Saint-Antoine Hospital, Paris. Medical Intensive Unit Care. Hafid Ait-Oufella, MD.PhD. Dyscalcemia. Dyskalemia
|
|
|
- Annabelle Dean
- 6 years ago
- Views:
Transcription

1 Dyskalemia Dyscalcemia Hafid Ait-Oufella, MD.PhD. Medical Intensive Unit Care Saint-Antoine Hospital, Paris

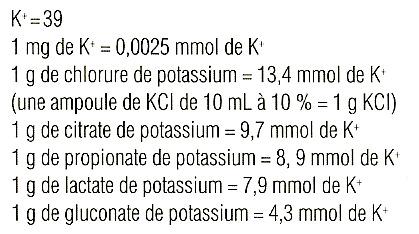
2 Potassium K + Molecular weight: 39 1gr K + =2.5mmol
3 Potassium disorders in ICU : Our experience Jul 1997 Dec patients Kalemia < 2,5 mmol/l, n = 1 Kaliemia > 6,5 mmol/l, n = 15 Kaliemia > 7 mmol/l, n = 10
4 Potassium: balance & distribution Western Diet: 100mEq K + K + Stool: 10 meq Urine: 90 meq
5 Distribution of Potassium Extracellular fluid Intracellular fluid K + = meq/l K + = meq/l 350 meq (10%) 3150 meq (90%) Plasma (0.4%) Interstitium (1%) Bone (8.6%) Muscle (75%) Liver (7%) Red cells (7%)
6 Potassium: balance & distribution Western Diet: 100mEq K + K + Stool: 10 meq Urine: 90 meq
7 Na+ Insulin 2K+ ATPase H+ Na+ 3Na+ ATPase 2K+ ß2 agonists
8 Distal convolted tubule Glomerulus Proximal convolted tubule Henle s loop Aldosterone Na 2+ K+
9 Hyperkalemia
10 Mechanisms of hyperkalemia Increase intake Oral (?) Perfusion Cellular Lysis Tumor lysis ExtraC transfer Acidosis Insulinopenia ß-adrenergic blockade K+ K+ Rabdomyolysis Hemolysis Catabolic state Digitalis intoxication Stool Urine Decreased renal excretion Renal failure K+ sparing diuretics NSAI drugs ACE inhibitors Mineralocorticoids deficiency
11 Hyperkalemia >6.5mmol/L our experience (5 years) N = 50 (1,1 %) Uree 28,8 + 22,1 mmol/l Drugs, n = 29 (58 %) ACE inhibitors (n = 10) K sparing diuretics (n = 10) Potassium per os (n = 8) Heparin (n = 7) NSAI drugs (n = 6) Betablockers (n = 6) Drugs association n=1 (13pts ); n=2 (10pts) ; n=3 (5pts) ; n=4 (1pt) Co-morbidity : Chronic renal failure n = 10, Diabetes n = 8 Age > 60 ans n=35 Age > 80 ans n=19
12 Messages Hyperkalemia frequently occurs in old patients with diabetes that have combination of nephrotoxic drugs. Life-threatening hyperkalemia is (almost) always associated with renal failure
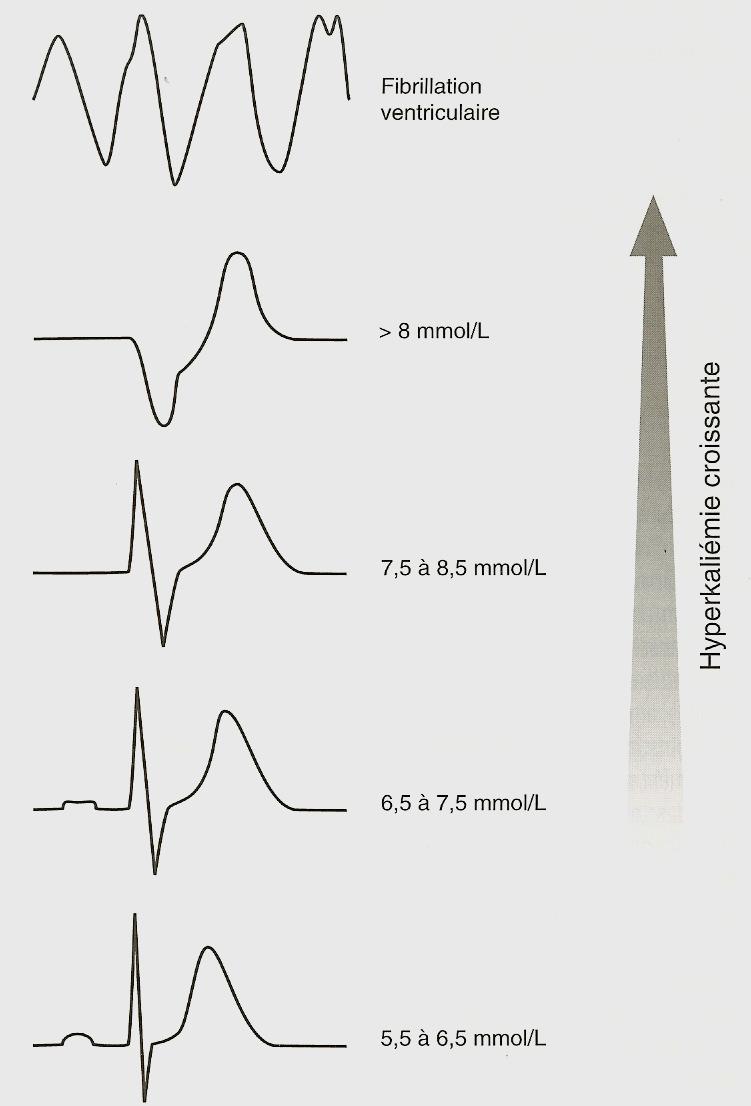
13 -120 Hyperpolarisation 37 C -100 THIN QRS fin QRS Silent Potentially lethal Induces cardiac arythmia Potentiel de membrane (mv) Membrane potential LARGE QRS QRS large Em=Tx1,7x Log10 (Ke/Ki) Dépolarisation Kaliémie (mmol/l) Hyperkalemia
 Genetic susceptibility No threshold")
14 Hyperkalemia & cardiac arythmia ECG modifications and cardiac arythmia depend on : Potassium level Time over which hyperkaliemia develops Co-morbidities Others electrolytic disorders Drugs (Digitalis) Genetic susceptibility No threshold for arythmia!



