lines lost, remaining the same, or gained in the Oculyzer and Topolyzer groups was not statistically significant by the t-test (P = 0.07). Tables 1 and 2 address the refractive predictability of the procedure at 6 months for all three cohorts and show that the predictability was good with both the Oculyzer and Topolyzer. This case series suggests that the predictability of achieving the target refraction with both devices in the pre-procedure myopic group was comparable. In the hyperopic group, the predictability was slightly better with the Oculyzer, but in the mixed astigmatism group, the predictability was slightly better with the Topolyzer. In some cases, it was found that the Oculyzer acquired good maps while the Topolyzer maps were not acceptable on the same eye. The Oculyzer maps were generally found to be consistently satisfactory.
12 12 Discussion Topography-guided procedures using two different topographical systems provided good outcomes in cases where wavefront maps could not be reliably acquired. Our experience with the WaveLight platform has shown that, in approximately 20 to 30% of seemingly normal eyes, good quality wavefront maps can not be acquired. It is our view that if wavefront maps cannot be validated, they should not be used for wavefront-guided treatments. The greatest potential for topography-guided treatments may be in severely aberrated corneas with decreased BSCVA for which even refraction is unreliable. The indications for topography-guided treatments include decentered ablations, the enlargement of the optical zone, irregular astigmatism following penetrating keratoplasty, 7-8 RK, asymmetrical astigmatism, keratoconus, and in hyperopic eyes with a decentered angle kappa. Because its measurements are based purely on the corneal surface, topography-guided treatments can also be used in cases with media opacities such as corneal scars. 6 It should also be noted that topography-guided treatments eliminate issues dealing with the pupil centroid as the pupil is undilated during topography and tomography as well as during the laser treatment. In comparison, wavefront maps must be acquired through dilated pupils while the surgery is performed with the pupil undilated, bringing the issue of a pupil centroid shift to the forefront. Topography-guided ablations attempt to re-contour the corneal surface to match an ideal curve and may have advantages over wavefront-guided treatments for complicated eyes. Holland and Lin (Holland SP, Lin D. Topographically-directed PRK for irregular astigmatism following penetrating keratoplasty. Poster presented at: 2006 AAO Annual Meeting, Las Vegas, Nevada) noted that in topography-guided treatments, the ablation profile is calculated based on the
13 13 topographical height maps, which are then adjusted based on the eye's overall refraction. With the Oculyzer, the ablation profiles are calculated from height maps obtained with the device. The Topolyzer creates customized algorithms by averaging up to eight topographical maps per eye and uses a Zernike-based algorithm to create an ablation profile that corrects for corneal irregularities. In addition, to preserve or re-establish the cornea s natural asphericity, it is possible to factor a Q-value into topography-guided treatments. 9 With primary treatments, the targeted Q-value was entered as the pre-operative value. For example, if the pre-operative value was -0.34, then was entered as the post-operative target. In secondary cases, the targeted Q-value was always entered as zero. In these cases, the pre-operative Q-values were always positive, indicating an oblate cornea. A disadvantage of topography-guided ablations is that, because the data concentrates mainly on the corneal contour, the procedure doesn t take into account the rest of the refracting media. Because topography-guided ablations only use data from the anterior corneal surface, one must compensate for the lack of refractive data collected by the topography system. This is accomplished by looking closely at the higher order ablation profile (the profile that the laser is going to use when the refraction is entered as zero or plano). A decision is made as to how much myopia or hyperopia the higher order ablation profile is going to induce and then, in order to compensate, the refraction entered into the ablation profile is modified. This is the basis of TNT (Topography Neutralization Technique) as described by Lin et al. 10 Other studies have explored the use of topography-guided ablations using the Allegretto Wave excimer laser in the treatment of aberrated corneas and decentered ablations and have found
14 topography-guided treatments to be of benefit Spadea and Di Gregorio 17 demonstrated the 14 safety and efficacy of this topography-guided approach in improving the BSCVA, contrast sensitivity, and aberrations of subjects. A further refinement was used in deciding whether the Oculyzer or the Topolyzer data would be used. Patients were asked to sketch the higher order errors that they were experiencing with their best spectacle-corrected vision and these higher order errors were compared to the higher order ablation profiles of the Oculyzer and Topolyzer platforms. In most cases, these higher order ablation profiles looked very similar if not identical, but when they differed, the ablation profile that best matched the patient s subjective complaints was selected. Specifically, patients were asked to describe or sketch a projected large white square and a smaller white dot looking through their full distance correction in the phoropter (see Figure 7). Patients were asked to sketch the edges of the square and we observed whether the edges were neat and tidy, blurred and smudged, whether there was a ghost image, or whether the corners were regular. When sketching the dot, we observed whether there was a halo around the dot, a half moon, or whether there were any spokes or starbursts radiating from the dot. These sketches served to illustrate the patient s higher order errors and provided us with additional information as to selecting the appropriate device for the treatment. We have found that, with experience in the use of these platforms, the ability to reliably achieve the predicted refractive outcome improves as does the ability to perfect the resultant visual quality. The Oculyzer, which uses tomography, is superior for use when the aberrations or irregularities are more centrally located in the cornea. This Scheimpflug technology is designed
15 15 to perform more central cornea data capture, but can be affected by eye movement and by any haze or clouding of the cornea such as sub-epithelial haze or arcus senilis. The Topolyzer, using the placido disk, is superior when the irregularities are located more peripherally. Placido disk technology is recognized as an accurate mode of obtaining topographical data, but does not provide full surface information and demonstrates less accuracy when the corneal issues are more centrally located. The limitation of this study is that it is a non-comparative case series rather than a randomized trial. However, because the optimal treatment selected was based on the repeatability of the maps and the location of the topographical errors, it would not have been possible to randomize patients as each case was treated with an individualized approach. This series shows that both the Oculyzer and Topolyzer provide good, comparable outcomes in pre-operative myopes and in patients with mixed astigmatism. The Oculyzer resulted in slightly better UCVAs in the pre-operative hyperopes. When a customized treatment is needed, but accurate wavefront maps cannot be acquired, topography-guided laser procedures are a sound treatment modality. References 1. Kanellopoulos JA. Topography-guided custom retreatments in 27 symptomatic eyes. J Refract Surg. 2005;21:S513-S Mrochen M, Krueger RR, Bueeler M, Seiler T. Aberration-sensing and wavefront-guided laser in situ keratomileusis: management of decentered ablation. J Refract Surg. 2002;18:
