Investor science event from ADA Orlando, 28 June 2010
|
|
|
- Ross Garrett
- 6 years ago
- Views:
Transcription

1 Investor science event from ADA 2010 Orlando, 28 June 2010
2 Forward-looking statements This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as believes, expects, anticipates, projects, intends, should, seeks, estimates, future or similar expressions or by discussion of, among other things, strategy, goals, plans or intentions. Various factors may cause actual results to differ materially in the future from those reflected in forward-looking statements contained in this presentation, among others: 1 pricing and product initiatives of competitors; 2 legislative and regulatory developments and economic conditions; 3 delay or inability in obtaining regulatory approvals or bringing products to market; 4 fluctuations in currency exchange rates and general financial market conditions; 5 uncertainties in the discovery, development or marketing of new products or new uses of existing products, including without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products; 6 increased government pricing pressures; 7 interruptions in production; 8 loss of or inability to obtain adequate protection for intellectual property rights; 9 litigation; 10 loss of key executives or other employees; and 11 adverse publicity and news coverage. Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to mean that Roche s earnings or earnings per share for this year or any subsequent period will necessarily match or exceed the historical published earnings or earnings per share of Roche. Please see for full information on Roche products mentioned. 2
3 Introduction Dr. Karl Mahler, Head of Investor Relations
4 Investor science events at major medical meetings At least five events will highlight Roche s leadership Date / location 6 June 2010 Chicago, USA 28 June 2010 Orlando, USA 26 July 2010 Anaheim, USA October 2010 Milan, Italy October 2010 Gothenburg, Sweden Meeting ASCO (American Society of Clinical Oncology) ADA (American Diabetes Association) AACC (American Association for Clinical Chemistry) ESMO (European Society for Medical Oncology) ECTRIMS (European Committee for Treatment and Research in Multiple Sclerosis) Key assets / newsflow Avastin, MabThera/Rituxan, RG3502(T-DM1), RG1273(pertuzumab), etc. Franchise update CardioMetabolism, RG1583(taspoglutide), etc. Diagnostics review & update Avastin, RG3502(T-DM1), etc. RG1594(ocrelizumab) Steady flow of important clinical data & results 4
5 Taspoglutide & the GLP-1 class: Product attributes along three distinct dimensions Taspoglutide: Potential for best-in-class convenience Convenience (Injection frequency (BID, QD or QW), need for corrections, simple injection vs reconstitution, needle gauge) Taspoglutide: Robust, consistent efficacy Taspoglutide: Work ongoing to refine profile All GLP-1s have specific safety / tolerability challenges Efficacy (HbA1c, % pts reaching <7.0, FBG, weight loss, persistence of efficacy, increased insulin secretion, beta cell function) Safety / Tolerability (Hypoglycemia, nausea, vomiting, diarrhea, hypersensitivity, pancreatitis, thyroid cancer) 5
6 Investor science event from ADA 2010 Programme 28 June pm Introduction Dr. Karl Mahler, Head of Investor Relations Franchise overview: CardioMetabolism Dr. Fouzia Laghrissi Thode, Global Product Strategy Head for Metabolism and Anemia Taspoglutide: Overview of data at ADA 2010 Dr. Bruce Cooper, Head of Global Medical Affairs Taspoglutide: T-emerge 5 - comparison w/insulin glargine Prof. Dr. med. Michael Nauck Taspoglutide: Next steps Dr. Bruce Cooper, Head of Global Medical Affairs Questions & Answers Moderator: Dr. Karl Mahler Expected duration up to 1½ hour Dinner reception 6

7 Franchise overview: CardioMetabolism Dr. Fouzia Laghrissi Thode, Global Product Strategy Head for Metabolism and Anemia
8 Recent announcement Risk mitigation plan implemented To date, out of approximately 3,000 taspoglutide-treated patients in the phase III programme, a total of 23 cases of serious hypersensitivity reactions have been reported as related to taspoglutide by investigators (i.e. incidence < 1%) Roche has identified a potential association between anti-drug antibodies (ADAs) and an increased risk for patients to experience serious hypersensitivity reactions ADA levels will be routinely monitored and patients that develop pre-specified ADA levels will discontinue treatment and continue to be monitored in the trial 8
9 Serious hypersensitivity reactions Hypersensitivity reactions judged by investigators as serious Anaphylaxis or other systemic allergic reactions (ie, urticaria, angioedema) Anaphylaxis symptoms included: Cutaneous reactions (skin and/or mucosa): e.g., urticaria, angioedema Gastrointestinal: e.g., prolonged nausea and/or vomiting Respiratory: e.g., dyspnea Cardiovascular: e.g., blood pressure and/or heart rate changes No anaphylactic shock All patients recovered without complications Only one patient hospitalized overnight for observation Some patients were treated with antihistamines, steroids and one case was treated with adrenaline
10 Our commitment to CardioMetabolism Development T-emerge most comprehensive program in diabetes to date Dalcetrapib largest patient trial undertaken by Roche Pharma Aleglitazar initiating in 24 countries CardioMetabolism franchise Building capabilities Establishing leadership in CardioMetabolism Research gred and pred programs Active partnering Preparing for mid and long-term success in new disease area 10

11 Value for patients Taspoglutide Glycemic control Minimizing hypoglycemia Reducing weight Aleglitazar Unique profile to reduce CV risk in Type 2 diabetes Dalcetrapib Improved CV outcomes by treating the underlying disease of atherosclerosis 11
12 Development programs to deliver first or best in class dal-heart Raising HDL through CETP modulation to reduce cardiovascular risk ALECARDIO CV risk reduction for patients with type 2 diabetes post-acs dal-outcomes 15,600 patients dal-vessel 450 patients dal-plaque ALECARDIO 6,000 patients ALENEPHRO 300 patients 130 patients dal-plaque2 900 patients 12
, expected regulatory filing in 2013 Targeted indication:")
13 RG1658(dalcetrapib) dal-outcomes phase III study now fully recruited Target population by risk status 1 Phase III dal-outcomes 15,600 CHD 2 pts w/recent ACS 3 Best standard of care +/- dalcetrapib 600 mg qd Event-driven trial First patient in Q2-08, last patient in Q2-10 Expected interim efficacy analysis in Q3-11 (event-driven), expected regulatory filing in 2013 Targeted indication: Prevention of cardiovascular event in very high risk patients Primary outcomes study supported by secondary phase II/III studies; dal-vessel, dal-plaque, dal-plaque2 1 Roche epidemiology prevalence projection based on National Center for Health Statistics NHANES data (2009) 2 CHD=Coronary heart disease 3 ACS=Acute coronary syndrome 13

14 RG1439(aleglitazar) ALECARDIO phase III study enrolling Target population growing fast 1 Phase III ALECARDIO in 24 countries 6,000 T2D 2 pts hospitalized w/acs 3 Best standard of care +/- aleglitazar 150 μg qd Event-driven trial First patient in Q1-10; enrollment on track Regulatory filing expected in 2014 Targeted indication: Prevention of cardiovascular event in Type 2 diabetes patients post ACS 1 Patients with T2D 2 and ACS 3 (excl CHF NYHA II-IV) 2 T2D=Type 2 diabetes 3 ACS=Acute Coronary Syndrome 14

