3/28/ Diabetes Clinical Practice Recommendations and Treatment Algorithms: What s New! Epidemiology of Diabetes. Outline
|
|
|
- Chrystal Lawrence
- 6 years ago
- Views:
Transcription


1 2013 Diabetes Clinical Practice Recommendations and Treatment Algorithms: What s New! The speaker has no conflict in relation to this program. David W. Bartels, PharmD, CDE Vice Dean and Clinical Professor University of Illinois at Chicago College of Pharmacy at Rockford Outline ADA 2013 Clinical Practice Recommendations ADA-EASD Position Statement on Type 2 Diabetes Management AACE/ACE Treatment Algorithm New Diabetes Treatments - Long-acting GLP-1 Agonists - Ultra Long-acting Insulin - SGLT2 Inhibitors No conflicts of interest to report Epidemiology of Diabetes Diabetes affects 25.8 million people of all ages 8.3% of the U.S. population Diagnosed: 18.8 million Undiagnosed: 7.0 million Leading cause of kidney failure, nontraumatic lower-limb amputation, new cases of blindness among adults Major cause of heart disease and stroke Seventh leading cause of death National Diabetes Information Clearinghouse. National Diabetes Statistics, Available at: r (millions) Number Number of Americans with Diagnosed Diabetes, Year STANDARDS OF MEDICAL CARE IN DIABETES
2 ADA Evidence Grading System for Clinical Recommendations Level of Evidence A B C E Description Clear or supportive evidence from adequately powered well-conducted, generalizable, randomized controlled trials Compelling nonexperimental evidence Supportive evidence from well-conducted cohort studies or case-control study Supportive evidence from poorly controlled or uncontrolled studies Conflicting evidence with the weight of evidence supporting the recommendation Expert consensus or clinical experience ADA. Diabetes Care 2013;36(suppl 1):S12; Table 1. Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific types of diabetes Genetic defects in β-cell function, insulin action Diseases of the exocrine pancreas Drug- or chemical-induced Gestational diabetes mellitus (GDM) ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S11. Criteria for the Diagnosis of Diabetes A1C 6.5% OR Fasting plasma glucose (FPG) 126 mg/dl OR 2-h plasma glucose 200 mg/dl during an OGTT OR A random plasma glucose 200 mg/dl ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 2. Prediabetes: IFG, IGT, Increased A1C Categories of increased risk for diabetes (prediabetes) * FPG mg/dl: IFG OR 2-h plasma glucose in the 75-g OGTT mg/dl: IGT OR A1C % *For all three tests, risk is continuous, extending below the lower limit of a range and becoming disproportionately greater at higher ends of the range. ADA. I. Classification and Diagnosis. Diabetes Care 2013;36(suppl 1):S13; Table 3. Criteria for Testing for Diabetes in Asymptomatic Adult Individuals Testing should be considered in all adults who are overweight (BMI 25 kg/m 2 *) and have additional risk factors: Physical inactivity First-degree relative with diabetes High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander) Women who delivered a baby weighing >9 lb or were diagnosed with GDM Hypertension ( 140/90 mmhg or on therapy for hypertension) HDL cholesterol level <35 mg/dl and/or a triglyceride level >250 mg/dl Women with polycystic ovary syndrome (PCOS) A1C 5.7%, IGT, or IFG on previous testing Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans) History of CVD *At-risk BMI may be lower in some ethnic groups. ADA. Testing for Diabetes in Asymptomatic Patients. Diabetes Care 2013;36(suppl 1):S14; Table 4. Prevention/Delay of Type 2 Diabetes Refer patients with IGT (A), IFG (E), or A1C % (E) to ongoing support program Targeting weight loss of 7% of body weight At least 150 min/week moderate physical activity Follow-up counseling important for success (B) Based on cost-effectiveness of diabetes prevention, third-party payers should cover such programs (E) ADA. IV. Prevention/Delay of Type 2 Diabetes. Diabetes Care 2013;36(suppl 1):S16. 2
3 Prevention/Delay of Type 2 Diabetes Consider metformin for prevention of type 2 diabetes if IGT (A), IFG (E), or A1C % (E) Especially for those with BMI >35 kg/m 2, age <60 years, and women with prior GDM (A) In those with prediabetes, monitor for development of diabetes annually (E) Screen for and treat modifiable risk factors for CVD (B) ADA. IV. Prevention/Delay of Type 2 Diabetes. Diabetes Care 2013;36(suppl 1):S16. Diabetes Care: Management People with diabetes should receive medical care from a team that may include Physicians, nurse practitioners, physician s assistants, nurses, dietitians, pharmacists, mental health professionals In this collaborative and integrated t team approach, essential that individuals with diabetes assume an active role in their care Management plan should recognize diabetes self-management education (DSME) and ongoing diabetes support ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S17. Diabetes Care: Glycemic Control Two primary techniques available for health providers and patients to assess effectiveness of management plan on glycemic control Patient self-monitoring of blood glucose (SMBG), or interstitial glucose A1C Glucose Monitoring Patients on multiple-dose insulin (MDI) or insulin pump therapy should do SMBG (B) At least prior to meals and snacks Occasionally postprandially At bedtime Prior to exercise When they suspect low blood glucose After treating low blood glucose until they are normoglycemic Prior to critical tasks such as driving ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S17. ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S17. Glucose Monitoring When prescribed as part of a broader educational context, SMBG results may be helpful to guide treatment decisions and/or patient selfmanagement for patients using less frequent insulin injections or noninsulin therapies (E) When prescribing SMBG, ensure that patients receive ongoing instruction and regular evaluation of SMBG technique and SMBG results, as well as their ability to use SMBG data to adjust therapy (E) ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S16. A1C Perform A1C test at least twice yearly in patients meeting treatment goals (and have stable glycemic control) (E) Perform A1C test quarterly in patients whose therapy has changed or who are not meeting glycemic goals (E) Use of point-of-care (POC) testing for A1C provides the opportunity for more timely treatment changes (E) ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S18. 3
4 Correlation of A1C with Average Glucose (AG) Mean plasma glucose A1C (%) mg/dl mmol/l These estimates are based on ADAG data of ~2,700 glucose measurements over 3 months per A1C measurement in 507 adults with type 1, type 2, and no diabetes. The correlation between A1C and average glucose was A calculator for converting A1C results into estimated average glucose (eag), in either mg/dl or mmol/l, is available at ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19; Table 8. Glycemic Goals in Adults Lowering A1C to below or around 7% has been shown to reduce microvascular complications and, if implemented soon after the diagnosis of diabetes, is associated with long-term reduction in macrovascular disease (B) Therefore, a reasonable A1C goal for many nonpregnant adults is <7% (B) ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19. Glycemic Goals in Adults Providers might reasonably suggest more stringent A1C goals (such as <6.5%) for selected individual patients, if this can be achieved without significant hypoglycemia or other adverse effects of treatment (C) Appropriate patients might include those with short duration of diabetes, long life expectancy, and no significant CVD (C) Glycemic Goals in Adults Less stringent A1C goals (such as <8%) may be appropriate for patients with (B) History of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, extensive comorbid conditions Those with longstanding diabetes in whom the general goal is difficult to attain despite diabetes selfmanagement education, appropriate glucose monitoring, and effective doses of multiple glucose lowering agents including insulin ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19. ADA. V. Diabetes Care. Diabetes Care 2013;36(suppl 1):S19. Glycemic, Blood Pressure, Lipid Control in Adults A1C <7.0% * Blood pressure <140/80 mmhg Lipids: LDL cholesterol <100 mg/dl Statin therapy for those with history of MI or age >40+ or other risk factors *More or less stringent glycemic goals may be appropriate for individual patients. Goals should be individualized based on: duration of diabetes, age/life expectancy, comorbid conditions, known CVD or advanced microvascular complications, hypoglycemia unawareness, and individual patient considerations. Based on patient characteristics and response to therapy, higher or lower systolic blood pressure targets may be appropriate. In individuals with overt CVD, a lower LDL cholesterol goal of <70 mg/dl, using a high dose of statin, is an option. ADA. VI. Prevention, Management of Complications. Diabetes Care 2013;36(suppl 1):S33; Table 10. Diabetes Care in the Hospital Goals for blood glucose levels Critically ill patients: Initiate insulin therapy for treatment of persistent hyperglycemia starting at a threshold of no greater than mg/dl. (A) More stringent goals, such as mg/dl may be appropriate for selected patients, if achievable without significant hypoglycemia (C) Critically ill patients require an IV insulin protocol with demonstrated efficacy, safety in achieving desired glucose range without increasing risk for severe hypoglycemia (E) ADA. IX. Diabetes Care in Specific Settings. Diabetes Care. 2013;36(suppl 1):S45. 4