16 16 3. Chalita MR, Chavala S, Xu M, Krueger RR. Wavefront analysis in post-lasik eyes and its correlation with visual symptoms, refraction, and topography. Ophthalmology. 2004;111: Montague AA, Manche EE. CustomVue laser in situ keratomileusis treatment after previous keratorefractive surgery. J Cataract Refract Surg. 2006;32: Jankov M. Topography for corneal irregularities. Cataract & Refractive Surgery Today. 2004: Campbell C. Corneal topography in corneal ablations. In: McRae SM, Krueger RR, Applegate RA eds. Customized Corneal Ablation: The Quest for Supervision. Thorofare, NJ: SLACK Inc.; 2001: Mularoni A, Laffi GL, Bassein L, Tassinari G. Two-step LASIK with topography-guided ablation to correct astigmatism after penetrating keratoplasty. J Refract Surg. 2006;22: Rajan MS, O'Brart DP, Patel P, Falcon MG, Marshall J. Topography-guided customized laser-assisted subepithelial keratectomy for the treatment of postkeratoplasty astigmatism. J Cataract Refract Surg. 2006;32: Seiler T, Dastjerdi MH. Customized corneal ablation. Curr Opin Ophthalmol. 2002;13: Lin DT, Holland SR, Rocha KM, Krueger RR. Method for optimizing topography-guided ablation of highly aberrated eyes with the Allegretto Wave Excimer Laser. J Refract Surg. 2008;24:S Jankov MR, Panagopoulou SI, Tsiklis NS, Hajitanasis GC, Aslanides M, Pallikaris G. Topography-guided treatment of irregular astigmatism with the Wavelight excimer laser. J Refract Surg. 2006;22:
17 Kymionis GD, Panagopoulou SI, Aslanides IM, Plainis S, Astyrakakis N, Pallikaris IG. Topographically supported customized ablation for the management of decentered laser in situ keratomileusis. Am J Ophthalmol. 2004;137: Alessio G, Boscia F, La Tegola MG, Sborgia C. Topography-driven excimer laser for the retreatment of decentralized myopic photorefractive keratectomy. Ophthalmology. 2001;108: Lee DH, Seo SJ, Shin SC. Topography-guided excimer laser ablation of irregular cornea resulting from penetrating injury. J Cataract Refract Surg. 2002;28: Alessio G, Boscia F, La Tegola MG, Sborgia C. Corneal interactive programmed topographic ablation customized photorefractive keratectomy for correction of post-keratoplasty astigmatism. Ophthalmology. 2001;108: Knorz MC, Jendritza B. Topographically-guided laser in situ keratomileusis to treat corneal irregularities. Ophthalmology. 2000;107: Spadea L, Di Gregorio A. Enhancement outcomes after photorefractive keratectomy and laser in situ keratomileusis using topographically guided excimer laser photoablation. J Cataract Refract Surg. 2005;31:
18 18 Tables TABLE 1 Clinical Data for Eyes That Received Topography-Guided Laser Surgery with the ALLEGRO Oculyzer Myopia Group Hyperopia Group Mixed Astigmatism Group Pre-op 6-Month Post-op Pre-op 6-Month Post-op Pre-op 6-Month Post-op Number of eyes Number of. Eyes within 0 (0) 20 (95) 3 (19) 8 (80) 6 (27) 9 (60) ± 0.5 D (%) Sphere [Diopters] ± ± ± ± ± ± 0.67 (range) (-8.25 to -1.00) (-1.25 to 0.25) (0.25 to 4.75) (-1.25 to 0.25) (4.50 to -6.25) (-1.50 to 0.75) Confidence Interval (Sphere) 0.14* 0.28* 0.34* Cylinder [Diopters] ± ± ± ± ± ± 0.94 (range) (-2.5 to -0.25) (-0.75 to 0.0) (0.0 to 4.25) (-1.5 to 0.0) (-8.0 to 3.75) (-4 to 0.0) Confidence Interval (Cylinder) 0.11* 0.32* 0.47* * Level of significance α = 0.05 TABLE 2 Clinical Data for Eyes That Received Topography-Guided Laser Surgery with the ALLEGRO Topolyzer Myopia Group Hyperopia Group Mixed Astigmatism Group Pre-op 6-Month Post-op Pre-op 6-Month Post-op Pre-op 6-Month Post-op Number of eyes Number of Eyes within ± 0.5 D (%) 3 (11) 14 (88) 3 (9) 18 (78) 1 (9) 2 (50)
19 19 Sphere (Diopters) ± ± ± ± ± ± 1.01 (range) (-6.50 to -0.25) (-1.00 to -0.75) (0.00 to 4.75) (-2.0 to 0.75) (-1.5 to 5.75) (-1.50 to 0.25) Confidence Interval (Sphere) 0.19* 0.28* 0.99* Cylinder (Diopters) (range) ± 1.15 (-4.5 to -0.25) ± 0.26 (-0.75 to 0.00) 1.14 ± 1.18 (0.0 to 4.0) ± 0.51 (-1.25 to 0.75) ± 2.21 (-3.50 to 3.50) ± 0.0 Confidence Interval (Cylinder) 0.15* 0.32* - * Level of significance α = 0.05 Figure Legends Figure 1. Graph of the efficacy data for the pre-operative myopia group. This graph compares the uncorrected visual acuity results at 6 months for the Oculyzer (Oculink) and the Topolyzer (T-CAT) cohorts. The actual number of patients represented by the percentages is in parentheses. Oculink and T-CAT refer to the portal software on the laser s laptop that link the Oculyzer data via Oculink to the laser and the Topolyzer data via T-CAT to the laser. Figure 2. Graph of the safety data for the pre-operative myopia group. This graph compares the pre-operative BSCVA to the 6 month post-procedure BSCVA. The actual number of patients represented by the percentages is in parentheses. Figure 3. Graph of the efficacy data for the pre-operative hyperopia group. This graph compares the uncorrected visual acuity results at 6 months for the Oculyzer and the Topolyzer cohorts. The actual number of patients represented by the percentages is in parentheses. Figure 4. Graph of the safety data for the pre-operative hyperopia group. This graph compares the pre-operative BSCVA to the 6 month post-procedure BSCVA. The actual number of patients represented by the percentages is in parentheses.
20 20 Figure 5. Graph of the efficacy data for the pre-operative mixed astigmatism group. This graph compares the uncorrected visual acuity results at 6 months for the Oculyzer and the Topolyzer cohorts. The actual number of patients represented by the percentages is in parentheses. Figure 6. Graph of the safety data for the pre-operative mixed astigmatism group. This graph compares the pre-operative BSCVA to the 6 month post-procedure BSCVA. The actual number of patients represented by the percentages is in parentheses. Figure 7. This figure shows the visual quality when a patient looks at a projected white dot and a large white square with best correction. If there are no quality problems, then a wavefront optimized treatment is indicated (this does not include any higher order ablation profile). When there are visual quality issues present, then a topography-guided procedure is indicated if wavefront data of sufficient quality cannot be obtained. If both Topolyzer and Oculyzer data is available, then the higher order ablation profile (when the refractive data is entered as zero) that best matches the patient sketch of the aberrations is used.
21
22
23
24
25
26







27 Figure 7: Images as seen by patient with full correction Ablation profile Higher Order Ablation Example 1: No complaints WFO profile No higher order ablation Example 2: Irregular halos, glare T-CAT ablation profile Higher order ablation Example 3: Irregular halos, glare Oculink ablation profile Higher order ablation
The pinnacle of refractive performance.
 The pinnacle of refractive performance. WaveLight REFRACTIVE PORTFOLIO Advancing REFRACTIVE SURGERY Contoura Vision sets a new standard in LASIK outcomes More than 98% of patients would choose it again.
The pinnacle of refractive performance. WaveLight REFRACTIVE PORTFOLIO Advancing REFRACTIVE SURGERY Contoura Vision sets a new standard in LASIK outcomes More than 98% of patients would choose it again.