15 Taspoglutide: Overview of data at ADA 2010 Dr. Bruce Cooper, Head of Global Medical Affairs
16 Phase 3 Program: Over 6000 Patients, >1000 sites, 50 Countries Study Name Patient Population Sample Size Taspoglutide Comparator T-emerge 1 T-emerge 2 T-emerge 3 T-emerge 4 T-emerge 5 T-emerge 6 T-emerge 7 T-emerge 8 Inadequately controlled on diet & exercise Inadequately controlled with Met, TZD, or Met + TZD Inadequately controlled with pioglitazone + Met Inadequately controlled with Met Inadequately controlled on Met + SU; SU withdrawn at pre-randomization Inadequately controlled with SU Met Inadequately controlled with Met (high BMI) Patients with higher cardiovascular risk mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* Placebo Exenatide BID Placebo Sitagliptin Placebo Insulin glargine Pioglitazone mg QW* Placebo mg QW* Placebo BID = twice daily; BMI = body mass index; Met = metformin; QW = once weekly; SU = sulfonylurea; TZD = thiazolidinedione. *10 mg taspoglutide QW for 4 weeks followed by 20 mg QW. 16

17 Taspoglutide in T2DM: Headline Results from ADA Study Description Headline Results/status H2H vs. exenatide Primary endpoint met: Superior HbA1c reduction versus twice-daily exenatide Early Disease Vs. placebo, monotherapy Primary endpoint met: Superior HbA1c reduction versus placebo Treatment Naïve H2H vs. sitagliptin vs. placebo Primary endpoint met: Superior HbA1c reduction versus sitagliptin Early Disease H2H vs. insulin glargine Primary endpoint met: Non-inferior HbA1c reduction versus insulin glargine Advanced Disease Vs. placebo, obese T2D patients Primary endpoint met: Superior HbA1c reduction versus placebo Early Disease T-emerge Included Treatment Naïve T2D Patients With Early & Advanced Disease 17
18 Study Design for the Active-Controlled Studies: T-emerge 2, 4, 5, and 6 Taspoglutide formulation Once-weekly SC injection 29-g needle Prefilled syringe Primary Endpoint Patient screening 10 mg* Taspoglutide 10 mg QW Taspoglutide 20 mg QW Taspoglutide 10 mg QW Taspoglutide 20 mg QW Follow-up 2-year long-term extension Active comparator Active comparator 4 4* 2 24 weeks 28-week extension 0 weeks Week weeks *Patients randomized to taspoglutide 20 mg QW will receive taspoglutide 10 mg QW for 4 weeks followed by the 20 mg QW dosing. Active comparator: TE-2, exenatide; TE-4, sitagliptin; TE-5, insulin glargine; TE-6, pioglitazone. TE-4: sitagliptin active comparator and also includes placebo-controlled group. 18
19 Study Design for the Placebo-Controlled Studies: T-emerge 1, 3, and 7 Taspoglutide formulation Once-weekly SC injection 29-g needle Prefilled syringe Primary Endpoint Patient screening 10 mg* Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW 10 mg* Taspoglutide 10 mg QW Taspoglutide 20 mg QW Taspoglutide 10 mg QW Taspoglutide 20 mg QW Follow-up 4 4* 2 24 weeks 28-week extension 0 weeks Week weeks *Patients randomized to taspoglutide 20 mg QW receive taspoglutide 10 mg QW for 4 weeks followed by the 20 mg QW dosing. TE-1: 3-week patient screening and 2-week placebo run-in. TE-7 trial does not include taspoglutide 10 mg QW dose group. 19
20 Overall Baseline Demographics and Disease Characteristics Mean (SD) unless specified TE-1 (N=354) TE-2 (N=1149) TE-4 (N=636) TE-5 (N=1028) TE-7 (N=292) Men n (%) 130 (37) 608 (53) 352 (55) 549 (53) 119 (41) Age, y 55 (10) 56 (10) 56 (10) 58 (9) 54 (10) Weight, kg 86.8 (18.0) 94.4 (19.2) 92.4 (19.3) 90.8 (19.5) (18.1) BMI, kg/m (5.1) 33.4 (5.2) 32.5 (5.1) 32.4 (5.3) 36.7 (4.9) HbA1c, % 7.60 ( (0.91) 7.96 (0.87) 8.28 (0.90) 7.55 (0.84) HbA1c baseline 8.0% n (%) 108 (31) 572 (50) 281 (44) 610 (59) 83 (28) FPG, mg/dl 158 (45) 178 (46) 173 (46) 201 (52) 130 (37) Diabetes duration, y 2.4 (2.5) 6.6 (5.4) 5.9 (4.7) 9.1 (6.0) 5.1 (4.2) History of CV disorders* n (%) 55 (15) 183 (16) 99 (15) 198 (19) 49 (16) Intent-to-treat population. *Patients in the safety population with 1 cardiovascular disorder. 20
 7.6 7.5 7.")
21 Primary Endpoint: HbA1c Change From Baseline After 24 Weeks of Treatment Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1 Monotherapy TE-2 Metformin, TZD, or both TE-4 Metformin TE-5 Metformin, SU withdrawal TE-7 Metformin Baseline (%) Exenatide Sitagliptin Insulin glargine * * * * * LOCF = last-observation-carried-forward; LSMean = least square mean; SE = standard error. *P<0.001 vs placebo; P<0.001 vs active comparator. Intent-to-treat population; LOCF analysis. TE-5: Sulfonylurea treatment withdrawn prior to randomization for all patients. 21
 * * LSMean = least square mean; SE = standard error. *P<0.001 vs placebo. Intent-to-treat population; last-observation-carried-forward analysis.")
22 Time Course Example: TE-1 HbA1c Change From Baseline Over 24 Weeks of Treatment Placebo (n=115) Taspoglutide 10 mg QW (n=112) Taspoglutide 20 mg QW (n=127) * * LSMean = least square mean; SE = standard error. *P<0.001 vs placebo. Intent-to-treat population; last-observation-carried-forward analysis. 22

23 Percentage of Patients Reaching Target HbA1c <7% After 24 Weeks of Treatment Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1* Monotherapy TE-2 Metformin, TZD, or both TE-4 Metformin TE-5 Metformin, SU withdrawal TE-7* Metformin Exenatide Sitagliptin Glargine *Baseline entry criterion for TE-1 and TE-7 trial was HbA1c 6.5%; this analysis excluded patients from TE-1 and TE-7 with baseline HbA1c <7%. 23
 156 158 162 179 177 178 174 176 174 169 190 190 203 158 163 * * Exenatide * * Sitagliptin Insulin glargine * LSMean =")
24 Fasting Plasma Glucose (mg/dl) Change From Baseline After 24 Weeks of Treatment Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1 Monotherapy TE-2 Metformin, TZD, or both TE-4 Metformin TE-5 Metformin, SU withdrawal TE-7 Metformin Baseline (mg/dl) * * Exenatide * * Sitagliptin Insulin glargine * LSMean = least square mean; SE = standard error; Intent-to-treat population; LOCF analysis *P<0.001 vs placebo; P<0.01 vs active comparator; P< vs active comparator. TE-5: Sulfonylurea treatment withdrawn prior to randomization of all patients. Insulin dose titrated to FPG target. 24
 Taspoglutide 10 mg QW (n=112)")

