Together 2 Goal Campaign Measurement Specifications American Medical Group Foundation Version 1.0 February 23, 2016
|
|
|
- Terence Sanders
- 6 years ago
- Views:
Transcription
1 Together 2 Goal Campaign Measurement Specifications American Medical Group Foundation Version 1.0 February 23, Purpose The purpose of this document is to provide guidance to participating medical groups on data to be submitted for the American Medical Group Foundation s (AMGF s) national diabetes campaign, Together 2 Goal. Measurement is essential for improvement. That s why measurement is a cornerstone of Together 2 Goal, not only to gauge the impact of the campaign but also to serve as vital tool for AMGA members to use in creating that change. At the same time, we don t want measurement to be an obstacle to participating in the campaign, nor an undue burden. So Together 2 Goal offers three data reporting tracks, to fit the capabilities and interests of each AMGA member. This document describes the four individual measures and the bundle measure that make up the core measurement track. The basic track consists of just the first measure in the core track, HbA 1C < 8%. The focus of the campaign is detection and longitudinal management of patients with type 2 diabetes, so the measures are designed to enable participating organizations to track improvement in their performance over the course of the campaign. These measures were recommended by the Scientific Advisory Committee and the Measurement Committee for Together 2 Goal and were approved by the National Advisory Committee. The work of these committees was informed by analyses of longitudinal EHR and outbound claims data from AMGA members who are using the Optum One population health analytics platform, through AMGA s partnership with Optum. We are grateful for these members contribution of their data, for their participation in AMGA s Optum One collaborative, and for Optum s support. 2. Overview of Measures These specifications describe the measures for the core measurement track. Among patients with type 2 diabetes, the core measures describe performance in hemoglobin A 1C (HbA 1C ) control (< 8%), blood pressure (BP) control (< 140/90 mm Hg), medical attention for nephropathy, and lipid management (statin prescribed). These measure specs are based on two measure sets from NCQA s HEDIS 2016 Technical Specifications for Physician Measurement: Comprehensive Diabetes Care (CDC) and Statin Therapy for Patients with Diabetes (SPD). We have tried to follow these national measures as closely as possible, but some differences are inevitable, mainly in constructing the denominator: Together 2 Goal focuses just on patients with type 2 diabetes, while national measures generally include all patients with diabetes mellitus. 1
2 HEDIS measures are developed initially for health plans, which have definitive data on member enrollment, but the HEDIS specs for physician measurement construct a denominator based on patients seen by a practice. We are taking the latter approach for Together 2 Goal. Other differences between these measures and HEDIS 2016 are described throughout the document. None of the measures produced from the AMGF Together 2 Goal campaign have been validated by NCQA. NCQA specifications provided in the AMGF Together 2 Goal campaign are for reference only and are not an indication of measure validity. HEDIS value sets are referenced throughout these specs and are provided in an accompanying Excel workbook (HEDIS Value Sets for T2G Measures v1.0.xlsx). We greatly appreciate NCQA s generosity in granting permission to use these value sets for Together 2 Goal. These specs are substantially clearer and a little easier to program, thanks to meticulous review of a draft version by several AMGA members and corporate partners. We are deeply grateful for their time and expertise. Numerical superscripts in the text refer to numbered notes at the end of each section or paragraph (see Section 3.1, for example). These notes are intended to assist in identifying comparable patient populations across organizations Measure Definitions Organizations participating in AMGF s Together 2 Goal campaign are asked to report seven values for each 12 month measurement period (MP). These values are defined in detail in Sections : (1) Active initial population Patients with two or more encounters in an ambulatory setting, over 18 months (2) Active initial population with type 2 diabetes (T2G cohort, the denominator) Patients with evidence of type 2 diabetes (diagnosis on a claim or the problem list) (3) T2G cohort (denominator) patients with HbA 1C in control (measure #1) Patients whose most recent HbA 1C is < 8% (4) T2G cohort (denominator) patients with BP in control (measure #2) Patients whose most recent ambulatory, in office blood pressure is < 140/90 mm Hg (5) T2G cohort (denominator) patients who received medical attention for nephropathy (measure #3) Patients with evidence of a nephropathy screening or monitoring test, a diagnosis of nephropathy, treatment for nephropathy, or evidence of the use of an angiotensin converting enzyme inhibitor (ACEi) or angiotensin II receptor blocker (ARB) (6) T2G cohort (denominator) patients who received lipid management (measure #4) Patients for whom a statin was prescribed or who had a documented reason not to receive stain therapy (7) T2G cohort (denominator) patients who are compliant with all elements of the T2G bundle (measure #5) Patients who are compliant for measures #1, #2, #3, and #4 2
3 Using the reported values described above, AMGF will calculate and track the following measures: Prevalence of type 2 diabetes HbA 1C control HbA 8% BP control Medical attention for nephropathy Lipid management T2G bundle Using Value Sets Accompanying this document is an Excel workbook (HEDIS Value Sets for T2G Measures v1.0.xlsx) which contains value sets from the HEDIS 2016 Technical Specifications for Physician Measurement. Value sets are lists of codes used to define diagnoses, procedures, or events. Value sets are referenced in this document as (HEDIS 2016: Value Set Name Value Set). Value set names correspond to worksheet tabs in the Excel workbook. For example, (HEDIS 2016: Pregnancy Value Set) refers to the worksheet Pregnancy. Some value sets contain multiple kinds of codes. For example, the ESRD value set contains diagnosis codes (ICD 9 CM, ICD 10 CM), institutional procedure codes (ICD 9 PCS, ICD 10 PCS), professional procedure codes (CPT, HCPCS), CMS place of service (POS) codes, UB revenue codes, and UB type 3
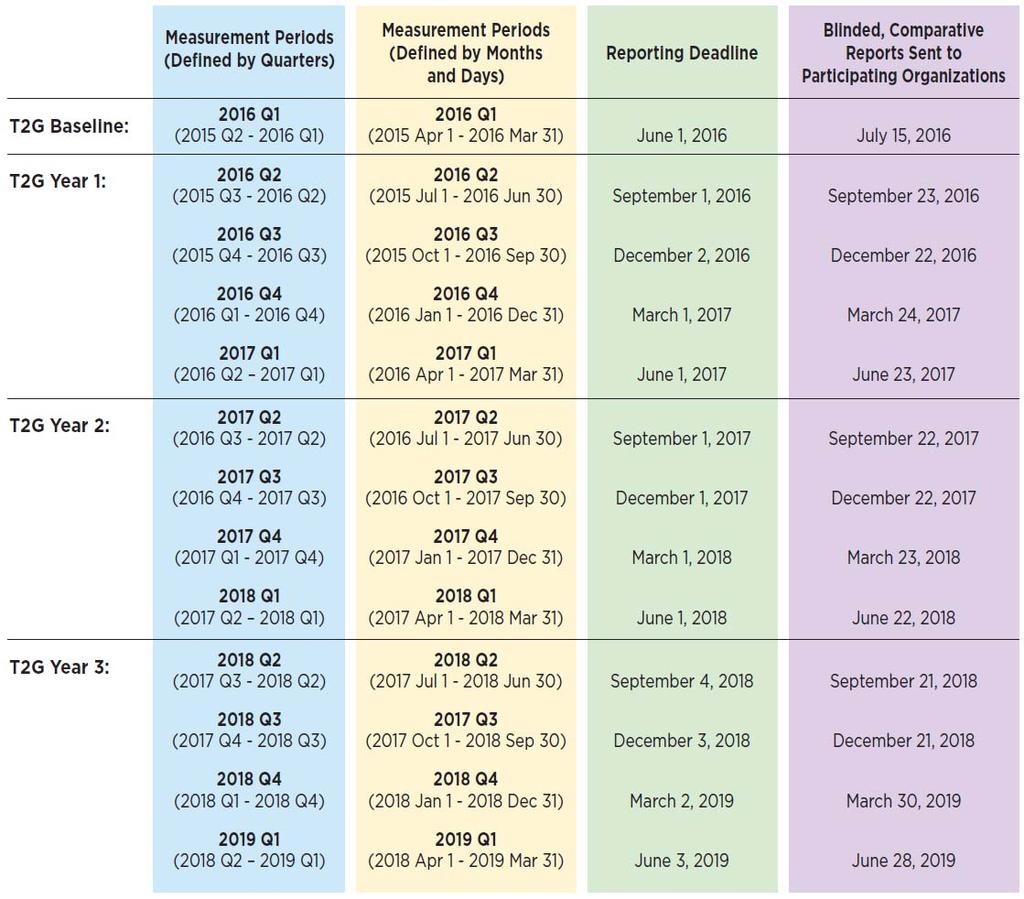
4 of bill (TOB) codes. This allows patients to be identified for the ESRD exclusion using any of several data sources. Most organizations have multiple source systems and data repositories, or ways of accessing EHR problem lists. While these specs dictate concepts for inclusion and exclusion criteria, we expect organizations to use their most convenient and reliable data sources to identify patients for these measures and to determine whether each patient is numerator compliant Measurement Periods Participating organizations are asked to report quarterly, using a rolling 12 month measurement period (MP). The first report will be designated 2016 Q1, which corresponds to a 12 month MP of 2015 Q Q1, or 2015 Apr Mar 31. These data will be used as a baseline, to track improvement over the course of the campaign. After the baseline period, organizations are asked to report quarterly for the duration of the threeyear campaign. Each report is due two months after the end of the 12 month MP, so the report for a period ending Q1 (March 31) will be due by June 1. Separate instructions will be provided for transmitting data, but briefly, there will be two options: enter the seven values needed for each quarter into a secure web portal for which participating organizations will be registered by campaign staff; or enter the seven values into an Excel template that will be provided, then either upload the Excel file to the portal or submit it by , using a special address that enables automatic parsing and consistency checking for submitted files. Among patients with type 2 diabetes seen during a typical 12 month period, about two thirds have their last office visit during the last three months. So a 12 month measure is naturally weighted to reflect recent performance. Reporting quarterly using a rolling 12 month MP maintains consistency with the typical time frame for quality measures and also provides for timely reflection of changes in care process. 4
5 5
