Common Chronic Disease- DM/HD/IHD. Dr W.B.Chan Clinical Director Qualigenics Diabetes Centre
|
|
|
- Esmond Anderson
- 6 years ago
- Views:
Transcription
1 Common Chronic Disease- DM/HD/IHD Dr W.B.Chan Clinical Director Qualigenics Diabetes Centre
2 Pattern of Mortality in Hong Kong
3 Cardiovascular Mortality
4 Cerebrovascular Mortality
5 Proportion Due to Cardiovascular Diseases Percentage of Cardiovascular death

6 What is coronary heart disease?
7 Symptom of CHD Chest pain Exertion related Radiate to arm and jaw Sweating Shortness of breath Nausea Syncope

8 What is stroke

9 Haemorrhagic Stroke

10 Ischaemic Stroke
11 Clinical Features of Stroke Hemiplegia Dysphasia Facial asymmetry Diplopia Coma or death Swallowing difficulty Incontinence Numbness Dribling of saliva Ref : 7 Central Health Education Unit (Hong Kong)

12 What is blood pressure? Blood pressure refers to the pressure exerted by circulating blood on the inner walls of the arteries that carry blood from the heart. the systolic pressure as the heart contracts and the diastolic pressure as it relaxes between beats.


13 Electronic Sphygomanometer
14 Classification of HT(JNC 7) SBP/DBP Category <120/80 Normal /80 139/ Prehypertension >140/90 Hypertension /90 159/ Stage 1 >160/100 Stage 2
15 Prevalence of hypertension*: North America and Europe Prevalence (%) Men Women Total United States Canada Europe Italy Sweden England Spain Finland Germany * BP 140/90 mmhg or treatment with antihypertensive medication Wolf-Maier K, et al. JAMA 2003;289:
16 Prevalence of HT in Hong Kong 70.00% 60.00% 50.00% 40.00% 30.00% 20.00% Male Female 10.00% 0.00% >65 Overall prevalence: 27.2% Male 30.1% Female 24.9%
17 Change of Blood Pressure with Age
18 Hazard Ratio of Stroke in Relation to SBP
19 Hazard Ratio of IHD in Relation to SBP
20 Composite Endpoint in Relation to SBP
21 Relative Contribution of DBP and SBP to Cardiovascular Risk
22 Elderly with Isolated Systolic Hypertension
23
24 Multiple antihypertensive agents are needed to achieve target BP Number of antihypertensive agents Trial Target BP (mmhg) UKPDS DBP <85 ABCD DBP <75 MDRD MAP <92 HOT DBP <80 AASK MAP <92 IDNT SBP <135/DBP <85 ALLHAT SBP <140/DBP <90 DBP, diastolic blood pressure; MAP, mean arterial pressure; SBP, systolic blood pressure Bakris GL, et al. Am J Kidney Dis 2000;36: ; Lewis EJ, et al. N Engl J Med 2001;345: ; Cushman WC, et al. J Clin Hypertens 2002;4:
25 WHO Criteria for diabetes (DM) Fasting Plasma Glucose 2 hour glucose (mmol/l( mmol/l) 5.5 normal IFG/IGT 7.0 DM < >11.1 IFG/IGT DM IFG=impaired fasting glycemia IGT=impaired glucose tolerance
26 Age-adjusted prevalence of type 2 DM in the age group 12.0% 10.0% 8.0% 10.2% 9.5% 6.0% 4.0% Women Men 2.0% 0.0% Prevalence Lam TH, et al. Diabet Med 2000;17:
27 Mortality rate is twice as great in patients with diabetes Mortality rate (deaths per 1000 patient-years) Ratio 2.5 Ratio 2.2 Ratio 2.1 Control Diabetes Whitehall study Paris Prospective study Helsinki Policemen study Balkau B et al. Lancet 1997; 350: 1680.
28 Diabetes and Life Expectancy Male Female Diabetic Nondiabetic Nondiabetic Diabetic Mortality(every 1000 person-year) Life Expectancy Health Adjusted Life Expectancy
29 Risk of MI is increased in type 2 diabetes * Risk of fatal or nonfatal MI (%) No prior MI Prior MI Nondiabetic subjects * Type 2 diabetic subjects n = 1304 n = 69 n = 890 n = year incidence in a Finnish-based cohort *p < versus no prior MI p < vs no diabetes Adapted from Haffner SM. New Engl J Med 1998; 339:
30 Diabetes is associated with major CVDs in Asia Pacific Fatal CHD Fatal cerebrovascular disease Other fatal CVD All fatal CVD Fatal CHD and nonfatal MI Fatal cerebrovascular disease and nonfatal stroke Hazard ratio associated with having diabetes (95% CI) Adapted from Asia Pacific Cohort Studies Collaboration. Diabetes Care 2003; 26:
31 Diabetes increases the risk of mortality in Asia Pacific 3 Data from 24 Asia Pacific cohort studies (n = 161,214) Crude annual death rate (%) % 2.4% CVD accounted for 46% of the known causes of death in those with diabetes 0 Without diabetes With diabetes Asia Pacific Cohort Studies Collaboration. Diabetes Care 2003; 26:
32 Incidence of diabetes in end-stage renal failure: Australia Type Type 2 (insulin requiring) Type 2 (non insulin) Total new patients Number of diabetic patients Number of new patients Year of entry 0 Australian and New Zealand Dialysis and Transplant Registry.
33 Hong Kong Renal Registry (95-99) 99) Diabetes Non-DM Overall 58% increase DM 100% increase Non-DM 48% increase No of cases of Renal replacement therapy Lui SF et al HK J Nephrology 2000
34 Visual Impairment Due to Diabetes