25 Time Course Example: TE-1 Fasting Plasma Glucose Over 24 Weeks of Treatment Placebo (n=115) Taspoglutide 10 mg QW (n=112) Taspoglutide 20 mg QW (n=127) FPG (mg/dl) (Mean SE) * * *P<0.001 vs placebo. Intent-to-treat population; last-observation-carried-forward analysis.
 87 88 85 95 93 95 91 94 92 93 90 91 91 101 104 Exenatide Sita Glar * Glar = insulin glargine; LSMean = least square mean; SE = standard error;")
26 Body Weight Change From Baseline After 24 Weeks of Treatment Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1 Monotherapy TE-2 Metformin, TZD, or both TE-4 Metformin TE-5 Metformin, SU withdrawal TE-7 Metformin Baseline (kg) Exenatide Sita Glar * Glar = insulin glargine; LSMean = least square mean; SE = standard error; Sita = sitagliptin; TZD = thiazolidinedione. *P<0.05 vs placebo; P<0.05 vs active comparator; P<0.01 vs placebo; P<0.001 vs placebo or vs active comparator. Intent-to-treat population; last-observation-carried-forward analysis. 26




 from baseline")





27 Time-Course of Body Weight Change From Baseline Over 24 Weeks of Treatment Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1 TE-2 TE-4 TE-5 TE-7 Change in body weight (kg) from baseline (LSMean SE) * Exenatide Sitagliptin Insulin glargine Diet & exercise LSMean = least square mean; SE = standard error. *P<0.05 vs placebo; P<0.05 vs active comparator; P<0.01 vs placebo; P<0.001 vs placebo or vs active comparator. Intent-to-treat population; last-observation-carried-forward analysis. 27


28 Body Weight Loss Responder Rates After 24 Weeks of Treatment: 5% Placebo Taspoglutide 10 mg QW Taspoglutide 20 mg QW Active comparator TE-1 Monotherapy TE-2 Metformin, TZD, or both TE-4 Metformin TE-5 Metformin TE-7 Metformin Exenatide Sita Glar Glar = insulin glargine; Sita = sitagliptin; TZD = thiazolidinedione. Intent-to-treat population; last-observation-carried-forward analysis. 28
29 Safety Overview at 24 Weeks Incidence of nausea: 26-47% Incidence of vomiting: 17-28% Injection site reactions generally mild to moderate and infrequently lead to discontinuation (1.4-5%) % withdrawals due to all adverse events 10mg: 9-17% 20mg: 21-28% Control: 7-16% % withdrawals due to nausea or vomiting (T-emerge 2; H2H vs. exenatide) 10mg: 4.1% 20mg: 7.6% Exenatide: 6.5% 29


30 Example: TE-2 Number of Episodes of Nausea or Vomiting Over 24 Weeks Taspoglutide 10 mg QW Taspoglutide 20 mg QW Exenatide 10 g BID Nausea Vomiting % of patients # of Episodes # of Episodes Safety population. Withdrawals due to nausea or vomiting: exenatide: 6.5%, taspoglutide 10 mg QW: 4.1%, taspoglutide 20 mg QW: 7.6% 30
31 Example: TE-2 Weekly Incidence of Nausea and Vomiting Over 24 Weeks Taspoglutide 10 mg QW Taspoglutide 20 mg QW Exenatide 10 g BID Up-titration from 10 mg to 20 mg Nausea Up-titration from 10 mg to 20 mg Vomiting Safety population 86% and 83% of vomiting occurred on Day of Injection for taspoglutide 10 mg QW and 20 mg QW, respectively 31
32 Summary T-emerge program studied taspoglutide across a wide spectrum of patient types (including treatment-naive and patients with early disease and advanced disease) and versus 4 active comparators (exenatide, sitagliptin, pioglitazone, and even the highest dose of insulin glargine used in a GLP-1 registration study) In the T-emerge Clinical Development Program, taspoglutide demonstrated evidence of consistent glycemic control with low risk of hypoglycemia and significant weight loss in a ready-to-use weekly injection As has been seen with other GLP-1 receptor agonists, the most frequently reported adverse events with taspoglutide were related to gastrointestinal tolerability * Based on T-emerge results to-date at 24 weeks 32
33 Taspoglutide: T-emerge 5 - comparison w/insulin glargine Prof. Dr. med. Michael Nauck
 Michael Nauck, 1 Edward Horton, 2 Mirjana Andjelkovic, 3 Javier Ampudia-Blasco, 4 Mark N.")
34 T-emerge 5 Taspoglutide, a Once-Weekly Human GLP-1 Analog, Provides Comparable Glycemic Control to Insulin Glargine, with Superior Weight Loss and Less Hypoglycemia in Type 2 Diabetes: A Phase 3, Open-Label Trial (T-emerge 5) Michael Nauck, 1 Edward Horton, 2 Mirjana Andjelkovic, 3 Javier Ampudia-Blasco, 4 Mark N. Boldrin, 5 Raffaella Balena 3 1 Diabeteszentrum Bad Lauterberg, Bad Lauterberg im Harz, Germany 2 Joslin Diabetes Center, Boston, MA, United States 3 F.Hoffmann-La Roche, Basel, Switzerland 4 Clinic University Hospital, Valencia, Spain 5 Roche Pharmaceuticals, Nutley, NJ, United States 34
35 Taspoglutide, a Once-Weekly Human GLP-1 Analog Phase 3 Program: Over 6000 Patients Study Name Patient Population Sample Size Taspoglutide Comparator T-emerge 1 T-emerge 2 T-emerge 3 T-emerge 4 T-emerge 5 T-emerge 6 T-emerge 7 T-emerge 8 Inadequately controlled on diet & exercise Inadequately controlled with Met, TZD, or Met + TZD Inadequately controlled with pioglitazone + Met Inadequately controlled with Met Inadequately controlled on Met + SU; SU withdrawn pre-randomization Inadequately controlled with SU Met Inadequately controlled with Met (high BMI) Patients with higher cardiovascular risk mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* 10 mg QW 20 mg QW* Placebo Exenatide BID Placebo Sitagliptin Placebo Insulin glargine Pioglitazone mg QW* Placebo mg QW* Placebo BID = twice daily; BMI = body mass index; Met = metformin; QW = once weekly; SU = sulfonylurea; TZD = thiazolidinedione. *10 mg taspoglutide QW for 4 weeks followed by 20 mg QW. 35
36 Objectives of Study Primary objective To demonstrate non-inferiority of taspoglutide to insulin glargine on glycemic control (HbA 1c ) after 24 weeks of treatment in insulin-naive type 2 diabetic patients inadequately controlled with metformin and sulphonylurea combination therapy Secondary objectives To assess the effects of taspoglutide on additional parameters of glycemic control, body weight, and cardiovascular risk factors after 24 weeks To assess the safety and the tolerability of taspoglutide after 24 and 52 weeks 36
 and sulfonylurea (any dose) BMI 25 (> 23 for Asians) and 45 kg/m 2 Stable weight 5 % for at least 12")
37 Study Design: Randomized, Open-label, Parallel Group, Active-Controlled Study population HbA 1c 7.0% and 10.0% Stable doses for 12 weeks of metformin ( 1500 mg/day or individual maximally tolerated dose) and sulfonylurea (any dose) BMI 25 (> 23 for Asians) and 45 kg/m 2 Stable weight 5 % for at least 12 weeks Primary Endpoint Patient screening 10 mg Taspoglutide 10 mg QW Taspoglutide 20 mg QW Insulin glargine* Taspoglutide 10 mg QW Taspoglutide 20 mg QW Insulin glargine Follow up Long-term extension up to 3 years Sulfonylurea treatment stopped 5 days prior to start of study 4 4* 24 weeks 28-week extension 0 weeks Week weeks *Forced titration scheme to target FPG 110 mg/dl (6.1 mmol/l) Patients will receive taspoglutide 10 mg QW for 4 weeks followed by the 20 mg QW dosing 37
38 Baseline Demographic Characteristics (N=1028) Mean (SD) unless specified Taspoglutide 10 mg QW (n=361) Taspoglutide 20 mg QW (n=348) Insulin glargine (n=319) Age, years 58 (10) 57 (9) 58 (9) BMI, kg/m (5.3) 32.4 (5.3) 32.7 (5.2) HbA 1c, % 8.2 (0.9) 8.3 (0.9) 8.3 (0.9) HbA 1c baseline > 8.0%, n (%) 208 (58) 206 (59) 196 (61) FPG, mg/dl 200 (54) 199 (52) 202 (51) Diabetes duration, years 9 (6) 9 (6) 9 (6) Intent-to-treat population. 38
 Insulin glargine* (n = 319) Non-inferiority")


