3/22/2017. Type 2 Diabetes Pathophysiology and Pharmacology Review. Accreditation Statement
|
|
|
- Frank Pope
- 6 years ago
- Views:
Transcription

1 Type 2 Diabetes Pathophysiology and Pharmacology Review Joshua J. Neumiller, PharmD, CDE, FASCP Vice Chair & Associate Professor, Department of Pharmacotherapy Washington State University Spokane, WA This educational activity is sponsored by Postgraduate Healthcare Education, LLC (PHE) and supported by an educational grant from Boehringer Ingelheim Pharmaceuticals Inc. and Lilly USA, LLC. Accreditation Statement PHARMACY Postgraduate Healthcare Education, LLC is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. UAN: L1-P H1-P Credits: 1. hour (.1 ceu) Type of Activity: Knowledge Media: Internet New Horizons in Diabetes Care: Reducing Cardiovascular Risks Through Advances in Pharmacotherapy This valuable and engaging 3-part webinar series was designed to inform and educate pharmacists in all practice settings who are involved in the care of patients with T2DM, bridging the gap of learning about the new classes of medications for T2DM, including their pathophysiologic basis of action across the continuum of care for patients with T2DM, while keeping in mind the cardiovascular safety of these -lowering medications. Attend one, two, or all three webinars and gain confidence in applying the results of recent studies to clinical practice. Part 1 - Type 2 Diabetes Pathophysiology and Pharmacology Review Wednesday, March 22, 217 at 1: PM EDT Part 2 Intensifying Therapy after Basal Insulin Optimization in Type 2 Diabetes Options for Targeting Postprandial Control Thursday, March 3, 217 at 1: PM EDT Part 3 Cardiovascular Outcome Trials (CVOTs): Practical Considerations for your Type 2 Diabetes Patients Wednesday, April 5, 217 at 1: PM EDT 1
2 Disclosures to Participants Conflicts of Interest and Financial Relationships Presenter and Program Chair: Joshua J. Neumiller, PharmD, CDE, FASCP Advisory Board/Consultant: Eli Lilly & Boehringer Ingelheim Research Grant Support to WSU: Novo Nordisk Content Reviewer: Tricia Russell, PharmD, BCPS, CDE has nothing to disclose. Learning Objectives After completing this webinar, participants will be able to: 1. Describe the clinical pharmacology of the dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagon-like peptide-1 (GLP-1) receptor agonists, and sodium- cotransporter-2 (SGLT-2) inhibitors 2. Understand the concept of implementing combination pharmacotherapy by addressing complementary pathophysiologic targets 3. Describe the role of DPP-4 inhibitors, GLP-1 receptor agonists, and SGLT-2 inhibitors as monotherapy and in combination with other medications for the treatment of type 2 diabetes (T2DM) Normal Regulation of Glucose Homeostasis Glucagon (α-cell) Pancreas Insulin (β-cell) Glucose output Liver Normal blood Glucose uptake Muscle Porte D Jr, Kahn SE. Clin Invest Med. 1995;18(4): Kahn CR, Saltiel AR. Joslin s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 25:
3 Dysregulation of Glucose Homeostasis in T2DM Islet cell dysfunction Glucagon (α-cell) Pancreas * Reduced effect of insulin indicating insulin resistance Glucose output Insulin (β-cell) Hyperglycemia * Glucose uptake Liver Muscle Del Prato S, MarchettiP. Horm Metab Res. 24;36(11-12): Porte D Jr, Kahn SE. Clin Invest Med. 1995;18(4): Kahn CR, Saltiel AR. Joslin s Diabetes Mellitus. 14th ed. Lippincott Williams & Wilkins; 25: Natural History of T2DM Years from diagnosis Diagnosis Onset Insulin resistance Insulin secretion Postprandial (PPG) Fasting (FPG) Pre-diabetes Microvascular complications Macrovascular complications T2DM Ramlo-Halsted BA, Edelman SV. Prim Care. 1999;26(4): Nathan DM. N Engl J Med. 22;347(17): Pathophysiologic Defects in T2DM Decreased incretin effect Impaired insulin secretion Islet b-cell lipolysis glucagon secretion Islet a- cell Hyperglycemia reabsorption hepatic production Decreased uptake Neurotransmitter dysfunction DeFronzo RA. Diabetes. 29;58(4):
4 Select Antihyperglycemic Pharmacotherapy Options Oral medications Biguanides Sulfonylureas Meglitinides Thiazolidinediones a-glucosidase inhibitors (AGIs) DPP-4 inhibitors SGLT-2 inhibitors Non-insulin injectable agents GLP-1 receptor agonists Amylin mimetic Insulin Prandial insulin Insulin lispro Insulin aspart Insulin glulisine Insulin human inhaled Regular human insulin Basal insulin Insulin NPH Insulin detemir Insulin glargine U-1 Insulin glargine U-3 Insulin degludec Cornell S, Dorsey VJ. Postgrad Med. 212;124(4): American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care. 217;4(Suppl 1):S64-S74. Pathophysiologic Defects in T2DM Decreased incretin effect Impaired insulin secretion Islet b-cell lipolysis glucagon secretion Islet a- cell Hyperglycemia reabsorption hepatic production Decreased uptake Neurotransmitter dysfunction DeFronzo RA. Diabetes. 29;58(4):
:46-52.")
5 Insulin (mu/l) Insulin (mu/l) 3/22/217 The Incretin Effect Control subjects (n = 8) People with T2DM (n = 14) Incretin effect Time (min) Time (min) 18 Oral load Intravenous infusion Nauck M, et al. Diabetologia. 1986;29(1): Endogenous GLP-1: Effects in Humans After food ingestion GLP-1 is secreted from L-cells of the jejunum and ileum GLP-1 then Stimulates -dependent insulin secretion Suppresses glucagon secretion Slows gastric emptying Increases satiety Drucker DJ. Curr Pharm Des. 21;7(14): Drucker DJ. Mol Endocrinol. 23;17(2): Drucker DJ. Cell Metab. 26;3(3): Pharmacological Strategies to Augment the Incretin Effect GLP-1 secretion is impaired in T2DM Natural GLP-1 has an extremely short half-life Block DPP-4 to slow the enzymatic degradation of GLP-1: Sitagliptin (Januvia) Saxagliptin (Onglyza) Linagliptin (Tradjenta) Alogliptin (Nesina) Add GLP-1 analogues with longer half-life: Exenatide (Byetta) Liraglutide (Victoza) Lixisenatide (Adlyxin) Once-weekly Exenatide (Bydureon) Albiglutide (Tanzeum) Dulaglutide (Trulicity) 5
6 Comparison of Incretin-based Therapies Select clinical properties of DPP-4 inhibitors and GLP-1 receptor agonists DPP-4 inhibitors GLP-1 receptor agonists Slow gastric emptying No Yes Effect on postprandial hyperglycemia Yes Yes (variable) Effect on weight Weight neutral Weight loss Route of administration Oral Subcutaneous injection Associated with hypoglycemia when used as monotherapy No No Neumiller JJ. Med Clin North Am. 215;99(1): Characteristic Hypoglycemia risk Initial dose (normal CrCl) Dose adjustment for renal impairment CrCl = creatinine clearance. Comparison of DPP-4 Inhibitors Currently Available in the United States (U.S.) Sitagliptin (Januvia) Saxagliptin (Onglyza) Linagliptin (Tradjenta) Alogliptin (Nesina) Low Low Low Low 1 mg daily 5 mg daily 5 mg daily 25 mg daily CrCl < 5 ml/min: 5 mg