INTERIM REPORT ON KIDNEY TRANSPLANTATION
|
|
|
- Eunice Porter
- 6 years ago
- Views:
Transcription


1 INTERIM REPORT ON KIDNEY TRANSPLANTATION 5 YEAR REPORT (1 OCTOBER SEPTEMBER 2016) PUBLISHED MARCH 2017 PRODUCED IN COLLABORATION WITH NHS ENGLAND
2 Contents
3 1 Executive Summary Introduction... 3 ADULT Transplant list Patients on the kidney transplant list as at 31 March and 30 September, Median waiting time to transplant, 1 October September Response to kidney offers... Error! Bookmark not defined. 4.1 Standard criteria offer decline rates, 1 April September Extended criteria offer decline rates, 1 April September Reallocation of kidneys, 1 April September Transplants Kidney only transplants, 1 October September Kidney donor risk-index 1, 1 October September Cold ischaemia time, 1 October September Kidney outcomes Deceased donor graft and patient survival Living donor graft and patient survival Appendix A1 Glossary of terms A2 Statistical methodology and risk-adjustment for survival rate estimation A3 Factors used in risk-adjusted models for patient survival from listing... 45
4 1 Executive Summary Executive Summary - 1 -
5 This report presents key figures about kidney transplantation in the UK. The period reported covers 5 years of transplant data, from 1 October 2011 to 30 September The report presents information on the number of transplants and survival analysis after first kidney only transplantation on a national and centre-specific basis. Key findings On 30 September 2016, there were 5,055 adult patients on the UK active kidney transplant list which represents a 5% decrease in the number of patients a year earlier. There were 1,442 adult kidney only transplants performed in the UK between 1 April 2016 and 30 September 2016, a decrease of 6% compared to the previous 6 month period. Of these, 549 were from DBD donors, 433 were from DCD donors and 460 were from living donors. The national rate of graft survival five years after first adult deceased donor kidney only transplant is 86%. These rates vary between centres, ranging from 81% to 93% (risk-adjusted). The national rate of graft survival five years after first adult living donor kidney only transplant is 93%. These rates vary between centres, ranging from 87% to 97% (risk-adjusted)
6 2 Introduction Introduction - 3 -
7 This report presents information on transplant activity between 1 October 2011 and 30 September 2016, for all 24 centres performing kidney transplantation in the UK. Data were obtained from the UK Transplant Registry, at NHS Blood & Transplant, that holds information relating to donors, recipients and outcomes for all kidney transplants performed in the UK. Graft and patient survival estimates are reported at one-year post-transplant for the period 1 October 2011 to 30 September 2015 and five-year post-transplant for the period 1 October 2007 to 30 September Results are described separately according to the type of donor (deceased and living). The centre specific results for survival estimates are adjusted for differences in risk factors between the centres. The risk models used are described in the Appendix. Patients requiring multi-organ transplants are excluded from all analyses and all results are described for adult patients (aged 18years) other than those presented in this Introduction section which also includes paediatric patients. Throughout this report West London Renal and Transplant Centre is labeled as WLRTC

8 Figure 2.1 shows the number of patients on the kidney transplant list at 31 March and 30 September each year between 2012 and The number of patients actively waiting for a kidney transplant decreased through each 6 monthly period from 6,633 at 31 March 2012 to 5,342 at 30 September Figure 2.2 shows the number of patients on the kidney transplant list at 30 September 2016 for each transplant centre. WLRTC has the largest active transplant list with 436 patients registered for a kidney transplant


9 Figure 2.3 shows the total number of kidney transplants performed in the last five years, in 6 month periods. The number of transplants has increased over the last 5 years from 1,439 between 1 October 2011 and 31 March 2012 to 1,591 between 1 April and 30 September Figure 2.4 shows the total number of kidney transplants performed between 1 April 2016 and 30 September 2016 at each transplant centre. Manchester performed the most kidney transplants in this period with 158 patients receiving a transplant
 were deceased donor kidney only transplants and 499 (31%) were living donor kidney transplants.")
10 Figure 2.5 details the 1592 kidney transplants performed in the UK between 1 April 2016 and 30 September Of these, 1014 (64%) were deceased donor kidney only transplants and 499 (31%) were living donor kidney transplants. Of the 79 multi-organ transplants, 71 were simultaneous kidney and pancreas transplants and 7 were kidney and liver transplants
11 ADULT 3 Transplant list Adult kidney transplant list - 8 -
12 3.1 Patients on the kidney transplant list as at 31 March and 30 September, Figure 3.1 shows the number of adult patients on the kidney only transplant list at 31 March and 30 September each year between 2012 and The number of patients actively waiting for a kidney transplant decreased across each 6 monthly period from 6,327 at 31 March 2012 to 5,055 at 30 September Figure 3.2 shows the number of adult patients on the active kidney only transplant list at 30 September 2016 by centre. In total, there were 5,052 adults patients. WLRTC had the largest proportion of the transplant list (9%) and Plymouth had the smallest (2%)
13 3.2 Median waiting time to transplant, 1 October September 2013 The length of time a patient waits for a kidney transplant varies across the UK. The median waiting time for adult deceased donor kidney only transplantation is shown in Figure 3.3 and Table 3.1 for patients registered at each individual unit. During this period local allocation arrangements were in place for DCD kidneys while DBD kidneys were allocated via the National Kidney Allocation Scheme. The data shown are for all adult patients, joining the list within the time period shown, including those still awaiting a transplant on the day of analysis. Patients who received a live donor or multi-organ transplant are not included. The national allocation scheme introduced in April 2006 is slowly reducing the variability in deceased donor kidney waiting times across the country but currently some variability remains. Waiting times across centres continue to differ in a way that it is difficult for centres to control, given that the National Kidney Allocation Scheme determines allocation of all kidneys available for transplant from donors after brain death (DBD). National Kidney Allocation Scheme Only kidneys from donors after brain death were allocated via a national allocation scheme during the time period analysed. Kidneys from donations after circulatory death (DCD) were allocated to patients through local allocation arrangements and these vary across the country because some centres have a larger DCD programme than others. As of 3 September 2014 one kidney from DCD donors aged between 5 and 49 years will be allocated within four pre-defined regions using the 2006 DBD allocation principles and as such we should start to see further reductions in variability in waiting times across the country. Kidneys from DBD are allocated to patients listed nationally through the Kidney Allocation Scheme. The Kidney Allocation Scheme introduced in April 2006 prioritises patients with ideal tissue matches (000 HLA mismatches) and then assigns points to patients based on the level of tissue match between donor and recipient, the length of time spent waiting for a transplant, age of the recipient (with a progressive reduction in points given after the age of thirty) and location points such that patients geographically close to the retrieval centre receive more points. The patients with the highest number of points for a donated kidney are preferentially offered the kidney, no matter where in the UK they receive their treatment. The median waiting time to transplant for adult patients registered on the kidney only transplant list between 1 October 2010 and 30 September 2013 is 869 days. This ranged from 358 days at Cambridge to 1,226 days at Birmingham
14 Table 3.1 Median waiting time to kidney only transplant in the UK, for adult patients registered 1 October September 2013 Transplant centre Number of patients Waiting time (days) registered Median 95% Confidence interval Adult Cambridge Newcastle Cardiff Leeds Plymouth Liverpool Oxford Nottingham Edinburgh Guy's Glasgow The Royal Free The Royal London St George s Belfast Manchester Leicester Coventry Sheffield Bristol Portsmouth WLRTC Birmingham UK
15 Response to adult kidney offers
16 Offer decline rates Kidney-only offers from DBD donors who had at least one kidney retrieved, offered directly and on behalf of a named individual patient and resulted in transplantation are included in the analysis. Any offers made through the reallocation of kidneys, declined kidney or fast track schemes were excluded, as were offers of kidneys from donations after circulatory death donors. In order to understand centre practices more fully, data are presented separately for standard and extended criteria donors (SCD & ECD). ECD have been defined as DBD donors aged 60 years at the time of death OR aged 50 to 59 years with at least two or three donor characteristics: hypertension, creatinine > 130 μmol/l or death due to intracranial haemorrhage. SCD are DBD donors that did not meet the ECD criteria. Funnel plots were used to compare centre specific offer decline rates and indicate how consistent the rates of the individual transplant centres are with the national rate. The overall national unadjusted offer decline rate is shown by the solid line while the 95% and 99.8% confidence lines are indicated via a thin and thick dotted line, respectively. Each dot in the plot represents an individual transplant centre. Centres that are positioned above the upper limits indicate an offer decline rate that is higher than the national rate, while centres positioned below the lower limits indicates an offer decline rate that is lower than the national rate. Patient case mix is known to influence the number of offers a centre may receive. In this analysis however only individual offers for named patients were considered which excluded any ABO- and HLA-incompatible patients. For this reason it was decided not to risk adjust for known centre differences in patient case mix
17 4.1 Standard criteria offer decline rates, 1 April September 2016 Figure 4.1 compares individual centre offer decline rates with the national rate for SCD over the time period, 1 April 2013 and 30 September Centres can be identified by the information shown in Table 4.1. Leicester, Birmingham, Bristol, Nottingham and WLRTC have offer decline rates consistently higher than the national rate
