Nephrology Grand Rounds. Vasishta Tatapudi, MD January 24 th, 2013
|
|
|
- Arthur Burke
- 6 years ago
- Views:
Transcription
1 Nephrology Grand Rounds Vasishta Tatapudi, MD January 24 th, 2013
2 Case Summary Chief complaint: A twenty-six year old African American female veteran presented to ER with left flank pain for two days. History of present illness: The patient complained of mild aching pain for several weeks. It worsened acutely two days prior to presentation. The patient had several episodes of similar pain in the past that resolved with bed rest. She did not report frequency, dysuria, hematuria, fever, change in bowel habits or any recent injuries.
3 Medical history: Hypertension, kidney disease, allergic rhinitis, recurrent urinary tract infections, PTSD. Surgical history: none. Medications: Lisinopril 10mg daily, loratidine 10mg daily, trimethoprim 100mg daily, citalopram 40mg daily. Allergies: Iodinated radio contrast.
4 Family history: Grandmother with ESRD, father with kidney disease. Social history: occasional alcohol use, no smoking or drug use.
5 Physical exam Vital signs: 99 F, HR 98, RR 20, BP 132/66 General: young female patient in acute distress. HEENT: normal. RS: normal vesicular breath sounds. CVS: S1, S2 normal, no added sounds. Abdomen: normal bowel sounds, no bruit, no palpable organomegaly, non tender, no guarding or rebound tenderness, no CVA tenderness. CNS: no focal deficits. Extremities: no edema, well perfused.
6 Laboratory data Hemoglobin 13.6 Sodium 141 Protein 7.9 Hematoctrit 39.1 Potassium 4.0 Albumin 4.6 MCV 83.1 Chloride 108 ALT 22 White count 5.3 Bicarbonate 24 AST 20 Platelets 374 Blood urea 24 ALP 58 Creatinine 0.6 Total Bilirubin 0.5 Glucose 107 Direct Bilirubin 0.2 Calcium 9.9 Amylase 51 AG 9.0 Lipase 24
7 Urinalysis Color Yellow Specific Gravity ph 6.5 Protein Negative Glucose Negative Bilirubin Negative Ketones Negative Blood Negative Leuk. Est. Negative EKG: normal sinus rhythm. Chest x-ray: clear lung fields. CT abdomen/pelvis w/o contrast: Innumerable bilateral renal cysts. Several are hyperdense, compatible with hemorrhagic cysts. Liver demonstrates multiple hypodense lesions compatible with cysts. Nitrite Negative RBC 0-2 WBC 0-2 Bacteria Negative

8 Polycystic kidney disease
9 Introduction Polycystic kidney disease (PKD) includes inherited diseases that cause an irreversible decline in kidney function. PKD may be inherited as an autosomal dominant or recessive trait. The autosomal dominant form (ADPKD) is the most common genetic cause of chronic kidney disease. ADPKD is caused by mutations of either PKD1 or PKD2. Patel V, et al, Curr Opin Nephrol Hypertens. 2009;18(2):99. Torres VE, Harris PC, Kidney Int. 2009;76(2):149.
10 Epidemiology Autosomal dominant PKD (ADPKD) occurs in all races. Reported prevalence is 1:400 to 1:1000. ADPKD is the underlying cause of kidney disease in approximately five percent of patients who initiate dialysis annually in the United States. It is the fourth leading cause of end-stage kidney disease in adults worldwide. Torres VE, Harris PC, Kidney Int. 2009;76(2):149
11 Epidemiology: PKD 1 vs PKD 2 PKD1 mutations are more common (approximately 85 percent) than PKD2 mutations (approximately 15 percent). The relative frequency of PKD1 and PKD2 mutations depends on the age of the population being studied. Patients with PKD2 mutations present at an older age and progress more slowly than patients with PKD1 mutations. Median age of patients who presented with renal failure is 54 and 74 years for those with PKD1 and PKD2, respectively. Rossetti S, et al, J Am Soc Nephrol. 2007;18(7):2143. Hateboer N, et al, Lancet. 1999;353(9147):103.
12 Clinical presentation Patients can present with hypertension, hematuria, proteinuria or renal insufficiency detected by routine laboratory examinations. Flank pain due to renal hemorrhage, calculi or urinary tract infection is the most common symptom reported by patients. Symptoms secondary to cysts in other organs - liver, pancreas, spleen, thyroid or epididymis. Torres VE,Lancet. 2007;369(9569):1287.

13 Progression of disease Chapman AB, et al, Kidney Disease (CRISP) cohort. Kidney, Int 2003;64: Patients develop renal enlargement prior to loss of renal function. Renal architecture is lost early. May account for the lack of successful interventional trials designed to slow the progression. It is necessary to identify reliable markers of disease progression other than renal function.
. ecrcl >70ml/min(107±28).")
14 Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease. Multicenter cohort study of 241 patients. Ages between 15 and 45(32.4±8.9). ecrcl >70ml/min(107±28). MR measurement of total renal volume, cyst volume and their relation to GFR measured by iothalamate clearance.