Wavefront-optimized Versus Wavefrontguided LASIK for Myopic Astigmatism With the ALLEGRETTO WAVE: Three-month Results of a Prospective FDA Trial
 Wavefront-optimized Versus Wavefrontguided LASIK for Myopic Astigmatism With the ALLEGRETTO WAVE: Three-month Results of a Prospective FDA Trial Karl G. Stonecipher, MD; Guy M. Kezirian, MD, FACS ABSTRACT
Wavefront-optimized Versus Wavefrontguided LASIK for Myopic Astigmatism With the ALLEGRETTO WAVE: Three-month Results of a Prospective FDA Trial Karl G. Stonecipher, MD; Guy M. Kezirian, MD, FACS ABSTRACT
Contoura TM Vision Correction
 Contoura TM Vision Correction Fernando Faria Correia, Financial Disclosures: Alcon/Wavelight Cairo (Egypt) 26/01/2018 Topography-guided ablations Topography guided ablations Evolution from complicated
Contoura TM Vision Correction Fernando Faria Correia, Financial Disclosures: Alcon/Wavelight Cairo (Egypt) 26/01/2018 Topography-guided ablations Topography guided ablations Evolution from complicated
Four-year Postoperative Results of the US ALLEGRETTO WAVE Clinical Trial for the Treatment of Hyperopia
 Four-year Postoperative Results of the US ALLEGRETTO WAVE Clinical Trial for the Treatment of Hyperopia Guy M. Kezirian, MD, FACS; Charles R. Moore, MD, FICS; Karl G. Stonecipher, MD; SurgiVision Consultants
Four-year Postoperative Results of the US ALLEGRETTO WAVE Clinical Trial for the Treatment of Hyperopia Guy M. Kezirian, MD, FACS; Charles R. Moore, MD, FICS; Karl G. Stonecipher, MD; SurgiVision Consultants
Summary Recommendations for Keratorefractive Laser Surgery June 2013
 Summary Recommendations for Keratorefractive Laser Surgery June 2013 Background Laser assisted in-situ keratomileusis (LASIK) surgery is the most commonly performed keratorefractive surgery; altering the
Summary Recommendations for Keratorefractive Laser Surgery June 2013 Background Laser assisted in-situ keratomileusis (LASIK) surgery is the most commonly performed keratorefractive surgery; altering the
Corneal transplantation (CT) is one of the most commonly
 is one of the most commonly") CLINICAL SCIENCE Irregular Astigmatism After Corneal Transplantation Efficacy and Safety of Topography-Guided Treatment Inês Laíns, MD, MSc,* Andreia M. Rosa, MD,* Marta Guerra, MD, MSc,* Cristina Tavares,
CLINICAL SCIENCE Irregular Astigmatism After Corneal Transplantation Efficacy and Safety of Topography-Guided Treatment Inês Laíns, MD, MSc,* Andreia M. Rosa, MD,* Marta Guerra, MD, MSc,* Cristina Tavares,
Simultaneous Topography-guided Surface Ablation with Collagen Cross-linking for Keratoconus
 IJKECD Case series Simultaneous Topography-guided Surface Ablation with Collagen 10.5005/jp-journals-10025-1124 Cross-linking for Keratoconus Simultaneous Topography-guided Surface Ablation with Collagen
IJKECD Case series Simultaneous Topography-guided Surface Ablation with Collagen 10.5005/jp-journals-10025-1124 Cross-linking for Keratoconus Simultaneous Topography-guided Surface Ablation with Collagen
Moving from Rx to measured
 Moving from Rx to measured The news magazine of the American Society of Cataract & Refractive Surgery Supplement to EyeWorld Daily News Sunday, May 7, 2017 Contoura Vision TopographyGuided Ablation Algorithms
Moving from Rx to measured The news magazine of the American Society of Cataract & Refractive Surgery Supplement to EyeWorld Daily News Sunday, May 7, 2017 Contoura Vision TopographyGuided Ablation Algorithms
Cataract Surgery in the Patient with a History of LASIK or PRK
 Cataract Surgery in the Patient with a History of LASIK or PRK #56996-RS April 2018 Sebastian Lesniak, MD Matossian Eye Associates None Disclosures Bio Matossian Eye Associates, Hopewell NJ, 7/2015 Present
Cataract Surgery in the Patient with a History of LASIK or PRK #56996-RS April 2018 Sebastian Lesniak, MD Matossian Eye Associates None Disclosures Bio Matossian Eye Associates, Hopewell NJ, 7/2015 Present
2/7/18. Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE. Who Patients Are Listening to
 Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE Glaukos Equinox Alcon Mitch Ibach OD, FAAO Vance Thompson Vision Who Patients Are Listening to Optometrist 36% People who've had surgery
Disclosures: Laser K s: Keratectomy to Keratomileusis with a SMILE Glaukos Equinox Alcon Mitch Ibach OD, FAAO Vance Thompson Vision Who Patients Are Listening to Optometrist 36% People who've had surgery
Refractive Surgery Dilemma
 Refractive Surgery Dilemma Section Editor: lireza aradaran-rafii, MD CSE PRESENTTION 33-year-old man seeking refractive surgery presented with refractive error of -1.75-4.0 20 in the right and -0.75-2.5
Refractive Surgery Dilemma Section Editor: lireza aradaran-rafii, MD CSE PRESENTTION 33-year-old man seeking refractive surgery presented with refractive error of -1.75-4.0 20 in the right and -0.75-2.5
Recent concerns regarding the depth of tissue ablation with
 Volume Estimation of Excimer Laser Tissue Ablation for Correction of Spherical Myopia and Hyperopia Damien Gatinel, 1 Thanh Hoang-Xuan, 1 and Dimitri T. Azar 1,2 PURPOSE. To determine the theoretical volumes
Volume Estimation of Excimer Laser Tissue Ablation for Correction of Spherical Myopia and Hyperopia Damien Gatinel, 1 Thanh Hoang-Xuan, 1 and Dimitri T. Azar 1,2 PURPOSE. To determine the theoretical volumes
White Paper. Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery
 White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
White Paper. Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery
 White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
White Paper Topography-Guided Laser Assisted In-Situ Keratomileusis vs Small- Incision Lenticule Extraction Refractive Surgery A Summary of Clinical Outcomes Andrea Petznick, Diplom-AO (FH), PhD Alcon
POST-LASIK ECTASIA MANAGEMENT
 POST-LASIK ECTASIA MANAGEMENT A. John Kanellopoulos MD 1,2 1: Laservision.gr Clinical & Research Eye Institute, Athens, Greece 2: NYU Medical School Department of Ophthalmology, NY, NY Financial interests:
POST-LASIK ECTASIA MANAGEMENT A. John Kanellopoulos MD 1,2 1: Laservision.gr Clinical & Research Eye Institute, Athens, Greece 2: NYU Medical School Department of Ophthalmology, NY, NY Financial interests:
Personal data. Curriculum Vitae. Experience. Date of birth 18 December 1969
 1 Curriculum Vitae Dr. Sophia I. Panagopoulou University of Crete Medical School, IVO 71003 Heraklion Greece Phone: +302810394645 FAX: +302810394653 e-mail: spanagop@med.uoc.gr Personal data Date of birth
1 Curriculum Vitae Dr. Sophia I. Panagopoulou University of Crete Medical School, IVO 71003 Heraklion Greece Phone: +302810394645 FAX: +302810394653 e-mail: spanagop@med.uoc.gr Personal data Date of birth
Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation
 Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation Mohammad Naser Hashemian, MD 1 Mahdi AliZadeh, MD 2 Hassan Hashemi, MD 1,3 Firoozeh Rahimi, MD 4 Abstract Purpose: To present
Management of Unpredictable Post-PRK Corneal Ectasia with Intacs Implantation Mohammad Naser Hashemian, MD 1 Mahdi AliZadeh, MD 2 Hassan Hashemi, MD 1,3 Firoozeh Rahimi, MD 4 Abstract Purpose: To present
L. Spadea, R. Ferrante, F. Romani, A. Di Gregorio
 University of L Aquila Eye Clinic Head: Prof. Leopoldo Spadea ULTRAFAST EXCIMER LASER FOR TRANS-EPITHELIAL CUSTOMIZED PHOTOREFRACTIVE SURGERIES: CLINICAL RESULTS WITH 6 MONTHS FOLLOW UP L. Spadea, R. Ferrante,
University of L Aquila Eye Clinic Head: Prof. Leopoldo Spadea ULTRAFAST EXCIMER LASER FOR TRANS-EPITHELIAL CUSTOMIZED PHOTOREFRACTIVE SURGERIES: CLINICAL RESULTS WITH 6 MONTHS FOLLOW UP L. Spadea, R. Ferrante,
ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM. Mickael Yablokov. I have no any financial interests in any products mentioned in this paper
 ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM Mickael Yablokov I have no any financial interests in any products mentioned in this paper Ophthalmology clinic Eye Surgery, Kostroma, Russia Goal
ONE THOUSAND WAVEFRONT GIDED TREATMENT ON MICROSCAN VISUM Mickael Yablokov I have no any financial interests in any products mentioned in this paper Ophthalmology clinic Eye Surgery, Kostroma, Russia Goal
Induced Secondary Astigmatism and Horizontal Coma after LASIK for Mixed Astigmatism
 Induced Secondary Astigmatism and Horizontal Coma after LASIK for Mixed Astigmatism S-Farzad Mohammadi, MD 1 Maryam Tahvildari, MD 2 Tahereh Abdolahinia, BS 3 Abstract Purpose: To describe a distinctive
Induced Secondary Astigmatism and Horizontal Coma after LASIK for Mixed Astigmatism S-Farzad Mohammadi, MD 1 Maryam Tahvildari, MD 2 Tahereh Abdolahinia, BS 3 Abstract Purpose: To describe a distinctive
LASIK for 6.00 to D of Myopia With up to 3.00 D of Cylinder Using the ALLEGRETTO WAVE: 3- and 6-month Results With the 200- and 400-Hz Platforms
 LASIK for 6.00 to 12.00 D of Myopia With up to 3.00 D of Cylinder Using the ALLEGRETTO WAVE: 3- and 6-month Results With the 200- and 400-Hz Platforms Karl G. Stonecipher, MD; Guy M. Kezirian, MD; Megan
LASIK for 6.00 to 12.00 D of Myopia With up to 3.00 D of Cylinder Using the ALLEGRETTO WAVE: 3- and 6-month Results With the 200- and 400-Hz Platforms Karl G. Stonecipher, MD; Guy M. Kezirian, MD; Megan
ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018
 efocus Innovation, Leadership, Passion for Perfection Issue 051 415.922.9500 www.pacificvision.org March 2018 ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018 Eye care has always been at
efocus Innovation, Leadership, Passion for Perfection Issue 051 415.922.9500 www.pacificvision.org March 2018 ADVANCES in REFRACTIVE, CORNEA, and CATARACT SURGERY UPDATE 2018 Eye care has always been at
PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET
 PATIENT INFORMATION BOOKLET") 616.365.5775 www.keillasik.com PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET Please read this entire booklet. Discuss its contents with your doctor so that questions are answered to your
616.365.5775 www.keillasik.com PHOTOREFRACTIVE KERATECTOMY (PRK) PATIENT INFORMATION BOOKLET Please read this entire booklet. Discuss its contents with your doctor so that questions are answered to your
Our experience with Athens protocol - simultaneous topo-guided photorefractive keratectomy followed by corneal collagen cross linking for keratoconus
 International Journal of Research in Medical Sciences Shah S et al. Int J Res Med Sci. 2016 Jul;4(7):2639-2644 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161924
International Journal of Research in Medical Sciences Shah S et al. Int J Res Med Sci. 2016 Jul;4(7):2639-2644 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20161924
Abdel Rahman ElSebaey, MD, PhD.
