Copyright 2017 by Sea Courses Inc.
|
|
|
- Andra Neal
- 6 years ago
- Views:
Transcription
1 Diabetes and Lipids
2 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical, including photocopying, recording, or information storage and retrieval systems without prior written permission of Sea Courses Inc. except where permitted by law. Sea Courses is not responsible for any speaker or participant s statements, materials, acts or omissions.
3
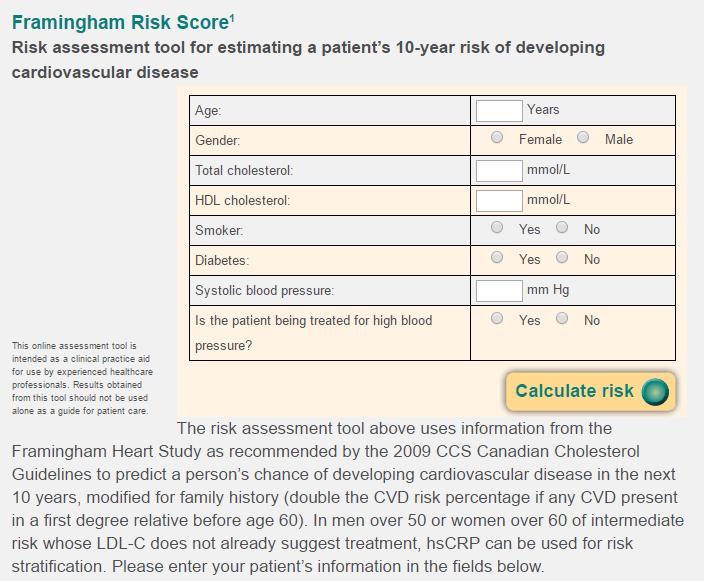
4 With respect to (LDL) cholesterol. Should we be checking LDL (or other lipid fractions)? What is the normal range? Is there an upper limit to the range? Is there a lower limit to the range? What are the targets in people with diabetes? What should the targets be? Is the cholesterol hypothesis proven? Hypothesis or fact?
5 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Small interfering RNA Etc..
6 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Small interfering RNA Etc..
7
8
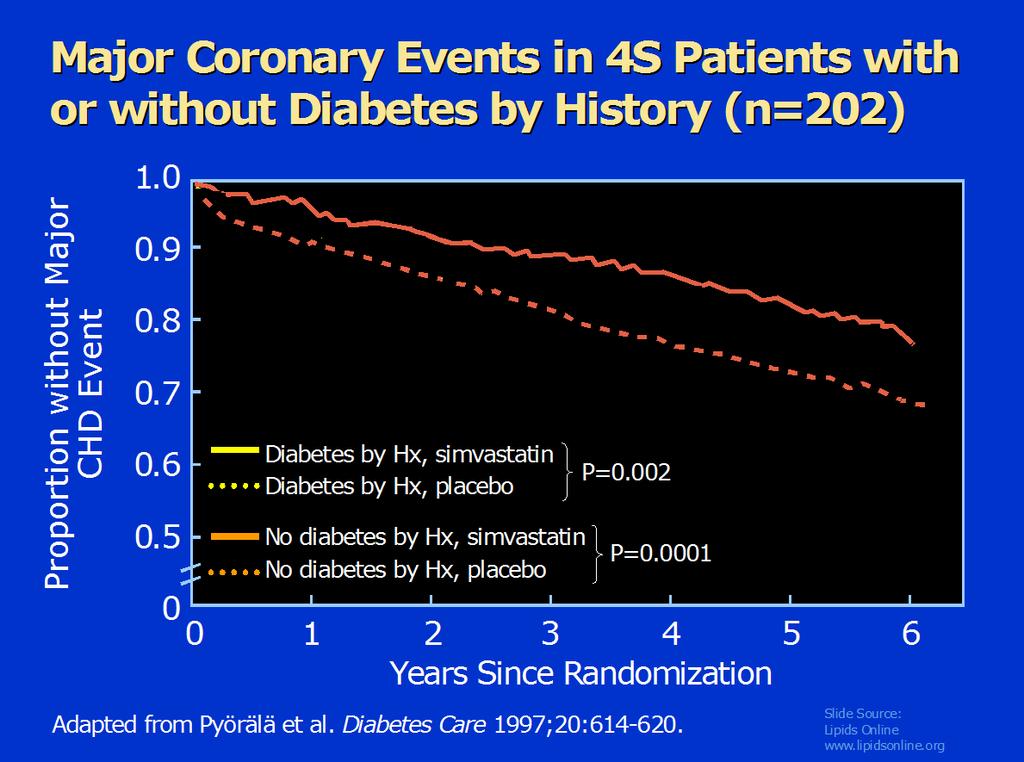
9 Proportion without Major CHD Event Major Coronary Events in 4S Patients with or without Diabetes by History (n=202) Diabetes by Hx, simvastatin Diabetes by Hx, placebo No diabetes by Hx, simvastatin No diabetes by Hx, placebo P=0.002 P= Years Since Randomization Adapted from Pyörälä et al. Diabetes Care 1997;20: Slide Source: Lipids Online
10 CARDS placebo Atorva 10
11 TNT: Diabetes Subgroup
12
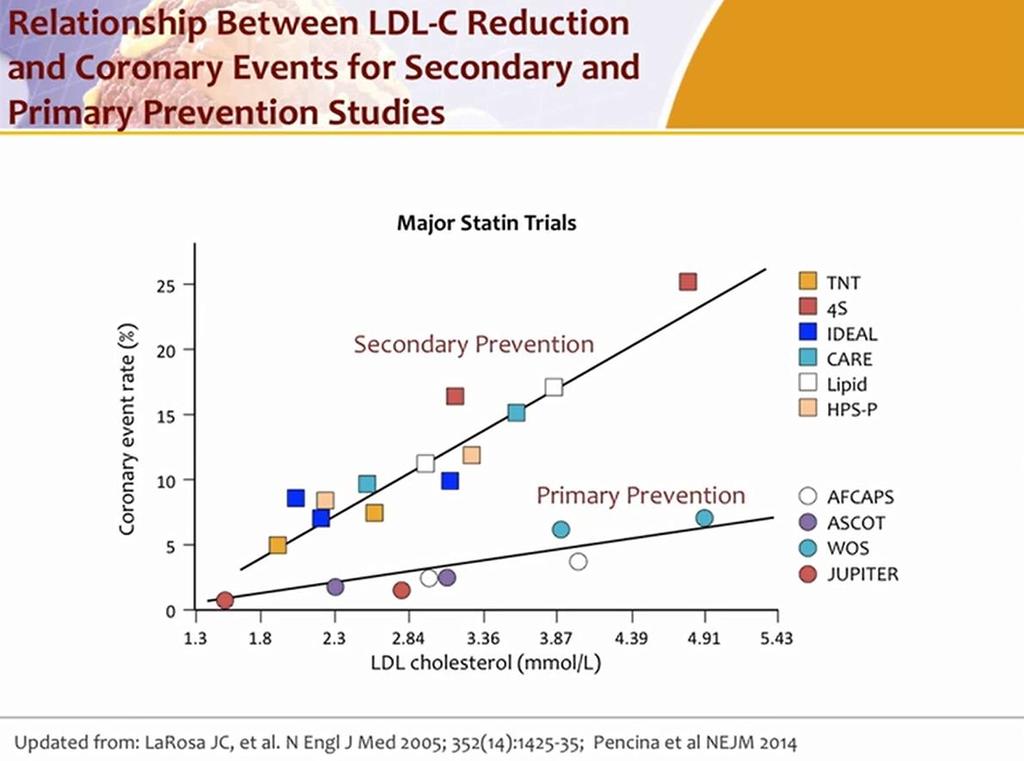
13 With DM There is no question that treating diabetics with statins lowers CV risk.
14 With DM The resulting lower risk achieved still exceeds non-diabetics

