WHEN (AND WHEN NOT) TO START DIALYSIS. Shahid Chandna, Ken Farrington
|
|
|
- Phebe Gilmore
- 6 years ago
- Views:
Transcription
1 WHEN (AND WHEN NOT) TO START DIALYSIS Shahid Chandna, Ken Farrington
2 Changing Perspectives Beta blockers 1980s Contraindicated in heart failure Now mainstay of therapy HRT 1990s must Now only if you have to Early Dialysis??? 1990s and 2000 Yes Now May be (Or even NOT)
3 Early Dialysis is Good Says Who? NKF (1997): Start dialysis with egfr ~ 10.5 (on the basis of the minimum target level of total (residual renal and dialysis) clearance for peritoneal dialysis. KDOQI (2006): RRT should be considered at egfr <15 egfr > 15 when patients have coexisting conditions or symptoms of uraemia Canadian Society of Nephrology: Start RRT egfr <12 dialysis can be deferred if there is no evidence of uraemia or malnutrition According to USRDS: patients starting dialysis with GFR > 10 19% in % in 2005
4 Early Dialysis is Good Says Who? Bonomini et al. Kidney Int Suppl Bonomini et al. Nephron Tattersall J, Greenwood R, Farrington K. Am J Nephrol consecutive CRF patients mean follow-up period of 10 ± 4.5 months 6 patients died n Higher age (p < 0.01) n Higher co-morbidity index (p < 0.05) n Lower mean Kt/V (p < 0.05) PROBLEM LEAD TIME BIAS
5 Wright et al. - Boston (USA) Clin J Am Soc Nephrol retrospective analysis USRDS n = 896,546 99,231 (11%) patients had an early dialysis start (egfr >15) White Male Higher comorbidity Diabetes Peritoneal dialysis 113,510 (12%) had a late start (egfr 5) reference group with an egfr of >5 to 10 Cox model adjusted for potential confounding variables Earliest start had increased risk of mortality Late start was associated with reduced risk of mortality CONCLUSIONS: Late initiation of dialysis is associated with a reduced risk of mortality despite the effect of lead time bias
6 Lassalle et al. French REIN Registry Kidney Int ,685 patients Dialysis at a higher egfr Older male had diabetes, cardiovascular diseases, or low body mass index and low albumin peritoneal dialysis Each 5-ml increase in egfr 40% increase in crude mortality risk 9% increased risk after adjusting for the above covariates. Age and patient condition strongly determine the decision to start dialysis and may explain most of the inverse association between egfr and survival
7 Wilson et al: Ontario, Canada Hemodial Int Retrospective cross-sectional study - n=271 17% started haemodialysis late (GFR<5) younger (p=0.008), females (p=0.013) more employed (p=0.051) less cardiac disease (p<0.001) Less peripheral vascular disease (p=0.031), Serum albumin was lower (p=0.023) At year 1, there was no difference in mortality At year 2, the earlier the dialysis, the greater the mortality rate (p=0.022) Adjustment for all these variables eliminated the significant association noted for the 2 year mortality in the early versus late dialysis start. HOWEVER -? LEAD TIME BIAS
8 Evans et al: Stockholm J Intern Med Population-based, prospective, observational cohort study - n = 901 Early-start dialysis egfr 7.5 late start of dialysis egfr <7.5) no dialysis Early start n = % died Late Start n = % died The adjusted HR for death was 0.84 [95% confidence interval (CI) 0.64, 1.10] among late versus early starters. No dialysis - mortality increased significantly at egfr below 7.5 ml Conclusion. No survival benefit from early initiation of dialysis
9 Rosansky: South Carolina, USA Arch Intern Med non-diabetic, 20- to 64-year-old, in-centre incident haemodialysis patients with no reported comorbidity besides hypertension piecewise proportional hazards model Unadjusted 1-year mortality by egfr ranged from 6.8% in the reference group (egfr <5.0 ml/min/ 1.73 m(2)) to 20.1% in the highest egfr group ( 15 Compared with the reference group, the HR for the HG was 1.27 (egfr, ml/min/1.73 m(2)), 1.53 (egfr, ml/min/1.73 m(2)), and 2.18 (egfr 15.0
10 IDEAL (Initiating Dialysis Early And Late) study Randomised Controlled Trial 32 centres in Australia and New Zealand 828 patients GFR (C&G) ml/min mean age, 60.4 years 355 (43%) with diabetes median follow-up period of 3.59 years GFR by Cockroft-Gault equation but a post hoc analysis with MDRD egfr. The study protocol permitted patients who were assigned to the late-start group to commence dialysis with GFR >7 if the treating physician recommended that they do so
11 IDEAL Study Early dialysis Group Planned to start dialysis with GFR Mean GFR at start of dilaysis12.0 [9.0 by MDRD equation] Median time to the initiation of dialysis: 1.8 months 75 (18.6%) started dialysis with an estimated GFR (C&G) of <10.0 HD = 188 n Temporary dialysis catheters in 15 PD = 195
12 IDEAL Study Late dialysis Group Planned to start dialysis with GFR 5 to 7 Mean GFR at start of dialysis 9.8 [7.2 by MDRD equation] Median time to the initiation of dialysis: 7.4 months 322 (75.9%) started dialysis with GFR > 7.0 ml HD = 215 Temporary dialysis catheters in 38 PD = 171
13 IDEAL Study - Results Mean difference in GFR 2.2 [1.8 by MDRD equation] a difference of 6 months between the groups in the start time for dialysis Early start group had more PD Fewer temporary dialysis catheters
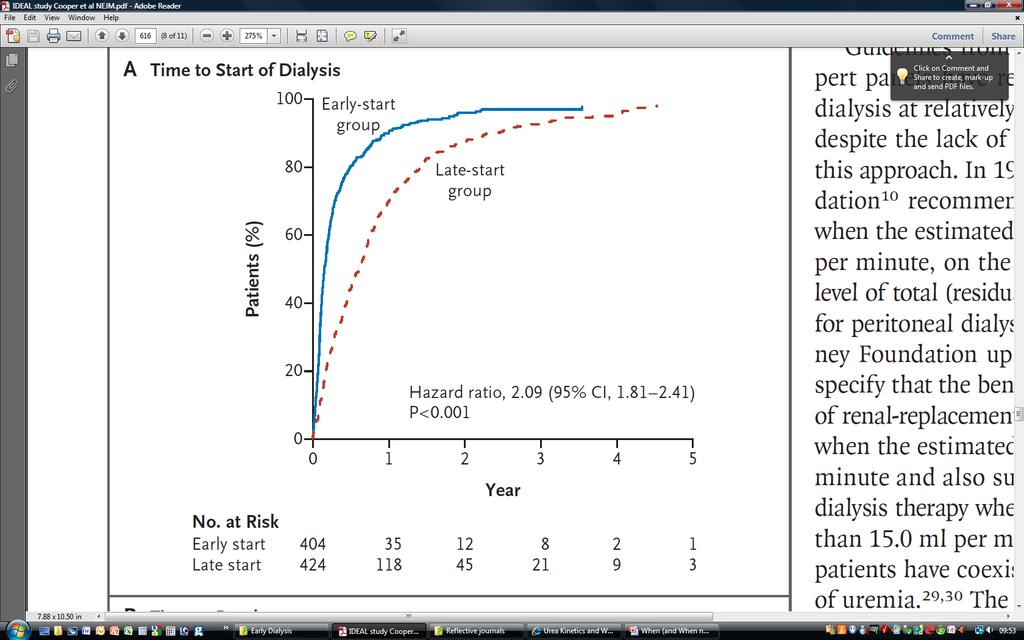
14
15 IDEAL Study - Survival No significant difference in survival, cardiovascular events, infections, or dialysis complications Mortality: 38% in early start group 37% in late start group Hazard ratio of 1.05 ( ) with early initiation
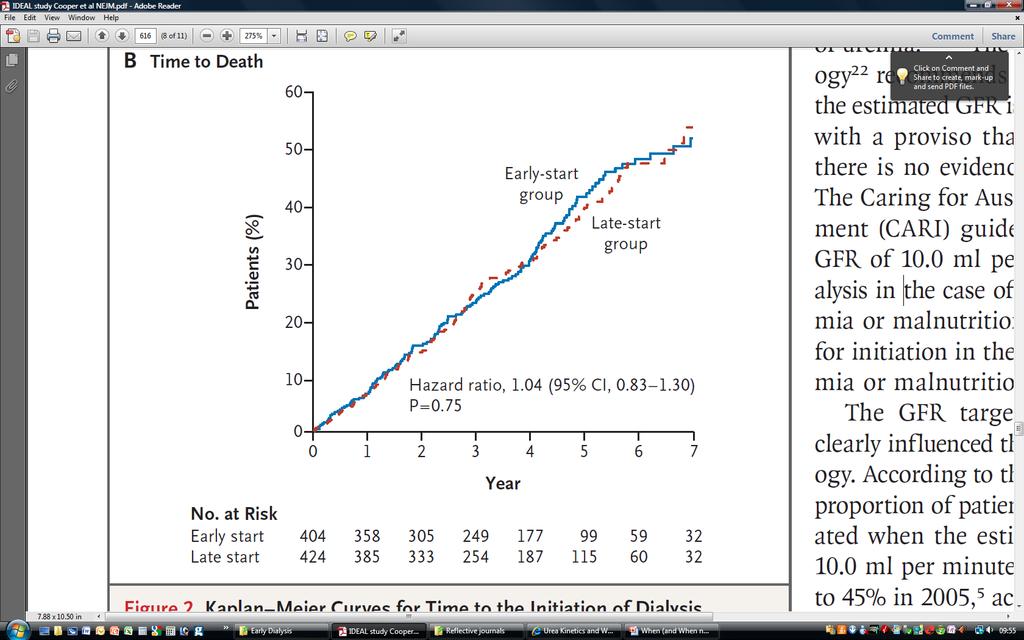
16
17 IDEAL Study - Conclusion With careful clinical management, dialysis may be delayed until either the GFR drops below 7.0 ml per minute or more traditional clinical indicators for the initiation of dialysis are present.
18 Lister Study Why do we need another retrospective study? Largest single centre study Not based on registry data Full information available on almost all patients Comorbidity from clinical record not coding for billing purposes As we have full information, we excluded Acute on Chronics (who started with low GFR not by choice)
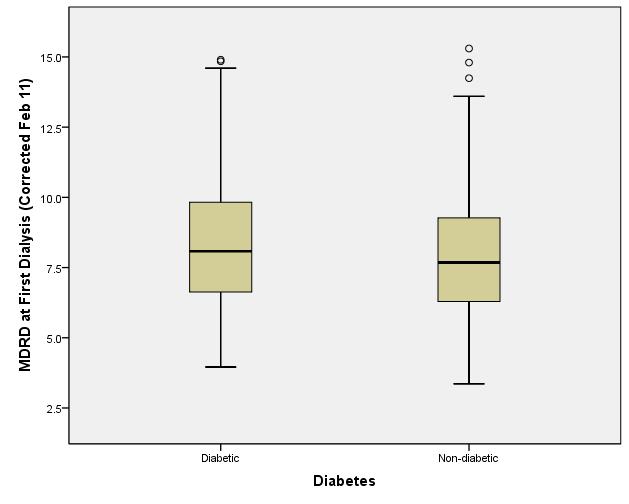
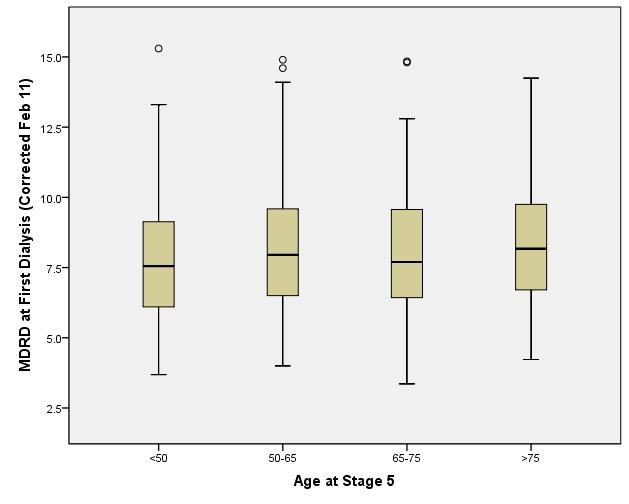
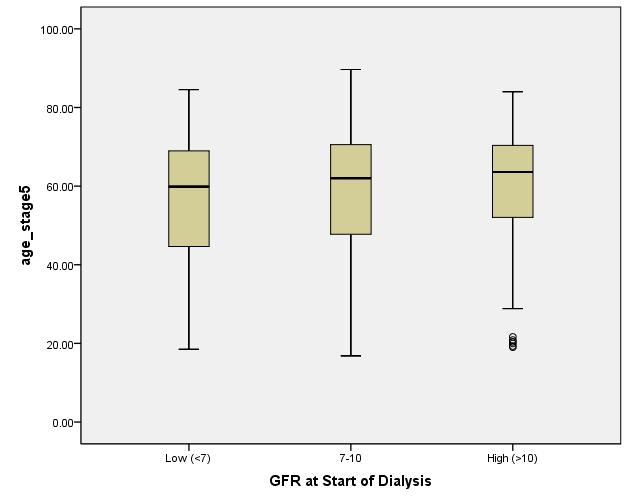
19 Lister Study 731 patients Age (mean 58.2) Male 66.7% White 82.7% Diabetic 33.1% GFR at start of dialysis 3.36 to 15.3 Mean 8.03 Median (19%) started dialysis with egfr > 10
20
21
22
23
24
25

26 Cox Model Adjusted for Age, Gender, Diabetes & Other Comorbidity
27 Cox Proportional Hazard Model p HR 95.0% CI Lowe r Upper High GFR Age High Comorbidity Diabetes Female Gender

28 Low risk patients (<65, non-diabetics, low comorbidity Low GFR High GFR P=0.09
29 Why is there a clamour for early dialysis Worse survival with unplanned dialysis start Everyone remembers patients who were known to renal services and yet had to start dialysis urgently Buck et al. Leicester (NDT- 2007) A retrospective survey of electronic and medical records known acute (starting dialysis urgently yet known to renal services > or =4 months) 49 of 109 (44%) - known acute Reasons n illness (21) n service (24) n patient related (17) n Multiple reasons (11)
30 Quality of Life Does early dialysis improve QOL? Korevaar et al. Am J Kidney Dis Effect of late versus timely initiation of dialysis on the course of healthrelated quality of life (HRQOL) Part of a large Dutch prospective multicenter study (Netherlands Cooperative Study on the Adequacy of Dialysis-2) 90 (38%) patients started dialysis late All patients showed marked improvement in HRQOL during the first 6 months after the start of dialysis treatment patients who started in time had significantly higher HRQOL for a number of dimensions immediately after the start of treatment After 12 months of dialysis treatment, these differences had disappeared What is not mentioned is the QOL in the late dialysed patients when they were not on dialysis
31 Symptoms of uraemia? Every Asian with fever is likely to have TB (Asian + Fever + Cough: MUST be TB) Every CKD patient with itching, nausea or tiredness MUST be uraemic The commonest Clinical detail on GP blood tests request T.A.T.T. Tired All The Time
32 So why should early dialysis be associated with poor survival There is something else wrong with the patient which we try to treat with dialysis (even when the recognised comorbidity is low) Patients with high comorbidity poorly tolerate dialysis Interaction between dialysis and other comorbidities. Dialysis is toxic
33 So what should we do? Whether early dialysis is detrimental or not the jury is out. There is certainly NO EVIDENCE that early dialysis is beneficial Don t by lazy - don t just follow the number. Assess the patient egfr Clinical condition (if tiredness is an indication for dialysis, >10% of population will be on dialysis) Assess the impact of dialysis on Patient s QOL Assess the prognosis with and without dialysis
The CARI Guidelines Caring for Australians with Renal Impairment. Level of renal function at which to initiate dialysis GUIDELINES
 Level of renal function at which to initiate dialysis Date written: September 2004 Final submission: February 2005 GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR
Level of renal function at which to initiate dialysis Date written: September 2004 Final submission: February 2005 GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR
The Effect of Residual Renal Function at the Initiation of Dialysis on Patient Survival
 ORIGINAL ARTICLE DOI: 10.3904/kjim.2009.24.1.55 The Effect of Residual Renal Function at the Initiation of Dialysis on Patient Survival Seoung Gu Kim 1 and Nam Ho Kim 2 Department of Internal Medicine,
ORIGINAL ARTICLE DOI: 10.3904/kjim.2009.24.1.55 The Effect of Residual Renal Function at the Initiation of Dialysis on Patient Survival Seoung Gu Kim 1 and Nam Ho Kim 2 Department of Internal Medicine,
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
When to start dialysis?
 Nephrol Dial Transplant (2006) 21 [Suppl 2]: ii20 ii24 doi:10.1093/ndt/gfl139 Original Article When to start dialysis? C. E. Douma 1 and W. Smit 2 1 Department of Nephrology, VU University Medical Center,
Nephrol Dial Transplant (2006) 21 [Suppl 2]: ii20 ii24 doi:10.1093/ndt/gfl139 Original Article When to start dialysis? C. E. Douma 1 and W. Smit 2 1 Department of Nephrology, VU University Medical Center,
The CARI Guidelines Caring for Australians with Renal Impairment. Other criteria for starting dialysis GUIDELINES
 Date written: September 2004 Final submission: February 2005 Other criteria for starting dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: September 2004 Final submission: February 2005 Other criteria for starting dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
The CARI Guidelines Caring for Australians with Renal Impairment. Monitoring patients on peritoneal dialysis GUIDELINES
 Date written: August 2004 Final submission: July 2005 Monitoring patients on peritoneal dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2004 Final submission: July 2005 Monitoring patients on peritoneal dialysis GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Survival of elderly patients with stage 5 CKD: comparison of conservative management and renal replacement therapy
 Nephrol Dial Transplant (2011) 26: 1608 1614 doi: 10.1093/ndt/gfq630 Advance Access publication 22 November 2010 Survival of elderly patients with stage 5 CKD: comparison of conservative management and
Nephrol Dial Transplant (2011) 26: 1608 1614 doi: 10.1093/ndt/gfq630 Advance Access publication 22 November 2010 Survival of elderly patients with stage 5 CKD: comparison of conservative management and
Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology
 Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology CKD Classification Stage Description GFR (ml/min/1.73.m2) 1 Kidney
Options in Renal Replacement Therapy: When, whom, which? Prof Dr. Serhan Tuğlular Marmara University Medical School Division of Nephrology CKD Classification Stage Description GFR (ml/min/1.73.m2) 1 Kidney
The CARI Guidelines Caring for Australians with Renal Impairment. Cardiovascular Risk Factors
 Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
You can sleep while I dialyze
 You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
You can sleep while I dialyze Nocturnal Peritoneal Dialysis Dr. Suneet Singh Medical Director, PD, VGH Division of Nephrology University of British Columbia Acknowledgements Melissa Etheridge You can sleep
KEEP 2.0 Annual Data Report Chapter Five
 KEEP 2. Annual Data Report Chapter Five Figure 5.1 percent distribution of KEEP participants with elevated serum creatinine levels, overall & by age 16 Percent of participants 12 8 4 All
KEEP 2. Annual Data Report Chapter Five Figure 5.1 percent distribution of KEEP participants with elevated serum creatinine levels, overall & by age 16 Percent of participants 12 8 4 All
Geriatric Nephrology. Murtener Tage
 Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
Geriatric Nephrology Murtener Tage 2014 Isabelle.Binet@kssg.ch www.nierenstiftung.ch Plan Geriatric nephrology The elderly with CKD The elderly on dialysis The elderly in transplantation Plan Geriatric
Outcomes of dialysis in the elderly. DNT March 2011 Dr Céline Foote
 Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
Outcomes of dialysis in the elderly DNT March 2011 Dr Céline Foote Increasing number of elderly patients on renal replacement therapy 500 500 Patients per million 400 300 200 100 400 300 200 100 TOTAL
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
The EQUAL study: a European study in chronic kidney disease stage 4 patients
 Nephrol Dial Transplant (2012) 27 (Supple 3): iii27 iii31 doi: 10.1093/ndt/gfs277 Advance Access publication 4 July 2012 Editorial Review The EQUAL study: a European study in chronic kidney disease stage
Nephrol Dial Transplant (2012) 27 (Supple 3): iii27 iii31 doi: 10.1093/ndt/gfs277 Advance Access publication 4 July 2012 Editorial Review The EQUAL study: a European study in chronic kidney disease stage
Impact of Timing of Initiation of Dialysis on Mortality
 J Am Soc Nephrol 14: 2305 2312, 2003 Impact of Timing of Initiation of Dialysis on Mortality SRINIVASAN BEDDHU,* MATTHEW H. SAMORE, MARK S. ROBERTS, GREGORY J. STODDARD, NIRUPAMA RAMKUMAR, LISA M. PAPPAS,
J Am Soc Nephrol 14: 2305 2312, 2003 Impact of Timing of Initiation of Dialysis on Mortality SRINIVASAN BEDDHU,* MATTHEW H. SAMORE, MARK S. ROBERTS, GREGORY J. STODDARD, NIRUPAMA RAMKUMAR, LISA M. PAPPAS,
The CARI Guidelines Caring for Australians with Renal Impairment. Mode of dialysis at initiation GUIDELINES
 Date written: September 2004 Final submission: February 2005 Mode of dialysis at initiation GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: September 2004 Final submission: February 2005 Mode of dialysis at initiation GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Difference in practical dialysis therapy between East Asia and US/EU
 Difference in practical dialysis therapy between East Asia and US/EU Jer-Ming Chang. M.D., Ph.D. 1 Professor, Attending physician, Kaohsiung Medical University Hospital; 2 Secretary General, Taiwan Society
Difference in practical dialysis therapy between East Asia and US/EU Jer-Ming Chang. M.D., Ph.D. 1 Professor, Attending physician, Kaohsiung Medical University Hospital; 2 Secretary General, Taiwan Society
Despite the widespread use of chronic dialysis, there
 Timing of Dialysis Initiation and Survival in ESRD Seth Wright,* Dalia Klausner, Bradley Baird, Mark E. Williams, Theodore Steinman, Hongying Tang, Regina Ragasa, and Alexander S. Goldfarb-Rumyantzev *Department
Timing of Dialysis Initiation and Survival in ESRD Seth Wright,* Dalia Klausner, Bradley Baird, Mark E. Williams, Theodore Steinman, Hongying Tang, Regina Ragasa, and Alexander S. Goldfarb-Rumyantzev *Department
Screening and early recognition of CKD. John Ngigi (FISN) Kidney specialist
 Kidney specialist") Screening and early recognition of CKD John Ngigi (FISN) Kidney specialist screening Why? Who? When? How? Primary diagnosis for patients who start dialysis Other 10% Glomerulonephritis 13% No. of dialysis
Screening and early recognition of CKD John Ngigi (FISN) Kidney specialist screening Why? Who? When? How? Primary diagnosis for patients who start dialysis Other 10% Glomerulonephritis 13% No. of dialysis
METABOLISM AND NUTRITION WITH PD OBESITY. Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle
 METABOLISM AND NUTRITION WITH PD OBESITY Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 Body Size in Patients New to Dialysis United States Body Mass Index, kg/m2 33 31
METABOLISM AND NUTRITION WITH PD OBESITY Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 Body Size in Patients New to Dialysis United States Body Mass Index, kg/m2 33 31
Early Initiation of Dialysis Fails to Prolong Survival in Patients with End-Stage Renal Failure
 J Am Soc Nephrol 13: 2125 2132, 2002 Early Initiation of Dialysis Fails to Prolong Survival in Patients with End-Stage Renal Failure JAMIE P. TRAYNOR,* KEITH SIMPSON,* COLIN C. GEDDES, CHRISTOPHER J. DEIGHAN,*
J Am Soc Nephrol 13: 2125 2132, 2002 Early Initiation of Dialysis Fails to Prolong Survival in Patients with End-Stage Renal Failure JAMIE P. TRAYNOR,* KEITH SIMPSON,* COLIN C. GEDDES, CHRISTOPHER J. DEIGHAN,*
Evidence Table. Study Type: Randomized controlled trial. Study Aim: To compare frequent nocturnal hemodialysis and conventional in-center dialysis.
 Evidence Table Clinical Area: Reference: Frequent home dialysis Culleton BF, Walsh M, Klarenbach SW et al. Effect of frequent nocturnal hemodialysis vs conventional hemodialysis on left ventricular mass
Evidence Table Clinical Area: Reference: Frequent home dialysis Culleton BF, Walsh M, Klarenbach SW et al. Effect of frequent nocturnal hemodialysis vs conventional hemodialysis on left ventricular mass
CARE FOR CHRONIC RENAL PATIENTS ROLE OF MULTIDISCIPLINARY APPROACH ÁGNES HARIS MD PHD, ST. MARGIT HOSPITAL, BUDAPEST BUDAPEST NEPHROLOGY SCHOOL, 2017
 CARE FOR CHRONIC RENAL PATIENTS ROLE OF MULTIDISCIPLINARY APPROACH ÁGNES HARIS MD PHD, ST. MARGIT HOSPITAL, BUDAPEST BUDAPEST NEPHROLOGY SCHOOL, 2017 RENEGOTIATING LIFE WITH CHRONIC KIDNEY DISEASE CONSTANTINI
CARE FOR CHRONIC RENAL PATIENTS ROLE OF MULTIDISCIPLINARY APPROACH ÁGNES HARIS MD PHD, ST. MARGIT HOSPITAL, BUDAPEST BUDAPEST NEPHROLOGY SCHOOL, 2017 RENEGOTIATING LIFE WITH CHRONIC KIDNEY DISEASE CONSTANTINI
The CARI Guidelines Caring for Australians with Renal Impairment. Blood urea sampling methods GUIDELINES
 Date written: November 2004 Final submission: July 2005 Blood urea sampling methods GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions are
Date written: November 2004 Final submission: July 2005 Blood urea sampling methods GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions are
Using the Knowledge to Action Cycle to Improve Timing of dialysis initiation
 Using the Knowledge to Action Cycle to Improve Timing of dialysis initiation Braden Manns University of Calgary Funded by The Kidney Foundation of Canada and the Canadian Institutes of Health Research
Using the Knowledge to Action Cycle to Improve Timing of dialysis initiation Braden Manns University of Calgary Funded by The Kidney Foundation of Canada and the Canadian Institutes of Health Research
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
Effect of previously failed kidney transplantation on peritoneal dialysis outcomes in the Australian and New Zealand patient populations
 NDT Advance Access published November 9, 2005 Nephrol Dial Transplant (2005) 1 of 8 doi:10.1093/ndt/gfi248 Original Article Effect of previously failed kidney transplantation on peritoneal dialysis outcomes
NDT Advance Access published November 9, 2005 Nephrol Dial Transplant (2005) 1 of 8 doi:10.1093/ndt/gfi248 Original Article Effect of previously failed kidney transplantation on peritoneal dialysis outcomes
Marginal Dialysis: Patient characteristics influencing outcomes
 Marginal Dialysis: Patient characteristics influencing outcomes Dr Celine Foote Staff specialist, Concord Repatriation General Hospital Post-Doctoral Research Fellow, The George Institute for Global Health
Marginal Dialysis: Patient characteristics influencing outcomes Dr Celine Foote Staff specialist, Concord Repatriation General Hospital Post-Doctoral Research Fellow, The George Institute for Global Health
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality
 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality Shannon H. Norris, BSN, RN June 6, 2018 Dialysis Initiation and Optimal Vascular Access: Outcomes and Mortality DISCUSSION: End Stage
Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly?
 Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly? Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University
Home Hemodialysis or Transplantation of the Treatment of Choice for Elderly? Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University
From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014
 From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014 Deux grands principes concernant la DP La dialyse péritonéale doit
From Peritoneal Dialysis to Hemodialysis How could we improve the transition? Th Lobbedez CHU de Caen Self Dialysis Meeting 22 May 2014 Deux grands principes concernant la DP La dialyse péritonéale doit
TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA
 & TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
& TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate
 Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Chapter 7: Adequacy of Haemodialysis and Serum Bicarbonate Summary. The urea reduction ratio (URR) has been rising year on year but now appears to have reached a plateau.. The URR increases the longer
Acceptance onto Dialysis Guidelines
 Guidelines John Kelly (Kogarah, New South Wales) Melissa Stanley (Melbourne, Victoria) David Harris (Westmead, New South Wales) Date written: December 2004 Final submission: June 2005 Predialysis education
Guidelines John Kelly (Kogarah, New South Wales) Melissa Stanley (Melbourne, Victoria) David Harris (Westmead, New South Wales) Date written: December 2004 Final submission: June 2005 Predialysis education
CHAPTER 2. Prevalence of Renal Replacement Therapy for End Stage Kidney Disease
 CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per
CHAPTER 2 Prevalence of Renal Replacement Therapy for End Stage Kidney Disease Summarising the number of prevalent renal replacement therapy patients in Australia and New Zealand, the prevalence rate per
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Chapter 12. End Stage Kidney Disease in Indigenous Peoples of Australia and Aotearoa/New Zealand. ANZDATA Registry 39th Annual Report
 Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Improvement in Pittsburgh Symptom Score Index After Initiation of Peritoneal Dialysis
 Advances in Peritoneal Dialysis, Vol. 24, 2008 Matthew J. Novak, 1 Heena Sheth, 2 Filitsa H. Bender, 1 Linda Fried, 1,3 Beth Piraino 1 Improvement in Pittsburgh Symptom Score Index After Initiation of
Advances in Peritoneal Dialysis, Vol. 24, 2008 Matthew J. Novak, 1 Heena Sheth, 2 Filitsa H. Bender, 1 Linda Fried, 1,3 Beth Piraino 1 Improvement in Pittsburgh Symptom Score Index After Initiation of
PART ONE. Peritoneal Kinetics and Anatomy
 PART ONE Peritoneal Kinetics and Anatomy Advances in Peritoneal Dialysis, Vol. 22, 2006 Paul A. Fein, Irfan Fazil, Muhammad A. Rafiq, Teresa Schloth, Betty Matza, Jyotiprakas Chattopadhyay, Morrell M.
PART ONE Peritoneal Kinetics and Anatomy Advances in Peritoneal Dialysis, Vol. 22, 2006 Paul A. Fein, Irfan Fazil, Muhammad A. Rafiq, Teresa Schloth, Betty Matza, Jyotiprakas Chattopadhyay, Morrell M.
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Stephen McDonald. Matthew Jose. Kylie Hurst INDIGENOUS 12-1
 ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
Malnutrition in advanced CKD
 Malnutrition in advanced CKD Malnutrition Lack of proper nutrition, caused by not having enough to eat, not eating enough of the right things or being unable to use the food that one does eat Jessica Stevenson
Malnutrition in advanced CKD Malnutrition Lack of proper nutrition, caused by not having enough to eat, not eating enough of the right things or being unable to use the food that one does eat Jessica Stevenson
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Renal Replacement Therapy - Indication and Follow up
 Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
Renal Replacement Therapy - Indication and Follow up Prof Brigadier General Mamun Mostafi FCPS, FRCP Chief Physician Combined Military Hospital Dhaka Bangladesh Primary Functions of the Kidney Removal
3/21/2017. Solute Clearance and Adequacy Targets in Peritoneal Dialysis. Peritoneal Membrane. Peritoneal Membrane
 3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
3/21/2017 Solute Clearance and Adequacy Targets in Peritoneal Dialysis Steven Guest MD Director, Medical Consulting Services Baxter Healthcare Corporation Deerfield, IL, USA Peritoneal Membrane Image courtesy
egfr 34 ml/min egfr 130 ml/min Am J Kidney Dis 2002;39(suppl 1):S17-S31
:S17-S31") Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
Update on Renal Therapeutics Caroline Ashley Lead Pharmacist Renal Services UCL Centre for Nephrology, Royal Free Hospital, London Kongress für Arzneimittelinformation January 2011 What are we going to
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION. Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle
 THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
Home dialysis in the Netherlands: Removing the barriers!
 Home dialysis in the Netherlands: Removing the barriers! Brigit van Jaarsveld & Alferso Abrahams Dialysis Initiatives Nefrologen September 21, 2017 No. of patients with ESKD 16000 Total no. of dialysis
Home dialysis in the Netherlands: Removing the barriers! Brigit van Jaarsveld & Alferso Abrahams Dialysis Initiatives Nefrologen September 21, 2017 No. of patients with ESKD 16000 Total no. of dialysis
Associations between comorbidities, treatment choice and outcome in the elderly with end-stage renal disease
 Nephrol Dial Transplant (2007) 22: 3246 3254 doi:10.1093/ndt/gfm400 Advance Access publication 5 July 2007 Original Article Associations between comorbidities, treatment choice and outcome in the elderly
Nephrol Dial Transplant (2007) 22: 3246 3254 doi:10.1093/ndt/gfm400 Advance Access publication 5 July 2007 Original Article Associations between comorbidities, treatment choice and outcome in the elderly
Dialysis versus Supportive Care
 Dialysis versus Supportive Care with a focus on the initial pathway in the elderly DNT Workshop. Glenelg, February 2017 Background: A better title would be dialysis v non-dialysis! For this discussion:
Dialysis versus Supportive Care with a focus on the initial pathway in the elderly DNT Workshop. Glenelg, February 2017 Background: A better title would be dialysis v non-dialysis! For this discussion:
FIRST RENAL REPLACEMENT
 FIRST RENAL REPLACEMENT THERAPY SELECTION IN DIABETIC PATIENTS Dr Cécile Couchoud (REIN registry, France) Davide Bolignano (ERBP, Italy) European Renal Best Practice Prof. Wim Van Biesen Chairman of ERBP
FIRST RENAL REPLACEMENT THERAPY SELECTION IN DIABETIC PATIENTS Dr Cécile Couchoud (REIN registry, France) Davide Bolignano (ERBP, Italy) European Renal Best Practice Prof. Wim Van Biesen Chairman of ERBP
Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access
 Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access Louise Moist Associate Professor Lead Vascular Access Ontario Renal Network Schulich School of Medicine University
Technical and Clinical Barriers to Implementing an Optimal Case Mix of Vascular Access Louise Moist Associate Professor Lead Vascular Access Ontario Renal Network Schulich School of Medicine University
When to initiate dialysis is an early start always better?
 Nephrol Dial Transplant (2011) 26: 2087 2091 doi: 10.1093/ndt/gfr181 Advance Access publication 4 May 2011 Editorial Reviews When to initiate dialysis is an early start always better? Tomasz Liberek 1,
Nephrol Dial Transplant (2011) 26: 2087 2091 doi: 10.1093/ndt/gfr181 Advance Access publication 4 May 2011 Editorial Reviews When to initiate dialysis is an early start always better? Tomasz Liberek 1,
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
Krediet slide di 18
 1 di 18 Assessment of fluid status in PD patients Raymond T. Krediet, Amsterdam, Netherlands Chairs:Walther H. Boer, Utrecht, The Netherlands F. Fevzi Ersoy, Antalya, Turkey Prof. Raymond T. Krediet DDivision
1 di 18 Assessment of fluid status in PD patients Raymond T. Krediet, Amsterdam, Netherlands Chairs:Walther H. Boer, Utrecht, The Netherlands F. Fevzi Ersoy, Antalya, Turkey Prof. Raymond T. Krediet DDivision
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
FULFILLMENT OF K/DOQI GUIDELINES 92 anemia treatment dialysis therapy vascular access
 INTRODUCTION ANEMIA TREATMENT hemoglobin levels epo treatment iron treatment FULFILLMENT OF K/DOQI GUIDELINES 2 anemia treatment dialysis therapy vascular access EPO DOSING PATTERNS 4 epo dosing per kg
INTRODUCTION ANEMIA TREATMENT hemoglobin levels epo treatment iron treatment FULFILLMENT OF K/DOQI GUIDELINES 2 anemia treatment dialysis therapy vascular access EPO DOSING PATTERNS 4 epo dosing per kg
23-Jun-15. Albuminuria Renal and Cardiovascular Consequences A history of progress since ,490,000. Kidney Center, UMC Groningen
 Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Chronic renal failure
 Chronic renal failure Dr. Alexander Woywodt Consultant Physician and Nephrologist / Hon. Senior Lecturer Lancashire Teaching Hospitals NHS Foundation Trust Fleetwood 23rd June 2009 Menu Epidemiology &
Chronic renal failure Dr. Alexander Woywodt Consultant Physician and Nephrologist / Hon. Senior Lecturer Lancashire Teaching Hospitals NHS Foundation Trust Fleetwood 23rd June 2009 Menu Epidemiology &
SAMPLE. Chronic Kidney Disease, Evidence-Based Practice, and the Nutrition Care Process. Chapter 1
 Chapter 1 Chronic Kidney Disease, Evidence-Based Practice, and the Nutrition Care Process This guide follows the steps of the Nutrition Care Process (NCP) nutrition assessment, nutrition diagnosis, nutrition
Chapter 1 Chronic Kidney Disease, Evidence-Based Practice, and the Nutrition Care Process This guide follows the steps of the Nutrition Care Process (NCP) nutrition assessment, nutrition diagnosis, nutrition
Time trends in initiation and dose of dialysis in end-stage renal disease patients in The Netherlands
 Nephrol Dial Transplant (2003) 18: 552 558 Original Article Time trends in initiation and dose of dialysis in end-stage renal disease patients in The Netherlands Fabian Termorshuizen 1, Johanna C. Korevaar
Nephrol Dial Transplant (2003) 18: 552 558 Original Article Time trends in initiation and dose of dialysis in end-stage renal disease patients in The Netherlands Fabian Termorshuizen 1, Johanna C. Korevaar
CHAPTER 9. End Stage Kidney Disease in Aotearoa/New Zealand
 CHAPTER 9 End Stage Kidney Disease in Aotearoa/New Zealand ANZDATA gratefully acknowledges the patients and their families and the clinicians who provided data, and the contributions of the Aotearoa/New
CHAPTER 9 End Stage Kidney Disease in Aotearoa/New Zealand ANZDATA gratefully acknowledges the patients and their families and the clinicians who provided data, and the contributions of the Aotearoa/New
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS
 GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
GUIDELINE FOR HAEMODIALYSIS PRESCRIPTION FOR NEW PATIENTS COMMENCING HAEMODIALYSIS RRCV CMG Nephrology Service 1. Introduction A first acute or chronic haemodialysis session may induce disequilibrium syndrome
Acceptance onto dialysis guidelines: St George Hospital
 Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Acceptance onto dialysis guidelines: St George Hospital The following information is a guideline to support clinicians in decision making regarding acceptance onto dialysis. A review of international guidelines
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Evaluation of Chronic Kidney Disease KDIGO. Paul E de Jong University Medical Center Groningen The Netherlands
 Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
21th Budapest Nephrology School Ágnes Haris, Kálmán Polner
 21th Budapest Nephrology School Ágnes Haris, Kálmán Polner 53 years old female, -worked as computer scientist, -lived with her husband and 2 children, -in excellent financial situation. Diagnosed with
21th Budapest Nephrology School Ágnes Haris, Kálmán Polner 53 years old female, -worked as computer scientist, -lived with her husband and 2 children, -in excellent financial situation. Diagnosed with
Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression?
 Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression? Laurent WEEKERS CHU SartTilman Layout Introduction Epidemiology A note of caution on causality and bias Patient survival
Back to dialysis after graft failure: Transplantectomy or not? Stop immunosuppression? Laurent WEEKERS CHU SartTilman Layout Introduction Epidemiology A note of caution on causality and bias Patient survival
Aging and renal diseases - Clinical management, treatment, ethics and complications
 ... Aging and renal diseases - Clinical management, treatment, ethics and complications Gijs Van Pottelbergh (ACHG KULeuven, IRSS UCLouvain), Pierre Wallemacq and Jan Degryse Overview Is there a high prevalence
... Aging and renal diseases - Clinical management, treatment, ethics and complications Gijs Van Pottelbergh (ACHG KULeuven, IRSS UCLouvain), Pierre Wallemacq and Jan Degryse Overview Is there a high prevalence
CKD Conservative care and preparation for dialysis Dr Anirudh Rao Registrar, UK Renal Registry. UK Renal Registry 2013 Annual Audit Meeting
 CKD Conservative care and preparation for dialysis Dr Anirudh Rao Registrar, UK Renal Registry UK Renal Registry 2013 Annual Audit Meeting Scope of the talk Background CK MAPPS EQUAL My Research Future
CKD Conservative care and preparation for dialysis Dr Anirudh Rao Registrar, UK Renal Registry UK Renal Registry 2013 Annual Audit Meeting Scope of the talk Background CK MAPPS EQUAL My Research Future
The CARI Guidelines Caring for Australians with Renal Impairment. 5. Classification of chronic kidney disease based on evaluation of kidney function
 5. Classification of chronic kidney disease based on evaluation of kidney function Date written: April 2005 Final submission: May 2005 GUIDELINES No recommendations possible based on Level I or II evidence
5. Classification of chronic kidney disease based on evaluation of kidney function Date written: April 2005 Final submission: May 2005 GUIDELINES No recommendations possible based on Level I or II evidence
The Health Problem: Guidelines: NHS Priority:
 PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation research project.
PRIORITY BRIEFING The purpose of this briefing paper is to aid Stakeholders in prioritising topics to be taken further by PenCLAHRC as the basis for a specific evaluation or implementation research project.
Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009
 Western University Scholarship@Western Electronic Thesis and Dissertation Repository June 2015 Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009 Ngan Lam The University
Western University Scholarship@Western Electronic Thesis and Dissertation Repository June 2015 Secular Trends in Cardiovascular Disease in Kidney Transplant Recipients: 1994 to 2009 Ngan Lam The University
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York
 Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York 4th International Conference on Nephrology & Therapeutics September 14, 2015 Baltimore,
Narender Goel et al. Middletown Medical PC, Montefiore Medical Center & Albert Einstein College of Medicine, New York 4th International Conference on Nephrology & Therapeutics September 14, 2015 Baltimore,
17 th Annual Meeting of JSHDF, Sept 3-4, 2011
 17 th Annual Meeting of JSHDF, Sept 3-4, 2011 Sug Kyun Shin 1, JY Moon 2, SW Han 3, DH Yang 4, SH Lee 2, HC Park 5, JK Kim 6 and YI Jo 7 1 Nephrology, NHIC Ilsan Hospital, 2 Kyunghee University Hospital
17 th Annual Meeting of JSHDF, Sept 3-4, 2011 Sug Kyun Shin 1, JY Moon 2, SW Han 3, DH Yang 4, SH Lee 2, HC Park 5, JK Kim 6 and YI Jo 7 1 Nephrology, NHIC Ilsan Hospital, 2 Kyunghee University Hospital
The CARI Guidelines Caring for Australasians with Renal Impairment. Biochemical Targets. Calcium GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Biochemical Targets CARMEL HAWLEY (Woolloongabba, Queensland) GRAHAME ELDER (Westmead, New South Wales) Calcium GUIDELINES
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Biochemical Targets CARMEL HAWLEY (Woolloongabba, Queensland) GRAHAME ELDER (Westmead, New South Wales) Calcium GUIDELINES
The CARI Guidelines Caring for Australasians with Renal Impairment. Specific management of IgA nephropathy: role of tonsillectomy GUIDELINES
 Specific management of IgA nephropathy: role of tonsillectomy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendation possible based on Level I or II
Specific management of IgA nephropathy: role of tonsillectomy Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendation possible based on Level I or II
Section Questions Answers
 Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
Section Questions Answers Guide to CKD Screening and Evaluation -Alec Otteman, MD Delaying Progression - Paul Drawz, MD, MHS, MS 1. Modifiable risk factors for CKD include: a. Diabetes b. Hypertension
K atching Up with KDOQI: Clinical Practice Guidelines & Clinical Practice Recommendations for Anemia of Chronic Kidney Disease 2006
 K atching Up with KDOQI: Clinical Practice Guidelines & Clinical Practice Recommendations for Anemia of Chronic Kidney Disease 2006 Why new guidelines? Rationale for KDOQI Anemia 2006 Expand scope to all
K atching Up with KDOQI: Clinical Practice Guidelines & Clinical Practice Recommendations for Anemia of Chronic Kidney Disease 2006 Why new guidelines? Rationale for KDOQI Anemia 2006 Expand scope to all
Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance
 Advances in Peritoneal Dialysis, Vol. 24, 2008 Rajesh Yalavarthy, Isaac Teitelbaum Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance Two indices of small-solute clearance, Kt/V urea and creatinine
Advances in Peritoneal Dialysis, Vol. 24, 2008 Rajesh Yalavarthy, Isaac Teitelbaum Peritoneal Dialysis Adequacy: Not Just Small- Solute Clearance Two indices of small-solute clearance, Kt/V urea and creatinine
End Stage Kidney Disease Among Indigenous Peoples of Australia and New Zealand
 Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Dialysis for everyone? Maurizio Gallieni
 Dialysis for everyone? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo, University of Milano, Milano, Italy Introduction NDT 2004; 19: 1357-1360 www.
Dialysis for everyone? Maurizio Gallieni Nephrology and Dialysis Unit Ospedale S. Carlo Borromeo, ASST Santi Paolo e Carlo, University of Milano, Milano, Italy Introduction NDT 2004; 19: 1357-1360 www.
ENDPOINTS FOR AKI STUDIES
 ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
ENDPOINTS FOR AKI STUDIES Raymond Vanholder, University Hospital, Ghent, Belgium SUMMARY! AKI as an endpoint! Endpoints for studies in AKI 2 AKI AS AN ENDPOINT BEFORE RIFLE THE LIST OF DEFINITIONS WAS
Concept and General Objectives of the Conference: Prognosis Matters. Andrew S. Levey, MD Tufts Medical Center Boston, MA
 Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Concept and General Objectives of the Conference: Prognosis Matters Andrew S. Levey, MD Tufts Medical Center Boston, MA General Objectives Topics to discuss What are the key outcomes of CKD? What progress
Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC
 Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC Aetiology Study effect of a risk factor on an outcome Consider potential confounding: other risk factor for
Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC Aetiology Study effect of a risk factor on an outcome Consider potential confounding: other risk factor for
. Time to transplant listing is dependent on. . In 2003, 9.1% of all prevalent transplant. . Patients with diabetes mellitus are less
 Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chronic Kidney Disease
 Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
Chronic Kidney Disease Presence of kidney damage or decreased kidney function for three or more months, - necessary to distinguish CKD from acute kidney disease. Ascertained either by kidney biopsy or
CHAPTER 3 DEATHS. Stephen McDonald Leonie Excell Brian Livingston
 CHAPTER 3 DEATHS Stephen McDonald Leonie Excell Brian Livingston DEATHS ANZDATA Registry 2008 Report INTRODUCTION AUSTRALIA NEW ZEALAND The total number of deaths was 1,452 (15.4 deaths per 100 patient
CHAPTER 3 DEATHS Stephen McDonald Leonie Excell Brian Livingston DEATHS ANZDATA Registry 2008 Report INTRODUCTION AUSTRALIA NEW ZEALAND The total number of deaths was 1,452 (15.4 deaths per 100 patient
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Acknowledgements. National Kidney Foundation of Connecticut Mark Perazella. Co-PI Slowing the progression of chronic kidney disease to ESRD
 A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
 Growth van Stralen KJ, et al., Kidney Int, 2014 Blood Pressure Management van Stralen KJ, et al., Kidney Int, 2014 Sodium Losses on PD Infants might need higher UF rate per BSA as compared to adults to
Growth van Stralen KJ, et al., Kidney Int, 2014 Blood Pressure Management van Stralen KJ, et al., Kidney Int, 2014 Sodium Losses on PD Infants might need higher UF rate per BSA as compared to adults to
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine
 Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Seung Hyeok Han, MD, PhD Department of Internal Medicine Yonsei University College of Medicine The Scope of Optimal BP BP Reduction CV outcomes & mortality CKD progression - Albuminuria - egfr decline
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY
 I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY GUIDELINE 1. INITIATION OF DIALYSIS 1.1 Preparation for kidney failure: Patients who reach chronic kidney disease (CKD) stage 4 (estimated
I. CLINICAL PRACTICE GUIDELINES FOR PERITONEAL DIALYSIS ADEQUACY GUIDELINE 1. INITIATION OF DIALYSIS 1.1 Preparation for kidney failure: Patients who reach chronic kidney disease (CKD) stage 4 (estimated
Las dos caras de la cretinina sérica The two sides of serum creatinine
 Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
Las dos caras de la cretinina sérica The two sides of serum creatinine ASOCIACION COSTARRICENSE DE MEDICINA INTERNA San José, Costa Rica June 2017 Kianoush B. Kashani, MD, MSc, FASN, FCCP 2013 MFMER 3322132-1
Strategies to assess and manage hypervolemia The invisible threat in dialysis
 Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission
Strategies to assess and manage hypervolemia The invisible threat in dialysis Rajiv Agarwal MD Professor of Medicine, Indiana University School of Medicine Volume excess is common and costly. Admission