FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
|
|
|
- Charleen Martin
- 6 years ago
- Views:
Transcription

1 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport
2
3 Fibrils in bundles nm d Diabetic fibrillosis

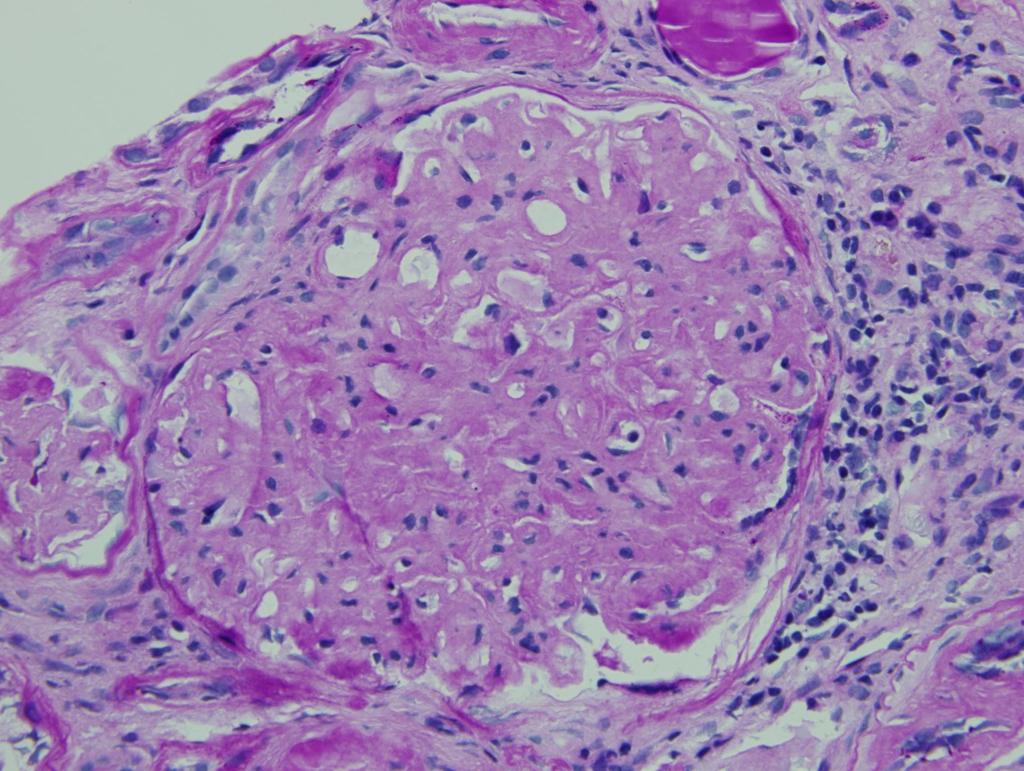
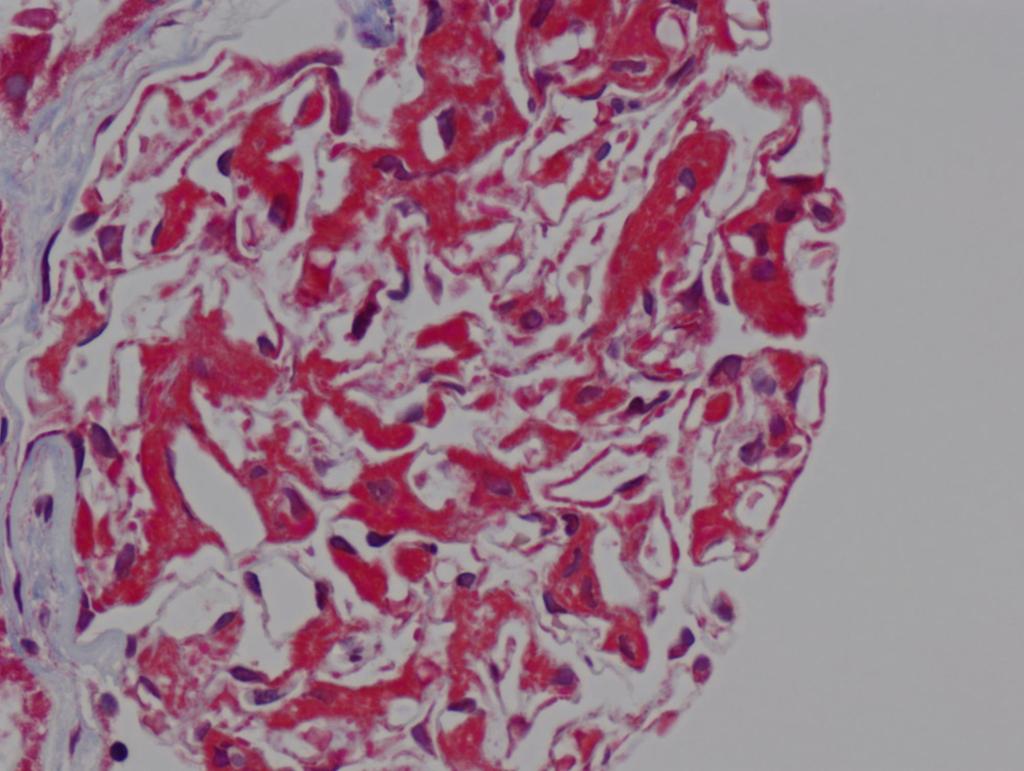
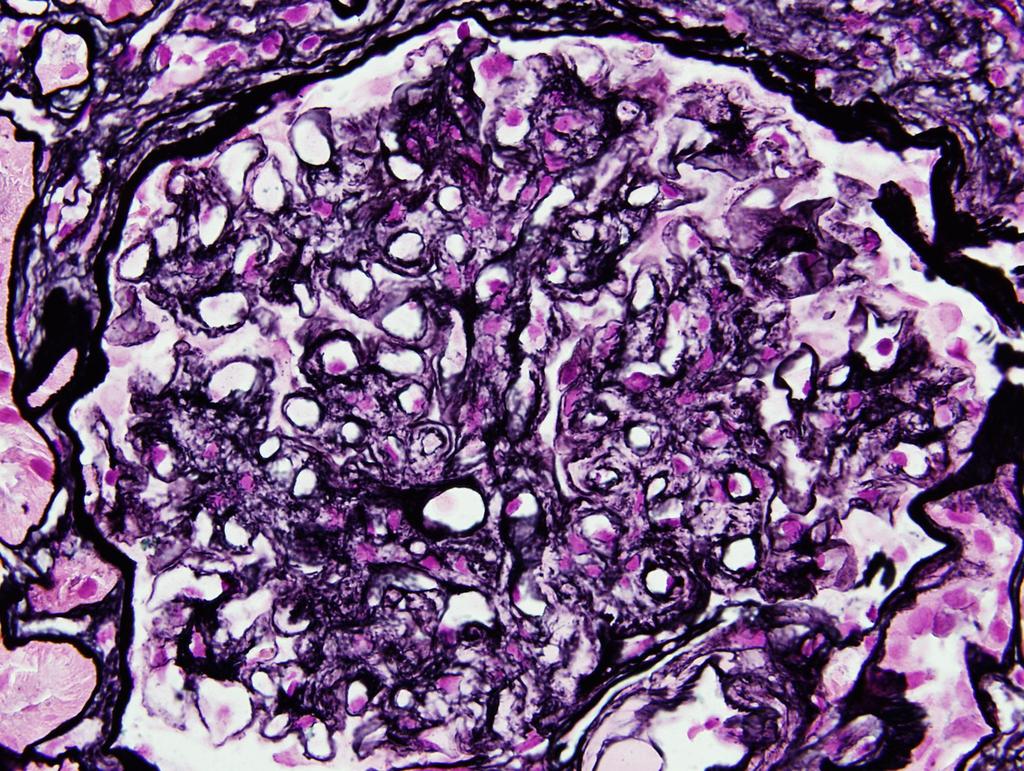
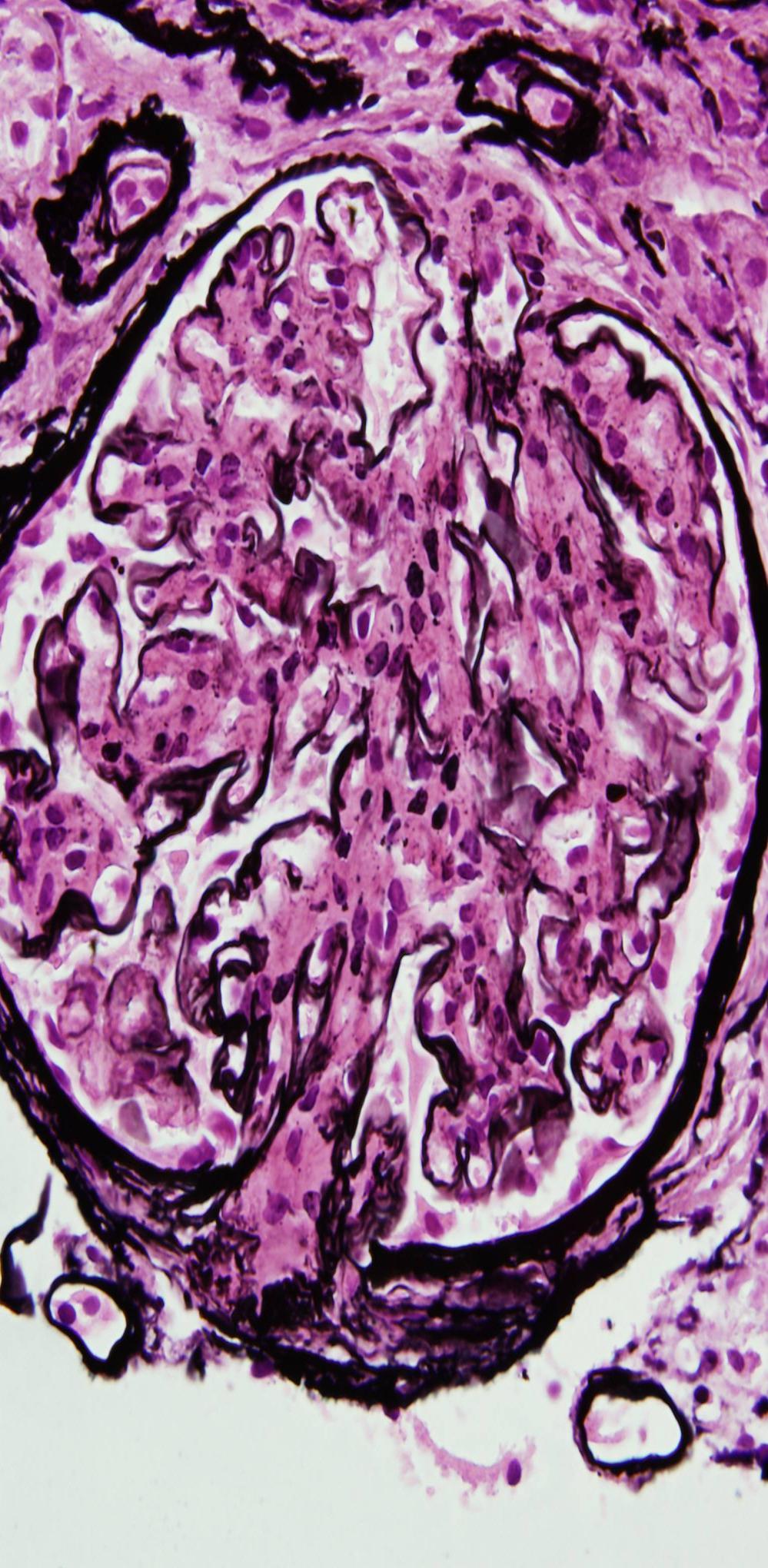
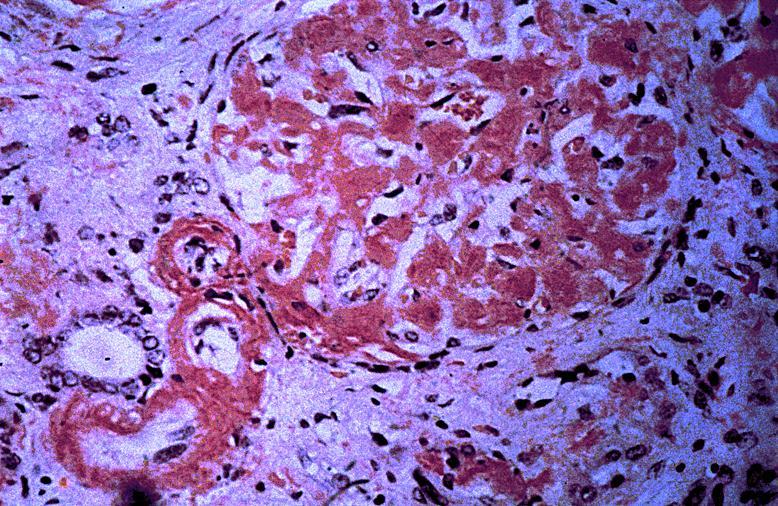
4 SILVER METHENAMINE STAIN
5
6 SEEN IN A CHILD 10 Y/O PROTEINURIA IS OFTEN SEVERE / 70% WITH HYPERTENSION ROUGHLY HALF OF THE PATIENTS TO ESRD WITHIN 2 YEARS AFTER DIAGNOSIS