:1035.")
15 Chapman AB, et al, Kidney Int. 2003;64(3):1035. Standardization studies
16 Chapman AB, et al, Kidney Int. 2003;64(3):1035. Volume vs GFR
17 3 year multicenter cohort study of 241 patients. Consortium for Radiologic Imaging Studies of Polycystic Kidney Disease. Ages between 15 and 45(32.4±8.9). ecrcl >70ml/min(107±28). MR measurement of total renal volume, cyst volume and their relation to GFR measured by iothalamate clearance. Rate of growth in PKD1 vs PKD 2 patients.
:2122.")
18 Grantham, N Engl J Med. 2006;354(20):2122. Volume vs age

19 Log transformed volume vs time Grantham, N Engl J Med. 2006;354(20):2122.
20 The mean (±SD) total kidney volume was 1060±642 ml at baseline and increased by a mean of 204±246 ml over a three-year period. 5.27±3.92%per year. Total cyst volume increased by 218±263 ml (P<0.001) during the same period.
21 Grantham, N Engl J Med. 2006;354(20):2122. Volume vs volume
:2122.")
22 Baseline volume vs slope of volume and GFR Grantham, N Engl J Med. 2006;354(20):2122.
:2122.")
23 Grantham, N Engl J Med. 2006;354(20):2122. PKD1 vs PKD 2
24 Discussion Patients with the largest kidneys at a given age should have the fastest rates of renal enlargement and decline in renal function. Total kidney volume is a marker of progression of disease. This supposition has practical value in judging the prognosis in individual patients. Study has implications for the design of clinical trials in ADPKD.
25 Other risk factors for progressive disease Genetic factors (PKD1 versus PKD2). Hypertension. Early onset of symptoms including proteinuria and hematuria. Male gender. Dipstick detectable proteinuria. Low birth weight. Decreased renal blood flow. Copeptin.
26 Genetic factors Careful attention to family history may allow the prediction of the mutation. Shown in a study of 484 patients from 90 families with well-characterized ADPKD mutations. The presence of at least one family member who developed ESRD before age 55 predicted a PKD1 mutation with a positive predictive value of 100 % and a sensitivity of 72 %. The presence of at least one family member who reached 70 years of age without ESRD predicted a PKD2 mutation with a positive predictive value of 100 % and a sensitivity of 74 %. Barua, J Am Soc Nephrol. 2009;20(8):1833.
27 Approach to treatment No specific treatment has been proven to prevent or delay progression of ADPKD. Promising therapies include: Vasopressin receptor antagonists, increased water intake, maximal inhibition of the renin-angiotensin-aldosterone system, use of mtor inhibitors and rigorous blood pressure control. Non-specific measures: dietary protein restriction, a low salt diet, and statins. Supportive therapy: pain control, bed rest during gross hematuria, and treatment of infection.
28 V2R antagonists In vitro evidence suggests that increased intracellular cyclic AMP (camp) plays a role in cystogenesis. camp plays a role in cyst epithelial cell proliferation and cyst fluid secretion in patients with PKD. Vasopressin leads to increased levels of camp in distal tubular epithelial cells. The vasopressin V2 receptor antagonists OPC and tolvaptan(opc-41061) decrease camp levels, inhibit cystogenesis and prevent renal enlargement and dysfunction in three different murine models. Calvet JP, Clin J Am Soc Nephrol. 2008;3(4):1205 Torres VE, Nat Med. 2004;10(4):363.
