New biological targets for CKD- MBD: From the KDOQI to the
|
|
|
- Chad Holmes
- 6 years ago
- Views:
Transcription
1 New biological targets for CKD- MBD: From the KDOQI to the KDIGO Guillaume JEAN, MD. Centre de Rein Artificiel, 42 avenue du 8 mai 1945, Tassin la Demi-Lune, France. guillaume-jean-crat@wanadoo.fr
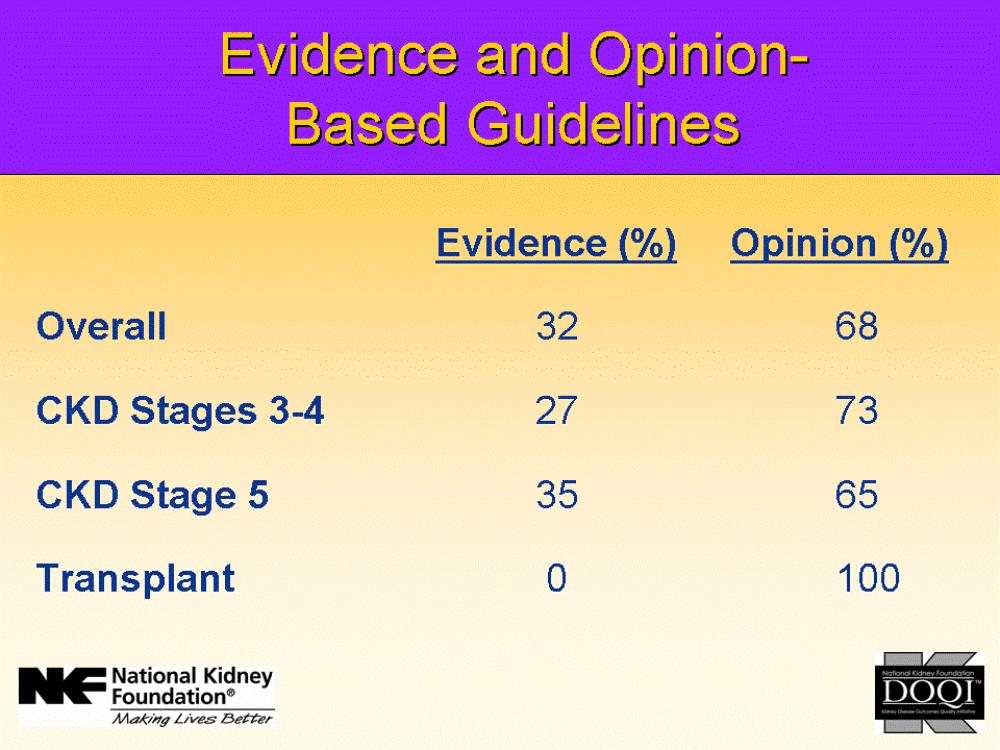
2 Introduction From 2003 to 2009 the recommendations were the Kidney Disease: Outcomes Quality Improvement (KDOQI) for mineral metabolism abnormalities. Biological targets and therapeutic strategies have been defined precisely and were used by nephrologists and in all clinical trials and observatories. In 2009, the new recommendations were released with the Kidney Disease: Improving Global Outcomes (KDIGO).
3
4 Grading differences KDIGO
5 KDOQI Grading evidence Highest quality Randomized controlled trials Matched controlled trials Prospective nonrandomized/nonmatched controlled trials Retrospective nonrandomized/nonmatched controlled trials KDIGO
6 NEW TARGET FOR PHOSPHATAEMIA
7
8 New KDIGO target In patients with CKD stages 3 5, we suggest maintaining serum phosphorus in the normal range (2C). In patients with CKD stage 5D, we suggest lowering elevated phosphorus levels toward the normal range (2C). Normal values for phosphaetamia 0,81 1,45 mmol/l (2,5 4,5 mg/dl) KDIGO
9 EVIDENCE? Risque Relatif de Mortalité (RR) KDOQI % Phosphorémie (mmol/l) +39 % +18 % Phosphorémie mmol/l Adapted from Block GA, et al. Am J Kidney Dis. 1998;31:
10 Observational data in the USA 2,5 mmol/l KDIGO GA Block et al. J Am Soc Nephrol 2004,15:2208.
11 Phosphataemia and survival in the DOPPS study <0,6 mmol > 2,2 mmol > 3 mmol KDIGO Tentori et al; AJKD 2008: 52: 519-
12 Phosphocalcic Metabolism and 1 year Survival (French cohort Photograph) Age (yr) < Gender F/M CV history < Diabetes BMI (kg/m2) < Low serum P High serum P Low serum PTH High serum PTH Low serum Ca High serum Ca Hemoglobin (g/l) < Albumin (g/l) < N = 4,937. Models were adjusted for age, sex, BMI, diabetes, history of CV disease, serum albumin, hemoglobin, and baseline serum levels of total calcium, phosphorus and PTH. Patients with recent parathyroidectomy (less than 6 months) were excluded from the analysis. D Fouque et al, WCN, Milan, 2009
13 Causes of hyperphosphataemia: Excess protein intake (> 1,2 g/kg/j) Excess phosphate intake (> 1000 mg/j) Inadequate dialysis removal : time, frequency, efficiency Inadequate phosphate binding: timing, dosage, side effects, compliance Excess active vitamin D (+ adynamic bone disease) Secondary hyperparathyroidism GA. Block et al, Am J Kidney Dis 2000,35:1226.
14 Phosphate intake is linked with protein intake Protein intake (g/kg/jour) Phosphate intake (mg) > ± ± ± ± 142 < ± 105 Rufino M, et al. Nephrol Dial Transplant. 1998;13:65 67.
15 The amount of phosphorus removal depends on clearance, frequency and treatment time. Gotch et al;blood Purif 2003, 21:51-57.
16 Achieving the old target KDOQI 60 1,13 1,78 mmol/l 50 Relative frequency (%) % 54% 29% ARNOS Rhône-Alpes, D. Fouque et al, 2005 Ph KDOQI
17 70% of dialysis patients in the USA were hyperphosphataemic in the 90s 25% Patients Above Normal Percentage of Patients 20% 15% 10% 5% 0% Serum Phosphorus (mmol/l) CMAS (1990) mean = 2.00 DMMS (1993) mean = Block GA, et al. Am J Kidney Dis. 1998;31:
18 Achieving the new target KDIGO mmol/ l 56% mmol/l Relative frequency (%) % 10 12% Ph KDIGO 2009
19 Questions What is the better day for biological sampling? 1st day of the week, mid-week? Morning, evening, nighttime? Circadian cycle and dietary intake? What is «lowering toward the normal range»? some pitfalls: Lowering phosphataemia from 3.5 to 2.5 mmol/l may seems enough Being happy with malnourish patient with phosphataemia at 1 mmol/l
20 Normal phosphataemia? Phosphataemia mmol Case n 1 Case n 2 Case n 3 1,1 1,1 1,1 Calcaemia mmol/l Albumin g/l PTH pg/ml B-ALP µg/l npcr g/kg/j Kt/V Session time 3 x 4h 3 x 4h 3 x 8 h Caco3 mg/j Alfacalcidol µg/s BMI kg/m² Age years
21 Conclusion on phosphataemia target (Tend to) normalizing phosphataemia would help (theoretically) in decreasing CV mortality (calcification), but this is not based on any data. Normalizing phosphataemia needs to: Decrease protein intake Increase phosphate binder dosage Increase dialysis (time/frequency) Increase medical cost, limited by compliance Post-dialysis hypophosphataemia (< 0.5 mmol/l) may be harmful (neuromuscular, osteomalacia)
22 NEW PTH TARGET
23

24 High turnover for PTH pg/ml

25 Low turnover for PTH < 60 pg/ml
26 PTH and «The optimal target level of PTHi in CKD is not know due to limitation of data available and the emerging consensus that those target levels may be lower than currently thought» PTHi diagnose adynamic bone disease when < 60 pg/ml and high turnover bone disease when > pg/ml Eknoyan, AJKD 2003 KDOQI
27 KDIGO target for PTH In patients with CKD stage 5D, we suggest maintaining ipth levels in the range of approximately two to nine times the upper normal limit for the assay (2C) pg/ml (Roche Elecsys ) We suggest that marked changes in PTH levels in either direction within this range prompt an initiation or change in therapy to avoid progression to levels outside of this

28 KDIGO: relationship between PTH levels and the risk for fractures