7 CLINICAL INFORMATION Mean age at diagnosis= 53 years Majority 95% caucasian patients Female to male ratio 1.2:1 PRESENTATION: PROTEINURIA- 100% (maybe massive), NEPHROTIC SYNDROME- 38%, RENAL INSUFFICIENCY- 66%, HEMATURIA- 52%, AND HYPERTENSION- 71% / few cases rapidly progressive renal disease Underlying diseases- malignancies- MOST COMMON CARCINOMA 23%, dysproteinemia- 17% and autoimmune diseases 15% of all patients in series Nasr, et al: Fibrillary glomerulonephritis: A report of 66 cases from a single institution. Clin J Am Soc Nephrol 6: , 2011
8


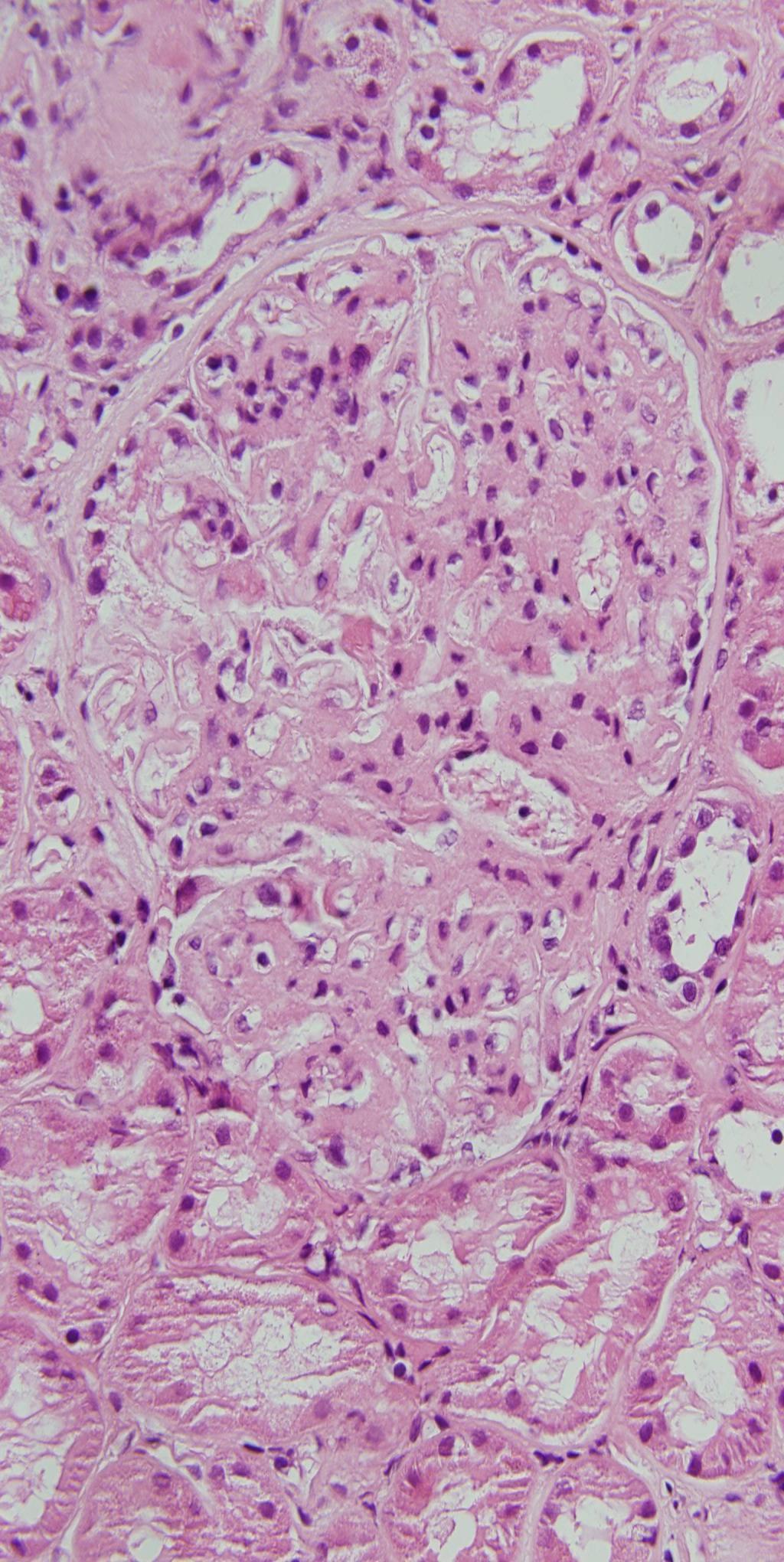
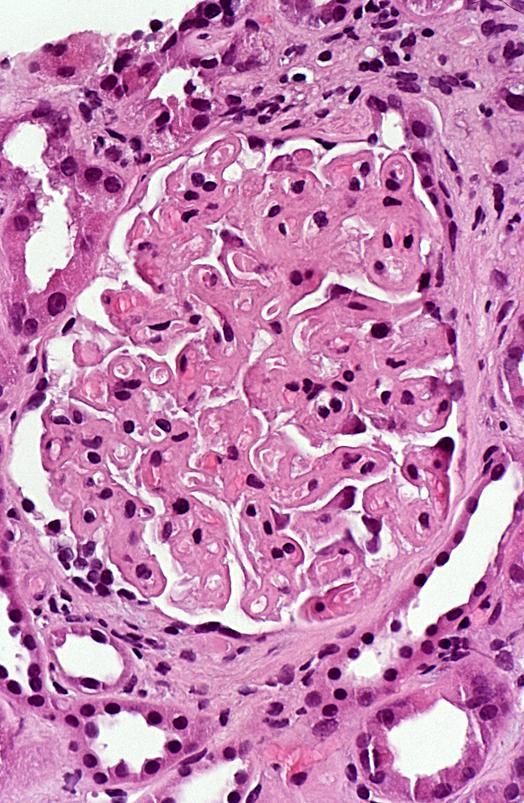
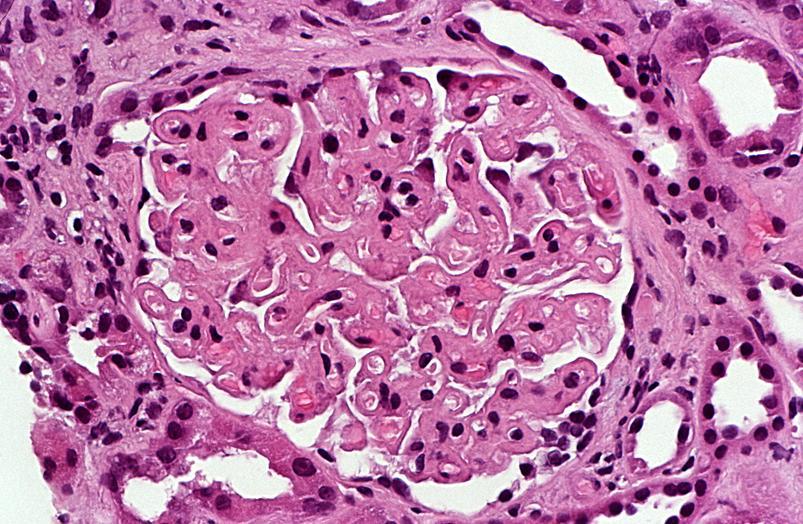
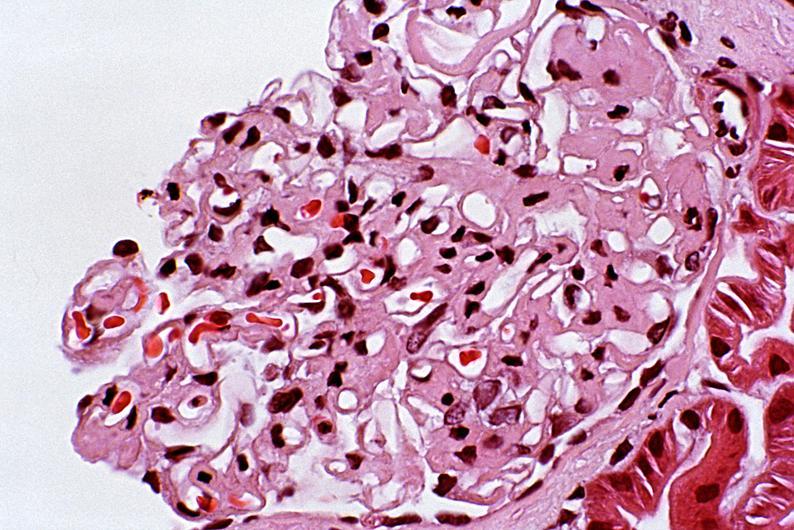
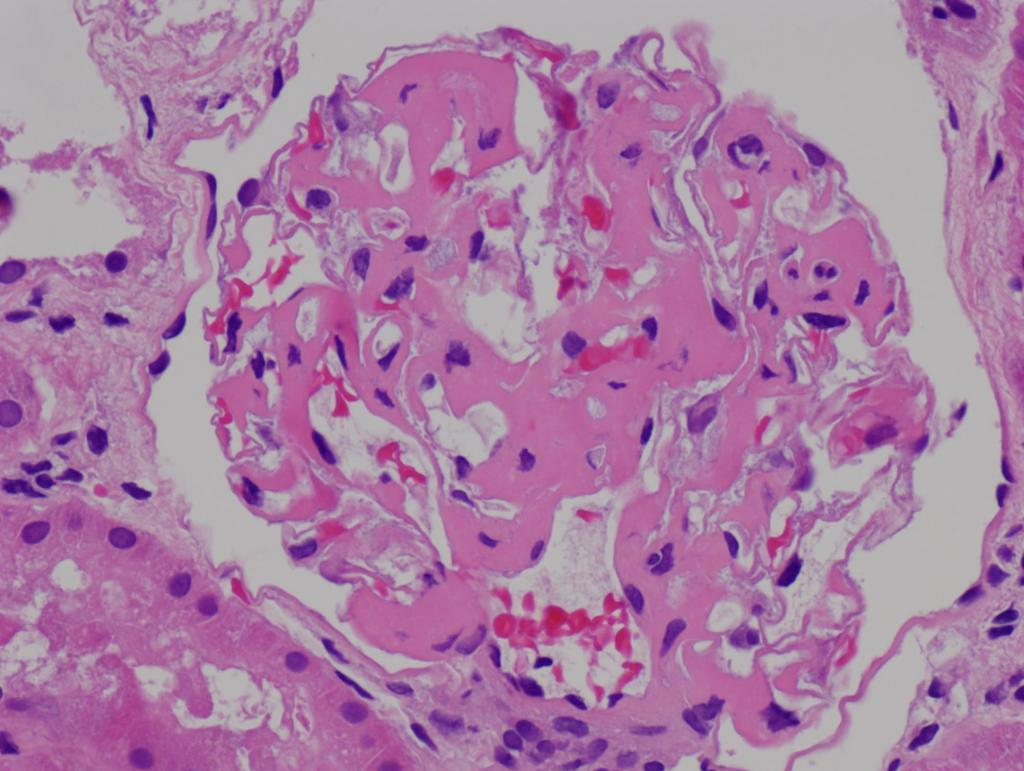
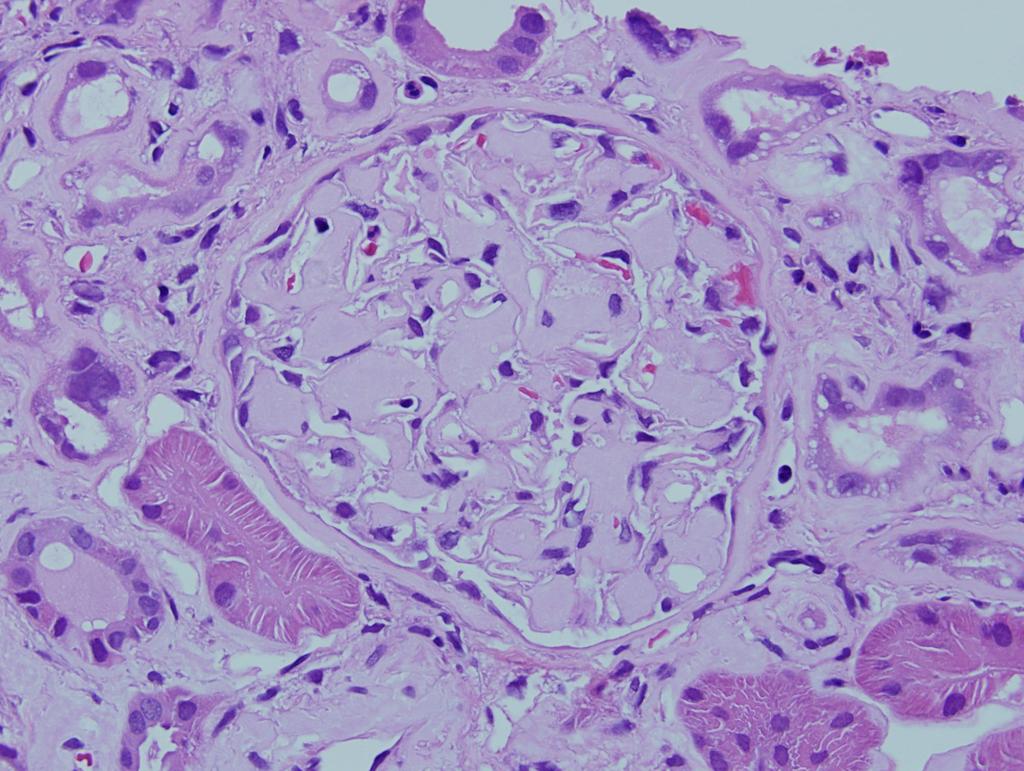
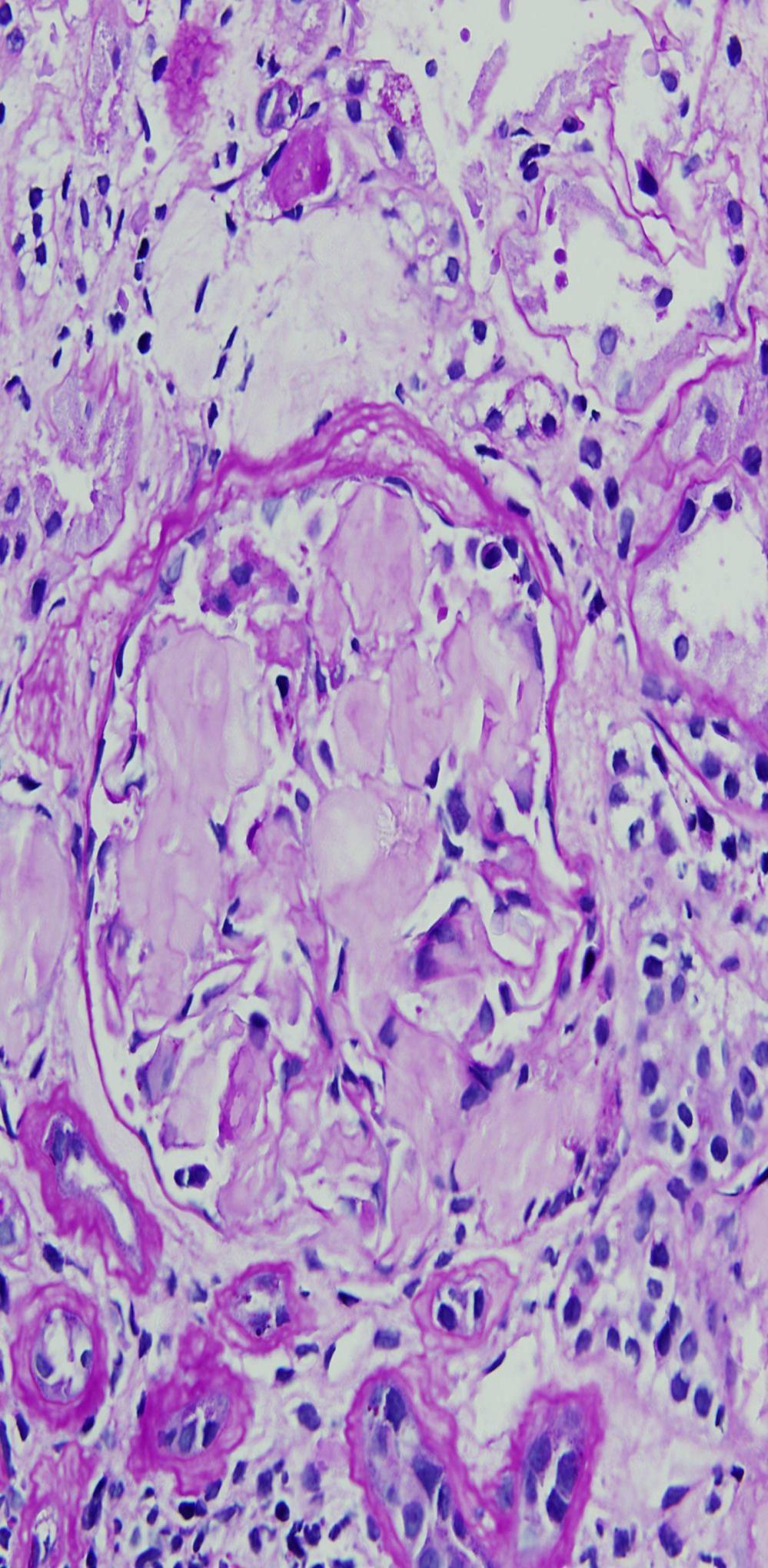
9 Light microscopy, IF, AND EM Varied morphologic patterns by LM MOST COMMON- Mesangial proliferative / sclerosing features followed by membranoproliferative in some cases mimics amyloidosis OR MEMBRANOUS NEPHROPATHY- CRESCENTS IN SOME CASES FINAL DIAGNOSIS MADE ULTRASTRUCTURALLY BUT IF PATTERN CAN BE DIAGNOSTIC (or highly suggestive)
10 A B
11
12
13
14
15
16

