Differential Diagnosis of Cushing s Syndrome
|
|
|
- Jane Lawson
- 6 years ago
- Views:
Transcription


1 Differential Diagnosis of Cushing s Syndrome Cushing s the Diagnostic Challenge Julia Kharlip, MD and Caitlin White, MD Endocrinology, Diabetes and Metabolism Perelman School of Medicine at the University of Pennsylvania Penn Pituitary Center 1
2 Disclosures Consultant, Chiasma 2
3 if you have never missed the diagnosis of ACTH-dependent Cushing syndrome, and you have never been fooled attempting to establish its cause, you should refer your patients with suspected hypercortisolism to somebody who has. 3 Findling J JCEM 2006
4 Overview Case of mild Cushing s disease: 1. Longitudinal observation with repetitive testing as means of achieving greater diagnostic certainty 2. Review testing for diagnosis versus localization. Exogenous Cushings and a role synthetic glucocorticoid serum testing to document occult systemic exposure 4
5 Cushing s Syndrome: Epidemiology Disorder of chronic excess of cortisol in endogenous Cushing s and synthetic glucocorticoid in exogenous Endogenous disease is rare: Incidence: 1-10 patients per million per year Cushingoid states due to exogenous steroid use are highly prevalent Difficulty and delay in diagnosis CD: 6 month to 10 years Bolland Clin Endocrinol 2011; Flitsch J Exp Clin Endocrinol Diabetes 2000; Psaras Exp Clin Endocrinol Diabetes 2011; Biller JCEM 2008; Clayton JCEM
6 Diagnostic Challenges Epidemiology: rarity Intra-individual variability related to severity of disease, duration and pre-morbid state Lack of a sensitive and specific diagnostic tests to follow the paradigm of: 1. Sensitive Screening Test 2. Specific Confirmatory Test 3. Reliable Localization Test for ACTH dependent Cushing s: Pituitary vs. Ectopic Source
7 Clinical Case #1: 32 yo F with Weight Gain Likelihood MOD LOW LOW-MOD Clinical Findings Physical Findings 40 lb weight gain; new pre- HTN menorrhagia, fatigue No DM, osteoporosis, easy bruising, muscle weakness Round face No centripetal adiposity No wide violaceous striae, no hirsutism No supraclavicular, dorsocervical fat pad 7
8 Clinical Case #1: 32 yo F with e Likelihood MOD Clinical Findings 40 lb weight gain; new pre- HTN menorrhagia, fatigue No DM, osteoporosis, easy bruising LOW LOW-MOD Physical Findings Round face No centripetal adiposity No wide violaceous striae, no hirsutism No supraclavicular, dorsocervical fat pad Biochem AM Cort: 12.2 ug/dl (6-19) ACTH: 50, 27 pg/ml (6-58) 24 UFC: 50 mcg/24 hr (< 50) 8

9 Initial Testing JCEM
10 Clinical Case #1: 32 yo F with e Likelihood MOD Clinical Findings 40 lb weight gain; New pre- HTN Irregular menses, fatigue No DM, osteoporosis LOW LOW-MOD Physical Findings Round face No centripetal adiposity No violaceous striae, no hirsutism No supraclavicular, dorsocervical fat pad Biochem AM Cort: 12.2 ug/dl (6-19) ACTH: 50, 27 pg/ml (6-58) 24 UFC: 59, 50 mcg/24 hr (< 50) LNSC 0.10, 0.09, 0.27 mcg/dl (<0.09) DST: Normal 10
11 Use of Repetitive Measurements To Overcome High Variability UFC and LNSC are highly variable within an individual patient Patients with Cushing s Disease: LNSC 35% (95% CI, 27-44%) 24 UFC 31% (95% CI, 24-39%) Obese: for LNSC 39% (95% CI, 26-57%); UFC: 48% (95% CI, 36-61%) Need at least 2 samples for LNSC and 24 UFC 11 Guttenberg et al in press ; Cost 1994; Elias JCEM 2014
12 Sensitivity and Specificity of Available Tests 12 Elamin JCEM 2014