39 Primary Endpoint: HbA 1c Over 24 Weeks of Treatment Taspoglutide 10 mg QW (n = 361) *Final mean daily insulin glargine dose = 36 IU Taspoglutide 20 mg QW (n = 348) Insulin glargine* (n = 319) Non-inferiority margin Taspoglutide 20 mg vs insulin glargine Taspoglutide 10 mg vs insulin glargine Treatment difference for HbA 1c (%, 95% CI) LSMean = least square mean; SE = standard error. Intent-to-treat population; last-observation-carried-forward analysis. 39 Non-inferiority/Superiority Summary of HbA1c Change from Baseline at Week 24 (LOCF, ITT)




40 Percentage of Patients Reaching Target HbA 1c After 24 Weeks of Treatment Taspoglutide 10 mg QW Taspoglutide 20 mg QW Insulin glargine* HbA 1c < 7.0% HbA 1c 6.5% n= Intent-to-treat population; last-observation-carried-forward analysis. * Final mean daily insulin glargine dose = 36 IU. 40
 Taspoglutide 20 mg (baseline=190 mg/dl)")
 Change in FPG (mg/dl)")
 (LSMean SD) 50 40 30 20 10 0 10 19")

41 Change in FPG and insulin titration Taspoglutide 10 mg (baseline=190 mg/dl) Taspoglutide 20 mg (baseline=190 mg/dl) Insulin glargine (baseline=203 mg/dl) Daily Dose of Insulin Glargine (IU) Change in FPG (mg/dl) from baseline (LSMean SE) - - * * mmol/l Insulin Dose (IU/day) (LSMean SD) Time (weeks) *P < vs insulin glargine. Intent-to-treat population; LOCF analysis. Forced titration scheme to target FPG 110 mg/dl (6.1 mmol/l) 41
 Taspoglutide 20 mg QW (n=36) Insulin glargine (n=35) Baseline Week 24-14.7-27.5-1.")

42 Two-hour Postprandial Glucose (PPG) (mg/dl): Corrected for Fasting Glucose at Baseline and Week 24* Taspoglutide 10 mg QW (n=31) Taspoglutide 20 mg QW (n=36) Insulin glargine (n=35) Baseline Week Hour post-meal glucose (mg/dl) (mean SD) *Subset of patients Glucose level at 2-hr post-meal minus fasting glucose at 0 hr Change from baseline for PPG (mg/dl; mean [95% CI]) 42

 Insulin")

 * * *")

43 Change in Body Weight Over 24 Weeks of Treatment Taspoglutide 10 mg QW (n=361) Taspoglutide 20 mg QW (n=348) Insulin glargine (n=319) Baseline (kg) Change in body weight (kg) from baseline (LSMean SE) * * * * *P < vs insulin glargine. Intent-to-treat population; last-observation-carried-forward analysis. Final mean daily insulin glargine dose = 36 IU. 43
44 Safety Overview During the 24 Week Treatment Period Taspoglutide 10 mg N=364 n (%) Taspoglutide 20 mg N=351 n (%) Insulin glargine N=322 n (%) Total pts with > 1 AE 285 (78.3) 301 (85.8) 187 (58.1) Serious AEs 14 (3.8) 16 (4.6) 11 (3.4) AEs leading to discontinuation 41 (11.3) 61 (17.4) 7 (2.2) Deaths 1 (0.3) 1 2 (0.6) 1 Hypoglycemia* Reported 18 (4.9) 21 (6.0) 56 (17.4) Confirmed (< 55 mg/dl) 1 (0.3) 3 (0.9) 10 (3.1) Severe *Reported: symptoms without or without confirmation by measured plasma glucose concentration. Confirmed: symptoms accompanied by measured plasma glucose concentration 55 mg/dl. Severe: requiring assistance to actively administer carbohydrate, glucagon, or other resuscitative actions. p < vs. insulin glargine 1 Non-drug related 44 Safety population.
45 Summary of Adverse Events With 5 % Incidence Rate Taspoglutide 10 mg N=364 n (%) Taspoglutide 20 mg N=351 n (%) Insulin glargine N=322 n (%) Gastrointestinal disorders Nausea 143 (39.3) 159 (45.3) 6 (1.9) Vomiting 72 (19.8) 80 (22.8) 4 (1.2) Diarrhea 48 (13.2) 46 (13.1) 18 (5.6) General disorders and administration site conditions Injection site nodule 39 (10.7) 55 (15.7) - Injection site pruritus 26 (7.1) 17 (4.8) 1 (0.3) Metabolism and nutrition disorders Hypoglycemia 18 (4.9) 21 (6.0) 56 (17.4) Decreased appetite 30 (8.2) 35 (10.0) 2 (0.6) Infections and infestations Nasopharyngitis 20 (5.5) 20 (5.7) 25 (7.8) Nervous system disorders Headache 25 (6.9) 30 (8.5) 16 (5.0) Dizziness 19 (5.2) 16 (4.6) 7 (2.2) Safety population 45
46 Summary of Patients Withdrawn, by Reason Taspoglutide 10 mg N=364 n (%) Taspoglutide 20 mg N=351 n (%) Insulin glargine N=322 n (%) Withdrawals for any reason 76 (20.9) 74 (21.1) 29 (9.0) Adverse event * 32 (8.8) 47 (13.4) 3 (0.9) Nausea 9 (2.5) 19 (5.4) Vomiting 7 (1.9) 9 (2.6) Diarrhea 2 (0.5) 2 (0.6) Injection site reaction 2 (0.5) 2 (0.6) Fatigue 2 (0.6) Hypersensitivity 1 (0.3) 3 (0.9) Hyperglycemia 9 (2.5) 6 (1.7) 3 (0.9) Withdrew consent 15 (4.1) 14 (4.0) 8 (2.5) Failure to return 3 (0.8) 1 (0.3) 7 (2.2) Insufficient therapeutic response 18 (4.9) 8 (2.3) 4 (1.2) Refused treatment did not cooperate 4 (1.1) 2 (0.6) 4 (1.2) Administrative/other 2 (0.5) - 2 (0.6) Violation of selection criteria at entry 2 (0.5) 1 (0.3) - Death - 1 (0.3) 1 (0.3) Safety population * For individual adverse events, only those occurring 0.5% in any group are reported. 46
 Taspoglutide 20 mg (n = 351) Insulin glargine (n = 322) Nausea Vomiting % of")