29 KDIGO: relationship between PTH levels, Bone ALP and bone turnover
30 PTHi Bone turnover relationship in the 90s KDOQI From: Q. QI, AJKD, 1995,26,4:622.
31 Relationship between coronary calcifications and low PTH and calcium carbonate Caractéristiques cliniques Score de calcification Age 41 48, p 0,001 Adaptation de Guérin, NDT,2000 Ancienneté en dialyse (mois) Ca. élé t (CaCO3) 1,35 (3,3) 1,35 (3,3) 1,5 (3,4) 1,8 (3,75) 2,18 (5,5) Tabagisme (Paquets/Année) Fibrinogène (g/l) 4 4,2 4,25 5 5,1 CRP (mg/l) 5,2 7 6, PTH (pg/ml) HyperCa (%) Ca.P (mmol2/l2) 4,4 4,54 4,57 4,14 4,64 0,001 0,001 0,01 0,001 0,001 0,047 0,034 NS
32 Low PTH level is associated with arterial calcification GM London et al: e. JASN 2004,15:1943.

33 KDIGO: bone disease according to CKD stage and treatment

34 Same as in the 21th century KDIGO Baretto et al,kidney Int 2008: 73; 771

35 Upper limits PTH reference levels are disturbed by vitamin D deficiency Non vitamin D-deficient Souberbielle, J.-C. et al. J Clin Endocrinol Metab 2001;86: Copyright 2001 The Endocrine Society

36 What is your PTH assay? KDIGO Souberbielle JC, et al;kidney Int 2006;70:
37 PTH level of 300 pg/ml can be associated with different bone turnover Calcaemia Phosph PTH 25(OH)D B ALP mmol/l mmol/l pg/ml nmol/l µg/l Mild SHPT 2,15 1, Adynamic BD 2,5 1, Severe HPT 2,
38 Case N 1 T0 3 mths 6 mths Lowering BT PTH pg/ml treatment Calcaemia mmol/l 2,36 2,45 2,5 Phosphataemia mmol/l 1,6 1,7 1,8 ALP total UI/ l Case N 2 PTH pg/ml Calcaemia mmol/l 2,5 2,45 2,29 Phosphataemia mmol/l 1,9 1,7 1,5 ALP total UI/ l
39 PTH and mortality in DOPPS < 600 Tentori, AJKD 2008,52:519 KDIGO

40 PTH and survival in the USA Kalantar-Zadeh et al; Kidney Int :
41 Impact of the PTH target in a French population ± 293 pg/ml 25 Relative frequency (%) KDOQI 30% KDIGO 50 % ARNOS Rhône-Alpes, D. Fouque et al, 2005 PTH pg/ml
42 Conclusion KDIGO PTH target is wider mainly based on bone turnover criteria (supposed) Consequences: Larger uncertain zone less affected by the assay Needs a dynamic rendition rather than based on a single value Needs of real bone marker (B-ALP) Less adynamic bone disease (increasing the mean value) Less lowering PTH therapies (calcium, calcitriol analogues, cinacalcet) More hyperparathyroidism Which consequences on bone disease, vascular calcification, survival?
