Meredith L. Seamon, MD February 11, 2016
|
|
|
- Elfrieda Edwards
- 6 years ago
- Views:
Transcription

1 Meredith L. Seamon, MD February 11, 2016


2 DISCLOSURE I have no relevant financial relationships to disclose in regard to the content of this presentation
3 Objectives Hematuria List some common causes of urinary discoloration that are not hematuria and the definition of microscopic hematuria Differentiate between glomerular and non-glomerular etiologies of hematuria Know the common causes as well as the initial management approach to both microscopic and gross hematuria Know when to call your friendly local pediatric nephrologist!
4 Objectives Proteinuria Know the prevalence, mechanisms, and etiologies of proteinuria in the pediatric population Understand the different ways to measure proteinuria and the limitations of office testing Know the initial diagnostic evaluation to determine the pattern of proteinuria Once again, know when to call your friendly local pediatric nephrologist!
5 Case #1 5 year-old previously healthy boy Feels well, no urinary complaints Positive urine dipstick for 3+ blood found during kindergarten physical exam Normal work-up including renal ultrasound, BP, CBC, BMP Urinalysis in Nephrology clinic revealed urine SG of 1.025, moderate blood, and negative protein Microscopy notable for RBCs/hpf, no casts or crystals
6 Case #2 PCH ED 22:00 12 year-old previously healthy girl who presents with a two day history of brown colored urine Further history notable for: Swelling of eyelids, hands, around ankles x 2 days Sore throat ~ 2 weeks ago. Siblings also with sore throats around that time- strep negative. Exam: T: 37 C, P: 72/min, R: 20/min, BP 151/94, repeat manual BP of 144/104 +Facial fullness Slightly diminished breath sounds in the bilateral lung bases Abd: mild tenderness to palpation right upper and lower quadrants Trace pretibial and pedal edema No rashes
7 Case #3 16 y/o male 2 months ago had ~1 week of dark urine Decided to quit drinking Dr. Pepper and Pepsi since he thought that was causing the dark urine Didn t mention the episode to his parents Urine cleared, but then had a cold last week, and urine turned dark on the second day of illness Referred to Nephrology without further evaluation
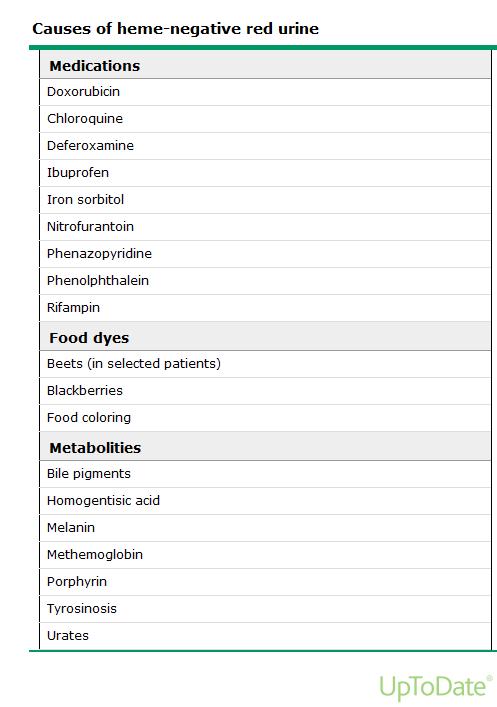
 Metabolites (like in")
8 Causes of Urinary Discoloration Blood (specifically hemoglobin) Myoglobin Pigments (found in some drugs and foods) Metabolites (like in porphyria)
9
10 Definition of Hematuria Abnormal presence of red blood cells (RBCs) in the urine Microscopic - Usually initially identified by positive urine dipstick - Confirmed with microscopy of spun urine specimen - ARUP says >2 RBCs/hpf is high (hpf = 40x objective) - Most papers use >5 RBCs/hpf (range 1-10) Gross - Discolored urine ~100 RBC/hpf or 1 ml/liter - Usually detected by anxious parents

11 Detecting Hematuria: Urine Dipsticks Reaction of Tetramethlybenzidine and hemoglobin/myoglobin turns blue-green False positives: alkaline urine or certain agents used to clean perineum False negatives are very rare Urine dipstick has a good negative predictive value for hematuria
12 Detecting Hematuria: Urine Microscopy Microscopy of centrifuged urine sediment looking for: Casts=Red, white, granular Acanthocytes to assess for glomerular bleeding Red supernatant without sediment indicates hemoglobinuria/myoglobinuria Crystals-Not often found, but cool when they are present


13 Urine Microscopy: Red Cell Casts RBC casts represent glomerulonephritis



14 Urine Microscopy: Acanthocytes Blebs occur as RBCs are squeezed through the glomerular basement membrane Kidney International, Vol. 59 (2001), pp Pediatrics in Review Vol.29 No.10 October 2008
15 Epidemiology of Hematuria ,954 Finnish students age 8-13 years old Hematuria defined as 1+ or greater on dipstick, which was confirmed by 6 or more RBCs/hpf on microscopy 4 samples were collected from each student and brought to school 35,784 urine samples J. Peds. 1979,
16 Epidemiology of Hematuria ~4% (364/8,954) were positive on a single sample 1% (95/8,954) had heme in 2 or more samples 0.2% (22/8,954) had heme in all 4 samples 72/95 with heme in 2 samples were evaluated All had normal kidney function. 5 UTI, 2 low C3, 4 with high ESR 28 biopsies 4 with actual kidney disease 2 IgA, 1 FSGS, 1 Alport syndrome J. Peds. 1979,
17 Epidemiology of Hematuria ~4% (364/8,954) were positive on a single sample 1% (95/8,954) had heme in 2 or more samples 0.2% (22/8,954) had heme in all 4 samples 72/95 with heme in 2 samples were evaluated All had normal kidney function. 5 UTI, 2 low C3, 4 with high ESR 28 biopsies 4 with actual kidney disease 2 IgA, 1 FSGS, 1 Alport syndrome J. Peds. 1979,