15 With DM There does not seem to be a LDL below which risk does not continue to drop
16 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Etc..
17 Should every diabetic be treated with a statin?
18 USA guidelines: how do they compare?
19 Who Should Receive Statins? yrs old or Macrovascular disease or Microvascular disease or DM >15 yrs duration and age >30 yrs or Warrant therapy based on (other) Canadian Cardiovascular Society lipid guidelines guidelines.diabetes.ca BANTING ( ) diabetes.ca Copyright 2013 Canadian Diabetes Association

20 If on therapy, target LDL 2.0 mmol/l (77.2 mg/dl)
21 Slide 21
22 Slide 22

23 USA guidelines: how do they compare?
24 24
25 A New Perspective on LDL-C and Non-HDL-C goals The expert panel was unable to find RCT evidence to support continued use of specific LDL-C and/or non-hdl-c treatment targets 25
26 Proportion without Major CHD Event Major Coronary Events in 4S Patients with or without Diabetes by History (n=202) Diabetes by Hx, simvastatin Diabetes by Hx, placebo No diabetes by Hx, simvastatin No diabetes by Hx, placebo P=0.002 P= Years Since Randomization Adapted from Pyörälä et al. Diabetes Care 1997;20: Slide Source: Lipids Online
27 placebo Atorva 10 CARDS

28 NEJM 350;15 April

29 TNT: Diabetes Subgroup
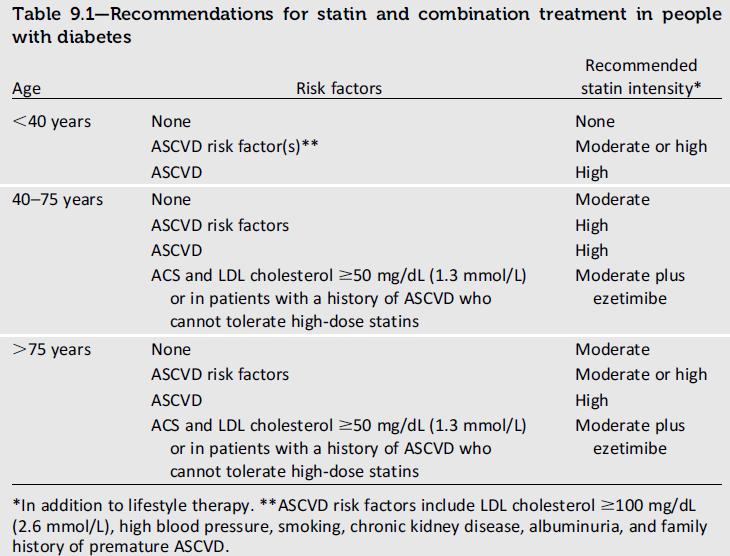
30 A New Perspective on LDL-C and Non-HDL-C goals The expert panel was unable to find RCT evidence to support continued use of specific LDL-C and/or non-hdl-c treatment targets 4 major statin benefit groups were identified for whom the ASCVD risk reduction clearly outweighs the risk of adverse events.3) diabetes aged years with LDL-C mg/dl and without ASCVD 30
31 A New Perspective on LDL-C and Non-HDL-C goals The expert panel was unable to find RCT evidence to support continued use of specific LDL-C and/or non-hdl-c treatment targets 4 major statin benefit groups were identified for whom the ASCVD risk reduction clearly outweighs the risk of adverse events.3) diabetes aged years with LDL-C mmol/l and without ASCVD 31
32 The difficulty of giving up the treat to goal paradigm was deliberated extensively over a 3-year period Use of LDL-C targets may result in under-treatment with evidence based statin therapy
33 33
34
35 Scenario 1 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.0 mmol/l (155 mg/dl) HDL: 1.1 mmol/l (42 mg/dl) LDL: 2.4 (96 mg/dl) Triglyceride: 2.2 mmol/l (200 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Would more information help?
36 Scenario 1 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.0 mmol/l (155 mg/dl) HDL: 1.1 mmol/l (42 mg/dl) LDL: 2.4 (96 mg/dl) Triglyceride: 2.2 mmol/l (200 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Would more information help?
37 Scenario 1 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.0 mmol/l (155 mg/dl) HDL: 1.1 mmol/l (42 mg/dl) LDL: 2.4 (96 mg/dl) Triglyceride: 2.2 mmol/l (200 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Would more information help?
38 39
39 Scenario 1 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.0 mmol/l (155 mg/dl) HDL: 1.1 mmol/l (42 mg/dl) LDL: 2.4 (96 mg/dl) Triglyceride: 2.2 mmol/l (200 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Would more information help?
40 Scenario 2 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 20 mg. TC: 3.75 mmol/l (150 mg/dl) HDL: 1.24 mmol/l (49.6 mg/dl) LDL: 1.7 mmol/l (68 mg/dl) Triglyceride: 1.55 mmol/l (141 mg/dl) A1c: 6.9% Are his lipids optimally controlled? 41
 HDL: 1.24 mmol/l (49.6 mg/dl) LDL: 1.7 mmol/l (68 mg/dl) Triglyceride: 1.55 mmol/l (141 mg/dl) A1c: 6.9% Are his lipids optimally controlled?")
41 Scenario 3 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 20 mg. Had an MI 6 mos ago TC: 3.75 mmol/l (150 mg/dl) HDL: 1.24 mmol/l (49.6 mg/dl) LDL: 1.7 mmol/l (68 mg/dl) Triglyceride: 1.55 mmol/l (141 mg/dl) A1c: 6.9% Are his lipids optimally controlled? 42
42 Scenario 4 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago TC: 2.4 mmol/l (95 mg/dl) HDL:.9 mmol/l (35 mg/dl) LDL: 1.0 mmol/l (39 mg/dl) Triglyceride: 1.1 mmol/l (100 mg/dl) A1c: 6.9% Are his lipids optimally controlled? 43
43 Scenario 4 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago TC: 2.4 mmol/l (95 mg/dl) HDL:.9 mmol/l (35 mg/dl) LDL: 1.0 mmol/l (39 mg/dl) Triglyceride: 1.1 mmol/l (100 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Would you decrease the statin? 44
44 Scenario 4 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago TC: 2.4 mmol/l (95 mg/dl) HDL:.9 mmol/l (35 mg/dl) LDL: 1.0 mmol/l (39 mg/dl) Triglyceride: 1.1 mmol/l (100 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Would you decrease the statin? Would LESS information help? 45
45 Scenario 4 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg. Had MI 6 mos ago TC: 2.4 mmol/l (96mg/dl) HDL:.9 mmol/l (36 mg/dl) LDL: 1.0 mmol/l (40mg/dl) Triglyceride: 1.1 mmol/l (100 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Would you decrease the statin? Would LESS information help? 46
46 The difficulty of giving up the treat to goal paradigm was deliberated extensively over a 3-year period Use of LDL-C targets may result in under-treatment with evidence based statin therapy