43 NEW CALCIUM TARGET
44 Evolution of recommendations 2003: Total corrected calcium must be maintained within the normal range for the laboratory (EVIDENCE) preferably toward the lower end (8.4 to 9.5 mg/dl [2.10 to 2.37 mmol/l]). (OPINION) KDIGO In CKD stage 3-5D, we suggest maintaining serum calcium in the normal range (2D, very low evidence). 2009: KDOQI
45 Factors Associated with Cardiac Calcification in Young Dialysis Patients KDOQI Coronary Calcification No Calcification Factor (N=14) (N=25) P Value Ca intake from calcium binders (mg/day) 6456 ± ± Serum P (mmol/l) 2.2 ± ± Ca P (mmol 2 /L 2 ) 5.3 ± ± Age (years) 26 ± 3 15 ± 5 <0.001 Mean duration of dialysis (years) 14 ± 5 4 ± 4 <0.001 Serum calcium was not significant. 1. Adapted from Goodman WG, et al. N Engl J Med. 2000;342:
46 Total calcaemia Severe Hypocalcaemia < 1.9 mmol/l Moderate Hypocalcaemia mmol/l Normal calcaemia mmol/l Mild Hypercalcaemia mmol/l Moderate Hypercalcaemia 3 3,3 mmol/l Severe Hypercalcaemia > 3.3 mmol/l Calcium, Lancet 1998,352:306. KDIGO
47 Calcium in the body
48 Calcium references? KDOQI : no reference of ionized Ca Ionized calcium is:«time consuming and money consuming» Better using Formulae: Corrected ca= Tot Ca (mg/dl) + 0,0704 X [34 alb g/l] Corrected ca= Tot Ca + 0,8 x [40 alb]
49 KDIGO Corrected calcium? Unfortunately, recent data have shown that it offers no superiority over total calcium alone and is less specific than ionized calcium measurements. The Work Group did not recommend that corrected calcium measurements be abandoned at present. Gauci C, J Am Soc Nephrol ; 1592
50 Relationship between PTH and i-calciumi the set-point PTH (%) Set point Severe SHPT Moderate SHPT Normal subject mg/dl mmol/l Ionized calcium Adapted, with permission, from Malberti F et al. Nephrol Dial Transplant 1999;14:
51 Baseline calcaemia = set-point Malberti, F., M. Farina, et al. (1999). "The PTH calcium curve and the set point of calcium in primary and secondary hyperparathyroidism." Nephrol Dial Transplant 14(10):
52 Survival and corrected calcaemia Survival and corrected calcaemia GA Block et al, Mineral metabolism, mortality and morbidity in maintenance hemodialysis. J Am Soc Nephrol 2004,15:2208.
53 Calcaemia and survival: DOPPS study 2,15 2,5 mmol/l Tentori, AJKD 2008,52:519 KDIGO
54 KDOQI 50 Relative frequency (%) % in the target mmol/l ,5 0,8 1,0 1,3 1,5 1,8 2,0 2,2 2,5 2,7 3,0 3,2 3,5 3,7 4,0 ARNOS Rhône-Alpes, D. Fouque et al, 2005 Alb-corrected calc mmol/l
55 KDIGO Relative frequency (%) % in the target mmol/l ,3 0,5 0,8 1,0 1,2 1,4 1,7 1,9 2,1 2,4 2,6 2,8 3,0 3,3 3,5 ARNOS Rhône-Alpes, D. Fouque et al, 2005 Calc totale mmol/l
56 Conclusion We move from a narrow target for albcorrected calcaemia (2.1 to 2.37 mmol/l) to a normal range for total calcaemia with twice more patients achieving the target. Consequences? Less low dialysate calcium? Less non-calcium based phosphate binder? Less SHPT? Less cinacalcet use? More vitamin D? Bone and vascular consequences?