5 Diabetes Care in the Hospital Goals for blood glucose levels Noncritically ill patients: No clear evidence for specific blood glucose goals If treated with insulin, premeal blood glucose targets (if safely achieved) Generally <140 mg/dl with random blood glucose <180 mg/dl Diabetes Care in the Hospital Scheduled subcutaneous insulin with basal, nutritional, and correction components is the preferred method for achieving and maintaining glucose control in non-critically ill patients (C) More stringent targets may be appropriate in stable patients with previous tight glycemic control Less stringent targets may be appropriate in those with severe comorbidities (E) ADA. IX. Diabetes Care in Specific Settings. Diabetes Care. 2013;36(suppl 1):S46. ADA. IX. Diabetes Care in Specific Settings. Diabetes Care. 2013;36(suppl 1):S46. Diabetes Care in the Hospital Initiate glucose monitoring in any patient not known to be diabetic who receives therapy associated with high-risk for hyperglycemia High-dose glucocorticoid therapy, initiation of enteral or parenteral nutrition, or other medications such as octreotide tid or immunosuppressive i medications (B) If hyperglycemia is documented and persistent, consider treating such patients to the same glycemic goals as patients with known diabetes (E) Diabetes Care in the Hospital A hypoglycemia management protocol should be adopted and implemented by each hospital or hospital system (E) Obtain A1C for all patients (E) If results within previous 2 3 months unavailable With diabetes risk factors who exhibit hyperglycemia Patients with hyperglycemia without a diagnosis of diabetes: document plans for follow-up testing and care at discharge (E) ADA. IX. Diabetes Care in Specific Settings. Diabetes Care. 2013;36(suppl 1):S46. ADA. IX. Diabetes Care in Specific Settings. Diabetes Care. 2013;36(suppl 1):S46. Impact of Intensive Therapy for Diabetes: Summary of Major Clinical Trials Study Microvasc CVD Mortality UKPDS DCCT / EDIC* ACCORD ADVANCE VADT Kendall DM, Bergenstal RM. International Diabetes Center 2009 UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998;352:854. Holman RR et al. N Engl J Med. 2008;359:1577. DCCT Research Group. N Engl J Med 1993;329;977. Nathan DM et al. N Engl J Med. 2005;353:2643. Gerstein HC et al. N Engl J Med. 2008;358:2545. Patel A et al. N Engl J Med 2008;358:2560. * in T1DM Initial Trial Long Term Follow up Diabetes Care, Diabetologia. 19 April 2012 Ismail-Beigi F, et al. Ann Intern Med 2011;154:554 5
6 ADA-EASD Position Statement: Management of Hyperglycemia in T2DM Anti-hyperglycemic Therapy Therapeutic options: Oral agents & non-insulin injectables - Metformin Meglitinides - Sulfonylureas - α-glucosidase inhibitors - Thiazolidinediones - Bile acid sequestrants - DPP-4 inhibitors - Dopamine-2 agonists - GLP-1 receptor agonists - Amylin mimetics ADA-EASD Position Statement: Management of Hyperglycemia in T2DM Anti-hyperglycemic Therapy Therapeutic options: Insulin - Neutral protamine Hagedorn (NPH) - Regular - Basal analogs (glargine, detemir) - Rapid analogs (lispro, aspart, glulisine) - Pre-mixed varieties Diabetes Care, Diabetologia. 19 April 2012 Diabetes Care, Diabetologia. 19 April 2012 Case: 55 yo obese man diagnosed with T2DM 10 years ago. A1C of 8.7% and fasting glucose levels of mg/dl on metformin 1000mg BID and pioglitazone 45mg daily. What is your next step in managing this patients diabetes? 1. Add GLP-1 receptor agonist 2. Add basal insulin 3. Add a DPP-4 inhibitor 4. Add a sulfonylurea Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) Case: 55 yo obese man diagnosed with T2DM 10 years ago. A1C of 8.7% and fasting glucose levels of mg/dl on metformin 1000mg BID and pioglitazone 45mg daily. Question: What is your next step in managing this patients diabetes? -Add a GLP-1 receptor agonist -Add basal insulin -Add a DPP-4 inhibitor -Add a sulfonylurea IMs (n=126) NPs (n=125) CDEs (n=121) Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) IMs (n=126) NPs (n=125) CDEs (n=121) Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) IMs (n=126) NPs (n=125) CDEs (n=121) Case: 55 yo obese man diagnosed with T2DM 10 years ago. A1C of 8.7% and fasting glucose levels of mg/dl on metformin 1000mg BID and pioglitazone 45mg daily. Question: What is your next step in managing this patients diabetes? -Add a GLP-1 receptor agonist -Add basal insulin -Add a DPP-4 inhibitor -Add a sulfonylurea 29.3% 24.7% 25.3% 19.3% 27.2% 29.8% 26.5% 15.9% 24.0% 28.0% 22.4% 20.0% Case: 55 yo obese man diagnosed with T2DM 10 years ago. A1C of 8.7% and fasting glucose levels of mg/dl on metformin 1000mg BID and pioglitazone 45mg daily. Question: What is your next step in managing this patients diabetes? -Add a GLP-1 receptor agonist -Add basal insulin -Add a DPP-4 inhibitor -Add a sulfonylurea 29.3% 24.7% 25.3% 19.3% 27.2% 29.8% 26.5% 15.9% 24.0% 28.0% 22.4% 20.0% 42.1% 24.8% 18.2% 9.9% 6