 Surface Ablation Refractive Surgery Abdel Rahman ElSebaey, MD, PhD. Menoufia University History Correction of optical defects of human eye started 1200 AD. Spherical error corrected by spectacle on 13
Surface Ablation Refractive Surgery Abdel Rahman ElSebaey, MD, PhD. Menoufia University History Correction of optical defects of human eye started 1200 AD. Spherical error corrected by spectacle on 13
Original Article High myopia as a risk factor for post-lasik ectasia: a case report
 Original Article High myopia as a risk factor for post-lasik ectasia: a case report Mona Harissi-Dagher, MD, a,b Sonja A. F. Frimmel, c and Samir Melki, MD, PhD a,d Author affiliations: a Massachusetts
Original Article High myopia as a risk factor for post-lasik ectasia: a case report Mona Harissi-Dagher, MD, a,b Sonja A. F. Frimmel, c and Samir Melki, MD, PhD a,d Author affiliations: a Massachusetts
The two currently accepted methods for correcting
 New Technique Therapeutic Alloplastic Laser in situ Keratomileusis for Myopia Arturo Maldonado-Bas, MD; Ruben Pulido-Garcia, MD ABSTRACT BACKGROUND: A new technique, therapeutic alloplastic laser in situ
New Technique Therapeutic Alloplastic Laser in situ Keratomileusis for Myopia Arturo Maldonado-Bas, MD; Ruben Pulido-Garcia, MD ABSTRACT BACKGROUND: A new technique, therapeutic alloplastic laser in situ
Wavefront-Optimized Technology in Hyperopic Correction Stability Using Different Optical Zones
 Med. J. Cairo Univ., Vol. 78, No. 1, December 559-563, 2010 www.medicaljournalofcairouniversity.com Wavefront-Optimized Technology in Hyperopic Correction Stability Using Different Optical Zones ADNAN
Med. J. Cairo Univ., Vol. 78, No. 1, December 559-563, 2010 www.medicaljournalofcairouniversity.com Wavefront-Optimized Technology in Hyperopic Correction Stability Using Different Optical Zones ADNAN
SCHWIND CAM Perfect Planning wide range of applications
 SCHWIND CAM Perfect Planning wide range of applications ORK-CAM PresbyMAX PTK-CAM 2 SCHWIND CAM the system solution The modular design of the SCHWIND CAM offers customised treatment planning for a uniquely
SCHWIND CAM Perfect Planning wide range of applications ORK-CAM PresbyMAX PTK-CAM 2 SCHWIND CAM the system solution The modular design of the SCHWIND CAM offers customised treatment planning for a uniquely
Laser in situ keratomileusis (LASIK) has proven to be
 has proven to be") Autorefractometry after laser in situ keratomileusis Dimitrios S. Siganos, MD, PhD, Corina Popescu, MD, Nikolaos Bessis, DOpt, Georgios Papastergiou, MD Purpose: To correlate cycloplegic subjective refraction
Autorefractometry after laser in situ keratomileusis Dimitrios S. Siganos, MD, PhD, Corina Popescu, MD, Nikolaos Bessis, DOpt, Georgios Papastergiou, MD Purpose: To correlate cycloplegic subjective refraction
Nature and Science 2017;15(11) Mohamed Elmoddather. MD
 Mohamed Elmoddather. MD") Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Mohamed Elmoddather. MD Ophthalmology Faculty of Medicine, Al-Azhar University, Assuit, Egypt shahdmsaleh@hotmail.com Abstract:
Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Mohamed Elmoddather. MD Ophthalmology Faculty of Medicine, Al-Azhar University, Assuit, Egypt shahdmsaleh@hotmail.com Abstract:
INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA)
 AND ADVANCE SURFACE ABLATION (ASA)") INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA) This information and the Patient Information booklet must be reviewed so you can make an informed decision regarding
INFORMED CONSENT FOR PHOTOREFRACTIVE KERATECTOMY (PRK) AND ADVANCE SURFACE ABLATION (ASA) This information and the Patient Information booklet must be reviewed so you can make an informed decision regarding
Clinical experience of 9,000 small aperture Inlays for presbyopia correction
 Clinical experience of 9,000 small aperture Inlays for presbyopia correction Minoru Tomita, MD, PhD Shinagawa LASIK Center, Tokyo, Japan September 7 th, 2012, ISOP meeting in Tokyo, JAPAN 1,060,666 Femto
Clinical experience of 9,000 small aperture Inlays for presbyopia correction Minoru Tomita, MD, PhD Shinagawa LASIK Center, Tokyo, Japan September 7 th, 2012, ISOP meeting in Tokyo, JAPAN 1,060,666 Femto
Innovation, Leadership, Passion for Perfection
 Innovation, Leadership, Passion for Perfection efocus P A C I F I C V I S I O N I N S T I T U T E Issue 052 415.922.9500 www.pacificvision.org May 2018 Bay Area optometrists observing topography-guided
Innovation, Leadership, Passion for Perfection efocus P A C I F I C V I S I O N I N S T I T U T E Issue 052 415.922.9500 www.pacificvision.org May 2018 Bay Area optometrists observing topography-guided
Description of iatrogenic corneal ectasia in patients without traditional risk factors
 ARTICLE Description of iatrogenic corneal ectasia in patients without traditional risk factors Julio Ortega-Usobiaga, MD, PhD 1 ; Rosario Cobo-Soriano, MD, PhD 1 ; Fernando Llovet-Osuna, MD, PhD 1 ; Stephan
ARTICLE Description of iatrogenic corneal ectasia in patients without traditional risk factors Julio Ortega-Usobiaga, MD, PhD 1 ; Rosario Cobo-Soriano, MD, PhD 1 ; Fernando Llovet-Osuna, MD, PhD 1 ; Stephan
Author s Affiliation. Original Article. Visual outcomes after LASIK (laser-assisted in-situ keratomileusis) for various refractive errors.
 for various refractive errors.") Original Article Visual outcomes after LASIK (laser-assisted in-situ keratomileusis) for various refractive errors. Author s Affiliation Sobia Tufail Imran Ahmad Asad Aslam Khan Correspondence Author:
Original Article Visual outcomes after LASIK (laser-assisted in-situ keratomileusis) for various refractive errors. Author s Affiliation Sobia Tufail Imran Ahmad Asad Aslam Khan Correspondence Author:
Outcomes of NIDEK Optical Path Difference Custom Ablation Treatments (OPDCAT) for Myopia With or Without Astigmatism
 for Myopia With or Without Astigmatism") Outcomes of NIDEK Optical Path Difference Custom Ablation Treatments (OPDCAT) for Myopia With or Without Astigmatism Shihao Chen, MD, OD, MS; Yibo Wang, MD; Qinmei Wang, MD ABSTRACT PURPOSE: To report
Outcomes of NIDEK Optical Path Difference Custom Ablation Treatments (OPDCAT) for Myopia With or Without Astigmatism Shihao Chen, MD, OD, MS; Yibo Wang, MD; Qinmei Wang, MD ABSTRACT PURPOSE: To report
The Effect of Ptosis on Cataract Surgical Planning
 Published online: April 14, 2015 1663 2699/15/0061 0132$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: April 14, 2015 1663 2699/15/0061 0132$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Management of postkeratoplasty ametropia: IntraLASIK after penetrating keratoplasty
 European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 877-885 Management of postkeratoplasty ametropia: IntraLASIK after penetrating keratoplasty R.B. KUCUMEN, N.M. YENEREL, E. GORGUN, M.L. ALIMGIL
European Journal of Ophthalmology / Vol. 18 no. 6, 2008 / pp. 877-885 Management of postkeratoplasty ametropia: IntraLASIK after penetrating keratoplasty R.B. KUCUMEN, N.M. YENEREL, E. GORGUN, M.L. ALIMGIL
Topography-Guided. Relevant Literature. March 10th / New York, NY. Become a Cornea Diagnostics & Topography - Guided Treatment Designing Expert!