47


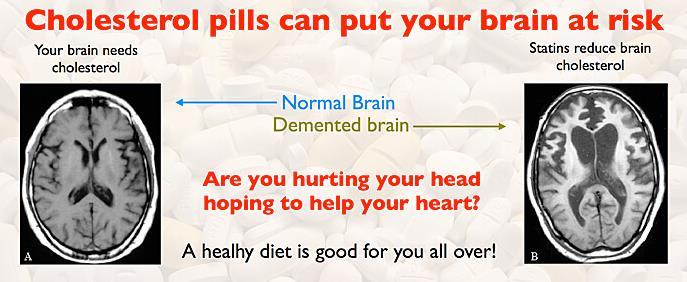
48 Media, internet, print, etc
49 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Etc..
50
 vs Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary")
51 IMProved Reduction of Outcomes: Vytorin Efficacy International Trial A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin (Ezetimibe/Simvastatin Tablet) vs Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary Syndrome
52 Study Design Patients stabilized post ACS 10 days: LDL-C mmol/l ( mmol/l if prior lipid-lowering Rx) N=18,144 Standard Medical & Interventional Therapy Simvastatin 40 mg Uptitrated to Simva 80 mg if LDL-C > 2.05 (adapted per FDA label 2011) Ezetimibe / Simvastatin 10 / 40 mg Follow-up Visit Day 30, every 4 months 90% power to detect ~9% difference Duration: Minimum 2 ½-year follow-up (at least 5250 events) Primary Endpoint: CV death, MI, hospital admission for UA, coronary revascularization ( 30 days after randomization), or stroke Cannon CP AHJ 2008;156:826-32; Califf RM NEJM 2009;361:712-7; Blazing MA AHJ 2014;168:
53 Mean LDL-C (mmol/l) LDL-C and Lipid Changes 1 Yr Mean LDL-C TC TG HDL hscrp 2.5 Simva mg/dl EZ/Simva mg/dl 2.25 Δ in mmol/l mg/dl Number at risk: QE R Time since randomization (months) 54
54 Mean LDL-C (mmol/l) LDL-C and Lipid Changes 1 Yr Mean LDL-C TC TG HDL hscrp 2.5 Simva mg/dl EZ/Simva mg/dl 2.25 Δ in mg/dl mg/dl Number at risk: QE R Time since randomization (months) 55

55 CV Death, Non-fatal MI, or Non-fatal Stroke HR 0.90 CI (0.84, 0.97) p=0.003 NNT= 56 Simva 22.2% 1704 events EZ/Simva 20.4% 1544 events 7-year event rates 56

56 Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015


57 Cannon CP, et al. N Engl J Med. 2015;372: Supplementary Appendix. Unpublished Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015