daily CrCl 3 ml/min: 25 mg daily CrCl 5 ml/min: 2.5 mg daily No adjustment recommended on the basis of renal function CrCl < 6 ml/min: 12.5 mg daily CrCl < 3 ml/min: 6.25 mg daily Sitagliptin prescribing information, 29. Saxagliptin prescribing information, 29. Linagliptinprescribing information, 212. Alogliptinprescribing information, 213. Effects of Currently Available DPP-4 Inhibitors Characteristic Average A1C lowering* Sitagliptin Saxagliptin Linagliptin Alogliptin (Januvia) (Onglyza) (Tradjenta) (Nesina).65% to.79%.36% to.82%.5% to.69%.47% to.85% Average weight change* +.3 to +1.2 kg -.51 to +1.3 kg +.33 to +1.1 kg +.14 to +.51 kg *PBO-subtracted change from baseline; baseline characteristics of study groups and concomitant medications varied among studies. A1C = Hemoglobin A1C. Neumiller JJ. Med Clin North Am. 215;99(1): Sitagliptin prescribing information, 29. Saxagliptin prescribing information, 29. Linagliptinprescribing information, 212. Alogliptinprescribing information,
7 Exenatide BID Exenatide QW Exenatide BID Exenatide QW Exenatide QW Liraglutide Exenatide BID Liraglutide Dulaglutide 1.5 mg Dulaglutide.75 mg Exenatide BID Liraglutide Dulaglutide 1.5 mg Lixisenatide Exenatide BID Liraglutide Albiglutide 3/22/217 Key Considerations for the Use of DPP-4 Inhibitors Oral administration Generally weight neutral Side effects: Headache Nasopharyngitis/upper respiratory tract infections Generally well tolerated Warnings/precautions: Pancreatitis Hypoglycemia (when added to secretagogues or insulin) Allergic reactions Heart failure? (saxagliptin & alogliptin) Comparison of A1C Reductions with GLP-1 Receptor Agonists Study DURATION-1 DURATION-5 DURATION-6 LEAD-6 AWARD-1 AWARD-6 GetGoal-X HARMONY Change in A1C (%) BID = twice daily; QW = once weekly. Adapted from Trujillo JM, et al. Ther Adv Endocrinol Metab. 215;6(1):19-28.; Erratum. 215;6(3): Madsbad S. Diabetes Obes Metab. 216;18(4): GLP-1 Receptor Agonists: Weight Change Ranges in Phase III Trials Lixisenatide 1-2 mcg QD -.28 to kg Albiglutide 3 mg QW +.28 to kg Dulaglutide 1.5 mg QW -1.3 to -3.3 kg Dulaglutide.75 mg QW +.21 to -2.6 kg Liraglutide 1.8 mg QD -.2 to -3.6 kg Liraglutide 1.2 mg QD +.3 to -2.6 kg Exenatide 2 mg QW -2. to -3.7 kg Exenatide 1 µg BID * -1.7 to -3.6 kg Weight reduction (kg) QD = once daily. Adapted from Triplitt C, Solis-Herrera C. Diabetes Educ. 215;41(suppl 1):32S-46S. 7
8 Comparison of Exenatide Products (3-week Data) Exenatide Exenatide BID extended-release suspension A1C reduction (%) FPG reduction (mg/dl) PPG reduction (mg/dl) Achievement of A1C < 7% 1.9 a 41 b 96 77% d c 61% Change in body weight (kg) a P =.23; b P <.1; c P =.124; d P =.39 versus comparator. Drucker DJ, et al. Lancet. 28;372(9645): Key Considerations for the Use of GLP-1 Receptor Agonists Subcutaneous administration Can result in weight loss Side effects: Nausea/vomiting Injection site reactions Contraindications: Personal/family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (long-acting products) Warnings/precautions: Pancreatitis Hypoglycemia (when added to secretagogues or insulin) Pathophysiologic Defects in T2DM Decreased incretin effect Impaired insulin secretion Islet b-cell lipolysis glucagon secretion Islet a- cell Hyperglycemia reabsorption hepatic production Decreased uptake Neurotransmitter dysfunction DeFronzo RA. Diabetes. 29;58(4):
:377-385.")