 Topography-Guided Become a Cornea Diagnostics & Topography - Guided Treatment Designing Expert! Relevant Literature March 10th / New York, NY Course Director A. John Kanellopoulos, MD Clinical Professor
Topography-Guided Become a Cornea Diagnostics & Topography - Guided Treatment Designing Expert! Relevant Literature March 10th / New York, NY Course Director A. John Kanellopoulos, MD Clinical Professor
PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik
 PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik SCHWIND eye-tech-solutions Lunch Symposium Prof. Jorge L. Alió MD, PhD. UNIVERSIDAD MIGUEL HERNÁNDEZ VISSUM INSTITUTO OFTALMOLÓGICO
PresbyMax Outcomes in Myopia, Hyperopia, Emmetropia and Patients post Lasik SCHWIND eye-tech-solutions Lunch Symposium Prof. Jorge L. Alió MD, PhD. UNIVERSIDAD MIGUEL HERNÁNDEZ VISSUM INSTITUTO OFTALMOLÓGICO
aberration induced by laser
 How is spherical aberration induced by laser refractive surgery? Geunyoung Yoon, PhD 1 Ian Cox, PhD 2 Scott MacRae,, MD 1 1 Department of Ophthalmology, Center for Visual Science University of Rochester,
How is spherical aberration induced by laser refractive surgery? Geunyoung Yoon, PhD 1 Ian Cox, PhD 2 Scott MacRae,, MD 1 1 Department of Ophthalmology, Center for Visual Science University of Rochester,
Photorefractive Keratectomy as A Retreatment of Residual Myopia after Previous Laser in Situ Keratomileusis
 Photorefractive Keratectomy as A Retreatment of Residual Myopia after Previous Laser in Situ Keratomileusis Alireza Ashtari, MD 1 Hassan Razmju, MD 2 Amin Masjedi, MD 3 Alireza Zandi, MD 1 Mehdi Tavakoli,
Photorefractive Keratectomy as A Retreatment of Residual Myopia after Previous Laser in Situ Keratomileusis Alireza Ashtari, MD 1 Hassan Razmju, MD 2 Amin Masjedi, MD 3 Alireza Zandi, MD 1 Mehdi Tavakoli,
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB
 Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
Pearls for the Refractive Technician Fadiah Alkhawaldeh, IMBA, COT, ROUB Cleveland Clinic Cole Eye Institute OOS, Columbus, OH February, 2014 alkhawf@ccf.org NO FINANCIAL DISCLOSURES A Puzzle of an Eye
One-year outcomes of a bilateral randomised prospective clinical trial comparing PRK with mitomycin C and LASIK
 Vision Institute, Federal University of São Paulo Department of Ophthalmology, São Paulo, Brazil Correspondence to: Dr A D Wallau, R Vaz e Silva, 41, 91040-150, Porto Alegre, RS, Brazil; anewallau@hotmail.com
Vision Institute, Federal University of São Paulo Department of Ophthalmology, São Paulo, Brazil Correspondence to: Dr A D Wallau, R Vaz e Silva, 41, 91040-150, Porto Alegre, RS, Brazil; anewallau@hotmail.com
Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by
 Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by Pentacam as A New Imaging Technique Mohammad Ali Zare, MD 1 Hassan
Comparison of Corneal and Anterior Chamber Parameters following Myopic laser in situ keratomileusis and photorefractive keratectomy by Pentacam as A New Imaging Technique Mohammad Ali Zare, MD 1 Hassan
Refractive and Keratometric Stability in High Myopic LASIK With High-Frequency Femtosecond and Excimer Lasers
 ORIGINAL ARTICLE Refractive and Keratometric Stability in High Myopic LASIK With High-Frequency Femtosecond and Excimer Lasers Anastasios John Kanellopoulos, MD; George Asimellis, PhD ABSTRACT PURPOSE:
ORIGINAL ARTICLE Refractive and Keratometric Stability in High Myopic LASIK With High-Frequency Femtosecond and Excimer Lasers Anastasios John Kanellopoulos, MD; George Asimellis, PhD ABSTRACT PURPOSE:
CLINICAL SCIENCES. Management of Post-LASIK Corneal Ectasia With Intacs Inserts
 Management of Post-LASIK Corneal Ectasia With Intacs Inserts One-Year Results CLINICAL SCIENCES George D. Kymionis, MD, PhD; Charalambos S. Siganos, MD, PhD; George Kounis, BSc; Nikolaos Astyrakakis, OD;
Management of Post-LASIK Corneal Ectasia With Intacs Inserts One-Year Results CLINICAL SCIENCES George D. Kymionis, MD, PhD; Charalambos S. Siganos, MD, PhD; George Kounis, BSc; Nikolaos Astyrakakis, OD;
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page
 Vol. 73 (9), Page") The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page 7580-7586 Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Department of Ophthalmology, Faculty
The Egyptian Journal of Hospital Medicine (October 2018) Vol. 73 (9), Page 7580-7586 Outcome of PRK in Management of Post LISIK Residual Myopia and Myopic Astigmatism Department of Ophthalmology, Faculty
In recent years, more and more studies have focused on. Characteristics of Straylight in Normal Young Myopic Eyes and Changes before and after LASIK
 Cornea Characteristics of Straylight in Normal Young Myopic Eyes and Changes before and after LASIK Jing Li and Yan Wang PURPOSE. To investigate the characteristics of straylight and relevant factors in
Cornea Characteristics of Straylight in Normal Young Myopic Eyes and Changes before and after LASIK Jing Li and Yan Wang PURPOSE. To investigate the characteristics of straylight and relevant factors in
Keratoconus Clinic. Optometric Co-management Opportunities
 Keratoconus Clinic Optometric Co-management Opportunities The Bochner Eye Institute established the first Keratoconus Clinic in Canada in 2008. The consultation and advanced imaging are OHIP covered. All
Keratoconus Clinic Optometric Co-management Opportunities The Bochner Eye Institute established the first Keratoconus Clinic in Canada in 2008. The consultation and advanced imaging are OHIP covered. All
Lens and Cataract Surgery Update 2008
 efocus Innovation. Leadership. Passion for Perfection PACIFIC V I S I O N I N S T I T U T E Life in Focus Issue 029 415.922.9500 --- www.pacificvision.org December 2008 Lens and Cataract Surgery Update
efocus Innovation. Leadership. Passion for Perfection PACIFIC V I S I O N I N S T I T U T E Life in Focus Issue 029 415.922.9500 --- www.pacificvision.org December 2008 Lens and Cataract Surgery Update
Clinical Outcomes of an Optimized Prolate Ablation Procedure for Correcting Residual Refractive Errors Following Laser Surgery
 pissn: 111-8942 eissn: 292-9382 Korean J Ophthalmol 217;31(1):16-24 ht tps://doi.org/1.3341/k jo.217.31.1.16 Original Article Clinical Outcomes of an Optimized Prolate Ablation Procedure for Correcting
pissn: 111-8942 eissn: 292-9382 Korean J Ophthalmol 217;31(1):16-24 ht tps://doi.org/1.3341/k jo.217.31.1.16 Original Article Clinical Outcomes of an Optimized Prolate Ablation Procedure for Correcting
Premium Implant Options for the Cataract Patient. Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota
 Premium Implant Options for the Cataract Patient Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota Glaukos Bausch and Lomb Alcon Allergan Bio- Tissue TearScience Reichert Trends
Premium Implant Options for the Cataract Patient Justin Schweitzer, OD, FAAO Vance Thompson Vision Sioux Falls, South Dakota Glaukos Bausch and Lomb Alcon Allergan Bio- Tissue TearScience Reichert Trends
Louis Probst. Commitment to Optometry. Cycloplegic Exam. Steroid free PRK. LASIK Enhancements made Ridiculously Simple 8/18/2017
 Louis Probst LASIK Enhancements made Ridiculously Simple Louis E. Probst MD National Medical Director, TLC Chief Surgeon, Central Midwest, USA TLC surgeon 22 years 7 books, 80 chapters, 50 papers, 11 instruments
Louis Probst LASIK Enhancements made Ridiculously Simple Louis E. Probst MD National Medical Director, TLC Chief Surgeon, Central Midwest, USA TLC surgeon 22 years 7 books, 80 chapters, 50 papers, 11 instruments
Research Article Effect of Mitomycin C on Myopic versus Astigmatic Photorefractive Keratectomy