17 FIBRILLARY GN LIGHT MICROSCOPIC FINDINGS Can be confused with membranous GN, mesangial proliferative and membrano proliferative GN, focal proliferative, and amyloidosis Crescents are seen in 25-33% of fibrillary GN cases, and; therefore, it can also be confused with crescentic GN.
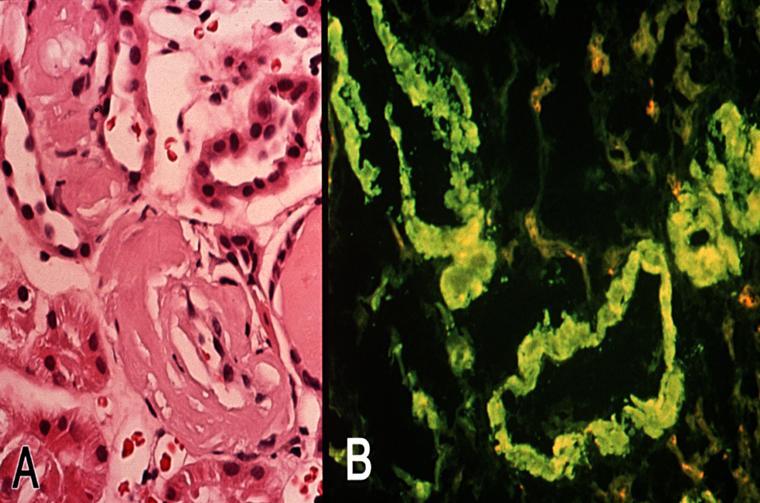
18 A IgG B

 AMYLOID P COMPONENT (SAP) PRESENT- may play a role in fibrillogenesis APO-E PRESENT AS IN")
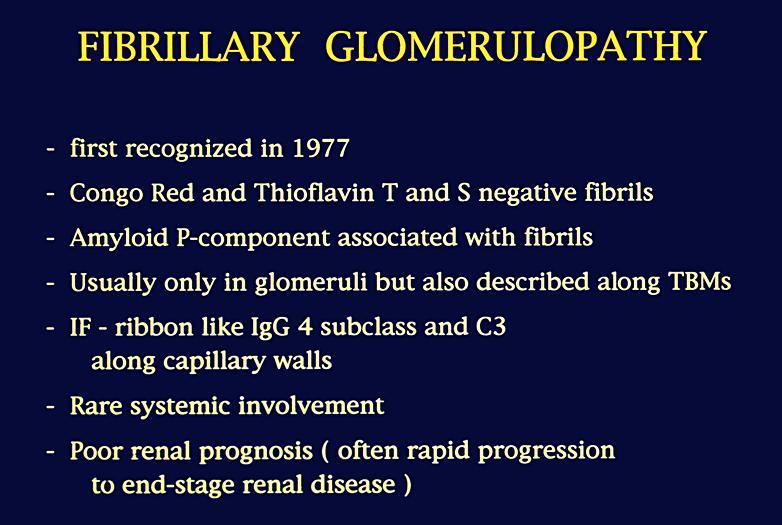
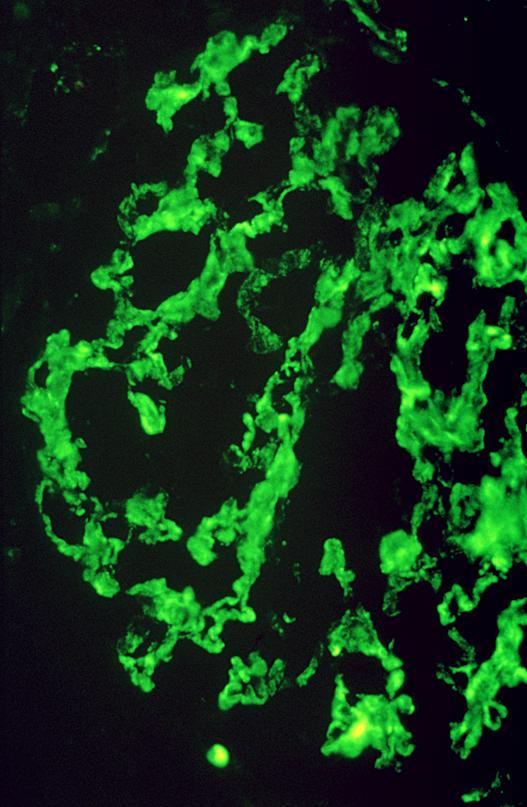
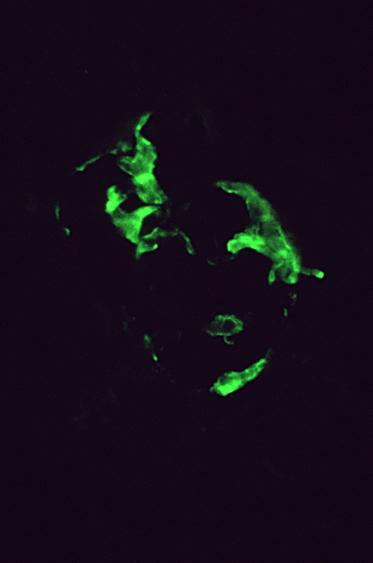
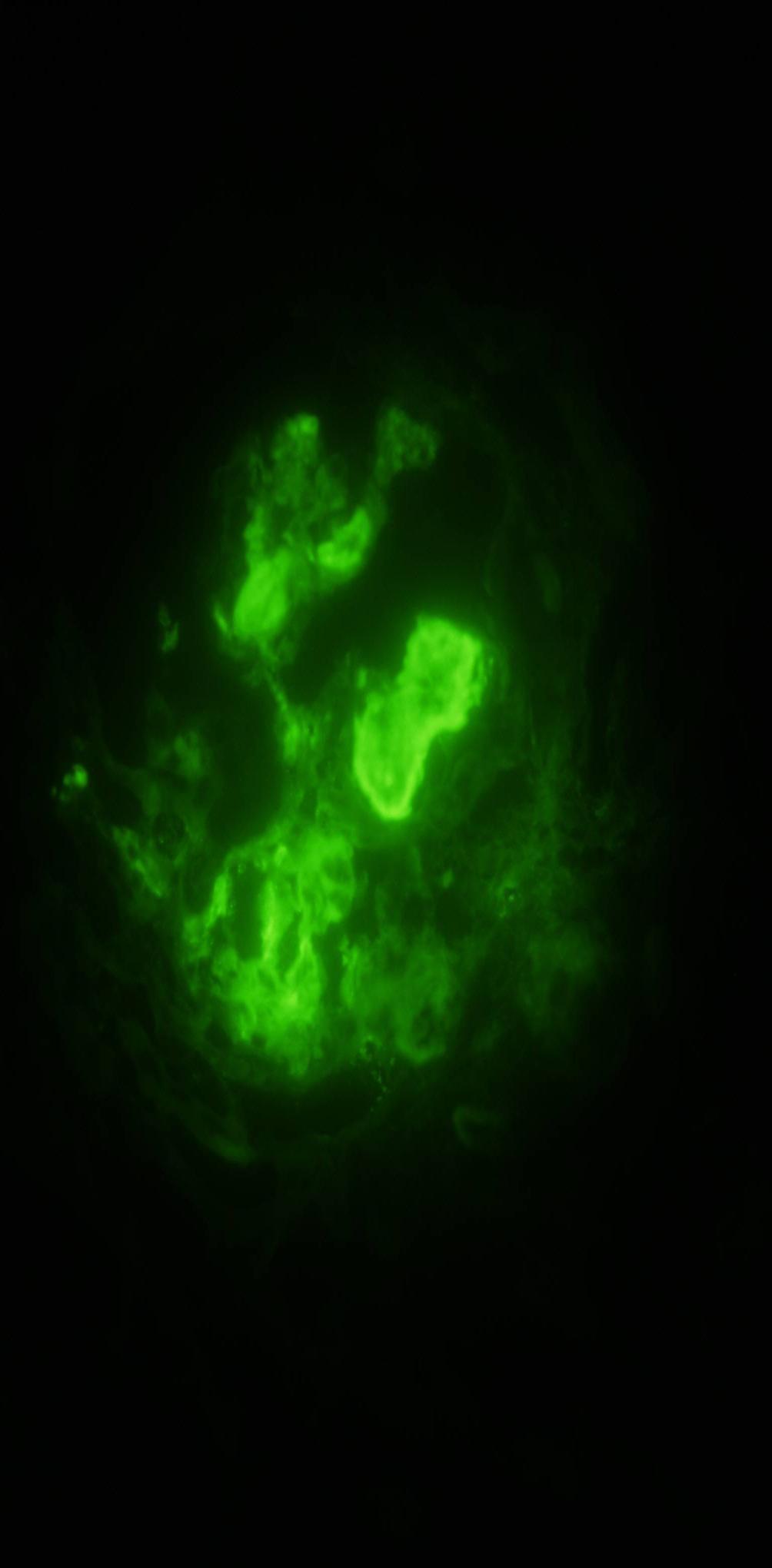
19 IMMUNOFLUORESCENCE Smudgy staining for IgG, C3, kappa and lambda light chains in most cases along peripheral capillary walls and / or in mesangium / IgA-IgM rare & small amounts C1q also rarely seen- but may be found in a few cases IgG 4 is the dominant IgG in the great majority of the cases (IgG1 in some cases) AMYLOID P COMPONENT (SAP) PRESENT- may play a role in fibrillogenesis APO-E PRESENT AS IN AMYLOID