13 Patient 1 Longitudinal Course 2013: Started acupuncture, herbal remedies, yoga therapy, calorie counting and exercise. Lost 20 lb, hypertension resolved, menstruation normalized. She felt better. 6 mos 1 yr 2 yrs 3 yrs 13
14 Subsequent Testing JCEM

15 Patient 1 Longitudinal Course Declined intervention 6 mos 1 yr 2 yrs 3 yrs 15

16 Patient 1 Longitudinal Course 2014: Gained 15 pounds, hypertension returned. Did not want surgery. Started on cabergoline 0.5 mg twice weekly 6 mos 1 yr 2 yrs 3 yrs 16
17 The Localization Studies: IPSS and CRH Stimulation Both capitalize on corticotroph adenoma cells retaining sensitivity to CRH Not a diagnostic test!!! Normal corticotroph cells will respond by in increase in ACTH and cortisol IPSS: Central: Peripheral ACTH 262 patients with CD, Ectopic and adrenal CS - IPS:P ratio of 2 in basal sample: Sens-ty 95%, Specificity 100% - IPS:P ratio of 3 in CRH-stim Sensitivity 100%, Specificity 100% 101 patients with CD and 17 patients with ectopic ACTH tumors ACTH inr of 35%: Sensitivity: 70-93%, Specificity 90-99% Cortisol incr of 20%: Sensitivity: 86-88%, Specificity 90-99% Nieman et al JCEM 1993; Oldfield NEJM 1991
18 The Localization Studies: IPSS and CRH Stimulation Both capitalize on corticotroph adenoma cells retaining sensitivity to CRH Not a diagnostic test!!! Normal corticotroph cells will respond by in increase in ACTH and cortisol 262 patients with CD, Ectopic and adrenal CS IPS:P ratio of 2 in basally: Sens 95%, Spec 100% IPS:P ratio of 3 with CRH-stim Sens 100%, Spec 100% CRH: 101 pts with CD and 17 pts with ectopic ACTH ACTH inr of 35%: Sens 70-93%, Spec 90-99% Cortisol incr of 20%: Sens 86-88%, Spec 90-99% 18
19 Patient 1 Localization CRH Stimulation March 20, 2015 ACTH (pg/ml) Cortisol (ug/dl) -15 MIN MIN MIN MIN 98.8 Max ACTH 15 MIN 93.3 Increase 24.5 >500% 30 MIN MIN MIN MIN 18.2 Dx of CD >35% ACTH >20% Cortisol Max Cortisol Increase 150% Nieman et al. JCEM 1993
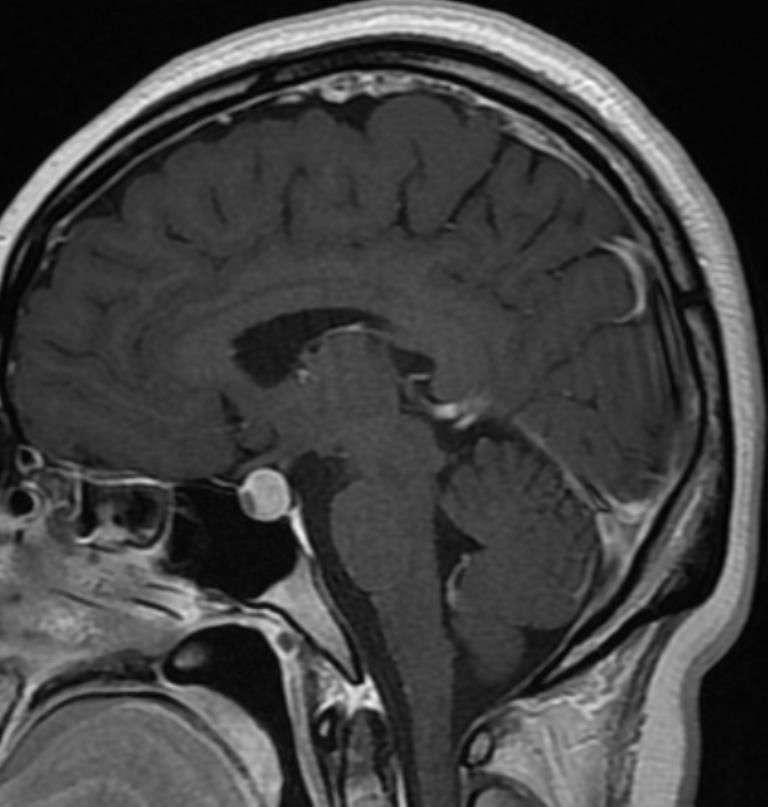
20 MRI 20
21 Patient 1 Longitudinal Course Agreed to TSS Path: Corticotroph Adenoma Lost 15lb BP and menses nl 6 mos 1 yr 2 yrs 3 yrs 21
22 Use of Repetitive Measurements Longitudinally Cushing s syndrome tends to progress: Accumulation of new features increases probability disease is present Endocrine Society Guidelines: We suggest further evaluation and follow-up for the few patients.. with discordant results, especially if the pretest probability of Cushing's syndrome is high (2 ). Timing of re-evaluation not deliniated

23 My Approach 1. Educate patients about diagnosis as a process 1. Multiple testing data points: 1. LNSC x 3; UFC x 2 2. Longitudinal re-evaluation (every 3-6 months) 3. Active surveillance with supportive clinical interventions Weight management Goal-directed PT aimed at abnormal weight re- -distribution and steroid myopathy Psychological counseling 23
24 24
25 Patient 1 - Conclusions 1. Mild Cushing s presents a diagnostic challenge 2. Cardinal clinical and physical stigmata may be absent 3. Biochemical results are often discrepant and/or minimally abnormal 4. Longitudinal repetitive testing leads to greater diagnostic certainty as the condition persists/evolves 5. In the meantime, supportive therapies can be given 25
26 Clinical Case #2: 36 yo F with fatigue and low cortisol AM Cortisol 2.1 mcg/dl, ACTH <5 pg/l L knee sports injury, s/p L knee replacement 5 months prior: Kenalog 40 mg (triamcinolone acetonide) L knee injection and 2 months before presentation another 80 mg ~400 mg HC Facial swelling & flushing, esophageal erosions, rapidly lost muscle mass collapsed on knee prosthesis within the month of 2 nd injection Physical Examination: Cushingoid appearing CT abdomen: normal adrenal glands 26