9 Renal Glucose Reabsorption Under Normal Conditions ~18 grams of filtered per day SGLT-2 Reabsorption of ~9% of filtered Virtually no urinary excretion SGLT-1 Reabsorption of ~1% of filtered Neumiller JJ, et al. Drugs. 21;7(4): SGLT-2 Inhibition Small intestine SGLT-1 Blood vessel SGLT-1 Glucose ~9% of filtered is reabsorbed through SGLT-2 transporters in the early proximal tubule Glomeruli SGLT-2 SGLT-2 inhibitor Urine Inhibition of SGLT-2 transporters in the proximal tubule blocks the reabsorption of filtered, leading to increased excretion via urine Idris I, Donnelly R. Diabetes Obes Metab. 29;11(2): Canagliflozin versus Glimepiride as Add-on to Metformin: Change in A1C CANA = canagliflozin; GLIM = glimepiride. Cefalu WT, et al. Poster presented at the 73rd Scientific Session of the ADA. June 21-25, 213; Chicago, IL. 9
10 Canagliflozin versus Glimepiride as Add-on to Metformin: Change in Weight Cefalu WT, et al. Poster presented at the 73rd Scientific Session of the ADA. June 21-25, 213; Chicago, IL. Comparison of SGLT-2 Inhibitors Currently Available in the U.S. Characteristic Hypoglycemia risk (as monotherapy) Canagliflozin (Invokana) Dapagliflozin (Farxiga) Empagliflozin (Jardiance) Low Low Low Dose 1 mg daily before breakfast; increase to 3 mg daily, if needed 5 mg daily in the morning; increase to 1 mg daily, if needed 1 mg daily in the morning; increase to 25 mg, if needed Effect on weight Weight loss Weight loss Weight loss Renal Dose Adjustment of SGLT-2 Inhibitors Agent Canagliflozin (Invokana) Dapagliflozin (Farxiga) Empagliflozin (Jardiance) Dosing in CKD stages 3, 4 and 5 (non-dialysis) egfr 6 ml/min/1.73 m 2 No dosage adjustment needed egfr ml/min/1.73 m 2 Do not exceed 1 mg/day by mouth egfr < 45 ml/min/1.73 m 2 Do not initiate and discontinue in patients currently receiving drug Do not initiate; discontinue with egfr < 6 ml/min/1.73 m 2 egfr 45 ml/min/1.73 m 2 No dosage adjustment needed egfr < 45 ml/min/1.73 m 2 Do not initiate and discontinue in patients currently receiving drug egfr = estimated glomerular filtration rate. Canagliflozin prescribing information, 217. Dapagliflozin prescribing information, 216. Empagliflozin prescribing information, 216. Kohan DE, et al. Kidney Int. 214;85(4):
11 Canagliflozin: Less A1C Reduction with Declining egfr Woo V, et al. Poster presented at the 73rd Scientific Session of the ADA. June 21-25, 213; Chicago, IL. Key Considerations for the Use of SGLT-2 Inhibitors Unique mechanism of action Have been studied in combination with a variety of other medication classes Oral administration Low hypoglycemia risk as monotherapy Caution when used with secretagogues or insulin Can result in weight loss and modest decrease in blood pressure Side effects: Genital mycotic infections Urinary tract infections Orthostasis (especially in elderly, chronic kidney disease, diuretic use) Watch volume status levels of low-density lipoproteins Euglycemic diabetic ketoacidosis American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care. 217;4(Suppl 1):S64-S74. 11
 Sulfonylurea Oral No Both 1.5 2. Metformin Oral Yes FPG 1.5 Glitazones Oral Yes Both 1. 1.5 Meglitinides Oral No PPG.5 2. AGIs Oral No PPG.5 1.")