20 IF FOR IgG
21 A B
22


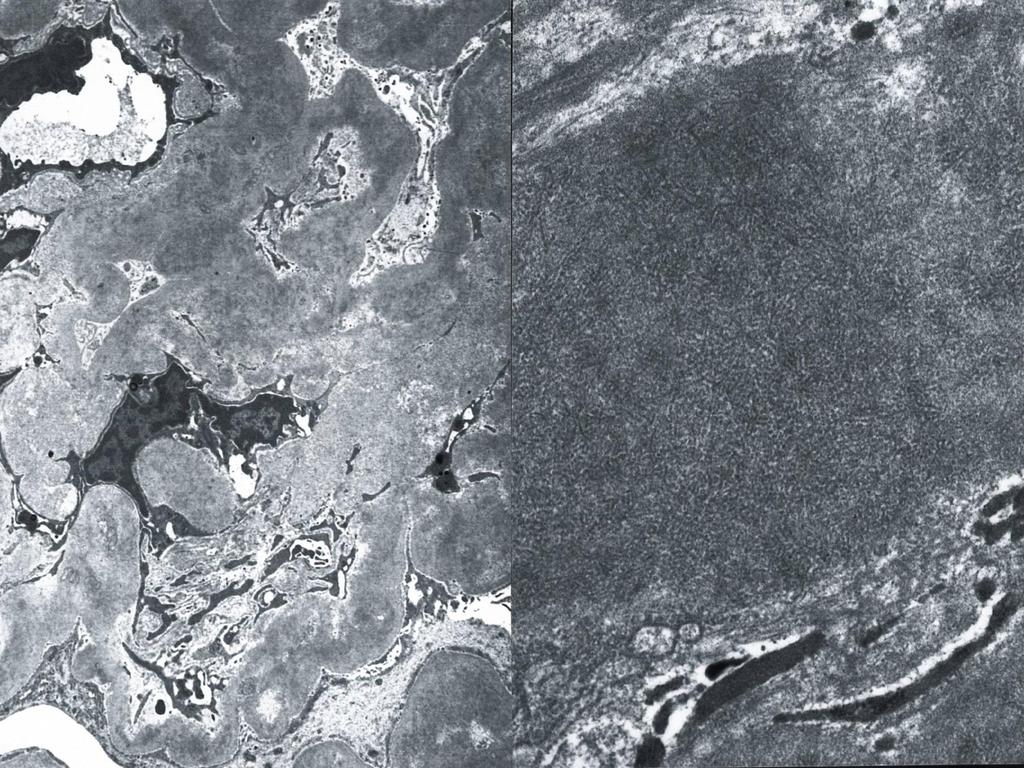
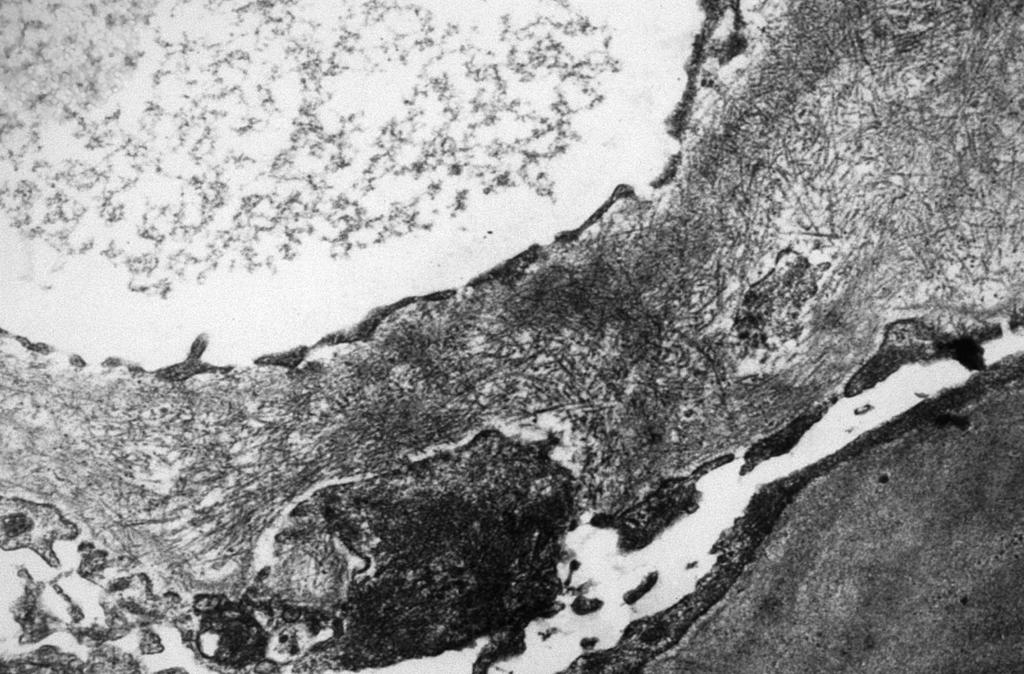
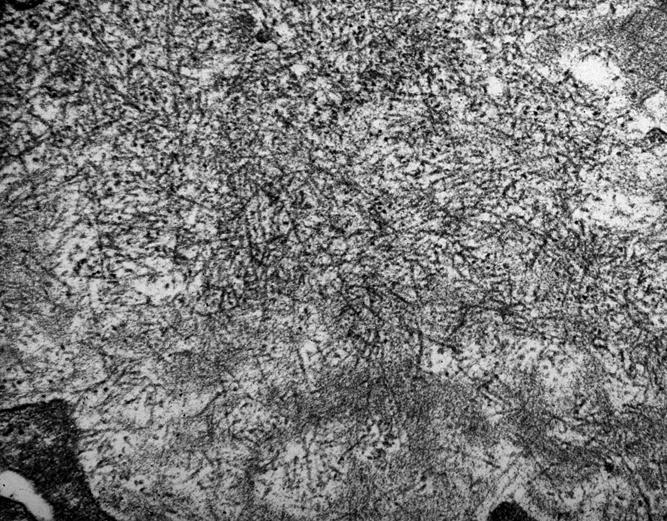
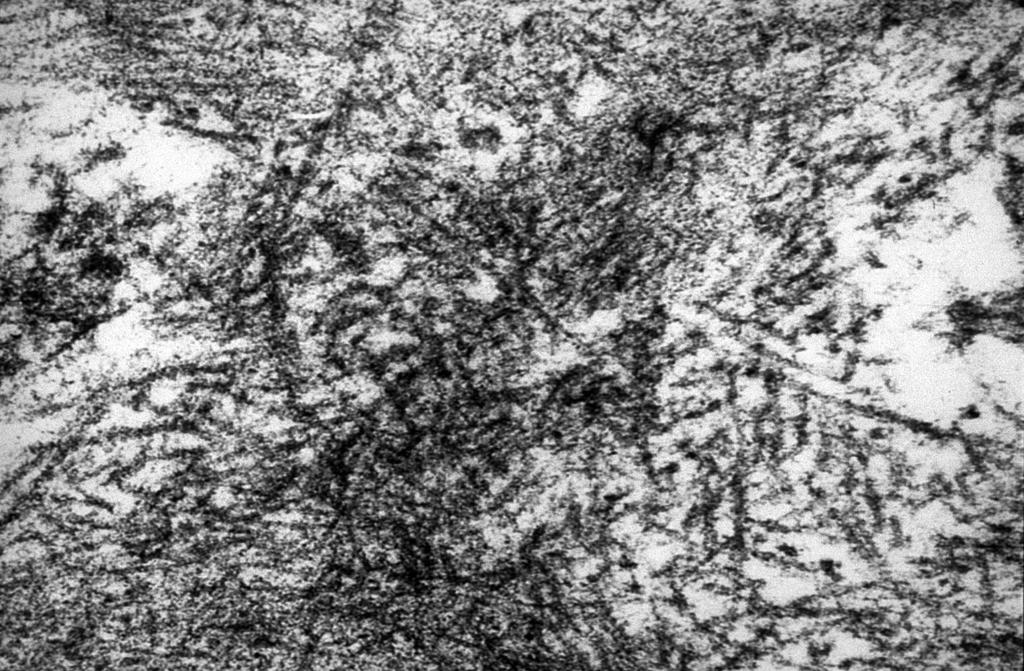
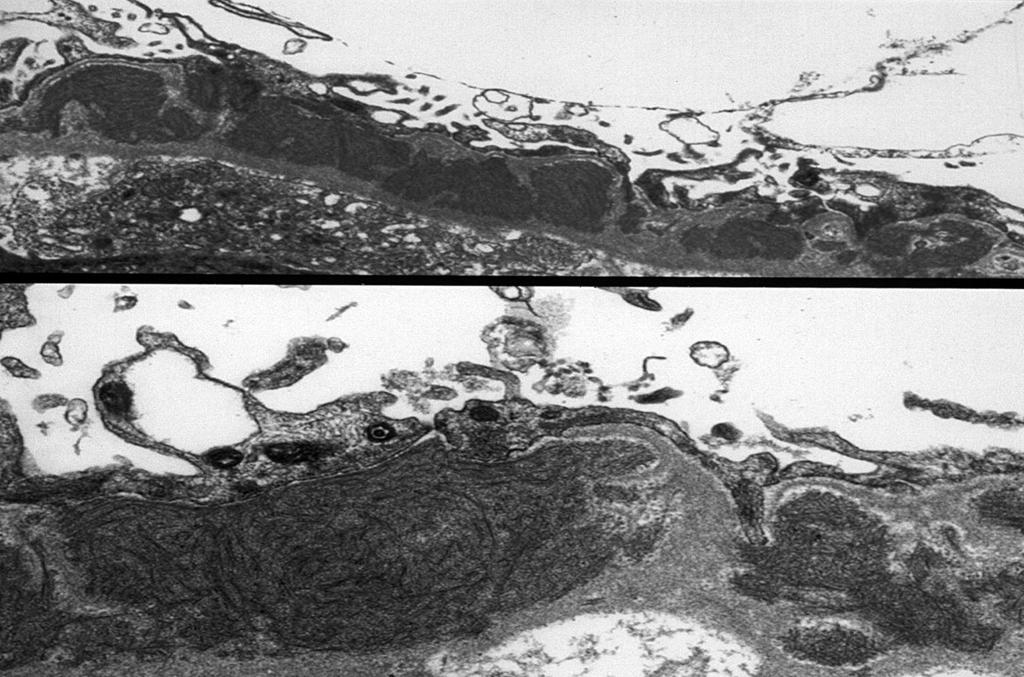
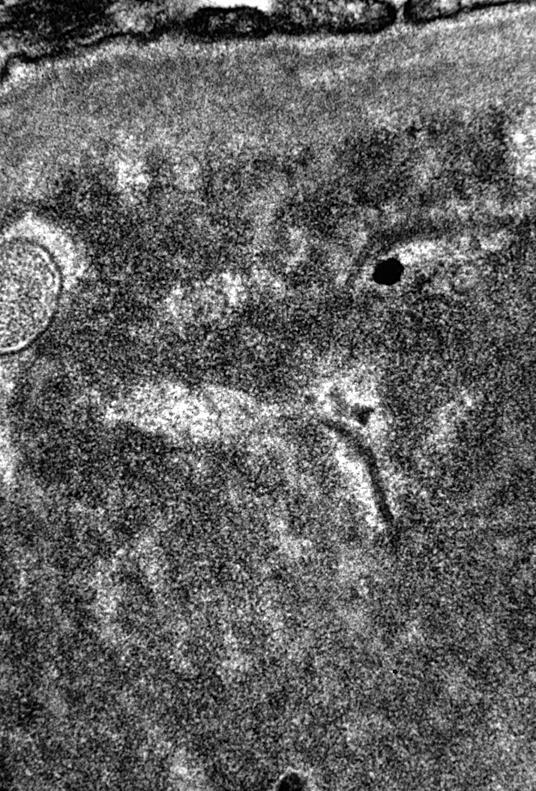
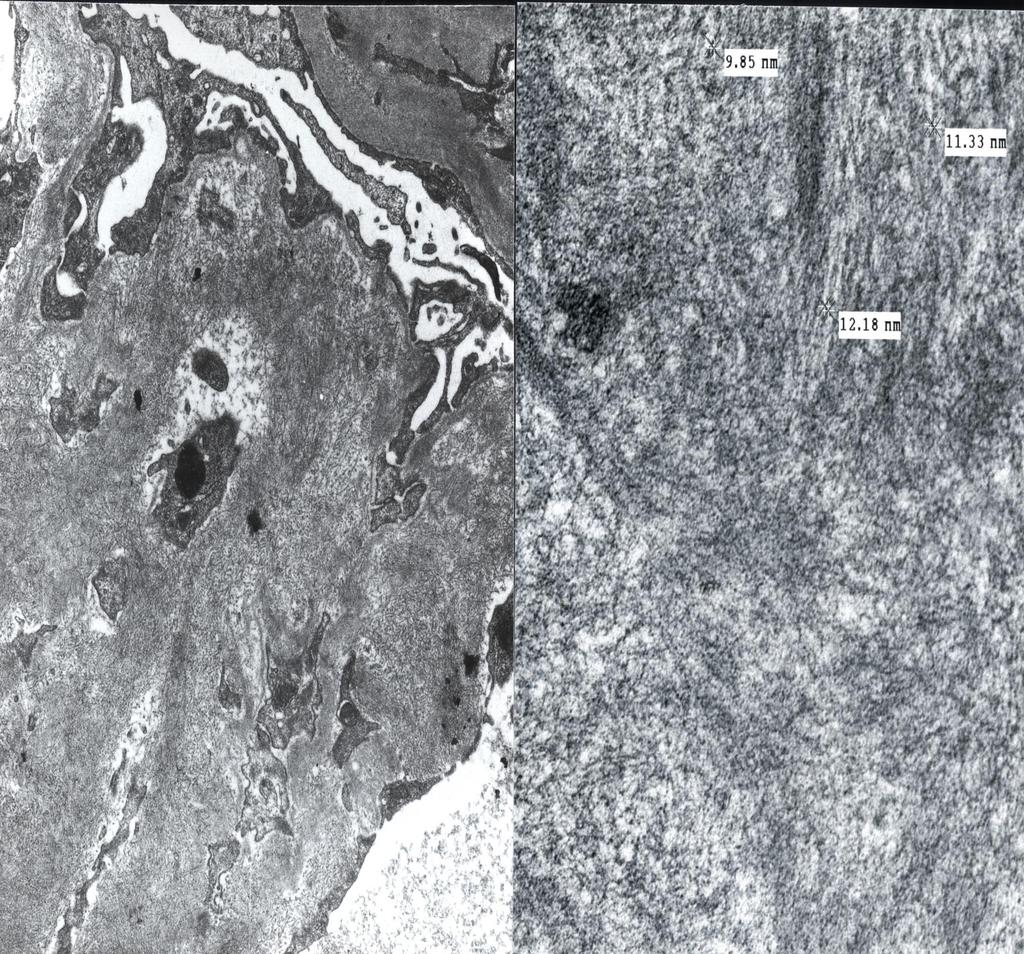
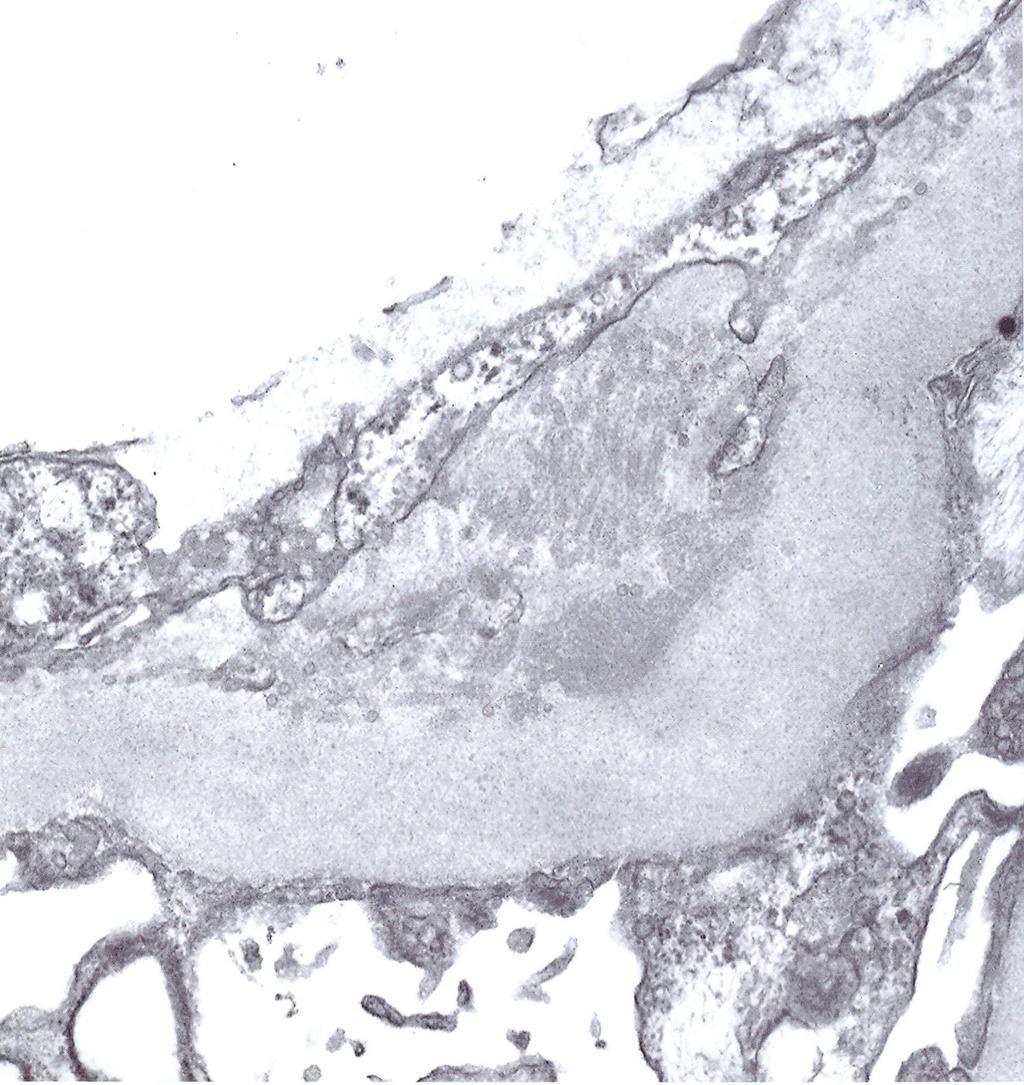