58 Cannon CP, et al. N Engl J Med. 2015;372: Supplementary Appendix. Giugliano et al. Hotline sessions, ESC2015, London, UK, August 30thth 2015
59
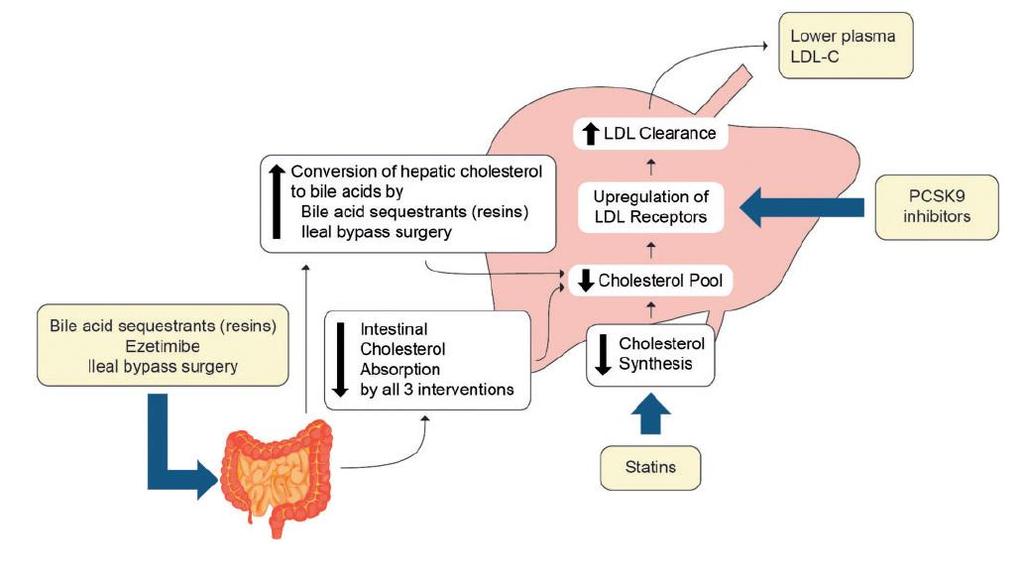
60 LDL Receptor Function and Life Cycle For illustration purposes only 61 61

61 The Role of PCSK9 in the Regulation of LDL Receptor Expression 62 For illustration purposes only
62 Impact of PCSK9 inhibitors on LDL Receptor Expression For illustration purposes only 63 63
63 LS mean (SE) % change in LDL-C Level at week 8/12 LOCF Pooled Results: % Change from Baseline in LDL-C at Week 8/12 by Baseline LDL-C, non-hdl-c and Apo B Placebo Alirocumab 150 mg Q2W 0% Baseline LDL-C subgroup Baseline non-hdl-c subgroup 3.36 mmol/l >3.36 mmol/l <4.3 mmol/l 4.3 mmol/l n=43 n=66 n=32 n=38 n=49 n=77 n=26 n=27 Baseline Apo B subgroup <1.1 g/l 1.1 g/l 130 mg/dl >130 mg/dl <166 mg/dl 166 mg/dl <110 mg/dl 110 mg/dl n=46 n=59 n=28 n=44-10% -20% -8.5% (2.9) -13.5% (3.2) -8.6% (2.9) -14.0% (4.2) -7.4% (2.8) -14.7% (3.8) -30% -40% -50% -60% -70% -69.7% (2.4) -66.4% (2.9) -68.4% (2.5) -68.1% (4.2) -69.2% (2.7) Cut-offs for LDL-C (3.36 mmol/l, 130 mg/dl) and non-hdl-c (4.3 mmol/l, 166 mg/dl) based on thresholds for starting therapy in patients at, respectively, moderate/moderately high cardiovascular (CV) risk in the most recent US cholesterol management (ATP III) guidelines -80% 1 and intermediate CV risk in the 2012 Canadian dyslipidemia guidelines 2. Cut-off for Apo B (1.1 g/l, 110 mg/dl) based on value derived by regression analysis from consensus target LDL-C and non-hdl-c values 3 and threshold for initiatiing therapy in intermediate-risk patients in the 2012 Canadian guidelines Grundy et al. Circulation. 2004;110: Anderson et al. Can J Cardiol. 2013; Soran et al. Ann Clin Biochem 2011;48[Pt6]: Data pooled from mitt population of studies 1003 (NCT ), (NCT ), and (NCT ) % (3.0) 64
64
65
66
67 i.e., MACE

68 Adverse events were NOT more common if LDL was VERY low Unpublished data
69 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Etc..