7 Case: 49 yo woman diagnosed with T2DM 9 months ago is overweight and has an A1C of 8.0%. She is on metformin 500mg TID and needs her treatment intensified. What is your next step in managing this patients diabetes? 1. Add a GLP-1 receptor agonist 2. Add basal insulin 3. Add a DPP-4 inhibitor 4. Add a TZD 5. Add a sulfonylurea 6. Other Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) Case: 49 yo woman -Add a GLP-1 diagnosed with type 2 receptor diabetes 9 months ago agonist is overweight and has an A1C of 8.0%. She -Add basal is on metformin 500mg insulin TID and needs her treatment intensified. -Add a DPP-4 inhibitor Question: What is your next step in -Add a TZD managing this patients diabetes? -Add a sulfonylurea IMs (n=126) NPs (n=125) CDEs (n=121) -Other Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) IMs (n=126) NPs (n=125) CDEs (n=121) Current Practice Patterns of Health Care Providers in Managing Type 2 Diabetes Case and Question Options FPs (n=150) IMs (n=126) NPs (n=125) CDEs (n=121) Case: 49 yo woman -Add a GLP-1 diagnosed with type 2 receptor diabetes 9 months ago agonist is overweight and has an A1C of 8.0%. She -Add basal is on metformin 500mg TID and needs her treatment intensified. Question: What is your next step in managing this patients diabetes? insulin -Add a DPP-4 inhibitor -Add a TZD -Add a sulfonylurea -Other 9.3% 12.7% 20.7% 22.7% 24.7% 10.0% 8.6% 17.2% 35.1% 19.2% 16.6% 3.3% 8.8% 16.0% 22.4% 18.4% 26.4% 8.0% Case: 49 yo woman -Add a GLP-1 diagnosed with type 2 receptor diabetes 9 months ago agonist is overweight and has an A1C of 8.0%. She -Add basal is on metformin 500mg TID and needs her treatment intensified. Question: What is your next step in managing this patients diabetes? insulin -Add a DPP-4 inhibitor -Add a TZD -Add a sulfonylurea -Other 9.3% 12.7% 20.7% 22.7% 24.7% 10.0% 8.6% 17.2% 35.1% 19.2% 16.6% 3.3% 8.8% 16.0% 22.4% 18.4% 26.4% 8.0% 25.6% 18.2% 25.6% 10.7% 15.7% 4.1% T2DM Antihyperglycemic Therapy: General Recommendations T2DM Antihyperglycemic Therapy: General Recommendations Diabetes Care, Diabetologia. 19 April 2012 Diabetes Care, Diabetologia. 19 April

- 40 & -119 agonists Protein Tyrosine Phosphatase (PTB)- 1b inhibitors Camitine- Palmitoyltransferase (CPT)- 1 inhibitors Acetyl COA Carboxylase (ACC)- 1 &")


8 T2DM Antihyperglycemic Therapy: General Recommendations Diabetes Care, Diabetologia. 19 April 2012 Diabetes Care, Diabetologia. 19 April 2012 DPP-4 Inhibitors Can be Used in All Lines of Therapy: AACE/ACE Algorithm for Glycemic Control* New Classes of Diabetes Medications in Development Long-acting GLP-1 receptor agonists Ultra long-acting insulin Ultra rapid-acting insulin Ranolazine Dual & Pan PPAR agonists 11 Hydroxysteroid Dehydrogenase (HSD)- 1 inhibitors Fructose 1,6-bisphosphatase inhibitors Glucokinase activators G protein-coupled Receptor (GPR)- 40 & -119 agonists Protein Tyrosine Phosphatase (PTB)- 1b inhibitors Camitine- Palmitoyltransferase (CPT)- 1 inhibitors Acetyl COA Carboxylase (ACC)- 1 & -2 inhibitors Glucagon receptor antagonists Salicylate derivatives Immunomodulatory drugs Sodium- Glucose Co-transporter (SGLT) {-1} & -2 inhibitors GLP-1 Effects in Humans: Glucoregulatory Role of Incretins Promotes satiety and reduces appetite Alpha cells: Postprandial glucagon secretion Microsphere Technology Provides a Continuous Level of Exenatide Patented Medisorb microspheres* deliver a constant presence of exenatide with a once-weekly dose Microspheres are made of a biodegradable polymer which dissipates into CO 2 and water This material is also used in dissolvable sutures and other long-acting therapies Beta cells: Enhances glucose-dependent insulin secretion GLP-1 secreted upon the ingestion of food Liver: Glucagon reduces hepatic glucose output Stomach: Slows gastric emptying Nauck MA, et al. Diabetologia. 1986;29:46-52; Drucker DJ. Diabetes. 1998;47: ; Flint A, et al. J Clin Invest 1998;101: ; Larsson H, et al. Acta Physiol Scand. 1997;160: ; Nauck MA, et al. Diabetologia. 1996;39: UKBDR00084c Sept 2011 Subcutaneous injection of microsphere suspension of exenatide Individual microspheres aggregate and there is initial release of exenatide Microsphere degradation leads to continued release of exenatide * The BYDUREON microsphere is made of PLGA (polylactide co-glycolide). Medisorb is a registered trade mark of Alkermes, Inc. Further degradation and metabolism of microsphere polymer provide sustained levels of exenatide DeYoungMB, et al. Diabetes Technol Ther.2011;13:
 Plasma exen Steady state achieved for continuous glycemic control Second dose minimum efficacious concentration achieved")
:65-74;. Intent-to-treat population.")