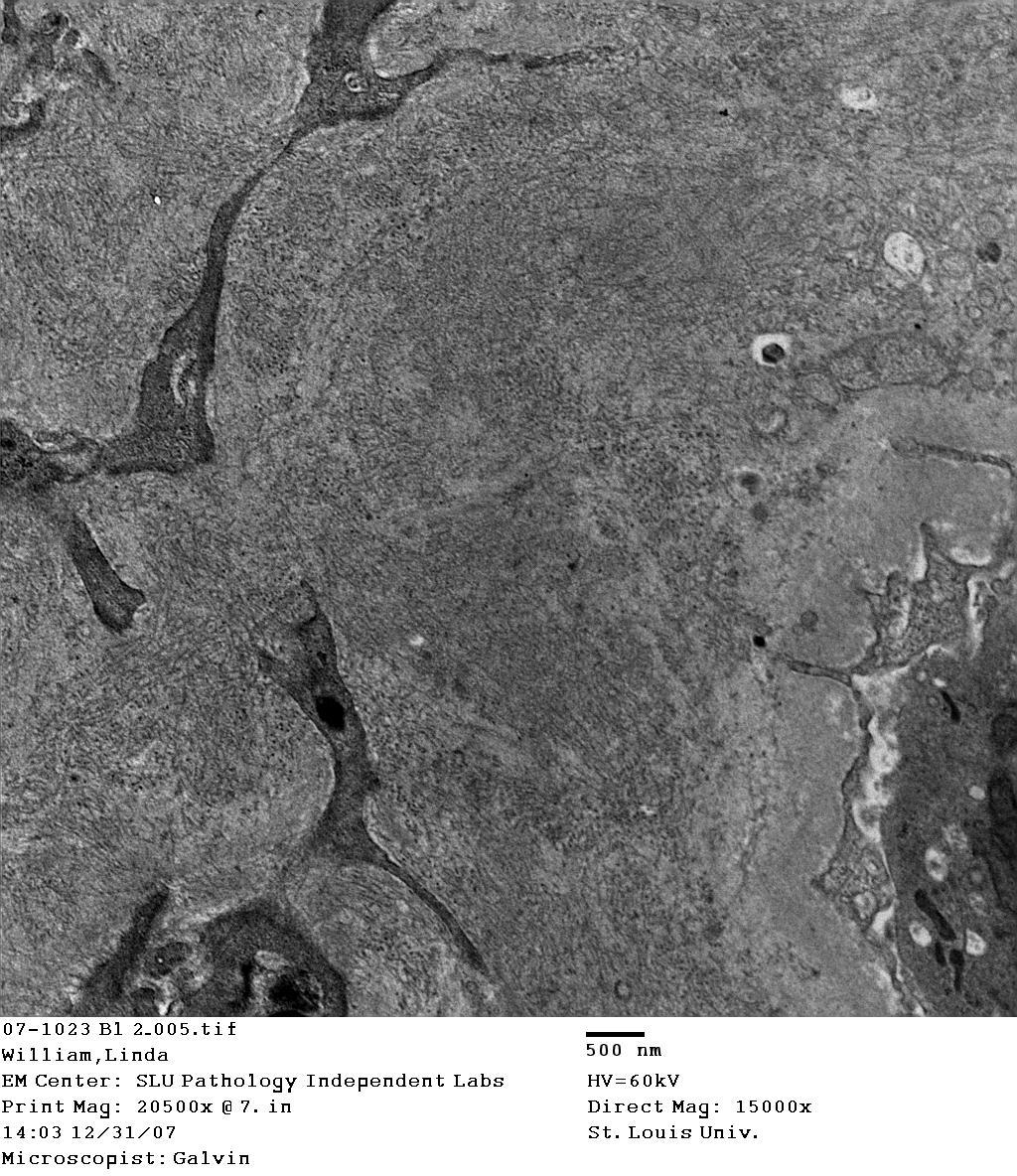
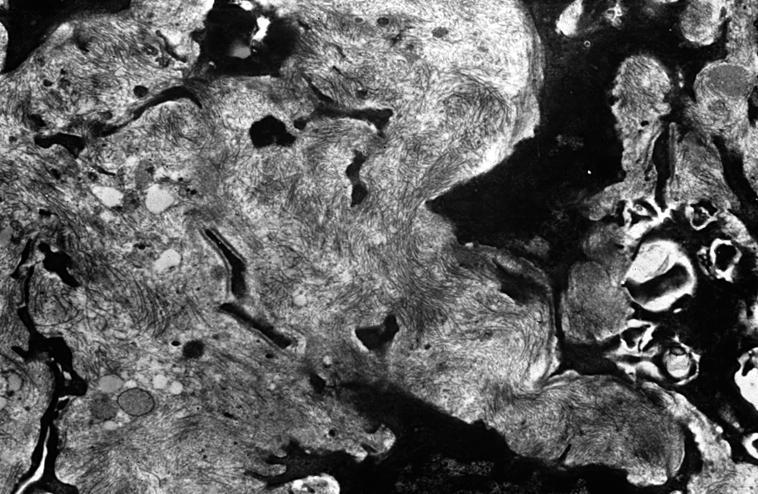
23 ELECTRON MICROSCOPY Characteristic fibrils which are randomly disposed, non-branching, and typically measure nm in diameter FIBRILS IN MESANGIUM AND IN MOST CASES ALSO ALONG PERIPHERAL CAPILLARY WALLS SIMILAR APPEARANCE TO AMYLOID BUT SIGNIFICANTLY THICKER
24
25
26
27