47 Number of Episodes of Nausea or Vomiting Over 24 Weeks Taspoglutide 10 mg (n = 364) Taspoglutide 20 mg (n = 351) Insulin glargine (n = 322) Nausea Vomiting % of patients # of Episodes # of Episodes Safety population. Withdrawals due to nausea or vomiting: taspoglutide 10 mg: 4% taspoglutide 20 mg: 7% insulin glargine: 0% 47



48 Weekly Incidence of Nausea and Vomiting Over 24 Weeks Taspoglutide 10 mg Taspoglutide 20 mg Insulin glargine Up-titration from 10 mg to 20 mg Nausea Up-titration from 10 mg to 20 mg Vomiting Safety population 81 % and 84 % of vomiting occurred on day of injection for taspoglutide 10 mg and 20 mg, respectively. 48
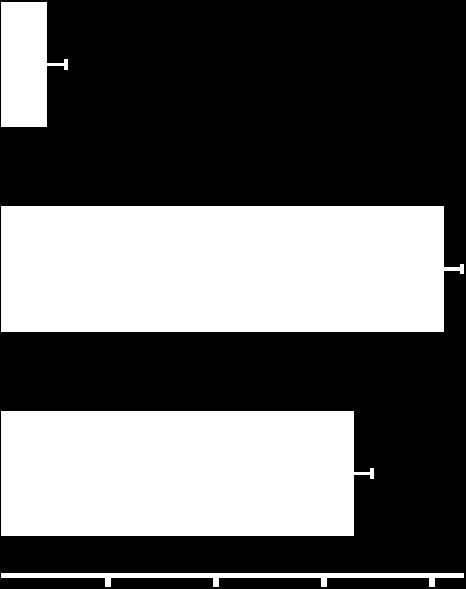
49 Summary Taspoglutide demonstrated non-inferior HbA 1c lowering ( % vs %) and better HbA 1c goal achievement of < 6.5% (24 % vs. 14 %) vs. well titrated insulin glargine (mean dose = 36 IU/d) Incidence of reported hypoglycemia was % for taspoglutide vs % for insulin glargine Taspoglutide demonstrated significant weight loss of kg (vs kg for insulin glargine) Most frequently reported adverse events for taspoglutide were gastrointestinal in nature Among patients reporting nausea or vomiting, there was predominantly a single episode that infrequently led to discontinuation and tended to occur early in treatment on the day of injection Conclusions As with other GLP-1 receptor agonists, the most common adverse events with taspoglutide are related to GI tolerability In patients with inadequate glycemic control on metformin and sulfonylurea, replacing a sulfonylurea with taspoglutide demonstrated comparable HbA 1c lowering and target HbA 1c control with a low risk of hypoglycemia and weight loss as compared to insulin glargine 49

50 Taspoglutide: Next steps Dr. Bruce Cooper, Head of Global Medical Affairs
51 Taspoglutide: The situation today Our challenge Filing delayed a minimum of 12 to 18 months Higher than expected incidence of serious hypersensitivity (<1%) Gastrointestinal tolerability profile Our response Risk mitigation plan to protect the safety of patients in the phase III programme Investigating root cause and assessing potential solutions to address hypersensitivity reactions Further studies to optimise the gastrointestinal profile Ongoing analysis of 52 weeks data from the overall T-emerge programme 51
52 What we know: Efficacy Combined benefits of robust A1c reduction, with low risk of hypoglycemia and clinically important weight loss in a simple ready-to-use weekly injection Consistent results across all studies and across a wide spectrum of Type 2 diabetes patients Statistically superior A1c reduction vs exenatide BID, sitagliptin and metformin getting up to 71% of patients to ADA HbA1c treatment goal Superior combined benefit to a well-titrated dose of insulin glargine (36IU) with significantly more patients reaching target HbA1c with less hypoglycemia and superior weight loss Both 10mg and 20mg doses are effective 20mg has higher weight loss 52
53 What we know: Safety & tolerability The type of adverse events reported are in line with the GLP-1 class Nausea and vomiting were higher than the targeted product profile, however, in general these events were mild to moderate, occurred early in the treatment course, usually on the day of injection and predominantly as a single episode Serious hypersensitivity reactions occurred late in the program and is being investigated and addressed with a risk mitigation plan Cross-study comparisons with other GLP-1s are valid only in well-conducted head to head trials 53
54 The path forward - I CV safety study T-emerge 8 continues to recruit Patients who develop anti-drug antibody levels above a pre-specified limit will be withdrawn from a study and continue to be followed up Hypersensitivity investigations Additional assessments of affected patients Additional antibody assessments including profile of other GLP-1 s Search for any factors that can be addressed Continued commitment to patient safety and transparency with decisions based on consultation with scientific, clinical and regulatory experts, and data analysis 54
55 The path forward - II Studies planned to optimise gastrointestinal tolerability E.g. dose timing, associated meal, site of injection Extension studies continue - data from T-emerge 2 at 52 weeks show: HbA1c superiority for both doses vs. exenatide Overall incidence of gastrointestinal adverse events and the incidence of adverse events leading to withdrawal were higher in each taspoglutide arm Analysis of the data ongoing Additional 52 weeks data from T-emerge trials are expected soon and will help us better inform the safety, tolerability and efficacy profile of taspoglutide Continued commitment to patient safety and transparency with decisions based on consultation with scientific, clinical and regulatory experts, and data analysis 55