70 71
71
72

73
74 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Etc..
75
76
77
78
79
80
81
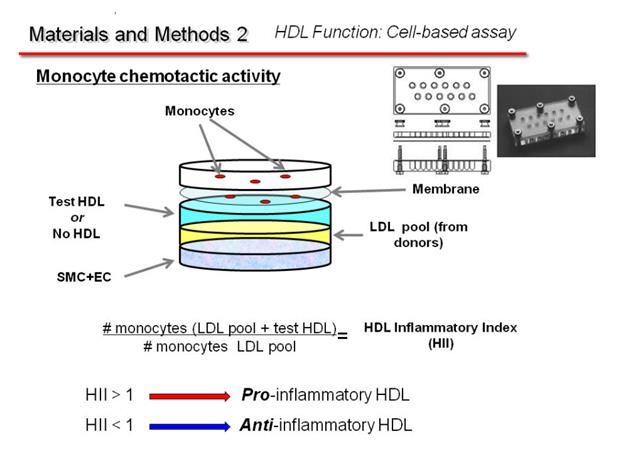
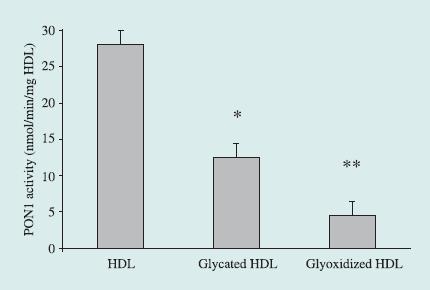
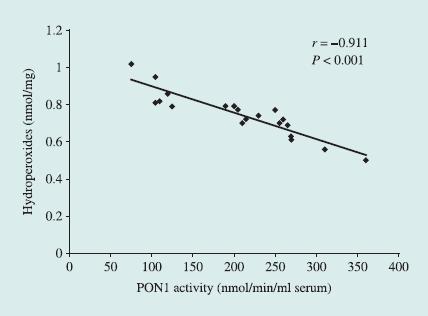
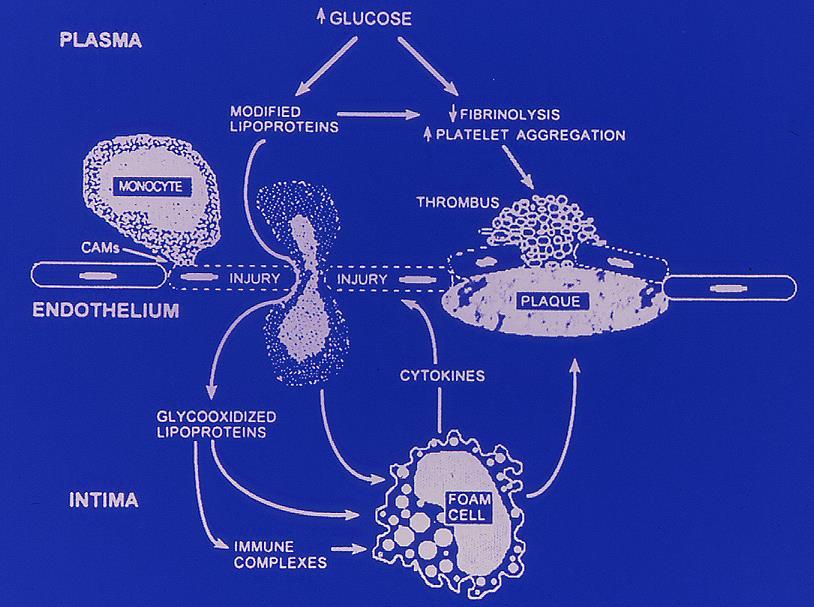
82 Does glycemic control affect the function of lipids? If it does, then should the degree of glycemic control affect our recommendations for treating the lipids?
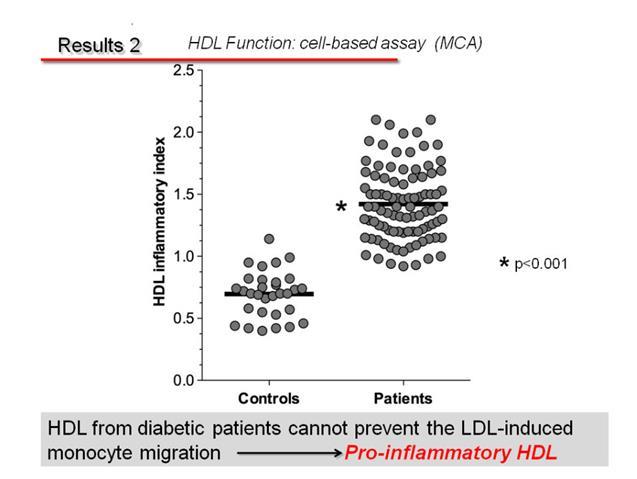
83 HDL and Anti-Atherosclerosis Inhibition of Adhesion Molecules Monocyte LDL Vessel Lumen Adhesion Molecules MCP-1 LDL Endothelium Cytokines Modified LDL Macrophage Foam Cell Intima Cockerill GW et al. Arterioscler Thromb Vasc Biol 1995;15: Slide Source: Lipids Online
84 HDL and Anti-Atherosclerosis Inhibition of Adhesion Molecules Monocyte HDL Inhibits Chemotaxis and inhibits Adhesion Molecule Expression LDL Vessel Lumen Adhesion Molecules Cytokines MCP-1 LDL Modified LDL Endothelium HDL Inhibit Oxidation of LDL Macrophage Foam Cell HDL Promote Cholesterol Efflux Intima Cockerill GW et al. Arterioscler Thromb Vasc Biol 1995;15: Slide Source: Lipids Online