15 Mr A.., 27-year-old, chronic hemodialysis, feeling of faintness K: 7,1 mmol/l HCO3: 27 mmol/l After dialysis K: 4,5 mmol/l Day1 K: 5,2 mmol/l
16

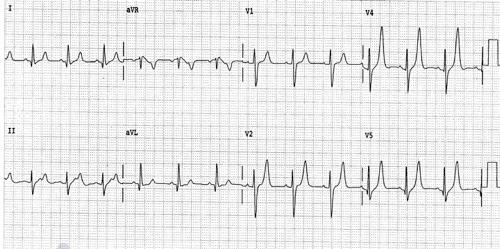
17 Message Hyperkalemia = Electrocardiogramm Modification QRS widening No ECG modification Emergency Caution
 K: 9,6 mmol/l Ph: 7,08 HCO3: 13 mmol/l 20mL calcium gluconate (10%) After dialysis K + : 3.")
18 Hyperkaliemia: treatment (1) ECG modifications: Calcium chloride (5ml of 10% solution) or calcium gluconate (10mL of 10% solution) K: 9,6 mmol/l Ph: 7,08 HCO3: 13 mmol/l 20mL calcium gluconate (10%) After dialysis K + : 3.1mmol/L
19 Hyperkalemia: treatment (2) Shift K+ into cells : minutes Product Doses Caution Glucose/ insulin Rapid Insulin Dextrose 10% 100ml Dextrose 10% glycemia 10UI Insulin Alkalinization Sodium bicarbonate ml Pulmonary overload ß2 adrenergic agonists Salbutamol Nebulization 1mg Sodium polystyrene sulfonate Binding resins: 1-2 hours kayexalate g every 4 hours Gut obstruction Threatening hyperkalemia
20 Hyperkalemia: treatment (3) Medical managment of hyperkalemia is the first step with ECG monitoring Dialysis is the definitive treatment Dialysis could be delayed or avoided if diuresis restarts
21 Hypokalemia
22 Mechanisms of hypokalemia Vomiting nasogastric drainage IntraC transfer Alkalosis Insulin ß-adrenergic agonists K+ K+ Theophyllin Intestinal losses Diarrhea Laxative abuse Stool Urine Increased renal excretion
23 Renal loss of potassium Potassium concentration in urines is high Normal blood pressure : Diuretics hypomagnesaemia Renal tubular acidosis Genetic defect (Bartter s syndrom, Gitelman s syndrom) High blood pressure Increased aldosterone : Primary (low renin) Secondary (high renin)
24 N = 22 Hypokalemia <2mmol/L our experience (5 years) Kalemia: 1,8 + 0,3 mmol/l No death Psychiatric disease et/ou denutrition, n = 11 (50 %) Diarrhea and/or vomiting, n = 18 (82 %) ph : 7,56 + 0,11 HCO3- : 40,3 + 15,7 mmol/l Drugs n = 7 Diuretics n = 7 Laxative n = 4 Beta 2 agonists n = 1
25 Clinical manifestations of hypokalemia Electrocardiogramm modifications and arythmia! Neuromuscular - Constipation/ileus - Weakness/cramps - Myalgies/ Rabdomyolysis - Paralysis
26 Hypokalemia : electrocardiogramm U wave U wave > T wave U/T wave fusion Sagging of ST segment Flattening of T wave QRS widening
27 Message : Do not treat numbers! K=1.5mmol/l
28 Treatment of hypokalemia ECG modification Intravenous potassium supplementation Infusion<1.5g/h Treating the underlying condition Magnesium supplementation

29 Magnesium depletion is frequently associated with hypokalemia Whang, Arch Int Med 1985
30 Treatment of hypokalemia Treating the underlying condition ECG modification No ECG modification Intravenous potassium supplementation No emergency Potassium supplementation Infusion<1.5g/h Magnesium supplementation
31 K supplementation
32 Conclusion Dyskalemia is not exceptional Dyskalemia could induce lethal cardiac arythmia Do not treat numbers! Management of dyskalemia depends on ECG modification
33
34 Hypercalcemia Admission in ICU for hypercalcemia is now exceptional since biphophonates use
35 Hypercalcemia : definition ionized Protein phosphate/citrate Elevated calcium level in the blood >105mg/l (2.6mmol/l) Adjusted Ca = Ca measured + [(40-albumin) X 0.025] Ionized Calcium level in the blood >53mg/l (1.3mmol/l)
36 Calcium metabolism Calcium : 1Kg 99% bone
37 Calcium metabolism
38 Hypercalcemia - Malignancy Multiple myeloma Metastasis (breast, lung, thyroid,kidney) - Hyperparathyroidism Malignancy and hyperparathyroidism represent 90% of hypercalcemia causes - Others : Vitamin D disorders (Vitamin D intoxication, sarcoidosis ) Chronic renal failure High bone turn over (hyperthyroidism, Paget s disease )
39 Clinical manifestations of hypercalcemia Symptoms of hypercalcemia are NOT SPECIFIC, depend on the underlying cause of the disease, the time over which it develops and the overall physical health of the patient. Nausea, vomiting,constipation, abdominal pain Polyuria-polydipsia Weakness Alteration of mental status, confusion, coma ECG : tachycardia, shortening of QT interval and risk of cardiac arythmia (digitalis treatment)