56 Questions & Answers Moderator: Dr. Karl Mahler


57 We Innovate Healthcare 57
Lilly Diabetes: Pipeline Update
 Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Lilly Diabetes: Pipeline Update June 16, 2014 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's current expectations, but actual results may differ
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) (908)
 (908)") News Release FOR IMMEDIATE RELEASE Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) 423-6537 (908) 423-5185 Tracy Ogden (267) 305-0960 FDA Approves Once-Daily JANUVIA, the First and Only DPP-4
News Release FOR IMMEDIATE RELEASE Media Contacts: Amy Rose Investor Contact: Graeme Bell (908) 423-6537 (908) 423-5185 Tracy Ogden (267) 305-0960 FDA Approves Once-Daily JANUVIA, the First and Only DPP-4
Merck & Co, Inc. Announced Approval of JANUVIA TM (INN: sitagliptin), a new oral treatment of diabetes, by the US FDA
, a new oral treatment of diabetes, by the US FDA") October 23, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Phone: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Phone: +81-3-6272-1001 Merck & Co, Inc. Announced Approval of JANUVIA
October 23, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Phone: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Phone: +81-3-6272-1001 Merck & Co, Inc. Announced Approval of JANUVIA
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Galvus the most comprehensively studied DPP-4 inhibitor
 Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
Galvus the most comprehensively studied DPP-4 inhibitor! >7 000 patients enrolled in clinical studies! >4 00 patients exposed to Galvus >1 300 patients exposed 2 weeks >300 patients exposed for 104 weeks!
ADA Analyst Presentation Saturday 9 th June
 ADA Analyst Presentation Saturday 9 th June Carlo Russo Senior Vice-President & Albiglutide Team Leader, GSK Property of GlaxoSmithKline Agenda Welcome & introduction to the Harmony Clinical Programme
ADA Analyst Presentation Saturday 9 th June Carlo Russo Senior Vice-President & Albiglutide Team Leader, GSK Property of GlaxoSmithKline Agenda Welcome & introduction to the Harmony Clinical Programme
New Drug Evaluation: lixisenatide injection, subcutaneous
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited
 SMC No. (748/11) Eli Lilly and Company Limited") exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
exenatide 2mg powder and solvent for prolonged-release suspension for injection (Bydureon ) SMC No. (748/11) Eli Lilly and Company Limited 09 December 2011 The Scottish Medicines Consortium (SMC) has completed
Adlyxin. (lixisenatide) New Product Slideshow
 New Product Slideshow") Adlyxin (lixisenatide) New Product Slideshow Introduction Brand name: Adlyxin Generic name: Lixisenatide Pharmacological class: Glucagon-like peptide-1 (GLP-1) receptor agonist Strength and Formulation:
Adlyxin (lixisenatide) New Product Slideshow Introduction Brand name: Adlyxin Generic name: Lixisenatide Pharmacological class: Glucagon-like peptide-1 (GLP-1) receptor agonist Strength and Formulation:
Eli Lilly and Company
 Eli Lilly and Company Strategic Diabetes Alliance with Boehringer Ingelheim January 11 th, 2011 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's
Eli Lilly and Company Strategic Diabetes Alliance with Boehringer Ingelheim January 11 th, 2011 Safe Harbor Provision This presentation contains forward-looking statements that are based on management's
Efficacy/pharmacodynamics: 85 Safety: 89
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor/Company: Sanofi Drug substance:
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor/Company: Sanofi Drug substance:
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Le incretine: un passo avanti. Francesco Dotta
 Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
Le incretine: un passo avanti Francesco Dotta U.O.C. Diabetologia, Policlinico Le Scotte Università di Siena Fondazione Umberto Di Mario ONLUS Toscana Life Science Park Incretins: multiple targets multiple
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
23-Aug-2011 Lixisenatide (AVE0010) - EFC6014 Version number: 1 (electronic 1.0)
 - EFC6014 Version number: 1 (electronic 1.0)") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top of metformin
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top of metformin
Scottish Medicines Consortium
 Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
Scottish Medicines Consortium liraglutide 6mg/mL prefilled pen for injection (3mL) (Victoza ) Novo Nordisk Ltd. No. (585/09) 06 November 2009 The Scottish Medicines Consortium (SMC) has completed its assessment
SYNOPSIS. Administration: subcutaneous injection Batch number(s):
:") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, 2-arm parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, 2-arm parallel-group, multicenter 24-week study followed by an extension assessing the efficacy and safety of AVE0010 on top
These results are supplied for informational purposes only.
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: sanofi-aventis ClinialTrials.gov
Amylin Pharmaceuticals: Creating Value as a Leader in the Treatment of Diabetes
 Amylin Pharmaceuticals: Creating Value as a Leader in the Treatment of Diabetes Daniel M. Bradbury President & Chief Executive Officer JPMorgan Healthcare Conference January 12, 2009 Safe Harbor Statement
Amylin Pharmaceuticals: Creating Value as a Leader in the Treatment of Diabetes Daniel M. Bradbury President & Chief Executive Officer JPMorgan Healthcare Conference January 12, 2009 Safe Harbor Statement
Sponsor Novartis. Generic Drug Name Vildagliptin/Metformin. Therapeutic Area of Trial Type 2 diabetes. Approved Indication Type 2 diabetes
 Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Clinical Trial Results Database Page 1 Sponsor Novartis Generic Drug Name Vildagliptin/Metformin Therapeutic Area of Trial Type 2 diabetes Approved Indication Type 2 diabetes Study Number CLMF237A2309
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
XP23829 PHASE 2 PSORIASIS TRIAL PRELIMINARY TOPLINE DATA PRESENTATION SEPTEMBER 15, 2015 COPYRIGHT 2015 XENOPORT, INC. ALL RIGHTS RESERVED.
 XP23829 PHASE 2 PSORIASIS TRIAL PRELIMINARY TOPLINE DATA PRESENTATION SEPTEMBER 15, 2015 COPYRIGHT 2015 XENOPORT, INC. ALL RIGHTS RESERVED. SAFE HARBOR DISCLAIMER These slides and the accompanying oral
XP23829 PHASE 2 PSORIASIS TRIAL PRELIMINARY TOPLINE DATA PRESENTATION SEPTEMBER 15, 2015 COPYRIGHT 2015 XENOPORT, INC. ALL RIGHTS RESERVED. SAFE HARBOR DISCLAIMER These slides and the accompanying oral
Xultophy 100/3.6. (insulin degludec, liraglutide) New Product Slideshow
 New Product Slideshow") Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
Xultophy 100/3.6 (insulin degludec, liraglutide) New Product Slideshow Introduction Brand name: Xultophy Generic name: Insulin degludec, liraglutide Pharmacological class: Human insulin analog + glucagon-like
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 2 December 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 2 December 2009 VICTOZA 6 mg/ml solution for injection in pre-filled pen Pack size of two 3 ml pens (CIP: 396 323-6)
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 2 December 2009 VICTOZA 6 mg/ml solution for injection in pre-filled pen Pack size of two 3 ml pens (CIP: 396 323-6)
To assess the safety and tolerability in each treatment group.
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
Results of Phase III Studies of Sitagliptin, new oral treatment of diabetes, were presented by Merck & Co., Inc. at ADA (The 2 nd Announcement)
") June 14, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Tel: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Tel: +81-3-6272-1001 Results of Phase III Studies of Sitagliptin, new
June 14, 2006 Ono Pharmaceutical Co., Ltd., Public Relations Tel: +81-6-6263-5670 Banyu Pharmaceutical Co., Ltd., Public Relations Tel: +81-3-6272-1001 Results of Phase III Studies of Sitagliptin, new