35 Retinopathy
36 UKPDS: increased risk of diabetes-related complications corresponding with a 1% increase in HbA 1c 1% increase in HbA 1c 0.9% decrease in HbA 1c 21% 14% 12% 37% 25% Increase in any diabetesrelated endpoint * Increase in risk of MI* Increase in risk of stroke** Increase in risk of microvascular complications* Decrease in risk of microvascular complications *p < ; **p = 0.035; p = Adapted from UKPDS Group. UKPDS 35. BMJ 2000; 321: ; UKPDS Group. UKPDS 33. Lancet 1998; 352:
37 Decline in β-cell function is associated with loss of glycaemic control 9 Conventional HbA 1c (%) 8 7 Intensive % = normal range of HbA 1c Years from randomisation Adapted from UKPDS Group. UKPDS 33. Lancet 1998; 352:
38 The UKPDS demonstrated progressive decline of β-cell function over time 100 β-cell function (% β) Mean β-cell function at diagnosis Start of treatment p < Time (years) HOMA model, diet-treated n = 376 Adapted from Holman RR. Diabetes Res Clin Pract 1998; 40 (Suppl): S21 5.

39 Incidence of Diabetic Endpoint with Regard to Glycaemic Control

40 Relative Risk of Death with Regard to Glycaemic Control

41 Relative Risk of Complications with Regard to Glycaemic Control
42 Medical Nutrition therapy (MNT) Diabetic Control Exercise Medications
43 Goals of medical nutrition therapy Address individual nutritional needs Attain and maintain optimal metabolic outcomes Blood glucose Lipid profiles Blood pressure Prevent and treat chronic complications Obesity, Hypertension, Cardiovascular disease, Renal impairment Improve overall health
44 Changes in DM dietary recommendations over the years Distribution of Calories Year CHO (%) Protein (%) Fat (%) Before 1921 Starvation Diets A A,B (CHO + MUFA) A,B A: Based on nutrition assessment B: < 10% saturated fat
45 ADA and EASD Recommendations Energy Reduce if BMI> 25 Protein 10-20% of total kcal Carbohydrates and fat Saturated fat < 10% Polyunsaturated 10% CHO + MUFA 60-70% Fiber g /day Depending on body weight
46 Guidelines for Nutrition Intervention An individualized meal plan Address age, current medication, personal food preferences, lifestyles and willingness to change Meal spacing ( meals a day) Spreading the nutrient loads, esp. CHO Minimize postprandial glucose response and maximize the use of endogenous insulin Moderate wt loss of 5-10% 5 in obese type 2 DM patients Improvement in glycemic control, BP and lipids
 Risk of co-morbidities Normal range 18.5 22.9 Average Overweight 23 Pre-obese 23 24.9 Increased Obese class I 25.0 29.9 Moderate Obese class II 30.0 34.9 Severe Obese class III 35.")
47 Asian Obesity Guideline: lower BMI Proposed classification of weight by BMI in adult Asians (Asia- Pacific Obesity Guideline 2000) Asian guidelines BMI > 23 overweight BMI > 25 obese Classification BMI (kg/m 2 ) Risk of co-morbidities Normal range Average Overweight 23 Pre-obese Increased Obese class I Moderate Obese class II Severe Obese class III 35.0 Very severe
48 Weight control principles Energy Intake > Energy expenditure Gain weight Energy Intake < Energy expenditure Lose weight Energy Intake = Energy expenditure Maintain weight
49 To lose 1-22 pound adipose tissue per week = promote negative energy balance = need to cut down kcal /week ( kcal per day) through diet and exercise