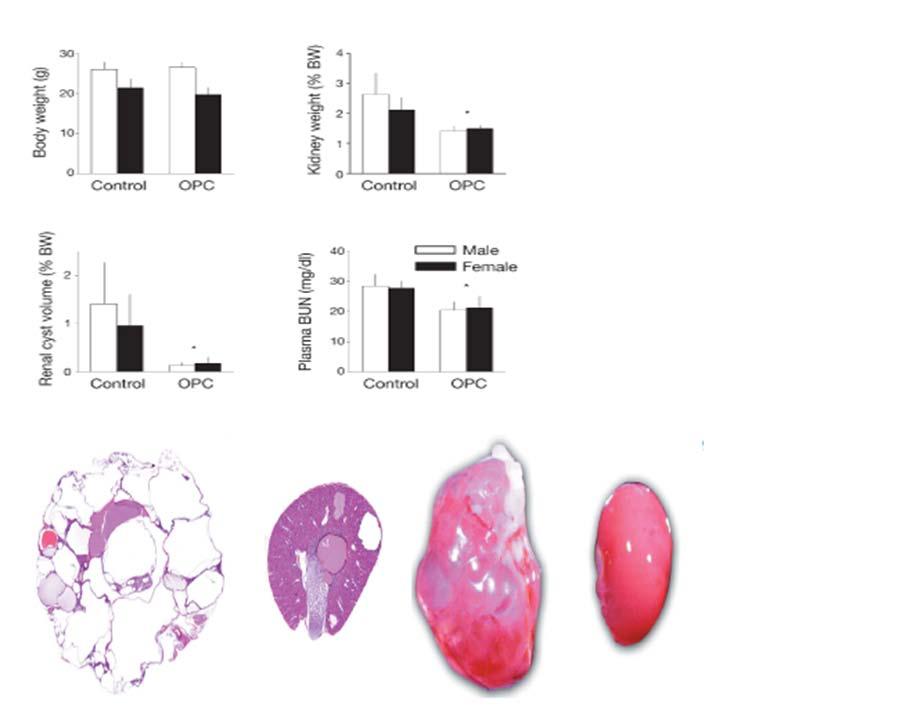
29 Torres VE, Nat Med. 2004;10(4):363. Torres VE, Nat Med. 2004;10(4):363.
30 Tolvaptan Efficacy and Safety in Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO) 3:4 trial
31 Methods 3-year, multicenter, double-blind, placebo-controlled, trial involving 1445 patients. Inclusion criteria: Patients 18 to 50 years of age, who had ADPKD with kidney volume of 750 ml or more and an estimated creatinine clearance of 60 ml per minute or more. Received tolvaptan at the highest of three twice-daily dose regimens or placebo.
32 Methods Primary outcome: annual rate of change in the total kidney volume (MRI at baseline and at months 12, 24, and 36). Secondary end points: composite of clinical progression. rate of kidney-function (inverse of Cr) decline. Composite outcome: Worsening kidney function(egfr by CKD EPI). Kidney pain. Hypertension. Albuminuria. Stratification: Age, gender, hypertension, GFR, total kidney volume.
33 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Enrollment and outcomes
34 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Enrollment and outcomes
:2407.")
35 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Baseline characteristics
:2407.")
36 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Baseline characteristics
:2407.")
37 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Baseline characteristics
38 Effect on total kidney volume Torres VE, et al, N Engl J Med. 2012;367(25):2407.
39 Effect on total kidney volume Torres VE, et al, N Engl J Med. 2012;367(25):2407.
:2407.")
40 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Effect on kidney function
41 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Effect on kidney function
:2407.")
42 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Secondary end points
43 Torres VE, et al, N Engl J Med. 2012;367(25):2407. Secondary endpoints

44 Adverse effects Torres VE, et al, N Engl J Med. 2012;367(25):2407.
45 Summary of results Over the 3-year period, total kidney volume increased by 2.8% per year (95% CI, 2.5 to 3.1) with tolvaptan versus 5.5% per year (95% CI, 5.1 to 6.0) with placebo. Slope of kidney function with a slope of 2.61 (mg per milliliter) 1 per year, as compared with 3.81 (mg per milliliter) 1 per year with placebo. Fewer ADPKD-related events with tolvaptan than with placebo (44 vs. 50 events; hazard ratio, 0.87; 95% CI, 0.78 to 0.97; P = 0.01).
46 Discussion Adverse effects and discontinuation. Long term outcome data. Tolvaptan effect on development of hypertension was not studied. Effect of water intake.
47
48 Methods 13 ADPKD patients and 10 healthy controls. The diagnosis of ADPKD was based on a positive family history and ultrasonographic diagnostic criteria. Inclusion criteria: older than 18 years, egfr > 60 ml/min per 1.73 m2 using the MDRD equation. Exclusion criteria: no history of syndrome of antidiuresis, vasopressin agonist or antagonist therapy, serum sodium concentrations of > 135 meq/l, PTH levels. (MRI) to assess kidney volumes. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
49 Methods The effects of acute and sustained water loading on levels of urine osmolality (Uosm) and camp in 13 subjects with ADPKD and 10 healthy controls were studied. Uosm and camp concentrations were measured before and after water loading. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
50 Acute water loading No food or drink for 12 hours before study visit to achieve maximal AVP secretion and urine concentration. No caffeine. A urine sample was obtained at the end of the thirsting period. 200 ml of bottled water every 15 minutes for 2.5 hours, for a total of 2L. A post-water loading urine sample was collected. All samples were aliquoted and frozen at 80 C within an hour of collection. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
51 Chronic water loading Participants collected a baseline 24-hour urine on their usual fluid intake. Subjects were then instructed to drink at least 3 L of water daily for 7 days. On days 6 and 7 of sustained water loading, participants collected two consecutive 24-hour urines, which were stored at 4 C. Aliquots of the 24-hour collections were frozen at 80 C until further analysis. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
52 Statistical analysis Changes in urine camp concentration were indexed to urine osmolality in the acute water loading part of the study to account for effects of dilution. In the chronic water loading phase, 24-hour total urine camp amount was indexed to 24-hour total urine creatinine. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
53 Baseline characteristics Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.

54 Effect of acute water load on camp Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.

55 Correlation between osmolality and camp Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
56 Effect of chronic water load on camp Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
57 Discussion Possibilities that could account for the inability to detect predictable changes in urine camp during chronic water loading: Other agonists can generate camp in the kidney, including PTH, catecholamines, caffeine, and a forskolin-like molecule Insufficient water intake to suppress AVP levels. Urine camp may not closely reflect kidney camp levels in some patients. Urine camp measurements to predict responders to water therapy. A larger longitudinal study will be needed to determine the potential of water as therapy for ADPKD using hard endpoints. Barash I, Ponda MP, Goldfarb DS, Skolnik EY, Clin J Am Soc Nephrol. 2010;5(4):693.