18 Epidemiology of Hematuria Take home message: 3-5% of Finnish children will have hematuria on a single sample and 0.5-1% on 2 or more samples Check multiple samples to confirm hematuria J. Peds. 1979,
19 Clinical Significance of Hematuria 570 children ages 1 month-19 years referred to Pediatric Nephrology at Riley Children s Hospital in Indianapolis from for asymptomatic hematuria Microscopic (>5 RBC/hpf) = 342 children Gross = 228 children Evaluation included: H & P with BP measurement CBC, UA, BMP, C3, urine culture Timed urine for CrCl Ultrasound or IVP Arch Pediatr Adolesc Med. 2005;159:
20 Clinical Significance of Microscopic Hematuria 342 children with microscopic hematuria No cause identified in 274 patients (80%) Most commonly identified cause was hypercalciuria without stones in 56 (16%) Post-strep GN in 4 children Duplex collecting system in 2 children 1 patient each with a kidney stone, IgA nephropathy, MPGN, single kidney, unilateral hypoplasia, and VUR. NO urinary tract infections identified (selection bias?) Basically 3/342 (0.01%) had a disease (IgA, MPGN, and VUR) that had potential for progressive CKD Arch Pediatr Adolesc Med. 2005;159:
21 Clinical Significance of Gross Hematuria 228 children with gross hematuria No cause identified in 86 patients (38%) 51 patients (22%) had hypercalciuria without stones 34 (15%) with IgA nephropathy 21 (9%) with post-strep GN 8 due to exercise 1 UTI 34/228 (15%) had a diagnosis that posed a risk of progressive CKD No SLE with gross hematuria alone Arch Pediatr Adolesc Med. 2005;159:
22 Clinical Significance of Hematuria Take away message from this study: Basically, 2-3/342 with isolated microscopic hematuria had an etiology with risk of progression of renal disease (MPGN, IgA, VUR), but none had proteinuria or hypertension Microscopic hematuria requires work-up (mainly repeating a urinalysis WITH MICROSCOPY), but does not need to be done emergently AAP no longer recommends routine urinalyses Important to reassure families Gross hematuria, however, requires investigation Arch Pediatr Adolesc Med. 2005;159:
23 ABCs of Hematuria Anatomic-obstruction or other structural abnormalities (collecting system duplication), nutcracker syndrome, renal vein thrombosis Boulders-stones Cancer Wilms Tumor, very, very rarely renal cell carcinoma Drugs Ingestions, interstitial nephritis Exercise Familial-Alport syndrome, thin basement membrane disease, Hereditary nephritis without deafness. Glomerulonephritis -Acute, chronic, hereditary Hemoglobinopathies/Coagulopathies/Myopathies Infection, Injury
24 Evaluation of Microscopic Hematuria Confirm hematuria with urinalysis with MICROSCOPY on sequential samples at least one week apart History: Recent illness, family history of nephrolithiasis, family history of hematuria, family history of hearing loss/vision problems, fluid intake Exam: Blood pressure, presence of edema?, meatal/perineal irritation, CVA tenderness Evaluation: Urine culture, urine for calcium to creatinine ratio (if elevated, obtain 24 hour urine collection), renal ultrasound, renal function panel, C3
25 Evaluation of Gross Hematuria History: Fever, urinary symptoms, rash, arthralgias, abdominal/flank pain, edema, proteinuria, hypertension Evaluation: Urine microscopy (glomerular vs. nonglomerula), urine culture, urine for calcium to creatinine ratio (if elevated, obtain 24 hour urine collection), imaging (possibly renal ultrasound or CT scan), and renal function panel. Additional labs to consider- C3, protein to creatinine ratio
26 Hematuria: Prognosis/Intervention Asymptomatic microscopic hematuria: -Most cases resolve within ~ 5 years -Most commonly identified cause is hypercalciuria -Provide counseling regarding increasing fluid/water intake -Why water? Only therapeutic intervention show to reduce frequency of kidney stones. -Monitor every 6-12 months Symptomatic microscopic, or gross, hematuria- depends on underlying pathophysiology Hypercalciuria/stones tend to recur Drink water IgA highly variable, watch for proteinuria. Post-strep resolves
27 Case #1 5 year-old boy RBCs/hpf found on 3 occasions Parents asked to give urine samples in clinic (kids love that part)- both negative (looking for thin basement membrane disease) Review of UAs showed Spec grav Spot Ca/Cr x 3 = mg/mg (nml < 0.2) Hypercalciuria stone risk. FH positive for mother and uncle with stones. Treat with increased fluid x 6 months. Water, Crystal Light, flavored water, Kool-Aid made with ½ recommended sugar.