 Hindawi Ophthalmology Volume 2017, Article ID 2841408, 5 pages https://doi.org/10.1155/2017/2841408 Research Article Effect of Mitomycin C on Myopic versus Astigmatic Photorefractive Keratectomy Ashwag
Hindawi Ophthalmology Volume 2017, Article ID 2841408, 5 pages https://doi.org/10.1155/2017/2841408 Research Article Effect of Mitomycin C on Myopic versus Astigmatic Photorefractive Keratectomy Ashwag
BJO Online First, published on November 4, 2009 as /bjo
 BJO Online First, published on November, 009 as 0./bjo.00.9 9 0 9 0 9 0 9 0 9 0 9 0 One Year Outcomes of a Bilateral Randomized Prospective Clinical Trial Comparing PRK with Mitomycin C and LASIK Anelise
BJO Online First, published on November, 009 as 0./bjo.00.9 9 0 9 0 9 0 9 0 9 0 9 0 One Year Outcomes of a Bilateral Randomized Prospective Clinical Trial Comparing PRK with Mitomycin C and LASIK Anelise
Analysis of eye movements during myopic laser in situ keratomileusis
 15th International SCHWIND User Meeting, Vancouver 2014 Analysis of eye movements during myopic laser in situ keratomileusis Thomas Kohnen Department of Ophthalmology Goethe-University, Frankfurt, Germany
15th International SCHWIND User Meeting, Vancouver 2014 Analysis of eye movements during myopic laser in situ keratomileusis Thomas Kohnen Department of Ophthalmology Goethe-University, Frankfurt, Germany
Facts You Need to Know About IDESIGN System Driven Laser Assisted In-Situ Keratomileusis (LASIK) Procedure for Monovision
 Procedure for Monovision") Facts You Need to Know About IDESIGN System Driven Laser Assisted In-Situ Keratomileusis (LASIK) Procedure for Monovision Patient Information Booklet For Monovision Treatment of Presbyopic Patients with
Facts You Need to Know About IDESIGN System Driven Laser Assisted In-Situ Keratomileusis (LASIK) Procedure for Monovision Patient Information Booklet For Monovision Treatment of Presbyopic Patients with
Enhancement of femtosecond lenticule extraction for visual symptomatic eye after myopia correction
 Zhao et al. BMC Ophthalmology 2014, 14:68 CASE REPORT Open Access Enhancement of femtosecond lenticule extraction for visual symptomatic eye after myopia correction Jing Zhao, Peijun Yao, Zhi Chen, Meiyan
Zhao et al. BMC Ophthalmology 2014, 14:68 CASE REPORT Open Access Enhancement of femtosecond lenticule extraction for visual symptomatic eye after myopia correction Jing Zhao, Peijun Yao, Zhi Chen, Meiyan
The WaveLight Refractive Suite:
 Supplement to November/December 2012 Sponsored by Alcon Laboratories, Inc. The WaveLight Refractive Suite: Clinical Data 2012 The latest research on the WaveLight EX500 excimer laser and the FS200 femtosecond
Supplement to November/December 2012 Sponsored by Alcon Laboratories, Inc. The WaveLight Refractive Suite: Clinical Data 2012 The latest research on the WaveLight EX500 excimer laser and the FS200 femtosecond
Comparison of outcomes of conventional WaveLight Allegretto Wave and Technolas excimer lasers in myopic laser in situ keratomileusis
 Clinical Ophthalmology open access to scientific and medical research Open Access Full Text Article Case Series Comparison of outcomes of conventional WaveLight Allegretto Wave and excimer lasers in myopic
Clinical Ophthalmology open access to scientific and medical research Open Access Full Text Article Case Series Comparison of outcomes of conventional WaveLight Allegretto Wave and excimer lasers in myopic
Number 80. Laser Eye Surgery in Myopia. Date of decision October 2017 Date of review October 2020 GUIDANCE
 Excluded: Procedure not routinely funded Bedfordshire, Hertfordshire, West Essex, Luton and Milton Keynes Priorities Forum statement - adapted for Bedfordshire CCG Number 80 Subject Date of decision October
Excluded: Procedure not routinely funded Bedfordshire, Hertfordshire, West Essex, Luton and Milton Keynes Priorities Forum statement - adapted for Bedfordshire CCG Number 80 Subject Date of decision October
ALLEGRETTO WAVE TM EYE-Q Scanning Spot LASIK Laser System
 ALLEGRETTO WAVE TM EYE-Q Scanning Spot LASIK Laser System Patient Information Booklet Facts You Need to Know About LASIK (Laser Assisted In-Situ Keratomileusis) Laser Treatment Information for patients
ALLEGRETTO WAVE TM EYE-Q Scanning Spot LASIK Laser System Patient Information Booklet Facts You Need to Know About LASIK (Laser Assisted In-Situ Keratomileusis) Laser Treatment Information for patients
ALLEGRETTO WAVE Scanning Spot LASIK Laser System
 TM ALLEGRETTO WAVE Scanning Spot LASIK Laser System Patient Information Booklet Information for patients considering Laser Assisted In-Situ Keratomileusis (LASIK) Surgery Information for patients considering
TM ALLEGRETTO WAVE Scanning Spot LASIK Laser System Patient Information Booklet Information for patients considering Laser Assisted In-Situ Keratomileusis (LASIK) Surgery Information for patients considering
Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia
 Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia Seyed Mohammad Reza Taheri, MD 1 Azita Kheiltash, MD, MPH 2 Hassan Hashemi, MD 1,3 Abstract Purpose: To
Comparison of Corneal Power and Intraocular Lens Power Calculation Methods after LASIK for Myopia Seyed Mohammad Reza Taheri, MD 1 Azita Kheiltash, MD, MPH 2 Hassan Hashemi, MD 1,3 Abstract Purpose: To
Patient Information Booklet
 FACTS YOU NEED TO KNOW ABOUT ADVANCED CUSTOMVUE LASER ASSISTED IN-SITU KERATOMILEUSIS (LASIK) LASER TREATMENT Patient Information Booklet For the reduction or elimination of myopia (nearsightedness) up
FACTS YOU NEED TO KNOW ABOUT ADVANCED CUSTOMVUE LASER ASSISTED IN-SITU KERATOMILEUSIS (LASIK) LASER TREATMENT Patient Information Booklet For the reduction or elimination of myopia (nearsightedness) up
Is Topography-guided Ablation Profile Centered on the Corneal Vertex Better Than Wavefront-guided Ablation Profile Centered on the Entrance Pupil?
 ABSTRACT PURPOSE: To illustrate the hypothesis that corneal vertex centration is superior to entrance pupil centration when guiding an ablation by wavefront. METHODS: In one case example of therapeutic
ABSTRACT PURPOSE: To illustrate the hypothesis that corneal vertex centration is superior to entrance pupil centration when guiding an ablation by wavefront. METHODS: In one case example of therapeutic
Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391
 Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391 Effective Date: November 2007 Last Review Date: January 2016 Coding Implications Revision Log See Important Reminder at the end of this
Clinical Policy: Refractive Surgery Reference Number: CP.MP. 391 Effective Date: November 2007 Last Review Date: January 2016 Coding Implications Revision Log See Important Reminder at the end of this
Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles
 Irregular Astigmatism & honing your K incision Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles Uday Devgan MD Current Disclosures: Aaren Scientific: consultant Accutome Inc: royalties
Irregular Astigmatism & honing your K incision Uday Devgan MD Private Practice, Devgan Eye Surgery, Los Angeles Uday Devgan MD Current Disclosures: Aaren Scientific: consultant Accutome Inc: royalties
BY MICHAEL W. BELIN, MD
 Point/Counterpoint: The Pentacam Ve The Pentacam s rotating imaging provides a more accurate picture of the cornea. BY MICHAEL W. BELIN, MD It was not long ago that discussions concerned whether topography
Point/Counterpoint: The Pentacam Ve The Pentacam s rotating imaging provides a more accurate picture of the cornea. BY MICHAEL W. BELIN, MD It was not long ago that discussions concerned whether topography
LASIK. What is LASIK? Eye Words to Know. Who is a good candidate for LASIK?