12 Blood (mmol/l) ΔA1C (%) ΔFPG (mmol/l) ΔBody weight (kg) 3/22/217 Comparison of Glucose-lowering Abilities of T2DM Pharmacotherapy Options Monotherapy Route of administration Targets insulin resistance Target : FPG or PPG A1C reduction* (%) Sulfonylurea Oral No Both Metformin Oral Yes FPG 1.5 Glitazones Oral Yes Both Meglitinides Oral No PPG.5 2. AGIs Oral No PPG.5 1. DPP-4 inhibitors Oral No PPG.5.7 Bile acid sequestrant Oral No PPG.4 Dopamine agonists Oral No PPG.4 SGLT-2 inhibitors Oral toxicity Both GLP-1 receptor agonists Injectable No Short-acting PPG Long-acting Both Amylin analogs Injectable No PPG.6 Insulin Injectable toxicity *A1C reduction data are not from head-to-head comparative studies. Basal FPG Bolus PPG as much as needed Unger J, Parkin CG. Postgrad Med. 21;122(3): Cornell S, Dorsey VJ. Postgrad Med. 212;124(4): Once FBG is optimized, start addressing PPG excursions: Add GLP-1 receptor agonist or Add 1 rapid-acting insulin injection to largest meal or Change to premixed insulin twice daily American Diabetes Association Standards of Medical Care in Diabetes. Approaches to glycemic treatment. Diabetes Care. 217;4(Suppl 1):S64-S74. GLP-1 Receptor Agonist vs. Bolus Insulin in Patients with T2DM and Optimized Basal Insulin Weeks since randomization a a a a a a a a Weeks since randomization 3 Insulin lispro Exenatide BID Pre Post Pre Post Pre Post 3AM Breakfast Lunch Dinner b b b b b Weeks since randomization b b b 3 a p <.1 for exenatide BID vs. insulin lispro b p <.1 for exenatide BID vs. insulin lispro Exenatide caused more gastrointestinal issues (47% vs. 13%) but fewer non-nocturnal episodes of hypoglycemia (15% vs. 34%) than insulin lispro Diamant M, et al. Diabetes Care. 214;37(1):

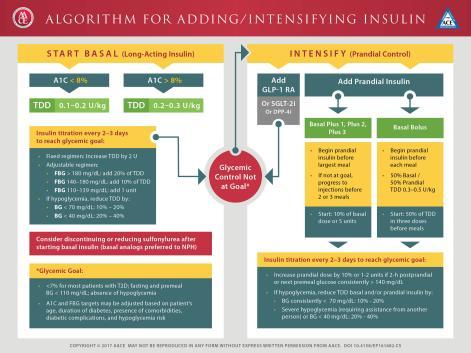
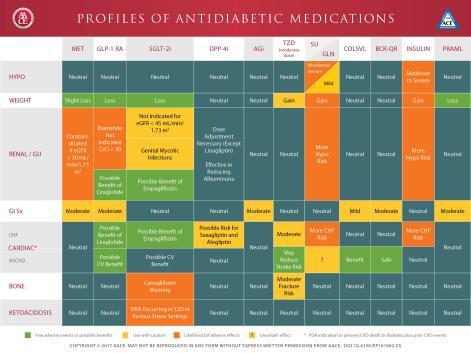
13 Reprinted with permission from American Association of Clinical Endocrinologists 217 AACE. Garber AJ, Abrahamson MJ, Barzilay JI, et al. AACE/ACE comprehensive type 2 diabetes management algorithm 217. Endocr Pract.217;23: Reprinted with permission from American Association of Clinical Endocrinologists 217 AACE. Garber AJ, Abrahamson MJ, Barzilay JI, et al. AACE/ACE comprehensive type 2 diabetes management algorithm 217. Endocr Pract.217;23: Reprinted with permission from American Association of Clinical Endocrinologists 217 AACE. Garber AJ, Abrahamson MJ, Barzilay JI, et al. AACE/ACE comprehensive type 2 diabetes management algorithm 217. Endocr Pract.217;23:
14 Don t Miss the Upcoming Webinars in This Series! Intensifying Therapy after Basal Insulin Optimization in Type 2 Diabetes Options for Targeting Postprandial Control Presenter: Dr. Susan Cornell Cardiovascular Outcome Trials (CVOTs): Practical Considerations for Your Type 2 Diabetes Patients Presenter: Dr. Curtis Triplitt Thank you! Special Thanks: Postgraduate Healthcare Education, LLC Susan Cornell, PharmD Curtis Triplitt, PharmD How To Earn Credit Click through the URL After reviewing the information, click on the Take Evaluation button located at the bottom of the page Sign in with your username and password Fill out the two screen evaluation form and click submit Your credit will be automatically uploaded to CPE Monitor IMPORTANT: In order to claim credit you must have been in attendance through the live event platform and watched and listened to the event in its entirety. Postgraduate Healthcare Education, LLC has the right to deny credit to individuals that have not attended and participated in this webinar in its entirety. Postgraduate Healthcare Education, LLC completes audits of attendees on a routine basis to ensure compliance with all ACPE standards. 14
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors. Bryce Fukunaga PharmD April 25, 2018
 Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Side Effects of: GLP-1 agonists DPP-4 inhibitors SGLT-2 inhibitors Bryce Fukunaga PharmD April 25, 2018 Objectives For each drug class: Identify the overall place in therapy Explain the mechanism of action