27 Triamcinolone Persisted in Circulation Beyond 5 Months Months after 2nd Kenalog injection ACTH pg/ml <2 < Cortisol ug/dl Triamcinolone ug/dl (<0.1) Neg
28 Clinical Case #2: 36 yo F with fatigue and low cortisol Oral estrogen in OCP likely delayed triamcinolone metabolism through p450 and renal clearance Recommendations: 1. Stop OCP or transition to transdermal Estrogen 2. Follow Sick day rules 3. Start physiologic replacement dose of HC 4. Physical Therapy to address steroid myopathy 28
29 HPA Axis Recovered 15 mo. After Last Triamcinolone Injection Hydrocortisone 29
30 Synthetic Glucocorticoid Screen: Send-out to Mayo Labs Ordering synthetic glucocorticoid screens: Test Name: Synthetic Glucocorticoid Screen, Serum Send out at hospital lab: Mayo Test Code: Quest Test Code: 99895, send to Mayo code #81031 Sample Requirement: 10mL red top or SST tube Method: LC-MS/MS 30
31 Patient 2 - Conclusion Use of synthetic glucocorticoid screen can be useful in detecting systemic absorption of glucocorticoids in patients with suppressed or low-normal ACTH, Cushingoid features and non-systemic forms of glucocorticoid use 31


32 Thank you 32
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
2
 1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
1 2 General % Obesity 90 Hypertension 85 Skin Plethora 70 Hirsutism/hair loss 75 Striae 50 Acne 35 Bruising/thinning 35 Musculoskeletal Osteopenia/porosis 80 Weakness 65 Neuropsych % Lability,euphoria,insomnia,
Cushing s syndrome and adrenal insufficiency
 Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cushing s syndrome and adrenal insufficiency Clinician expectations 1 ALIREZA ESTEGHAMATI,MD PROFESSOR OF ENDOCRINOLOGY TUMS APRIL 2016 Main Challenges Rare but important Mild forms (unrecognized) Cyclic
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS
 ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
ACTH-dependent Cushing s Syndrome Update AACE MI Chapter Annual Meeting September 22, 2018 Lynnette K. Nieman DEOB, NIDDK, NIH, DHHS Objectives At the conclusion of this presentation, participants should
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypercortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Adrenal
Audit of Adrenal Function Tests. Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK
 Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Audit of Adrenal Function Tests Kate Davies Senior Lecturer in Children s Nursing London South Bank University London, UK Introduction Audit Overview of adrenal function tests Education Audit why? Explore
Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO
 Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO I will not be discussing any off-label uses of medications. I am a paid speaker for: Amylin, BMS, BI, and
Sean Hamlett DO FACOI Endocrinology, Diabetes, and Metabolism Freeman Health System Joplin, MO I will not be discussing any off-label uses of medications. I am a paid speaker for: Amylin, BMS, BI, and
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Assessing Adrenal Function in Ill, Hospitalized Patients. Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism
 Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Therapeutic Objectives. Cushing s Disease Surgical Results. Cushing s Disease Surgical Results: Macroadenomas 10/24/2015
 Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