 2014 2015 What is? (laser in situ keratomileusis) is a type of refractive surgery. This kind of surgery uses a laser to treat vision problems caused by refractive errors. You have a refractive error when
2014 2015 What is? (laser in situ keratomileusis) is a type of refractive surgery. This kind of surgery uses a laser to treat vision problems caused by refractive errors. You have a refractive error when
Edward Manche, MD. Professor of Ophthalmology at Stanford University Medical Center
 Professor of Ophthalmology at Stanford University Medical Center CLINICAL OFFICES Stanford Byers Eye Institute 2452 Watson Ct MC 5353 Palo Alto, CA 94303 Tel (650) 723-6995 Fax (650) 565-8297 Stanford
Professor of Ophthalmology at Stanford University Medical Center CLINICAL OFFICES Stanford Byers Eye Institute 2452 Watson Ct MC 5353 Palo Alto, CA 94303 Tel (650) 723-6995 Fax (650) 565-8297 Stanford
FEP Medical Policy Manual
 FEP Medical Manual 9.03.05 Corneal Topography/Computer-Assisted Corneal Topography/ Photokeratoscopy Last Review: September 2016 Next Review: September 2017 Related Policies 9.03.28 Corneal Collagen Cross-linking
FEP Medical Manual 9.03.05 Corneal Topography/Computer-Assisted Corneal Topography/ Photokeratoscopy Last Review: September 2016 Next Review: September 2017 Related Policies 9.03.28 Corneal Collagen Cross-linking
Laser in Situ Keratomileusis versus Laser Assisted Subepithelial Keratectomy for the Correction of Low to Moderate Myopia and Astigmatism
 Laser in Situ Keratomileusis versus Laser Assisted Subepithelial Keratectomy for the Correction of Low to Moderate Myopia and Astigmatism Seyed Javad Hashemian, MD 1 Hossein Aghaei, MD 2 Alireza Foroutan,
Laser in Situ Keratomileusis versus Laser Assisted Subepithelial Keratectomy for the Correction of Low to Moderate Myopia and Astigmatism Seyed Javad Hashemian, MD 1 Hossein Aghaei, MD 2 Alireza Foroutan,
Yu Ling Liu, Chien Chi Tseng, Chang Ping Lin
 Original Article Taiwan J Ophthalmol 2017;7:82 88 Access this article online Quick Response Code: Visual performance after excimer laser photorefractive keratectomy for high myopia Yu Ling Liu, Chien Chi
Original Article Taiwan J Ophthalmol 2017;7:82 88 Access this article online Quick Response Code: Visual performance after excimer laser photorefractive keratectomy for high myopia Yu Ling Liu, Chien Chi
Presby LASIK Topographies
 Presby LASIK Topographies SurgiVision Consultants, Inc. DataLink kforum June 1, 2009 Not for Distribution Introduction Case review of presby LASIK procedures performed with the WaveLight Eye Q Laser Presentation
Presby LASIK Topographies SurgiVision Consultants, Inc. DataLink kforum June 1, 2009 Not for Distribution Introduction Case review of presby LASIK procedures performed with the WaveLight Eye Q Laser Presentation
CATARACT SURGERY AFTER RADIAL KERATOTOMY
 AFTER RADIAL KERATOTOMY How to avoid disappointment. BY BERNARD MATHYS, MD CATARACT SURGERY Radial keratotomy (RK; Figure 1) was a popular refractive surgical procedure to correct myopia in the 1970s and
AFTER RADIAL KERATOTOMY How to avoid disappointment. BY BERNARD MATHYS, MD CATARACT SURGERY Radial keratotomy (RK; Figure 1) was a popular refractive surgical procedure to correct myopia in the 1970s and
The Comparison of Central and Mean True-Net Power (Pentacam) in Calculating IOL-Power After Refractive Surgery
 in Calculating IOL-Power After Refractive Surgery") 접수번호 :08-024 Korean Journal of Ophthalmology 2009;23:1-5 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.1.1 The Comparison of Central and Mean True-Net Power (Pentacam) in Calculating IOL-Power After Refractive
접수번호 :08-024 Korean Journal of Ophthalmology 2009;23:1-5 ISSN : 1011-8942 DOI : 10.3341/kjo.2009.23.1.1 The Comparison of Central and Mean True-Net Power (Pentacam) in Calculating IOL-Power After Refractive
LASIK: Basic steps for great results
 LASIK: Basic steps for great results ESCRS 2009 A. John Kanellopoulos, M.D. Associate Professor of Ophthalmology l NYU Medical School, NY Director: Laservision.gr Eye Institute, Athens, Greece My Background
LASIK: Basic steps for great results ESCRS 2009 A. John Kanellopoulos, M.D. Associate Professor of Ophthalmology l NYU Medical School, NY Director: Laservision.gr Eye Institute, Athens, Greece My Background
Efficacy of Photorefractive Keratectomy for Military Pilot Recruitment in an Asian Air Force
 Efficacy of Photorefractive Keratectomy for Military Pilot Recruitment in an Asian Air Force Brian See, Gerard Nah, Wee Hoe Gan, Robin Low AsMA Annual Scientific Meeting 2013 Chicago, IL, USA Disclosure
Efficacy of Photorefractive Keratectomy for Military Pilot Recruitment in an Asian Air Force Brian See, Gerard Nah, Wee Hoe Gan, Robin Low AsMA Annual Scientific Meeting 2013 Chicago, IL, USA Disclosure
Interpretation of corneal tomography
 Interpretation of corneal tomography Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of Sydney Page 1
Interpretation of corneal tomography Presented by Chameen Samarawickrama - Westmead Hospital - Liverpool Hospital - University of Sydney - University of New South Wales The University of Sydney Page 1
Facts You Need to Know About CustomVue Laser Assisted In-Situ Keratomileusis (LASIK) Laser Treatment
 Laser Treatment") Facts You Need to Know About CustomVue Laser Assisted In-Situ Keratomileusis (LASIK) Laser Treatment Patient Information Booklet For Nearsightedness (Myopia) up to -6 D with less than -3 D Astigmatism
Facts You Need to Know About CustomVue Laser Assisted In-Situ Keratomileusis (LASIK) Laser Treatment Patient Information Booklet For Nearsightedness (Myopia) up to -6 D with less than -3 D Astigmatism
LASIK has been the primary type of corneal refractive surgery
 Cornea Higher-Order Aberrations of Anterior and Posterior Corneal Surfaces in Patients With Keratectasia After LASIK Naoyuki Maeda, 1 Tomoya Nakagawa, 1 Ryo Kosaki, 1 Shizuka Koh, 1 Makoto Saika, 2 Takashi
Cornea Higher-Order Aberrations of Anterior and Posterior Corneal Surfaces in Patients With Keratectasia After LASIK Naoyuki Maeda, 1 Tomoya Nakagawa, 1 Ryo Kosaki, 1 Shizuka Koh, 1 Makoto Saika, 2 Takashi
Informed Consent for Excimer Laser Surface Ablation Surgery (PRK, LASEK, epi-lasik, and others)
") Informed Consent for Excimer Laser Surface Ablation Surgery (PRK, LASEK, epi-lasik, and others) Patient name (printed): Patient date of birth: Please review this information so you can make an informed
Informed Consent for Excimer Laser Surface Ablation Surgery (PRK, LASEK, epi-lasik, and others) Patient name (printed): Patient date of birth: Please review this information so you can make an informed
CLINICAL STUDY. BJ Choi 1, YM Park 2 and JS Lee 2
 (2015) 29, 356 362 & 2015 Macmillan Publishers Limited All rights reserved 0950-222X/15 www.nature.com/eye CLINICAL STUDY Clinical outcomes between optical path difference custom aspheric treatment and
(2015) 29, 356 362 & 2015 Macmillan Publishers Limited All rights reserved 0950-222X/15 www.nature.com/eye CLINICAL STUDY Clinical outcomes between optical path difference custom aspheric treatment and
SAMPLE WHAT LASIK CAN DO