85 86
86 87
87 88
88 89
89 90

90 Presented at ADA San Diego
91 92
92 93
93 94

94 Mean A1c 7.6% 95
95 96
96 97
97 98
98 99
99 100
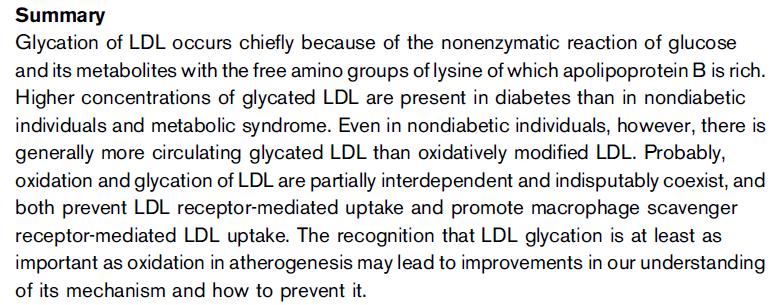
100 Glycated LDL and HDL Glycemic control may play a role in how atherogenic the lipoproteins may be Guidelines don t specifically recommend it, but if you have someone with an A1c of 6.5% vs A1c of 8.5%, you might choose to be more aggressive treating the lipids of the latter. Some Type 1 s have HDL of 2 or more. If their A1c is 10%, do we care? Is the HDL doing anything? At what point are we assured?
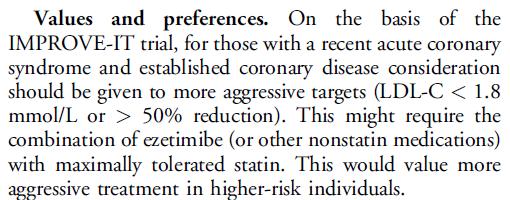
101 Summary and conclusions Statins lower CV risk in essentially all diabetics. The use of statins should be guided by perceived CV risk, as per guidelines (which guidelines???) Lifetime risk should also be considered Correct LDL first In people in whom you cannot decide, measuring an apob, non-hdl might provide further information
102 Summary and conclusions: cont d The addition of Ezetemibe to statin with subsequent lowering of LDL does lower risk more (at least in diabetics) Targets are changing (at least in the US) in view of IMPROVE-IT and FOURIER PCSK9 inhibitors..
103 104
104 105
105 106
106
107
108
109 With respect to (LDL) cholesterol. Should we be checking LDL (or other lipid fractions)? What is the normal range? Is there an upper limit to the range? Is there a lower limit to the range? What are the targets in people with diabetes? What should the targets be? Is the cholesterol hypothesis proven? Hypothesis or fact?
110 Learning objectives: Review the importance of statins to lower CV risk in diabetes To review lipid guidelines (Canadian and American) as they pertain to diabetes Is lower better (at least for diabetes)? To review results with Ezetemibe and PCSK9 inhibitors Are studies with these drugs going to impact guidelines? Does glycemic control matter wrt lipids/targets? To review where triglyceride management might fit in Is statin intolerance real? Does it matter? Do statins cause diabetes? Does it matter? Small interfering RNA Etc..
111 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.22 mmol/l (163 mg/dl) HDL:.99 mmol/l (38 mg/dl) LDL: 1.42mmol/L (55 mg/dl) Triglyceride: 3.98 mmol/l (349 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
112 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.22 mmol/l (163 mg/dl) HDL:.99 mmol/l (38 mg/dl) LDL: 1.42mmol/L (54 mg/dl) Triglyceride: 3.98 mmol/l (349 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
113 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.22 mmol/l (163 mg/dl) HDL:.99 mmol/l (38 mg/dl) LDL: 1.42mmol/L (54 mg/dl) Triglyceride: 3.98 mmol/l (349 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
114 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.22 mmol/l (163 mg/dl) HDL:.99 mmol/l (38 mg/dl) LDL: 1.42mmol/L (54 mg/dl) Triglyceride: 3.98 mmol/l (349 mg/dl) A1c: 6.9% Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
115 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 10 mg TC: 4.22 mmol/l (163 mg/dl) HDL:.99 mmol/l (38 mg/dl) LDL: 1.42mmol/L (54 mg/dl) Triglyceride: 3.98 mmol/l (349 mg/dl) apob:.94 Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
116 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg TC: 3.52 mmol/l (136 mg/dl) HDL:.89 mmol/l (34 mg/dl) LDL: 1.07 mmol/l (41 mg/dl) Triglyceride: 3.5 mmol/l (310 mg/dl) apob.79 Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
117 Mr. M. S., age 58, diabetic Meds include Metformin 1 gm bid, Ramipril 10 mg, Metoprolol 50 mg bid and Atorvastatin 80 mg TC: 3.52 mmol/l (136 mg/dl) HDL:.89 mmol/l (34 mg/dl) LDL: 1.07 mmol/l (41 mg/dl) Triglyceride: 3.5 mmol/l (310 mg/dl) apob.79 Are his lipids optimally controlled? Should you add more statin? Should you add a fibrate?
118 119
119 BIP: Effects of baseline Triglycerides on response to treatment Circulation, 2000;102:21-27
 HDL-C 42 (1.1) 42 (1.1) TG 153 (1.73) 154 (1.74) Dyslipidemic*, % 37 39 *TG >150 (1.7) and HDL <40 mg/dl (1.03) for men or <50 mg/dl (1.29) for women The FIELD Study Investigators.")
120 Baseline Characteristics Characteristic Placebo (n = 4900) Fenofibrate (n = 4895) Male, % No Prior CVD, % Lipid parameters, mg/dl (mmol/l) TC LDL-C 119 (3.07) 119 (3.07) HDL-C 42 (1.1) 42 (1.1) TG 153 (1.73) 154 (1.74) Dyslipidemic*, % *TG >150 (1.7) and HDL <40 mg/dl (1.03) for men or <50 mg/dl (1.29) for women The FIELD Study Investigators. Lancet [Early Online Publication]. November 14, 2005.
121
122