:431-39; Drucker DJ, et al.lancet. 2008;372(9645):1240-50; Blevins T, et al. J Clin Endocrin Metab. 2011; 96(5):2010-81; Buse JB, et al.")


:1240-50; Blevins T, et al. J Clin Endocrin Metab. 2011;96(5):2010-81; Buse JB, et al.")

:S38; Diamant M, et al. Lancet.")
 polymer microsphere formulations Most individual nodules were asymptomatic, although some were")
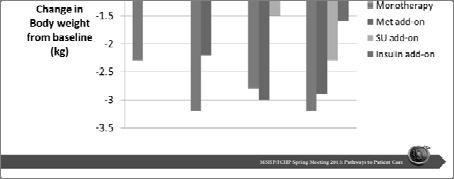
9 Microsphere Technology: Steady-state Exenatide Concentrations Ensuring Minimal Peak-to-Trough Fluctuations HbA 1c Reduction from Baseline by Exenatide Once-Weekly Ranged from 1.3% to 1.9% Establishing steady-state exenatide levels atide (pg/ml) Plasma exen Steady state achieved for continuous glycemic control Second dose minimum efficacious concentration achieved Steady state is maintained with subsequent weekly doses LS mean change in HbA 1c (%) Days Week DURATION-2 DURATION-1 DURATION-5 DURATION-6 DURATION-3. Fineman M, et al. Clin Pharmacokinet. 2011;50(1):65-74;. Intent-to-treat population. HbA 1c=glycosylated hemoglobin; LS=least squares; BID=twice-daily; 100 mg sitagliptin, 45 mg pioglitazone, mean dose of insulin glargine 31 units at 6 months. Bergenstal RM, et al. Lancet. 2010;376(9739):431-39; Drucker DJ, et al.lancet. 2008;372(9645): ; Blevins T, et al. J Clin Endocrin Metab. 2011; 96(5): ; Buse JB, et al. Diabetologia 2011;54(Suppl 1):S38; Diamant M, et al. Lancet. 2010;375(9733): Proportion of Subjects Achieving HbA 1c Target of 7% vs Comparators Exenatide Once-Weekly Changes in Body Weight vs Comparators Sitagliptin or pioglitazone Exenatide BID Liraglutide 1.8mg Insulin glargine on (%) Proportio n body weight (kg) LS mean change in DURATION-2 DURATION-1 DURATION-5 DURATION-6 DURATION-3 n=216 n=212 DURATION-1, 3: evaluable population. DURATION-5, -2, and : intent-to-treat population. DURATION-5, -6 and -3: target of <7%. BID: twice-daily 100 mg sitagliptin, 45 mg pioglitazone, mean dose of insulin glargine 31 units at 6 months. Bergenstal RM, et al. Lancet. 2010;376(9739):431-39; Drucker DJ, et al. Lancet. 2008;372(9645): ; Blevins T, et al. J Clin Endocrin Metab. 2011;96(5): ; Buse JB, et al. Diabetologia 2011;54(Suppl 1):S38; Diamant M, et al. Lancet. 2010;375(9733): Data on file, Eli Lilly and Company / Amylin Pharmaceuticals, Inc; DURATION-2 DURATION-1 DURATION-5 DURATION-6 DURATION-3 Rapid weight loss at a rate of >1.5 kg per week has been reported in patients treated with exenatide. Weight loss of this rate may have harmful consequences. Baseline weight values for individual groups are not currently published Bergenstal RM, et al. Lancet. 2010;376(9739):431-39; Drucker DJ, et al. Lancet. 2008;372(9645): ; Blevins T, et al. J Clin Endocrin Metab. 2011;96(5): ; Buse JB, et al. Diabetologia 2011;54(Suppl 1):S38; Diamant M, et al. Lancet. 2010;375(9733): ; Subcutaneous Injection Site Nodules: Known Response to Microsphere Technology These appear as small bumps and have been observed very frequently in clinical trials These are consistent with the known properties of poly (D,L -lactide co-glycolide) polymer microsphere formulations Most individual nodules were asymptomatic, although some were associated with redness and itching, and resolved over 4 to 8 weeks Mostly small, average size is 0.5 cm to 0.75 cm in diameter; smaller than the average pea May not be detected visually May not appear right away More than 1 bump may be present at any given time In clinical trials, withdrawal due to injection site reactions occurred in <1% in exenatide once-weekly-treatment groups Data on file, Eli Lilly and Company / Amylin Pharmaceuticals, Inc. How Do the Pharmacodynamics of Basal Insulin Preparations Affect Outcomes 9

: 1614-1620 *P<0.05 Riddle et al.")
.")





10 Biologic Activity Over 24-hours More Consistent for Basal Insulin Analogs Less Hypoglycemia with Basal Analogs vs. NPH Insulin detemir * * * * GIR = Glucose Infusion Rate Heise et al. Diabetes 2004; 53 (6): *P<0.05 Riddle et al. Diabetes Care 2003; 26: Philis-Tsimikas et al. Clin Ther 2006; 28 (10). Improving on Current Basal Insulin Analogs Molecular Size Determines Rate of Subcutaneous Absorption Extend duration of action Flat pharmacodynamic profile Reduced day-to-day variability Molecular size Insulin association state Absorption rate Subcutaneous tissue 6 kda 36 kda 72 kda >5000 kda Zn 2+ Zn 2+ Zn 2+ High molecular weight forms Capillary membrane Rapid absorption Slow absorption Brange et al. Diabetes Care 1990;13: Insulin Degludec from Solution to Subcutaneous Depot Insulin Degludec: Slow Release Following Injection Phenol Zn 2+ Insulin degludec injected As phenol from the vehicle diffuses degludec d hexamers link up via single side-chain contacts Subcutaneous depot Zn 2+ Insulin degludec multi-hexamers Long multi-hexamers assemble Zinc diffuses slowly causing individual hexamers to disassemble, releasing monomers Monomers are absorbed from the depot into the circulation 10
 CV (%) Degludec (n=773) Glargine (n=257) Terminal half-life lif (steady state) Degludec 24.5 23 Glargine 12.2 56 0.")
")




11 Terminal Half-life & Coefficient of Variation at Steady State No Difference in HbA 1c Decrease over Time Between Degludec & Glargine Harmonic mean (h) CV (%) Degludec (n=773) Glargine (n=257) Terminal half-life lif (steady state) Degludec Glargine Time (weeks) Mean±SEM; FAS; LOCF Comparisons: Estimates adjusted for multiple covariates Data on file: NN ; Accepted for presentation at ADA 2012 Lower Nocturnal Confirmed Hypoglycemia with Insulin Degludec The Kidneys Play an Important Role in Glucose Control Degludec (n=773) Glargine (n=257) 36% p<0.05 Normal Renal Glucose Physiology 180 g of glucose is filtered each day Virtually all glucose reabsorbed in the proximal tubules & reenters the circulation SGLT2 reabsorbs about 90% of the glucose SGLT1 reabsorbs about 10% of the glucose Time (weeks) Comparisons: Estimates adjusted for multiple covariates Data on file: NN ; Accepted for presentation at ADA 2012 Virtually no glucose excreted in urine Mather, A & Pollock, C. Kidney International. 2011;79:S1-S6. Targeting the Kidney Rationale for SGLT2 Inhibitors SGLT2 is a low-affinity, high capacity glucose transporter located in the proximal tubule and is responsible for 90% of glucose reabsorption Selective SGLT2 inhibitors have a novel & unique mechanism of action reducing blood glucose levels by increasing renal excretion of glucose Decreased glycemia will decrease glucose toxicity leading to further improvements in glucose control Selective SGLT2 inhibition, would also cause urine loss of the calories from glucose, potentially leading to weight loss Chao EC, et al. Nat Rev Drug Discovery. 2010;9: Brooks AM, Thacker SM. Ann Pharmacother. 2009;42(7):



:2223-2233.")


 Low risk of hypoglycemia Blood pressure")


12 SGLT2 Inhibitors in Phase 3 Development Empagliflozin Changes from Baseline in A1C in Phase 3 Dapagliflozin Studies Placebo Dapa 2.5mg Dapa 5mg Dapa 10mg Canagliflozin Dapagliflozin Ipragliflozin Wilding JPH, et al. Abstract 78-OR. ADA 2010; Strojek K, et al. Abstract 870. EASD 2010; Ferrannini E, et al. Diabetes Care. 2010;33(10): ; Bailey CJ, et al. Lancet. 2010;375(9733): Changes from Baseline in Fasting Glucose in Phase 3 Dapagliflozin Studies Changes from Baseline in Body Weight in Phase 3 Dapagliflozin Studies 5 Placebo Dapa 2.5mg Dapa 5mg Dapa 10mg 0 5 mg/dl Wilding JPH, et al. Abstract 78-OR. ADA 2010; Strojek K, et al. Abstract 870. EASD 2010; Ferrannini E, et al. Diabetes Care. 2010;33(10): ; Bailey CJ, et al. Lancet. 2010;375(9733): Wilding JPH, et al. Abstract 78-OR. ADA 2010; Strojek K, et al. Abstract 870. EASD 2010; Ferrannini E, et al. Diabetes Care. 2010;33(10): ; Bailey CJ, et al. Lancet. 2010;375(9733): Perspectives on SGLT2 Inhibition Potential advantages Insulin Independence Weight loss (75g urine glucose = 300kcal/day) Low risk of hypoglycemia Blood pressure lowering? Concerns Polyuria Electrolyte disturbances Bacterial urinary tract infections Fungal genital infections Malignancies 12
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES
 Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Janice Lazear, DNP, FNP-C, CDE DIAGNOSIS AND CLASSIFICATION OF DIABETES Objectives u At conclusion of the lecture the participant will be able to: 1. Differentiate between the classifications of diabetes
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS
 Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Management of Hyperglycemia in Type 2 Diabetes Celeste C. Thomas MD, MS Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure
Diabetes 2013: Achieving Goals Through Comprehensive Treatment. Session 2: Individualizing Therapy
 Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Diabetes 2013: Achieving Goals Through Comprehensive Treatment Session 2: Individualizing Therapy Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
9/12/2014. Main Pathophysiological Defect in T1DM. Main Pathophysiological Defects in T2DM. Personalizing Diabetes Care: The Alphabet Soup of Options
 9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
9/12/2014 Baptist Health South Florida 13th Annual Primary Focus Symposium June 28, 2014 Silvio Inzucchi MD Section of Endocrinology Yale University School of Medicine Half-Century of HTN & T2DM Medications
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale
 Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Diabetes Review Chris Paras, D.O. Assistant Prof of Medicine, NYIT & Touro COM Designated Institutional Official & Assoc. Clinical Dean, Brookdale University Hospital Diabetes Care 2018 Jan; 41 Objectives
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
STANDARDS OF MEDICAL CARE IN DIABETES 2014
 STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
STANDARDS OF MEDICAL CARE IN DIABETES 2014 I. CLASSIFICATION AND DIAGNOSIS Classification of Diabetes Type 1 diabetes β-cell destruction Type 2 diabetes Progressive insulin secretory defect Other specific
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Changing Diabetes: The time is now!
 Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
Midwest Cardiovascular Research Foundation Welcomes DANITA HARRISON, ARNP Ms. Harrison discloses speaking relationships with Lilly, Novo Nordisk and Pfizer. Changing Diabetes: The time is now! Danita Harrison
The National Diabetes Prevention Program in Washington State March 2012
 The National Diabetes Prevention Program in Washington State March 2012 Session Objectives 1. Overview of pre-diabetes. 2. Describe the Diabetes Prevention Program (DPP). 3. Eligibility for the DPP. 4.
The National Diabetes Prevention Program in Washington State March 2012 Session Objectives 1. Overview of pre-diabetes. 2. Describe the Diabetes Prevention Program (DPP). 3. Eligibility for the DPP. 4.
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead
 Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
Dr Aftab Ahmad Consultant Diabetologist at Royal Liverpool University Hospital Regional Diabetes Network Lead Today s Presentation HbA1c & diagnosing Diabetes What is Impaired Glucose & IGR? Implications
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone
 Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Index Abbreviations DPP-IV dipeptidyl peptidase IV DREAM Diabetes REduction Assessment with ramipril and rosiglitazone Medication GAD glutamic acid decarboxylase GLP-1 glucagon-like peptide 1 NPH neutral
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Addressing Addressing Challenges in Type 2 Challenges in Type 2 Diabetes Diabetes Speaker:
 Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Addressing Challenges in Type 2 Diabetes Geneva Briggs, PharmD,, BCPS Addressing Challenges in Type 2 Diabetes Speaker: Dr. Geneva Clark Briggs, a board-certified Pharmacotherapy Specialist, received her
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Diabetes Update: Diabetes Management In Primary Care. Jonathon M. Firnhaber, MD, FAAFP
 Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes Update: Diabetes Management In Primary Care Jonathon M. Firnhaber, MD, FAAFP Learning objectives 1. Critically evaluate the evidence emerging within diabetes research as it applies to recommendations
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017
 TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
TREATMENT OF DIABETES AFTER METFORMIN GREGG GERETY, MD ALBANY MEDICAL COLLEGE, DIVISION OF COMMUNITY ENDOCRINOLOGY JULY 14, 2017 Outline Review treatment algorithms from ADA/ EASD & ACE/AACE. Review positive
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Initiation and Titration of Insulin in Diabetes Mellitus Type 2
 Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
Initiation and Titration of Insulin in Diabetes Mellitus Type 2 Greg Doelle MD, MS April 6, 2016 Disclosure I have no actual or potential conflicts of interest in relation to the content of this lecture.
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Standards of Medical Care in Diabetes 2016
 Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
Standards of Medical Care in Diabetes 2016 Care Delivery Systems 33-49% of patients still do not meet targets for A1C, blood pressure, or lipids. 14% meet targets for all A1C, BP, lipids, and nonsmoking
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care
 Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
Diabetes Day for Primary Care Clinicians Advances in Diabetes Care Elliot Sternthal, MD, FACP, FACE Chair New England AACE Diabetes Day Planning Committee Welcome and Introduction This presentation will:
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Standards of Care in Diabetes What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE
 Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Standards of Care in Diabetes 2016-- What's New? Veronica Brady, FNP-BC, PhD, BC-ADM,CDE Karmella Thomas, RD, LD,CDE Terminology No longer using the term diabetic. Diabetes does not define people. People
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011
 New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
New basal insulins Are they any better? Matthew C. Riddle, MD Professor of Medicine Oregon Health & Science University Keystone Colorado 15 July 2011 Presenter Disclosure I have received the following
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach
 Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
Management of Hyperglycemia in Type 2 Diabetes, 2015: A Patient-Centered Approach Update to a Position Statement of the American Diabetes Association (ADA) and the European Association f the Study of Diabetes
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
CE on SUNDAY Newark, NJ October 18, 2009
 CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 2:45 PM 3:45 PM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Addressing Challenges in Type 2 Diabetes ACPE #
CE on SUNDAY Newark, NJ October 18, 2009 Date: Sunday, October 18, 2009 Time: 2:45 PM 3:45 PM Location: Sheraton Newark Airport Hotel Title: Speaker(s): Addressing Challenges in Type 2 Diabetes ACPE #
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Clinical Practice Guidelines
 Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Clinical Practice Guidelines Diabetes Objective The purpose is to guide the appropriate diagnosis and management of Diabetes. This guideline is designed to assist the clinician by providing a framework
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
OBJECTIVES 4/7/2014. Diabetes Update Overview of the Diabetes Epidemic in the United States. ISHP Annual Spring Meeting
 Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
Diabetes Update 2014 ISHP Annual Spring Meeting Hayley Miller MD April 13, 2014 OBJECTIVES Review diabetes guidelines. Understand diabetes management targets. Discuss current therapeutic strategies. Overview
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
Helpful Hints for Taking Care of Your Diabetes. Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center
 Helpful Hints for Taking Care of Your Diabetes Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center Objectives How big of a problem is diabetes? What is diabetes? How is
Helpful Hints for Taking Care of Your Diabetes Farahnaz Joarder, MD and Don Kain, MA, RD,CDE Harold Schnitzer Diabetes Health Center Objectives How big of a problem is diabetes? What is diabetes? How is
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Noninsulin Treatment of Diabetes: What the PCP Needs to Know
 Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Non Insulin Treatment of Type 2 Diabetes: What the PCP Needs to Know Martin J. Abrahamson, MD Senior Vice President for Medical Affairs Joslin Diabetes Center Associate Professor of Medicine Harvard Medical
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Diabetes Meds Update Disclaimer and Important Info. Objectives. Page 1. Copyright , Diabetes Education Services
 Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Diabetes Meds Update 2016 Beverly Dyck Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Disclaimer and Important Info This content is for educational purposes only. Please see Package
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
American Diabetes Association 2018 Guidelines Important Notable Points
 American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
American Diabetes Association 2018 Guidelines Important Notable Points The Standards of Medical Care in Diabetes-2018 by ADA include the most current evidencebased recommendations for diagnosing and treating
Diabetes Risk Assessment and Treatment
 Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
Diabetes Risk Assessment and Treatment Todd T. Brown, MD, PhD Professor of Medicine and Epidemiology Division of Endocrinology, Diabetes, & Metabolism Johns Hopkins University Baltimore, Maryland, USA
CANA DAPA EMPA. Change in Baseline Body Weight (kg) *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.
 *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.") CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
How to Use the ADA Type 2 Diabetes Treatment Algorithm. Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP
 How to Use the ADA Type 2 Diabetes Treatment Algorithm Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP 8 ACOFP 55th Annual Convention & Scientific Seminars ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please
How to Use the ADA Type 2 Diabetes Treatment Algorithm Eric L. Johnson, MD Jay Shubrook, Jr., DO, FACOFP 8 ACOFP 55th Annual Convention & Scientific Seminars ACOFP FULL DISCLOSURE FOR CME ACTIVITIES Please
Clinical Practice Guidelines for Diabetes Management
 Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
Clinical Practice Guidelines for Diabetes Management Diabetes is a disease in which blood glucose levels are above normal. Over the years, high blood glucose damages nerves and blood vessels, which can
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is