28 AMYLOID FIBRILLARY GN
29 A B
 is dominant in many (?")
30 FIBRILLARY GN PATHOGENESIS Most likely a result of polymerization of immune complexes and, possibly monoclonal light chains in some cases Role that amyloid-p component plays still unclear but may be significant The fact that a particular IgG (IgG4) is dominant in many (?all- some IgG1) of the cases probably represents an important pathogenetic consideration HIGHLY STRUCTURED IMMUNE COMPLEXES

31 FIBRILLARY GN TREATMENT RENIN ANGIOTENSIN SYSTEM BLOCKADE (ACE inhibitors) STEROIDS ADDITIONAL IMMUNOSUPPRESANTS SUCH AS CYTOXAN / MMF S/T combined RITUXIMAB IN COMBINATION WITH STEROIDS OR ALONE IMMUNOMODULATION

 Diabetic fibrillosis may be an important differential diagnosis in patients")
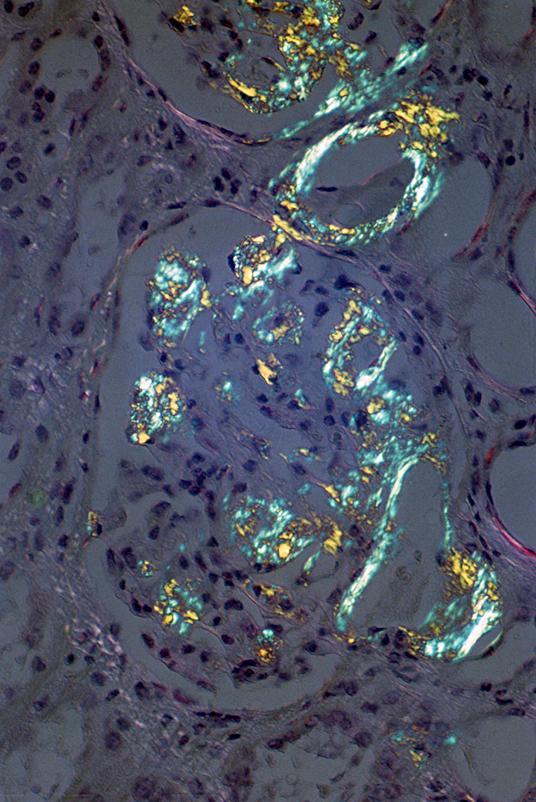
32 FIBRILLARY GN OTHER IMPORTANT FACTS Mostly a renal limited disorder Thioflavin T may be very rarely positive and be confused with amyloidosis / However these cases are Congo red negative Diverse glomerular morphology Membranous variant can also be confusingoften kappa restricted (r/o underlying lymphoproliferative disorder) Diabetic fibrillosis may be an important differential diagnosis in patients with diabetic nephropathy
33 FIBRILLARY GN PROGNOSIS Average follow-up months of 61 patients 13% complete or partial remission 43% persistent renal dysfunction 44% progressed to ESRD recurrence in 36% of 14 patients with renal transplants PREDICTORS OF ESRD- Older age, higher serum creatinine and proteinuria at the time of biopsy Nasr et al: Clin J Am Soc Nephrol. 6: , 2011
34 FIBRILLARY GN AND RENAL TRANSPLANTATION 15 TRANSPLANTED KIDNEYS IN 12 PATIENTS Group 1-5 patients WITH FIB GN alone Group 2-7 patients WITH FIB GN AND MONOCLONAL GAMMOPATHY RECURRENCE DID NOT OCCUR IN GROUP 1 BUT DEVELOPED IN 5 kidneys OF patients from GROUP 2 7 allografts failed- 1 in Group 1 (graft thromboembolism) and 6 in Group 2. Czarnecki et al: Long-term outcome of kidney transplantation in patients with fibrillary glomerulonephritis or mononclonal gammopathy with fibrillary deposits. Kid Int 75: , 2009
35 DIFFERENTIAL DIAGNOSIS

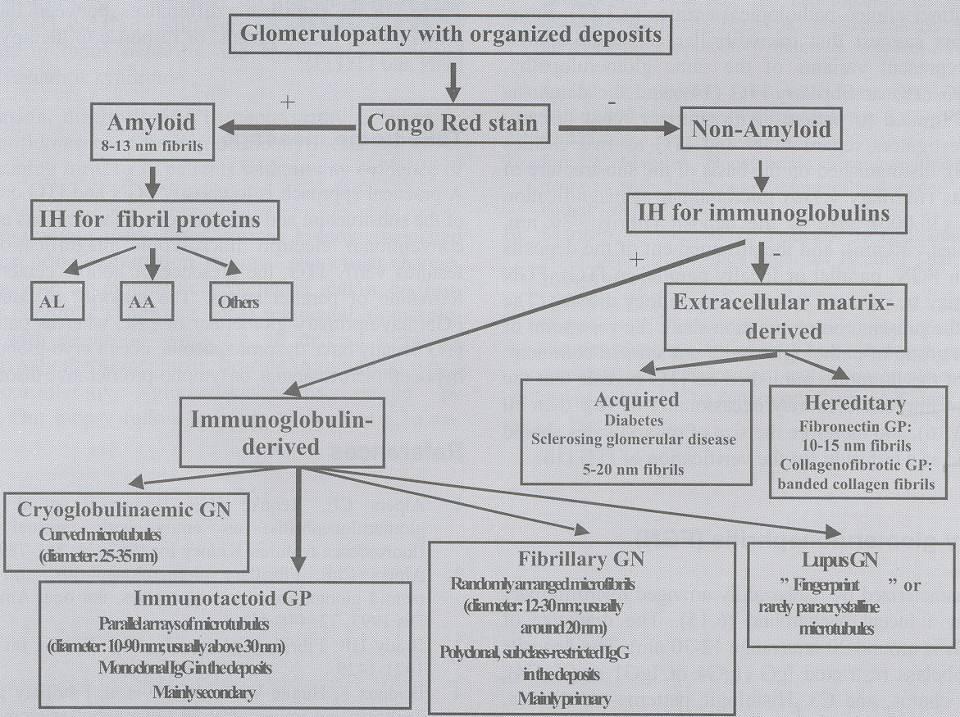
36 FIBRILLARY GN DIFFERENTIAL DIAGNOSIS Membranous GN- when only IF available Amyloidosis Immunotactoid glomerulopathy Diabetic fibrillosis Fibrillary collagen

37 AMYLOIDOSIS Systemic disorder Involvement of all 3 renal compartments Congo red / Thioflavin T positive More than 30 amyloid precursor proteins IF- addresses light and heavy chains / fibrinogen IH- AA amyloidosis, β2 microglobulin, calcitonin, LEC-2 and so forth Stains for serum amyloid protein and Apo E Can be confused with hyalinosis (especially vascular)
38
39
40 A B
41 A B THIOFLAVIN T
42 Thioflavin T

43 AMYLOID VIEWED UNDER TEXAS RED FLUORESCENCE GATE
44 A B

45 DIAGNOSIS OF AMYLOIDOSIS IS MADE THEN WHAT?? DETERMINING TYPE OF AMYLOID look for light and heavy chain monoclonality- IF evaluate fibrinogen IF stain perform pertinent immunohistochemical stains ie. AA protein, B-2 microglobulin, calcitonin, transthyretin, lactoferrin, lysozyme and so forth* PROBLEMS: DIFFICULTY IDENTIFYING HEREDITARY AMYLOIDOSES AND SOME ABNORMAL LIGHT CHAINS DEPOSITED IN TISSUES *TYPE OF AMYLOID IDENTIFIED IN 92% OF THE CASES (formalin fixed and paraffin embedded) IN SURGICAL PATHOLOGY SPECIMENS. Kebbel and Rocken Am J Surg Pathol 2006; 30:

46 AMYLOID-A PROTEIN IH
 Most gamma HC-associated Similar light and EM features as other amyloidoses Pathogenesis")
47 Heavy chain amyloidosis AH-amyloidosis Only a handful of cases reported (one with ultrastructural labeling) Most gamma HC-associated Similar light and EM features as other amyloidoses Pathogenesis unclear

48 LIGHT AND HEAVY CHAIN AMYLOIDOSIS (AL/AH) 16 patients with AL/AH amyloidosis Typing using laser microdissection and mass spectroscopy (LMD/MS) (12) and by IF (4) Median age at biopsy- 63 All caucasian WHEN COMPARED WITH AL-AMYLOIDOSIS Less cardiac involvement Higher incidence of hematuria Better survival 42% of patients could have been diagnosed with IF Nasr, SH et al: The diagnosis and characteristics of renal heavy chain/light chain amyloidosis and comparison with renal light-chain amyloidosis. Kidney Int 2013; 83:

49 LIGHT / HEAVY CHAIN AMYLOIDOSIS (AL/AH) MORPHOLOGICAL DIFFERENCES WITH AL-AMYLOIDOSIS More hypercellularity in mesangial areas with amyloid deposition Strong PAS staining associated with amyloid deposits Silver staining in areas with amyloid deposition
50
51
52 EVEN C1q in selected cases MAY VARY FROM NM FREQUENTLY PARALLEL TO EACH OTHER
53
54 IF- IgG
55
56
57
58
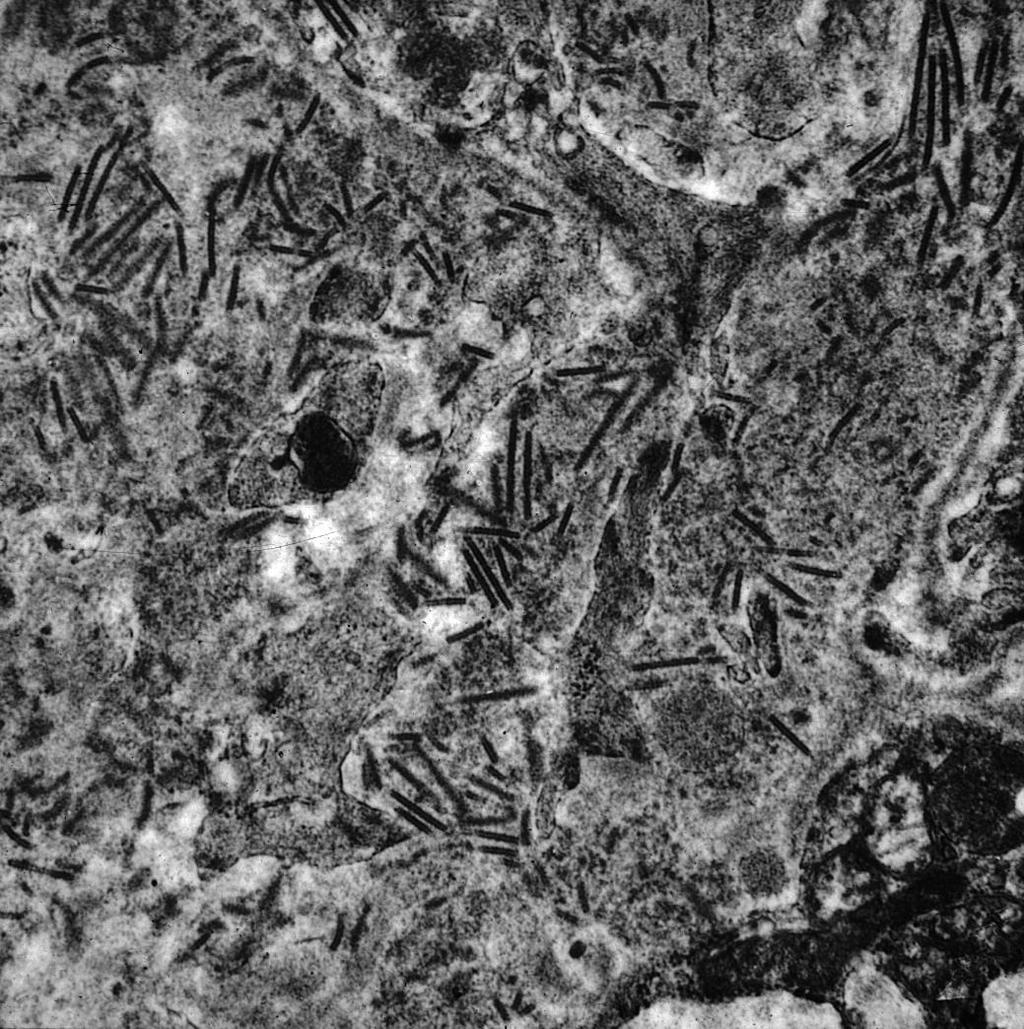
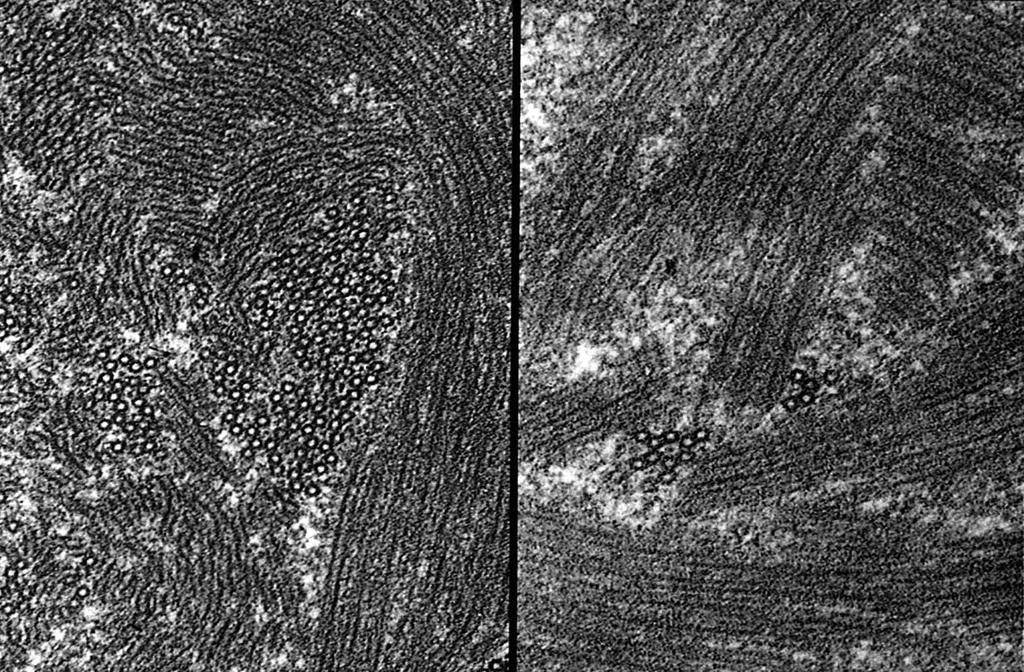
59 IMMUNOTACTOID GN MICROTUBULAR STRUCTURES CAN BE LONG AND GENERALLY ORGANIZED IN PARALLEL BUNDLES ORGANIZED MICROTUBULAR STRUCTURES WHICH MEASURE NM IN WIDTH NEGATIVE FOR CONGO RED AND THIOFLAVIN T MAIN DIFFERENTIAL DX IS CRYOS
60