Sponsor: Sanofi. According to template: QSD VERSION N 5.0 (04-APR-2016) Page 1
 Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor: Sanofi Drug substance(s):
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Study Code: Date: 27 July 2007
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Soliqua 100/33. (insulin glargine, lixisenatide) New Product Slideshow
 New Product Slideshow") Soliqua 100/33 (insulin glargine, lixisenatide) New Product Slideshow Introduction Brand name: Soliqua 100/33 Generic name: Insulin glargine (rdna origin), lixisenatide Pharmacological class: Human insulin
Soliqua 100/33 (insulin glargine, lixisenatide) New Product Slideshow Introduction Brand name: Soliqua 100/33 Generic name: Insulin glargine (rdna origin), lixisenatide Pharmacological class: Human insulin
Roche Diagnostics Daniel O Day COO Roche Diagnostics. Société Générale - The Premium Review Conference, Paris December 2, 2011
 This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as believes, expects, anticipates, projects, intends, should, seeks, estimates,
This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as believes, expects, anticipates, projects, intends, should, seeks, estimates,
Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes
 PRESS RELEASE Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes Dublin, Ireland (15 June 2012) Sanofi presented results
PRESS RELEASE Sanofi Announces Results of ORIGIN, the World s Longest and Largest Randomised Clinical Trial in Insulin in Pre- and Early Diabetes Dublin, Ireland (15 June 2012) Sanofi presented results
CURRENT CONTROVERSIES IN DIABETES CARE
 CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
CURRENT CONTROVERSIES IN DIABETES CARE Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Diabetes Mellitus: U.S. Impact
SYNOPSIS 2/198 CSR_BDY-EFC5825-EN-E02. Name of company: TABULAR FORMAT (For National Authority Use only)
") SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, fixed-dose (rimonabant 20 mg) multicenter study of long-term glycemic control with rimonabant in treatment-naïve
SYNOPSIS Title of the study: A randomized, double-blind, placebo-controlled, parallel-group, fixed-dose (rimonabant 20 mg) multicenter study of long-term glycemic control with rimonabant in treatment-naïve
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Science, patient benefits and productivity
 Science, patient benefits and productivity Alan Hippe, CFO Roche Group London, November 2017 This presentation contains certain forward-looking statements. These forward-looking statements may be identified
Science, patient benefits and productivity Alan Hippe, CFO Roche Group London, November 2017 This presentation contains certain forward-looking statements. These forward-looking statements may be identified
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Roche Lazard Capital Markets 7 th Annual Healthcare Conference. Thomas Kudsk Larsen, 17 November 2010
 Roche Lazard Capital Markets 7 th Annual Healthcare Conference Thomas Kudsk Larsen, 17 November 2010 This presentation contains certain forward-looking statements. These forward-looking statements may
Roche Lazard Capital Markets 7 th Annual Healthcare Conference Thomas Kudsk Larsen, 17 November 2010 This presentation contains certain forward-looking statements. These forward-looking statements may
Sponsor / Company: Sanofi Drug substance(s): Insulin Glargine. Study Identifiers: NCT
: Insulin Glargine. Study Identifiers: NCT") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
A Review of the Long-Term Efficacy, Tolerability, and Safety of Exenatide Once Weekly for Type 2 Diabetes
 Adv Ther (2017) 34:1791 1814 DOI 10.1007/s12325-017-0499-6 REVIEW A Review of the Long-Term Efficacy, Tolerability, and Safety of Exenatide Once Weekly for Type 2 Diabetes Stefano Genovese. Edoardo Mannucci.
Adv Ther (2017) 34:1791 1814 DOI 10.1007/s12325-017-0499-6 REVIEW A Review of the Long-Term Efficacy, Tolerability, and Safety of Exenatide Once Weekly for Type 2 Diabetes Stefano Genovese. Edoardo Mannucci.
Pricing and Reimbursement Assessment for Roche s RO507 in Germany. Final Report Excerpt
 Pricing and Reimbursement Assessment for Roche s RO507 in Germany Final Report Excerpt February 29, 2008 Current Treatment and Reimbursement Situation in Germany Final Report_Roche Diabetes February 29,
Pricing and Reimbursement Assessment for Roche s RO507 in Germany Final Report Excerpt February 29, 2008 Current Treatment and Reimbursement Situation in Germany Final Report_Roche Diabetes February 29,
CURRENT ISSUES IN DIABETES MANAGEMENT. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test. Diagnosis of Diabetes 2013
 CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
CURRENT ISSUES IN DIABETES MANAGEMENT Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening for Diabetes 2013 BMI
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
T max V d t 1/ hours 100 L 3 hours
 Brand Name: Adlyxin Generic Name: lixisenatide Manufacturer: Sanofi-Aventis U.S. LLC 1 Drug Class: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonist 2,3,4 Uses: Labeled Uses 1,2,3,4,5 : Type 2 diabetes
Brand Name: Adlyxin Generic Name: lixisenatide Manufacturer: Sanofi-Aventis U.S. LLC 1 Drug Class: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonist 2,3,4 Uses: Labeled Uses 1,2,3,4,5 : Type 2 diabetes
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
SCIENTIFIC STUDY REPORT
 PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
PAGE 1 18-NOV-2016 SCIENTIFIC STUDY REPORT Study Title: Real-Life Effectiveness and Care Patterns of Diabetes Management The RECAP-DM Study 1 EXECUTIVE SUMMARY Introduction: Despite the well-established
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO
 The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
The Highlights of the AWARD Clinical Program FRANCESCO GIORGINO DEPARTMENT OF EMERGENCY AND ORGAN TRANSPLANTATION SECTION OF INTERNAL MEDICINE, ENDOCRINOLOGY, ANDROLOGY AND METABOLIC DISEASES Disclaimer
ClinialTrials.gov Identifier: HOE901_4020 Insulin Glargine Date: Study Code: This was a multicenter study that was conducted at 59 US sites
 These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription Sponsor/company: Generic drug name:
Beyond Topline Results for the Oral (Non-Peptide) GLP-1R Agonist TTP273 in Type 2 Diabetes: How Much and When?
 GLP-1R Agonist TTP273 in Type 2 Diabetes: How Much and When?") Beyond Topline Results for the Oral (Non-Peptide) GLP-1R Agonist TTP273 in Type 2 Diabetes: How Much and When? Jennifer LR Freeman, Imogene Dunn and Carmen Valcarce Disclaimers The statements made in this
Beyond Topline Results for the Oral (Non-Peptide) GLP-1R Agonist TTP273 in Type 2 Diabetes: How Much and When? Jennifer LR Freeman, Imogene Dunn and Carmen Valcarce Disclaimers The statements made in this
GLP-1 Receptor Agonists and SGLT-2 Inhibitors. Debbie Hicks
 GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
GLP-1 Receptor Agonists and SGLT-2 Inhibitors Debbie Hicks Prescribing and Adverse Event reporting information is available at this meeting from the AstraZeneca representative The views expressed by the
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: Last Review Date: 02.
 Receptor Agonists Reference Number: HIM.PA.53 Effective Date: Last Review Date: 02.") Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.19 Line of Business: HIM Revision Log See Important Reminder
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.19 Line of Business: HIM Revision Log See Important Reminder
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace See Important
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace See Important
Clinical Trial Synopsis TL-OPI-518, NCT#
 Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Clinical Trial Synopsis, NCT# 00225264 Title of Study: A Double-Blind, Randomized, Comparator-Controlled Study in Subjects With Type 2 Diabetes Mellitus Comparing the Effects of Pioglitazone HCl vs Glimepiride
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Sponsor / Company: Sanofi Drug substance(s): Insulin Glargine (HOE901) Insulin Glulisine (HMR1964)
: Insulin Glargine (HOE901) Insulin Glulisine (HMR1964)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Roche Committed to innovation and profitable growth. Dr. Alan Hippe CFO Roche. Zurich, May 2011
 Roche Committed to innovation and profitable growth Dr. Alan Hippe CFO Roche Zurich, May 2011 2 This presentation contains certain forward-looking statements. These forward-looking statements may be identified
Roche Committed to innovation and profitable growth Dr. Alan Hippe CFO Roche Zurich, May 2011 2 This presentation contains certain forward-looking statements. These forward-looking statements may be identified
SYNOPSIS OF RESEARCH REPORT (PROTOCOL BC20779)
") TITLE OF THE STUDY / REPORT No. / DATE OF REPORT INVESTIGATORS / CENTERS AND COUNTRIES Clinical Study Report Protocol BC20779: Multicenter, double-blind, randomized, placebo-controlled, dose ranging phase
TITLE OF THE STUDY / REPORT No. / DATE OF REPORT INVESTIGATORS / CENTERS AND COUNTRIES Clinical Study Report Protocol BC20779: Multicenter, double-blind, randomized, placebo-controlled, dose ranging phase
CURRENT STATEGIES IN DIABETES MELLITUS DIABETES. Recommendations for Adults CURRENT STRATEGIES IN DIABETES MELLITUS. Diabetes Mellitus: U.S.
 CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
CURRENT STATEGIES IN DIABETES MELLITUS Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Diabetes Mellitus: U.S. Impact ~1 Million Type 1 DIABETES 16.7 Million IFG (8.3%) 12.3
Clinical Trial Synopsis TL-OPI-525, NCT#
 Clinical Trial Synopsis, NCT#00762736 Title of Study: A Phase II, Double-Blind, Randomized, Placebo-Controlled, Proof-of-Concept Study of the Efficacy, Safety, and Tolerability of Pioglitazone HCl (ACTOS
Clinical Trial Synopsis, NCT#00762736 Title of Study: A Phase II, Double-Blind, Randomized, Placebo-Controlled, Proof-of-Concept Study of the Efficacy, Safety, and Tolerability of Pioglitazone HCl (ACTOS
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018
 GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
GLP-1 RECEPTOR AGONIST SHOULD I TRY IT? VERONICA BRADY, PHD, BC-ADM, CDE PROJECT ECHO JUNE 21, 2018 SOMETHING TO CONSIDER IF YOU COULD PRESCRIBE A MEDICATION FOR YOUR PATIENT WITH DIABETES THAT: DECREASED
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
National Horizon Scanning Centre. Saxagliptin (BMS ) for type 2 diabetes. April 2008
 for type 2 diabetes. April 2008") Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
Sponsor / Company: Sanofi Drug substance(s): AMARYL M (1/250 mg) / HOE490
: AMARYL M (1/250 mg) / HOE490") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Jefferies Healthcare Conference. June 25, 2008
 Jefferies Healthcare Conference June 25, 2008 Safe Harbor Statement Except for the historical information set forth herein, the matters set forth in this presentation,including without limitation statements
Jefferies Healthcare Conference June 25, 2008 Safe Harbor Statement Except for the historical information set forth herein, the matters set forth in this presentation,including without limitation statements
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Results of Phase II Studies of Sitagliptin (MK-0431 / ONO-5345) Investigational Treatment for Type 2 Diabetes Presented by Merck & Co., Inc.
 Investigational Treatment for Type 2 Diabetes Presented by Merck & Co., Inc.") Ono Pharmaceutical Co., Ltd., Public Relations Tel: +81-6-6263-5670 June 13, 2005 Banyu Pharmaceutical Co., Ltd., Public Relations Tel: +81-3-5203-8105 Results of Phase II Studies of Sitagliptin (MK-0431
Ono Pharmaceutical Co., Ltd., Public Relations Tel: +81-6-6263-5670 June 13, 2005 Banyu Pharmaceutical Co., Ltd., Public Relations Tel: +81-3-5203-8105 Results of Phase II Studies of Sitagliptin (MK-0431
Sponsor / Company: Sanofi Drug substance(s): HOE901-U300 (insulin glargine) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1
: HOE901-U300 (insulin glargine) According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
AVEO and Astellas Announce Positive Findings from TIVO-1 Superiority Study of Tivozanib in First-Line Advanced RCC
 FOR IMMEDIATE RELEASE AVEO and Astellas Announce Positive Findings from TIVO-1 Superiority Study of Tivozanib in First-Line Advanced RCC - Tivozanib is the First Agent to Demonstrate Greater than One Year
FOR IMMEDIATE RELEASE AVEO and Astellas Announce Positive Findings from TIVO-1 Superiority Study of Tivozanib in First-Line Advanced RCC - Tivozanib is the First Agent to Demonstrate Greater than One Year
Management of Diabetes Mellitus: A Primary Care Perspective
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Study 2 ( ) Pivotal Phase 3 Study Top-Line Results. October 29, 2018
 Pivotal Phase 3 Study Top-Line Results. October 29, 2018") Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
Study 2 (1002-047) Pivotal Phase 3 Study Top-Line Results October 29, 2018 Safe Harbor Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection
 New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
New Drug Evaluation: Insulin degludec/aspart, subcutaneous injection Date of Review: March 2016 End Date of Literature Search: November 11, 2015 Generic Name: Insulin degludec and insulin aspart Brand
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
Management of Diabetes Mellitus: A Primary Care Perspective. Screening for Diabetes Advantages of HbA1c as a Diagnostic Test
 Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Management of Diabetes Mellitus: A Primary Care Perspective Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest Screening
Sponsor / Company: Sanofi Drug substance(s): Insulin Glargine. According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1
: Insulin Glargine. According to template: QSD VERSION N 4.0 (07-JUN-2012) Page 1") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
NCT Number: NCT
 Efficacy and safety of insulin glargine 300 U/mL vs insulin degludec 100 U/mL in insulin-naïve adults with type 2 diabetes mellitus: Design and baseline characteristics of the BRIGHT study Alice Cheng
Efficacy and safety of insulin glargine 300 U/mL vs insulin degludec 100 U/mL in insulin-naïve adults with type 2 diabetes mellitus: Design and baseline characteristics of the BRIGHT study Alice Cheng
American Diabetes Association 65 th Annual Scientific Sessions. Investor Reception June 12, 2005
 American Diabetes Association 65 th Annual Scientific Sessions Investor Reception June 12, 2005 Safe Harbor Statement > This presentation contains forward-looking statements about Amylin. Our actual results
American Diabetes Association 65 th Annual Scientific Sessions Investor Reception June 12, 2005 Safe Harbor Statement > This presentation contains forward-looking statements about Amylin. Our actual results
R. Ratner, M. Nauck*, C. Kapitza, V. Asnaghi, M. Boldrin and R. Balena
 Original Article: Treatment Safety and tolerability of high doses of taspoglutide, a once-weekly human GLP-1 analogue, in diabetic patients treated with metformin: a randomized double-blind placebo-controlled
Original Article: Treatment Safety and tolerability of high doses of taspoglutide, a once-weekly human GLP-1 analogue, in diabetic patients treated with metformin: a randomized double-blind placebo-controlled
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP
 Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the
Sitagliptin: first DPP-4 inhibitor to treat type 2 diabetes Steve Chaplin MSc, MRPharmS and Andrew Krentz MD, FRCP KEY POINTS sitagliptin (Januvia) is a DPP-4 inhibitor that blocks the breakdown of the