28 Case #2 12 year-old girl with hypertension and brown urine Labs Na: 140 Cl: 107 BUN: 15 Gluc: 79 K: 4 CO2: 22 Cr: 0.68 Ca 8.7, Albumin 3.1 Urinalysis: SG 1.025, ph 6.5, 1+ ketones, large heme, 3+ protein. Micro: TNTC dysmorphic RBCs, occasional red cell casts C4 15 (nl 11-61), C3 12 (nl ) AntiDNase B 1570 (nl 0-170) First a.m. UPC- 1.1 mg/mg
29 Case #2 Hospital Course - Required inpatient management for ~ 2 days for management of hypertension - Blood pressure trend improved with amlodipine and Lasix - Discharged on amlodipine 7.5 mg PO BID Follow-up.. - C3 normalized ~7 weeks after her initial presentation - Ongoing increased urinary protein excretion with first a.m. prot/cr ~ 1 mg/mg two months after her initial presentation, thus amlodipine discontinued, and started on lisinopril
30 Case #3 16 y/o male with recurrent gross hematuria; second episode clearly associated with illness Cutting out soda did not help UA with 3+ protein, Prot/Cr 1.8, BP 145/88, Cr 1 mg/dl Biopsy = IgA; started on ACEi
31 Proteinuria
32 Case #1 17 year-old girl; found to have 3+ proteinuria at cheerleading physical Straight A high school senior Healthy, very active, c/o some joint pain and fatigue x 6 months Remote history of UTI x 2, no hospitalizations, no fever, no edema Seen by adult nephrologist Normal U/S and VCUG, ANA & Anti dsdna neg x2, ANCA neg x2, complement studies neg x2, CT angiogram normal, 24 hour with 760 mg protein, course of steroids made no difference
33 Case #1 Nephrology clinic: Mother exceedingly anxious Patient s physical exam: -Healthy appearing athlete -Ht 50% Wt 25% BMI HR 65 BP 100/72 T Otherwise normal Screening test -Urine dip 2+ protein, no heme
34 Case #2 5 year-old boy with 3 month history of swelling Tried Benadryl, which didn t help. Allergy testing negative. Swelling worse around eyes in a.m., then feet get swollen in p.m. Shoes hurt. Unremarkable PMH and FH Urine dip shows 4+ protein, trace blood. Labs done at InstaCare last week showed Na 131, Cr 0.4, alb 1.4, Ca 7.9, lytes otherwise normal
35 Proteinuria Proteinuria is well established as a marker of renal disease Even though proteinuria is more likely to be associated with renal disease than hematuria, the work-up is easier because of the smaller differential diagnosis Normal protein excretion is up to 100 mg/m2/day, or ~150mg/day in older children; higher in neonates Urinary albumin excretion is usually < 20 mg/day
36 Proteinuria Proteinuria is well established as a marker of renal disease Even though proteinuria is more likely to be associated with renal disease than hematuria, the work-up is easier because of the smaller differential diagnosis Normal protein excretion is up to 100 mg/m2/day, or ~150mg/day in older children; higher in neonates Urinary albumin excretion is usually < 20 mg/day
37 Proteinuria: Epidemiology ,954 Finnish students age 8-13 years old Proteinuria present in 959/8,954 (~11%) after one sample Two samples: 223/8,954 (2.5%) positive 9/8,954 (0.1%) had protein in four samples J Pediatr Nov;101(5):661-8.