61 IMMUNOTACTOID GN EXTRARENAL DEPOSITS ARE EXTREMELY RARE SIMILAR ENTITY IN THE EYE- relationship to renal disease unclear Can be confused with cryoglobulinemic nephropathy as the deposits are microtubular not FIBRILLARY
 AND OCCURS IN THE SETTING OF NODULAR")
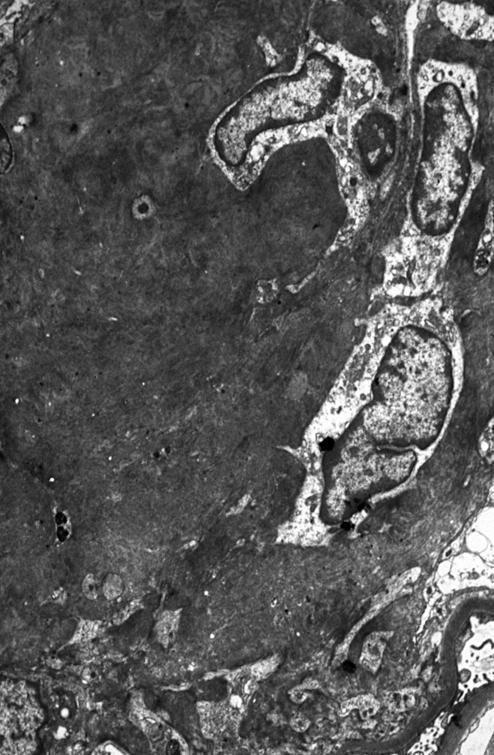
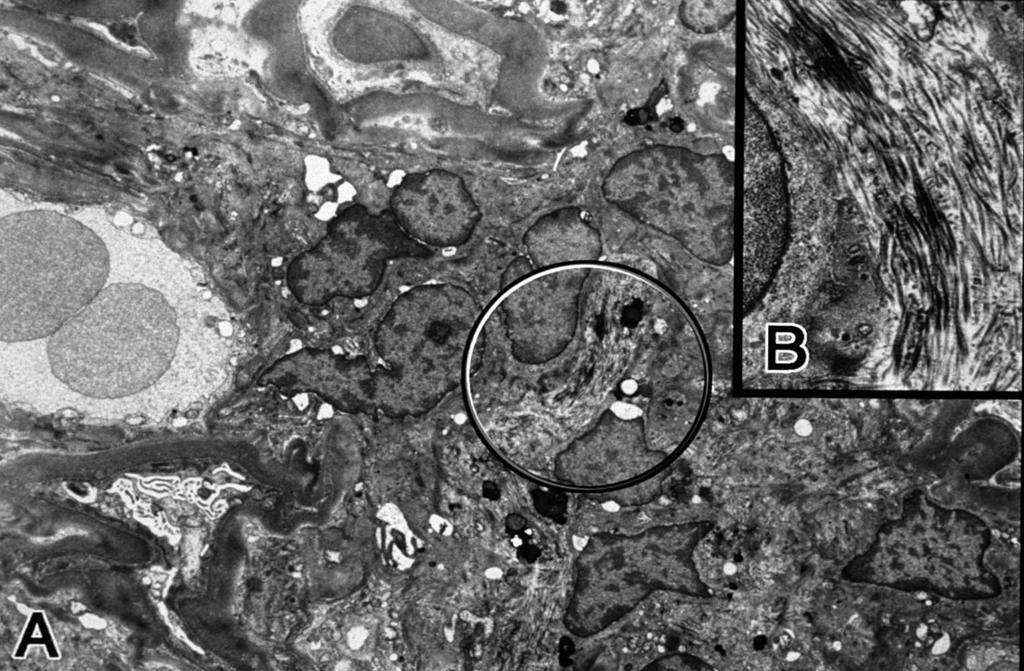
62 DIABETIC FIBRILLOSIS Appearance of fibrils ultrastructurally identical to FIBRILLARY GN BUT FIBRILS ONLY IN MESANGIUM IF IS NEGATIVE FOR IgG / kappa / lambda (LINEAR IgG and albumin seen in DN) AND OCCURS IN THE SETTING OF NODULAR GLOMERULOSCLEROSIS
63 DIABETIC FIBRILLOSIS
64
65
66
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA
 C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
C3G An Update What is C3 Glomerulopathy Anyway? Patrick D. Walker, M.D. Nephropath Little Rock, Arkansas USA C3 Glomerulopathy Overview Discuss C3 Glomerulopathy (C3G) How did we get to the current classification
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME
 CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
CASE 3 AN UNUSUAL CASE OF NEPHROTIC SYNDROME Dr Seethalekshmy N.V., Dr.Annie Jojo, Dr Hiran K.R., Amrita institute of Medical Sciences, Kochi, Kerala Case history 34 year old gentleman Nephrotic range
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Rituximab treatment for fibrillary glomerulonephritis
 Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Nephrol Dial Transplant (2014) 29: 1925 1931 doi: 10.1093/ndt/gfu189 Advance Access publication 27 May 2014 Rituximab treatment for fibrillary glomerulonephritis Jonathan Hogan, Michaela Restivo, Pietro
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Article. Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy
 Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Article Laser Microdissection and Proteomic Analysis of Amyloidosis, Cryoglobulinemic GN, Fibrillary GN, and Immunotactoid Glomerulopathy Sanjeev Sethi,* Jason D. Theis,* Julie A. Vrana,* Fernando C. Fervenza,
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Amyloidosis is caused by extracellular deposition of
 Mass Spectrometry Based Proteomic Diagnosis of Renal Immunoglobulin Heavy Chain Amyloidosis Sanjeev Sethi,* Jason D. Theis,* Nelson Leung, Angela Dispenzieri,* Samih H. Nasr,* Mary E. Fidler,* Lynn D.
Mass Spectrometry Based Proteomic Diagnosis of Renal Immunoglobulin Heavy Chain Amyloidosis Sanjeev Sethi,* Jason D. Theis,* Nelson Leung, Angela Dispenzieri,* Samih H. Nasr,* Mary E. Fidler,* Lynn D.
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
substance staining with IgG, C3 and IgA (trace) Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ
 Linear deposition of IgG(+), IgA.M(trace) and C3(+++) at the DEJ") Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Direct Immunofluorescence: Skin Diagnosis Findings Picture Pemphigus Vulgaris and it s Intracellular cement variants substance staining with IgG, C3 and IgA (trace) Bullous Pemphigoid and it s variants
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Overview of glomerular diseases
 Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Overview of glomerular diseases *Endothelial cells are fenestrated each fenestra: 70-100nm in diameter Contractile, capable of proliferation, makes ECM & releases mediators *Glomerular basement membrane
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Sheena Surindran Grand Rounds 2/15/11
 Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
Sheena Surindran Grand Rounds 2/15/11 Affects 5 12 person per million / year 5 10% associated with myeloma Median survival without treatment is 12 40 months Most commonly affected organs are kidney, heart
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Clinical history. 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Cardiac catheterization: no CAD
 CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
CASE 8 Clinical history 73 yo man with chest pain Systemic hypertension and WG Stress EKG N Stress echocardiogram: Concentric hypertrophy Hypokinesis of LV-Inf Cardiac catheterization: no CAD Technique
Complement in vasculitis and glomerulonephritis. Andy Rees Clinical Institute of Pathology Medical University of Vienna
 Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Complement in vasculitis and glomerulonephritis Andy Rees Clinical Institute of Pathology Medical University of Vienna 41 st Heidelberg Nephrology Seminar March 2017 The complement system An evolutionary
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
IgA nephropathy: unusual forms
 IgA nephropathy: unusual forms Khalil EL KAROUI Service de néphrologie et transplantation rénale, INSERM U1151 Hôpital Henri Mondor, Créteil Actualités Néphrologiques J. Hamburger 23 Avril 2018 Introduction:
IgA nephropathy: unusual forms Khalil EL KAROUI Service de néphrologie et transplantation rénale, INSERM U1151 Hôpital Henri Mondor, Créteil Actualités Néphrologiques J. Hamburger 23 Avril 2018 Introduction:
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
C3 Glomerulonephritis versus C3 Glomerulopathies?
 Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Washington University School of Medicine Digital Commons@Becker Kidneycentric Kidneycentric 2016 C3 Glomerulonephritis versus C3 Glomerulopathies? T. Keefe Davis Washington University School of Medicine
Diabetic Nephropathy. Introduction/Clinical Setting. Pathologic Findings Light Microscopy. J. Charles Jennette
 12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
12 Diabetic Nephropathy J. Charles Jennette Introduction/Clinical Setting Diabetic nephropathy is a clinical syndrome in a patient with diabetes mellitus that is characterized by persistent albuminuria,
What s hiding behind IgA nephropathy?
 What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
What s hiding behind IgA nephropathy? Bauerova L. Department of Pathology, the First Faculty of Medicine and General Hospital, Charles University Prague (nephropathology training: Department of Clinical
Renal manifestations of IgG4-related systemic disease
 Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
Renal manifestations of IgG4-related systemic disease Lynn D. Cornell, M.D. Mayo Clinic Rochester, MN While autoimmune pancreatitis (AIP) has been recognized since the first description by Sarles et al
A case of heavy chain deposition disease complicated by acquired angioedema.
 Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
Case Report http://www.alliedacademies.org/pathology-and-disease-biology/ A case of heavy chain deposition disease complicated by acquired angioedema. Rafia Chaudhry 1 *, Gautam Bhave 2, Rachel Fissell
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias
 Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Expanding Spectrum of Diseases Associated with Plasma Cell Dyscrasias Eva Honsova Institute for Clinical and Experimental Medicine Prague, Czech Republic eva.honsova@ikem.cz Plasma cell dyscrasias Plasma
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease
 Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
Case Study TheScientificWorldJOURNAL (2009) 9, 1348 1354 ISSN 1537-744X; DOI 10.1100/tsw.2009.164 A Case of Immunotactoid Glomerulopathy with Rapid Progression to End-Stage Renal Disease Shikha Jain 1,
Jon Von Visger 1, Clarissa Cassol 2, Uday Nori 1, Gerardo Franco-Ahumada 1, Tibor Nadasdy 2 and Anjali A. Satoskar 2*
 Von Visger et al. BMC Nephrology (2019) 20:53 https://doi.org/10.1186/s12882-019-1239-8 CASE REPORT Open Access Complete biopsy-proven resolution of deposits in recurrent proliferative glomerulonephritis
Von Visger et al. BMC Nephrology (2019) 20:53 https://doi.org/10.1186/s12882-019-1239-8 CASE REPORT Open Access Complete biopsy-proven resolution of deposits in recurrent proliferative glomerulonephritis
Amyloidosis is a generic term for a group of diseases
 Typing of Amyloidosis in Renal Biopsies Diagnostic Pitfalls Anjali A. Satoskar, MD; Kelly Burdge, MD; Daniel J. Cowden, MD; Gyongyi M. Nadasdy, MD; Lee A. Hebert, MD; Tibor Nadasdy, MD Context. Amyloidosis
Typing of Amyloidosis in Renal Biopsies Diagnostic Pitfalls Anjali A. Satoskar, MD; Kelly Burdge, MD; Daniel J. Cowden, MD; Gyongyi M. Nadasdy, MD; Lee A. Hebert, MD; Tibor Nadasdy, MD Context. Amyloidosis
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft
 Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Glomerulonephritis. Dr Rodney Itaki Anatomical Pathology Discipline.
 Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Glomerulonephritis Dr Rodney Itaki Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Gross anatomy Ref: Goggle Images Microanatomy
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Monoclonal gammopathies consist of. Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis REVIEW
 REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
REVIEW Monoclonal GammopathyeAssociated Proliferative Glomerulonephritis Sanjeev Sethi, MD, PhD, and S. Vincent Rajkumar, MD Abstract Monoclonal gammopathy is characterized by circulating monoclonal immunoglobulin
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
EDEMA IN A PATIENT WITH RECURRENT RESPIRATORY INFECTIONS - Case Report
 EDEMA IN A PATIENT WITH RECURRENT RESPIRATORY INFECTIONS - Case Report Alain SOUPART, MD, PhD, FACP.hon Department of General Internal Medicine, Jolimont/Tubize and Erasmus University Hospital, Free University
EDEMA IN A PATIENT WITH RECURRENT RESPIRATORY INFECTIONS - Case Report Alain SOUPART, MD, PhD, FACP.hon Department of General Internal Medicine, Jolimont/Tubize and Erasmus University Hospital, Free University
Update on Treatments for Systemic Amyloidosis
 Update on Treatments for Systemic Amyloidosis Laura M. Dember, M.D. Renal, Electrolyte and Hypertension Division University of Pennsylvania ANZSN Update Course Darwin, Australia September 2, 2017 Disclosure
Update on Treatments for Systemic Amyloidosis Laura M. Dember, M.D. Renal, Electrolyte and Hypertension Division University of Pennsylvania ANZSN Update Course Darwin, Australia September 2, 2017 Disclosure
Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome
 Castano et al. BMC Nephrology (2015) 16:64 DOI 10.1186/s12882-015-0046-0 RESEARCH ARTICLE Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome Open Access Ekaterina
Castano et al. BMC Nephrology (2015) 16:64 DOI 10.1186/s12882-015-0046-0 RESEARCH ARTICLE Comparison of amyloid deposition in human kidney biopsies as predictor of poor patient outcome Open Access Ekaterina
J Nephropharmacol. 2014; 3(2): Journal of Nephropharmacology
: Journal of Nephropharmacology") J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
29th Annual Meeting of the Glomerular Disease Collaborative Network
 29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
29th Annual Meeting of the Glomerular Disease Collaborative Network Updates on the Pathogenesis IgA Nephropathy and IgA Vasculitis (HSP) J. Charles Jennette, M.D. Brinkhous Distinguished Professor and
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS
 GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
GOODPASTURE'S SYNDROME WITH CONCOMITANT IMMUNE COMPLEX MIXED MEMBRANOUS AND PROLIFERATIVE GLOMERULONEFRITIS VESNA JURČIĆ 1, ANDREJA ALEŠ RIGLER 2, INSTITUTE OF PATHOLOGY, FACULTY OF MEDICINE, UNIVERSITY
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Multiple Myeloma Advances for clinical pathologists & histopathologists
 Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Multiple Myeloma Advances for clinical pathologists & histopathologists CME in Haematology 2014 IAPP & Dept of Pathology, BVDUMC, Pune Sunday, 4 th May 2014 Dr. M.B. Agarwal, MD, MNAMS Head, Dept of Haematology
Characterization and outcomes of renal leukocyte chemotactic factor 2-associated amyloidosis
 http://www.kidney-international.org & 2014 International Society of Nephrology see commentary on page 229 Characterization and outcomes of renal leukocyte chemotactic factor 2-associated amyloidosis Samar
http://www.kidney-international.org & 2014 International Society of Nephrology see commentary on page 229 Characterization and outcomes of renal leukocyte chemotactic factor 2-associated amyloidosis Samar
CJASN epress. Published on September 28, 2010 as doi: /CJN
 CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
DIABETIC NEPHROPATHY is a major
 KIDNEY BIOPSY TEACHING CASES Nodular Glomerulopathy in a 50-Year-Old Diabetic Man Erika R. Bracamonte, MD, Peter Hullman, MD, and Kelly D. Smith, MD, PhD INDEX WORDS: Diabetes; membranoproliferative glomerulonephritis;
KIDNEY BIOPSY TEACHING CASES Nodular Glomerulopathy in a 50-Year-Old Diabetic Man Erika R. Bracamonte, MD, Peter Hullman, MD, and Kelly D. Smith, MD, PhD INDEX WORDS: Diabetes; membranoproliferative glomerulonephritis;
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Clinical, morphologic, and genetic features of renal leukocyte chemotactic factor 2 amyloidosis
 http://www.kidney-international.org & 2014 International Society of Nephrology see commentary on page 229 Clinical, morphologic, and genetic features of renal leukocyte chemotactic factor 2 amyloidosis
http://www.kidney-international.org & 2014 International Society of Nephrology see commentary on page 229 Clinical, morphologic, and genetic features of renal leukocyte chemotactic factor 2 amyloidosis
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy. Patohistological Aspects
 HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
HRZZ project: Genotype-Phenotype correlation in Alport's syndrome and Thin Glomerular Basement Membrane Nephropathy Patohistological Aspects Petar Šenjug, MD 1 Professor Danica Galešić Ljubanović, MD,
Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis
 Kidney International, Vol. 65 (2004), pp. 85 96 Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis SAMIH H. NASR, GLENS. MARKOWITZ,
Kidney International, Vol. 65 (2004), pp. 85 96 Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis SAMIH H. NASR, GLENS. MARKOWITZ,
Proliferative Glomerulonephritis with Monoclonal IgG Deposits
 JASN Express. Published on May 21, 2009 as doi: 10.1681/ASN.2009010110 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Samih H. Nasr,* Anjali Satoskar, Glen S. Markowitz,* Anthony M. Valeri,
JASN Express. Published on May 21, 2009 as doi: 10.1681/ASN.2009010110 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Samih H. Nasr,* Anjali Satoskar, Glen S. Markowitz,* Anthony M. Valeri,
Dense deposit disease with steroid pulse therapy
 Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Case Report Dense deposit disease with steroid pulse therapy Jun Odaka, Takahiro Kanai, Takane Ito, Takashi Saito, Jun Aoyagi, and Mariko Y Momoi Abstract Treatment of dense deposit disease DDD has not
Yijuan Sun, Amarpreet Sandhu, Darlene Gabaldon, Jonathan Danaraj, Karen S. Servilla, and Antonios H. Tzamaloukas
 Case Reports in Nephrology Volume 2012, Article ID 573650, 5 pages doi:10.1155/2012/573650 Case Report Development of Renal Failure without Proteinuria in a Patient with Monoclonal Gammopathy of Undetermined
Case Reports in Nephrology Volume 2012, Article ID 573650, 5 pages doi:10.1155/2012/573650 Case Report Development of Renal Failure without Proteinuria in a Patient with Monoclonal Gammopathy of Undetermined
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy
 Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive Nephrotic Syndrome
 J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Original. IgAN. Key words : IgA nephropathy, IgM deposition, proteinuria, tonsillectomy, steroid pulse therapy. Introduction
 Showa Univ J Med Sci 27 3, 167 174, September 2015 Original Prominent IgM Deposition in Glomerulus Is Associated with Severe Proteinuria and Reduced after Combined Treatment of Tonsillectomy with Steroid
Showa Univ J Med Sci 27 3, 167 174, September 2015 Original Prominent IgM Deposition in Glomerulus Is Associated with Severe Proteinuria and Reduced after Combined Treatment of Tonsillectomy with Steroid
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
Membranoproliferative Glomerulonephritis
 Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
Membranoproliferative Glomerulonephritis MPGN is characterizedby alterations in the GBM and mesangium and by proliferation of glomerular cells. 5% to 10% of cases of 1ry nephrotic syndrome in children
C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon?
 NDT Plus (2009) 2: 285 291 doi: 10.1093/ndtplus/sfp055 Advance Access publication 9 May 2009 Case Report C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon? Mordi Muorah 1,ManishD.Sinha
NDT Plus (2009) 2: 285 291 doi: 10.1093/ndtplus/sfp055 Advance Access publication 9 May 2009 Case Report C1q nephropathy: a true immune complex disease or an immunologic epiphenomenon? Mordi Muorah 1,ManishD.Sinha
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
considered for patients with cryoglobulinemic kidney diseases. (Weak)
") http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
http://www.kidney-international.org & 2008 DIGO Guideline 5: Diagnosis and management of kidney diseases associated with HCV infection idney International (2008) 73 (Suppl 109), S69 S77; doi:10.1038/ki.2008.88
Immunotactoid glomerulopathy: clinicopathologic and proteomic study
 Immunotactoid glomerulopathy 4137 23. Mosteller RD. Simplified calculation of body-surface area. N Engl J Med 1987; 317: 1098 24. Levey AS, Bosch JP, Lewis JB et al. A more accurate method to estimate
Immunotactoid glomerulopathy 4137 23. Mosteller RD. Simplified calculation of body-surface area. N Engl J Med 1987; 317: 1098 24. Levey AS, Bosch JP, Lewis JB et al. A more accurate method to estimate