123

124
125
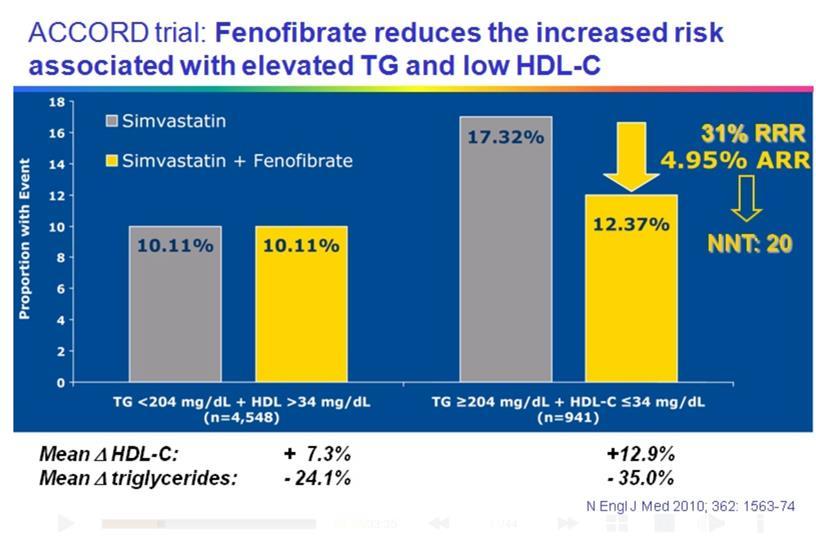
126 127
127
128
129 130

130 131
131 132
132 133
133 Lipid Goals for Individuals at Risk for ASCVD Lipid parameter Goal (mg/dl) TC <200 LDL-C Non HDL-C TG <150 Apo B <130 (low risk) <100 (moderate risk) <100 (high risk) <70 (very high risk) <55 (extreme risk) 30 above LDL-C goal; 25 above LDL-C goal (extreme risk individuals) <90 (individuals at high risk of ASCVD, including those with diabetes) <80 (individuals at very high risk with established ASCVD or diabetes plus 1 additional risk factor) <70 (individuals at extreme risk) Abbreviations: apo, apolipoprotein; ASCVD, atherosclerotic cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides. AACE/ACE 2017;epub ahead of print; Baigent C, et al. Lancet. 2010;376: ; Boekholdt SM, et al. J Am Coll Cardiol. 2014;64(5): ; Brunzell JD, et al. Diabetes Care. 2008;31: ; Cannon CP, et al. N Engl J Med. 2015;372(25): ; Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22; Jellinger P, Handelsman Y, Rosenblit P, et al. Endocr Practice. 2017;23(4): ; Ridker PM, J Am Coll Cardiol. 2005;45: ; Sever PS, et al. Lancet. 2003;361: ; Shepherd J, et al. Lancet. 2002;360: ; Weiner DE, et al. J Am Soc Nephrol. 2004;15(5):
134 Recommendations associated with this question: Question: How are different drugs used to treat dyslipidemia? Statins, Fibrates R55. In individuals at risk for ASCVD, aggressive lipid-modifying therapy is recommended to achieve appropriate LDL-C goals (Grade A, BEL 1). Statins R56. Statin therapy is recommended as the primary pharmacologic agent to achieve target LDL-C goals on the basis of morbidity and mortality outcome trials (Grade A; BEL 1). R57. For clinical decision making, mild elevations in blood glucose levels and/or an increased risk of newonset T2DM associated with intensive statin therapy do not outweigh the benefits of statin therapy for ASCVD risk reduction (Grade A, BEL 1). R58. In individuals within high-risk and very high-risk categories, further lowering of LDL-C beyond established targets with statins results in additional ASCVD event reduction and may be considered (Grade A, BEL 1). R59. Very high-risk individuals with established coronary, carotid, and peripheral vascular disease, or diabetes, who also have at least 1 additional risk factor, should be treated with statins to target a reduced LDL-C treatment goal of <70 mg/dl (Grade A, BEL 1). R60. Extreme risk individuals should be treated with statins or with combination therapy to target an even lower LDL-C treatment goal of <55 mg/dl (Grade A, BEL 1). Fibrates R61. Fibrates should be used to treat severe hypertriglyceridemia (TG >500 mg/dl) (Grade A; BEL 1). R62. Fibrates may improve ASCVD outcomes in primary and secondary prevention when TG concentrations are 200 mg/dl and HDL-C concentrations <40 mg/dl (Grade A; BEL 1). Abbreviations: ASCVD, atherosclerotic cardiovascular disease; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides. Jellinger P, Handelsman Y, Rosenblit P, et al. Endocr Practice. 2017;23(4):
135 136
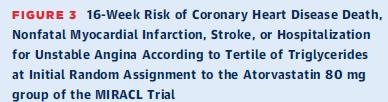
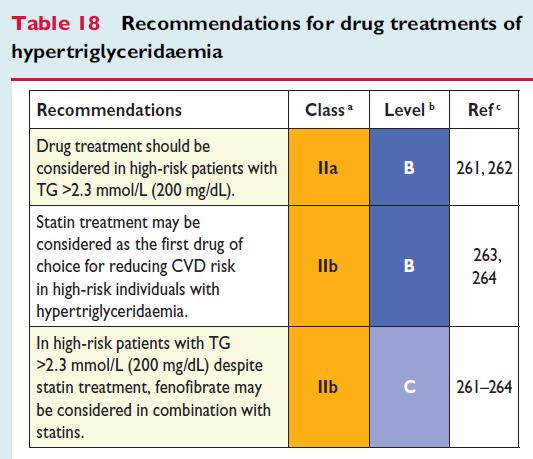
136 Summary and conclusions: cont d Most guidelines around the world are coming around to the same conclusion, i.e., that in the presence of atherogenic dyslipidemia, there is reasonable evidence that fibrates decrease CV risk (Gemfibrozil should not be used with a statin)
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine
 Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
Hyperlipidemia Guidelines: What s New in 2015? Eva Lonn, MD, MSc Professor of Medicine The new england journal of medicine Original Article Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Glucose and CV disease
 Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Glucose and CV disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic,
Triglyceride as Vascular Risk Factor
 Curriculum Vitae Name : Prof. Dr. dr. Idrus Alwi SpPD, KKV, FINASIM, FACP, FACC, FESC, FAPSIC Current Position : - President of the Indonesian Society of Internal Medicine Medical Student : Faculty of
Curriculum Vitae Name : Prof. Dr. dr. Idrus Alwi SpPD, KKV, FINASIM, FACP, FACC, FESC, FAPSIC Current Position : - President of the Indonesian Society of Internal Medicine Medical Student : Faculty of
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Glucose Control: Does it lower CV risk?
 Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Glucose Control: Does it lower CV risk? Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
PCSK9 Inhibitors and Modulators
 PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
PCSK9 Inhibitors and Modulators Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Disclosures Speaker s
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Educational Objectives. Disease Trajectories and CVD Risk Reduction. Hypercholesterolemia Support for LDL-C Causality
 Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Educational Objectives At the conclusion of this activity, participants should be able to: Evaluate the extent of residual CVD risk to which ASCVD patients are exposed, and treat additional CVD risk elements
Disclosures. Speakers Bureau Novo Nordisk, Astra Zeneca, Amgen, Boehringer Ingelheim, Merck, Janssen
 Interpreting Lipid Guidelines: How Low Should You Go? Paul S. Jellinger, MD, MACE Chair, 2017 AACE/ACE Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Professor of Clinical