38 Proteinuria: Mechanisms Glomerular Filtration of blood proteins across glomerular capillary wall May result in edema, hypoalbuminemia and elevated cholesterol (nephrotic syndrome) Tubular Loss of low molecular weight proteins such as beta-2-microglobulin and retinol binding protein due to inability of tubular cells to reabsorb the proteins (example, interstitial nephritis) Overflow Excretion of proteins due to overproduction as in multiple myeloma
39 Proteinuria: Patterns Transient: May occur with stress or increased activity such as fever, seizure, acute illness, dehydration, or vigorous exercise Orthostatic (Postural): Blood flow to kidney decreases in recumbent and increases in standing position Accounts for about 60-75% of childhood and adolescent proteinuria Present in ~2-5% of older children and adolescents Increased urinary protein excretion while upright Typically benign, 80% resolve 20 years after diagnosis Persistent (6-12 months): Usually indicates underlying renal disease Concomitant hematuria, may represent glomerulonephritis

40 Proteinuria: Detection Urine dipstick measures albumin in a semi-quantitative way Albumin reacts with tetrabromophenol and turns blue Does not measure other proteins, so low molecular weight proteins not assessed
41 Proteinuria: Detection Urine dipsticks measure urine protein concentration, but not excretion rates A very concentrated urine may have 1-2+ protein, but the patient may not actually have increased protein excretion Proteinuria may be quantified with a spot urine pr/cr ratio Removes the urine concentration from the equation Normal is < 0.2 mg/mg Nephrotic range is >2 mg/mg Measures albumin and LMW proteins Spot pr/cr is comparable and much easier than 24 hour collection
42 Proteinuria: Initial Evaluation If greater than trace proteinuria, obtain a first morning urine sample for a protein to creatinine ratio (normal <0.2 mg/mg) Obtain after a 24 hour period without vigorous excercise Patient should empty bladder before bed Renal function panel (BMP + albumin + phosphorus) Blood pressure measurement
43 Orthostatic Proteinuria Blood flow to kidney decreases in recumbent and increases in standing position Affected individuals usually tall and thin, but not always Some individuals have mild hyperfiltration when standing mild proteinuria Proteinuria disappears/greatly reduced when recumbent Diagnosis: First morning protein to creatinine ratio normal with elevated urinary protein excretion on clinic samples Considered benign Monitor annually with first morning prot/cr ratio
44 Fixed Proteinuria History: Febrile UTIs (renal scarring), edema, gross hematuria, family history Check BP Initial labs: CBC, RFP, lipid panel (if nephrotic range) Renal ultrasound, C3, C4, ANA, anti-dsdna, hepatitis serologies Biopsy MCD, FSGS, Membranous nephropathy, Lupus nephritis, MPGN
45 Case #1 17 y/o female Seen by adult nephrologist Normal US and VCUG, ANA & Anti dsdna x2, ANCA x2, Complement studies x2, CT angiogram normal, 24 hour urine with 760 mg protein, course of steroids made no difference. Cost ~ $10,000? Family expected a kidney biopsy that day, in clinic. 1 st am urine negative, urine dipstick ~ cents. Cured. Mother still concerned about fatigue, malaise. Orthostatic proteinuria Hydrostatic forces increase protein excretion typically in young, thin adolescents and children Benign, 80% resolve within 20 years 24 hour urine typically with mg/day, rarely nephrotic range 50 year follow up of some cases showed no increase risk of CKD
46 Case #2 5 year-old boy with 3 month history of swelling Tried Benadryl, which didn t help. Allergy testing negative. Swelling worse around eyes in a.m., then feet get swollen in p.m. Shoes hurt. Unremarkable PMH and FH Urine dip shows 4+ protein, trace blood. Labs done at InstaCare last week showed Na 131, Cr 0.4, alb 1.4, Ca 7.9, lytes otherwise normal Up/c 5.8, cholesterol 720, ica 1.25.
47 Case #2 Nephrotic Syndrome Podocytopathy? Immune dysfunction Treatment: steroids ~85% in children will have minimal change disease 15-30% may have associated microscopic hematuria Hypocalcemia due to hypoalbuminemia, normal ica Hypercholesterolemia due to increased hepatic synthetic activity
48 Summary: Hematuria Routine urine screening no longer recommended by AAP Asymptomatic hematuria: Confirm hematuria with repeat dipsticks AND microscopy Microscopy to assess appearance of RBCs and for presence of casts Ultrasound Urine culture, RFP, CBC Other steps: C3, C4, antidnase B, ANA, anti-dsdna, 24 hour urine for stone panel, CT scan depending on history.
49 Summary: Proteinuria Proteinuria Confirm presence of fixed proteinuria with first morning urine for protein to creatinine ratio If confirmed: Obtain RFP, CBC, C3, C4, ANA, anti-dsdna, hepatitis serologies Ultrasound History and physical- especially BP measurement and assessment of any edema HTN: To reinforce, if there are concerns for any renal disease in children, BP must be obtained


50 Who Ya Gonna Call? Pediatric Nephrology at University of Utah/Primary Children s Hospital Dr. Raoul Nelson Dr. Joseph Sherbotie Dr. Matt Grinsell Dr. Meredith Seamon Debra Sandt, CPNP Beth Esparza, RN Cindy Terrill, RD Clinic scheduling: On call: Physician Access Line:
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Dr P Sigwadi 30 May 2012
 Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Dr P Sigwadi 30 May 2012 Introduction Haematuria Positive blood on urine dipstick 5 red blood cells/ microliter of urine Prevalence Gross haematuria ( macroscopic) 0.13 % Microscopic- 1.5% Haematuria +
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Examination by dipstick: (Orthotoluidine & organic peroxidase) Hemoglobin free in urine. Hemoglobin from red blood cells in urine.