 DECIDING ON LASIK Imagine being able to work, drive, and play sports without having to depend on glasses or contact lenses. LASIK (laser in-situ keratomileusis) may make this a reality for you. This laser
DECIDING ON LASIK Imagine being able to work, drive, and play sports without having to depend on glasses or contact lenses. LASIK (laser in-situ keratomileusis) may make this a reality for you. This laser
REFRACTIVE OUTCOME IN PRESBYOPIC PATIENTS TREATED WITH SHWIND AMARIS PRESBYMAX LASER TREATMENT
 COMBINED SELECTIVE CORNEAL WAVEFRONT-GUIDED PHOTOREFRACTIVE KERATECTOMY AND CORNEAL CROSS-LINKING IN EYES WITH PROGRESSIVE MILD TO MODERATE KERATOCONUS Session Title: CRS/RLE Session Date/Time: Saturday
COMBINED SELECTIVE CORNEAL WAVEFRONT-GUIDED PHOTOREFRACTIVE KERATECTOMY AND CORNEAL CROSS-LINKING IN EYES WITH PROGRESSIVE MILD TO MODERATE KERATOCONUS Session Title: CRS/RLE Session Date/Time: Saturday
JACK T. HOLLADAY, MD, MSEE, FACS (MODERATOR) MICHAEL W. BELIN, MD, FACS ARTURO S. CHAYET, MD MATTHIAS MAUS, MD PAOLO VINCIGUERRA, MD
 MICHAEL W. BELIN, MD, FACS ARTURO S. CHAYET, MD MATTHIAS MAUS, MD PAOLO VINCIGUERRA, MD") Next-Generation Technology for the Cataract & Refractive Surgeon Produced under an unrestricted educational grant from Oculus, Inc., and Oculus Optikgeraete GmbH. This monograph is based on an educational
Next-Generation Technology for the Cataract & Refractive Surgeon Produced under an unrestricted educational grant from Oculus, Inc., and Oculus Optikgeraete GmbH. This monograph is based on an educational
Visual outcome and patient satisfaction after corneal and refractive surgery
 Visual outcome and patient satisfaction after corneal and refractive surgery Copyright NG Tahzib, Maastricht 2008 ISBN: 978 90 5278 751 0 Cover Design: M. Schreuder en N.G. Tahzib Layout: Datawyse Printed
Visual outcome and patient satisfaction after corneal and refractive surgery Copyright NG Tahzib, Maastricht 2008 ISBN: 978 90 5278 751 0 Cover Design: M. Schreuder en N.G. Tahzib Layout: Datawyse Printed
What Makes a Good. Refractive Procedures
 What Makes a Good Refractive Procedure? Surgeons discuss their preferred treatments for various refractive errors. By Frik J. Potgieter, MB ChB (Stell), FCS (SA), MMed (Pret), FRCS (Edin); David T.C. Lin,
What Makes a Good Refractive Procedure? Surgeons discuss their preferred treatments for various refractive errors. By Frik J. Potgieter, MB ChB (Stell), FCS (SA), MMed (Pret), FRCS (Edin); David T.C. Lin,
FACTS YOU NEED TO KNOW ABOUT ADVANCED CUSTOMVUE LASER ASSISTED IN- SITU KERATOMILEUSIS (LASIK) LASER TREATMENT. Patient Information Booklet
 LASER TREATMENT. Patient Information Booklet") FACTS YOU NEED TO KNOW ABOUT ADVANCED CUSTOMVUE LASER ASSISTED IN- SITU KERATOMILEUSIS (LASIK) LASER TREATMENT Patient Information Booklet For mixed astigmatism from 1 to 5 diopters Please read this entire
FACTS YOU NEED TO KNOW ABOUT ADVANCED CUSTOMVUE LASER ASSISTED IN- SITU KERATOMILEUSIS (LASIK) LASER TREATMENT Patient Information Booklet For mixed astigmatism from 1 to 5 diopters Please read this entire
Effect of treatment zone diameter on the clinical results of femtosecond laser-assisted in situ
 Clinical and Experimental Vision and Eye Research Journal (2018), 1, 1 6 ORIGINAL ARTICLE Effect of treatment zone diameter on the clinical results of femtosecond laser-assisted in situ keratomileusis
Clinical and Experimental Vision and Eye Research Journal (2018), 1, 1 6 ORIGINAL ARTICLE Effect of treatment zone diameter on the clinical results of femtosecond laser-assisted in situ keratomileusis
Visual outcomes of Femto-LASIK for correction of residual refractive error after corneal graft
 Graefes Arch Clin Exp Ophthalmol (2013) 251:2601 2608 DOI 10.1007/s00417-013-2458-5 REFRACTIVE SURGERY Visual outcomes of Femto-LASIK for correction of residual refractive error after corneal graft Mohammad
Graefes Arch Clin Exp Ophthalmol (2013) 251:2601 2608 DOI 10.1007/s00417-013-2458-5 REFRACTIVE SURGERY Visual outcomes of Femto-LASIK for correction of residual refractive error after corneal graft Mohammad
Comparison of Newer IOL Power Calculation Methods for Eyes With Previous Radial Keratotomy PATIENTS AND METHODS. Patients
 Special Issue Comparison of Newer IOL Power Calculation Methods for Eyes With Previous Radial Keratotomy Jack X. Ma, 1 Maolong Tang, 2 Li Wang, 3 Mitchell P. Weikert, 3 David Huang, 2 and Douglas D. Koch
Special Issue Comparison of Newer IOL Power Calculation Methods for Eyes With Previous Radial Keratotomy Jack X. Ma, 1 Maolong Tang, 2 Li Wang, 3 Mitchell P. Weikert, 3 David Huang, 2 and Douglas D. Koch
Retrospective Testing of the Score for the Detection of Ectasia Susceptibility: A Case Report of Ectasia 7 Years after LASIK
 IJKECD 10.5005/jp-journals-10025-1055 Case Retrospective Report Testing of the Score for the Detection of Ectasia Susceptibility: Case Report of Ectasia 7 Years after LSIK Retrospective Testing of the
IJKECD 10.5005/jp-journals-10025-1055 Case Retrospective Report Testing of the Score for the Detection of Ectasia Susceptibility: Case Report of Ectasia 7 Years after LSIK Retrospective Testing of the
Abstracts. Edited by Dr. Tahir Mahmood. Effect of phacoemulsification on intraocular pressure in eyes with pseudoexfoliation Single-surgeon series
 Abstracts Edited by Dr. Tahir Mahmood Effect of phacoemulsification on intraocular pressure in eyes with pseudoexfoliation Single-surgeon series Shingleton BJ, Laul A, Nagao K, Wolff B, Donoghue MO, Eagan
Abstracts Edited by Dr. Tahir Mahmood Effect of phacoemulsification on intraocular pressure in eyes with pseudoexfoliation Single-surgeon series Shingleton BJ, Laul A, Nagao K, Wolff B, Donoghue MO, Eagan
A Patients Guide to Excimer Laser Refractive Surgery
 A Patients Guide to Excimer Laser Refractive Surgery March 2006 Contents 1. Introduction 2. Understanding your refractive error 3. Changing the eye s focus by surgery (refractive surgery) 4. Indications
A Patients Guide to Excimer Laser Refractive Surgery March 2006 Contents 1. Introduction 2. Understanding your refractive error 3. Changing the eye s focus by surgery (refractive surgery) 4. Indications
AcuTarget Measurements: Repeatability and Comparison to OPD-Scan III
 ORIGINAL ARTICLE AcuTarget Measurements: Repeatability and Comparison to OPD-Scan III Emmanuel Guilbert, MD; Alain Saad, MD; Damien Gatinel, MD ABSTRACT PURPOSE: To evaluate repeatability of the AcuTarget
ORIGINAL ARTICLE AcuTarget Measurements: Repeatability and Comparison to OPD-Scan III Emmanuel Guilbert, MD; Alain Saad, MD; Damien Gatinel, MD ABSTRACT PURPOSE: To evaluate repeatability of the AcuTarget
Examination of the cornea by very highfrequency
 Epithelial and Stromal Changes Induced by Intacs Examined by Three-dimensional Very Highfrequency Digital Ultrasound Dan Z. Reinstein, MD, MA(Cantab), FRCSC; Sabong Srivannaboon, MD; Simon P. Holland,
Epithelial and Stromal Changes Induced by Intacs Examined by Three-dimensional Very Highfrequency Digital Ultrasound Dan Z. Reinstein, MD, MA(Cantab), FRCSC; Sabong Srivannaboon, MD; Simon P. Holland,