57 KDOQI strategy: a real pitfall T0 T3 T6 T9 PTH pg/ml Alb-corrected calcaemia Total calcaemia mmol/l Phosphataemia mmol/l Ca dialysate mmol 1, CacO3 g/day 2g g Sevelamer mg/day Cinacalcet mg/day Un-alpha µg/week
58 With the KDIGO T0 T3 PTH pg/ml Corrected 2,5 2,45 calcaemia mmol/l Total calcaemia 2,45 2,4 Phosphataemia mmol/l 1,8 1,5 Ca dialysate 1,5 1,5 CacO3 g/day Lanthanum g/d 0 1 g Cinacalcet 0 0 Un alpha 0 0 Cholecalciferol U/mths
59 MORE RECOMMENDATIONS
60 KDOQI: native vitamin D In patients with more advanced CKD (Stage 5) and in dialysis patients, it is not established that nutritional replacement with vitamin D (ergocalciferol or cholecalciferol) will be effective since the ability to generate adequate levels of 1,25(OH)2D3 is markedly reduced or is unlikely.
61 KDIGO and native vitamin D In patients with CKD stages 3 5D, we suggest that 25(OH)D (calcidiol) levels might be measured, and repeated testing determined by baseline values and therapeutic interventions (2C). We suggest that vitamin D deficiency and insufficiency be corrected using treatment strategies recommended for the general population (2C).
.")
62 nmol/l Melamed, M. L.,, et al. (2008). Arch Intern Med 168(15): 1629-
63 KDIGO and bone markers In patients with CKD stages 3 5D, we suggest that measurements of serum PTH or bone-specific alkaline phosphatase can be used to evaluate bone disease
64 Ca x P product In patients with CKD stages 3 5D, we suggest that individual values of serum calcium and phosphorus, evaluated together, be used to guide clinical practice rather than the mathematical construct of calciumphosphorus product (CaxP) (2D).
65 Biological target evolution Target Calcaemia Phosphataemia PTH Ca x P Normal range but 1,13 1, < 4,4 preferably toward mmol/l pg/ml mmol²/l² KDOQI the lower end (2,1 2,37 mmol/l ) Normal range (2,1 Toward the 2 9 time the No more 2,55 mmol/l) normal range upper limit of target KDIGO (0,8 1,45 mmol/l) the assay
66 Take home message The evidence level requirement has increased with the KDIGO, but the level of evidence remains poor. However, most of the recommendations make sense and constitute an improvement of the KDOQI, beyond the targets: The idea of dynamic rather than static interpretation Individualization rather than one size fits all A global approach not based on only one parameter To prevent rather than to cure
Secondary hyperparathyroidism in dialysis patients
 Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
Secondary hyperparathyroidism in dialysis patients ( a critical approach of pharmacological treatments) Dominique JOLY Néphrologie Hôpital NECKER, Paris DFG Finn WF. J Am Soc Nephrol. 24;15:271A. Ca ++
Renal Association Clinical Practice Guideline in Mineral and Bone Disorders in CKD
 Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
Nephron Clin Pract 2011;118(suppl 1):c145 c152 DOI: 10.1159/000328066 Received: May 24, 2010 Accepted: December 6, 2010 Published online: May 6, 2011 Renal Association Clinical Practice Guideline in Mineral
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015)
 Final Version (01/03/2015)") CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
CLINICAL PRACTICE GUIDELINE CKD-MINERAL AND BONE DISORDERS (CKD-MBD) Final Version (01/03/2015) Dr Simon Steddon, Consultant Nephrologist, Guy s and St Thomas NHS Foundation Trust, London Dr Edward Sharples,
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital
 Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
Do We Do Too Many Parathyroidectomies in Dialysis? Sagar Nigwekar MD, MMSc Massachusetts General Hospital E-mail: snigwekar@mgh.harvard.edu March 13, 2017 Disclosures statement: Consultant: Allena, Becker
2017 KDIGO Guidelines Update
 2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
2017 KDIGO Guidelines Update Clinic for Hemodialysis Clinical Center University of Sarajevo 13 th Congress of the Balkan cities Association of Nephrology, Dialysis, and Artificial Organs Transplantation
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
( ) , (Donabedian, 1980) We would not choose any treatment with poor outcomes
 , (Donabedian, 1980) We would not choose any treatment with poor outcomes") ..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
..., 2013 Amgen. 1 ? ( ), (Donabedian, 1980) We would not choose any treatment with poor outcomes 1. :, 2. ( ): 3. :.,,, 4. :, [Biomarkers Definitions Working Group, 2001]., (William M. Bennet, Nefrol
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale. Maurizio Gallieni Università degli Studi di Milano
 Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
Ipovitaminosi D e metabolismo calcio-fosforo in dialisi peritoneale Maurizio Gallieni Università degli Studi di Milano G Ital Nefrol 2018 - ISSN 1724-5990 Nutrients 2017, 9, 328 Vitamin D deficiency (
02/27/2018. Objectives. To Replace or Not to Replace: Nutritional Vitamin D in Dialysis.