Therapeutic Objectives Update on the Management of Lewis S. Blevins, Jr., M.D. Correct the syndrome by lowering daily cortisol secretion to normal Eradicate any tumor that might threaten the health of
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia)
") The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia) Formulated by Ingrid. C.E. Wilkinson, Martin O. Savage, William M. Drake and Helen L. Storr in February 2018. Centre for
The Investigation of suspected paediatric Cushing s Syndrome (hypercortisolaemia) Formulated by Ingrid. C.E. Wilkinson, Martin O. Savage, William M. Drake and Helen L. Storr in February 2018. Centre for
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
A short & obese - girl
 A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
A short & obese - girl Presented by :Dr.Amit P Ghawade (DNB Resident-1st Year ) Guide :Dr.S.Ramkumar MD(pediatrics) ICH & HC, Chennai, DM(endocrinology) AIIMS, Delhi Department of Pediatric Endocrinology
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
14 Girl with Cushing s Disease: An Update. Kristen Dillard, MD Endorama October 17, 2013
 14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
14 Girl with Cushing s Disease: An Update Kristen Dillard, MD Endorama October 17, 2013 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Kristen Dillard, M.D. Endorama December 6, 2012
 Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the
Kristen Dillard, M.D. Endorama December 6, 2012 12 7/12 yo girl with h/o Cushing s disease presented to OSH with concern for CVA Consumed ½plate of food the night before, had raisins and diet soda on the
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
62-year-old woman with severe headache. Celeste Thomas November 1, 2012
 62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
62-year-old woman with severe headache Celeste Thomas November 1, 2012 History of Present Illness History of hypertension and hyperlipidemia Presented to outside hospital after awakening from sleep with
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
Challenging Pituitary Cases. Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine
 Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
Challenging Pituitary Cases Laurence Katznelson, MD Professor of Medicine and Neurosurgery Stanford University School of Medicine 1 34 yo male has incidental finding of large macroadenoma, with prolactin
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS
 The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
The analysis of Glucocorticoid Steroids in Plasma, Urine and Saliva by UPLC/MS/MS Brett McWhinney, Supervising Scientist, HPLC Section, Pathology Central, Pathology Queensland Overview 1. Overview of Pathology
CUSHING S SYNDROME. Chapter 8. Case: A 43-year-old man with delusions
 Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
Chapter 8 CUSHING S SYNDROME Case: A 43-year-old man with delusions A previously healthy 43-year-old man is brought to the emergency department for evaluation of confusion. The patient has complained to
CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES
 HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
HORMONES OF ADRENAL CORTEX R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty CHOLESTEROL IS THE PRECURSOR OF STERIOD HORMONES CONVERSION OF CHOLESTROL TO PREGNENOLONE MINERALOCORTICOCOIDES
Cortisol (serum, plasma)
") Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Cortisol (serum, plasma) 1 Name and description of analyte 1.1 Name of analyte Cortisol 1.2 Alternative names Hydrocortisone, 11β; 17, 21 trihydroxypregn 4 ene 3,20 dione 1.3 NMLC code 1.4 Description
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
Physiology. The Hypothalamic Pituitary Adrenal Axis. Elena A Christofides, MD, FACE
 Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
Elena A Christofides, MD, FACE Endocrinology Associates, Inc Endocrinology Research Associates, Inc Physiology 2 The Hypothalamic Adrenal Axis A Complex Set of Feedback Influences* Hypothalamus releases
Endogenous Cushing s syndrome: The Philippine general hospital experience
 ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
ORIGINAL ARTICLE Endogenous Cushing s syndrome: The Philippine general hospital experience Tom Edward N. Lo, Joyce M. Cabradilla, Sue Ann Lim, Cecilia A. Jimeno Section of Endocrinology and Metabolism,
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Endocrine Emergencies: Recognition and Management
 Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Endocrine Emergencies: Recognition and Management John Wass Department of Endocrinology, Oxford University, UK An Update on Acute Medical Emergencies for Psychiatrists Royal College of Psychiatrists' address
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Lawrence S. Kirschner, MD, PhD Professor of Medicine
 Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology
 Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Stelios Mantis, MD DuPage Medical Group Pediatric Endocrinology 4 11 13 Initial Presentation Pt initially presented to pediatrician for school physical in fall 2012. Pt was found to be overweight (BMI:
Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome
 Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
Case Reports in Endocrinology Volume 2013, Article ID 782068, 4 pages http://dx.doi.org/10.1155/2013/782068 Case Report Metyrapone for Long-Term Medical Management of Cushing s Syndrome Andrea N. Traina,
CUSHING'S SYNDROME. Bharath University, Chrompet, Chennai, Tamil Nadu, India
 TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Jun 2016, 57-62 TJPRC Pvt. Ltd. CUSHING'S SYNDROME R. RAMANI 1 & V. HEMAVATHY 2 1 Associate Professor,
TJPRC: International Journal of Nursing and Patient Safety & Care (TJPRC: IJNPSC) Vol. 1, Issue 1, Jun 2016, 57-62 TJPRC Pvt. Ltd. CUSHING'S SYNDROME R. RAMANI 1 & V. HEMAVATHY 2 1 Associate Professor,
Practical Management of Steroids in Non-Endocrine Practice
 Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
Practical Management of Steroids in Non-Endocrine Practice Dr Miguel Debono MD MRCP PhD Consultant Physician in Endocrinology and Honorary Senior Lecturer February 2016 Outline Epidemiology of steroids
10 yo boy w/chiari/pseudotumor seen for obesity. 8/22/13 Jess Hwang
 10 yo boy w/chiari/pseudotumor seen for obesity 8/22/13 Jess Hwang HPI Kids at school have been teasing him about his weight and the skin darkening around his neck 127lb was peak weight Quit desserts/soda
10 yo boy w/chiari/pseudotumor seen for obesity 8/22/13 Jess Hwang HPI Kids at school have been teasing him about his weight and the skin darkening around his neck 127lb was peak weight Quit desserts/soda
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease
 J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
J Neurosurg 83:1087 1091, 1995 False-positive inferior petrosal sinus sampling in the diagnosis of Cushing s disease Report of two cases YOSHIHIRO YAMAMOTO, M.D., D.M.SC., DUDLEY H. DAVIS, M.D., TODD B.
