DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol. Glycemic Task Force September 2014
|
|
|
- Franklin Fowler
- 6 years ago
- Views:
Transcription
1 DKA : Diabetic Ketoacidosis & HHS: Hyperlgycemic Hyperosmolar Syndrome Protocol Glycemic Task Force September 2014
2 Hyperglycemic Crises: Pathophysiology DKA HHS Hyperglycemia DKA HHS Umpierrez, In Shoemaker, Textbook Critical Care 71, 797, 1999.
3 Precipitating factors for DKA Nonadherence, not taking insulin Infection MI Cocaine Pregnancy Pancreatitis Steroids
4 Diagnostic Criteria for DKA Mild Moderate Severe HHS Plasma glucose (mg/dl) ph Bicarbonate (meq/l) Urine ketones* Serum ketones* Effective serum Osmol (mosm/kg) Alteration in sensoria > positive positive variable alert or mental obtundation * Nitroprusside reaction method Calculation: 2[measured Na (meq/l)] + glucose (mg/dl)/18 > positive positive variable Alert & drowsy ADA, Kitabchi et al, Diabetes Care 24: , 2001 >250 <7.0 <10 positive positive variable Stupor- coma > 600 >7.30 > 15 small small >320
5 Clinical Presentation of DKA Symptoms Polydipsia Polyuria Weakness Weight loss Nausea Vomiting Abdominal pain Signs Hypothermia Tachycardia Tachypnea Kussmaul breathing Ileus Acetone breath Altered sensorium The onset of DKA is usually relative short, ranging from hours to a day or two. ADA, Kitabchi et al, Diabetes Care 24: , 2001
6 Diagnostic Criteria for HHS Plasma glucose >600 Arterial ph >7.30 Serum bicarbonate >18 Urine ketones: negative or small Serum ketones: negative or small Serum osmolality >320 Anion gap: variable Elevated serum creatnine and BUN Total body stores of sodium, potassium, and phosphorus are usually low
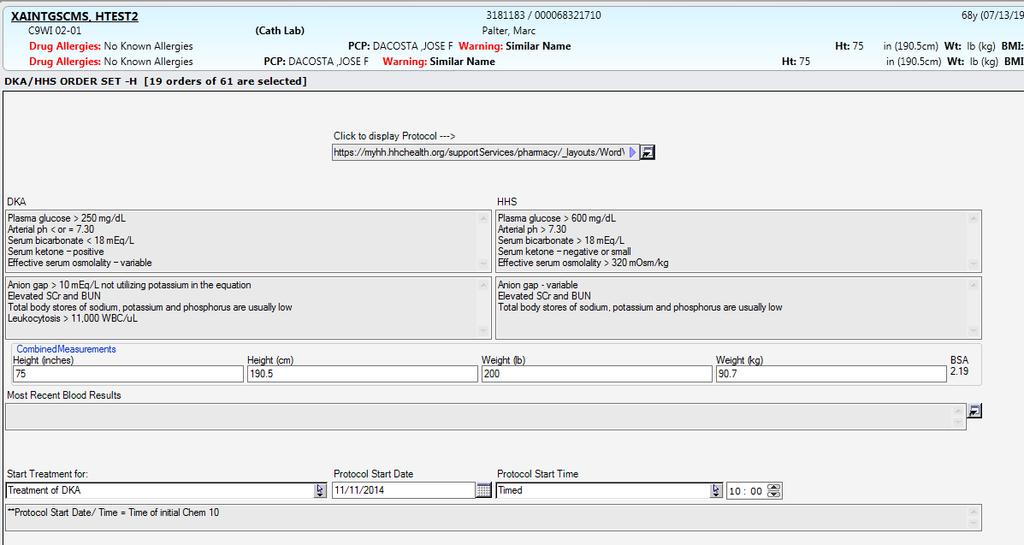
7 Initial Laboratory Studies for DKA and HHS Immediate determination of blood glucose and serum acetone ABG s OR venous ph CBC with differential Chem 10 Serum acetone Urinalysis Consider Bacterial cultures Cardiac enzymes Consider utox hcg if child bearing age
8 Serum Sodium Sodium may falsely appear to be low when blood sugar is elevated because there are more glucose molecules compared to sodium molecules and there is a movement of water into the extracellular compartment Serum glucose H 2 O H 2 O H 2 O H 2 O Na +
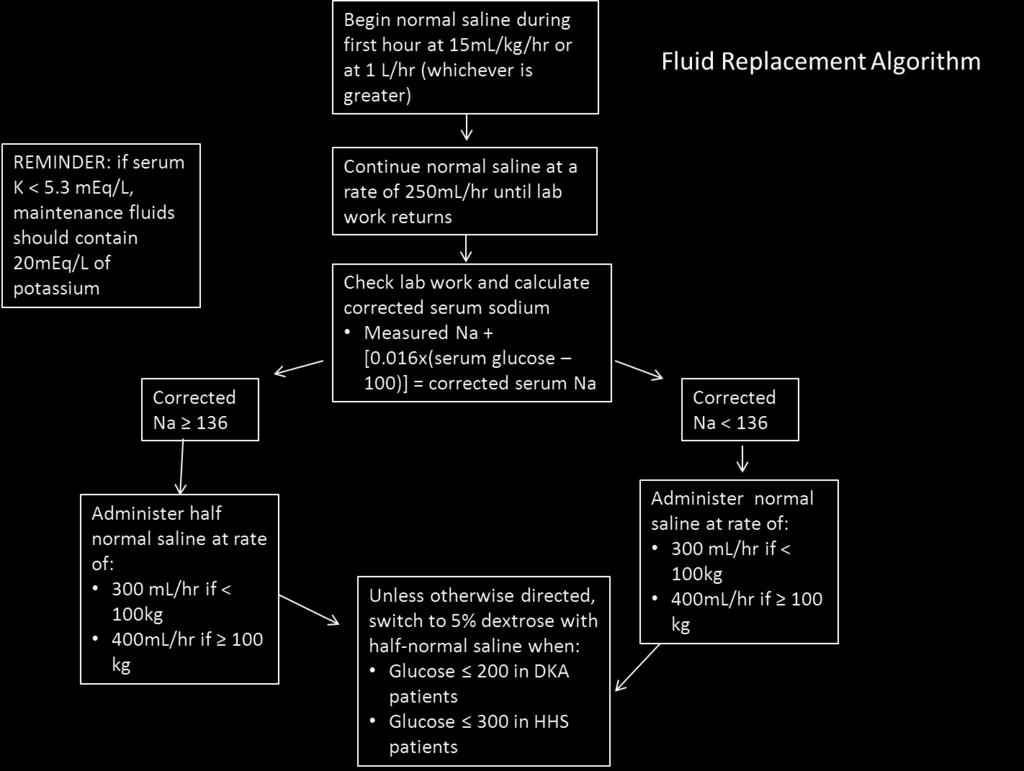
9 Serum Sodium in DKA patients If glucose greater than 250mg/dl, patient will have falsely low sodium This will help the provider determine what type of IV fluids the patient needs The provider needs to calculate a corrected sodium: Corrected sodium = measured sodium x (serum glucose 100)