58 Thank you.
Autosomal Dominant Polycystic Kidney Disease. Dr. Sameena Iqbal Nephrologist CIUSSS West Island
 Autosomal Dominant Polycystic Kidney Disease Dr. Sameena Iqbal Nephrologist CIUSSS West Island Disclosure Honorarium for Consulting on the Reprise trial from Otsuka Mayo clinic preceptorship for PKD with
Autosomal Dominant Polycystic Kidney Disease Dr. Sameena Iqbal Nephrologist CIUSSS West Island Disclosure Honorarium for Consulting on the Reprise trial from Otsuka Mayo clinic preceptorship for PKD with
Autosomal dominant polycystic kidney disease (AD-
 A Pilot Clinical Study to Evaluate Changes in Urine Osmolality and Urine camp in Response to Acute and Chronic Water Loading in Autosomal Dominant Polycystic Kidney Disease Irina Barash,* Manish P. Ponda,*
A Pilot Clinical Study to Evaluate Changes in Urine Osmolality and Urine camp in Response to Acute and Chronic Water Loading in Autosomal Dominant Polycystic Kidney Disease Irina Barash,* Manish P. Ponda,*
Shuma Hirashio 1,2, Shigehiro Doi 1 and Takao Masaki 1*
 Hirashio et al. Renal Replacement Therapy (2018) 4:24 https://doi.org/10.1186/s41100-018-0164-9 CASE REPORT Open Access Magnetic resonance imaging is effective for evaluating the therapeutic effect of
Hirashio et al. Renal Replacement Therapy (2018) 4:24 https://doi.org/10.1186/s41100-018-0164-9 CASE REPORT Open Access Magnetic resonance imaging is effective for evaluating the therapeutic effect of
Introduction to Clinical Diagnosis Nephrology
 Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
Introduction to Clinical Diagnosis Nephrology I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of Florida College
New Treatments for ADPKD how close are we?
 New Treatments for ADPKD how close are we? Leicester General Hospital 28 Jan 2012 Professor Albert Ong a.ong@sheffield.ac.uk The cystic degeneration of the kidneys, once it reaches the point where it can
New Treatments for ADPKD how close are we? Leicester General Hospital 28 Jan 2012 Professor Albert Ong a.ong@sheffield.ac.uk The cystic degeneration of the kidneys, once it reaches the point where it can
A New Approach for Evaluating Renal Function and Predicting Risk. William McClellan, MD, MPH Emory University Atlanta
 A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
A New Approach for Evaluating Renal Function and Predicting Risk William McClellan, MD, MPH Emory University Atlanta Goals Understand the limitations and uses of creatinine based measures of kidney function
ADPKD, what have the last 10 years taught us? Arlene B. Chapman MD Professor of Medicine Director, Section of Nephrology University of Chicago
 2016 ADPKD, what have the last 10 years taught us? Arlene B. Chapman MD Professor of Medicine Director, Section of Nephrology University of Chicago 2016 Can we TRUMP the cysts? Disclosures Consultant for
2016 ADPKD, what have the last 10 years taught us? Arlene B. Chapman MD Professor of Medicine Director, Section of Nephrology University of Chicago 2016 Can we TRUMP the cysts? Disclosures Consultant for
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Research Introduction
 Research Introduction 9.17.13 Altered metabolism in polycystic kidney disease Telomerase activity in polycystic kidney disease cells Autosomal dominant polycystic kidney disease ADPKD is the most common
Research Introduction 9.17.13 Altered metabolism in polycystic kidney disease Telomerase activity in polycystic kidney disease cells Autosomal dominant polycystic kidney disease ADPKD is the most common
Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD)
") Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD) Cardiovascular and Renal Drugs Advisory Committee August 5, 2013 Introduction Robert McQuade, PhD Executive Vice President
Tolvaptan: Slowing Progression of Autosomal Dominant Polycystic Kidney Disease (ADPKD) Cardiovascular and Renal Drugs Advisory Committee August 5, 2013 Introduction Robert McQuade, PhD Executive Vice President
Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
 Clinical Kidney Journal, 2017, 1 5 doi: 10.1093/ckj/sfw153 Original Article ORIGINAL ARTICLE Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
Clinical Kidney Journal, 2017, 1 5 doi: 10.1093/ckj/sfw153 Original Article ORIGINAL ARTICLE Patient Survey of current water Intake practices in autosomal dominant Polycystic kidney disease: the SIPs survey
Clinical Pearls in Renal Medicine
 Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Clinical Pearls in Renal Medicine Joel A. Gordon MD Professor of Medicine Nephrology Division Staff Physician Kidney Disease and Blood Pressure Clinic Disclosures None of my financial holdings will have
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
11/9/2015. Childhood Nephrotic Syndrome: The Clinical Pathway. Learning Objectives. Nephrotic Syndrome - Definition. Proteinuria.
 Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
Childhood Nephrotic Syndrome: The Clinical Pathway Cherry Mammen, MD, FRCPC, MHSc Douglas G. Matsell, MDCM, FRCPC Division of Nephrology, BC Children s Hospital Grand Rounds Nov 13th, 2015 Learning Objectives
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Tolvaptan bei ADPKD: Kritische Beurteilung der Studien
 Tolvaptan bei ADPKD: Kritische Beurteilung der Studien Johannes Mann & Stewart Lambie * KfH Nierenzentrum München Schwabing, Klinik für Nieren- & Hochdruckkrankheiten, Friedrich Alexander Univ. Erlangen-Nürnberg
Tolvaptan bei ADPKD: Kritische Beurteilung der Studien Johannes Mann & Stewart Lambie * KfH Nierenzentrum München Schwabing, Klinik für Nieren- & Hochdruckkrankheiten, Friedrich Alexander Univ. Erlangen-Nürnberg
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist. Hirslanden, 22 March 2018 Stefan Russmann
 SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist Hirslanden, 22 March 2018 Stefan Russmann 4 th of July 2004 Database development with outcomes and safety
SUISSE ADPKD Cohort Treatment and Outcomes with Tolvaptan, first in class Vasopressin V2 Antagonist Hirslanden, 22 March 2018 Stefan Russmann 4 th of July 2004 Database development with outcomes and safety
HHS Public Access Author manuscript Am J Kidney Dis. Author manuscript; available in PMC 2017 July 05.
 HHS Public Access Author manuscript Published in final edited form as: Am J Kidney Dis. 2017 March ; 69(3): 482 484. doi:10.1053/j.ajkd.2016.10.021. Performance of the Chronic Kidney Disease Epidemiology
HHS Public Access Author manuscript Published in final edited form as: Am J Kidney Dis. 2017 March ; 69(3): 482 484. doi:10.1053/j.ajkd.2016.10.021. Performance of the Chronic Kidney Disease Epidemiology
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
3 generations of ADPKD. 1 long-awaited treatment.
 3 generations of ADPKD. 1 long-awaited treatment. HOPE is finally here now that treatment is available for people with autosomal dominant polycystic kidney disease (ADPKD). JYNARQUE is proven to slow kidney
3 generations of ADPKD. 1 long-awaited treatment. HOPE is finally here now that treatment is available for people with autosomal dominant polycystic kidney disease (ADPKD). JYNARQUE is proven to slow kidney
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression
 CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
CKDinform: A PCP s Guide to CKD Detection and Delaying Progression Learning Objectives Describe suitable screening tools, such as GFR and ACR, for proper utilization in clinical practice related to the
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin
 Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin Briefing Document for 5 August 2013 Advisory Committee Meeting
Delaying Progression of Renal Complications of Autosomal Dominant Polycystic Kidney Disease by Tolvaptan Inhibition of Arginine Vasopressin Briefing Document for 5 August 2013 Advisory Committee Meeting
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Objectives. Pre-dialysis CKD: The Problem. Pre-dialysis CKD: The Problem. Objectives
 The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
The Role of the Primary Physician and the Nephrologist in the Management of Chronic Kidney Disease () By Brian Young, M.D. Assistant Clinical Professor of Medicine David Geffen School of Medicine at UCLA
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Evaluation of Chronic Kidney Disease KDIGO. Paul E de Jong University Medical Center Groningen The Netherlands
 Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
Evaluation of Chronic Kidney Disease Paul E de Jong University Medical Center Groningen The Netherlands Evaluation and Management of CKD 1. Definition and classification of CKD 2. Definition and impact
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Documentation Dissection
 History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
History of Present Illness: Documentation Dissection The patient is a 50-year-old male c/o symptoms for past 4 months 1, severe 2 bloating and stomach cramps, some nausea, vomiting, diarrhea. In last 3
Renal Cystic Disease. Dr H Bierman
 Renal Cystic Disease Dr H Bierman Objectives Be able to diagnose renal cystic disease Genetic / non-genetic Be able to describe patterns of various renal cystic disease on routine imaging studies Be able
Renal Cystic Disease Dr H Bierman Objectives Be able to diagnose renal cystic disease Genetic / non-genetic Be able to describe patterns of various renal cystic disease on routine imaging studies Be able
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Vasishta Tatapudi, M.D. October 23 rd, 2012.