18 Table 4.1 compares individual centre offer decline rates for SCD over time. Leicester has had an offer decline rate that is consistently higher than national rate since 2013/14; however their offer decline rate has improved from 72% in to 35% between 1 April and 30 September Table 4.1 Adult standard criteria DBD donor kidney offer decline rates by transplant centre, 1 April 2013 and 30 September 2016 Centre Code 2013/ / /16 1 Apr - 30 Sep Overall N (%) N (%) N (%) N (%) N (%) Belfast A 38 (53) 32 (41) 17 (41) 15 (27) 102 (43) Birmingham B 101 (58) 100 (48) 98 (52) 50 (60) 349 (54) Bristol C 60 (50) 58 (57) 44 (50) 35 (54) 197 (53) Cambridge D 23 (39) 32 (25) 19 (37) 14 (29) 88 (32) Cardiff E 16 (31) 23 (43) 24 (38) 11 (36) 74 (38) Coventry F 24 (50) 23 (35) 12 (42) 10 (30) 69 (41) Edinburgh G 29 (55) 26 (46) 39 (49) 8 (38) 102 (49) Glasgow H 41 (27) 44 (39) 57 (46) 31 (52) 173 (40) Guy's J 24 (58) 37 (46) 51 (43) 24 (42) 136 (46) Leeds K 25 (32) 32 (19) 39 (23) 17 (18) 113 (23) Leicester L 113 (72) 101 (68) 40 (53) 23 (35) 277 (65) Liverpool M 27 (44) 34 (59) 40 (55) 10 (20) 111 (50) Manchester N 85 (28) 83 (41) 59 (34) 32 (50) 259 (36) Newcastle O 17 (41) 23 (65) 32 (44) 14 (43) 86 (49) Nottingham P 38 (68) 28 (57) 27 (48) 17 (53) 110 (58) Oxford Q 31 (39) 24 (38) 27 (26) 19 (37) 101 (35) Plymouth R 19 (47) 18 (33) 16 (25) 7 (43) 60 (37) Portsmouth S 21 (38) 37 (43) 20 (35) 23 (17) 101 (35) Sheffield T 33 (42) 37 (43) 32 (47) 9 (56) 111 (45) St George s U 52 (40) 48 (27) 50 (40) 21 (48) 171 (37) The Royal Free V 27 (26) 52 (40) 32 (28) 13 (23) 124 (32) The Royal London W 48 (31) 58 (36) 56 (43) 25 (20) 187 (35) WLRTC X 67 (49) 78 (51) 55 (51) 37 (65) 237 (53) UK 959 (47) 1028 (46) 886 (43) 465 (43) 3338 (45)
19 4.2 Extended criteria offer decline rates, 1 April September 2016 Figure 4.2 compares individual centre offer decline rates with the national rate for ECD over the time period, 1 April 2013 and 30 September Centres can be identified by the information shown in Table 4.2. Birmingham, Leicester, Cardiff, Sheffield and The Royal London have offer decline rates consistently higher than the national rate
20 Table 4.2 compares individual centre offer decline rates for ECD over time. Leicester has shown improvements in their ECD offer decline rates over time. Leicester s ECD offer decline rate has decreased from 82% in 2013/14 to 46% between 1 April and 30 September Between 1 April 2015 and 31 March 2016, Leicester now has an offer decline rate that is in line with the national rate. Table 4.2 Adult extended criteria DBD donor kidney offer decline rates by transplant centre, 1 April 2013 and 30 September 2016 Centre Code 2013/ / /16 1 Apr - 30 Sep Overall N (%) N (%) N (%) N (%) N (%) Belfast A 36 (58) 19 (42) 27 (44) 14 (64) 96 (52) Birmingham B 137 (80) 96 (72) 98 (53) 43 (70) 374 (70) Bristol C 63 (62) 45 (51) 89 (67) 38 (74) 235 (64) Cambridge D 21 (52) 32 (56) 24 (50) 7 (57) 84 (54) Cardiff E 24 (75) 12 (67) 21 (71) 16 (88) 73 (75) Coventry F 17 (41) 18 (67) 11 (55) 4 (50) 50 (54) Edinburgh G 31 (52) 28 (64) 32 (72) 13 (62) 104 (63) Glasgow H 31 (39) 37 (49) 59 (53) 39 (59) 166 (51) Guy's J 36 (56) 31 (48) 56 (46) 26 (62) 149 (52) Leeds K 18 (28) 28 (39) 29 (38) 15 (53) 90 (39) Leicester L 103 (82) 94 (81) 42 (62) 26 (46) 265 (75) Liverpool M 21 (33) 29 (69) 33 (64) 13 (69) 96 (59) Manchester N 77 (47) 64 (61) 106 (41) 43 (42) 290 (47) Newcastle O 21 (67) 19 (58) 29 (59) 17 (47) 86 (58) Nottingham P 39 (69) 18 (67) 24 (50) 14 (50) 95 (61) Oxford Q 18 (50) 17 (47) 37 (54) 11 (45) 83 (51) Plymouth R 15 (67) 11 (36) 12 (25) 6 (33) 44 (43) Portsmouth S 48 (42) 45 (36) 40 (58) 26 (50) 159 (45) Sheffield T 41 (61) 42 (67) 37 (68) 22 (77) 142 (67) St George s U 42 (38) 38 (45) 57 (60) 22 (50) 159 (49) The Royal Free V 23 (65) 24 (46) 37 (57) 18 (50) 102 (55) The Royal London W 56 (71) 46 (54) 57 (75) 34 (62) 193 (67) WLRTC X 85 (58) 74 (58) 94 (53) 44 (66) 297 (58) UK 1003 (61) 867 (59) 1051 (56) 511 (59) 3432 (59)
21 4.3 Reallocation of kidneys, 1 April September 2016 Since 3 April 2006 all kidneys from donation after brain death (DBD) donors have been allocated through the 2006 National Kidney Allocation Scheme (KAS). There are however certain situations when a kidney can be reallocated to an alternative patient of the centre s choice. This occurs when the kidney is accepted and dispatched to a named patient but is subsequently declined and there are no other patients listed nationally who fall within Tiers A to D of the kidney allocation scheme (000 mismatched adult and paediatric patients or favourably matched paediatric patients). In this situation the centre in receipt of the kidney can reallocate the organ to a locally listed patient of their choice based on an individual centre matching run. Funnel plots were used to compare centre specific reallocation rates and indicate how consistent the rates of the individual transplant centres are with the national rate. The overall national reallocation rate is shown by the solid line while the 95% and 99.8% confidence lines are indicated via a thin and thick dotted line, respectively. Each dot in the plot represents an individual transplant centre. Centres that are positioned above the upper limits indicate a reallocation rate that is higher than the national rate, while centres positioned below the lower limits indicates a reallocation rate that is lower than the national rate. Figure 4.3 compares individual centre reallocation rates with the national rate over the time period, 1 April 2013 to 30 September Centres can be identified by the information shown in Table 4.3. Nationally 5% of all DBD kidney only transplants used kidneys that had been reallocated. Leicester and the WLRTC have reallocation rates consistently higher than the national rate
22 Table 4.3 compares individual reallocation rates over time by financial year. Birmingham, Cardiff and St. George s have all shown improvements in their reallocation rates over time. Since , all centres have a reallocation rate that is in line with the national rate. Table 4.3 Local reallocation of DBD donor kidneys following an acceptance of an adult offer through the national allocation scheme Centre Code 2013/ / /16 1 Apr - 30 Sep Overall N (%) N (%) N (%) N (%) N (%) Belfast A 37 (8) 30 (0) 27 (7) 18 (0) 112 (4) Birmingham B 79 (10) 88 (8) 96 (1) 33 (0) 296 (5) Bristol C 61 (7) 50 (4) 55 (4) 26 (0) 192 (4) Cambridge D 41 (7) 50 (2) 29 (0) 20 (0) 140 (3) Cardiff E 31 (10) 20 (0) 28 (4) 12 (0) 91 (4) Coventry F 22 (0) 23 (9) 14 (7) 10 (0) 69 (4) Edinburgh G 33 (6) 32 (0) 39 (3) 11 (0) 115 (3) Glasgow H 58 (10) 53 (6) 62 (5) 31 (0) 204 (6) Guy's J 47 (4) 56 (4) 84 (1) 31 (3) 218 (3) Leeds K 52 (8) 62 (5) 73 (0) 39 (5) 226 (4) Leicester L 62 (11) 58 (16) 42 (7) 33 (3) 195 (10) Liverpool M 39 (8) 35 (11) 39 (8) 14 (7) 127 (9) Manchester N 111 (4) 91 (13) 108 (2) 48 (2) 358 (5) Newcastle O 27 (4) 20 (0) 35 (6) 20 (0) 102 (3) Nottingham P 30 (17) 27 (11) 30 (13) 16 (6) 103 (13) Oxford Q 34 (0) 41 (2) 50 (4) 22 (0) 147 (2) Plymouth R 18 (6) 22 (14) 22 (5) 8 (0) 70 (7) Portsmouth S 44 (5) 52 (4) 31 (3) 33 (3) 160 (4) Sheffield T 41 (10) 37 (5) 32 (9) 10 (10) 120 (8) St George s U 59 (2) 59 (0) 55 (2) 23 (4) 196 (2) The Royal Free V 37 (8) 68 (6) 49 (4) 26 (0) 180 (5) The Royal London W 58 (9) 65 (5) 57 (12) 34 (3) 214 (7) WLRTC X 80 (11) 82 (11) 77 (5) 31 (3) 270 (9) UK 1101 (7) 1121 (6) 1134 (4) 549 (2) 3905 (5)
23 5 Transplants Adult kidney transplants
 increased from 342 between 1 October 2011 and 31 March 2012 to 481 between 1 October 2015 and 31 March 16, before decreasing")
24 5.1 Kidney only transplants, 1 October September 2016 Figure 5.1 shows the total number of adult kidney only transplants performed in the last five years, by type of donor. The number of adult transplants from donors after circulatory death (DCD) increased from 342 between 1 October 2011 and 31 March 2012 to 481 between 1 October 2015 and 31 March 16, before decreasing by 10% to 433 between 1 April 2016 and 30 September The number of transplants from donors after brain death (DBD) increased from 452 between 1 October 2011 and 31 March 2012 to 584 between 01 October 2015 and 31 March 2016 before decreasing by 6% to 549 between 01 April 2016 and 30 September The number of adult living kidney transplants performed reached a high of 538 between 1 October 2013 and 31 March 2014 before decreasing by 15% to 459 between 1 April 2016 and 30 September

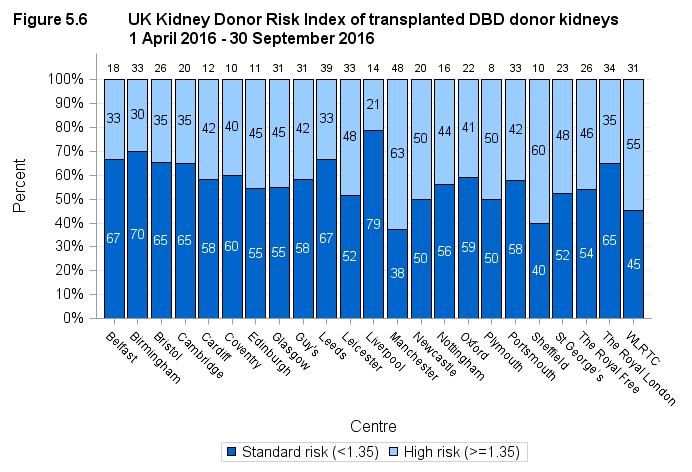
25 Figure 5.2 shows the total number of adult kidney only transplants performed between 1 April 2016 and 30 September 2016, by centre and type of donor. The same information is presented in Figure 5.3 but this shows the proportion of DBD, DCD and living donor transplants performed at each centre
26 5.2 Kidney donor risk-index 1, 1 April September 2016 The severe shortage of deceased donor (DD) organs available for transplantation has led to increased use of kidneys from suboptimal donors with potentially less good transplant outcome. Categorising such kidneys according to anticipated outcome is important because it enables clinicians to be better informed when making decisions about organ allocation and allows appropriate counselling of potential recipients. Kidneys from suboptimal donors are variously referred to as marginal, extended criteria, or expanded criteria organs. Although categorising DD kidneys as either standard or expanded criteria has the advantage of simplicity, it does not adequately reflect the wide spectrum of donor kidney quality, and this has led to the development of more refined approaches to assessing the quality of DD kidneys. A donor risk index was developed by determining the factors that influence transplant survival, the time from transplant to the earlier of graft failure or patient death. A UK donor risk index was derived from the parameter estimates of the donor factors in the Cox model developed for overall transplant survival. This gives the following index: UKKDRI = exp{ x (donor age <40) x (donor age 60) x (history of hypertension) x [donor weight(kg)-75]/10) x (days in hospital) x (adrenaline)} Reference 1 Watson CJE, Johnson RJ, Birch R, Collett D, Bradley JA. A simplified donor risk index for predicting outcome after deceased donor kidney transplantation. Transplantation, 2012; 93:

27 Figure 5.4 shows the number of transplanted DBD donor kidneys over the last five years by kidney donor risk index group. Between 1 October 2011 and 31 March 2012, 35% of all transplants were performed using kidneys from donors categorised as high risk (UK Donor risk index 1.35) compared with 43% between 1 April and 30 September Figure 5.5 shows the number of transplanted DBD donor kidneys between 1 April 2016 and 30 September 2016 by kidney donor risk index group for each transplant centre. The same information is presented in Figure 5.6 but this shows the proportion of standard risk and high risk donor transplants performed at each centre
28 - 25 -
29 5.3 Cold ischaemia time, 1 October September 2016 The length of time that elapses between a kidney being removed from the donor to its transplantation into the recipient is called the Cold Ischaemia Time (CIT). Generally, the shorter this time, the more likely the kidney is to work immediately and the better the longterm outcome. One of the reasons why live donor kidney transplantation is so successful is because the CIT is only one to two hours long. For deceased donor renal transplants, CIT can never be as short as this, but efforts are made to keep the time to a minimum. Evidence indicates that the outcome is only adversely affected when CIT is longer than 20 hours, although many deceased donor kidney transplants with a CIT of more than 20 hours have been very successful. The factors which determine CIT include a) transportation of the kidney from the retrieval hospital to the hospital where the transplant is performed, b) the need to tissue type the donor and cross-match the donor and potential recipients, c) the occasional necessity of moving the kidney to another hospital if a transplant cannot go ahead, d) contacting and preparing the recipient for the transplant and e) access to the operating theatre. Median CITs are shown in addition to inter-quartile ranges. Fifty percent of the transplants have a CIT within the inter-quartile range. There is some variation in average (median) CIT between different transplant centres although all centres continually try to reduce this time
30 Figure 5.7 shows the median total ischaemia time in adult DBD donor kidney only transplants over the last 5 years. The median total ischaemia time has decreased from 15 hours between 1 October 2011 and 31 March 2012 to 13 hours between 1 April 2016 and 30 September Figure 5.8 shows the median total ischaemia time in adult DBD donor kidney only transplants between 1 April 2016 and 30 September 2016 for each transplant centre. Sheffield had the longest median cold ischaemia time, 18 hours between 1 April and 30 September 2016 compared with St. George s who had the shortest, 9 hours
31 Figure 5.9 shows the median total ischaemia time in adult DCD donor kidney only transplants over the last 5 years. The median total ischaemia time has fallen over the last 5 years from 14 hours between 1 October 2011 and 31 March 2012 to 13 hours between 1 April 2016 and 30 September Figure 5.10 shows the median total ischaemia time in adult DCD donor kidney only transplants between 1 April 2016 and 30 September 2016 for each transplant centre. Plymouth had the longest median cold ischaemia time, 16 hours between April and September 2016 compared with Belfast who had the shortest, 8 hours
32 Figure 5.11 shows the median total ischaemia time in adult living donor kidney transplants over the last 5 years. The median total ischaemia time has remained stable over the last five years. Figure 5.12 shows the median total ischaemia time in adult living donor kidney transplants between 1 April 16 and 30 September 16 for each transplant centre
33 6 Kidney outcomes Adult kidney outcomes
34 We present a visual comparison of survival rates among centres that is based on a graphical display known as a funnel plot (1, 2). This display is used to show how consistent the rates of the different transplant units are with the national rate. Funnel plots show the risk-adjusted survival rate plotted against the number of transplants for each centre, with the overall national unadjusted survival rate (solid line), and its 95% (thin dotted lines) and 99.8% (thick dotted lines) confidence limits superimposed. Each dot in the plot represents one of the centres. Note that many patients return to local renal units for follow-up care after their transplant and although we report survival according to transplant unit, patients may in fact be followed up quite distantly from their transplant centre. Interpreting the funnel plots If a centre lies within all the limits, then that centre has a survival rate that is statistically consistent with the national rate. If a centre lies outside the 95% confidence limits, this serves as an alert that the centre may have a rate that is significantly different from the national rate. If a centre lies outside the 99.8% limits, then further investigations may be carried out to determine the reasons for the possible difference. When a centre lies above the upper limits, this indicates a survival rate that is higher than the national rate, while a centre that lies below the lower limits has a survival rate that is lower than the national rate. It is important to note that adjusting for patient mix through the use of risk-adjustment models may not account for all possible causes of centre differences. There may be other factors that are not taken into account in the risk-adjustment process that may affect the survival rate of a particular centre. References 1. Tekkis PP, McCulloch P, Steger AC, Benjamin IS, Poloniecki JD. Mortality control charts for comparing performance of surgical units: validation study using hospital mortality data. British Medical Journal 2003; 326: Stark J, Gallivan S, Lovegrove J, Hamilton JRL, Monro JL, Pollock JCS, Watterson KG. Mortality rates after surgery for congenital heart defects in children and surgeons performance. Lancet 2000; 355:
35 6.1 Deceased donor graft and patient survival The funnel plots show that, for the most part, the centres lie within the confidence limits. Some of the funnel plots show some centres to be above the upper 99.8% confidence limit. This suggests that these centres may have survival rates that are considerably higher than the national rate. Centres can be identified by the information shown in Table
36 - 33 -
37 Table 6.1 One and five year first adult kidney-only graft and patient survival using kidneys from deceased donors Kidney graft survival Patient survival One-year* Five-year** One-year* Five-year** Centre Code % (95% CI) % (95% CI) % (95% CI) % (95% CI) Belfast A 97 (93-99) 89 (79-95) 95 (90-98) 87 (76-94) Birmingham B 94 (91-96) 83 (77-88) 97 (95-99) 92 (87-96) Bristol C 97 (93-99) 85 (78-90) 95 (91-98) 88 (82-92) Cambridge D 96 (93-98) 88 (84-91) 97 (94-98) 88 (84-92) Cardiff E 96 (93-98) 90 (85-94) 95 (92-97) 89 (84-93) Coventry F 91 (81-96) 81 (68-90) 95 (87-99) 88 (77-95) Edinburgh G 96 (91-99) 84 (77-89) 98 ( (82-93) Glasgow H 92 (88-95) 93 (88-96) 95 (92-98) 92 (87-96) Guy's J 93 (90-95) 88 (82-92) 97 (95-99) 89 (84-94) Leeds K 94 (91-96) 84 (79-88) 97 (95-99) 85 (80-89) Leicester L 93 (89-96) 89 (82-94) 98 ( (81-93) Liverpool M 93 (88-96) 87 (81-92) 94 (90-97) 81 (74-87) Manchester N 97 (95-99) 88 (83-91) 95 (93-97) 92 (88-95) Newcastle O 95 (91-97) 83 (76-88) 96 (92-98) 86 (79-90) Nottingham P 95 (91-98) 88 (80-93) 98 ( (77-90) Oxford Q 95 (92-97) 88 (82-92) 97 (94-99) 88 (83-92) Plymouth R 93 (86-97) 82 (74-88) 93 (87-97) 92 (86-95) Portsmouth S 91 (85-95) 82 (73-89) 95 (91-98) 85 (78-91) Sheffield T 94 (89-97) 87 (79-92) 96 (92-99) 92 (86-96) St George s U 93 (88-96) 89 (82-94) 97 (94-99) 95 (89-98) The Royal Free V 94 (90-96) 87 (82-92) 98 (96-99) 90 (84-93) The Royal London W 90 (84-93) 83 (77-88) 93 (88-97) 82 (75-88) WLRTC X 95 (92-97) 86 (81-90) 97 (95-99) 91 (87-94) UK 94 (94-95) 86 (85-87) 96 (96-97) 88 (87-89) * Includes transplants performed between 1 October September 2015 ** Includes transplants performed between 1 October September
38 6.2 Living donor graft and patient survival The funnel plots show that, for the most part, the centres lie within the confidence limits. Some of the funnel plots show some centres to be above the upper 99.8% confidence limit. This suggests that these centres may have survival rates that are considerably higher than the national rate. Centres can be identified by the information shown in Table
39 - 36 -
40 Table 6.2 One and five year first adult kidney-only graft and patient survival using kidneys from living donors Kidney graft survival Patient survival One-year* Five-year** One-year* Five-year** Centre Code % (95% CI) % (95% CI) % (95% CI) % (95% CI) Belfast A 97 (93-99) 94 (86-98) 100 N/A 93 (83-98) Birmingham B 97 (94-99) 93 (89-96) 99 ( (89-98) Bristol C 97 (92-99) 95 (90-98) 100 N/A 95 (89-98) Cambridge D 98 ( (91-99) 99 ( (88-98) Cardiff E 97 (91-99) 89 (81-94) 96 (89-99) 97 (91-99) Coventry F 99 ( (86-98) 100 N/A 95 (87-99) Edinburgh G 100 N/A 88 (78-94) 100 N/A 93 (84-98) Glasgow H 97 (92-99) 91 (83-96) 100 N/A 91 (80-97) Guy's J 98 (95-99) 95 (92-97) 98 ( (92-98) Leeds K 97 (92-99) 88 (81-93) 99 ( (89-98) Leicester L 98 ( (84-94) 97 (91-99) 94 (89-97) Liverpool M 97 (91-99) 88 (79-94) 98 ( (86-99) Manchester N 98 (95-99) 95 (91-98) 99 ( (87-96) Newcastle O 99 ( (88-97) 100 N/A 95 (89-98) Nottingham P 98 ( (79-96) 97 ( (82-99) Oxford Q 96 (92-99) 94 (89-97) 99 ( (88-97) Plymouth R 98 ( (76-96) 100 N/A 94 (84-99) Portsmouth S 100 N/A 94 (84-98) 99 ( (84-99) Sheffield T 99 ( ( N/A 98 ( St George s U 99 ( (89-97) 99 ( (90-97) The Royal Free V 99 ( (89-98) 100 N/A 96 (90-99) The Royal London W 97 (94-99) 87 (80-93) 99 ( (84-98) WLRTC X 97 (94-99) 90 (85-94) 99 ( (90-97) UK 98 (97-98) 93 (92-93) 99 (99-99) 95 (94-95) * Includes transplants performed between 1 October September 2015 ** Includes transplants performed between 1 October September
41 Appendix
42 A1 Glossary of terms ABO The most important human blood group system for transplantation is the ABO system. Every human being is of blood group O, A, B or AB, or of one of the minor variants of these four groups. ABO blood groups are present on other tissues and, unless special precautions are taken, a group A kidney transplanted to a group O patient will be rapidly rejected. Active transplant list When a patient is registered for a transplant, they are registered on what is called the active transplant list. This means that when a donor kidney becomes available, the patient is included among those who are matched against the donor to determine whether or not the kidney is suitable for them. It may sometimes be necessary to take a patient off the transplant list, either temporarily or permanently. This may be done, for example, if someone becomes too ill to receive a transplant. The patient is told about the decision to suspend them from the list and is informed whether the suspension is temporary or permanent. If a patient is suspended from the list, they are not included in the matching of any donor kidneys that become available. Case mix The types of patients treated at a unit for a common condition. This can vary across units depending on the facilities available at the unit as well as the types of people in the catchment area of the unit. The definition of what type of patient a person is depends on the patient characteristics that influence the outcome of the treatment. For example the case mix for patients registered for a kidney transplant is defined in terms of various factors such as the blood group, tissue type and age of the patient. These factors have an influence on the chance of a patient receiving a transplant. Confidence interval (CI) When an estimate of a quantity such as a survival rate is obtained from data, the value of the estimate depends on the set of patients whose data were used. If, by chance, data from a different set of patients had been used, the value of the estimate may have been different. There is therefore some uncertainty linked with any estimate. A confidence interval is a range of values whose width gives an indication of the uncertainty or precision of an estimate. The number of transplants or patients analysed influences the width of a confidence interval. Smaller data sets tend to lead to wider confidence intervals compared to larger data sets. Estimates from larger data sets are therefore more precise than those from smaller data sets. Confidence intervals are calculated with a stated probability, usually 95%. We then say that there is a 95% chance that the confidence interval includes the true value of the quantity we wish to estimate. Confidence limit The upper and lower bounds of a confidence interval. Cox Proportional Hazards model A statistical model that relates the instantaneous risk (hazard) of an event occurring at a given time point to the risk factors that influence the length of time it takes for the event to occur. This model can be used to compare the hazard of an event of interest, such as graft failure or patient death, across different groups of patients
43 Cross-match A cross-match is a test for patient antibodies against donor antigens. A positive crossmatch shows that the donor and patient are incompatible. A negative cross-match means there is no reaction between donor and patient and that the transplant may proceed. Donor after brain death (DBD) A donor whose heart is still beating when their entire brain has stopped working so that they cannot survive without the use of a ventilator. Organs for transplant are removed from the donor while their heart is still beating, but only after extensive tests determine that the brain cannot recover and they have been certified dead. Donor after circulatory death (DCD) A donor whose heart stops beating before their brain stops working and who is then certified dead. The organs are then removed. Funnel plot A graphical method that shows how consistent the survival rates of the different transplant units are compared to the national rate. The graph shows for each unit, a survival rate plotted against the number of transplants undertaken, with the national rate and confidence limits around this national rate superimposed. In this report, 95% and 99.8% confidence limits were used. Units that lie within the confidence limits have survival rates that are statistically consistent with the national rate. When a unit is close to or outside the limits, this is an indication that the centre may have a rate that is considerably different from the national rate. Graft survival rate The percentage of patients whose grafts are still functioning. This is usually specified for a given time period after transplant. For example, a five-year transplant survival rate is the percentage of transplants still functioning five years after transplant. HLA mismatch Human Leucocyte Antigen (HLA) antigens are carried on many cells in the body and the immune system can distinguish between those that can be recognised as self (belonging to you or identical to your own) and those that can be recognised as nonself. The normal response of the immune system is to attack foreign/non-self material by producing antibodies against the foreign material. This is one of the mechanisms that provide protection against infection. This is unfortunate from the point of view of transplantation as the immune system will see the graft as just another infection to be destroyed, produce antibodies against the graft and rejection of the grafted organ will take place. To help overcome this response, it is recognised that matching the recipient and donor on the basis of HLA (and blood group) reduces the chances of acute rejection and, with the added use of immunosuppressive drugs, very much improves the chances of graft survival. Matching refers to the similarity of the recipient HLA type and donor HLA type. HLA mismatch refers to the number of mismatches between the donor and the recipient at the A, B and DR (HLA) loci. There can only be a total of two mismatches at each locus. For example, an HLA mismatch value of 000, means that the donor and recipient are identical at all three loci, while an HLA mismatch value of 210 means that the donor and recipient differ completely at the A locus, are partly the same at the B locus and are identical at the DR locus
44 Inter-quartile range The values between which the middle 50% of the data fall. The lower boundary is the lower quartile, the upper boundary the upper quartile. Kaplan-Meier method A method that allows patients with incomplete follow-up information to be included in estimating survival rates. For example, in a cohort for estimating one year patient survival rates, a patient was followed up for only nine months before they relocated. If we calculated a crude survival estimate using the number of patients who survived for at least a year, this patient would have to be excluded as it is not known whether or not the patient was still alive at one year after transplant. The Kaplan-Meier method allows information about such patients to be used for the length of time that they are followed-up, when this information would otherwise be discarded. Such instances of incomplete follow-up are not uncommon and the Kaplan-Meier method allows the computation of estimates that are more meaningful in these cases. Live donor A donor who is a living person and who is usually, but not always, a relative of the transplant patient. For example, a parent may donate one of their kidneys to their child. Median The midpoint in a series of numbers, so that half the data values are larger than the median, and half are smaller. Multi-organ transplant A transplant in which the patient receives more than one organ. For example, a patient may undergo a transplant of a kidney and liver. National Kidney Allocation Scheme A nationally agreed set of rules for sharing and allocating kidneys for transplant between transplant centres in the UK. The scheme is administered by NHS Blood and Transplant. Patient survival rate The percentage of patients who are still alive (whether the graft is still functioning or not). This is usually specified for a given time period after transplant. For example, a five-year patient survival rate is the percentage of patients who are still alive five years after their first transplant. p value In the context of comparing survival rates across centres, the p value is the probability that the differences observed in the rates across centres occurred by chance. As this is a probability, it takes values between 0 and 1. If the p value is small, say less than 0.05, this implies that the differences are unlikely to be due to chance and there may be some identifiable cause for these differences. If the p value is large, say greater than 0.1, then it is quite likely that any differences seen are due to chance. Pre-emptive Patients that are placed on the kidney transplant list or receive a transplant prior to the need for dialysis are termed as pre-emptive. Patients listed pre-emptively will usually require dialysis within six months of being placed on the transplant list
45 Risk-adjusted survival rate Some transplants have a higher chance than others of failing at any given time. The differences in expected survival times arise due to differences in certain factors, the risk factors, among patients. A risk-adjusted survival rate for a centre is the expected survival rate for that centre given the case mix of their patients. Adjusting for case mix in estimating centre-specific survival rates allows valid comparison of these rates across centres and to the national rate. Risk factors These are the characteristics of a patient, transplant or donor that influence the length of time that a graft is likely to function or a patient is likely to survive following a transplant. For example, when all else is equal, a transplant from a younger donor is expected to survive longer than that from an older donor and so donor age is a risk factor. Unadjusted survival rate Unadjusted survival rates do not take account of risk factors and are based only on the number of transplants at a given centre and the number and timing of those that fail within the post-transplant period of interest. In this case, unlike for risk-adjusted rates, all transplants are assumed to be equally likely to fail at any given time. However, some centres may have lower unadjusted survival rates than others simply because they tend to undertake transplants that have increased risks of failure. Comparison of unadjusted survival rates across centres and to the national rate is therefore inappropriate
46 A2 Statistical methodology and risk-adjustment for survival rate estimation Unadjusted and risk-adjusted estimates of patient and graft survival are given for each centre. Unadjusted rates give an estimate of what the survival rate at a centre is, assuming that all patients at the centre have the same chance of surviving a given length of time after transplant. In reality, patients differ and a risk-adjusted rate that allows for these differences would give a more meaningful estimate of survival. Computing unadjusted survival rates Unadjusted survival rates were calculated using the Kaplan-Meier method, which allows patients with incomplete follow-up information to be included in the computation. For example, in a cohort for estimating one-year patient survival rates, a patient was followed up for only nine months before they relocated. If we calculated a crude survival estimate using the number of patients who survived for at least a year, this patient would have to be excluded, as it is not known whether or not the patient was still alive one year after transplant. The Kaplan-Meier method allows information about such patients to be used for the length of time that they are followed-up, when this information would otherwise be discarded. Such instances of incomplete follow-up are not uncommon in the analysis of survival data and the Kaplan-Meier method therefore allows the computation of survival estimates that are more meaningful. Computing risk-adjusted survival rates A risk-adjusted survival rate is an estimate of what the survival rate at a centre would have been if they had had the same mix of patients as that seen nationally. The risk-adjusted rate therefore presents estimates in which differences in patient mix across centres have been removed as much as possible. For that reason, it is valid to only compare centres using risk-adjusted rather than unadjusted rates, as differences among the latter can be attributed to differences in patient mix. Risk-adjusted survival estimates were obtained through indirect standardisation. A Cox Proportional Hazards model was used to determine the probability of survival for each patient based on their individual risk factor values. The sum of these probabilities for all patients at a centre gives the number, E, of patients or grafts expected to survive at least one year or five years after transplant at that centre. The number of patients who actually survive the given time period is given by O. The risk-adjusted estimate is then calculated by multiplying the ratio O/E by the overall unadjusted survival rate across all centres. The risk-adjustment models used were based on results from previous studies that looked at factors affecting the survival rates of interest. The factors included in the models are shown in the table below
47 Risk adjustment factors Adult patient transplants First transplants from deceased donors 1 year graft survival Donor age, donor type, donor cause of death, recipient age, waiting time to transplant, primary renal disease, HLA mismatch group, cold ischaemic time*, recipient ethnicity 1 year patient survival Donor age, recipient age, waiting time to transplant, primary renal disease, HLA mismatch group, cold ischaemic time* 5 year graft survival Graft year, donor age, donor type, donor cause of death, recipient age, waiting time to transplant, primary renal disease, HLA mismatch group, recipient ethnicity 5 year patient survival Graft year, donor age, recipient age, waiting time to transplant, primary renal disease Transplants from live donors 1 year graft survival Donor age, recipient age, primary renal disease, number of HLA mismatches 1 year patient survival Recipient age 5 year graft survival Graft year, donor age, recipient age, primary renal disease, number of HLA mismatches 5 year patient survival Recipient age, primary renal disease *Time between retrieval of kidney from the donor and time of transplant in the patient
48 Prepared by: Statistics and Clinical Studies, NHS Blood and Transplant Miss Chloe Brown and Ms Lisa Mumford
The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
NHS BLOOD AND TRANSPLANT KIDNEY OFFERING SCHEME WORKING GROUP ENDORSEMENT OF A NEW NATIONAL KIDNEY OFFERING SCHEME
 NHS BLOOD AND TRANSPLANT KIDNEY OFFERING SCHEME WORKING GROUP ENDORSEMENT OF A NEW NATIONAL KIDNEY OFFERING SCHEME INTRODUCTION 1 Three working groups were established to consider whether changes were
NHS BLOOD AND TRANSPLANT KIDNEY OFFERING SCHEME WORKING GROUP ENDORSEMENT OF A NEW NATIONAL KIDNEY OFFERING SCHEME INTRODUCTION 1 Three working groups were established to consider whether changes were
Summary of Significant Changes. Policy
 This Policy replaces POL186/2 Copy Number Effective 01/04/14 Summary of Significant Changes Clarification of policy approval process Paragraph 2.2.1 Clarification of Kidney Fast Track Scheme offering criteria
This Policy replaces POL186/2 Copy Number Effective 01/04/14 Summary of Significant Changes Clarification of policy approval process Paragraph 2.2.1 Clarification of Kidney Fast Track Scheme offering criteria
The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015
 6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015 The number of pancreas donors after
6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 7% during the year, to 252 at 31 March 2015 The number of pancreas donors after
The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017
 6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017 The number of pancreas donors after
6 Pancreas Activity Pancreas Activity Key messages The number of patients waiting on the pancreas transplant list fell by 1% during the year, to 224 at 31 March 2017 The number of pancreas donors after
ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION
 ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION REPORT FOR 2014/2015 (1 APRIL 2005 31 MARCH 2015) PUBLISHED SEPTEMBER 2015 PRODUCED IN COLLABORATION WITH NHS ENGLAND - 1 - Contents 1 Executive Summary...
ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION REPORT FOR 2014/2015 (1 APRIL 2005 31 MARCH 2015) PUBLISHED SEPTEMBER 2015 PRODUCED IN COLLABORATION WITH NHS ENGLAND - 1 - Contents 1 Executive Summary...
Transplant Activity in the UK
 Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
Transplant Activity in the UK 2006-2007 This document has been produced by the Statistics and Audit Directorate. UK Transplant August 2007 Cover pictures: Members of Glamorgan County cricket team help
TRANSPLANT ACTIVITY IN THE UK
 Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
Activity Report 2010/11 TRANSPLANT ACTIVITY IN THE UK www.nhsbt.nhs.uk PREFACE This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report
United Kingdom Transplant Activity UK Transplant. Every statisticisaperson.
 United Kingdom Transplant Activity 2001 UK Transplant Every statisticisaperson. Cover photograph: Caroline and John Fowler s daughter Aimee, now aged two, shared a donated liver in the first operation
United Kingdom Transplant Activity 2001 UK Transplant Every statisticisaperson. Cover photograph: Caroline and John Fowler s daughter Aimee, now aged two, shared a donated liver in the first operation
This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant.
 Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 20 May 2013 for the UK
Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 20 May 2013 for the UK
The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016
 8 Liver Activity Liver Activity Key messages The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016 The number of liver donors after brain death increased
8 Liver Activity Liver Activity Key messages The number of patients on the active liver transplant list at 31 March 2017 was 530, a fall of 8% from 2016 The number of liver donors after brain death increased
This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant.
 Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 17 June 2012 for the UK
Preface This report has been produced by Statistics and Clinical Audit, NHS Blood and Transplant. All figures quoted in this report are as reported to NHS Blood and Transplant by 17 June 2012 for the UK
ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION
 ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION REPORT FOR 2016/2017 (1 APRIL 2007 31 MARCH 2017) PUBLISHED JULY 2017 PRODUCED IN COLLABORATION WITH NHS ENGLAND - 1 - Contents 1 Executive Summary...
ANNUAL REPORT ON PANCREAS AND ISLET TRANSPLANTATION REPORT FOR 2016/2017 (1 APRIL 2007 31 MARCH 2017) PUBLISHED JULY 2017 PRODUCED IN COLLABORATION WITH NHS ENGLAND - 1 - Contents 1 Executive Summary...
NHS BLOOD AND TRANSPLANT LIVER ADVISORY GROUP WAITING TIMES AND DEATHS ON THE LIST BY BLOOD GROUP SUMMARY
 NHS BLOOD AND TRANSPLANT LIVER ADVISORY GROUP WAITING TIMES AND DEATHS ON THE LIST BY BLOOD GROUP BACKGROUND SUMMARY 1 Restrictions in the allocation of livers were introduced in 2006 to reverse the increasingly
NHS BLOOD AND TRANSPLANT LIVER ADVISORY GROUP WAITING TIMES AND DEATHS ON THE LIST BY BLOOD GROUP BACKGROUND SUMMARY 1 Restrictions in the allocation of livers were introduced in 2006 to reverse the increasingly
Manchester Royal Infirmary Renal & Pancreas Transplant Unit / 2011 Activity Annual Report
 Manchester Royal Infirmary Renal & Pancreas Transplant Unit 21 / 211 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
Manchester Royal Infirmary Renal & Pancreas Transplant Unit 21 / 211 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
UK Liver Transplant Audit
 November 2012 UK Liver Transplant Audit In patients who received a Liver Transplant between 1 st March 1994 and 31 st March 2012 ANNUAL REPORT Advisory Group for National Specialised Services Prepared
November 2012 UK Liver Transplant Audit In patients who received a Liver Transplant between 1 st March 1994 and 31 st March 2012 ANNUAL REPORT Advisory Group for National Specialised Services Prepared
Manchester Royal Infirmary Renal & Pancreas Transplant Unit / 2012 Activity Annual Report
 Manchester Royal Infirmary Renal & Pancreas Transplant Unit 211 / 212 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
Manchester Royal Infirmary Renal & Pancreas Transplant Unit 211 / 212 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE FOURTH MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 28 APRIL 2010 IN MEETING
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE FOURTH MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 28 APRIL 2010 IN MEETING
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE FIRST MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 22 OCTOBER 2008 IN CONFERENCE
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE FIRST MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 22 OCTOBER 2008 IN CONFERENCE
. Time to transplant listing is dependent on. . In 2003, 9.1% of all prevalent transplant. . Patients with diabetes mellitus are less
 Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
New Zealand Kidney Allocation Scheme
 New Zealand Kidney Allocation Scheme The New Zealand Kidney Allocation Scheme (NZKAS) has been developed to ensure that kidney allocation in NZ is performed on an equitable, accountable and transparent
New Zealand Kidney Allocation Scheme The New Zealand Kidney Allocation Scheme (NZKAS) has been developed to ensure that kidney allocation in NZ is performed on an equitable, accountable and transparent
U.S. changes in Kidney Allocation
 U.S. changes in Kidney Allocation Match kidneys with longest survival to patients with longest survival No parallel matching for kidneys with lower survival potential Decrease discard of kidneys with lower
U.S. changes in Kidney Allocation Match kidneys with longest survival to patients with longest survival No parallel matching for kidneys with lower survival potential Decrease discard of kidneys with lower
Manchester Royal Infirmary Renal & Pancreas Transplant Unit / 2010 Activity Annual Report
 Manchester Royal Infirmary Renal & Pancreas Transplant Unit 29 / 21 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
Manchester Royal Infirmary Renal & Pancreas Transplant Unit 29 / 21 Activity Annual Report Vicki Bowman Renal Transplant Audit & Data Manager Dr Susan Martin Consultant Clinical Scientist / Transplantation
PARTICULARS, SCHEDULE 2 THE SERVICES, A SERVICE SPECIFICATION. A03/S(HSS)/a Pancreas transplantation service (Adult)
/a Pancreas transplantation service (Adult)") A03/S(HSS)/a NHS STANDARD CONTRACT FOR PANCREAS TRANSPLANTATION SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A SERVICE SPECIFICATION Service Specification No. Service Commissioner Lead Provider
A03/S(HSS)/a NHS STANDARD CONTRACT FOR PANCREAS TRANSPLANTATION SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A SERVICE SPECIFICATION Service Specification No. Service Commissioner Lead Provider
Paired Donation. Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle. Cambridge University NHS Hospitals NHS Foundation trust
 Paired Donation Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle Cambridge University NHS Hospitals NHS Foundation trust Showing a preference 1860 John Calcott Horsley UK Living Donor kidney transplant
Paired Donation Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle Cambridge University NHS Hospitals NHS Foundation trust Showing a preference 1860 John Calcott Horsley UK Living Donor kidney transplant
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE THIRD MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON TUESDAY, 24 NOVEMBER 2009 IN CONFERENCE
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE THIRD MEETING OF THE PAEDIATRIC SUB-GROUP OF THE KIDNEY ADVISORY GROUP HELD ON TUESDAY, 24 NOVEMBER 2009 IN CONFERENCE
Organ Donation and Transplantation. Activity Report 2017/18
 Organ Donation and Transplantation Activity Report 2017/18 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation Activity Report 2017/18 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2017/2018 (1 April March 2018)
 communities. Report for 2017/2018 (1 April March 2018)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 07/0 ( April 0 March 0) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 07/0 ( April 0 March 0) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
NHS BLOOD AND TRANSPLANT CARDIOTHORACIC ADVISORY GROUP URGENT HEART ALLOCATION SCHEMES 2015/2016 ACTIVITY SUMMARY
 INTRODUCTION NHS BLOOD AND TRANSPLANT CARDIOTHORACIC ADVISORY GROUP URGENT HEART ALLOCATION SCHEMES 2015/2016 ACTIVITY SUMMARY 1 This paper is a review of the usage of the Adult Urgent Heart Allocation
INTRODUCTION NHS BLOOD AND TRANSPLANT CARDIOTHORACIC ADVISORY GROUP URGENT HEART ALLOCATION SCHEMES 2015/2016 ACTIVITY SUMMARY 1 This paper is a review of the usage of the Adult Urgent Heart Allocation
Summary of Significant Changes. Policy. Purpose
 This Policy replaces POL196/4.1 Copy Number Effective 20/03/2018 Summary of Significant Changes Policy rewritten to reflect the new liver offering scheme Clarification of combined liver and kidney patient
This Policy replaces POL196/4.1 Copy Number Effective 20/03/2018 Summary of Significant Changes Policy rewritten to reflect the new liver offering scheme Clarification of combined liver and kidney patient
Summary of Significant Changes. Policy
 This Policy replaces POL193/6 Copy Number Effective 13/05/16 Summary of Significant Changes Para 1.3.1.6 - Amendment to donor and recipient age match points to reflect the fact that paediatric recipients
This Policy replaces POL193/6 Copy Number Effective 13/05/16 Summary of Significant Changes Para 1.3.1.6 - Amendment to donor and recipient age match points to reflect the fact that paediatric recipients
Therapeutic Apheresis Services Annual Review 2016/17
 Therapeutic Apheresis Services Annual Review 2016/17 NHS Blood and Transplant (NHSBT) is a major provider of Therapeutic Apheresis Services (TAS) in the NHS. Services are provided across England. Collection
Therapeutic Apheresis Services Annual Review 2016/17 NHS Blood and Transplant (NHSBT) is a major provider of Therapeutic Apheresis Services (TAS) in the NHS. Services are provided across England. Collection
Organ Donation and Transplantation. Activity Report 2015/16
 Organ Donation and Transplantation Activity Report 2015/16 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation Activity Report 2015/16 Preface This report has been produced by Statistics and Clinical Studies, NHS Blood and Transplant. All figures quoted in this report are as reported
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2015/2016 (1 April March 2016)
 communities. Report for 2015/2016 (1 April March 2016)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 2015/2016 (1 April 2010 31 March 2016) INTRODUCTION This report provides information related to
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 2015/2016 (1 April 2010 31 March 2016) INTRODUCTION This report provides information related to
Renal Transplant Registry Report 2008
 Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
NHSBT Board July Update on UK Living Kidney Sharing Scheme
 1. Status Public 2. Executive Summary NHSBT Board July 27 2017 Update on UK Living Kidney Sharing Scheme This paper provides an update on activity and plans for the UK Living Kidney Sharing Scheme (UKLKSS),
1. Status Public 2. Executive Summary NHSBT Board July 27 2017 Update on UK Living Kidney Sharing Scheme This paper provides an update on activity and plans for the UK Living Kidney Sharing Scheme (UKLKSS),
Consent and donor choice in lung and heart-lung transplantation
 Consent and donor choice in lung and heart-lung transplantation A patient s guide 1 Lung transplantation is a good option for carefully selected patients with end stage lung disease but sadly there is
Consent and donor choice in lung and heart-lung transplantation A patient s guide 1 Lung transplantation is a good option for carefully selected patients with end stage lung disease but sadly there is
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities. Report for 2016/2017 (1 April March 2017)
 communities. Report for 2016/2017 (1 April March 2017)") Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 6/7 ( April March 7) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Organ Donation and Transplantation data for Black, Asian and Minority Ethnic (BAME) communities Report for 6/7 ( April March 7) CONTENTS EXECUTIVE SUMMARY... INTRODUCTION... ORGAN DONOR REGISTER (ODR)...
Transplant First: Addressing inequality in access to Kidney Transplantation in the West Midlands
 Project Mandate Transplant First: Addressing inequality in access to Kidney Transplantation in the West Midlands West Midlands Cardiovascular Strategic Clinical Network Project Mandate Transplant First:
Project Mandate Transplant First: Addressing inequality in access to Kidney Transplantation in the West Midlands West Midlands Cardiovascular Strategic Clinical Network Project Mandate Transplant First:
The New Kidney Allocation System (KAS) Frequently Asked Questions
 Frequently Asked Questions") The New Kidney Allocation System (KAS) Frequently Asked Questions Contents General: The Need for the New System and Key Implementation Details... 4 Why was the newly revised KAS necessary?... 4 What were
The New Kidney Allocation System (KAS) Frequently Asked Questions Contents General: The Need for the New System and Key Implementation Details... 4 Why was the newly revised KAS necessary?... 4 What were
Current status of kidney and pancreas transplantation in the United States,
 American Journal of Transplantation 25; 5 (Part 2): 94 915 Blackwell Munksgaard Blackwell Munksgaard 25 Current status of kidney and pancreas transplantation in the United States, 1994 23 Gabriel M. Danovitch
American Journal of Transplantation 25; 5 (Part 2): 94 915 Blackwell Munksgaard Blackwell Munksgaard 25 Current status of kidney and pancreas transplantation in the United States, 1994 23 Gabriel M. Danovitch
NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE PANCREAS ADVISORY GROUP AUDIT OF STANDARD CRITERIA FOR LISTING SUMMARY
 INTRODUCTION NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE PANCREAS ADVISORY GROUP AUDIT OF STANDARD CRITERIA FOR LISTING SUMMARY 1 Selection criteria for patients onto the national
INTRODUCTION NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE PANCREAS ADVISORY GROUP AUDIT OF STANDARD CRITERIA FOR LISTING SUMMARY 1 Selection criteria for patients onto the national
NHS BLOOD AND TRANSPLANT MINUTES OF THE THIRTIETH MEETING OF THE KIDNEY ADVISORY GROUP HELD AT A.M. ON MONDAY 5 TH DECEMBER 2016 AT ODT, BRISTOL
 NHS BLOOD AND TRANSPLANT MINUTES OF THE THIRTIETH MEETING OF THE KIDNEY ADVISORY GROUP HELD AT 10.30 A.M. ON MONDAY 5 TH DECEMBER 2016 AT ODT, BRISTOL PRESENT: Prof Chris Watson Ms Lorna Marson Mr John
NHS BLOOD AND TRANSPLANT MINUTES OF THE THIRTIETH MEETING OF THE KIDNEY ADVISORY GROUP HELD AT 10.30 A.M. ON MONDAY 5 TH DECEMBER 2016 AT ODT, BRISTOL PRESENT: Prof Chris Watson Ms Lorna Marson Mr John
Renal Transplantation: Allocation challenges and changes. Renal Transplantation. The Numbers 1/13/2014
 Renal Transplantation: Allocation challenges and changes Mark R. Wakefield, M.D., F.A.C.S. Associate Professor of Surgery/Urology Director Renal Transplantation Renal Transplantation Objectives: Understand
Renal Transplantation: Allocation challenges and changes Mark R. Wakefield, M.D., F.A.C.S. Associate Professor of Surgery/Urology Director Renal Transplantation Renal Transplantation Objectives: Understand
Social deprivation, ethnicity and access to kidney transplantation in England and Wales. Udaya Udayaraj
 Social deprivation, ethnicity and access to kidney transplantation in England and Wales Udaya Udayaraj Introduction (1) Kidney transplantation Improved survival compared to remaining on dialysis Better
Social deprivation, ethnicity and access to kidney transplantation in England and Wales Udaya Udayaraj Introduction (1) Kidney transplantation Improved survival compared to remaining on dialysis Better
UEMS & EBS: DIVISION OF TRANSPLANT SURGERY
 CURRICULUM AND SYLLABUS TRANSPLANTATION Module 1: Multi-organ retrieval Ability to evaluate donor suitability Ability to retrieve abdominal organs for transplantation Evaluation of donor/ organs suitability
CURRICULUM AND SYLLABUS TRANSPLANTATION Module 1: Multi-organ retrieval Ability to evaluate donor suitability Ability to retrieve abdominal organs for transplantation Evaluation of donor/ organs suitability
NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE MINUTES OF THE FOURTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 26 NOVEMBER 2008 IN CONFERENCE SUITE 2, ODT, BRISTOL
NHS BLOOD AND TRANSPLANT ORGAN DONATION AND TRANSPLANTATION DIRECTORATE MINUTES OF THE FOURTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 26 NOVEMBER 2008 IN CONFERENCE SUITE 2, ODT, BRISTOL
Rishi Pruthi a, Rachel Hilton b, Laura Pankhurst c, Nizam Mamode b, Alex Hudson c, Paul Roderick d, Rommel Ravanan e
 UK Renal Registry 16th Annual Report: Chapter 4 Demography of Patients Waitlisted for Renal Transplantation in the UK: National and Centre-specific Analyses Rishi Pruthi a, Rachel Hilton b, Laura Pankhurst
UK Renal Registry 16th Annual Report: Chapter 4 Demography of Patients Waitlisted for Renal Transplantation in the UK: National and Centre-specific Analyses Rishi Pruthi a, Rachel Hilton b, Laura Pankhurst
Chronic renal histological changes at implantation and subsequent deceased donor kidney transplant outcomes: a single-centre analysis
 Chronic renal histological changes at implantation and subsequent deceased donor kidney transplant outcomes: a single-centre analysis Benedict Phillips 1, Kerem Atalar 1, Hannah Wilkinson 1, Nicos Kessaris
Chronic renal histological changes at implantation and subsequent deceased donor kidney transplant outcomes: a single-centre analysis Benedict Phillips 1, Kerem Atalar 1, Hannah Wilkinson 1, Nicos Kessaris
Oxford Transplant Centre. Live donor kidney transplantation what if we are not a match?
 Oxford Transplant Centre Live donor kidney transplantation what if we are not a match? page 2 You will already have been provided with information about different types of kidney transplant and the tests
Oxford Transplant Centre Live donor kidney transplantation what if we are not a match? page 2 You will already have been provided with information about different types of kidney transplant and the tests
Summary of Significant Changes. Policy
 This Policy replaces POL196/4 Copy Number Effective 14/12/2015 Offering to Group 2 patients Super urgent registrations Timing of fast-track offers Summary of Significant Changes Policy This policy has
This Policy replaces POL196/4 Copy Number Effective 14/12/2015 Offering to Group 2 patients Super urgent registrations Timing of fast-track offers Summary of Significant Changes Policy This policy has
Chapter 9. Kidney Donors. ANZDATA Registry 37th Annual Report. Data to 31-Dec-2013
 Chapter 9 Kidney Donors 214 37th Annual Report Data to 31-Dec-213 9-2 Deceased Kidney Donors The data for this section come from the Australia and New Zealand Organ Donor (ANZOD) Registry. Much more information
Chapter 9 Kidney Donors 214 37th Annual Report Data to 31-Dec-213 9-2 Deceased Kidney Donors The data for this section come from the Australia and New Zealand Organ Donor (ANZOD) Registry. Much more information
Kidney and Pancreas Transplantation in the United States,
 American Journal of Transplantation 2006; 6 (Part 2): 1153 1169 Blackwell Munksgaard No claim to original US government works Journal compilation C 2006 The American Society of Transplantation and the
American Journal of Transplantation 2006; 6 (Part 2): 1153 1169 Blackwell Munksgaard No claim to original US government works Journal compilation C 2006 The American Society of Transplantation and the
Summary of Significant Changes. Policy
 This Policy replaces POL230/5 Copy Number Effective 17/05/17 Summary of Significant Changes Policy rewritten to incorporate changes to the existing lung allocation scheme and the introduction of the new
This Policy replaces POL230/5 Copy Number Effective 17/05/17 Summary of Significant Changes Policy rewritten to incorporate changes to the existing lung allocation scheme and the introduction of the new
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION
 PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
Frequently Asked Questions about Kidney Transplantation
 NHS Logo here Frequently Asked Questions about Kidney Transplantation Patient Information Health & care information you can trust The Information Standard Certified Member Working together for better patient
NHS Logo here Frequently Asked Questions about Kidney Transplantation Patient Information Health & care information you can trust The Information Standard Certified Member Working together for better patient
Donation and Transplantation Kidney Paired Donation Program Data Report
 Donation and Transplantation Kidney Paired Donation Program Data Report 2009-2013 Extracts of the information in this report may be reviewed, reproduced or translated for educational purposes, research
Donation and Transplantation Kidney Paired Donation Program Data Report 2009-2013 Extracts of the information in this report may be reviewed, reproduced or translated for educational purposes, research
Living Donor Paired Exchange (LDPE)
") Living Donor Paired Exchange (LDPE) Why do we need Living Donation? 3,796 patients waiting for an organ transplant 2,679 (71%) waiting for a kidney transplant 249 people died while waiting for an organ
Living Donor Paired Exchange (LDPE) Why do we need Living Donation? 3,796 patients waiting for an organ transplant 2,679 (71%) waiting for a kidney transplant 249 people died while waiting for an organ
The UK Pancreas Allocation Scheme for Whole Organ and Islet Transplantation
 American Journal of Transplantation 2015; 15: 2443 2455 Wiley Periodicals Inc. C Copyright 2015 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.13284
American Journal of Transplantation 2015; 15: 2443 2455 Wiley Periodicals Inc. C Copyright 2015 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.13284
The New Kidney Allocation Policy: Implications for Your Patients and Your Practice
 The New Kidney Allocation Policy: Implications for Your Patients and Your Practice Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Explain
The New Kidney Allocation Policy: Implications for Your Patients and Your Practice Clinical Practice Today CME Co-provided by Learning Objectives Upon completion, participants should be able to: Explain
lnhs BLOOD AND TRANSPLANT RESEARCH, INNOVATION AND NOVEL TECHNOLOGIES ADVISORY GROUP DCD HEART ACTIVITY
 lnhs BLOOD AND TRANSPLANT RESEARCH, INNOVATION AND NOVEL TECHNOLOGIES ADVISORY GROUP INTRODUCTION DCD HEART ACTIVITY 1 DCD heart retrieval began in February 2015 for a 15 month initial evaluation period
lnhs BLOOD AND TRANSPLANT RESEARCH, INNOVATION AND NOVEL TECHNOLOGIES ADVISORY GROUP INTRODUCTION DCD HEART ACTIVITY 1 DCD heart retrieval began in February 2015 for a 15 month initial evaluation period
KIDNEY TRANSPLANT - A TREATMENT OPTION
 KIDNEY TRANSPLANT - A TREATMENT OPTION Page 1/5 WHAT IS A KIDNEY TRANSPLANT? When kidney failure becomes very advanced, your kidneys are so damaged they can no longer do their job. A transplant is a treatment
KIDNEY TRANSPLANT - A TREATMENT OPTION Page 1/5 WHAT IS A KIDNEY TRANSPLANT? When kidney failure becomes very advanced, your kidneys are so damaged they can no longer do their job. A transplant is a treatment
Hong Kong Journal Nephrol of 2000;(2): Nephrology 2000;2(2): BR HAWKINS ORIGINAL A R T I C L E A point score system for allocating cadaver
: Nephrology 2000;2(2): BR HAWKINS ORIGINAL A R T I C L E A point score system for allocating cadaver") Hong Kong Journal Nephrol of 2000;(2):79-83. Nephrology 2000;2(2):79-83. ORIGINAL A R T I C L E A point score system for allocating cadaveric kidneys for transplantation based on patient age, waiting time
Hong Kong Journal Nephrol of 2000;(2):79-83. Nephrology 2000;2(2):79-83. ORIGINAL A R T I C L E A point score system for allocating cadaveric kidneys for transplantation based on patient age, waiting time
Utilisation of an embedded specialist nurse and collaborative care pathway increases potential organ donor referrals in the emergency department
 1 Norfolk and Norwich University Hospital NHS Trust, Norwich, Norfolk, UK 2 NHS Blood and Transplant, Addenbrookes Hospital, Cambridge, UK Correspondence to Dr Julian Garside, Emergency Medicine Registrar,
1 Norfolk and Norwich University Hospital NHS Trust, Norwich, Norfolk, UK 2 NHS Blood and Transplant, Addenbrookes Hospital, Cambridge, UK Correspondence to Dr Julian Garside, Emergency Medicine Registrar,
LUNG ALLOCATION SCORE SYSTEM UPDATE
 LUNG ALLOCATION SCORE SYSTEM UPDATE Current Lung Allocation System System was implemented on May 4, 25 The Lung Allocation Score (LAS) is based on a combination of Expected survival in next year without
LUNG ALLOCATION SCORE SYSTEM UPDATE Current Lung Allocation System System was implemented on May 4, 25 The Lung Allocation Score (LAS) is based on a combination of Expected survival in next year without
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE NINETEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD AT 12.30 PM ON WEDNESDAY, 25 MAY 2011 AT THE SOCIETY OF CHEMICAL
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE NINETEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD AT 12.30 PM ON WEDNESDAY, 25 MAY 2011 AT THE SOCIETY OF CHEMICAL
Chapter 9. Kidney Donors. ANZDATA Registry 39th Annual Report. Data to 31-Dec-2015
 Chapter 9 Kidney Donors 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Deceased Kidney Donors The data for this section come from the Australia and New Zealand Organ Donor (ANZOD) Registry.
Chapter 9 Kidney Donors 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Deceased Kidney Donors The data for this section come from the Australia and New Zealand Organ Donor (ANZOD) Registry.
The New Kidney Allocation System: What You Need to Know. Quality Insights Renal Network 3 Annual Meeting October 2, 2014
 The New Kidney Allocation System: What You Need to Know Quality Insights Renal Network 3 Annual Meeting October 2, 2014 Pre Dialysis Era Dialysis Status in USA 500,000 patients on dialysis in 2013 100,000
The New Kidney Allocation System: What You Need to Know Quality Insights Renal Network 3 Annual Meeting October 2, 2014 Pre Dialysis Era Dialysis Status in USA 500,000 patients on dialysis in 2013 100,000
Pancreas transplants. What you need to know. Information for patients Sheffield Kidney Institute (Renal Unit)
") Pancreas transplants What you need to know Information for patients Sheffield Kidney Institute (Renal Unit) page 2 of 16 What is the pancreas and why is it transplanted? The pancreas is part of the digestive
Pancreas transplants What you need to know Information for patients Sheffield Kidney Institute (Renal Unit) page 2 of 16 What is the pancreas and why is it transplanted? The pancreas is part of the digestive
Organ Donation Activity
 3 Organ Donation Activity Organ Donation Activity Key messages There has been a 11% increase in deceased donors (to 1,574) and a
3 Organ Donation Activity Organ Donation Activity Key messages There has been a 11% increase in deceased donors (to 1,574) and a
Overview of organ donation and transplantation
 BTS Congress, March 2018 Overview of organ donation and transplantation Rachel Johnson Statistics and Clinical Studies NHS Blood and Transplant Organ Donation and Transplantation: the headlines Subject
BTS Congress, March 2018 Overview of organ donation and transplantation Rachel Johnson Statistics and Clinical Studies NHS Blood and Transplant Organ Donation and Transplantation: the headlines Subject
DCD Heart Transplantation Papworth Perspective
 DCD Heart Transplantation Papworth Perspective Simon Messer Stephen Large Objectives Heart transplantation in the UK DCD donation in the UK DCD impact on heart function Normothermic Regional Perfusion
DCD Heart Transplantation Papworth Perspective Simon Messer Stephen Large Objectives Heart transplantation in the UK DCD donation in the UK DCD impact on heart function Normothermic Regional Perfusion
UK TRANSPLANT. Professor Dave Collett Director of Statistics & Audit, UKT. Director of Donor Care & Co-ordination, UKT
 UK TRANSPLANT MINUTES OF THE THIRTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 11 JUNE 2008 IN CONFERENCE SUITE 2, UK TRANSPLANT, BRISTOL PRESENT: Professor Andrew Bradley Chairman Mr
UK TRANSPLANT MINUTES OF THE THIRTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 11 JUNE 2008 IN CONFERENCE SUITE 2, UK TRANSPLANT, BRISTOL PRESENT: Professor Andrew Bradley Chairman Mr
Making connections. Bilateral Cochlear Implant Audit
 Making connections. Bilateral Cochlear Implant Audit Results from the National Paediatric Bilateral Cochlear Implant Audit Who was involved? The project included 1001 children, aged from a few months to
Making connections. Bilateral Cochlear Implant Audit Results from the National Paediatric Bilateral Cochlear Implant Audit Who was involved? The project included 1001 children, aged from a few months to
Overview of Organ Donation and Transplantation
 2 Overview of Organ Donation and Transplantation Overview of Organ Donation and Transplantation A summary of organ donation and transplantation activity in the UK during the financial year from April 207
2 Overview of Organ Donation and Transplantation Overview of Organ Donation and Transplantation A summary of organ donation and transplantation activity in the UK during the financial year from April 207
Three Sides to Allocation. ECD Extended Criteria Donor
 Kidney Allocation- Optimal Use of Deceased Donors The New US System..and impact on wait list management Three Sides to Allocation Justice Peter G Stock MD, PhD Utility Efficiency Standard Criteria Donor
Kidney Allocation- Optimal Use of Deceased Donors The New US System..and impact on wait list management Three Sides to Allocation Justice Peter G Stock MD, PhD Utility Efficiency Standard Criteria Donor
Transplant Update New Kidney Allocation System Transplant Referral Strategies. Antonia Harford, MD University of New Mexico
 Transplant Update New Kidney Allocation System Transplant Referral Strategies Antonia Harford, MD University of New Mexico Financial Disclosures Doctor Harford has received financial support for dialysis
Transplant Update New Kidney Allocation System Transplant Referral Strategies Antonia Harford, MD University of New Mexico Financial Disclosures Doctor Harford has received financial support for dialysis
The Art and Science of Increasing Authorization to Donation
 The Art and Science of Increasing Authorization to Donation OPO Metrics: The Good, The Bad, and The Maybe Charlotte Arrington, MPH Arbor Research Collaborative for Health Alan Leichtman, MD University
The Art and Science of Increasing Authorization to Donation OPO Metrics: The Good, The Bad, and The Maybe Charlotte Arrington, MPH Arbor Research Collaborative for Health Alan Leichtman, MD University
Welcome to Transplantation
 Renal Services Welcome to Transplantation Introductory guide to kidney transplantation. Welcome to Transplantation Kidney transplantation is not a cure for your renal disease it is just another form of
Renal Services Welcome to Transplantation Introductory guide to kidney transplantation. Welcome to Transplantation Kidney transplantation is not a cure for your renal disease it is just another form of
Update on the National HPB Audit. Richard M Charnley Iain C Cameron
 Update on the National HPB Audit Richard M Charnley Iain C Cameron Initial Steps 2007 - Expressions of interest sought from HPB surgeons by AUGIS Council Series of Meetings Agreed - Audit of HPB cancer
Update on the National HPB Audit Richard M Charnley Iain C Cameron Initial Steps 2007 - Expressions of interest sought from HPB surgeons by AUGIS Council Series of Meetings Agreed - Audit of HPB cancer
Access and Outcomes Among Minority Transplant Patients, , with a Focus on Determinants of Kidney Graft Survival
 American Journal of Transplantation 2010; 10 (Part 2): 1090 1107 Wiley Periodicals Inc. Special Feature No claim to original US government works Journal compilation C 2010 The American Society of Transplantation
American Journal of Transplantation 2010; 10 (Part 2): 1090 1107 Wiley Periodicals Inc. Special Feature No claim to original US government works Journal compilation C 2010 The American Society of Transplantation
Chapter 7. Australian Waiting List. ANZDATA Registry 39th Annual Report. Data to 31-Dec-2015
 Chapter 7 Australian Waiting List 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Stock and Flow The waiting list data reported here are derived from the Australian National Organ Matching System
Chapter 7 Australian Waiting List 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Stock and Flow The waiting list data reported here are derived from the Australian National Organ Matching System
Kidney Allocation- Will it ever be fair? Peter G Stock MD, PhD UCSF Department of Surgery. Would you accept this offer?
 Kidney Allocation- Will it ever be fair? Peter G Stock MD, PhD UCSF Department of Surgery Question 1: A 19 y/o deceased donor kidney (O mismatch) from NYC is allocated to a 72 y/o highly sensitized caucasian
Kidney Allocation- Will it ever be fair? Peter G Stock MD, PhD UCSF Department of Surgery Question 1: A 19 y/o deceased donor kidney (O mismatch) from NYC is allocated to a 72 y/o highly sensitized caucasian
Update on Kidney Allocation
 Update on Kidney Allocation 23rd Annual Conference Association for Multicultural Affairs in Transplantation Silas P. Norman, M.D., M.P.H. Associate Professor Division of Nephrology September 23, 2015 Disclosures
Update on Kidney Allocation 23rd Annual Conference Association for Multicultural Affairs in Transplantation Silas P. Norman, M.D., M.P.H. Associate Professor Division of Nephrology September 23, 2015 Disclosures
Recipients and Recipient Transplant Coordinators. April 2014 Helen Tincknell Lead Nurse Recipient Coordination NHSBT
 Recipients and Recipient Transplant Coordinators April 2014 Helen Tincknell Lead Nurse Recipient Coordination NHSBT 1 UK Transplanting Centres 24 Kidney 8 Pancreas 8 Liver 7 Heart & Lung 4 Small bowel/multi
Recipients and Recipient Transplant Coordinators April 2014 Helen Tincknell Lead Nurse Recipient Coordination NHSBT 1 UK Transplanting Centres 24 Kidney 8 Pancreas 8 Liver 7 Heart & Lung 4 Small bowel/multi
Recent Developments in Cardiothoracic Transplantation
 Recent Developments in Cardiothoracic Transplantation Sally Rushton Statistics and Clinical Studies NHS Blood and Transplant BTS March 2018 Content Heart and lung transplant activity over last decade Heart
Recent Developments in Cardiothoracic Transplantation Sally Rushton Statistics and Clinical Studies NHS Blood and Transplant BTS March 2018 Content Heart and lung transplant activity over last decade Heart
Concepts for Kidney Allocation
 ORGAN PROCUREMENT AND TRANSPLANTATION NETWORK Concepts for Kidney Allocation The Organ Procurement and Transplantation Network (OPTN) is seeking feedback regarding the use of two concepts in the allocation
ORGAN PROCUREMENT AND TRANSPLANTATION NETWORK Concepts for Kidney Allocation The Organ Procurement and Transplantation Network (OPTN) is seeking feedback regarding the use of two concepts in the allocation
50 years Anniversary of First Kidney Transplant at Manchester Royal Infirmary
 50 years Anniversary of First Kidney Transplant at Manchester Royal Infirmary Consultant Transplant Surgeon Clinical Lead for Manchester /North west Paediatric Transplantation & Abdominal National Organ
50 years Anniversary of First Kidney Transplant at Manchester Royal Infirmary Consultant Transplant Surgeon Clinical Lead for Manchester /North west Paediatric Transplantation & Abdominal National Organ
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE
 NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE SIXTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 9 DECEMBER 2009 AT ODT, BRISTOL PRESENT: Prof. Andrew
NHS BLOOD AND TRANSPLANT ORGAN DONATION & TRANSPLANTATION DIRECTORATE MINUTES OF THE SIXTEENTH MEETING OF THE KIDNEY ADVISORY GROUP HELD ON WEDNESDAY, 9 DECEMBER 2009 AT ODT, BRISTOL PRESENT: Prof. Andrew
From Better to Best: Improving the availability of organs for transplant
 From Better to Best: Improving the availability of organs for transplant Elisabeth Buggins CBE Strategy Oversight Group Chair Presentation outline Progress 2004-2014 Strategy and work underway Outcomes
From Better to Best: Improving the availability of organs for transplant Elisabeth Buggins CBE Strategy Oversight Group Chair Presentation outline Progress 2004-2014 Strategy and work underway Outcomes
Antibody incompatible kidney transplantation from a deceased donor
 Antibody incompatible kidney transplantation from a deceased donor This leaflet explains more about antibody incompatible renal transplantation from a deceased donor. It will tell you why you were offered
Antibody incompatible kidney transplantation from a deceased donor This leaflet explains more about antibody incompatible renal transplantation from a deceased donor. It will tell you why you were offered
For more information about how to cite these materials visit
 Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Yorkshire and the Humber Kidney Transplant Forum NOTES
 Yorkshire and the Humber Kidney Transplant Forum Wednesday 11 November 2015 0900-1215 Waterton Park Hotel, Walton Hall, Walton, Wakefield, West Yorkshire, WF2 6PW NOTES AGENDA ITEMS 1. Welcome, Introductions,
Yorkshire and the Humber Kidney Transplant Forum Wednesday 11 November 2015 0900-1215 Waterton Park Hotel, Walton Hall, Walton, Wakefield, West Yorkshire, WF2 6PW NOTES AGENDA ITEMS 1. Welcome, Introductions,
The transplant benefit score and the national liver offering scheme
 The transplant benefit score and the national liver offering scheme New national offering scheme The development of a national set of rules to offer livers to named adult patients on the elective liver
The transplant benefit score and the national liver offering scheme New national offering scheme The development of a national set of rules to offer livers to named adult patients on the elective liver
East of Scotland Renal Transplantation Service. Annual Report. The Royal Infirmary of Edinburgh
 East of Scotland Renal Transplantation Service Annual Report The Royal Infirmary of Edinburgh April 1 st 29 to March 31 st 21 November 21 CONTENTS Page Introduction 3-4 Recipient Transplant Co-ordinators
East of Scotland Renal Transplantation Service Annual Report The Royal Infirmary of Edinburgh April 1 st 29 to March 31 st 21 November 21 CONTENTS Page Introduction 3-4 Recipient Transplant Co-ordinators
Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
 Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Pediatr Transplantation 2013: 17: 436 440 2013 John Wiley & Sons A/S. Pediatric Transplantation DOI: 10.1111/petr.12095 Predictors of cardiac allograft vasculopathy in pediatric heart transplant recipients
Information for potential living kidney donors
 Feedback We appreciate and encourage feedback. If you need advice or are concerned about any aspect of care or treatment please speak to a member of staff or contact the Patient Advice and Liaison Service
Feedback We appreciate and encourage feedback. If you need advice or are concerned about any aspect of care or treatment please speak to a member of staff or contact the Patient Advice and Liaison Service