CUSHING S SYNDROME AND CUSHING S DISEASE
 PATIENT INFORMATION CUSHING S SYNDROME AND CUSHING S DISEASE YOUR QUESTIONS ANSWERED 2013 Update Contents What are Cushing s syndrome and Cushing s disease? What causes Cushing s syndrome and Cushing s
PATIENT INFORMATION CUSHING S SYNDROME AND CUSHING S DISEASE YOUR QUESTIONS ANSWERED 2013 Update Contents What are Cushing s syndrome and Cushing s disease? What causes Cushing s syndrome and Cushing s
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System
 PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Case Report Mifepristone Improves Octreotide Efficacy in Resistant Ectopic Cushing s Syndrome
 Case Reports in Endocrinology Volume 2016, Article ID 8453801, 5 pages http://dx.doi.org/10.1155/2016/8453801 Case Report Mifepristone Improves Octreotide Efficacy in Resistant Ectopic Cushing s Syndrome
Case Reports in Endocrinology Volume 2016, Article ID 8453801, 5 pages http://dx.doi.org/10.1155/2016/8453801 Case Report Mifepristone Improves Octreotide Efficacy in Resistant Ectopic Cushing s Syndrome
UW MEDICINE PATIENT EDUCATION. Cushing s Syndrome DRAFT. What is Cushing s syndrome? What is cortisol? What are the symptoms of Cushing s syndrome?
 UW MEDICINE PATIENT EDUCATION Cushing s Syndrome Causes, symptoms, diagnosis, and treatments This handout explains Cushing s syndrome, its causes, symptoms, and how it is diagnosed. It also includes a
UW MEDICINE PATIENT EDUCATION Cushing s Syndrome Causes, symptoms, diagnosis, and treatments This handout explains Cushing s syndrome, its causes, symptoms, and how it is diagnosed. It also includes a
Outline. Adrenal Insufficiency The Real & The Mythical. Primary vs Secondary
 Outline Adrenal Insufficiency The Real & The Mythical Leslie Eiland, MD Assistant Professor of Medicine Medical Director, Endocrine Telehealth Program Division of Diabetes, Endocrinology & Metabolism Adrenal
Outline Adrenal Insufficiency The Real & The Mythical Leslie Eiland, MD Assistant Professor of Medicine Medical Director, Endocrine Telehealth Program Division of Diabetes, Endocrinology & Metabolism Adrenal
Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study
Challenging Pituitary Cases
 Challenging Pituitary Cases Sue Samson, MD, PhD, FRCPC, FACE Associate Professor of Medicine and Neurosurgery Medical Director Pituitary Center Baylor College of Medicine, Houston TX Tom Blevins, MD, FNLA,
Challenging Pituitary Cases Sue Samson, MD, PhD, FRCPC, FACE Associate Professor of Medicine and Neurosurgery Medical Director Pituitary Center Baylor College of Medicine, Houston TX Tom Blevins, MD, FNLA,
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism
 Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
Adrenal Disorders for the USMLE, Step One: Abnormalities of the Fasciculata: Hypocortisolism Howard Sachs, MD Patients Course, 2017 Associate Professor of Clinical Medicine UMass Medical School Manifestations
I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT
 I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia Sezione di Endocrinologia, Università Federico II di Napoli, Italy 1 Treatment
I farmaci ad azione surrenalica: METIRAPONE ed OSILODROSTAT Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia Sezione di Endocrinologia, Università Federico II di Napoli, Italy 1 Treatment
X/97/$03.00/0 Vol. 82, No. 6 Journal of Clinical Endocrinology and Metabolism Copyright 1997 by The Endocrine Society
 0021-972X/97/$03.00/0 Vol. 82, No. 6 Journal of Clinical Endocrinology and Metabolism Printed in U.S.A. Copyright 1997 by The Endocrine Society Effectiveness Versus Efficacy: The Limited Value in Clinical
0021-972X/97/$03.00/0 Vol. 82, No. 6 Journal of Clinical Endocrinology and Metabolism Printed in U.S.A. Copyright 1997 by The Endocrine Society Effectiveness Versus Efficacy: The Limited Value in Clinical
Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy
 ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
ISPUB.COM The Internet Journal of Urology Volume 9 Number 1 Adrenal Ganglioneuroma Presenting With Adrenal Insufficiency After Unilateral Adrenalectomy S Bontha, N Sanalkumar, M Istarabadi, G Lepsien,
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
Emerging Challenges in Primary Care: Primary Care Endocrinology: The Adrenal and Pituitary Herding Horses and Zebras
 Emerging Challenges in Primary Care: 2017 Primary Care Endocrinology: The Adrenal and Pituitary Herding Horses and Zebras 1 Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty:
Emerging Challenges in Primary Care: 2017 Primary Care Endocrinology: The Adrenal and Pituitary Herding Horses and Zebras 1 Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty:
AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS
 Case Report AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS Gonul Catli, MD 1 ; Ayhan Abaci, MD 2 ; Ozgur Tanrisever, MD 3 ; Cemil Kocyigit, MD 4 ; P. Sule Can, MD 1 ; Bumin
Case Report AN UNUSUAL PRESENTATION OF PEDIATRIC CUSHING DISEASE: DIABETIC KETOACIDOSIS Gonul Catli, MD 1 ; Ayhan Abaci, MD 2 ; Ozgur Tanrisever, MD 3 ; Cemil Kocyigit, MD 4 ; P. Sule Can, MD 1 ; Bumin
ASTHMA TREATMENT AND THE HPA AXIS
 ASTHMA TREATMENT AND THE HPA AXIS Paul A. Greenberger, M.D. 7/12/2010 10:30-10:50 10:50 Objectives To review HPA axis suppression and its clinical significance in adults and children To describe methods
ASTHMA TREATMENT AND THE HPA AXIS Paul A. Greenberger, M.D. 7/12/2010 10:30-10:50 10:50 Objectives To review HPA axis suppression and its clinical significance in adults and children To describe methods
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules. Celeste Thomas November 1, 2012
 57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
57-year-old man with anxiety, diaphoresis, fatigue and bilateral adrenal nodules Celeste Thomas November 1, 2012 History of Present Illness 8 months prior to presentation developed intermittent right flank
Evaluation and Management of Pituitary Failure. Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS
, FRCPC Professor of Medicine Dalhousie University, Halifax, NS") Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Evaluation and Management of Pituitary Failure Dr S. Ali Imran MBBS, FRCP (Edin), FRCPC Professor of Medicine Dalhousie University, Halifax, NS Conflict of Interest None Objectives Diagnostic approach
Cushings Syndrome. Cushings Syndrome
 We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
Endocrine System Physiology
 M53_MARI0000_00_SE_EX04.qxd 7/15/11 4:32 PM Page 369 4 E X E R C I S E Endocrine System Physiology Advance Preparation/Comments Consider covering the following topics to prepare students for the simulation:
M53_MARI0000_00_SE_EX04.qxd 7/15/11 4:32 PM Page 369 4 E X E R C I S E Endocrine System Physiology Advance Preparation/Comments Consider covering the following topics to prepare students for the simulation:
Dr John Quin. Royal Sussex County Hospital, Brighton. BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions. None
 BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Dr John Quin Royal Sussex County Hospital, Brighton COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Dr John Quin None
BHIVA AUTUMN CONFERENCE 2013 Including CHIVA Parallel Sessions Dr John Quin Royal Sussex County Hospital, Brighton COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Dr John Quin None
Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male
 575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
Update on Cushing s disease (CD)
") Update on Cushing s disease (CD) Beverly MK Biller, MD Professor of Medicine Harvard Medical School Neuroendocrine Clinical Center Massachusetts General Hospital Boston, MA Disclosure of potential relevant