 To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
To Replace or Not to Replace: Nutritional Vitamin D in Dialysis. Michael Shoemaker-Moyle, M.D. Assistant Professor of Clinical Medicine Objectives Review Vitamin D Physiology Review Current Replacement
Treatment Options for Chronic Kidney
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia The 17th Budapest Nephrology School, August 29, 2010 Session Objectives Definition
The CARI Guidelines Caring for Australasians with Renal Impairment. Serum phosphate GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Serum phosphate GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL CARE (Suggestions
TRANSPARENCY COMMITTEE OPINION. 22 July 2009
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 22 July 2009 PHOSPHOSORB 660 mg, film-coated tablet Container of 200 (CIP: 381 466-0) Applicant: FRESENIUS MEDICAL
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Contents. Authors Name: Christopher Wong: Consultant Nephrologist Anne Waddington: Renal Pharmacist Eimear Fegan : Renal Dietitian
 Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
Cheshire and Merseyside Renal Units Guidelines on the Management of Chronic Kidney Disease - Mineral Bone Disorder (adapted from Greater Manchester) Authors Name: Christopher Wong: Consultant Nephrologist
West Midlands guidelines for managing Chronic Kidney Disease related Mineral and Bone Disorders in Haemodialysis Patients
 West Midlands Renal Network West Midlands guidelines for managing Chronic Kidney Disease related Mineral and Bone Disorders in Haemodialysis Patients WMRN/Regional Bone Management Guidelines /1010/Final
West Midlands Renal Network West Midlands guidelines for managing Chronic Kidney Disease related Mineral and Bone Disorders in Haemodialysis Patients WMRN/Regional Bone Management Guidelines /1010/Final
IMPLEMENTATION OF THE CKD-MBD PRACTICE. Goce Spasovski, R. Macedonia
 IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
IMPLEMENTATION OF THE CKD-MBD GUIDELINES Introduction INTO CLINICAL to Renagel PRACTICE Goce Spasovski, R. Macedonia Antalya, Turkey, September 16 2012 Session Objectives Guidelines needs and controversy
Cinacalcet treatment in advanced CKD - is it justified?
 Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Cinacalcet treatment in advanced CKD - is it justified? Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia TSN Congress October 21, 2017, Antalya Session Objectives From ROD to
Sensipar (cinacalcet)
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients
 Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
Ca, Phos and Vitamin D Metabolism in Pre-Dialysis Patients A. WADGYMAR, MD Credit Valley Hospital, Mississauga, Ontario, Canada. June 1, 2007 1 Case: 22 y/o referred to Renal Clinic Case: A.M. 29 y/o Man
OPEN. Masahiro Yoshikawa 1,2, Osamu Takase 1,2, Taro Tsujimura
 www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
www.nature.com/scientificreports Received: 26 September 2017 Accepted: 19 March 2018 Published: xx xx xxxx OPEN Long-term effects of low calcium dialysates on the serum calcium levels during maintenance
Treatment Options for Chronic Kidney. Goce Spasovski, R. Macedonia
 Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Treatment Options for Chronic Kidney Disease: Metabolic Introduction Bone Disease to Renagel Goce Spasovski, R. Macedonia Budapest, August 29, 2011 Session Objectives Definition of the problem of CKD-MBD
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis
 Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Vascular calcification in stage 5 Chronic Kidney Disease patients on dialysis Seoung Woo Lee Div. Of Nephrology and Hypertension, Dept. of Internal Medicine, Inha Unv. College of Medicine, Inchon, Korea
Therapeutic golas in the treatment of CKD-MBD
 Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Therapeutic golas in the treatment of CKD-MBD Hemodialysis clinic Clinical University Center Sarajevo Bantao, 04-08.10.2017, Sarajevo Abbvie Satellite symposium 06.10.2017 Chronic Kidney Disease Mineral
Management of CKD. Goce Spasovski, R. Macedonia
 Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Management of CKD complications Introduction Bone disease to Renagel Goce Spasovski, R. Macedonia Istanbul, June 4, 2011 Session Objectives - Mineral and Bone Disorders (MBD) Bone disease a part of CKD