50 食物中的隱藏脂肪 卡路里 脂肪佔卡路里比例 燒賣 45 60% (1 粒 ) 鰻魚 % (100 克 )

 山竹牛肉 98")
51 食物中的隱藏脂肪 卡路里脂肪佔卡路里比例 貢丸 95 72% (2 粒 ) 山竹牛肉 98 75% (1 粒 )

52 食炒粉炒麵 = 飲油? 資料來源 : 東方日報 2004 年 8 月 18
")

53 甜品不油膩? 食物 油份 ( 克 ) 食物 油份 ( 克 ) 4 粒芝麻湯丸 15 > 1 包細薯條 12
")

54 甜品不油膩? 食物 油份 ( 克 ) 食物 油份 ( 克 ) 1 件甘筍蛋糕 29 > 1 條油炸鬼 13
55 Effect of Seeing Dietitian

56 Effect of Self Monitoring

57 Effect of DM educator
58
59 Short Term Effect of Exercise in Type 2 Diabetes Exercise at fasting state tend not to affect plasma glucose Exercise post-meal tend to lower plasma glucose
60 Long Term Effect of Exercise in Type 2 Diabetes Type 2 diabetes has predominant insulin resistance especially in Caucasian population Exercise reduce insulin resistance through mechanism similar to mechanism in normal subjects and weight loss A reduction in glucose 12 hour after exercise
61 Long Term Effect of Exercise in Type 2 Diabetes However, FBS and glucose tolerance no longer improve 72 hour after exercise, therefore recommended exercise at least every days Meta-analysis analysis showed an average improvement of HbA1c by 0.7% in different exercise program
62 Long Term Effect of Exercise in Type 2 Diabetes Main limitation is the improvement in HbA1c is not sustained Likely due to non-compliance Compliance drop to as low as 20% 1 year after enrollment in an education program Diabetes with maintenance of exercise has lower cardiovascular mortality




63 AMARYL : the only drug to provide dual action Action on insulin resistance Action on insulin secretion HbA1 C reduction Amaryl Conventional Sulfonylureas / % to 2% 1% to 2% Glinides 0 ++ Biguanides Glitazones to 1.7% 1% to 2% 0.5% to 1.3% α-glucosidase inhibitors % to 1% Data from Henry. Endocrinol Metab Clin. 1997;26: Gitlin, et al. Ann Intern Med. 1998;129: Neuschwander-Tetri, et al. Ann Intern Med. 1998;129:38-41 Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998: Fonseca, et al. J Clin Endocrinol Metab. 1998;83: Data from Bell & Hadden. Endocrinol Metab Clin. 1997;26: De Fronzo, et al. N Engl J Med. 1995;333: Bailey & Turner. N Engl J Med. 1996;334: Medical Management of Type 2 Diabetes. 4th ed. Alexandria, Va: American Diabetes Association; 1998: Goldberg, et al. Diabetes Care 21:

64 Mortality in Relation to Blood Pressure Control

65 Complications in Relation to Blood Pressure Control

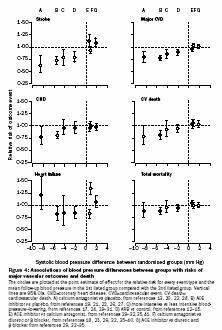
66 Systolic Blood Pressure in Relation to Complications
67 Diastolic Blood Pressure in Relation to Cardiovascular Event (HOT Study) Incidence per 1000 patient-year follow up Major Cardiovascular Endpoint Cardiovascular Mortality 90 mmhg 85 mmhg 80 mmhg
68 Salient Points Establish the importance of blood pressure control in diabetes Establish the target of 130/80 in diabetic patients Establish the need for polypharmacy in controlling blood pressure
69 CARDS Study 2838 diabetes patients aged years LDL-cholesterol concentration of 4.14 mmol/l or lower, a fasting triglyceride amount of 6.78 mmol/l or less, at least one of the following: retinopathy, albuminuria, current smoking, or hypertension randomised to placebo (n=1410) or atorvastatin 10 mg daily (n=1428)
70 CARDS Study
71 Impact of Atorvastatin on Cardiovascular Event
72 National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) (ATPIII) Risk Category LDL-C Goal LDL-C C Level for Initiating TLC* Consider Drug Therapy CHD / CHD risk equivalents (10 yr. CHD risk >20%) Multiple (2+) risk factors (10 yr. CHD risk <20%) 0-11 Risk factor <2.6 mmol/l <3.4 mmol/l <4.1 mmol/l > mmol/l > 3.4 mmol/l > 4.1 mmol/l > 3.4 mmol/l ( mmol/l: : drug optional) 10-yr risk 10%-20%: > 3.4 mmol/l 10-yr risk <10%: > 4.1 mmol/l > 5.2 mmol/l ( mmol/l: drug optional) *TLC: Therapeutic Lifestyle Changes
73 Salient Points Type 2 diabetes is IHD risk equivalent LDL lowering with statin to 2.6mmol/l or lower is a must LDL-C C down to 1.8 is preferred in high risk DM patients Statins are mostly safe with long term use