40 Treatment of hypercalcemia Treatment of the underlying disease Hydratation Hypokalemia correction Name Action time Indications Mechanisms Biphosphonates Calcitonin Corticosteroids Gallium nitrate Pamidronate Etidronate Clodronate Cibacalcin Methyl prednisolone Ganite hours 6-12 hours Few days Few days Reference Emergency Metastasis, myeloma, sarcoidosis Inhibition of bone resorption Inhibition of bone reabsorption and increase renal excretion Increase urinary excretion decrease intestinal absorption Inhibition of bone resorption
41 Hypocalcemia Hypocalcemia is not a problem in ICU Calcium level in the blood <90mg/l (2.1mmol/l) Ionized Calcium level in the blood <45mg/l (1.1mmol/l) Mechanisms of hypocalcemia - Hypoparathyroidism - Peripheral resistance to parathormon Clinical manifestations are not specific - Perioral tigling, parasthesia, tetany, carpopedal spasm - Trousseau s sign Chvosteck s sign Treatment : calcium gluconate 10%, 20ml if hypocalcemia is severe
42 Conclusion Dyskalemia could induce lethal cardiac arythmia ECG analysis has a crucial role to manage dyskalemia Life-threatening hypercalcemia is now exceptional since biphophonates use
43 Question 1 Was is the first think(s) to do in front of hyperkalemia? A) Injection of calcium gluconate B) Electrocardiogramm C) Measure calcemia D) Analyze patient s medications E) Dialysis
44 Question 2 The risk of cardiac arythmia induced by hyperkalemia depends on : A) Potassium level B) Time of hyperkalemia development C) Overall physical health D) Associated dyscalcemia E) Doesn t exist when kalemia <6.5mmol/l
45 Question 3 About hypokalemia: A) Hypokalemia is the most frequent electrolytic disorder in ICU B) ECG has to been done only if K + <2mmol/l C) Hypermagnesemia is frequently associated with hypokalemia D) Hypokalemia could induce torsade E) Intravenous potassium replacement is required if K + <2mmol/l
46 Question 4 Hypercalcemia : A) Is a daily problem in ICU B) Induces cardiac arythmia C) Is prevented by bisphophonates D) Is always associated with renal failure E) Requires hydratation
47 Clinical case 96-year-old patient admitted for arterial hypotension Severe diarrhea for 5 days with fever Her medications include thiazidique diuretic & ACE inhibitor for hypertension and insulin for diabetes. Arterial Pressure: 90/60, 125 beats/mn, clinical signs of deshydration, no urine in urinary catheter. Na 130mmol/l, K 6,8 mmol/l, Urea 45mmol/l, creatinine 610µmol/l, HCO3 17mmol/l, glycemia 12mmol/l
48 ECG
49 Hydratation and alkalinization Isotonic saline solution 1000ml + Sodium bicarbonate ml Kayexalate 100g orally H1: diuresis restarts 50ml H0 H4 H8 H24 K HCO Creatinine Urinary output (ml/h)
50 Clinical case 25-year-old patient was admitted in emergency room for feeling faintness Clinical examination is normal, no fever No chronic medication Na 137mmol/l, K 7.8mmol/l, urea 3mmol/l, creatinine 54µmol/l, HCO3 22mmol/l. How do you manage hyperkalemia?
Electrolyte Imbalance and Resuscitation. Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine
 Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
Electrolyte Imbalance and Resuscitation Dr. Mehmet Okumuş Sütçü Imam University Faculty of Medicine Department of Emergency Medicine Presentation plan Definition of the electrolyte disturbances Conditions
WATER, SODIUM AND POTASSIUM
 WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
WATER, SODIUM AND POTASSIUM Attila Miseta Tamás Kőszegi Department of Laboratory Medicine, 2016 1 Average daily water intake and output of a normal adult 2 Approximate contributions to plasma osmolality
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Nephrology / Urology. Hyperkalemia Causes and Definition Lecturio Online Medical Library. Definition. Epidemiology of Hyperkalemia.
 Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
Nephrology / Urology Hyperkalemia Causes and Definition Lecturio Online Medical Library See online here Hyperkalemia is defined by the serum potassium level when it is higher than 5.5mEq/L. It is usually
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 7 Caring for Clients with Altered Fluid, Electrolyte, or Acid-Base Balance Water Primary component of
ELECTROLYTES RENAL SHO TEACHING
 ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
ELECTROLYTES RENAL SHO TEACHING Metabolic Alkalosis 2 factors are responsible for generation and maintenance of metabolic alkalosis this includes a process that raises serum bicarbonate and a process that
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
3.Which is not a cause of hypokalemia? a) insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD
 insulin administration b) adrenaline infusion c) alkalosis d) toluene toxicity e) digoxin OD") Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Fluids and Electrolytes MCQs 1Which is incorrect with regards to the fluid and its content? a) Normal Saline 150mmol Na+/L b) Hartmans 131mmol Na+/L c) Hartmans 131mmolCl-/L d) D5W- 50gm glucose/l e) Hartmans-
Normal range of serum potassium is meq/l true hyperkalemia manifests clinically as : Clinical presentation : muscle and cardiac dysfunction
 Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Potassium Disorders hyperkalemia Potassium is mainly an cation? What is the major physiological role of potassium in the body? What is the major regulatory system of serum potassium level? Which part of
Electrolytes and other equally exciting topics
 Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Electrolytes and other equally exciting topics Rebecca A. Snyder Summer School 2010 Why do we care? Why do we care? Why do we care? Torsades is bad. Because medical records cares even more. Because apparently
Instrumental determination of electrolytes in urine. Amal Alamri
 Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
Instrumental determination of electrolytes in urine Amal Alamri What is the Electrolytes? Electrolytes are positively and negatively chargedions, Found in Within body's cells extracellular fluids, including
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Volume and Electrolytes. Fluid and Electrolyte Management. Why 125ml? Question. Normal fluid requirement. Normal losses
 Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Volume and Electrolytes Fluid and Electrolyte Management Pre-existing deficits of excesses Ongoing losses or gains Ajai K. Malhotra, MD VCU School of Medicine 1 2 Question Why 125ml? Intern said so Chief
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
ECG & ELECTROLYTES IMBALANCE
 ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
ECG & ELECTROLYTES IMBALANCE Ayman Khairy, MD Ass. Prof. of Cardiovascular Medicine Assiut University, EGYPT Mohamed Aboel-Kassem, MD Lecturer of Cardiovascular Medicine Assiut University, EGYPT Systematic
VanderbiltEM.com. ACEP 2013 Electrolyte Emergencies. Mastering Emergency Medicine. Electrolyte Emergency Questions. Electrolyte Emergency Questions
 ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
ACEP 2013 Electrolyte Emergencies VanderbiltEM.com Camiron L. Pfennig, M.D. Corey M. Slovis, M.D. Vanderbilt University Medical Center Nashville, TN Mastering Emergency Medicine Secure the ABC s Consider
Hypocalcemia 6/8/12. Normal value. Physiologic functions. Nephron a functional unit of kidney. Influencing factors in Calcium and Phosphate Balance
 Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
Normal value Hypocalcemia Serum calcium Total mg/dl Ionized mg/dl Cord blood 9.0 ~ 11.5 5.0 ~ 6.o New born (1 st 24 hrs) 9.0 ~ 10.6 4.3 ~ 5.1 24~ 48 hrs 7.0 ~12.0 4.0 ~4.7 Child 8.8 ~10.8 4.8 ~4.92 There
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults
 NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
NHS Grampian Staff Guideline for the Management of Acute Hypokalaemia in Adults Co-ordinators: Medicines Information Pharmacist Consultation Group: See relevant page in guidance Approver: Medicine Guidelines
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Major intra and extracellular ions Lec: 1
 Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Major intra and extracellular ions Lec: 1 The body fluids are solutions of inorganic and organic solutes. The concentration balance of the various components is maintained in order for the cell and tissue
Hyperkalemia Protect, Shift, and Eliminate
 Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
Disclosure Michael C. Thomas reports no relevant financial relationships. Lytes Off in Vegas! The Acute Management of Potassium and Calcium Disorders Program Objectives Design a plan to replace and monitor
TUBULOPATHY Intensive Care Unit Sina Hospital
 TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
TUBULOPATHY Intensive Care Unit Sina Hospital A 13 years old female who is known case of Scoliosis. She was operated 2 months ago for spinal curve repair. PMH:EMG-MCV In 2 years old =>No Motoneuron Disease
Potassium A NNA VINNIKOVA, M. D.
 Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
Potassium A NNA VINNIOVA, M. D. DIVISION OF NEPHROLOGY Graphics by permission from The Fluid, Electrolyte and Acid-Base Companion, S. Faubel and J. Topf, http://www.pbfluids.com Do you want to hear a Sodium
A Mnemonic for the Treatment of Hyperkalemia. Nick Wolters, PGY1 Resident Grandview Medical Center
 A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
A Mnemonic for the Treatment of Hyperkalemia Nick Wolters, PGY1 Resident Grandview Medical Center Hyperkalemia 30 YOF, ESRD, missed 2 dialysis sessions over the last week Potassium level came back at 7
Water, Electrolytes, and Acid-Base Balance
 Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Chapter 27 Water, Electrolytes, and Acid-Base Balance 1 Body Fluids Intracellular fluid compartment All fluids inside cells of body About 40% of total body weight Extracellular fluid compartment All fluids
Na concentration in the extracellular compartment is 140
 هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
هللامسب Na regulation: Na concentration in the extracellular compartment is 140 meq\l. Na is important because: -It determines the volume of extracellular fluid : the more Na intake will expand extracellular
K+ Ann Crawford, RN, PhD, CNS, CEN
 Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hyperkalemia: Management of a Critical Electrolyte Disturbance K+ Ann Crawford, RN, PhD, CNS, CEN Balancing Fluid Intracellular fluid (ICF) Extracellular fluid (ECF) Intravascular interstitial Hormonal
Hypoglycemia, Electrolyte disturbances and acid-base imbalances
 Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Hypoglycemia, Electrolyte disturbances and acid-base imbalances Pediatric emergency PICU division Pediatric department Medical faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Hypoglycemia
Chapter 2. Fluid, Electrolyte, and Acid-Base Imbalances
 Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Chapter 2 Fluid, Electrolyte, and Acid-Base Imbalances Review of Concepts and Processes The major component of the body is water. Water is located in these compartments: Intracellular fluid (ICF) compartment
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis
 Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Investigations for Disorders of Calcium, Phosphate and Magnesium Homeostasis Tutorial for Specialist Portfolio Biomedical Scientists 03/02/2014 Dr Petros Kampanis Clinical Scientist 1. Calcium Most abundant
Potassium secretion. E k = -61 log ([k] inside / [k] outside).
![Potassium secretion. E k = -61 log ([k] inside / [k] outside).](/thumbs/80/80478709.jpg "Potassium secretion. E k = -61 log ([k] inside / [k] outside).") 1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
1 Potassium secretion In this sheet, we will continue talking about ultrafiltration in kidney but with different substance which is K+. Here are some informations that you should know about potassium;
A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor
 A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor Amy Trottier University of Calgary Internal Medicine, PGY1 November 14, 2013 2013 Rocky Mountain/ACP Internal Medicine Conference
A Case of Severe Hypomagnesemia with Long-term Use of a Proton Pump Inhibitor Amy Trottier University of Calgary Internal Medicine, PGY1 November 14, 2013 2013 Rocky Mountain/ACP Internal Medicine Conference
POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION
 POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION NAME OF THE MEDICINE Potassium Dihydrogen Phosphate Synonyms: potassium biphosphate, potassium acid phosphate, monopotassium phosphate, or monoibasic
POTASSIUM DIHYDROGEN PHOSPHATE 13.6% CONCENTRATED INJECTION NAME OF THE MEDICINE Potassium Dihydrogen Phosphate Synonyms: potassium biphosphate, potassium acid phosphate, monopotassium phosphate, or monoibasic
A case of DYSELECTROLYTEMIA. Dr. Prathyusha Dr. Lalitha janakiraman s unit
 A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
A case of DYSELECTROLYTEMIA Dr. Prathyusha Dr. Lalitha janakiraman s unit CASE SUMMARY 4 month old, female infant 1 st born to NC parents, term, b.wt: 3.25kg No neonatal hospitalization Attained head control
PP-US-DSE Relypsa, Inc. All rights reserved. Relypsa and the Relypsa logo are trademarks of Relypsa, Inc.
 1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
1 2 There are 4 main objectives that I d like to cover with you today: First, to review the definition, prevalence, and risk of hyperkalemia in certain populations Second, to review why RAASi are recommended
Chapter 24 Water, Electrolyte and Acid-Base Balance
 Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Chapter 24 Water, Electrolyte and Acid-Base Balance Total body water for 150 lb. male = 40L 65% ICF 35% ECF 25% tissue fluid 8% blood plasma, lymph 2% transcellular fluid (CSF, synovial fluid) Water Movement
Composition: Each Tablet contains. Pharmacokinetic properties:
 Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Composition: Each Tablet contains Torsemide 5/10/20/40/100mg Pharmacokinetic properties: Torsemide is well absorbed from the gastrointestinal tract. Peak serum concentrations are achieved within 1 hour
Kidneys in regulation of homeostasis
 Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Kidneys in regulation of homeostasis Assoc. Prof. MUDr. Markéta Bébarová, Ph.D. Department of Physiology Faculty of Medicine, Masaryk University This presentation includes only the most important terms
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
HYPERKALEMIA. Best Practices in Managing. in Chronic Kidney Disease
 + Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
+ Best Practices in Managing HYPERKALEMIA in Chronic Kidney Disease Hyperkalemia in Chronic Kidney Disease (CKD) Treatment with RAAS Inhibitors (RAASi) in CKD Diagnosis and Evaluation of Hyperkalemia Treatment
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION
 DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
Remember Taking Care of Patients & Managing Electrolytes is a Team Sport! EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities
 EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
EleK + trolyte Ca ++ MP Approach to Electrolyte Abnormalities 11 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Clinical Professor of Medicine Nephrology
A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease
 Case Report A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease D H Sudusinghe 1, J indrakumar 2 1 Department of Physiology, Faculty
Case Report A case of severe hyperkalaemia presenting with cardiac arrythmias: An uncommon initial manifestation of chronic kidney disease D H Sudusinghe 1, J indrakumar 2 1 Department of Physiology, Faculty
Fluids & Electrolytes
 Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Fluids & Electrolytes Keihan Golshani, MD. Assistant professor of Clinical Emergency Medicine Emergency Medicine Department, Alzahra Hospital Isfahan Universities of Medical Sciences Physiology - Backround
Electrolyte Abnormalities in the Transplant Recipient
 Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Abnormalities in the Transplant Recipient Michael J. Goldstein, MD Assistant Professor of Surgery Overview Sodium Potassium Calcium Magnesium Phosphorus Sodium Balance Na + determines extracellular
Electrolyte Emergencies
 Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
Electrolyte Emergencies Hyponatremia/hypernatremia Hypokalemia/hyperkalemia Hypocalcemia/hypercalcemia Hypomagnesemia/hypermagnesemia Hypophosphatemia/hyperphosphatemia Hyponatremia Symptomatic: headaches,
Electrolyte abnormalities are commonly associated with
 Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
Electrolyte abnormalities are commonly associated with cardiovascular emergencies. These abnormalities may cause or contribute to cardiac arrest and may hinder resuscitative efforts. In some cases therapy
CALCIUM BALANCE. James T. McCarthy & Rajiv Kumar
 CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
CALCIUM BALANCE James T. McCarthy & Rajiv Kumar CALCIUM BALANCE TOTAL BODY CALCIUM (~ 1000g in a normal 60 kg adult) - > 99% in bones - ~ 0.6% in the intracellular space - ~ 0.1% in the extracellular space
Diabetic Ketoacidosis
 Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Diabetic Ketoacidosis Definition: Diabetic Ketoacidosis is one of the most serious acute complications of diabetes. It s more common in young patients with type 1 diabetes mellitus. It s usually characterized
Physio 12 -Summer 02 - Renal Physiology - Page 1
 Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
Physiology 12 Kidney and Fluid regulation Guyton Ch 20, 21,22,23 Roles of the Kidney Regulation of body fluid osmolarity and electrolytes Regulation of acid-base balance (ph) Excretion of natural wastes
5/18/2017. Specific Electrolytes. Sodium. Sodium. Sodium. Sodium. Sodium
 Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
Specific Electrolytes Hyponatremia Hypervolemic Replacing water (not electrolytes) after perspiration Freshwater near-drowning Syndrome of Inappropriate ADH Secretion (SIADH) Hypovolemic GI disease (decreased
The Crushing Truth. Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia. Carson City Fire Department
 The Crushing Truth Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia Carson City Fire Department John Mohler, RN, BSN, CFRN, CCRN REMSA Care Flight Carson City Fire Department 1 Crushing
The Crushing Truth Crush Injury Syndrome Compartment Syndrome Acute Traumatic Ischemia Carson City Fire Department John Mohler, RN, BSN, CFRN, CCRN REMSA Care Flight Carson City Fire Department 1 Crushing
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE
 Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
Chapter 27: WATER, ELECTROLYTES, AND ACID-BASE BALANCE I. RELATED TOPICS Integumentary system Cerebrospinal fluid Aqueous humor Digestive juices Feces Capillary dynamics Lymph circulation Edema Osmosis
50% Concentrated Injection
 NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
NAME OF THE MEDICINE. The molecular weight of the compound is 246.5 and the CAS registry number is 10034-99-8. The molecular formula is MgSO4, 7H2O. DESCRIPTION MAGNESIUM SULFATE HEPTAHYDRATE 50% CONCENTRATED
PRINCIPLES OF DIURETIC ACTIONS:
 DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
DIURETIC: A drug that increases excretion of solutes Increased urine volume is secondary All clinically useful diuretics act by blocking Na + reabsorption Has the highest EC to IC ratio = always more sodium
Electrolyte Disorders in ICU. Debashis Dhar
 Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Electrolyte Disorders in ICU Debashis Dhar INTRODUCTION Monovalent ions most important Na,K main cations and Cl &HCO - 3 main anions Mg,Ca & Phosphate are major divalent ions Normal Physiology Body tries
Hyperkalemia. Katarzyna Bigaj PGY -1
 Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Hyperkalemia Katarzyna Bigaj PGY -1 Definition Hyperkalaemia is defined as a potassium level > 5.5 meq/l Moderate hyperkalaemia is a serum potassium > 6.0 meq/l Severe hyperkalaemia is a serum potassium
Acute Kidney Injury in the ED
 + Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
+ Acute Kidney Injury in the ED + Dr Eric Clark, MD FRCPC University of Ottawa Canada Canadian Association of Emergency Physicians + Outline 1. Diagnostic challenges 2. ED treatment 3. Contrast induced
Chapter 20 8/23/2016. Fluids and Electrolytes. Fluid (Water) Fluid (Water) (Cont.) Functions
 Fluid (Water) (Cont.) Functions") Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
Chapter 20 Fluids and Electrolytes All items and derived items 2015, 2011, 2006 by Mosby, Inc., an imprint of Elsevier Inc. All rights reserved. Fluid (Water) Functions Provides an extracellular transportation
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
FLUIDS AND ELECTROLYTES
 FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
FLUIDS AND ELECTROLYTES J a s leen G r ewal, M D J u ly 2 017 A d a p te d f ro m B indu S waro o p, M D W illiam G r a h a m, M D S a m Lai, M D FLUIDS & ELECTROLY TES: OBJECTIVES Understand replacement
CSI (Clinical Scenario Investigation): Hyperkalemia
: Hyperkalemia") CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
CSI (Clinical Scenario Investigation): Hyperkalemia Alison Thomas, RN(EC), MN, CNeph(C) Ann Jones, RN(EC), MSN, CNeph(C) Joyce Hunter, RN, Vascular Access Co-ordinator Simcoe Muskoka Regional Kidney Care
Chapter 21. Diuretic Agents. Mosby items and derived items 2008, 2002 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
Chapter 21 Diuretic Agents Renal Structure and Function Kidneys at level of umbilicus Each weighs 160 to 175 g and is 10 to 12 cm long Most blood flow per gram of weight in body 22% of cardiac output (CO)
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09. Terminal Learning Objective. References. Hours: 2.0 Last updated: November 2015
 SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
SOCM Fluids Electrolytes and Replacement Products PFN: SOMRXL09 Hours: 2.0 Last updated: November 2015 Slide 1 Terminal Learning Objective Action: Communicate knowledge of Fluid, Electrolyte, and Acid
Diuretics having the quality of exciting excessive excretion of urine. OED. Inhibitors of Sodium Reabsorption Saluretics not Aquaretics
 Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
Diuretics having the quality of exciting excessive excretion of urine. OED Inhibitors of Sodium Reabsorption Saluretics not Aquaretics 1 Sodium Absorption Na Entry into the Cell down an electrochemical
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia
 BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
BCCA Protocol Summary Guidelines for the Diagnosis and Management of Malignancy Related Hypercalcemia Protocol Code Tumour Group Supportive Care Group Contacts SCHYPCAL Supportive Care Lisa Wanbon (VIC)
PRODUCT MONOGRAPH K-DUR. (Potassium Chloride) Sustained Release Tablets mg - 20 mmol (meq)
 Sustained Release Tablets mg - 20 mmol (meq)") PRODUCT MONOGRAPH K-DUR (Potassium Chloride) Sustained Release Tablets 1500 mg - 20 mmol (meq) Merck Canada Inc. 16750 route Transcanadienne Kirkland, Quebec H9H 4M7 DATE OF PREPARATION: March 2, 2011
PRODUCT MONOGRAPH K-DUR (Potassium Chloride) Sustained Release Tablets 1500 mg - 20 mmol (meq) Merck Canada Inc. 16750 route Transcanadienne Kirkland, Quebec H9H 4M7 DATE OF PREPARATION: March 2, 2011
NORMAL POTASSIUM DISTRIBUTION AND BALANCE
 NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
NORMAL POTASSIUM DISTRIBUTION AND BALANCE 98% of body potassium is contained within cells, principally muscle cells, and is readily exchangeable. Only 2% is in ECF. Daily intake exceeds the amount in ECF.
diabetes in adults Metabolic complications of
 Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Metabolic complications of diabetes in adults Dimitri MARGETIS MD ICU St ANTOINE PARIS Definition Diabetic acidoketosis Serious complication in type I diabetes : Hyperglycemia Metabolic acidosis Acidic
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Acid Base Balance. Chapter 26 Balance. ph Imbalances. Acid Base Balance. CO 2 and ph. Carbonic Acid. Part 2. Acid/Base Balance
 Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
Acid Base Balance Chapter 26 Balance Part 2. Acid/Base Balance Precisely balances production and loss of hydrogen ions (ph) The body generates acids during normal metabolism, tends to reduce ph Kidneys:
ECG Metabolic Abnormalities. Joe M. Moody, Jr, MD UTHSCSA and STVAHCS
 ECG Metabolic Abnormalities Joe M. Moody, Jr, MD UTHSCSA and STVAHCS Electrolyte Disturbances with Significant ECG Effects Hyperkalemia, hypokalemia Hypercalcemia, hypocalcemia Hypothermia Hyperkalemia
ECG Metabolic Abnormalities Joe M. Moody, Jr, MD UTHSCSA and STVAHCS Electrolyte Disturbances with Significant ECG Effects Hyperkalemia, hypokalemia Hypercalcemia, hypocalcemia Hypothermia Hyperkalemia
Hyponatremia and Hypokalemia
 Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
Hyponatremia and Hypokalemia Critical Care in the ED March 21 st, 2019 Hannah Ferenchick, MD 1 No financial disclosures 2 1 Outline: 1. Hyponatremia Diagnosis Initial treatment 2. Hyperkalemia Diagnosis
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018
 CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
CRRT Interactive Hyperkalemia Cases AKI & CRRT conference 2018 Case 1 Potassium Clearance A 70 kg male is placed on CVVH with a total ultrafiltration rate (effluent rate) of 20 ml/kg/hr. The Blood Flow
Composition of Body Fluids
 Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Water and electrolytes disturbances Fluid and Electrolyte Disturbances Hao, Chuan-Ming MD Huashan Hospital Sodium balance Hypovolemia Water balance Hyponatremia Hypernatremia Potassium balance Hypokelemia