 Vasishta Tatapudi, M.D. October 23 rd, 2012. Case Summary Chief complaint: 45 year old African American male patient presented with left shoulder pain after minor trauma. History of present illness: Two
Vasishta Tatapudi, M.D. October 23 rd, 2012. Case Summary Chief complaint: 45 year old African American male patient presented with left shoulder pain after minor trauma. History of present illness: Two
Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification
 in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification") Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification Roslyn Simms NIHR Clinical Lecturer in Nephrology NIHR Clinical Trials Fellow Monday 23 rd
Total Kidney Volume (TKV) in Autosomal Dominant Polycystic Kidney Disease as model for biomarker qualification Roslyn Simms NIHR Clinical Lecturer in Nephrology NIHR Clinical Trials Fellow Monday 23 rd
Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD)
 for the treatment of autosomal dominant polycystic kidney disease (ADPKD)") Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD) The NCPE has issued a recommendation regarding the cost-effectiveness of tolvaptan (Jinarc
Cost-effectiveness of tolvaptan (Jinarc ) for the treatment of autosomal dominant polycystic kidney disease (ADPKD) The NCPE has issued a recommendation regarding the cost-effectiveness of tolvaptan (Jinarc
ADPedKD: detailed description of data which will be collected in this registry
 ADPedKD: detailed description of data which will be collected in this registry I. Basic data 1. Patient ID: will be given automatically 2. Personal information - Date of informed consent: DD/MM/YYYY -
ADPedKD: detailed description of data which will be collected in this registry I. Basic data 1. Patient ID: will be given automatically 2. Personal information - Date of informed consent: DD/MM/YYYY -
CASE-BASED SMALL GROUP DISCUSSION MHD II
 MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
MHD II, Session 11, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD II Session 11 April 11, 2016 STUDENT COPY MHD II, Session 11, Student Copy Page 2 CASE HISTORY 1 Chief complaint: Our baby
Chapter 23. Composition and Properties of Urine
 Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
Chapter 23 Composition and Properties of Urine Composition and Properties of Urine (1 of 2) urinalysis the examination of the physical and chemical properties of urine appearance - clear, almost colorless
Acknowledgements. National Kidney Foundation of Connecticut Mark Perazella. Co-PI Slowing the progression of chronic kidney disease to ESRD
 A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
A Practical Approach to Chronic Kidney Disease Management for the Primary Care Practioner: A web-site sponsored by the National Kidney Foundation of Connecticut Robert Reilly, M.D. Acknowledgements National
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
BASELINE CHARACTERISTICS OF THE STUDY POPULATION
 COMPARISON OF TREATING METABOLIC ACIDOSIS IN CKD STAGE 4 HYPERTENSIVE KIDNEY DISEASE WITH FRUITS & VEGETABLES OR SODIUM BICARBONATE This was a 1-year, single-center, prospective, randomized, interventional
COMPARISON OF TREATING METABOLIC ACIDOSIS IN CKD STAGE 4 HYPERTENSIVE KIDNEY DISEASE WITH FRUITS & VEGETABLES OR SODIUM BICARBONATE This was a 1-year, single-center, prospective, randomized, interventional
Elevation of Serum Creatinine: When to Screen, When to Refer. Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC
 Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
Elevation of Serum Creatinine: When to Screen, When to Refer Bruce F. Culleton, MD, FRCPC; and Jolanta Karpinski, MD, FRCPC Presented at the University of Calgary s CME and Professional Development 2006-2007
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Lise BANKIR. Nadine BOUBY, Daniel BICHET, Pascale BARDOUX, Julie PERUCCA, Gilberto VELHO, Ronan ROUSSEL
 Lise BANKIR Nadine BOUBY, Daniel BICHET, Pascale BARDOUX, Julie PERUCCA, Gilberto VELHO, Ronan ROUSSEL March 7 2017 INSERM Unit 1138 Cordeliers Research Center Paris, France ØIntroduction about vasopressin
Lise BANKIR Nadine BOUBY, Daniel BICHET, Pascale BARDOUX, Julie PERUCCA, Gilberto VELHO, Ronan ROUSSEL March 7 2017 INSERM Unit 1138 Cordeliers Research Center Paris, France ØIntroduction about vasopressin
tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15)
 Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15)") tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15) 04 December 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
tolvaptan 15mg, 30mg, 45mg, 60mg and 90mg tablets (Jinarc ) Otsuka Pharmaceuticals (UK) Ltd SMC No. (1114/15) 04 December 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
The National Quality Standards for Chronic Kidney Disease
 The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
The National Quality Standards for Chronic Kidney Disease Dr Robert Lewis Chief of Service, Wessex Kidney Centre, Portsmouth Specialist Committee Member Quality Standard for Chronic Kidney Disease, NICE
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358
 Tolvaptan for treating autosomal dominant polycystic kidney disease Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358 NICE 2017. All rights reserved. Subject to Notice
Tolvaptan for treating autosomal dominant polycystic kidney disease Technology appraisal guidance Published: 28 October 2015 nice.org.uk/guidance/ta358 NICE 2017. All rights reserved. Subject to Notice
Supplementary materials
 Supplementary materials Table S Adverse events identified by participants diary logs and blood hematologic and biochemical tests (n=2) group (n=) Placebo group (n=) P value for chi-squared test Asthma
Supplementary materials Table S Adverse events identified by participants diary logs and blood hematologic and biochemical tests (n=2) group (n=) Placebo group (n=) P value for chi-squared test Asthma
Chronic kidney disease in cats
 Chronic kidney disease in cats What is chronic kidney disease (CKD)? Chronic kidney disease (CKD) is the name now used to refer to cats with kidney failure (or chronic kidney failure). CKD is one of the
Chronic kidney disease in cats What is chronic kidney disease (CKD)? Chronic kidney disease (CKD) is the name now used to refer to cats with kidney failure (or chronic kidney failure). CKD is one of the
CKD IN THE CLINIC. Session Content. Recommendations for commonly used medications in CKD. CKD screening and referral
 CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
CKD IN THE CLINIC Family Physician Refresher Course Lisa M. Antes, MD April 19, 2017 No disclosures Session Content 1. 2. Recommendations for commonly used medications in CKD Basic principles /patient
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Chronic Kidney Disease: Optimal and Coordinated Management
 Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Chronic Kidney Disease: Optimal and Coordinated Management Michael Copland, MD, FRCPC Presented at University of British Columbia s 42nd Annual Post Graduate Review in Family Medicine Conference, Vancouver,
Nephrology - the study of the kidney. Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system
 Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
Urinary System Nephrology - the study of the kidney Urology - branch of medicine dealing with the male and female urinary systems and the male reproductive system Functions of the Urinary System 1. Regulation
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Clinical Experience with Tolvaptan. Prof. Dr. med. O. Devuyst
 Clinical Experience with Tolvaptan Prof. Dr. med. O. Devuyst 1 Outline 1. ADPKD generalities and tolvaptan in ADPKD 2. Who to treat with tolvaptan? How to start? 3. Clinical experience with tolvaptan in
Clinical Experience with Tolvaptan Prof. Dr. med. O. Devuyst 1 Outline 1. ADPKD generalities and tolvaptan in ADPKD 2. Who to treat with tolvaptan? How to start? 3. Clinical experience with tolvaptan in
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4:
 Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
Virtual Mentor American Medical Association Journal of Ethics April 2007, Volume 9, Number 4: 295-299. Clinical pearl Hyperkalemia: newer considerations by Amar D. Bansal and David S. Goldfarb, MD Maintenance
KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD)
") KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD) January 16 19, 2014 Edinburgh, United Kingdom Kidney Disease: Improving Global Outcomes (KDIGO) is an international
KDIGO Controversies Conference on Autosomal Dominant Polycystic Kidney Disease (ADPKD) January 16 19, 2014 Edinburgh, United Kingdom Kidney Disease: Improving Global Outcomes (KDIGO) is an international
CRRT Fundamentals Pre-Test. AKI & CRRT 2017 Practice Based Learning in CRRT
 CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
CRRT Fundamentals Pre-Test AKI & CRRT 2017 Practice Based Learning in CRRT Question 1 A 72-year-old man with HTN presents to the ED with slurred speech, headache and weakness after falling at home. He
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Predictors of Autosomal Dominant Polycystic Kidney Disease Progression
 Predictors of Autosomal Dominant Polycystic Kidney Disease Progression Robert W. Schrier,* Godela Brosnahan,* Melissa A. Cadnapaphornchai,* Michel Chonchol,* Keith Friend, Berenice Gitomer,* and Sandro
Predictors of Autosomal Dominant Polycystic Kidney Disease Progression Robert W. Schrier,* Godela Brosnahan,* Melissa A. Cadnapaphornchai,* Michel Chonchol,* Keith Friend, Berenice Gitomer,* and Sandro
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012
 Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Irish Practice Nurses Association Annual Conference Tullamore Court Hotel OCTOBER 6 th 2012 Susan McKenna Renal Clinical Nurse Specialist Cavan General Hospital Renal patient population ACUTE RENAL FAILURE
Creatinine & egfr A Clinical Perspective. Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC
 Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Creatinine & egfr A Clinical Perspective Suheir Assady MD, PhD Dept. of Nephrology & Hypertension RHCC CLINICAL CONDITIONS WHERE ASSESSMENT OF GFR IS IMPORTANT Stevens et al. J Am Soc Nephrol 20: 2305
Case Studies: Renal and Urologic Impairments Workshop
 Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Case Studies: Renal and Urologic Impairments Workshop Justine Lee, MD, DBIM New York Life Insurance Co. Gina Guzman, MD, DBIM, FALU, ALMI Munich Re AAIM Triennial October, 2012 The Company You Keep 1 Case
Primary Care Physicians and Clinicians. XXX on behalf of the Upper Midwest Fistula First Coalition. Chronic Kidney Disease (CKD) Resources
 Resources") August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
August 10, 2007 To: From: RE: Primary Care Physicians and Clinicians XXX on behalf of the Upper Midwest Fistula First Coalition Chronic Kidney Disease (CKD) Resources Caring for patients with chronic kidney
Prof. Armando Torres Nephrology Section Hospital Universitario de Canarias University of La Laguna Tenerife, Canary Islands, Spain.
 Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Does RAS blockade improve outcomes after kidney transplantation? Armando Torres, La Laguna, Spain Chairs: Hans De Fijter, Leiden, The Netherlands Armando Torres, La Laguna, Spain Prof. Armando Torres Nephrology
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Trial to Reduce. Aranesp* Therapy. Cardiovascular Events with
 Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
Trial to Reduce Cardiovascular Events with Aranesp* Therapy John J.V. McMurray, Hajime Uno, Petr Jarolim, Akshay S. Desai, Dick de Zeeuw, Kai-Uwe Eckardt, Peter Ivanovich, Andrew S. Levey, Eldrin F. Lewis,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER. The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR
 CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
CHRONIC RENAL FAILURE: WHAT THE PRIMARY CARE CAN OFFER The annual conference of the Lebanese Society of Family Medicine October 2017 Dr Hiba AZAR OUTLINE: A journey through CKD Screening for CKD: The why,
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE
 MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
MHD I SESSION X. Renal Disease
 MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
MHD I, Session X, Student Copy Page 1 CASE-BASED SMALL GROUP DISCUSSION MHD I SESSION X Renal Disease Monday, November 11, 2013 MHD I, Session X, Student Copy Page 2 Case #1 Cc: I have had weeks of diarrhea
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney Disease
 Pacific University CommonKnowledge School of Physician Assistant Studies Theses, Dissertations and Capstone Projects Fall 9-20-2013 Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney
Pacific University CommonKnowledge School of Physician Assistant Studies Theses, Dissertations and Capstone Projects Fall 9-20-2013 Tolvaptan: a Possible Treatment for Autosomal Dominant Polycystic Kidney
Autosomal dominant polycystic kidney disorder (ADPKD)
") CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.03950510 Water Prescription in Autosomal Dominant Polycystic Kidney Disease: A Pilot Study Connie J. Wang, Catherine Creed, Franz T. Winklhofer,
CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.03950510 Water Prescription in Autosomal Dominant Polycystic Kidney Disease: A Pilot Study Connie J. Wang, Catherine Creed, Franz T. Winklhofer,
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hyponatraemia. Detlef Bockenhauer
 Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
Hyponatraemia Detlef Bockenhauer Key message Plasma sodium can be low due to either excess water or deficiency of salt In clinical practice, dysnatraemias almost always reflect an abnormality of water
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERENCE CARDS Chronic Kidney Disease
 PROVIDER REFERENCE CARDS Chronic Kidney Disease") VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
VA/DoD Clinical Practice Guideline for the Management of Chronic Kidney Disease in Primary Care (2008) PROVIDER REFERECE CARDS Chronic Kidney Disease CKD VA/DoD Clinical Practice Guideline for the Management
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION. Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle
 THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
THERAPEUTIC INTERVENTIONS TO PRESERVE RESIDUAL KIDNEY FUNCTION Rajnish Mehrotra Harborview Medical Center University of Washington, Seattle 1 2 Outline of Presentation Refinements in our understanding
Nephrology Case Presentation for PCKD. Douglas A. Stahura 24 January 2002 With update 2018
 Nephrology Case Presentation for PCKD Douglas A. Stahura 24 January 2002 With update 2018 Case Presentation l 48 y/o WM presents with back pain Sharp, over L side/ribs Intermittent but severe 8/10 No radiation
Nephrology Case Presentation for PCKD Douglas A. Stahura 24 January 2002 With update 2018 Case Presentation l 48 y/o WM presents with back pain Sharp, over L side/ribs Intermittent but severe 8/10 No radiation
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy
CHRONIC KIDNEY DISEASE WHY WOMEN MAY BE AT RISK?
 CHRONIC KIDNEY DISEASE WHY WOMEN MAY BE AT RISK? Dr. Judy A Geissler, DNP, APNP, FNP-BC, CNN Vascular Access Advanced Practice Provider Employer- Medical College of Wisconsin No financial disclosures Barbara
CHRONIC KIDNEY DISEASE WHY WOMEN MAY BE AT RISK? Dr. Judy A Geissler, DNP, APNP, FNP-BC, CNN Vascular Access Advanced Practice Provider Employer- Medical College of Wisconsin No financial disclosures Barbara
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
Blood Pressure Monitoring in Chronic Kidney Disease
 Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Blood Pressure Monitoring in Chronic Kidney Disease Aldo J. Peixoto, MD FASN FASH Associate Professor of Medicine (Nephrology), YSM Associate Chief of Medicine, VACT Director of Hypertension, VACT American
Office Management of Reduced GFR Practical advice for the management of CKD
 Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE
Office Management of Reduced GFR Practical advice for the management of CKD CKD Online Education CME for Primary Care April 27, 2016 Monica Beaulieu, MD FRCPC MHA CHAIR PROVINCIAL KIDNEY CARE COMMITTEE