74 Intensive Therapy v.s. Traditional Therapy
75 Intensive Therapy v.s. Traditional Therapy
76 Steno-2 2 study: effect of aggressive versus conventional treatment on complications of type 2 diabetes 60 No. at risk Primary composite endpoint (%) Conventional therapy Intensive therapy Conventional therapy Intensive therapy Months of follow-up p = Gaede P et al. N Engl J Med 2003; 348:
77 Characteristics of Chronic Diseases Common Asymptomatic especially at early stage of disease Not curable, therefore need life long treatment Patient need to play active role in the treatment of disease Benefit of treatment not readily seen during early stage Treatment per se may induce symptom Complication once develop, mostly not reversible
78 Barrier to Successful Treatment Late presentation of disease Lack of understanding of the diseases Unwillingness to comply to life long treatment Patients play passive instead of active role Unwilling to accept treatment induced symptom Lack of awareness of doctor in detection and strict control Lack of infra-structure for education Financial/resources barrier
79 Key to Success Screening for early detection Public education to improve awareness Policy to improve incentive of accepting treatment Continues medical education Develop infra-structure for patient education Structure care emphasizing on target reaching Use of disease modifying drug, simple treatment regime and drugs with less side effect Appropriate resources allocation
Common Chronic Disease- DM/HD/IHD. Dr W.B.Chan Clinical Director Qualigenics Diabetes Centre
 Common Chronic Disease- DM/HD/IHD Dr W.B.Chan Clinical Director Qualigenics Diabetes Centre Pattern of Mortality in Hong Kong Cardiovascular Mortality Cerebrovascular Mortality Proportion Due to Cardiovascular
Common Chronic Disease- DM/HD/IHD Dr W.B.Chan Clinical Director Qualigenics Diabetes Centre Pattern of Mortality in Hong Kong Cardiovascular Mortality Cerebrovascular Mortality Proportion Due to Cardiovascular
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Burden of the Diabetic Heart
 The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Burden of the Diabetic Heart Dr. Ghaida Kaddaha (MBBS, MRCP-UK, FRCP-london) Diabetes Unit Rashid Hospital Dubai U.A.E Risk of CVD in Diabetes Morbidity and mortality from CVD is 2-4 fold higher than
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
The target blood pressure in patients with diabetes is <130 mm Hg
 Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
Controversies in hypertension, About Diabetes diabetes and and metabolic Cardiovascular syndrome Risk ESC annual congress August 29, 2011 The target blood pressure in patients with diabetes is
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes?
 Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Implications of The LookAHEAD Trial: Is Weight Loss Beneficial for Patients with Diabetes? Boston, MA November 7, 213 Edward S. Horton, MD Professor of Medicine Harvard Medical School Senior Investigator
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study
 LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study") Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Felix Vallotton Ball (1899) LDL-C management in Asian diabetes: moderate vs. high intensity statin --- a lesson from EMPATHY study Conflict of interest disclosure None Committee of Scientific Affairs Committee
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
A Fork in the Road: Navigating Through New Terrain
 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for Diabetes
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus. Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre
 Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
Initiating Insulin in Primary Care for Type 2 Diabetes Mellitus Dr Manish Khanolkar, Diabetologist, Auckland Diabetes Centre Outline How big is the problem? Natural progression of type 2 diabetes What
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease
 The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
The promise of the thiazolidinediones in the management of type 2 diabetes-associated cardiovascular disease Steve Smith, Group Director Scientific Affairs, Diabetes & Metabolism GlaxoSmithKline R & D
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes
 A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
A factorial randomized trial of blood pressure lowering and intensive glucose control in 11,140 patients with type 2 diabetes Hypotheses: Among individuals with type 2 diabetes, the risks of major microvascular
Causes of Poor BP control Rates
 Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
Goals Of Hypertension Management in Clinical Practice World Hypertension League (WHL) Meeting Adel E. Berbari, MD, FAHA, FACP Professor of Medicine and Physiology Head, Division of Hypertension and Vascular
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