 Hemoglobin free in urine. Hemoglobin from red blood cells in urine.") Examination by dipstick: (Orthotoluidine & organic peroxidase) Hemoglobin free in urine Hemoglobin from red blood cells in urine Myoglobin Normal erythrocyte excretion rate * 0 425.000/12 h. ( mean 65.750
Examination by dipstick: (Orthotoluidine & organic peroxidase) Hemoglobin free in urine Hemoglobin from red blood cells in urine Myoglobin Normal erythrocyte excretion rate * 0 425.000/12 h. ( mean 65.750
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Hematuria. Ramzi El-Baroudy (ESPNT)
") Hematuria Ramzi El-Baroudy (ESPNT) Hematuria is the presence of RBCs in urine. If the amount of blood in urine is big enough, the urine will, then, look red. Something which is, undoubtedly, terrifying.
Hematuria Ramzi El-Baroudy (ESPNT) Hematuria is the presence of RBCs in urine. If the amount of blood in urine is big enough, the urine will, then, look red. Something which is, undoubtedly, terrifying.
AN APPROACH TO HEMATURIA. Dr Saima Ali
 AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
AN APPROACH TO HEMATURIA Dr Saima Ali Definition Microscopic hematuria hematuria is defined as the presence of 5 or more RBCs per high-power field in 3 of 3 consecutive centrifuged specimens obtained at
MODULE 5: HEMATURIA LEARNING OBJECTIVES DEFINITION. KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer
 MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
MODULE 5: HEMATURIA KEY WORDS: Hematuria, Cystoscopy, Urine Cytology, UTI, bladder cancer LEARNING OBJECTIVES At the end of this clerkship, the learner will be able to: 1. Define microscopic hematuria.
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Pediatric Nephrology Consult and Referral Guidelines
 Pediatric Nephrology Consult and Referral Guidelines Introduction We see children and teens from birth to 21 years. The most common reasons patients are referred to pediatric nephrology services include:
Pediatric Nephrology Consult and Referral Guidelines Introduction We see children and teens from birth to 21 years. The most common reasons patients are referred to pediatric nephrology services include:
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Urinalysis Competition Dr. Katharine Dahl Dr. Brenda Shinar
 Urinalysis Competition 2017 Dr. Katharine Dahl Dr. Brenda Shinar Question 1. (PGY-1) An appropriate collection technique must be used in order to interpret urinalysis correctly. Which of the following
Urinalysis Competition 2017 Dr. Katharine Dahl Dr. Brenda Shinar Question 1. (PGY-1) An appropriate collection technique must be used in order to interpret urinalysis correctly. Which of the following
Guidelines for the management of a child with haematuria
 Guidelines for the management of a child with haematuria Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the author(s)
Guidelines for the management of a child with haematuria Children s Kidney Centre University Hospital of Wales Cardiff CF14 4XW DISCLAIMER: These guidelines were produced in good faith by the author(s)
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome. Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium
 Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Clots and Foamy Urine: Thrombotic Complications of Nephrotic Syndrome Prayus Tailor, MD October 5, 2013 Renal and Hypertension Symposium Objectives Discuss the pathophysiology of thrombosis in nephrotic
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
RED URINE. 24 th June 2016 Dr Amrit Kaur
 RED URINE 24 th June 2016 Dr Amrit Kaur 4 year old male with macroscopic haematuria 5 month h/o intermittent MaH 12 episodes, coca-cola urine Treated for UTIs, urine cultures negative Urine dipstick always
RED URINE 24 th June 2016 Dr Amrit Kaur 4 year old male with macroscopic haematuria 5 month h/o intermittent MaH 12 episodes, coca-cola urine Treated for UTIs, urine cultures negative Urine dipstick always
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
H(a)ematuria. FX Keeley Consultant Urologist Bristol Urological Institute
ematuria. FX Keeley Consultant Urologist Bristol Urological Institute") H(a)ematuria FX Keeley Consultant Urologist Bristol Urological Institute From Philadelphia to Bristol, England Southmead Hospital, 1916 Southmead Hospital, 2013 Southmead Hospital, 2014 H(a)ematuria Blood
H(a)ematuria FX Keeley Consultant Urologist Bristol Urological Institute From Philadelphia to Bristol, England Southmead Hospital, 1916 Southmead Hospital, 2013 Southmead Hospital, 2014 H(a)ematuria Blood
Foamy Urine and Sickled Cells. Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA
 Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane / Ochsner Residency Program New Orleans, LA Foamy Urine and Sickled Cells Margaret Prat Huntwork, MD, MSEd Tulane University Health
URINE DIPSTICK AND SULPHOSALICYLIC ACID TEST. Špela Borštnar UREX 2015, Ljubljana, Slovenia
 URINE DIPSTICK AND SULPHOSALICYLIC ACID TEST Špela Borštnar UREX 2015, Ljubljana, Slovenia KIDNEY DISEASE? severity of kidney disease = estimating GFR cause of kidney disease = urinalysis URINE EXAMINATION
URINE DIPSTICK AND SULPHOSALICYLIC ACID TEST Špela Borštnar UREX 2015, Ljubljana, Slovenia KIDNEY DISEASE? severity of kidney disease = estimating GFR cause of kidney disease = urinalysis URINE EXAMINATION