6 3. Patient Counts to be Reported Sections describe the values we are asking participating organizations to report for each 12 month measurement period. Each value is a number of patients. AMGF will compute the ratios for prevalence and performance rates, as previously specified Active Initial Population 1 Patients aged 18 75, as of the last day of the 12 month measurement period (MP), with two or more eligible face to face encounters (Table 1) in an ambulatory 2 setting during the 12 month MP plus the prior 6 months (18 months total), with an eligible provider specialty (Table 2). The two visits need not be with the same provider or the same specialty. Note 1: An active initial population will allow Together 2 Goal to calculate and track increases in prevalence of type 2 diabetes as additional patients are discovered through practice based case detection (screening). Patients who are newly diagnosed will count toward the campaign goal of improved care for 1 million patients with type 2 diabetes. Together 2 Goal will report prevalence so groups can track changes over time, not for comparative purposes. For health plans, HEDIS requires continuous enrollment during the measurement year. Since providers don t have enrollment data, the Together 2 Goal visit type, specialty, and time frame requirements are an attempt to define a cohort of patients for whom the organization is likely to feel accountable for providing care for their type 2 diabetes. Note 2: Ambulatory settings include office visits, plus those in urgent care (distinct from ED), and retail or convenience clinics. To the extent possible, exclude encounters in ambulatory surgery, ED, observation, and inpatient settings. Also exclude telemedicine encounters and visits at the patient s home or in a nursing home. It is possible that patients whose only encounters occurred in a group s retail or urgent care clinics are not receiving their on going primary care at the respective group, and thus the group should not be held accountable for their diabetes care. For this reason, groups may optionally exclude patients whose only encounters during the 12 month MP plus the prior 6 months (18 months total) were in retail or urgent care clinics. 6
7 Table 1: Codes to Identify Visits CPT/HCPCS Codes Description , Evaluation & Management Office Visit Evaluation & Management Office Consultation , Evaluation & Management Preventive Visit Preventative Medicine: Individual Counseling Visit Preventative Medicine: Group Counseling Visit 99420, Other Preventive Medicine Services G0402 Initial Preventive Physical Examination ( Welcome to Medicare Visit) G0438, G0439 Medicare Annual Wellness Visit G0463 T1015 Hospital outpatient clinic visit for assessment and management of a patient Clinic visit/encounter, all inclusive Table 2: Eligible Provider Specialties Provider Specialty* Primary Care Provider (e.g., Family Medicine, Internal Medicine, Geriatrics, Pediatrics, General Practice) Endocrinologist Cardiologist Nephrologist * Eligible providers include: Doctor of Medicine (MD), Doctor of Osteopathy (DO), Physician Assistant (PA), Advanced Practice Registered Nurse (APRN, ARNP), and other advanced practice professionals (APPs). Organizations should use their own definition for classifying a PCP, using this list as a guide. 7
8 Exclusions 3 Required Exclusions Exclude patients who: 1. Had a diagnosis for pregnancy (HEDIS 2016: Pregnancy Value Set) on any claim or the problem list, in any setting, during the 12 month measurement period (MP) plus the prior 6 months, or 2. Died prior to the end of the 12 month MP. Optional Exclusions Organizations may choose to exclude patients who had either of the following on a claim or problem list, in any setting, during the 12 month MP plus the prior 6 months: 1. Had a diagnosis of polycystic ovary syndrome (PCOS) (Table 3), or 2. Had a diagnosis of gestational or steroid induced diabetes (HEDIS 2016: Diabetes Exclusions Value Set), or 3. Evidence of palliative care (Table 4), hospice, or an order to discontinue diabetes treatment. Note 3: Beyond the mandatory exclusion of women who were pregnant, the optional exclusions for PCOS, gestational diabetes, steroid induced diabetes, and palliative care allow each organization to determine whether there are compelling reasons to remove these patients from their cohort. Since PCOS, gestational diabetes, and steroid induced diabetes are established exclusions (historically, although PCOS was removed in HEDIS 2016), the campaign will retain them as optional exclusions. Thus organizations who have been using these exclusions internally may reflect them in their reporting for Together 2 Goal, if they choose. Table 3: Codes to Identify Patients with Polycystic Ovary Syndrome (Optional Exclusion) Diagnosis Codes for PCOS ICD ICD 10 E28.2 Table 4: Codes to Identify Patients with Palliative Care (Optional Exclusion) Encounter for Palliative Care ICD 9 V66.7 ICD 10 Z51.5 8
9 3.2. T2G Cohort (Denominator for Together 2 Goal Measures) Detailed Description Number of patients from the active initial population with evidence of type 2 diabetes (Table 5). Evidence of type 2 diabetes is a diagnosis during the 12 month measurement period (MP) plus the prior 6 months, on either: 4 1. the patient s problem list, 5 or 2. a claim for a face to face visit in an ambulatory setting. 4,5 Table 5: Codes to Identify Patients with Type 2 Diabetes Codes ICD 9 ICD *0 or 250.*2, where * is any valid character E11.*, where * is any valid character string Note 4: Please use the CPT/HCPCS codes in Table 1 and the care settings in Note 2 to identify face toface encounters in the ambulatory setting. Diabetes diagnoses on other claims, such as for lab tests, should not be considered, because they may have been used in a rule out sense. Include all diagnoses on claims for any of the CPT/HCPCS codes in Table 1, in any of the settings in Note 2, regardless of the specialty of the provider who renders or bills for the service. Although T2G requires two visits with certain specialties within 18 months in order to be in the active initial population, we require a diagnosis code for type 2 diabetes on only one claim for a face to face visit in an ambulatory setting, or on the patient s problem list in the EHR. This differs from HEDIS, which requires a diagnosis code on claims for two ambulatory visits (absent an inpatient admission with type 2 diabetes among the discharge diagnoses). Since Together 2 Goal focuses on longitudinal management, we do not count diagnosis codes on inpatient discharges. In a health system that includes hospitals with open staff models, not all patients who are discharged from a system hospital would be expected to receive on going primary care from the system s medical group. 9
10 Note 5: A minority of patients included in the T2G cohort (diagnosis code for type 2 diabetes on a claim or problem list) also have a diagnosis code for type 1 diabetes. In the data from AMGA s Optum One collaborative, 4.8% of patients (range %, across provider organizations) included in the T2G cohort also had at least one eligible diagnosis code for type 1 diabetes on a claim or problem list in the 12 month MP plus the prior 6 months. Groups may use whatever logic they believe is appropriate to exclude patients with evidence of both type 1 and type 2 diabetes during the 12 month MP plus the prior 6 months. Options include: (a) excluding patients with any evidence of type 1 diabetes; (b) applying an algorithm (e.g., exclude patients with 1 diagnosis code for type 1 diabetes and fewer than 3 diagnosis codes for type 2 diabetes, 2 codes for type 1 and fewer than 6 codes for type 2, or 3 or more codes for type 1); or (c) not excluding these patients at all. In the Optum One data, patients with diagnosis code evidence of both type 1 and type 2 diabetes have similar rates of performance on BP control, nephropathy, and lipid management, and significantly worse performance on HbA 1C control, compared to those with just evidence of type 2 diabetes. Note 6: ICD 10 codes O24 (diabetes mellitus in pregnancy, childbirth, and the puerperium) are not included here as exclusions, because we are already excluding patients who were pregnant at any time during the 12 month MP plus the prior 6 months. Note 7: Together 2 Goal does not use pharmacy data (claims, dispensing, e prescribing, or medication list) to identify patients with diabetes. Only claim/encounter data (diagnosis codes) and EHR data (problem list) are used. Together 2 Goal is focused on patients with type 2 diabetes, and many patients who have only pharmacy evidence of diabetes cannot be definitively classified as having type 2 diabetes and therefore are not included in the T2G cohort. As part of the campaign, organizations are encouraged to identify patients who have evidence of diabetes in the EHR (elevated HbA 1C or fasting glucose, or medications for glycemic control, except metformin along with evidence of other conditions associated with insulin resistance) and to place a diagnosis on their problem list, as appropriate, and on relevant claims. But these patients do not enter the T2G cohort until the diagnosis of type 2 diabetes is recorded. 10

11 T2G Cohort Diagram 11
12 3.3. Measure #1 HbA 1C Control Detailed Description Numerator Number of denominator patients whose most recent HbA 1C in the 12 month measurement period (MP) is < 8.0%. 8 Additional Notes Use most recent HbA 1C test result in the 12 month MP, regardless of setting (ambulatory, urgent care, ER, inpatient, etc.). Patients whose most recent HbA 1C is < 8.0% are numerator compliant. Patients whose most recent HbA 1C is 8.0% or who have no HbA 1C result recorded during the 12 month MP are not numerator compliant. For organizations that use LOINC codes, HbA 1C results may be identified by: , , or Note 8: For Together 2 Goal, we use only a single threshold, < 8.0%. Other HbA 1C control measures use a threshold of < 7.0% or > 9.0%. This was a topic of much discussion by the Scientific Advisory Committee, since therapeutic targets should be individualized, and a target lower than 8.0% may be appropriate for many patients. The Committee concluded that since the intent of the campaign is to measure glycemic control across a broad patient population, the < 8% threshold is the best choice, provided that campaign materials emphasize the need to establish an individual target for each patient. Using this population threshold for the campaign avoids the need for exclusions and allows for a consistent denominator across all four elements of the bundled measure. 12

13 Diagram 13
14 3.4. Measure #2 BP Control Detailed Description Numerator Number of denominator patients whose most recent ambulatory, 9 in office blood pressure reading in the 12 month measurement period (MP) is < 140/90 mm Hg. Additional Notes Exclude home BP readings and ambulatory BP monitoring data. Exclude BP measurements from urgent care, emergency department, or inpatient settings. 9 Both the systolic and diastolic readings must occur on the same day. If there are multiple blood pressures on the same date, use the lowest systolic and the lowest diastolic blood pressure, even if they were not measured together. Patients where both systolic BP is < 140 and diastolic BP < 90 are numerator compliant. Patients where either systolic BP is 140 or diastolic BP 90 are not numerator compliant. Patients with no valid BP recorded during the 12 month MP are not numerator compliant. Note 9: A BP measurement from an urgent care, ED, or inpatient setting may optionally be considered, but only if it is the most recent recorded BP and is < 140/90 mm Hg. 14

15 Diagram 15
16 3.5. Measure #3 Medical Attention for Nephropathy Detailed Description Numerator Number of denominator patients who had evidence of medical attention for nephropathy during the 12 month measurement period (MP). Evidence includes: a nephropathy screening or monitoring test, a diagnosis of nephropathy or treatment for nephropathy, or evidence of use of an angiotensin converting enzyme inhibitor (ACEi) or angiotensin II receptor blocker (ARB). Nephropathy screening or monitoring tests can be identified using: HEDIS 2016: Urine Protein Tests Value Set, or 2. A result in the EHR for one of the following urine tests (this list is based on the instructions for medical record review for the hybrid method, in the HEDIS 2016 Technical Specifications for Physician Measurement): a. Urine microalbumin. b. 24 hour urine or other timed urine for albumin or protein. c. Spot or random urine for albumin or protein. d. Urine for albumin/creatinine ratio. Diagnosis of nephropathy or treatment for nephropathy can be identified using: Any of the following value sets: a. HEDIS 2016: Nephropathy Treatment Value Set b. HEDIS 2016: CKD Stage 4 Value Set c. HEDIS 2016: ESRD Value Set d. HEDIS 2016: Kidney Transplant Value Set, or 2. At least one visit with a nephrologist, using the CPT/HCPCS codes in Table 1. ACE inhibitor or ARB use can be identified by: e Prescribing transaction within the 12 month MP for at least one of the drugs in Table 6, or 16

17 2. At least one of the drugs in Table 6 active on the patient s medication list in the EHR, as of the end of the 12 month MP. Note 10: Diagnosis codes in the value sets for this measure may be identified on a claim or on the patient s problem list. CPT/HCPCS codes may be identified on a claim. Note 11: Patients with documented intolerance or contraindications to ACE inhibitors or ARBs may be considered numerator compliant. Groups may use whatever codes they believe are appropriate for this optional step. The following codes for ACEi/ARB intolerance or contraindications may be used as a reference. ICD 9: , 972.6, 972.9, E942.6, V64.1 ICD 10: T46.4, T46.5 Table 6: ACE Inhibitors/ARBs* * Based on Table CDC L: ACE Inhibitors/ARBs. HEDIS 2016 Technical Specifications for Physician Measurement, p
18 Diagram 18
19 3.6. Measure #4 Lipid Management Detailed Description Numerator Number of denominator patients who had a statin prescribed or had documentation of a reason not to receive a statin. Statin use can be identified by: e Prescribing transaction within the 12 month measurement period (MP) for at least one of the drugs in Table 7, or 2. At least one of the drugs in Table 7 active on the patient s medication list in the EHR, as of the end of the 12 month MP. Note 11: Although the ACC/AHA guidelines for lipid management specify that patients should be on a moderate or high statin dose, the Measurement Committee recognized that it may be difficult to determine the prescribed dose, so we do not require organizations to assess the dose. For Together 2 Goal, we accept evidence of any statin use. This is consistent with the approach used in HEDIS. Documented reasons for not receiving a statin include: 12,13 1. Any of the following during the 12 month MP plus the prior 6 months: a. In vitro fertilization (HEDIS 2016: IVF Value Set or supplemental codes 14 ) b. Prescription for clomiphene (Clomid): i. e Prescribing transaction, or ii. Clomiphene on the active medication list in the EHR at any time during the 12 month MP plus the prior 6 months c. End stage renal disease (HEDIS 2016: ESRD Value Set) d. Cirrhosis (HEDIS 2016: Cirrhosis Value Set) 2. Myalgia, myositis, myopathy, or rhabdomyolysis (HEDIS 2016: Muscular Pain and Disease Value Set) during the 12 month MP Most recent low density lipoprotein (LDL) during the 12 month MP plus the prior 6 months < 70 mg/dl 16 (Optional) 4. Active liver disease (e.g., hepatitis) during the 12 month MP plus the prior 6 months 16 (Optional) 19
20 5. Age < 40 (as of the end of the MP) and none of the following 17 (Optional): a. A cardiovascular event or diagnosis of overt cardiovascular disease (CVD) during the 12 month MP plus the prior 6 months: i. Myocardial infarction (HEDIS 2016: MI Value Set) ii. Coronary artery bypass graft (HEDIS 2016: CABG Value Set) iii. Percutaneous coronary intervention (HEDIS 2016: PCI Value Set) iv. Other revascularization procedure (HEDIS 2016: Other Revascularization Value Set) v. Ischemic vascular disease (HEDIS 2016: IVD Value Set) b. CVD risk factors any time during the 12 month MP plus the prior 6 months: i. Most recent LDL cholesterol 100 mg/dl, or ii. Diagnosis of hypertension (Table 8), or iii. Current smoker, or iv. Most recent BMI 25 kg/m 2 Note 12: Patients with a documented reason not to receive a statin are considered numerator compliant. Although it would be logical to exclude them from the denominator for the statin measure, we want to maintain the same denominator as for the other three measures, so we can include lipid management in the bundle measure. Note 13: Diagnosis codes in the value sets for the lipid management measure may be identified either on a claim or on the patient s problem list. CPT/HCPCS codes may be identified on a claim. LDL, BMI, and smoking status may be used if these values are available in the EHR. Note 14: The HEDIS value set for in vitro fertilization (IVF) includes only HCPCS codes. Groups may choose to use CPT codes to define IVF and may use the following, in addition to others they believe are appropriate. CPT: 58970, 58974, Note 15: The HEDIS value set referenced here includes only those muscular pain and disease diagnosis codes that we would expect to be associated specifically with statin intolerance, rather than general muscle pain. Also note that while we use an 18 month period for all other reasons for not receiving a statin, we use a 12 month period for this exclusion. The Scientific Advisory Committee stressed the importance of statin therapy for patients with diabetes and discussed the need to re try patients on statins, after complaints of myalgia or transient elevation in liver enzymes. They felt it might be reasonable not to expect re trying statins within 12 months of muscle complaints, so the patient is considered numerator compliant if these symptoms occurred during the 12 month MP. But if these symptoms were last reported in the 6 months prior to the 12 month 20

21 MP, the Committee believed statins should be re tried within the MP. This is consistent with the approach used in HEDIS. Note 16: In an effort to reduce the burden of reporting for Together 2 Goal and to accommodate potential objections from providers, we have included optional exclusions for patients with LDL < 70 mg/dl and patients with active liver disease. This is consistent with the approach used by Minnesota Community Measurement. Note 17: The ADA guidelines specify that patients < 40 years of age with CVD risk factors or overt CVD should be on a statin, while patients < 40 with neither are exempt. In the data from AMGA s Optum One collaborative, 5.1% of patients included in the T2G cohort are < 40 years of age, and 93% of these patients have at least one CVD risk factor. Considering the small proportion of patients who meet this criterion and its complexity, it is optional for Together 2 Goal reporting. If organizations choose not to look for CVD risk factors or overt CVD, patients < 40 years of age need evidence of statin use or another reason for not receiving a statin to be considered numerator compliant. Table 7: Statin Prescriptions* * Based on Table CDC L: SPD A: High, Moderate, and Low Intensity Statin Prescriptions. HEDIS 2016 Technical Specifications for Physician Measurement, p Table 8: Codes to Identify Patients with Hypertension Codes ICD 9 ICD *, 402.*, 403.*, 404.*, or 405.*, where * is any valid character string I10.*, I11.*, I12.*, I13.*, I15.*, where * is any valid character string 21

22 Diagram 22
23 3.7. Measure #5 T2G Bundle Measure Detailed Description Numerator Number of patients who were numerator compliant for all four measures above. Patients are considered numerator compliant if they met each of the following: 1. Most recent HbA 1C < 8% (measure #1), and 2. Most recent BP < 140/90 (measure #2), and 3. Received medical attention for nephropathy (measure #3), and 4. Statin prescribed or documented reason not to prescribe a statin (measure #4). Patients who are not numerator compliant in any of the four measures are not numerator compliant for the bundle measure. Note 18: An all or none, or bundle, measure best reflects the patient s perspective, and it encourages provider organizations to think of each patient as a whole and to take a system oriented approach to improvement. We owe each patient attention to all of his or her needs. It is sobering to learn how difficult it can be to achieve high performance rates on a bundle measure, even with what feels like good performance on the individual components. 23

24 Diagram 24
Measure Owner Designation. AMA-PCPI is the measure owner. NCQA is the measure owner. QIP/CMS is the measure owner. AMA-NCQA is the measure owner
 2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
2011 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
Data Orientation Webinar. February 16, 2016 Nikita Stempniewicz, John Cuddeback, Rich Stempniewicz, and Cori Rattelman
 Data Orientation Webinar February 16, 2016 Nikita Stempniewicz, John Cuddeback, Rich Stempniewicz, and Cori Rattelman AGENDA Background Scope of Together 2 Goal campaign Measurement tracks Measurement
Data Orientation Webinar February 16, 2016 Nikita Stempniewicz, John Cuddeback, Rich Stempniewicz, and Cori Rattelman AGENDA Background Scope of Together 2 Goal campaign Measurement tracks Measurement
QBPC Claims Based Provider Quick Reference Guide
 QBPC Claims Based Provider Quick Reference Guide Category: Diabetes Chronic Suite ICD-10-CM diagnosis HbA1c Test Codes LOINC Evidence of Treatment for Nephropathy Codes E10; E11; E13 83036-37 17856-6,
QBPC Claims Based Provider Quick Reference Guide Category: Diabetes Chronic Suite ICD-10-CM diagnosis HbA1c Test Codes LOINC Evidence of Treatment for Nephropathy Codes E10; E11; E13 83036-37 17856-6,
Measuring Hypertension Control. Reporting Methods for Measure Up/Pressure Down
 Measuring Hypertension Control and Reporting Methods for Measure Up/Pressure Down November 2013 Agenda Recent guideline activity regarding cardiovascular disease Current measurement approach for Measure
Measuring Hypertension Control and Reporting Methods for Measure Up/Pressure Down November 2013 Agenda Recent guideline activity regarding cardiovascular disease Current measurement approach for Measure
Consensus Core Set: ACO and PCMH / Primary Care Measures Version 1.0
 Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
Consensus Core Set: ACO and PCMH / Primary Care s 0018 Controlling High Blood Pressure patients 18 to 85 years of age who had a diagnosis of hypertension (HTN) and whose blood pressure (BP) was adequately
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN ISCHEMIC VASCULAR DISEASE (IVD) MEASURES GROUP: #204. Ischemic Vascular Disease (IVD):
IHA P4P Measure Manual Measure Year Reporting Year 2018
 ADULT PREVENTIVE CARE IHA P4P Measure Manual Measure Year 2017 - Reporting Year 2018 *If line of business not labeled, measure is Commercial only Adult BMI (Medicare) 18-74 Medicare members ages 18-74
ADULT PREVENTIVE CARE IHA P4P Measure Manual Measure Year 2017 - Reporting Year 2018 *If line of business not labeled, measure is Commercial only Adult BMI (Medicare) 18-74 Medicare members ages 18-74
Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
 CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
CMS-1345-P 174 Table 1. Proposed Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings AIM: Better Care for Individuals 1. Patient/Care Giver Experience
DIABETES MEASURES GROUP OVERVIEW
 2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
2014 PQRS OPTIONS F MEASURES GROUPS: DIABETES MEASURES GROUP OVERVIEW 2014 PQRS MEASURES IN DIABETES MEASURES GROUP: #1. Diabetes: Hemoglobin A1c Poor Control #2. Diabetes: Low Density Lipoprotein (LDL-C)
Cardiovascular Health and Diabetes Screening for People with Schizophrenia
 Cardiovascular Health and Diabetes Screening for People with Schizophrenia The percentage of members 25 years and older with a schizophrenia diagnosis and who were prescribed any antipsychotic medication,
Cardiovascular Health and Diabetes Screening for People with Schizophrenia The percentage of members 25 years and older with a schizophrenia diagnosis and who were prescribed any antipsychotic medication,
Blue Cross and Blue Shield of Louisiana 2016 Healthcare Effectiveness Data and Information Set (HEDIS) Coding and Documentation Guide
 Coding and Documentation Guide") Blue Cross and Blue Shield of Louisiana 2016 Healthcare Effectiveness Data and Information Set (HEDIS) Coding and Documentation Guide Measure Measure Description Protocol or Documentation Required Coding
Blue Cross and Blue Shield of Louisiana 2016 Healthcare Effectiveness Data and Information Set (HEDIS) Coding and Documentation Guide Measure Measure Description Protocol or Documentation Required Coding
Quality Payment Program: Cardiology Specialty Measure Set
 Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Measure Title * Reportable via PINNACLE α Reportable via Diabetes Collaborative CQMC v1.0 Measure High Priority Measure Cross Cutting Measure Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor
Clinical Quality Measures Summary of Upcoming Enhancements
 Upcoming coding enhancements will impact the logic behind the clinical quality indicators applicable to your practice specialty. Please refer to this grid for a summary of the coding enhancements and some
Upcoming coding enhancements will impact the logic behind the clinical quality indicators applicable to your practice specialty. Please refer to this grid for a summary of the coding enhancements and some
Florida Blue QUALITY PERFORMANCE METRIC STANDARDS FEBRUARY 2013
 Florida Blue QUALITY PERFORMANCE METRIC STANDARDS FEBRUARY 2013 QUALITY PERFORMANCE METRIC CALCULATION QUALITY METRICS SELECTED FOR MEASUREMENT Per Section 3.2 of the Agreement, HCPP must meet the following
Florida Blue QUALITY PERFORMANCE METRIC STANDARDS FEBRUARY 2013 QUALITY PERFORMANCE METRIC CALCULATION QUALITY METRICS SELECTED FOR MEASUREMENT Per Section 3.2 of the Agreement, HCPP must meet the following
2017 MSSP Clinical Quality Measures
 *The information contained in this document relies heavily on information supplied by CMS. GPRO CARE-1 (NQF 0097): Medication Reconciliation Post-Discharge DESCRIPTION: Percentage of discharges from any
*The information contained in this document relies heavily on information supplied by CMS. GPRO CARE-1 (NQF 0097): Medication Reconciliation Post-Discharge DESCRIPTION: Percentage of discharges from any
HEDIS QUICK REFERENCE GUIDE: DOCUMENTATION TIPS FOR ADULT MEASURES
 HEDIS QUICK REFERENCE GUIDE: DOCUMENTATION TIPS FOR ADULT MEASURES For Health Care Providers January 2018 Helping you improve your scores, as you improve the health of your patients. Healthcare Effectiveness
HEDIS QUICK REFERENCE GUIDE: DOCUMENTATION TIPS FOR ADULT MEASURES For Health Care Providers January 2018 Helping you improve your scores, as you improve the health of your patients. Healthcare Effectiveness
MHSPHP Metrics Forum. Diabetes.
 MHSPHP Metrics Forum Diabetes Judith.rosen.1.ctr@us.af.mil Overview Methodology of the HEDIS metrics What is the future of LDL metrics? How does the action list differ from the metrics FAQs 2 Diabetes
MHSPHP Metrics Forum Diabetes Judith.rosen.1.ctr@us.af.mil Overview Methodology of the HEDIS metrics What is the future of LDL metrics? How does the action list differ from the metrics FAQs 2 Diabetes
MEASURING CARE QUALITY
 MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
MEASURING CARE QUALITY Region December 2013 For Clinical Effectiveness of Care Measures of Performance From: Healthcare Effectiveness Data and Information Set (HEDIS ) HEDIS is a set of standardized performance
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care
: Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
2017 CMS Web Interface Reporting
 2017 CMS Web Interface Reporting Measure Specification Review May 18, 2017 Sherry Grund, Telligen Mary Schrader, Telligen Medicare Shared Savings Program and Next Generation ACO Model DISCLAIMER This presentation
2017 CMS Web Interface Reporting Measure Specification Review May 18, 2017 Sherry Grund, Telligen Mary Schrader, Telligen Medicare Shared Savings Program and Next Generation ACO Model DISCLAIMER This presentation
2014 Evidence-Based HTN Guideline: Preliminary Data from AMGA s Anceta Collaborative
 2014 Evidence-Based HTN Guideline: Preliminary Data from AMGA s Anceta Collaborative February 2014 Patient Population Measure spec for MU/PD generally follows NQF 0018 (used for HEDIS, PQRS, and MU) 1.6
2014 Evidence-Based HTN Guideline: Preliminary Data from AMGA s Anceta Collaborative February 2014 Patient Population Measure spec for MU/PD generally follows NQF 0018 (used for HEDIS, PQRS, and MU) 1.6
2016 Internal Medicine Preferred Specialty Measure Set
 1 0059 Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients 18-75 years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period 5 0081 Registry, EHR, 9 0105
1 0059 Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients 18-75 years of age with diabetes who had hemoglobin A1c > 9.0% during the measurement period 5 0081 Registry, EHR, 9 0105
Measure Owner Designation. AMA-PCPI/NCQA (contract) is the measure owner. AMA-PCPI is the measure owner. AMA-PCPI/ASCO/NCCN is the measure owner
 is the measure owner. AMA-PCPI is the measure owner. AMA-PCPI/ASCO/NCCN is the measure owner") 2012 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
2012 EHR Measure Specifications The specifications listed in this document have been updated to reflect clinical practice guidelines and applicable health informatics standards that are the most current
Medicare Advantage Measurement Period Handbook for Enhanced Personal Health Care Measurement Period beginning January 1, 2015
 Medicare Advantage Measurement Period Handbook for Enhanced Personal Health Care Measurement Period beginning January 1, 2015 Amerivantage is an HMO plan with a contract with the New Mexico Medicare program.
Medicare Advantage Measurement Period Handbook for Enhanced Personal Health Care Measurement Period beginning January 1, 2015 Amerivantage is an HMO plan with a contract with the New Mexico Medicare program.
PCMH 2018 Enrollment and Update August 25, 2017
 PCMH 2018 Enrollment and Update August 25, 2017 Enrollment Requirements Anne Santifer HealthCare Innovations Department of Human Services 2018 Enrollment Requirements A physician practice that is enrolled
PCMH 2018 Enrollment and Update August 25, 2017 Enrollment Requirements Anne Santifer HealthCare Innovations Department of Human Services 2018 Enrollment Requirements A physician practice that is enrolled
HEDIS Adult. Documentation and Coding Guidelines Medical record documentation required. Measure description. Coding ICD-10: Z68.1 Z68.45, Z68.
 HEDIS Adult Documentation and Guidelines 2017 description Adult BMI Assessment (ABI) Members 18 74 years of age who had an outpatient visit and whose body mass index (BMI) was documented during the measurement
HEDIS Adult Documentation and Guidelines 2017 description Adult BMI Assessment (ABI) Members 18 74 years of age who had an outpatient visit and whose body mass index (BMI) was documented during the measurement
Hedis Behavioral Health Measures
 Hedis Behavioral Health Measures Generating better health outcomes and improving HEDIS scores is a positive outcome for everyone. Magellan Complete Care is offering support by providing the details of
Hedis Behavioral Health Measures Generating better health outcomes and improving HEDIS scores is a positive outcome for everyone. Magellan Complete Care is offering support by providing the details of
HEDIS Documentation and Coding Adult Guidelines 2017
 HEDIS Documentation and Coding Adult Guidelines 2017 Reproduced with permission from HEDIS 2017, Volume 2: Technical Specifications for Health Plans by the National Committee for Quality Assurance (NCQA).
HEDIS Documentation and Coding Adult Guidelines 2017 Reproduced with permission from HEDIS 2017, Volume 2: Technical Specifications for Health Plans by the National Committee for Quality Assurance (NCQA).
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Process
 MEASURE TYPE: Process") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Management of Chronic Conditions 2019 COLLECTION
Consensus Core Set: Cardiovascular Measures Version 1.0
 Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
Consensus Core Set: Cardiovascular s NQF 0330 Hospital 30-day, all-cause, riskstandardized readmission rate (RSRR) following heart failure hospitalization 0229 Hospital 30-day, all-cause, riskstandardized
CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016
 EFFICIENCY REPORT EXPLANATION January 4, 2016") CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016 WHAT IS AN EPISODE OF CARE? An episode of care is a grouping of a patient s health care claims for a unique
CLINICAL PROCESS IMPROVEMENT INITIATIVE (CPII) EFFICIENCY REPORT EXPLANATION January 4, 2016 WHAT IS AN EPISODE OF CARE? An episode of care is a grouping of a patient s health care claims for a unique
Adult Diabetes Clinician Guide NOVEMBER 2017
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Diabetes Clinician Guide Introduction NOVEMBER 2017 This evidence-based guideline summary is based on the 2017 KP National Diabetes Guideline.
Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care
 Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
Quality ID #438: Statin Therapy for the Prevention and Treatment of Cardiovascular Disease National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE
THERE ARE TWO SUBMISSION CRITERIA FOR THIS MEASURE: 1) Patients who are 18 years and older with a diagnosis of CAD with LVEF < 40%
 Patients who are 18 years and older with a diagnosis of CAD with LVEF < 40%") Quality ID #118 (NQF 0066): Coronary Artery Disease (CAD): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy - Diabetes or Left Ventricular Systolic Dysfunction
Quality ID #118 (NQF 0066): Coronary Artery Disease (CAD): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy - Diabetes or Left Ventricular Systolic Dysfunction
WCHQ MEASURES AT A GLANCE
 WCHQ Ambulatory Measures A1C Blood Sugar Testing A1C Blood Sugar Control Patients with diabetes Patients with diabetes office visit in. Gestational Diabetes (code 648.8) is office visit in. Compliance
WCHQ Ambulatory Measures A1C Blood Sugar Testing A1C Blood Sugar Control Patients with diabetes Patients with diabetes office visit in. Gestational Diabetes (code 648.8) is office visit in. Compliance
Achieving Quality and Value in Chronic Care Management
 The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
The Burden of Chronic Disease One of the greatest burdens on the US healthcare system is the rapidly growing rate of chronic disease. These statistics illustrate the scope of the problem: Nearly half of
Meaningful Use Clinical Quality Measures for Eligible Professionals
 Meaningful Use Clinical Quality Measures for Eligible Professionals Measure Type NQF ID CMS ID Description Title: Adult Weight Screening and Follow-Up 1 NQF 0421 PQRI 128 calculated BMI in the past six
Meaningful Use Clinical Quality Measures for Eligible Professionals Measure Type NQF ID CMS ID Description Title: Adult Weight Screening and Follow-Up 1 NQF 0421 PQRI 128 calculated BMI in the past six
2010 Physician Quality Reporting Initiative Measures Groups Specifications Manual
 2010 Physician Quality Reporting Initiative Measures Groups Specifications Manual This manual contains specific guidance for reporting 2010 Physician Quality Reporting Initiative (PQRI) Measures Groups.
2010 Physician Quality Reporting Initiative Measures Groups Specifications Manual This manual contains specific guidance for reporting 2010 Physician Quality Reporting Initiative (PQRI) Measures Groups.
Clinical Quality Measures
 Core Measures Preventive Care and Screening Measure Pair: a. Tobacco Use Assessment, b. Tobacco Cessation Intervention. Percentage of patients aged 18 years and older who have been seen for at least 2
Core Measures Preventive Care and Screening Measure Pair: a. Tobacco Use Assessment, b. Tobacco Cessation Intervention. Percentage of patients aged 18 years and older who have been seen for at least 2
Preferred Care Partners. HEDIS Technical Standards
 Preferred Care Partners HEDIS Technical Standards 1 HEDIS What is HEDIS HEDIS Overview Adults HEDIS Overview Pediatrics HEDIS is a registered trademark of the National Committee for Quality Assurance 2
Preferred Care Partners HEDIS Technical Standards 1 HEDIS What is HEDIS HEDIS Overview Adults HEDIS Overview Pediatrics HEDIS is a registered trademark of the National Committee for Quality Assurance 2
Introduction to HEDIS 2016 Presented by the Quality Improvement Department at Gold Coast Health Plan
 Introduction to HEDIS 2016 Presented by the Quality Improvement Department at Gold Coast Health Plan Ventura County s Medi-Cal Managed Care Plan Serving Ventura County since July 1, 2011 1 Contents I.
Introduction to HEDIS 2016 Presented by the Quality Improvement Department at Gold Coast Health Plan Ventura County s Medi-Cal Managed Care Plan Serving Ventura County since July 1, 2011 1 Contents I.
Best Practices in Adult Immunizations Collaborative Data Orientation Webinar. June 14, 2017
 Best Practices in Adult Immunizations Collaborative Data Orientation Webinar June 14, 2017 Welcome to Group 3 participating organizations! 2 Agenda Topic Speaker 1. Welcome Danielle Casanova, AMGA 2. Collaborative
Best Practices in Adult Immunizations Collaborative Data Orientation Webinar June 14, 2017 Welcome to Group 3 participating organizations! 2 Agenda Topic Speaker 1. Welcome Danielle Casanova, AMGA 2. Collaborative
Anthem Pay-for- Performance (HEDIS )*
*") Serving Hoosier Healthwise, Healthy Indiana Plan Anthem Pay-for- Performance (HEDIS )* [Candace Adye, RN Amanda Gonzalez, RN] *HEDIS is a registered trademark of the National Committee for Quality Assurance
Serving Hoosier Healthwise, Healthy Indiana Plan Anthem Pay-for- Performance (HEDIS )* [Candace Adye, RN Amanda Gonzalez, RN] *HEDIS is a registered trademark of the National Committee for Quality Assurance
2017 Diabetes. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
2017 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Program Evaluation Program Title: Diabetes Program Evaluation Period: January 1, 2017 December
HEALTHCARE EFFECTIVENESS DATA AND INFORMATION SET (HEDIS )
") STARS MEASURES 2015 HEALTHCARE EFFECTIVENESS DATA AND INFORMATION SET (HEDIS ) Developed by the National Committee for Quality Assurance (NCQA), HEDIS is the most widely used set of performance measures
STARS MEASURES 2015 HEALTHCARE EFFECTIVENESS DATA AND INFORMATION SET (HEDIS ) Developed by the National Committee for Quality Assurance (NCQA), HEDIS is the most widely used set of performance measures
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 Office of Media Affairs MEDICARE FACT SHEET FOR IMMEDIATE RELEASE
Comprehensive ESRD Care (CEC) Model Proposed Quality Measures for Public Comment. Table of Contents
 Model Proposed Quality Measures for Public Comment. Table of Contents") Comprehensive ESRD Care (CEC) Model Proposed Quality s for Public Comment Table of Contents Page # Introduction 3 Summaries by Domain Technical Expert Panel Recommended CEC Quality s 4 s that were recommended
Comprehensive ESRD Care (CEC) Model Proposed Quality s for Public Comment Table of Contents Page # Introduction 3 Summaries by Domain Technical Expert Panel Recommended CEC Quality s 4 s that were recommended
Quality Care Plus 2015 Primary Care Physician Incentive Program. Now includes Medicare patients!
 Quality Care Plus 2015 Primary Care Physician Incentive Program Now includes Medicare patients! Health Partners Plans (HPP) would like to express our appreciation for the invaluable role our primary care
Quality Care Plus 2015 Primary Care Physician Incentive Program Now includes Medicare patients! Health Partners Plans (HPP) would like to express our appreciation for the invaluable role our primary care
Quality Payment Program: Cardiology Specialty Measure Set
 Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
Quality Payment Program: Cardiology Specialty Set Title Number CMS Reporting Method(s) Heart Failure (HF): Angiotensin- Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for
2016 General Practice/Family Practice Preferred Specialty Measure Set
 1 0059 5 0081 41 N/A 50 N/A 65 0069, EHR 66 0002, EHR Effective Clinical Care Effective Clinical Care Effective Clinical Care Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients
1 0059 5 0081 41 N/A 50 N/A 65 0069, EHR 66 0002, EHR Effective Clinical Care Effective Clinical Care Effective Clinical Care Diabetes: Hemoglobin A1c (HbA1c) Poor Control (>9%): Percentage of patients
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
NEW JERSEY 2011 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health and Senior Services Health Care Quality Assessment
CORONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW
 MEASURES GROUP OVERVIEW") CONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN CONARY ARTERY DISEASE (CAD) MEASURES GROUP: #6. Coronary Artery Disease (CAD): Antiplatelet
CONARY ARTERY DISEASE (CAD) MEASURES GROUP OVERVIEW 2014 PQRS OPTIONS F MEASURES GROUPS: 2014 PQRS MEASURES IN CONARY ARTERY DISEASE (CAD) MEASURES GROUP: #6. Coronary Artery Disease (CAD): Antiplatelet
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO
 The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
The table below includes the quality measures an ACO is required to submit to CMS as a participant in an MSSP Track 3 ACO ACO-1 ACO-2 Getting Timely Care, Appointments, and Information How Well Your Providers
Table of Contents. Page 2 of 20
 Page 1 of 20 Table of Contents Table of Contents... 2 NMHCTOD Participants... 3 Introduction... 4 Methodology... 5 Types of Data Available... 5 Diabetes in New Mexico... 7 HEDIS Quality Indicators for
Page 1 of 20 Table of Contents Table of Contents... 2 NMHCTOD Participants... 3 Introduction... 4 Methodology... 5 Types of Data Available... 5 Diabetes in New Mexico... 7 HEDIS Quality Indicators for
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Chapter 2: Identification and Care of Patients With CKD
 Chapter 2: Identification and Care of Patients With CKD Over half of patients in the Medicare 5% sample (aged 65 and older) had at least one of three diagnosed chronic conditions chronic kidney disease
Chapter 2: Identification and Care of Patients With CKD Over half of patients in the Medicare 5% sample (aged 65 and older) had at least one of three diagnosed chronic conditions chronic kidney disease
December 2018 CTC/OHIC Measure Specifications
 Overarching Principles and Definitions Active Patients: Patients seen by a primary care clinician of the PCMH anytime within the last 24 months Definition of primary care clinician includes the following:
Overarching Principles and Definitions Active Patients: Patients seen by a primary care clinician of the PCMH anytime within the last 24 months Definition of primary care clinician includes the following:
For Electronic Measure Specification Information go to:
 Diabetes Recognition NQF 0421 PQRI 128 Title: Adult Weight Screening and Follow-Up Description: Percentage of patients aged 18 years and older with a calculated BMI in the past six months or during the
Diabetes Recognition NQF 0421 PQRI 128 Title: Adult Weight Screening and Follow-Up Description: Percentage of patients aged 18 years and older with a calculated BMI in the past six months or during the
CLINICAL QUALITY MEASURES Stage 1 Meaningful Use
 CLINICAL QUALITY MEASURES Stage 1 Meaningful Use * Eligible professionals (EPs) must report on 3 required core clinical quality measures (CQMs). If the denominator of 1 or more of the required core measures
CLINICAL QUALITY MEASURES Stage 1 Meaningful Use * Eligible professionals (EPs) must report on 3 required core clinical quality measures (CQMs). If the denominator of 1 or more of the required core measures
Quality Measures Guide. Medicare Star Rating and HEDIS measures
 Quality Measures Guide Medicare Star Rating and HEDIS measures February 2018 About the Quality Measures Guide A key component of our Quality Program is Healthcare Effectiveness Data and Information Set