Guidelines and new evidence on CKD - MBD treatment
 Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
Guidelines and new evidence on CKD - MBD treatment Goce Spasovski ERBP Advisory Board member University of Skopje, R. Macedonia ERA-EDTA CME course IV Congress of Nephrology of B&H, April 25, 2015, Sarajevo,
CKD-MBD CKD mineral bone disorder
 CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
CKD Renal bone disease Dr Mike Stone University Hospital Llandough Affects 5 10 % of population Increasingly common Ageing, diabetes, undetected hypertension Associated with: Cardiovascular disease Premature
Month/Year of Review: September 2012 Date of Last Review: September 2010
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016
 Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Ramzi Vareldzis, MD Avanelle Jack, MD Dept of Internal Medicine Section of Nephrology and Hypertension LSU Health New Orleans September 13, 2016 1 MBD + CKD in Elderly patients Our focus for today: CKD
Clinical Guideline Bone chemistry management in adult renal patients on dialysis
 Clinical Guideline Bone chemistry management in adult renal patients on dialysis This guidance covers how to: Maintain serum phosphate 0.8 to 1.7mmol/L 1 Maintain serum corrected calcium 2.1 to 2.5mmol/L
Clinical Guideline Bone chemistry management in adult renal patients on dialysis This guidance covers how to: Maintain serum phosphate 0.8 to 1.7mmol/L 1 Maintain serum corrected calcium 2.1 to 2.5mmol/L
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD
 The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
The Calcium Conundrum: When, What and How to Give Calcium in Pediatric CKD/ESRD Jess Tower MS RD LD 3/18/19 Children s Mercy Hospital jdtower@cmh.edu 816 460 1067 Disclosures Nothing to disclose 1 How
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience
 Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Incorporating K/DOQI Using a Novel Algorithm Approach: Regina Qu Appelle s Experience Michael Chan, Renal Dietitian Regina Qu Appelle Health Region BC Nephrology Days There is a strong association among
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Nutrition and Renal Disease Update
 Nutrition and Renal Disease Update Denis FOUQUE Department of Nephrology Centre de Recherche en Nutrition Humaine University Claude Bernard Lyon - France What have we learned? 1. Chronic kidney disease:
Nutrition and Renal Disease Update Denis FOUQUE Department of Nephrology Centre de Recherche en Nutrition Humaine University Claude Bernard Lyon - France What have we learned? 1. Chronic kidney disease:
Cardiovascular (CV) disease is the main cause of death
 disease is the main cause of death") www.kidney-international.org Low parathyroid hormone status induced by high dialysate calcium is an independent risk factor for cardiovascular death in hemodialysis patients OPEN Emilie Merle 1, Hubert
www.kidney-international.org Low parathyroid hormone status induced by high dialysate calcium is an independent risk factor for cardiovascular death in hemodialysis patients OPEN Emilie Merle 1, Hubert
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL
 PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
PREVALENCE AND PATTERNS OF HYPERPARATHYROIDISM AND MINERAL BONE DISEASE IN PATIENTS WITH CHRONIC KIDNEY DISEASE AT KENYATTA NATIONAL HOSPITAL DR. ANNE MUGERA The Problem Chronic Kidney disease is a worldwide
Outline. The Role of Vitamin D in CKD. Essential Role of Vitamin D. Mechanism of Action of Vit D. Mechanism of Action of Vit D 7/16/2010
 Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Outline The Role of Vitamin D in CKD Priscilla How, Pharm.D., BCPS Assistant Professor National University of Singapore Principal Clinical Pharmacist National University Hospital (Pharmacy and Nephrology,
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416)
") Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Nuove terapie in ambito Nefrologico: Etelcalcetide (AMG-416) Antonio Bellasi, MD, PhD U.O.C. Nefrologia & Dialisi ASST-Lariana, Ospedale S. Anna, Como, Italy Improvement of mineral and bone metabolism
Ying Liu, 1 Wen-Chin Lee, 2 Ben-Chung Cheng, 2 Lung-Chih Li, 2 Chih-Hsiung Lee, 2 Wen-Xiu Chang, 1 and Jin-Bor Chen 2. 1.