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Exploring Non-Insulin Therapies in Type 1 Diabetes
 Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
Exploring Non-Insulin Therapies in Type 1 Diabetes Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Disclosures Dr. Cornell: Advanced
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
What s New? An Antihyperglycemic Medications Update
 What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
What s New? An Antihyperglycemic Medications Update WADE 2016 Annual Conference Josh Neumiller, PharmD, CDE, FASCP Associate Professor Department of Pharmacotherapy Washington State University Disclosures
2/9/2016. The Evolving Armamentarium for Type 2 Diabetes: Incorporating New Classes in the Treatment of Our Patients. Objectives: Pharmacists
 WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
WAYNE STATE UNIVERSITY COLLEGE OF PHARMACY & HEALTH SCIENCES FEBRUARY 28, 2016 The Evolving Armamentarium for Type 2 Diabetes: Clinical Assistant Professor, Department of Pharmacy Practice Ambulatory Care
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
FARXIGA (dapagliflozin) Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)
 Jardiance (empagliflozin) tablets. Synjardy (empagliflozin and metformin hydrochloride) tablets. GLUCOPHAGE* (metformin)") Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Type 2 Medications Drug Class How It Works Brand and Generic Names Manufacturers Usual Starting Dose The kidneys filter sugar and either absorb it back into your body for energy or remove it through your
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Exploring Non-Insulin Therapies in Type 1 Diabetes. Objectives. Pre-Assessment Question #1. Disclosures
 Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
Exploring Non-Insulin Therapies in Type 1 Diabetes Disclosures Dr. Cornell: Advanced Practitioner Advisory Board and Speakers Bureau: Novo Nordisk Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Table 1. Antihyperglycemic agents for use in type 2 diabetes
 Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
Table 1. Antihyperglycemic agents for use in type 2 diabetes DRUG IN ALPHA-GLUCOSIDASE INHIBITOR: inhibits pancreatic alpha-amyle and intestinal alpha-glucoside Acarbose (Glucobay) 0.6% Negligible Not
STEP THERAPY CRITERIA
 CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
CATEGORY DRUG CLASS BRAND NAME (generic) STEP THERAPY CRITERIA AMYLIN ANALOG: SYMLIN/SYMLINPEN (pramlintide acetate) ANTIDIABETIC AGENTS GLUCAGON-LIKE PEPTIDE-1 RECEPTOR AGONIST (GLP-1): ADLYXIN (lixisenatide)
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Drug Class Review Newer Diabetes Medications and Combinations
 Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Drug Class Review Newer Diabetes Medications and Combinations Final Update 2 Report July 2016 The purpose reports is to make available information regarding the comparative clinical effectiveness and harms
Antihyperglycemic Agents in Diabetes. Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014
 Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
Antihyperglycemic Agents in Diabetes Jamie Messenger, PharmD, CPP Department of Family Medicine East Carolina University August 18, 2014 Objectives Review 2014 ADA Standards of Medical Care in DM as they
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Objectives. How Medicine Works to Control Blood Sugar Levels. What Happens When We Eat? What is diabetes? High Blood Glucose (Hyperglycemia)
") How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
How Medicine Works to Control Blood Sugar Levels Stacie Petersen, RN, CDE Objectives Define Diabetes List how medications work (ominous octet) Identify side effects of medications for diabetes What is
RPCC Pharmacy Forum. The Type 2 Diabetes Issue. Type 2 Diabetes: The Basics
 Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Nov/Dec 2015 Issue 11 RPCC Pharmacy Forum Special Interest Articles: Diabetes Medication Chart Insulin Chart Afreeza Did you know? Exanatide, marketed as Byetta, is the synthetic form of exendin-4, which