Renal Quiz - June 22, 21001
 Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
Renal Quiz - June 22, 21001 1. The molecular weight of calcium is 40 and chloride is 36. How many milligrams of CaCl 2 is required to give 2 meq of calcium? a) 40 b) 72 c) 112 d) 224 2. The extracellular
K-TAB (potassium chloride extended-release tablets, USP)
") K-TAB (potassium chloride extended-release tablets, USP) DESCRIPTION K-TAB (potassium chloride extended-release tablets) is a solid oral dosage form of potassium chloride containing 8 meq, 10 meq and 20
K-TAB (potassium chloride extended-release tablets, USP) DESCRIPTION K-TAB (potassium chloride extended-release tablets) is a solid oral dosage form of potassium chloride containing 8 meq, 10 meq and 20
SEVERE HYPERKALEMIA WITHOUT ELECTROCARDIOGRAPHIC CHANGES IN A PATIENT WITH ADDISON DISEASE
 Case Report doi: 10.4183/aeb.2010.251 SEVERE HYPERKALEMIA WITHOUT ELECTROCARDIOGRAPHIC CHANGES IN A PATIENT WITH ADDISON DISEASE S. Isik 1, D. Berker* 1, Y. Aydin 2, U. Ozuguz 1, Y. Tutuncu 1, Y. Simsek
Case Report doi: 10.4183/aeb.2010.251 SEVERE HYPERKALEMIA WITHOUT ELECTROCARDIOGRAPHIC CHANGES IN A PATIENT WITH ADDISON DISEASE S. Isik 1, D. Berker* 1, Y. Aydin 2, U. Ozuguz 1, Y. Tutuncu 1, Y. Simsek
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES
 GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
GUIDELINE FOR THE MANAGEMENT AND PREVENTION OF ACUTE TUMOUR LYSIS SYNDROME IN HAEMATOLOGICAL MALIGNANCIES Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target
H 2 O, Electrolytes and Acid-Base Balance
 H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
H 2 O, Electrolytes and Acid-Base Balance Body Fluids Intracellular Fluid Compartment All fluid inside the cells 40% of body weight Extracellular Fluid Compartment All fluid outside of cells 20% of body
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title.
 Author: Contact Name and Job Title.") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title of Fluid and Electrolytes in Neonates D2 (prev.d14) Version 3 : Dr. Ai May Lee,
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Author: Contact Name and Job Title of Fluid and Electrolytes in Neonates D2 (prev.d14) Version 3 : Dr. Ai May Lee,
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
K+ Na+ Na+ Na+ 4/28/2018. What does Potassium do for you? Regulation of Muscle and Nerve Function. Regulation of Muscle and Nerve Function
 What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
What does Potassium do for you? Aids in the conversion of glucose into glycogen Assists in carbohydrate and protein metabolism 2018 Spring Fling EMS Conference Maintains balance between cells and body
DBL CALCIUM GLUCONATE INJECTION BP
 Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
Description DBL CALCIUM GLUCONATE INJECTION BP DBL Calcium Gluconate Injection BP is a clear, colourless solution containing in each 10 ml, Calcium Gluconate BP 953 mg and Calcium Saccharate U.S.P. 30
Metabolic Alkalosis: Vomiting
 RENAL ANL) ACID-BASE PHYSIOLOGY 213 Case 37 Metabolic Alkalosis: Vomiting Maria Cuervo is a 20-year-old philosophy major at a state university. When the "24-hour" stomach flu went around campus during
RENAL ANL) ACID-BASE PHYSIOLOGY 213 Case 37 Metabolic Alkalosis: Vomiting Maria Cuervo is a 20-year-old philosophy major at a state university. When the "24-hour" stomach flu went around campus during
ISPUB.COM. Electrolyte Replacement: A Review. B Phillips INTRODUCTION ELECTROLYTES I. CALCIUM
 ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
ISPUB.COM The Internet Journal of Internal Medicine Volume 5 Number 1 Electrolyte Replacement: A Review B Phillips Citation B Phillips. Electrolyte Replacement: A Review. The Internet Journal of Internal
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Management of Acute Kidney Injury in the Neonate. Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital
 Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Management of Acute Kidney Injury in the Neonate Carolyn Abitbol, M.D. University of Miami Miller School of Medicine / Holtz Children s Hospital Objectives Summarize the dilemmas in diagnosing & recognizing
Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari
![Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari](/thumbs/90/104323364.jpg "Pharmacology I [PHL 313] Diuretics. Dr. Mohammad Nazam Ansari") Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Pharmacology I [PHL 313] Diuretics Dr. Mohammad Nazam Ansari Renal Pharmacology Kidneys: Each adult kidney weighs 125-170g in males and 115-155g in females, represent 0.5% of total body weight, but receive
Diuretic Use in Neonates
 Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
Neonatal Nursing Education Brief: Diuretic Use in the Neonate http://www.seattlechildrens.org/healthcareprofessionals/education/continuing-medical-nursing-education/neonatalnursing-education-briefs/ Diuretics
DIURETICS. Assoc. Prof. Bilgen Başgut
 DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
DIURETICS Assoc. Prof. Bilgen Başgut Classification of Diuretics The best way to classify diuretics is to look for their Site of action in the nephron A. Diuretics that inhibit transport in the Proximal
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University
 RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)
RENAL FAILURE IN CHILDREN Dr. Mai Mohamed Elhassan Assistant Professor Jazan University OBJECTIVES By the end of this lecture each student should be able to: Define acute & chronic kidney disease(ckd)