Update on Cushing s disease (CD) Beverly MK Biller, MD Professor of Medicine Harvard Medical School Neuroendocrine Clinical Center Massachusetts General Hospital Boston, MA Disclosure of potential relevant
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
LIMITATIONS OF BASAL CORTISOL IN THE DIAGNOSIS OF CUSHING S SYNDROME
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Therapeutic Cohort Results
 Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
Patient: SAMPLE PATIENT DOB: Sex: MRN: Menopause Plus - Salivary Profile Therapeutic Cohort Results Hormone Average Result QUINTILE DISTRIBUTION 1st 2nd 3rd 4th 5th Therapeutic Range* Estradiol (E2) 8.7
A case of failed bariatric surgery
 A case of failed bariatric surgery Gabriel I. Uwaifo, MD, FACP, FACE, FTOS, Department of Endocrinology, diabetes, metabolism and weight management, Ochsner medical center Case Presentation DH is a 35
A case of failed bariatric surgery Gabriel I. Uwaifo, MD, FACP, FACE, FTOS, Department of Endocrinology, diabetes, metabolism and weight management, Ochsner medical center Case Presentation DH is a 35
Transitions For the CAH Patient
 Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
Transitions For the CAH Patient Richard J. Auchus, M.D., Ph.D. Division of Metabolism, Endocrinology & Diabetes Department of Internal Medicine DSD Program University of Michigan Disclosures Contracted
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM
 DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
DIAGNOSIS OF CANINE HYPERADRENOCORTICISM: A CASE-BASED APPROACH Ellen N. Behrend, VMD, PhD, DACVIM Case 1: Signalment: 10 yr old, CM, Miniature poodle; History: Presented for teeth cleaning; PE: Severe
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
Cushings Syndrome. Cushings Syndrome
 We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
We have made it easy for you to find a PDF Ebooks without any digging. And by having access to our ebooks online or by storing it on your computer, you have convenient answers with cushings syndrome. To
Challenging Pituitary Cases
 Challenging Pituitary Cases Sue Samson, MD, PhD, FRCPC, FACE Associate Professor of Medicine and Neurosurgery Medical Director Pituitary Center Baylor College of Medicine, Houston TX Tom Blevins, MD, FNLA,
Challenging Pituitary Cases Sue Samson, MD, PhD, FRCPC, FACE Associate Professor of Medicine and Neurosurgery Medical Director Pituitary Center Baylor College of Medicine, Houston TX Tom Blevins, MD, FNLA,
Iatrogenic Cushing s Syndrome with Co-Administered Ritonavir and Corticosteroid via Inhaled, Intranasal, & Topical Route
 Abstract #384 Category A1 Iatrogenic Cushing s Syndrome with Co-Administered Ritonavir and Corticosteroid via Inhaled, Intranasal, & Topical Route Rory Okasaki-Gutierrez, Pharm.D. Co-Investigators: Patricia
Abstract #384 Category A1 Iatrogenic Cushing s Syndrome with Co-Administered Ritonavir and Corticosteroid via Inhaled, Intranasal, & Topical Route Rory Okasaki-Gutierrez, Pharm.D. Co-Investigators: Patricia
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London.
 In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
In memory of Thomas Addison M.D. Son of Joseph and Sarah Addison. Died June 29th 1860 aged 66 years. For 36 years physician to Guy s Hospital London. Adrenal insufficiency & Sick Day Rules Case history
Limitations of nocturnal salivary cortisol and urine free cortisol in the diagnosis of mild Cushing s syndrome
 European Journal of Endocrinology (2007) 157 725 731 ISSN 0804-4643 CLINICAL STUDY Limitations of nocturnal salivary cortisol and urine free cortisol in the diagnosis of mild Cushing s syndrome Srividya
European Journal of Endocrinology (2007) 157 725 731 ISSN 0804-4643 CLINICAL STUDY Limitations of nocturnal salivary cortisol and urine free cortisol in the diagnosis of mild Cushing s syndrome Srividya