Very Practical Tips for Managing Type 2 Diabetes
 Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Very Practical Tips for Managing Type 2 Diabetes Jean-François Yale, MD, FRCPC McGill University Health Centre, Montreal, Canada Jean-francois.yale@mcgill.ca www.dryale.ca OBJECTIVES DISCLOSURES The participant
Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University - Chicago College of Pharmacy Objectives Describe the mechanism of action
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA 2012 Virginia Mason Medical
 Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Jonathan Stoehr, MD PhD Endocrinology, Diabetes, Metabolism and Nutrition Virginia Mason Medical Center Seattle, WA There is no conflict of interest that could be perceived as prejudicing the impartiality
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South ALSHP Fall Meeting September 30, 2016
 Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
Joshua Settle, PharmD Clinical Pharmacist Baptist Medical Center South jjsettle@baptistfirst.org ALSHP Fall Meeting September 30, 2016 Objectives Describe the current information concerning newly approved
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD. Disclosures. Objectives 9/1/2015
 Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Update Bryan Heart Conference September 5, 2015 Shannon Wakeley, MD Disclosures I speak on behalf of the following companies: Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Sanofi and
Diabetes Mellitus. Intended Learning Objectives:
 Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Intended Learning Objectives: Diabetes Mellitus 1. Compare and contrast the differences between the drug therapy recommendations of several of the latest and leading diabetes guidelines. 2. Assess the
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Date of Review: September 2016 Date of Last Review: September 2015
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Objectives. Why is Glucose Control Important? 11/2/2016. Jeopardy: Update on Diabetes Pharmacotherapy
 Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Jeopardy: Update on Diabetes Pharmacotherapy Susan Cornell, BS, PharmD, CDE, FAPhA, FAADE Associate Professor Midwestern University Chicago College of Pharmacy Objectives Describe the mechanism of action
Updates in Diabetes Care
 Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Updates in Diabetes Care Disclosures Nothing to disclose Pharmacist Objectives 1. List strategies for improving diabetes care 2. Understand benefits and risks associated with newer pharmacotherapeutic
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
DIABETES. overview of pharmacologic agents used in the management of. Overview 4/3/2014 OBJECTIVES. Injectable Agents
 overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
overview of pharmacologic agents used in the management of DIABETES Kyle Roberts, Pharm.D. PGY-1 Pharmacy Resident Saint Alphonsus RMC 1. List the different classes of diabetes medications, including the
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Objectives. Recognize all available medical treatment options for diabetes. Individualize treatment and glycemic target based on patient factors
 No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
No disclosure Objectives Recognize all available medical treatment options for diabetes Individualize treatment and glycemic target based on patient factors Should be able to switch to more affordable
GLYXAMBI (empagliflozin-linagliptin) oral tablet
 oral tablet") GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
2018 Diabetes Summit Managing Diabetes: An Art and a Science
 2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
2018 Diabetes Summit Managing Diabetes: An Art and a Science Natasha Petry, PharmD, BCACP NDSU College of Health Professions, School of Pharmacy, Department of Pharmacy Practice Patient-Centered Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
DIABETES UPDATE 2018
 DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