Interpreting Lipid Guidelines: How Low Should You Go? Paul S. Jellinger, MD, MACE Chair, 2017 AACE/ACE Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Professor of Clinical
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
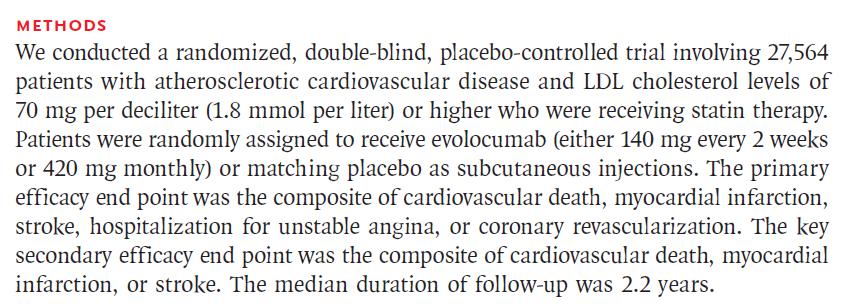
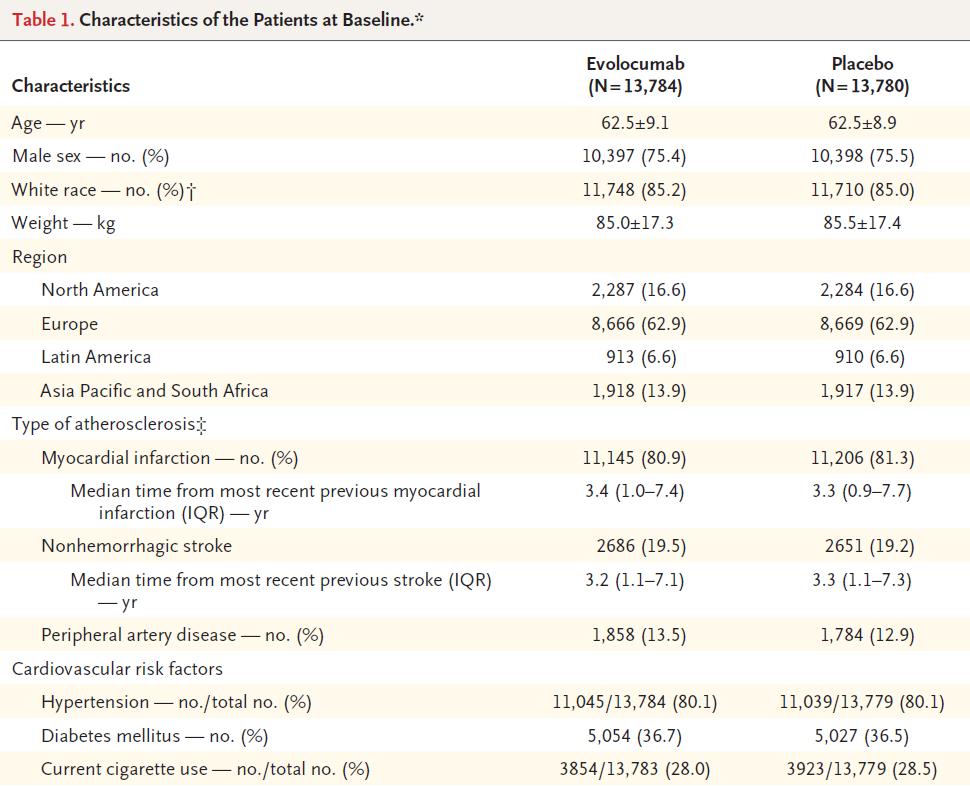
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial
 Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
Clinical Efficacy and Safety of Achieving Very Low LDL-C Levels With the PCSK9 Inhibitor Evolocumab in the FOURIER Outcomes Trial RP Giugliano, TR Pedersen, AC Keech, PS Sever, JG Park, and MS Sabatine,
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy
 PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
PCSK9 Inhibitors: Narnia vs. Medicare Bankruptcy Sergio Fazio, MD, PhD William and Sonja Connor Professor of Preventive Cardiology Professor of Medicine, Physiology & Pharmacology Director, Center for
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease
 American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul
American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Statins and PCSK9 inhibitors for stroke prevention
 Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Statins and PCSK9 inhibitors for stroke prevention Haralampos Milionis Professor of Internal Medicine School of Medicine, University of Ioannina Ioannina, Greece Reduction in CV events (%) Every 1 mmol/l
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors
 Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Best Practices Lipid Control Today: Management within the Context of other Cardiovascular Risk Factors James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA, FASPC Lipidology & Cardiovascular Disease Prevention
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Cholesterol Medicines New & Old: What to Use When
 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia. Prof. Alberto Corsini University of Milan, Italy
 Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP
 Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
Update on Lipid Guidelines and Intense Treatment of LDL-C with PCSK9 Inhibitors Carl J. Lavie, MD,FACC,FACP,FCCP Professor of Medicine Medical-Director, Preventive Cardiology John Ochsner Heart and Vascular
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Macrovascular Management. What s next beyond standard treatment?
 Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Macrovascular Management What s next beyond standard treatment? Are Lifestyle Modifications Still Relevant in Diabetic Patients? Diet Omega-6 and omega-3 fatty acids have been shown to improve CVD risk
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Copyright 2017 by Sea Courses Inc.
 Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
Pre-Diabetes: Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or mechanical,
THE CRUCIAL PROBLEM OF ASCVD Can New Therapeutic Options Resolve It? THE CRUCIAL PROBLEM OF ASCVD Can New Therapeutic Options Resolve It?
 James A. Underberg, MD, MS, FACPM, FACP, FNYAM, FASPC, FNLA Lipidology and Cardiovascular Disease Prevention Clinical Assistant Professor of Medicine NYU Medical School and NYU Center for CV Prevention
James A. Underberg, MD, MS, FACPM, FACP, FNYAM, FASPC, FNLA Lipidology and Cardiovascular Disease Prevention Clinical Assistant Professor of Medicine NYU Medical School and NYU Center for CV Prevention
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
PCSK9 Agents Drug Class Prior Authorization Protocol
 PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
PCSK9 Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P & T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of medical
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2062-8 Program Prior Authorization/Medical Necessity Medication Praluent (alirocumab) P&T Approval Date 5/2015, 8/2015, 9/2015,
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Robyn Cruz, PharmD, BCPS, BCPP 1
 Robyn Cruz, PharmD, BCPS, BCPP ISHP Spring Meeting April 2014 Identify major changes in treating hyperlipidemia according to the 2013 ACC/AHA Blood Cholesterol Guidelines Discuss clinical trial data that
Robyn Cruz, PharmD, BCPS, BCPP ISHP Spring Meeting April 2014 Identify major changes in treating hyperlipidemia according to the 2013 ACC/AHA Blood Cholesterol Guidelines Discuss clinical trial data that
The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C
 The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine
The Atherogenic Dyslipidemia of Diabetes Mellitus- Not just a question of LDL-C Eun-Jung Rhee Department of Endocrinology and Metabolism Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo?
 Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane
 Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
New Horizons in Dyslipidemia Management in Primary Care
 New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
New Horizons in Dyslipidemia Management in Primary Care Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Hyperlipidemia: Past and Present. Rebecca Khaimova, PharmD The Brooklyn Hospital Center
 Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2017 P 2063-8 Program Prior Authorization/Medical Necessity Medication Repatha (evolocumab) P&T Approval Date 5/2015, 9/2015, 11/2015,
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO