Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
|
|
|
- Alfred Andrews
- 6 years ago
- Views:
Transcription

1 Kerry Cooper M.D. Arizona Kidney Disease and Hypertension Center April 30, 2009
2
3 DR. KERRY COOPER IS ON THE SPEAKER BUREAU OF AMGEN, ABBOTT, GENZYME, SHIRE, AND BMS DR. COOPER IS ALSO INVOLVED IN CLINICAL TRIALS SPONSORED BY AMGEN, ABBOTT, GENZYME, AND SHIRE

4 Review the differential diagnosis of proteinuric syndromes Review the pathology of primary and secondary glomerular disorders Review diagnostic tools for evaluation of proteinuria Review treatment options for proteinuric syndromes
5
6
7
8

9
10
11

12
13 Albuminuria Timed Collection (µg/min) Spot Collection (µg/mg Cr) 24-Hour Collection (mg/24 hr) Normo- <20 <30 <30 Micro Macro
14
15 Heavy proteinuria ( 3 gm/24 hrs) Hypoalbuminemia Edema formation Hypercholesterolemia
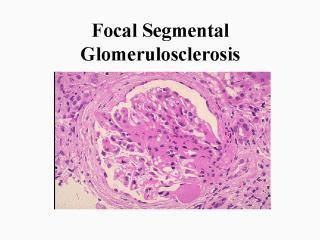
16 Minimal change disease Focal segmental glomerulosclerosis Membranous nephropathy Mesangiocapillary glomerulonephritis
17 Infectious diseases Post-streptococcal GN Hepatitis B/Hepatitis C HIV Parasitic infections Autoimmune diseases Systemic lupus Wegener s granulomatosis Malignancy Solid tumors/membranous nephropathy Lymphoproliferative disorders/minimal change disease Drug induced Non-steroidal agents Gold/penicillamine
18 Fever Congestive heart failure Dehydration
19
20 Anti-nuclear antibody Complement levels Serum/urine immunoelectropheresis Hepatitis B/C serologies HIV status Anti-neutrophil cytoplasmic antibody Renal biopsy
21 Anasarca Systemic infection Hypercoagulability Deep venous thrombosis Renal vein thrombosis
22 Dyslipidemia Male Sex Hypertension Hyperinsulinemia Microalbuminuria Age> 60 years Relative Risk of Coronary Artery Disease Tuttle KR et al. Am J Kidney Dis. 1999;34:
23 Hypertension Age (men, >55 yr; women, >65 yr) Diabetes mellitus Dyslipidemia Microalbuminuria or estimated GFR <60 ml/min Family history of premature CVD (men, <55 yr; women, <65 yr) Obesity (BMI 30 kg/m 2 ) Physical inactivity Cigarette smoking
24
25

26
27
28

29
30
31
32
33
34
35
36

37
38
39
40 Diuretics/sodium restriction ACE I, ARB Glucocorticoids Immunosuppressive agents Chlorambucil Cyclophosphamide Calcineurin inhibitors Mycophenalate mofetil

41
42
43
44 Microalbuminuria Proteinuria CV Events Death Doubling of Serum Creatinine Levels End-Stage Renal Disease


45 MC GFR CL Autoregulation through feedback mechanisms normally keeps GFR and renal blood flow constant 1 EC EA EA Resistance Angiotensin II Renin JA AA Angiotensin II plays a key role in autoregulation through increasing efferent arteriolar pressure 1 Prolonged inappropriate increase in angiotensin II leads to decreased GFR and renal blood flow as well as release of various cytokines and growth factors 1,2
46 Progression to Death, Dialysis, or Transplant (%) 40 Placebo 30 Captopril
 could be added to all groups to help achieve target BP levels.")
47 Patients (%) Control (n=201)* Irbesartan 150 mg/d (n=195)* Irbesartan 300 mg/d (n=194)* RRR=39% P= RRR=70% P< Follow-up (mo) RRR, relative risk reduction. Control defined as placebo. * Adjunctive antihypertensive therapies (excluding ACE inhibitors, ARBs, and dihydropyridine CCBs) could be added to all groups to help achieve target BP levels. Adapted from Parving H-H et al. N Engl J Med. 2001;345:
48 Patients (%) P= Control (n=201) 150 mg/d (n=195) 300 mg/d (n=194) Irbesartan
49 Irbesartan (n=579) RRR=23% P=.006 Amlodipine (n=567) RRR=20% P=.02 P=NS Control (n=569) Follow-up (mo) Control defined as placebo. SeCr, serum creatinine; ESRD, end-stage renal disease; RRR, relative risk reduction. Adapted from Lewis EJ et al. N Engl J Med. 2001;345:
50 Change in UPE (%) 3 Months Years 1, Control -1% Amlodipine 10 mg/d -4% Irbesartan 300 mg/d Control -10% Amlodipine 10 mg/d -6% Irbesartan 300 mg/d % -35 P=NS P<.001 P<.001 Control defined as placebo. UPE, urinary protein excretion (g/24h). 1. Data on file, Bristol-Myers Squibb Company. 2. Lewis EJ et al. N Engl J Med. 2001;345: P=NS P<.001 P< %
51 Reduction From Baseline (%) 0 Fosinopril 20 mg/d After 6 Weeks of Therapy Irbesartan 150 mg/d Irbesartan 150 mg/d + Fosinopril 20 mg/d P=.039
52 Change in AER (%) Change in AER (%) 0 Hypertensive (n=64) Placebo Irbesartan 0 Normotensive (n=60) Placebo Irbesartan Reduction in SBP/DBP (mm Hg) Baseline: 160/96 mm Hg Baseline: 126.5/81.5 mm Hg Placebo Irbesartan Placebo Irbesartan -1.5/ / -6.5 Reduction in SBP/DBP -3/ / -1 (mm Hg)
53
54
RENAAL, IRMA-2 and IDNT. Three featured trials linking a disease spectrum IDNT RENAAL. Death IRMA 2
 Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
Treatment of Diabetic Nephropathy and Proteinuria Background End stage renal disease is a major cause of death and disability among diabetics BP reduction is important to slow the progression of diabetic
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
Diabetic Nephropathy 2009
 Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Diabetic Nephropathy 2009 Michael T McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetic Nephropathy Clinical Stages Hyperfunction
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
The CARI Guidelines Caring for Australians with Renal Impairment. Specific effects of calcium channel blockers in diabetic nephropathy GUIDELINES
 Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Specific effects of calcium channel blockers in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Non-dihydropyridine calcium channel
Nephrotic Syndrome NS
 Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Nephrotic Syndrome NS By : Dr. Iman.M. Mudawi Pediatric Nephrology Unit Gaafar Ibn Auf Hospital Definitions: In children NS is applied to any condition with a triad of: Heavy proteinuria (UACR ratio >200
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers. Robert D. Toto, MD
 R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
R e v i e w P a p e r Management of Hypertensive Chronic Kidney Disease: Role of Calcium Channel Blockers Robert D. Toto, MD Both the prevalence and incidence of end-stage renal disease have been increasing
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Renal Protection Staying on Target
 Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Update Staying on Target James Barton, MD, FRCPC As presented at the University of Saskatchewan's Management of Diabetes & Its Complications (May 2004) Gwen s case Gwen, 49, asks you to take on her primary
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s. Part 1: Clinical
 Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Focal Segmental Glomerulosclerosis and the Nephro6c Syndrome Dr. A. Gangji Dr. P. Marge>s Part 1: Clinical Pa#ent DM 18 year old McMaster student Back pain, severe fa#gue Oct 2006 Leg swelling to ER Nov
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Nephrotic syndrome in children. Bashir Admani KPA Nephrology Precongress 24/4/2018
 Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
Nephrotic syndrome in children Bashir Admani KPA Nephrology Precongress 24/4/2018 What is Nephrotic syndrome?? Nephrotic syndrome is caused by renal diseases that increase the permeability across the glomerular
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Diabetes is the most common cause of end-stage renal
 Pharmacoeconomic Challenges in the Management of Diabetic Nephropathy ROGER A. RODBY, MD ABSTRACT BACKGROUND: Diabetes is the most common cause of end-stage renal disease (ESRD) kidney failure to the point
Pharmacoeconomic Challenges in the Management of Diabetic Nephropathy ROGER A. RODBY, MD ABSTRACT BACKGROUND: Diabetes is the most common cause of end-stage renal disease (ESRD) kidney failure to the point
The CARI Guidelines Caring for Australasians with Renal Impairment. ACE Inhibitor and Angiotensin II Antagonist Combination Treatment GUIDELINES
 ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
ACE Inhibitor and Angiotensin II Antagonist Combination Treatment Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES No recommendations possible based on Level
Update on HIV-Related Kidney Diseases. Agenda
 Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Update on HIV-Related Kidney Diseases ANDY CHOI THE MEDICAL MANAGEMENT OF HIV/AIDS DECEMBER 15, 2006 Agenda 1. EPIDEMIOLOGY: A) END STAGE RENAL DISEASE (ESRD) B) CHRONIC KIDNEY DISEASE (CKD) 2. HIV-ASSOCIATED
Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009
 www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers PROTEINURIA
www.ivis.org Proceedings of the 34th World Small Animal Veterinary Congress WSAVA 2009 São Paulo, Brazil - 2009 Next WSAVA Congress : Reprinted in IVIS with the permission of the Congress Organizers PROTEINURIA
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Proteinuria. Louisiana State University
 Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Proteinuria W S A V A W C P, 2005 David F. Senior Louisiana State University The normal glomerulus is a highly selective barrier for filtration based on size (and on charge in the case of larger molecules).
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
The CARI Guidelines Caring for Australasians with Renal Impairment. Protein Restriction to prevent the progression of diabetic nephropathy GUIDELINES
 Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Protein Restriction to prevent the progression of diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. A small volume of evidence suggests
Chronic kidney disease-what can you do and when to refer?
 Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE
 Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Nephrotic syndrome Dr.Basma Adel FIFTH GRADE 2017-2018 At the end of this lecture you should know: Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. 12/3/2017
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Proteinuria DR. SANJAY PANDEYA MD. FRCPC.
 Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Proteinuria DR. SANJAY PANDEYA MD. FRCPC. Objectives Define normal and abnormal range(s) of proteinuria Evaluation of proteinuria Be aware of complications of proteinuria When to refer and when not to
Comparison between the efficacy of double blockade and single blockade of RAAS in diabetic kidney disease
 International Journal of Advances in Medicine Gupta A et al. Int J Adv Med. 2018 Aug;5(4):931-935 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20183122
International Journal of Advances in Medicine Gupta A et al. Int J Adv Med. 2018 Aug;5(4):931-935 http://www.ijmedicine.com pissn 2349-3925 eissn 2349-3933 Original Research Article DOI: http://dx.doi.org/10.18203/2349-3933.ijam20183122
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence?
 Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
Reviews ACE Inhibitors and Protection Against Kidney Disease Progression in Patients With Type 2 Diabetes: What s the Evidence? George L. Bakris, MD; 1 and Matthew Weir, MD 2 Although angiotensin-converting
ACEIs / ARBs NDHP dihydropyridine ( DHP ) ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )
 ACEIs ARBs ACEIs ARBs NDHP. ( GFR ) 60 ml/min/1.73m ( chronic kidney disease, CKD )") 005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
005 16 175-180 1 1 ( chronic kidney disease, CKD ) 003 ( end-stage renal disease, ESRD ) Angiotensin-converting enzyme inhibitors ( ) angiotensin receptor blockers ( ) nondihydropyridine ( NDHP ) / NDHP
Diabetic Nephropathy
 Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
Diabetic Nephropathy Outline Introduction of diabetic nephropathy Manifestations of diabetic nephropathy Staging of diabetic nephropathy Microalbuminuria Diagnosis of diabetic nephropathy Treatment of
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009
 The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
The Diabetes Kidney Disease Connection Missouri Foundation for Health February 26, 2009 Teresa Northcutt, RN BSN Primaris Program Manager, Prevention - CKD MO-09-01-CKD This material was prepared by Primaris,
ACP Brief Fall 2006 prioritization. Angiotensin II Receptor Blockers (ARBs) for Proteinuria, Hypertension (HTN) and Congestive Heart Failure (CHF)
 for Proteinuria, Hypertension (HTN) and Congestive Heart Failure (CHF)") ACP Brief Fall 2006 prioritization Angiotensin II Receptor Blockers (ARBs) for Proteinuria, Hypertension (HTN) and Congestive Heart Failure (CHF) Background This topic was submitted by BC PharmaCare during
ACP Brief Fall 2006 prioritization Angiotensin II Receptor Blockers (ARBs) for Proteinuria, Hypertension (HTN) and Congestive Heart Failure (CHF) Background This topic was submitted by BC PharmaCare during
Diabetes and Kidney Disease. Kris Bentley Renal Nurse practitioner 2018
 Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
Diabetes and Kidney Disease Kris Bentley Renal Nurse practitioner 2018 Aims Develop an understanding of Chronic Kidney Disease Understand how diabetes impacts on your kidneys Be able to recognise the risk
University of Groningen. Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste
 University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
University of Groningen Evaluation of renal end points in nephrology trials Weldegiorgis, Misghina Tekeste IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol
 Josep M. Campistol") Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Considering the early proactive switch from a CNI to an mtor-inhibitor (Case: Male, age 34) Josep M. Campistol Patient details Name DOB ESRD Other history Mr. B.I.B. 12 January 1975 (34yo) Membranous GN
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
E.Ritz Heidelberg (Germany)
") Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
Predictive capacity of renal function in cardiovascular disease E.Ritz Heidelberg (Germany) If a cure is not achieved, the kidneys will pass on the disease to the heart Huang Ti Nei Ching Su Wen The Yellow
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications.
 Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
Types Pathophysiology Clinical manifestations D.Dx. Investigations. Treatment. Complications. Nephrotic syndrome affects 1-3 per 100,000 children
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
The CARI Guidelines Caring for Australasians with Renal Impairment. Antihypertensive therapy in diabetic nephropathy GUIDELINES
 Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Antihypertensive therapy in diabetic nephropathy Date written: September 2004 Final submission: September 2005 Author: Kathy Nicholls GUIDELINES a. Adequate control of blood pressure (BP) slows progression
Hasan Fattah 3/19/2013
 Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Hypertension is a major risk factor for
 OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
OPTIMAL RISK MANAGEMENT OF THE HYPERTENSIVE PATIENT WITH MULTIPLE RISK FACTORS * Keith C. Ferdinand, MD, FACC ABSTRACT To determine the risk of cardiovascular disease in patients with hypertension, it
Evaluation and Management of Proteinuria. Negiin Pourafshar, MD University of Virginia Division of Nephrology
 Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Evaluation and Management of Proteinuria Negiin Pourafshar, MD University of Virginia Division of Nephrology Case A 30-year-old man, is turned down for life insurance because of the presence of an unspecified
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
신장환자의혈압조절 나기영. Factors involved in the regulation of blood pressure
 신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
신장환자의혈압조절 K/DOQI Clinical practice guidelines on Hypertension and Antihypertensive agents in CKD 나기영 Factors involved in the regulation of blood pressure Renal function curve MAP (mmhg) Central role of
The Heart and the Kidney
 1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
1 3 6 The Heart and the Kidney Martin R. Cowie The Epidemiologic Association Between the Kidney and the Heart............................... 2819 The Burden of Chronic Kidney Disease............ 2820 The
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Caring for Australians with Renal Impairment. BP lowering and CVD
 Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Caring for Australians with Renal Impairment BP lowering and CVD Questions: Conflicts of Interest: RH, TN, HHL- no conflict VP- level II conflict Speakers fees: Abbott, Astra Zeneca, Roche, Servier Grant
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care
: Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care") Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #119 (NQF 0062): Diabetes: Medical Attention for Nephropathy National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS F INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Special Challenges and Co-Morbidities
 Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Special Challenges and Co-Morbidities Renal Disease/ Hypertension/ Diabetes in African-Americans M. Keith Rawlings, MD Medical Director Peabody Health Center AIDS Arms, Inc Dallas, TX Chair, Internal Medicine
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Management of early chronic kidney disease
 Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
Management of early chronic kidney disease GREENLANE SUMMER GP SYMPOSIUM 2018 Jonathan Hsiao Renal and General Physician Introduction A growing public health problem in NZ and throughout the world. Unknown
RATIONALE. chapter 4 & 2012 KDIGO
 http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
http://www.kidney-international.org chapter 4 & 2012 KDIGO Chapter 4: Blood pressure management in CKD ND patients with diabetes mellitus Kidney International Supplements (2012) 2, 363 369; doi:10.1038/kisup.2012.54
The real picture. Prorenin (Renin) PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009
 PRR AT3 AT4. AT4 receptor. PAI 1 Abassi, Biochem Pharm, 2009") The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
The real picture. Prorenin (Renin) PRR AT3-8 AT4 AT10-12 AT3 AT4 receptor PAI 1 Abassi, Biochem Pharm, 2009 Resistant Hypertension; Case based discussion Moving Targets? RAAS blockade in hypertensive CKD
CLINICIAN INTERVIEW A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY. Interview with Ralph Rabkin, MD
 A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
A REVIEW OF THE CURRENT TREATMENT MODALITIES FOR DIABETIC NEPHROPATHY Interview with Ralph Rabkin, MD Dr Rabkin is Professor of Medicine, Emeritus, Active, at Stanford University School of Medicine, Stanford,
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
ALLHAT RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR)
") 1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
1 RENAL DISEASE OUTCOMES IN HYPERTENSIVE PATIENTS STRATIFIED INTO 4 GROUPS BY BASELINE GLOMERULAR FILTRATION RATE (GFR) 6 / 5 / 1006-1 2 Introduction Hypertension is the second most common cause of end-stage
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been