The CARI Guidelines Caring for Australians with Renal Impairment. Cardiovascular Risk Factors
 Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
Cardiovascular Risk Factors ROB WALKER (Dunedin, New Zealand) Lipid-lowering therapy in patients with chronic kidney disease Date written: January 2005 Final submission: August 2005 Author: Rob Walker
Objectives. Objectives. Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015
 Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
Alejandro J. de la Torre, MD Cook Children s Hospital May 30, 2015 Presentation downloaded from http://ce.unthsc.edu Objectives Understand that the obesity epidemic is also affecting children and adolescents
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Management of Hypertension in the Diabetic Patient:
 Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
Management of Hypertension in the Diabetic Patient: Nicolas W. Shammas, MS, MD Research Director, Cardiovascular Medicine, PC Presentation Objectives To review: The relationship between HTN, insulin resistance
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
Glycemic index, glycemic load, and the risk of acute myocardial infarction in middle-aged Finnish men:
 Glycemic index, glycemic load, and the risk of acute myocardial infarction in middle-aged Finnish men: The Kuopio Ischaemic Heart Disease Risk Factor Study Jaakko Mursu, Jyrki K. Virtanen, Tiina H. Rissanen,
Glycemic index, glycemic load, and the risk of acute myocardial infarction in middle-aged Finnish men: The Kuopio Ischaemic Heart Disease Risk Factor Study Jaakko Mursu, Jyrki K. Virtanen, Tiina H. Rissanen,
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
7/6/2012. University Pharmacy 5254 Anthony Wayne Drive Detroit, MI (313)
") University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
University Pharmacy 5254 Anthony Wayne Drive Detroit, MI 48202 (313) 831-2008 Be able to identify the signs of a heart attack or stoke Identify what puts you at a higher risk for cardiovascular disease,
Update on CVD and Microvascular Complications in T2D
 Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on CVD and Microvascular Complications in T2D Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention?
 well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
well-targeted primary prevention of cardiovascular disease: an underused high-value intervention? Rod Jackson University of Auckland, New Zealand October 2015 Lancet 1999; 353: 1547-57 Findings: Contribution
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS
 BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Slide 1. Slide 2. Slide 3. A Fork in the Road: Navigating Through New Terrain. Diabetes Standards of Care Then and Now
 Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Slide 1 A Fork in the Road: Navigating Through New Terrain Carol Hatch Wysham, MD Clinical Associate Professor of Medicine University of Washington School of Medicine Section Head, Rockwood Center for
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Traditional Asian Soyfoods. Proven and Proposed Cardiovascular Benefits of Soyfoods. Reduction (%) in CHD Mortality in Eastern Finland ( )
 in CHD Mortality in Eastern Finland ( )") Proven and Proposed Cardiovascular Benefits of Soyfoods Mark Messina, PhD, MS Soy Nutrition Institute Loma Linda University Nutrition Matters, Inc. markjohnmessina@gmail.com 1000 80 20 60 40 40 60 20 80
Proven and Proposed Cardiovascular Benefits of Soyfoods Mark Messina, PhD, MS Soy Nutrition Institute Loma Linda University Nutrition Matters, Inc. markjohnmessina@gmail.com 1000 80 20 60 40 40 60 20 80
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents
 Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Tailored Statin Treatment for Type 2 Diabetes. Han, Ki Hoon Asan Medical Center University of Ulsan
 Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
Blood Pressure Targets in Diabetes
 Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
Stockholm, 29 th August 2010 ESC Meeting Blood Pressure Targets in Diabetes Peter M Nilsson, MD, PhD Department of Clinical Sciences University Hospital, Malmö Sweden Studies on BP in DM2 ADVANCE RCT (Lancet
American Academy of Insurance Medicine
 American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
American Academy of Insurance Medicine October 2012 Dr. Alison Moy Liberty Mutual Dr. John Kirkpatrick Thrivent Financial for Lutherans 1 59 year old male, diagnosed with T2DM six months ago Nonsmoker
Pre-diabetes. Pharmacological Approaches to Delay Progression to Diabetes
 Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Pre-diabetes Pharmacological Approaches to Delay Progression to Diabetes Overview Definition of Pre-diabetes Risk Factors for Pre-diabetes Clinical practice guidelines for diabetes Management, including
Key causes of preventable deaths in New Zealand In a population of 10,000 New Zealanders, every year there will be about:
 Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
Preventive care - Chronic Disease Management in primary care: a population perspective Rod Jackson University of Auckland New Zealand (22/11/8) Key causes of preventable deaths in New Zealand In a population
ACCORD, ADVANCE & VADT. Now what do I do in my practice?
 ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
ACCORD, ADVANCE & VADT Now what do I do in my practice? Richard M. Bergenstal, MD International Diabetes Center Park Nicollet Health Services University of Minnesota Minneapolis, MN richard.bergenstal@parknicollet.com
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
The CARI Guidelines Caring for Australians with Renal Impairment. Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy
 Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
Control of Hypercholesterolaemia and Progression of Diabetic Nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. All hypercholesterolaemic diabetics
American Diabetes Association: Standards of Medical Care in Diabetes 2015
 American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
American Diabetes Association: Standards of Medical Care in Diabetes 2015 Synopsis of ADA standards relevant to the 11 th Scope of Work under Task B.2 ASSESSMENT OF GLYCEMIC CONTROL Recommendations: Perform
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Diabetes Treatment Update
 Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Diabetes Treatment Update Timothy C. Evans, MD PhD FACP University of Washington Department of Medicine Disclosure: Dr. Evans has no significant financial interest in any of the products or manufacturers
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Proven and Proposed Cardiovascular Benefits of Soyfoods
 Proven and Proposed Cardiovascular Benefits of Soyfoods Mark Messina, PhD, MS Soy Nutrition Institute Loma Linda University Nutrition Matters, Inc. markjohnmessina@gmail.com Alpro Foundation 20 years symposium
Proven and Proposed Cardiovascular Benefits of Soyfoods Mark Messina, PhD, MS Soy Nutrition Institute Loma Linda University Nutrition Matters, Inc. markjohnmessina@gmail.com Alpro Foundation 20 years symposium
Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review.
 ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
ISPUB.COM The Internet Journal of Cardiovascular Research Volume 7 Number 1 Statins in the Treatment of Type 2 Diabetes Mellitus: A Systematic Review. C ANYANWU, C NOSIRI Citation C ANYANWU, C NOSIRI.
Pasta: A High-Quality Carbohydrate Food
 Pasta: A High-Quality Carbohydrate Food Cyril W.C. Kendall Department of Nutritional Sciences, Faculty of Medicine, University of Toronto; Clinical Nutrition & Risk Factor Modification Center, St. Michael
Pasta: A High-Quality Carbohydrate Food Cyril W.C. Kendall Department of Nutritional Sciences, Faculty of Medicine, University of Toronto; Clinical Nutrition & Risk Factor Modification Center, St. Michael
Glycemic control a matter of life and death
 Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Glycemic control a matter of life and death Linda Garcia Mellbin MD PhD Specialist in Cardiology & Internal medicine Dep of Cardiology Karolinska University Hospital /Karolinska Institutet Mortality (%)
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Identification of subjects at high risk for cardiovascular disease
 Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Identification of subjects at high risk for cardiovascular disease Lars Rydén Karolinska Institutet
Master Class in Preventive Cardiology Focus on Diabetes and Cardiovascular Disease Geneva April 14 2011 Identification of subjects at high risk for cardiovascular disease Lars Rydén Karolinska Institutet
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Nutritional Recommendations for the Diabetes Managements
 In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
In the name of God Nutritional for the Diabetes Managements Zohreh Mazloom. PhD Shiraz University of Medical Sciences School of Nutrition and Food Sciences Department of Clinical Nutrition OVERVIEW Healthful
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management
 Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Explore the Rationale for the Dual Mechanism CCB/ARB Approach in Hypertension Management Jeong Bae Park, MD,PhD Dept of Med/Cardiology, Cheil General Hospital, Kwandong University College of Medicine Apr
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Prof. Renata Cífková, MD, CSc.
 Prof. Renata Cífková, MD, CSc. Head of the Department of Preventive Cardiology, Thomayer Teaching Hospital, Prague Focuses on arterial hypertension epidemiology, clinical trials, target organ damage prevention
Prof. Renata Cífková, MD, CSc. Head of the Department of Preventive Cardiology, Thomayer Teaching Hospital, Prague Focuses on arterial hypertension epidemiology, clinical trials, target organ damage prevention