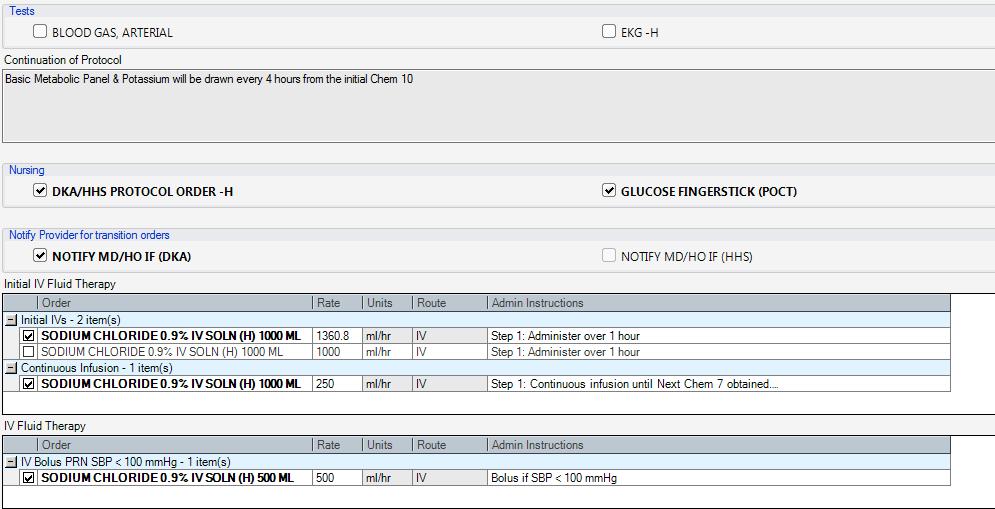
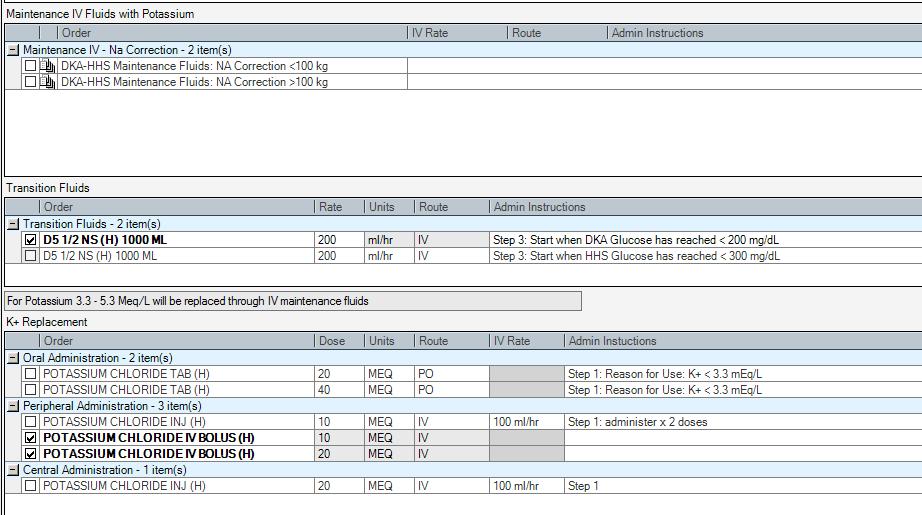
10 IV Fluids Start with NS to replace volume, unless there is a contraindication to aggressive fluid replacement. Once hemodynamically stable (typically after 1 liter), If corrected sodium is >136, change to ½ NS If corrected sodium is <136, continue NS Change to 5% dextrose with ½ NS once blood glucose is < 200 in DKA or < 300 in HHS
11 IVF:
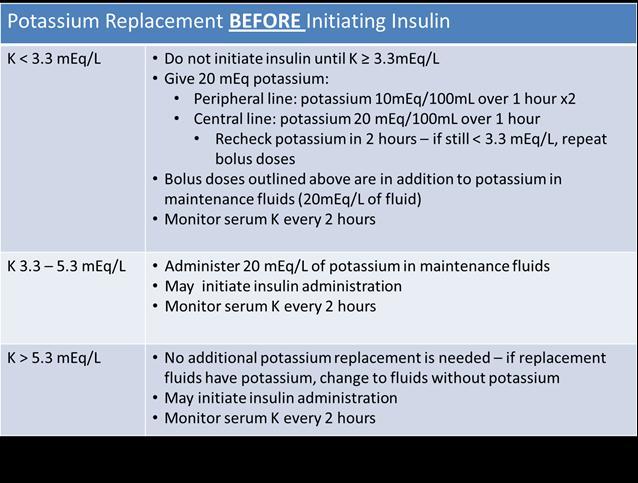
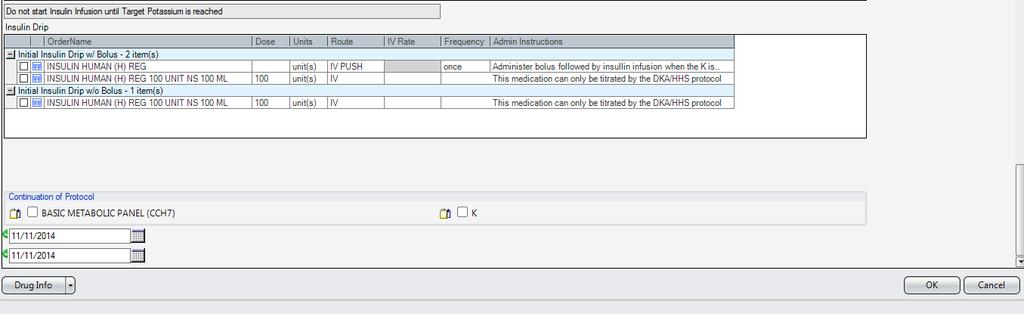
12 Serum Potassium Serum potassium will be falsely elevated. Lack of insulin causes potassium to shift out of the cell. Once patient is given insulin, potassium shifts back into the cell and levels will drop. Check potassium prior to starting insulin. Must be > 3.3 to start insulin drip If potassium <3.3, per protocol, give 20mEq of KCL IV before starting insulin drip If patient only has peripheral line, must infuse 10mEq x 2 If potassium , per protocol, place 20mEq/liter in IV fluid IF potassium >5.3, per protocol, no potassium in IV fluid
13 Potassium

14 Potassium During Insulin Infusion
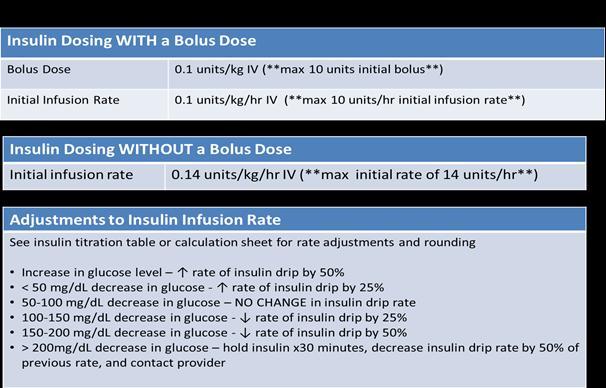
15 Insulin Initial rate of insulin infusion will be based on patient s weight in kg Initiation can be done with or without bolus as determined by provider s order Titration will be done based on how quickly patient blood sugar is rising or falling and nurse will be directed via protocol (similar to heparin dosing protocol) Insulin rates should be rounded to the nearest 0.5 units/hr Blood sugar should not fall more than mg/dL per hour If patient becomes hypoglycemic, follow Hypoglycemia Protocol
16 Insulin Dosing Initial Dosing with bolus: Bolus regular insulin at a dose of 0.1 unit/kg IV (maximum initial bolus of 10 units) and begin regular insulin drip at a starting rate of 0.1 unit/kg/hour IV maximum initial infusion rate of 10 units/hr Initial Dosing without bolus: Begin regular insulin drip at a starting rate of 0.14 unit/kg/hour IV maximum initial infusion rate of 14 units/hr
17 Insulin
18 ADA Position Statement. Diabetes Care 26:S109-S117, 2009 Intravenous Insulin Therapy in DKA I.V. Bolus: 0.1 U/kg body Wgt I.V. drip: 0.1 U/kg/h body Wgt Glucose < 250 mg/dl I.V. drip: U/kg/h Until resolution of ketoacidosis
19 DKA/HHS Insulin Infusion Titration Current Drip Rate (units/hr) Decrease by 50% to: (units/hr) Decrease by 25% to: (units/hr) No change (units/hr) Increase by 25% to: (units/hr) Increase by 50% to: (units/hr)

20 Monitoring Parameters
21 Bicarbonate
22 Bicarbonate Therapy in DKA Randomized controlled trial in 21 patients with ph between 6.9 and 7.1 showed no benefit. 1 An additional 9 controlled studies with 434 patients were summarized with the conclusion of no benefit 2 1. Morris LR, Murphy MB, Kitabchi AE. Bicarbonate therapy in severe diabetic ketoacidosis. Ann Intern Med 1986;105: Viallon A, Zeni F, Lafond P, Venet C,Tardy B, Page Y, Bertrand JC. Does bicarbonate therapy improve the management of severe diabetic ketoacidosis? Crit Care Med 1999;27:
23 Nursing Responsibilities Inititate 2 separate IV sites Ensure labs drawn Obtain insulin drip from pharmacy. Check potassium before starting insulin drip. Make sure it is above 3.3 Monitor fingersticks every hour until transition to subcutaneous insulin
24 Transitioning off of IV insulin to subcutaneous insulin There needs to be a minimum of two hour overlap for those patients transitioning off of intravenous insulin to subcutaneous insulin (basal/bolus regime). Ordering basal insulin earlier while an insulin drip is running is encouraged After two hours, the insulin infusion can be turned off There needs to be hourly fingersticks during the overlap of therapy
25 Transition to Subcutaneous Insulin Continue IV insulin until DKA or HHS is resolved. Criteria for resolution of DKA: BG < 200 mg/dl Serum bicarbonate level 15 meq/l Venous ph > 7.3 Anion Gap <12 (primary target) Criteria for resolution of HHS: Improvement of mental status BG 300 mg/dl Serum osmolality of less than 320 mosm/kg
26 Basal-Bolus Insulin Standard of Care Basal insulin Controls glucose production between meals and overnight Nearly constant levels 50% of daily needs Bolus insulin (mealtime or prandial) Limits hyperglycemia after meals Immediate rise and sharp peak at 1 hour postmeal 10% to 20% of total daily insulin requirement at each meal
27 Basal-Bolus Insulin Standard of Care For ideal insulin replacement therapy Both components are needed Each component should come from a different insulin with a specific profile Correctional insulin (Supplemental insulin) Supplemental doses of rapid or short acting insulin to correct blood glucose elevations that occur despite use of basal and prandial insulin. Usually administered before meals together with prandial insulin.
28 Transition to Subcutaneous Insulin Avoiding Pitfalls: Timing Give the basal insulin at least 2 hours prior to stopping the insulin drip Consider continuing the drip so that the basal insulin can be given at 8am or HS
29 Transition to Subcutaneous Insulin Avoiding Pitfalls: Basal Dosing Give enough basal Limited evidence-based data regarding transitions Can use the past 6 or 12 hours of stable drip rate to calculate 80% of 24 hour averaged dose Can use a weight based approach and adjust for stress Can use the patient s usual dose adjusted for stress Stress is ~50% excess for 1 st day post DKA
30 Transition to Subcutaneous Insulin Avoiding Pitfalls: Prandial Dosing Give prandial dose if eating 50% or more of meals generally will be 1/3 of basal dose, given qac Give a correction dose ONLY AS AN ADDITION to prandial dose Check 3am FS for at least 1 night post insulin drip use

31
32
33
34
Management of Hyperglycemic Crises
 Management of Hyperglycemic Crises Guillermo E. Umpierrez, MD, CDE, FACP, FACE Professor of Medicine Director Clinical Research, Diabetes & Metabolism Center Emory University School of Medicine Chief,
Management of Hyperglycemic Crises Guillermo E. Umpierrez, MD, CDE, FACP, FACE Professor of Medicine Director Clinical Research, Diabetes & Metabolism Center Emory University School of Medicine Chief,
DKA/HHS Pathway Phase 1 (Adult) Insulin Potassium Bicarbonate
 Insulin Potassium Bicarbonate") Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
Approved by Diabetes Steering Committee, MMC, 2015 DKA/HHS Pathway Phase 1 (Adult) DKA Diagnostic Criteria (See page 3 for more details): Blood glucose >250 mg/dl, Arterial ph
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES
 TREATMENT GUIDELINES") ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
ADVOCATE CHRIST MEDICAL CENTER DKA (DIABETIC KETOACIDOSIS) TREATMENT GUIDELINES DEFINITION -Glucose >250 mg/dl*, anion gap > 16, + ketones * Glucose < 250 does not exclude DKA especially if anion gap >
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State. Adam Bursua, Pharm.D., BCPS
 Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
Diabetic Emergencies: Ketoacidosis and the Hyperglycemic Hyperosmolar State Adam Bursua, Pharm.D., BCPS Objectives Describe the epidemiology of diabetic ketoacidosis (DKA) and the hyperglycemic hyperosmolar
DKA Adult ICU Powerplan
 DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
DKA Adult ICU Powerplan Key Points for ED to ICU DKA power plan In addition to NS fluids and maintenance the regular insulin drip will either already be infusing from ED or needs to be initiated. Regular
Diabetic Ketoacidosis
 October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
October 2015 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Case History HPI: 24 yo man with recent 8 lb. weight loss, increased thirst and frequent
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017
 CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
CDE Exam Preparation Presented by Wendy Graham RD CDE May 4, 2017 DKA at organ level 3 Diabetic Ketoacidosis Characteristics Ketones positive Anion Gap > 12 (High) Blood Sugar > 14 (High) Bicarbonate
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Arterial blood gas Capillary blood glucose every hour. Continue to monitor hourly capillary blood glucose as per protocol (See Appendix A and B)
") Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
Page 1 of 6 Hyperglycemic Emergency Management (DKA/HHS 1 ) - Adult PATIENT PRESENTATION Patient with history of Type 1 or 2 Diabetes Mellitus or presenting with polyuria, polydipsia, nausea/ vomiting,
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: DKA / HHNS PATIENTS REQUIRING INTRAVENOUS INSULIN DRIPS -ADULTS Nursing DATE: REVIEWED: PAGES: 12/14 5/18 1 of 8 RESPONSIBILITY: *RN (Renal/Diabetes/Wound
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked
 are unchecked") Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Available at: BMC-B BMC-D BMC-N BMC-S Condition/Status ***(NOTE)***For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS than 12
Improving Glycemic Control in the Critical Care
 Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
Improving Glycemic Control in the Critical Care Setting /Hospitalists Outline Review current guidelines Review current glycemic targets DKA Treatment Building a perfect glycemic control protocol Transition
AACN PCCN Review. Endocrine
 AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
AACN PCCN Review Endocrine Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com Endocrine I. INTRODUCTION Disorders
Chapter Goal. Learning Objectives 9/12/2012. Chapter 25. Diabetic Emergencies
 Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
Chapter 25 Diabetic Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with diabetic emergencies Learning Objectives Describe pathophysiology
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
DRUG AND TREATMENT *****ALSO ORDER SUB ACUTE DKA IV FLUIDS REGIMEN & SUB ACUTE ELECTROLYTE REPLACEMENT on separate forms ***** Condition/Status For purpose of this DKA Regimen, DKA is considered clear
Diabetic Emergencies DKA, HHS, Hypoglycemia. Disclosure. Learning Objectives
 Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
Diabetic Emergencies DKA, HHS, Hypoglycemia October 2018 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Disclosure Michael McDermott has no conflict
ADMIT DIABETIC KETOACIDOSIS (DKA) PLAN - Phase: Begin Immediately/Emergency Center
 PLAN - Phase: Begin Immediately/Emergency Center") - Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
- Phase: Begin Immediately/Emergency Center Weight PHYSICIAN S Allergies Admit/Discharge/Transfer Patient Status Requested Location: MICU, Pt Status: Inpatient (LOS > 2 midnights) Requested Location: 5E
Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18. High Sugar / Hyperglycemia: Causes, Complications and Management
 Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18 High Sugar / Hyperglycemia: Causes, Complications and Management Case Presentation A 45 year old obese man comes to your clinic with a
Anne Leake, PhD, APRN, BC-ADM ECHO Diabetes Learning Group 4/4/18 High Sugar / Hyperglycemia: Causes, Complications and Management Case Presentation A 45 year old obese man comes to your clinic with a
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
DRUG AND TREATMENT Acute Diabetic Ketoacidosis Condition/Status ***(NOTE)*** For purpose of this DKA Regimen, DKA is considered clear only when the CO2 is GREATER than 18 meq/l and the anion gap is LESS
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!!
 Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis: When Sugar Isn t Sweet!!! W Ricks Hanna Jr MD Assistant Professor of Pediatrics University of Tennessee Health Science Center LeBonheur Children s Hospital Introduction Diabetes
Diabetic Ketoacidosis (DKA) Critical Care Guideline Two Bag System
 Critical Care Guideline Two Bag System") Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Critical Care Guideline Two Bag System Inclusion Criteria (Definition of DKA): Blood glucose (BG) > 200 mg/dl Acidosis (bicarbonate < 15 or blood gas ph < 7.3) Associated glycosuria, ketonuria &/or ketonemia
Diabetic Emergencies in Pregnancy. Brian A. Mason, MS, MD
 Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
Diabetic Emergencies in Pregnancy Brian A. Mason, MS, MD Objectives Recognize the three major risks of major morbidity in the diabetic gravida. Treat these 3 risks promptly and effectively. Diabetic Emergencies
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
With Dr. Sarah Reid and Dr. Sarah Curtis
 5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
5. Headaches 6. Known diabetes 7. Specific high risk groups (ie. Teenagers, children on insulin pumps and those from lower socio-economic status). Episode 63 Pediatric Diabetic Ketoacidosis With Dr. Sarah
DIABETES AND PREGNANCY. CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor
 DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
DIABETES AND PREGNANCY CDE Exam Preparation March 22 & 27, 2018 Presented by Wendy Graham RD CDE Mentor OBJECTIVES Describe targets for blood glucose in pregnancy Discuss the risks to baby if blood glucose
For The Management Of. Diabetic Ketoacidosis
 Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
Guidelines For The Management Of Diabetic Ketoacidosis By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs Kurdistan Higher Council
In - Hospital Diabetes Care. A review and personal experience
 In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
In - Hospital Diabetes Care A review and personal experience Hyperglycemia in the Hospital The Problem Hospitalizations with Diabetes http://www.cdc.gov/diabetes/statistics/dmany/fig1.htm Prevalence of
diabetes in adults Metabolic complications of
 Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology
 Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Vinaya Simha, M.D. Assistant Professor, Division of Endocrinology Faculty photo will be placed here Simha.aj@mayo.edu 2015 MFMER 3543652-1 Diabetic Ketoacidosis a few pearls Mayo School of Continuous Professional
Is a Priming Dose of Insulin Necessary in a Low-Dose Insulin Protocol for the Treatment of Diabetic Ketoacidosis?
 Clinical Care/Education/Nutrition/Psychosocial Research O R I G I N A L A R T I C L E Is a Priming Dose of Insulin Necessary in a Low-Dose Insulin Protocol for the Treatment of Diabetic Ketoacidosis? ABBAS
Clinical Care/Education/Nutrition/Psychosocial Research O R I G I N A L A R T I C L E Is a Priming Dose of Insulin Necessary in a Low-Dose Insulin Protocol for the Treatment of Diabetic Ketoacidosis? ABBAS
Hyperglycaemic Emergencies GRI EDUCATION
 Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Hyperglycaemic Emergencies GRI EDUCATION LEARNING OUTCOMES Develop and describe your system of blood gas interpretation and recognise common patterns of acid-base abnormality. Describe the pathophysiology
Is A Priming Dose Of Insulin Necessary In A Low Dose Insulin Protocol For The Treatment Of Diabetic Ketoacidosis?
 Diabetes Care Publish Ahead of Print, published online August 11, 2008 Is A Priming Dose Of Insulin Necessary In A Low Dose Insulin Protocol For The Treatment Of Diabetic Ketoacidosis? Abbas E. Kitabchi,
Diabetes Care Publish Ahead of Print, published online August 11, 2008 Is A Priming Dose Of Insulin Necessary In A Low Dose Insulin Protocol For The Treatment Of Diabetic Ketoacidosis? Abbas E. Kitabchi,
Multiple c hoice q uestions
 Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
Multiple c hoice q uestions Chapter 1 1. The pathogenesis of hyperglycemia in diabetic ketoacidosis includes all the following mechanisms except for: a. Increased glycogenolysis in the liver b. Increased
Diabetic ketoacidosis and. adults. By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences
 IN THE NAME OF GOD Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences DKA AND HHS Diabetic ketoacidosis
IN THE NAME OF GOD Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults By Dr Karimifar Assistant Prof. of Endocrinology Isfahan University of Medical Sciences DKA AND HHS Diabetic ketoacidosis
Case TWO. Vital Signs: Temperature 36.6degC BP 137/89 HR 110 SpO2 97% on Room Air
 Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Mr N is a 64year old Chinese gentleman who is a heavy drinker, still actively drinking, and chronic smoker of >40pack year history. He has a past medical history significant for Hypertension, Hyperlipidemia,
Diabetes: Inpatient Glucose control
 Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
Diabetes: Inpatient Glucose control Leanne Current, PharmD, BCPS This activity is funded through the Medicaid section 1115(a) Demonstration Texas Healthcare Transformation and Quality Improvement Program
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1
 K E M I A D E Y E R I, P G Y - 1") DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DIABETIC KETOACIDOSIS (DKA) K E M I A D E Y E R I, P G Y - 1 QUESTION # 1 7 year old boy comes to the ER with a 2 week history of abdominal pain and weight loss. Further history reveals polyuria and polydipsia,
DKA: Tripping on Acidosis
 DKA: Tripping on Acidosis Grace Chan Oei, MD, MA Attending Physician, Division of Pediatric Critical Care, Loma Linda University Children s Hospital Assistant Professor of Pediatrics, Loma Linda University
DKA: Tripping on Acidosis Grace Chan Oei, MD, MA Attending Physician, Division of Pediatric Critical Care, Loma Linda University Children s Hospital Assistant Professor of Pediatrics, Loma Linda University
COMPLIANCE WITH THIS DOCUMENT IS MANDATORY
 COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
COVER SHEET `NAME OF DOCUMENT TYPE OF DOCUMENT at Shoalhaven Hospital Group Critical Care Procedure DOCUMENT NUMBER DATE OF PUBLICATION February 2018 RISK RATING Medium REVIEW DATE February 2021 FORMER
Clinical Guideline DKA
 Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
Clinical Guideline DKA Pediatric Emergency & Critical Care Medicine! This guideline should not replace clinical judgment. Inclusion criteria: Known Diabetes Mellitus Concern for new onset Diabetes Mellitus
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow September 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood
Diabetic Emergencies. Goals. Diabetic Ketoacidosis (DKA) 11/6/2008. James Hardy, MD
 11/6/2008. James Hardy, MD") Diabetic Emergencies James Hardy, MD Assistant Clinical Professor Department of Emergency Medicine, UCSF Goals DKA and Hyperosmolar hyperglycemic state (HHS) Treatment guidelines (Peds vs Adult) Interesting
Diabetic Emergencies James Hardy, MD Assistant Clinical Professor Department of Emergency Medicine, UCSF Goals DKA and Hyperosmolar hyperglycemic state (HHS) Treatment guidelines (Peds vs Adult) Interesting
Please inform the Diabetes Nurse Specialist that this patient has been admitted within 24hrs of admission.
 Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
Adult Diabetic Ketoacidosis Care Bundle (V1. Issued October 2014 Review October 2015) Improving patient care This pack includes: DKA Management Guideline Name: (Patient Addressograph) DOB: Hospital No:
DONATION AFTER CARDIAC DEATH PLAN
 DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
DONATION AFTER CARDIAC DEATH PLAN Diagnosis Weight Allergies Patient Care Core Body Temperature Monitoring Maintain body temp 96-99 degrees Farenheit. Utilize Hyper/Hypothermia blanket prn Insert Gastric
Diabetes Related Emergencies
 Diabetes Related Emergencies Dr Ketan Dhatariya MBBS MSc MD MS FRCP PhD Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals Disclosures I am the lead author of the updated
Diabetes Related Emergencies Dr Ketan Dhatariya MBBS MSc MD MS FRCP PhD Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals Disclosures I am the lead author of the updated
Diabetic Ketoacidosis in Adults. Dr. Jessica Ross, Lakeridge Health Port Perry Katrina Manning, RN, BScN
 Diabetic Ketoacidosis in Adults Dr. Jessica Ross, Lakeridge Health Port Perry Katrina Manning, RN, BScN Presenter Disclosures Presenter: Dr. Jessica Ross Relationships with commercial interest: not applicable
Diabetic Ketoacidosis in Adults Dr. Jessica Ross, Lakeridge Health Port Perry Katrina Manning, RN, BScN Presenter Disclosures Presenter: Dr. Jessica Ross Relationships with commercial interest: not applicable
Diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS) are
 and hyperosmolar hyperglycemic state (HHS) are") FEATURE Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome Management H. Evan Dingle, MD; Corey Slovis, MD In this review, the authors discuss the similarities and differences between diabetic
FEATURE Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic Syndrome Management H. Evan Dingle, MD; Corey Slovis, MD In this review, the authors discuss the similarities and differences between diabetic
LETTER TO THE EDITOR
 LETTER TO THE EDITOR A PHYSICOCHEMICAL ACID-BASE APPROACH FOR MANAGING DIABETIC KETOACIDOSIS doi: 10.1590/S1807-59322009000700018 Alexandre Toledo Maciel, Marcelo Park INTRODUCTION Diabetic ketoacidosis
LETTER TO THE EDITOR A PHYSICOCHEMICAL ACID-BASE APPROACH FOR MANAGING DIABETIC KETOACIDOSIS doi: 10.1590/S1807-59322009000700018 Alexandre Toledo Maciel, Marcelo Park INTRODUCTION Diabetic ketoacidosis
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It
 The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
The Hospitalized Child with Diabetes/Hyperglycemia: Don t Sugar Coat It Cassie Brady, MD Assistant Professor of Pediatrics Division of Endocrinology and Diabetes Monroe Carell Junior Children s Hospital
Hyperosmolar Hyperglycemic State (HHS) Erica Kretchman DO October
 Erica Kretchman DO October") Hyperosmolar Hyperglycemic State (HHS) Erica Kretchman DO October 19 2018 Speaker for Valeritas, Medtronic, AstraZenica, Boehringer Ingelheim. These do not influence this presentation Objective Review
Hyperosmolar Hyperglycemic State (HHS) Erica Kretchman DO October 19 2018 Speaker for Valeritas, Medtronic, AstraZenica, Boehringer Ingelheim. These do not influence this presentation Objective Review
George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital
 George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital Disclosure Statement of Financial Interest I, George Ford MD MS, DO NOT have a financial interest/arrangement
George Ford MD MS Assistant Professor Pediatric Endocrinology ETSU and Niswonger Children s Hospital Disclosure Statement of Financial Interest I, George Ford MD MS, DO NOT have a financial interest/arrangement
Inpatient Management of Diabetes Mellitus. Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy
 Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Inpatient Management of Diabetes Mellitus Jessica Garza, Pharm.D. PGY-1 Pharmacotherapy Resident TTUHSC School of Pharmacy 2 Disclosure Jessica Garza does not have any actual or potential conflicts of
Special Situations 1
 Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Special Situations 1 Outline Continuous Nutrition Tube feeds TPN Steroids Pumps Perioperative BG Control 2 Patient receiving continuous TF or TPN Continuous nutrition coverage options: Analog q4hr Regular
Nothing to disclose. Disclosure
 Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
Nothing to disclose. Disclosure Inpatient Management of Diabetes Mellitus Cindy Chin, MD Pediatrics in the Red Rocks 2015 Objectives Name 3 diagnostic criteria for diabetes mellitus. Understand and apply
Lynda Astbury Lead Diabetes Specialist Nurse
 Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Lynda Astbury Lead Diabetes Specialist Nurse WARNING SIGNS AND SYMPTOMS Is patient Feeling unwell? Blood glucose level above 13mmol/L Or higher than the patients day to day readings (even if not eating)
Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY
 Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY Outline Definitions and Pathophysiology of DKA Clinical Presentation/Diagnosis Treatment Process Monitoring in Hospital
Diabetic Ketoacidosis In Children JACQUELYN PETERS PHARMD CANDIDATE 2016 U OF W PHARMACY Outline Definitions and Pathophysiology of DKA Clinical Presentation/Diagnosis Treatment Process Monitoring in Hospital
DIABETES MELLITUS. IAP UG Teaching slides
 DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
DIABETES MELLITUS 1 DIABETES MELLITUS IN CHILDREN Introduction, Definition Classification, pathogenesis Clinical features Investigations and diagnosis Therapy and follow up Complications Carry home message
CCRN/PCCN Review Course May 30, 2013
 A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
A & P Review CCRN/PCCN Review Course May 30, 2013 Endocrine Anterior pituitary Growth hormone: long bone growth Thyroid stimulating hormone: growth, thyroid secretion Adrenocorticotropic hormone: growth,
Diagnosis and Management of DKA and Hyperglycemic, Hyperosmolar States
 Diagnosis and Management of DKA and Hyperglycemic, Hyperosmolar States Lindsay K. Buchert, MSN, RN, ANP-BC Department of Internal Medicine Carolinas Medical Center, Charlotte, NC 2017 Nurse Practitioner
Diagnosis and Management of DKA and Hyperglycemic, Hyperosmolar States Lindsay K. Buchert, MSN, RN, ANP-BC Department of Internal Medicine Carolinas Medical Center, Charlotte, NC 2017 Nurse Practitioner
Glucose Management in Critically Ill Patients
 Glucose Management in Critically Ill Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell Medical
Glucose Management in Critically Ill Patients October 15, 2016 Archana R. Sadhu, MD., FACE Director of System Diabetes Program Director of Transplant Endocrinology Assistant Professor, Weill Cornell Medical
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Diabetic Ketoacidosis. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Objectives. Why is blood glucose important? Hypoglycaemia. Hyperglycaemia. Acute Diabetes Emergencies (DKA,HONK)
") Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Acute Diabetes Emergencies Ross Buchan, DSN North Glasgow June 2017 Objectives Why is blood glucose important? Hypoglycaemia Hyperglycaemia Acute Diabetes Emergencies (DKA,HONK) Importance of Blood Glucose
Diabetes Mellitus Case Study
 COLORADO STATE UNIVERSITY Diabetes Mellitus Case Study Medical Nutrition Therapy By: Emily Lancaster 9/28/2012 [Type the abstract of the document here. The abstract is typically a short summary of the
COLORADO STATE UNIVERSITY Diabetes Mellitus Case Study Medical Nutrition Therapy By: Emily Lancaster 9/28/2012 [Type the abstract of the document here. The abstract is typically a short summary of the
SARASOTA MEMORIAL HOSPITAL
 SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE CARE OF THE INTRAPARTUM PATIENT RECEIVING CONTINUOUS INTRAVENOUS INSULIN ADMINISTRATION (obs25) DATE: REVIEWED: PAGES: 9/93 12/17 1 of 5 PS1094 ISSUED
SARASOTA MEMORIAL HOSPITAL TITLE: NURSING PROCEDURE CARE OF THE INTRAPARTUM PATIENT RECEIVING CONTINUOUS INTRAVENOUS INSULIN ADMINISTRATION (obs25) DATE: REVIEWED: PAGES: 9/93 12/17 1 of 5 PS1094 ISSUED
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Pathogenesis of disease diabetic ketoacidosis
 Pathogenesis of disease diabetic ketoacidosis Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals None Disclosures Diagnostic Criteria
Pathogenesis of disease diabetic ketoacidosis Dr Ketan Dhatariya MBBS MSc MD MS FRCP Consultant in Diabetes and Endocrinology Norfolk and Norwich University Hospitals None Disclosures Diagnostic Criteria
The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA
 The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA Introduction When a mentally altered patient arrives on the scene at any veterinary
The Mentally Altered Diabetic Diagnosis and Management of Hyperosmolar Hyperglycemic Syndrome Christy Michael, BVMS, MBA Introduction When a mentally altered patient arrives on the scene at any veterinary
Two of the most common metabolic emergencies
 CLINICAL DIFFERENTIATING BETWEEN AND Authors: Christy McDonald Lenahan, MSN, RN, FNP-BC, and Brenda Holloway, DNSc, MSN, RN, FNP-BC, Lafayette, LA, Mobile, AL Earn Up to 8.5 CE Hours. See page 270. Two
CLINICAL DIFFERENTIATING BETWEEN AND Authors: Christy McDonald Lenahan, MSN, RN, FNP-BC, and Brenda Holloway, DNSc, MSN, RN, FNP-BC, Lafayette, LA, Mobile, AL Earn Up to 8.5 CE Hours. See page 270. Two
Pediatric Diabetic Ketoacidosis Guidelines
 Pediatric Diabetic Ketoacidosis Guidelines For new onset diabetes in a pediatric patient NOT in DKA (see criteria below) These guidelines may not be appropriate Consult endocrine and pediatric admit resident
Pediatric Diabetic Ketoacidosis Guidelines For new onset diabetes in a pediatric patient NOT in DKA (see criteria below) These guidelines may not be appropriate Consult endocrine and pediatric admit resident
Obstetrics Guidelines. B. Maternal mortality rates are generally less than 1%.
 Page: 1 of 8 SUBJECT: DIABETIC KETOACIDOSIS IN PREGNANCY I. Overview A. Diabetic ketoacidosis (DKA) is an acute medical emergency associated with fetal loss rates in excess of 50%. B. Maternal mortality
Page: 1 of 8 SUBJECT: DIABETIC KETOACIDOSIS IN PREGNANCY I. Overview A. Diabetic ketoacidosis (DKA) is an acute medical emergency associated with fetal loss rates in excess of 50%. B. Maternal mortality
Ketoacidosis and hyperosmolar hyperglycemia
 P O S I T I O N S T A T E M E N T Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia are the two most serious acute metabolic
P O S I T I O N S T A T E M E N T Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia are the two most serious acute metabolic
Ketoacidosis and hyperosmolar hyperglycemia
 P O S I T I O N S T A T E M E N T Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia are the two most serious acute metabolic
P O S I T I O N S T A T E M E N T Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia are the two most serious acute metabolic
LIBERTYHEALTH. Jersey City Medical Center Department of Patient Care Services. Approved by Policy Committee:
 LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
LIBERTYHEALTH Jersey City Medical Center Department of Patient Care Services Guidelines: CRITICAL CARE INSULIN PROTOCOL (MICU/SICU, CCU, ED) Developed by: Pharmacy Dept Approved by: Rita Smith, DNP Senior
Diabetic Ketoacidosis. Raed Abu Sham a, M.D
 Diabetic Ketoacidosis Raed Abu Sham a, M.D Type 1 DM Autoimmune destruction of the pancreatic islet cell Hallmark = lymphocytic infiltration of islets Progresses over years Leads to insulin deficiency
Diabetic Ketoacidosis Raed Abu Sham a, M.D Type 1 DM Autoimmune destruction of the pancreatic islet cell Hallmark = lymphocytic infiltration of islets Progresses over years Leads to insulin deficiency
Published in
 Published in WWW.ENDOTEXT.ORG 2018 HYPERGLYCEMIC CRISES: DIABETIC KETOACIDOSIS (DKA) AND HYPERGLYCEMIC HYPEROSMOLAR STATE (HHS) Aidar R. Gosmanov, M.D., Ph.D., F.A.C.E., Associate Professor of Medicine,
Published in WWW.ENDOTEXT.ORG 2018 HYPERGLYCEMIC CRISES: DIABETIC KETOACIDOSIS (DKA) AND HYPERGLYCEMIC HYPEROSMOLAR STATE (HHS) Aidar R. Gosmanov, M.D., Ph.D., F.A.C.E., Associate Professor of Medicine,
DIABETIC KETOACIDOSIS
 DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
DIABETIC KETOACIDOSIS DANA BARTLETT, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU and ER experience and over 20 years of as a poison
Ketoacidosis and hyperosmolar hyperglycemia
 Reviews/Commentaries/Position P O S I T I O N S T A T E M E N T Statements Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia
Reviews/Commentaries/Position P O S I T I O N S T A T E M E N T Statements Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION Ketoacidosis and hyperosmolar hyperglycemia
Ketoacidosis and hyperosmolar
 Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION The recommendations in this paper are based on the evidence reviewed in the following publication: Management of hyperglycemic
Hyperglycemic Crises in Patients With Diabetes Mellitus AMERICAN DIABETES ASSOCIATION The recommendations in this paper are based on the evidence reviewed in the following publication: Management of hyperglycemic
Diabetic ketoacidosis (DKA) Hyperglycemic Crisis in Adults: Pathophysiology, Presentation, Pitfalls, and Prevention. Michael Fowler, MD
 Hyperglycemic Crisis in Adults: Pathophysiology, Presentation, Pitfalls, and Prevention. Michael Fowler, MD") Hyperglycemic Crisis in Adults: Pathophysiology, Presentation, Pitfalls, and Prevention Michael Fowler, MD Editor s note: This article is the 9th in a 12-part series reviewing the fundamentals of diabetes
Hyperglycemic Crisis in Adults: Pathophysiology, Presentation, Pitfalls, and Prevention Michael Fowler, MD Editor s note: This article is the 9th in a 12-part series reviewing the fundamentals of diabetes
Country Health SA Local Health Network. Version control and change history
 Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Country Health SA Local Health Network Protocol (Clinical) Title: Diabetic Ketoacidosis Management in Adults with Type 1 Diabetes Protocol developed by: CHSALHN Diabetes Service Protocol Sponsor: CHSALHN,
Name: Oasis: Questions EPCP. Professional Development: Diabetes
 EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
EPCP Professional Development: Diabetes Name: Oasis: Questions 1) Type 1 diabetes in characterized by which of the following: 1) adult onset, obesity 2) juvenile onset, lean build 3) auto-immune beta cell
Transforming Diabetes Care
 Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
Transforming Diabetes Care Meeting the Challenge of Inpatient Glycemic Management in the Critical Care Setting Jane Jeffrie Seley, DNP, MSN, MPH, GNP, BC-ADM, CDE, CDTC, FAAN, FAADE Diabetes Nurse Practitioner,
LOW BLOOD GLUCOSE (Hypoglycemia)
") Section Four DAILY CRISES In this section, you will learn about: Low blood glucose High blood glucose Diabetic Ketoacidosis Hyperosmolar Hyperglycemic Nonketotic Syndrome LOW BLOOD GLUCOSE (Hypoglycemia)
Section Four DAILY CRISES In this section, you will learn about: Low blood glucose High blood glucose Diabetic Ketoacidosis Hyperosmolar Hyperglycemic Nonketotic Syndrome LOW BLOOD GLUCOSE (Hypoglycemia)
Disordered Glucose Metabolism
 CHAPTER 137 Disordered Glucose Metabolism Elamin M. Elamin and Chakrapol Sriaroon Introduction Disordered glucose metabolism is a significant medical problem in the outpatient, emergency room, ward, and
CHAPTER 137 Disordered Glucose Metabolism Elamin M. Elamin and Chakrapol Sriaroon Introduction Disordered glucose metabolism is a significant medical problem in the outpatient, emergency room, ward, and
Diabetes mellitus - diagnosis, classification and acute complications. David Karásek 3rd Department of Internal Medicine University Hospital Olomouc
 Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Diabetes mellitus - diagnosis, classification and acute complications David Karásek 3rd Department of Internal Medicine University Hospital Olomouc Diabetes mellitus is a group of metabolic diseases, characterized
Hypoglycemia, Sick Days/DKA and Hospitalization
 Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
Hypoglycemia, Sick Days/DKA and Hospitalization General survival skills for your client with diabetes at home and in Hospital Diabetes Canada guidelines for your client with diabetes while they are in
PHYSICIAN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol
 DTE PROVIDENCE HOSPITL 6801 irport Boulevard, Mobile L 36608, PHYSICIN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol 1. Discontinue all previous insulin and oral diabetic medications
DTE PROVIDENCE HOSPITL 6801 irport Boulevard, Mobile L 36608, PHYSICIN S ORDERS Page 1 of 1 Providence Hospital ICU Insulin Drip Protocol 1. Discontinue all previous insulin and oral diabetic medications
Deepika Reddy MD Department of Endocrinology
 Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
Deepika Reddy MD Department of Endocrinology Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review
SCENARIO. Maternal Medicine -DKA LEARNING OBJECTIVES
 SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
SCENARIO Maternal Medicine -DKA LEARNING OBJECTIVES Recognition of the of the seriously ill patient Diagnosis of DKA in pregnancy Recognition of precipitating factors for DKA Initiate emergency management
Management of Adult patients with Diabetic Ketoacidosis (DKA) & Hyperosmolar Non-ketotic Coma (HONK) Most current literature relevant to critical care
 & Hyperosmolar Non-ketotic Coma (HONK) Most current literature relevant to critical care") NAME OF DOCUMENT TYPE OF DOCUMENT Management of Adult patients with Diabetic Ketoacidosis (DKA) & Hyperosmolar Non-ketotic Coma (HONK) GUIDELINE DOCUMENT NUMBER ED CLIN GL 04 DATE OF PUBLICATION May 2013
NAME OF DOCUMENT TYPE OF DOCUMENT Management of Adult patients with Diabetic Ketoacidosis (DKA) & Hyperosmolar Non-ketotic Coma (HONK) GUIDELINE DOCUMENT NUMBER ED CLIN GL 04 DATE OF PUBLICATION May 2013
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS
 10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
10. ACUTE COMPLICATIONS OF DIABETES MELLITUS Prof. Oren Zinder, Ph.D. Rambam Medical Center, and the Technion Faculty of Medicine, Haifa, Israel 1.1. Hypoglycaemia Hypoglycaemia is a lowered blood glucose
FREQUENCY OF DIABETIC KETOACIDOSIS IN DIABETIC PATIENTS
 Original Article IN DIABETIC PATIENTS Ghulam Abbas Sheikh 1, Dilshad Muhammad 2, Khalid Amin 3 1 Consultant Physician, Aziz Fatimah Hospitals, Faisalabad. 2 Senior Registrar, DHQ Hospital, Faisalabad.
Original Article IN DIABETIC PATIENTS Ghulam Abbas Sheikh 1, Dilshad Muhammad 2, Khalid Amin 3 1 Consultant Physician, Aziz Fatimah Hospitals, Faisalabad. 2 Senior Registrar, DHQ Hospital, Faisalabad.
Inpatient Diabetes and Hyperglycaemia. Philip Dyer Heart of England NHS Foundation Trust Birmingham
 Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham A Case of Inpatient Diabetes 22.09.15 Mrs DE Ketosis-prone T2DM on bd Humulin-I, Metformin and Linagliptin
Inpatient Diabetes and Hyperglycaemia Philip Dyer Heart of England NHS Foundation Trust Birmingham A Case of Inpatient Diabetes 22.09.15 Mrs DE Ketosis-prone T2DM on bd Humulin-I, Metformin and Linagliptin
Gen: Mild distress but A&O x 3. Heart: RHB, Lungs: OK 36.8, 120, 34, 132/88 HEENT: WNL. no rebound. Case 1 PE: No fever/chills, URI s/s
 Diabetic Emergencies 32 y/o F: N/V and diffuse abd pain for 24 hr PHx: type 1 DM for 7 yr Meds: Insulin 70/30 28UqAM, 16UqPM What do you like to know? Case Presentation No fever/chills, URI s/s Urinary
Diabetic Emergencies 32 y/o F: N/V and diffuse abd pain for 24 hr PHx: type 1 DM for 7 yr Meds: Insulin 70/30 28UqAM, 16UqPM What do you like to know? Case Presentation No fever/chills, URI s/s Urinary
PEDIATRIC DIABETIC KETOACIDOSIS
 PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois EMSC Pediatric DKA Data Dictionary Confidential for QI purposes only AIM Statement: To provide safe and effective care
PEDIATRIC DIABETIC KETOACIDOSIS October 2011 Quality Improvement Resources Illinois EMSC Pediatric DKA Data Dictionary Confidential for QI purposes only AIM Statement: To provide safe and effective care
APPENDIX American Diabetes Association. Published online at
 APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
APPENDIX 1 INPATIENT MANAGEMENT OF TYPE 2 DIABETES No algorithm applies to all patients with diabetes. These guidelines apply to patients with type 2 diabetes who are not on glucocorticoids, have no
Glycemic care pathway patient and/or Diabetes noted preoperatively. confirm BG order / write order holding area. TARGET mg/dL
 BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding
BG check options POCT glucometer (pre/pacu) POCT istat (intraop) venous/arterial BG venous BG (lab) Glycemic care pathway patient and/or Diabetes noted preoperatively confirm BG order / write order holding