Quality Measures Guide Medicare Star Rating and HEDIS measures February 2018 About the Quality Measures Guide A key component of our Quality Program is Healthcare Effectiveness Data and Information Set
Clinical Quality Measures for Submission by Medicare or Medicaid EP/s for the 2011 and 2012 Payment Year
 1 NQF 0059 1 NQF 0064 2 NQF 0061 3 Title: Diabetes: Hemoglobin A1c Poor Control Description: Percentage of patients 18-75 years of age with diabetes (type 1 or type 2) who had hemoglobin A1c > 9.0%. Title:
1 NQF 0059 1 NQF 0064 2 NQF 0061 3 Title: Diabetes: Hemoglobin A1c Poor Control Description: Percentage of patients 18-75 years of age with diabetes (type 1 or type 2) who had hemoglobin A1c > 9.0%. Title:
Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide
 Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org Rev:
Bridges to Excellence Coronary Artery Disease Care Recognition Program Guide Altarum Bridges to Excellence 3520 Green Court, Suite 300 Ann Arbor, MI 48105 bte@altarum.org www.bridgestoexcellence.org Rev:
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
The Renal Physicians Association Quality Improvement Registry
 In collaboration with CECity The Renal Physicians Association Quality Improvement Registry This registry is approved by CMS as a Qualified Clinical Data Registry (QCDR) for Eligible Professionals and GPRO
In collaboration with CECity The Renal Physicians Association Quality Improvement Registry This registry is approved by CMS as a Qualified Clinical Data Registry (QCDR) for Eligible Professionals and GPRO
Provider STAR Ratings Quick Reference Guide 2016 Dates of Service. Updated January 20, 2016
 Provider STAR Ratings Quick Reference Guide 2016 Dates of Service Updated January 20, 2016 Adult BMI (Body Mass Index) Assessment (ABA) EXCLUSIONS: Members who have a diagnosis of pregnancy during the
Provider STAR Ratings Quick Reference Guide 2016 Dates of Service Updated January 20, 2016 Adult BMI (Body Mass Index) Assessment (ABA) EXCLUSIONS: Members who have a diagnosis of pregnancy during the
Practice-Level Executive Summary Report
 PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
PINNACLE Registry Metrics 0003, Test Practice_NextGen [Rolling: 1st April 2015 to 31st March 2016 ] Generated on 5/11/2016 11:37:35 AM American College of Cardiology Foundation National Cardiovascular
HEDIS Guidelines for Health Care Providers
 75 Vanderbilt Ave Staten Island NY 10304 1-844-CPHL-CARES www.centersplan.com HEDIS Guidelines for Health Care Providers Adult BMI Assessment (ABA) Members 18-74 years of age who had an outpatient visit
75 Vanderbilt Ave Staten Island NY 10304 1-844-CPHL-CARES www.centersplan.com HEDIS Guidelines for Health Care Providers Adult BMI Assessment (ABA) Members 18-74 years of age who had an outpatient visit
Instructions and Technical Documentation for the BridgeIt PHASE Report Set Version 8b, By Ben Fouts, Redwood Community Health Coalition. May, 2017.
 Instructions and Technical Documentation for the BridgeIt PHASE Report Set Version 8b, By Ben Fouts, Redwood Community Health Coalition. May, 2017. Introduction A BridgeIT report is available from RCHC
Instructions and Technical Documentation for the BridgeIt PHASE Report Set Version 8b, By Ben Fouts, Redwood Community Health Coalition. May, 2017. Introduction A BridgeIT report is available from RCHC
STARS SYSTEM 5 CATEGORIES
 TMG STARS 2018 1 2 STARS Program Implemented in 2008 by CMS. Tool to inform beneficiaries of quality of various health plans 5-star rating system Used to adjust payments to health plans (bonus to plans
TMG STARS 2018 1 2 STARS Program Implemented in 2008 by CMS. Tool to inform beneficiaries of quality of various health plans 5-star rating system Used to adjust payments to health plans (bonus to plans
Reporting Periods in 2010
 Reporting Periods in 2010 1. Full Year (January 1, 2010 December 31, 2010) eligible professionals (EP) whose PQRI quality measure information is successfully submitted (via claims, measures group, or registry)
Reporting Periods in 2010 1. Full Year (January 1, 2010 December 31, 2010) eligible professionals (EP) whose PQRI quality measure information is successfully submitted (via claims, measures group, or registry)
Key Elements in Managing Diabetes
 Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
Key Elements in Managing Diabetes Presentor Disclosure No conflicts of interest to disclose Presented by Susan Cotey, RN, CDE Lennon Diabetes Center Stephanie Tubbs Jones Health Center Cleveland Clinic
HEDIS Documentation & Coding Guidelines 2015
 Effectiveness of Care: Prevention & Screening Members 18 74 years of age who had an outpatient visit and BMI ICD-9: V85.0 - V85.45 whose body mass index (BMI) was documented during the measurement year
Effectiveness of Care: Prevention & Screening Members 18 74 years of age who had an outpatient visit and BMI ICD-9: V85.0 - V85.45 whose body mass index (BMI) was documented during the measurement year
2013 Hypertension Measure Group Patient Visit Form
 Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
Please complete the form below for 20 or more unique patients meeting patient sample criteria for the measure group for the current reporting year. A majority (11 or more) patients must be Medicare Part
Program Metrics. New Unique ID. Old Unique ID. Metric Set Metric Name Description. Old Metric Name
 Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for, Atrial Fibrillation, Hypertension and.
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
NEW JERSEY 2012 HOSPITAL PERFORMANCE REPORT TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment June 2013 NEW JERSEY
Monthly Campaign Webinar. May 19, 2016
 Monthly Campaign Webinar May 19, 2016 WEBINAR REMINDERS Webinar will be recorded today and available the week of May 23 rd Together2Goal.org Website (Improve Patient Outcomes Webinars) Email distribution
Monthly Campaign Webinar May 19, 2016 WEBINAR REMINDERS Webinar will be recorded today and available the week of May 23 rd Together2Goal.org Website (Improve Patient Outcomes Webinars) Email distribution
LRE Executive Dashboard Integrated Care Delivery Platform (ICDP)
") Data in Report As Of: 2/17/2018 LRE Executive Dashboard Integrated Care Delivery Platform (ICDP) Key Performance Indicators (KPIs) Report Created by: Paige Horton LAKESHORE REGIONAL ENTITY Performance
Data in Report As Of: 2/17/2018 LRE Executive Dashboard Integrated Care Delivery Platform (ICDP) Key Performance Indicators (KPIs) Report Created by: Paige Horton LAKESHORE REGIONAL ENTITY Performance
Performance Outcomes: Measure & Metric Details
 Performance Outcomes: Measure & Metric Details Adherence to Antipsychotic Medications for People with Schizophrenia Numerator: Number of people who remained on an antipsychotic for at least 80% of their
Performance Outcomes: Measure & Metric Details Adherence to Antipsychotic Medications for People with Schizophrenia Numerator: Number of people who remained on an antipsychotic for at least 80% of their
Frequently Asked Questions (FAQ) IHA Align. Measure. Perform. (AMP) Programs January Audit Audit Roadmap Posted 1/23/19
 IHA Align. Measure. Perform. (AMP) Programs January Audit Audit Roadmap Posted 1/23/19") Frequently Asked Questions (FAQ) IHA Align. Measure. Perform. (AMP) Programs January 2019 Audit Audit Roadmap Question: For the AMP MY 2018 Roadmap, is the last part of question 5.2W in Section 5, Describe
Frequently Asked Questions (FAQ) IHA Align. Measure. Perform. (AMP) Programs January 2019 Audit Audit Roadmap Question: For the AMP MY 2018 Roadmap, is the last part of question 5.2W in Section 5, Describe
May 2016 CTC/OHIC Measure Specifications
 Active Patients: Overarching Principles and Definitions Out patients seen by a primary care clinician of the PCMH anytime within the last 24 months. Definition of primary care clinician includes the following:
Active Patients: Overarching Principles and Definitions Out patients seen by a primary care clinician of the PCMH anytime within the last 24 months. Definition of primary care clinician includes the following:
2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY. MEASURE TYPE: Process
 Quality ID #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
Quality ID #7 (NQF 0070): Coronary Artery Disease (CAD): Beta-Blocker Therapy Prior Myocardial Infarction (MI) or Left Ventricular Systolic Dysfunction (LVEF < 40%) National Quality Strategy Domain: Effective
The University of Mississippi School of Pharmacy
 LONG TERM PERSISTENCE WITH ACEI/ARB THERAPY AFTER ACUTE MYOCARDIAL INFARCTION: AN ANALYSIS OF THE 2006-2007 MEDICARE 5% NATIONAL SAMPLE DATA Lokhandwala T. MS, Yang Y. PhD, Thumula V. MS, Bentley J.P.
LONG TERM PERSISTENCE WITH ACEI/ARB THERAPY AFTER ACUTE MYOCARDIAL INFARCTION: AN ANALYSIS OF THE 2006-2007 MEDICARE 5% NATIONAL SAMPLE DATA Lokhandwala T. MS, Yang Y. PhD, Thumula V. MS, Bentley J.P.
Quality Metrics and Goal Setting
 Quality Metrics and Goal Setting Pavan Chava DO Ochsner Department of Endocrinology Director for Diabetes Management for Ochsner Health System 9/17/2016 Disclosures Sanofi- Research and travel grant Goals
Quality Metrics and Goal Setting Pavan Chava DO Ochsner Department of Endocrinology Director for Diabetes Management for Ochsner Health System 9/17/2016 Disclosures Sanofi- Research and travel grant Goals
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 2: Identification and Care of Patients With CKD Over half of patients from the Medicare 5 percent sample have either a diagnosis of chronic kidney disease
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 2: Identification and Care of Patients With CKD Over half of patients from the Medicare 5 percent sample have either a diagnosis of chronic kidney disease
Chronic Benefit Application Form Cardiovascular Disease and Diabetes
 Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
Chronic Benefit Application Form Cardiovascular Disease and Diabetes 19 West Street, Houghton, South Africa, 2198 Postnet Suite 411, Private Bag X1, Melrose Arch, 2076 Tel: +27 (11) 715 3000 Fax: +27 (11)
Quality ID #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care
: Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care") Quality ID #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate Outcome
Quality ID #236 (NQF 0018): Controlling High Blood Pressure National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Intermediate Outcome
Measurement Name Beta-Blocker Therapy Prior Myocardial Infarction (MI)
") Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
Program Metrics The list below includes the metrics that will be calculated by the PINNACLE Registry for the outpatient office setting. These include metrics for Artery, Atrial Fibrillation, Hypertension
QUALITY IMPROVEMENT Section 9
 Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
Quality Improvement Program The Plan s Quality Improvement Program serves to improve the health of its members through emphasis on health maintenance, education, diagnostic testing and treatment. The Quality
Validating and Reporting the 2017 UDS Clinical Measures (Version 1)
") Validating and Reporting the 2017 UDS Clinical Measures Author: Ben Fouts, Informatics Redwood Community Health Coalition 1310 Redwood Way Petaluma, California 94954 support@rchc.net Document Last Updated:
Validating and Reporting the 2017 UDS Clinical Measures Author: Ben Fouts, Informatics Redwood Community Health Coalition 1310 Redwood Way Petaluma, California 94954 support@rchc.net Document Last Updated:
Star Measures At-A-Glance Guide
 Star Measures At-A-Glance Guide This guide alerts you to important preventive care and services that you can provide to patients to help boost Star Ratings. ASSESSMENT AND SCREENING At Easy Choice, we
Star Measures At-A-Glance Guide This guide alerts you to important preventive care and services that you can provide to patients to help boost Star Ratings. ASSESSMENT AND SCREENING At Easy Choice, we
HEALTHCARE REFORM. September 2012
 HEALTHCARE REFORM Accountable Care Organizations: ACOs 101 September 2012 The enclosed slides are intended to provide you with a general overview of accountable care organizations (ACOs), created within
HEALTHCARE REFORM Accountable Care Organizations: ACOs 101 September 2012 The enclosed slides are intended to provide you with a general overview of accountable care organizations (ACOs), created within
NQF Measure Number & PQRI Implementation Number
 Title NQF Steward s Adult Weight Screening and Follow-Up Hypertension: Blood Pressure ment Preventive Care and Screening Pair: a. Tobacco Use Assessment, b. Tobacco Cessation Intervention with a calculated
Title NQF Steward s Adult Weight Screening and Follow-Up Hypertension: Blood Pressure ment Preventive Care and Screening Pair: a. Tobacco Use Assessment, b. Tobacco Cessation Intervention with a calculated
New indicators to be added to the NICE menu for the QOF and amendments to existing indicators
 New indicators to be added to the for the QOF and amendments to existing indicators 1 st September 2015 Version 1.1 This document was originally published on 3 rd August 2015, it has since been updated.
New indicators to be added to the for the QOF and amendments to existing indicators 1 st September 2015 Version 1.1 This document was originally published on 3 rd August 2015, it has since been updated.
2013 Physician Quality Reporting System (PQRS) Measures Groups Specifications Manual
 Measures Groups Specifications Manual") 2013 Physician Quality Reporting System (PQRS) Measures Groups Specifications Manual 12/19/2012 CPT only copyright 2012 American Medical Association. All rights reserved. CPT is a registered trademark
2013 Physician Quality Reporting System (PQRS) Measures Groups Specifications Manual 12/19/2012 CPT only copyright 2012 American Medical Association. All rights reserved. CPT is a registered trademark
2017 Medicare STARs Provider Quality Indicators Guide
 2017 Medicare STARs Provider Quality Indicators Guide Medicare STARs Rating Centers for Medicare & Medicaid Services (CMS) created a Five-Star Quality Rating System to help measure the quality in care
2017 Medicare STARs Provider Quality Indicators Guide Medicare STARs Rating Centers for Medicare & Medicaid Services (CMS) created a Five-Star Quality Rating System to help measure the quality in care
2014 ACO GPRO Audit What this means for your practice. Sheree M. Arnold ACO Clinical Transformation Specialist
 2014 ACO GPRO Audit What this means for your practice Sheree M. Arnold ACO Clinical Transformation Specialist Agenda Catholic Medical Partners ACO overview Attribution and sampling of patients ACO quality
2014 ACO GPRO Audit What this means for your practice Sheree M. Arnold ACO Clinical Transformation Specialist Agenda Catholic Medical Partners ACO overview Attribution and sampling of patients ACO quality
2015 Diabetes. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Care Program Evaluation Program Title: Diabetes Care Program Evaluation Period: January
2015 Diabetes Program Evaluation Our mission is to improve the health and quality of life of our members Diabetes Care Program Evaluation Program Title: Diabetes Care Program Evaluation Period: January
Medicare Shared Savings Program Accountable Care Organization (ACO) Measure Deep Dive Series
 Measure Deep Dive Series") Medicare Shared Savings Program Accountable Care Organization (ACO) Measure Deep Dive Series Preventive Care and Screening (Prev-13) Measure 42 Statin Therapy for the Prevention and Treatment of Cardiovascular
Medicare Shared Savings Program Accountable Care Organization (ACO) Measure Deep Dive Series Preventive Care and Screening (Prev-13) Measure 42 Statin Therapy for the Prevention and Treatment of Cardiovascular
Medicare STRIDE SM Physician Quality Program 2019 Program Overview
 Medicare STRIDE SM Quality Program 2019 Program Overview Health Services- Managed by Network Medical Management 2019 Program 1 Medicare Advantage Quality Program Program Overview The Plan will support
Medicare STRIDE SM Quality Program 2019 Program Overview Health Services- Managed by Network Medical Management 2019 Program 1 Medicare Advantage Quality Program Program Overview The Plan will support
Clinical Practice Guideline Key Points
 Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark
Clinical Practice Guideline Key Points Clinical Practice Guideline 2008 Key Points Diabetes Mellitus Provided by: Highmark Endocrinology Clinical Quality Improvement Committee In accordance with Highmark