DIABETES UPDATE 2018 Jerome V. Tolbert, M.D., Ph.D. Assistant Professor of Medicine Icahn School of Medicine at Mt. Sinai Division of Endocrinology and Bone Diseases 317 East 17 th Street New York, New
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
What the Pill Looks Like. How it Works. Slows carbohydrate absorption. Reduces amount of sugar made by the liver. Increases release of insulin
 Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Diabetes s Oral s - Pills These are some of the pills that are currently available in Canada to treat diabetes. Each medication has benefits and side effects you should be aware of. Your diabetes team
Presented By: Creative Educational Concepts, Inc. Lexington, KY
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions. Insulins. Rapid Short Intermediate Long Mix
 Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medications Diabetes Medications Type 1 Insulin is needed Type 2 Oral Diabetes Medications Or Oral Diabetes Medications plus Insulin Or Insulin Alone Diabetes Medications Secretagogues Glipizide
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018
 Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
Diabetes Medication Updates Erica Bukovich, PharmD, BC-ADM, CDE September 20, 2018 Learning Objectives Identify medication classes available for treatment of individuals with diabetes. Demonstrate understanding
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
4/9/2018 HOW TO REGULATE DIABETES MEDICATIONS. By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE. Diagnosis
 HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
HOW TO REGULATE DIABETES MEDICATIONS By Sarah Froemsdorf MSN, RNC, CDE, FNP DISCLOSURES NONE Diagnosis 1 NORMAL BODY The normal pancreas releases one unit of insulin every hour all day. The normal pancreas
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy
 New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
SGLT2 Inhibitors
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: SGLT2 Inhibitors Page: 1 of 7 Last Review Date: June 22, 2018 SGLT2 Inhibitors Description Invokana
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes
 St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Diabetes: Definition Pathophysiology Treatment Goals. By Scott Magee, MD, FACE
 Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
Diabetes: Definition Pathophysiology Treatment Goals By Scott Magee, MD, FACE Disclosures No disclosures to report Definition of Diabetes Mellitus Diabetes Mellitus comprises a group of disorders characterized
A New Therapeutic Strategey for Type II Diabetes: Update 2008
 Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Faculty. Concentrated Insulin: Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management. Disclosures. Learning Objectives
 Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
Examining the Necessity of Newer Insulins for In-Hospital Diabetes Management Faculty Susan Cornell, PharmD, CDE, FAPhA, FAADE Associate Professor of Pharmacy Practice Associate Director of Experiential
New Therapies for Diabetes
 Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
Type 2 diabetes is increasingly prevalent New Therapies for Diabetes Lynn Mack, M.D. Associate Professor Diabetes, Endocrinology, & Metabolism The Nebraska Medical Center lmack@unmc.edu No Conflicts of
9/16/2013. Sherwin D Souza, M.D.
 Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
Sherwin D Souza, M.D. Burden of disease in 2013 Type 2 DM Glucose Management Goals-understand the new guidelines by ADA/ AACE Drugs available for management of diabetes in 2013 (non insulin and insulin
The Diabetes Guidelines Trek: The Next Generation. Inpatient Diabetes Guidelines. Learning Objectives. Current Inpatient Guidelines
 The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
The Diabetes Guidelines Trek: The Next Generation J. Christopher Lynch, PharmD, BCACP Southern Illinois University Edwardsville School of Pharmacy Susan Cornell BS, PharmD, CDE, FAPhA, FAADE Midwestern
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has