CKD FOR PRIMARY CARE MINNESOTA ACADEMY OF PHYSICIANS 2017 HEATHER ANN MUSTER, MD MS
 CKD FOR PRIMARY CARE MINNESOTA ACADEMY OF PHYSICIANS 2017 HEATHER ANN MUSTER, MD MS PLoS One. 2014 Nov 26;9(11):e110535. Of the 445 PCPs who enrolled at least 10 patients, 19 (4.3%) had >50% likelihood
CKD FOR PRIMARY CARE MINNESOTA ACADEMY OF PHYSICIANS 2017 HEATHER ANN MUSTER, MD MS PLoS One. 2014 Nov 26;9(11):e110535. Of the 445 PCPs who enrolled at least 10 patients, 19 (4.3%) had >50% likelihood
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Alterations of Renal and Urinary Tract Function
 Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
Alterations of Renal and Urinary Tract Function Chapter 29 Urinary Tract Obstruction Urinary tract obstruction is an interference with the flow of urine at any site along the urinary tract The obstruction
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi
 Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Dr. Rai Muhammad Asghar Head of Paediatric Department BBH Rawalpindi Acute Post streptococcal Glomerulonephritis Sudden onset of Gross hematuria Edema Hypertension Renal insufficiency Cause of AGN Post
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Lab 3, case 1. Is this an example of nephrotic or nephritic syndrome? Why? Which portion of the nephron would you expect to be abnormal?
 Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Lab 3, case 1 12-year-old Costa Rican boy is brought into clinic by his parents because of dark brownish-red urine over the last 24 hours. The family has been visiting friends in Indianapolis for two weeks.
Pediatric GU Dysfunction
 Pediatric GU Dysfunction Assessment of pediatric renal function Signs and symptoms Laboratory tests Radiological tests Nursing considerations Psychosocial and developmental considerations GU Disorders
Pediatric GU Dysfunction Assessment of pediatric renal function Signs and symptoms Laboratory tests Radiological tests Nursing considerations Psychosocial and developmental considerations GU Disorders
GENERAL URINE EXAMINATION (URINE ANALYSIS)
") GENERAL URINE EXAMINATION (URINE ANALYSIS) Physiology Lab-8 December, 2018 Lect. Asst. Zakariya A. Mahdi MSc Pharmacology Background Urine (from Latin Urina,) is a typically sterile liquid by-product of
GENERAL URINE EXAMINATION (URINE ANALYSIS) Physiology Lab-8 December, 2018 Lect. Asst. Zakariya A. Mahdi MSc Pharmacology Background Urine (from Latin Urina,) is a typically sterile liquid by-product of
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6
 Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
Advanced Pathophysiology Unit 7: Renal-Urologic Page 1 of 6 Learning Objectives for this File: 1. Understand how clinical presentation drives the diagnostic workup 2. Recognize how patient education is
PRINCIPLE OF URINALYSIS
 PRINCIPLE OF URINALYSIS Vanngarm Gonggetyai Objective Can explain : the abnormalities detected in urine Can perform : routine urinalysis Can interprete : the results of urinalysis Examination of urine
PRINCIPLE OF URINALYSIS Vanngarm Gonggetyai Objective Can explain : the abnormalities detected in urine Can perform : routine urinalysis Can interprete : the results of urinalysis Examination of urine
Professor Suetonia Palmer
 Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Professor Suetonia Palmer Department of Medicine Nephrologist Christchurch Hospital Christchurch 14:00-14:55 WS #108: The Kidney Test - When To Test and When to Refer ( and When Not To) 15:05-16:00 WS
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
Nephrotic Syndrome. Sara Alsharhan PharmD candidate, KSU 2014
 Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
Nephrotic Syndrome Sara Alsharhan PharmD candidate, KSU 2014 Outline Introduction Nephrotic syndrome classifications Signs and symptoms Diagnoses Management Complications Monitoring Case presentation Introduction
CKD FOR INTERNISTS. Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College
 CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
CKD FOR INTERNISTS Dr Ahmed Hossain Associate professor Medicine Sir Salimullah Medical College INTRODUCTION In 2002, the National Kidney Foundation s Kidney Disease Outcomes Quality Initiative(KDOQI)
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Nephrology
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Nephrology 1. GOAL: Understand the general pediatrician's role in diagnosis and management of hypertension in children.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Nephrology 1. GOAL: Understand the general pediatrician's role in diagnosis and management of hypertension in children.
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Urinary tract infections, renal malformations and scarring
 Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Urinary tract infections, renal malformations and scarring Yaacov Frishberg, MD Division of Pediatric Nephrology Shaare Zedek Medical Center Jerusalem, ISRAEL UTI - definitions UTI = growth of bacteria
Hey Doc, there s blood in my urine Evaluation of hematuria. Christian S. Kuhr, MD FACS May 4, 2018
 Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
GOOD MORNING. Welcome Applicants! Friday, October 31, (Happy Halloween!)
") GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
GOOD MORNING Welcome Applicants! Friday, October 31, 2014 (Happy Halloween!) PREP QUESTION A 14-year-old girl has had 3 days of new, unremitting headache associated with vomiting and awakening from sleep
HIHIM 409 7/26/2009. Kidney and Nephron. Fermamdo Vega, M.D. 1
 Function of the Kidneys Nephrology Fernando Vega, M.D. Seattle Healing Arts Center Remove Wastes Regulate Blood Pressure Regulate Blood Volume Regulates Electrolytes Converts Vitamin D to active form Produces
Function of the Kidneys Nephrology Fernando Vega, M.D. Seattle Healing Arts Center Remove Wastes Regulate Blood Pressure Regulate Blood Volume Regulates Electrolytes Converts Vitamin D to active form Produces
PRE-RENAL AKI: DOES IT LEAD TO ATN. Sushma Bhusal
 PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
PRE-RENAL AKI: DOES IT LEAD TO ATN Sushma Bhusal 9.9.14 CASE PRESENTATION CC : 31 AAM presented with Fatigue, malaise and body aches x 10 days HPI: STD testing done 2 weeks prior, all results negative
Nursing Care for Children with Genitourinary Dysfunction I
 Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Nursing Care for Children with Genitourinary Dysfunction I 1 Assessment of renal function Clinical manifestations Laboratory tests Urinalysis Urine culture and sensitivity Renal/bladder ultrasound Testicular
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
16.1 Risk of UTI recurrence in children
 16. UTI prognosis 16.1 Risk of UTI recurrence in children Key question: What is the risk of recurrent UTI in children with no known structural or functional abnormalities of the urinary tract with a first
16. UTI prognosis 16.1 Risk of UTI recurrence in children Key question: What is the risk of recurrent UTI in children with no known structural or functional abnormalities of the urinary tract with a first
Steroid Resistant Nephrotic Syndrome. Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta
 Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
Steroid Resistant Nephrotic Syndrome Sanjeev Gulati, Debashish Sengupta, Raj K. Sharma, Ajay Sharma, Ramesh K. Gupta*, Uttam Singh** and Amit Gupta From the Departments of Nephrology, Pathology* and Biostatistics**,
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions. Jonathan Evans Paediatric Nephrologist
 The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Taking a dip into urinalysis
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Taking a dip into urinalysis Author : Christine Jameison Categories : RVNs Date : July 1, 2009 Christine Jameison RVN, probes
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Taking a dip into urinalysis Author : Christine Jameison Categories : RVNs Date : July 1, 2009 Christine Jameison RVN, probes
Acute Kidney Injury (AKI)
") (Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
(Last Updated: 08/22/2018) Created by: Socco, Samantha Acute Kidney Injury (AKI) Thambi, M. (2017). Acute Kidney Injury. Lecture presented at PHAR 503 Lecture in UIC College of Pharmacy, Chicago. AKI This
Henoch-Schonlein Purpura Guidelines
 Henoch-Schonlein Purpura Guidelines Henoch-Schonlein purpura (HSP) is the commonest vasculitis of childhood which is selflimiting in majority of cases. Epidemiology: Incidence varies from 10-20 per 100000
Henoch-Schonlein Purpura Guidelines Henoch-Schonlein purpura (HSP) is the commonest vasculitis of childhood which is selflimiting in majority of cases. Epidemiology: Incidence varies from 10-20 per 100000
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Health Examination Result Description Oct
 Health Examination Result Description Oct.15.2011 Height and Weight 1. There are two commonly used methods for calculating the standard weight as the followings: (1) Body mass index (BMI)= weight (kg)
Health Examination Result Description Oct.15.2011 Height and Weight 1. There are two commonly used methods for calculating the standard weight as the followings: (1) Body mass index (BMI)= weight (kg)
Approach to Proteinuria and Hematuria
 Approach to Proteinuria and Hematuria 5 Clinical Scenarios Common to the Boards Ajay K. Singh, MB., FRCP Physician, Renal Division, Brigham and Women s Hospital, Senior Associate Dean for Postgraduate
Approach to Proteinuria and Hematuria 5 Clinical Scenarios Common to the Boards Ajay K. Singh, MB., FRCP Physician, Renal Division, Brigham and Women s Hospital, Senior Associate Dean for Postgraduate
Detection and Estimation of Some Abnormal Constituents. Amal Alamri
 Detection and Estimation of Some Abnormal Constituents Amal Alamri Lecture Over view Abnormal constituent of urine Urine analysis Experiments Physical Chemical Micro/Macro 1-Detection of some abnormal
Detection and Estimation of Some Abnormal Constituents Amal Alamri Lecture Over view Abnormal constituent of urine Urine analysis Experiments Physical Chemical Micro/Macro 1-Detection of some abnormal
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, Controversies in Urinary Tract Infections
 Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Scott Williams, MD Pediatric Nephrology OLOL Children s Hospital September 29, 2013 Controversies in Urinary Tract Infections Disclaimer I have no affiliations with any pharmaceutical or equipment company
Dr.Nahid Osman Ahmed 1
 1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
1 ILOS By the end of the lecture you should be able to Identify : Functions of the kidney and nephrons Signs and symptoms of AKI Risk factors to AKI Treatment alternatives 2 Acute kidney injury (AKI),
HAEMATURIA and it s management. Dr Sanjeev Bandi MBBS.,FRCSI, FRACS(Urology) Consultant Urologist Mackay Urology
 Consultant Urologist Mackay Urology") HAEMATURIA and it s management Dr Sanjeev Bandi MBBS.,FRCSI, FRACS(Urology) Consultant Urologist Mackay Urology Definition: Haematuria is the presence of red blood cells in the urine. The presence of 10
HAEMATURIA and it s management Dr Sanjeev Bandi MBBS.,FRCSI, FRACS(Urology) Consultant Urologist Mackay Urology Definition: Haematuria is the presence of red blood cells in the urine. The presence of 10
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
NATIONAL KIDNEY MONTH
 NATIONAL KIDNEY MONTH According to the WebMD website, kidneys have several specific roles: Maintain your body s balance of water and concentration of minerals, such as sodium, potassium, magnesium and
NATIONAL KIDNEY MONTH According to the WebMD website, kidneys have several specific roles: Maintain your body s balance of water and concentration of minerals, such as sodium, potassium, magnesium and
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017
 ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
ASYMPTOMATIC MICROSCOPIC HEMATURIA IN WOMEN JOLYN HILL, MD ASSISTANT PROFESSOR, CLINICAL UROGYNECOLOGY FEBRUARY14, 2017 DISCLOSURES No financial disclosures Urogynecologist via Ob/Gyn pathway ASYMPTOMATIC
Management of Nephrotic Syndrome
 Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Management of Nephrotic Syndrome 1. Introduction Incidence 2-4/100,000. Boys > girls 3:2; age of onset 2-6 years 80% of cases in children is due to minimal change (MCD) of which 80% will respond to steroid
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
URINANLYSIS. Pre-Lab Guide
 URINANLYSIS Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions on
URINANLYSIS Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions on
VCRC-OMERACT ANCA-Vasculitis Outcome Measure Initiative Comparative Outcome Measure Exercise-Training Cases
 Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase
 By Dr. Lindokuhle Mahlase") UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
UTIs in children ( with controversies ) By Dr. Lindokuhle Mahlase Epidemiology By age 7 years, 8 % of girls and 2 % of boys will have had a UTI. Most infections occur in the first 2 years of life ; boys
High Impact Rheumatology
 High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
High Impact Rheumatology Systemic Lupus Erythematosus Bernard Rubin, DO MPH Case 1: History A 45-year-old woman presents with severe dyspnea and cough. She was in excellent health until 4 weeks ago when
Kidney Biopsy. Table of Contents. Test Overview. Why It Is Done. Test Overview. Why It Is Done. How to Prepare. How It Is Done.
 Kidney Biopsy Table of Contents Test Overview Why It Is Done How to Prepare How It Is Done Results What Affects the Test? Test Overview The two kidneys {IMAGE LINK 1} are found on either side of the spine,
Kidney Biopsy Table of Contents Test Overview Why It Is Done How to Prepare How It Is Done Results What Affects the Test? Test Overview The two kidneys {IMAGE LINK 1} are found on either side of the spine,
Nephrotic Syndrome. Department of pediatrics The first affiliated hospital Sun Yat Sen University. Yue Zhihui ( 岳智慧 )
") Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Nephrotic Syndrome Department of pediatrics The first affiliated hospital Sun Yat Sen University Yue Zhihui ( 岳智慧 ) yuezhihui810@yahoo.com.cn Contents Definition Pathophysiology Clinical manifestation
Chronic Kidney Disease of Uncertain Aetiology - Clinical Features. Dr. Tilak Abeysekera Consultant Nephrologist
 Chronic Kidney Disease of Uncertain Aetiology - Clinical Features Dr. Tilak Abeysekera Consultant Nephrologist Geographical Distribution Dry Zone Factors Considered for the Diagnosis of CKDu >5 years stay
Chronic Kidney Disease of Uncertain Aetiology - Clinical Features Dr. Tilak Abeysekera Consultant Nephrologist Geographical Distribution Dry Zone Factors Considered for the Diagnosis of CKDu >5 years stay
The McMaster at night Pediatric Curriculum
 The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
The McMaster at night Pediatric Curriculum Robinson, J, et al. and the Canadian Pediatric Society. Urinary tract infection in infants and children: Diagnosis and management. Pediatr Child Health 2014;
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome
 P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
P a g e 1 DEFINITION Paediatrics Dr. Bakr Lecture 3 Nephrotic Syndrome Definition: nephrotic syndrome is a disorder characterized by heavy proteinuria with hypoprpteinimia,hyper lipidemia and edema. It
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200