 BioMed Research International Volume 2016, Article ID 1523124, 7 pages http://dx.doi.org/10.1155/2016/1523124 Research Article Association between the Achievement of Target Range CKD-MBD Markers and Mortality
BioMed Research International Volume 2016, Article ID 1523124, 7 pages http://dx.doi.org/10.1155/2016/1523124 Research Article Association between the Achievement of Target Range CKD-MBD Markers and Mortality
The CARI Guidelines Caring for Australasians with Renal Impairment. Biochemical Targets. Calcium GUIDELINES
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Biochemical Targets CARMEL HAWLEY (Woolloongabba, Queensland) GRAHAME ELDER (Westmead, New South Wales) Calcium GUIDELINES
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Biochemical Targets CARMEL HAWLEY (Woolloongabba, Queensland) GRAHAME ELDER (Westmead, New South Wales) Calcium GUIDELINES
Month/Year of Review: May 2014 Date of Last Review: September New Drug Evaluation: Sucrofferic Oxyhydroxide (Velphoro )
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
New Medicines Profile. December 2013 Issue No. 13/04. Colestilan
 New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
New Medicines Profile December 2013 Issue. 13/04 Concise evaluated information to support the managed entry of new medicines in the NHS Summary (BindRen ) is an oral, non-absorbed, non-calcium, nonmetallic
HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE ON MAINTENANCE DIALYSIS THERAPY
 UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
UK RENAL PHARMACY GROUP SUBMISSION TO THE NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE on CINACALCET HYDROCHLORIDE FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS WITH END-STAGE RENAL DISEASE
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism
 CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
CKD-MBD in 2017 What s new? Focus on Sec Hyperparathyroidism Pieter Evenepoel Nephrology, Dialysis, and Transplantation University Hospitals Leuven April 2017, FMC Herbeumont Disclosures Research support:
Chronic Kidney Disease Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol
 Dietetic Management Protocol") This is an official Northern Trust policy and should not be edited in any way Chronic Kidney Disease Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol Reference Number: NHSCT/12/553 Target
This is an official Northern Trust policy and should not be edited in any way Chronic Kidney Disease Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol Reference Number: NHSCT/12/553 Target
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism
 The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
The Journal of International Medical Research 2011; 39: 978 987 Total Parathyroidectomy with Forearm Autotransplantation as the Treatment of Choice for Secondary Hyperparathyroidism J NARANDA 1,2, R EKART
Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis
 ORIGINAL ARTICLE Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis Masaki Ohya 1, Haruhisa Otani 2,KeigoKimura 3, Yasushi Saika 4, Ryoichi Fujii 4, Susumu
ORIGINAL ARTICLE Improved Assessment of Aortic Calcification in Japanese Patients Undergoing Maintenance Hemodialysis Masaki Ohya 1, Haruhisa Otani 2,KeigoKimura 3, Yasushi Saika 4, Ryoichi Fujii 4, Susumu
Chapter 5: Evaluation and treatment of kidney transplant bone disease Kidney International (2009) 76 (Suppl 113), S100 S110; doi: /ki.2009.
 76 (Suppl 113), S100 S110; doi: /ki.2009.") http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
http://www.kidney-international.org & 2009 KDIGO Chapter 5: Evaluation and treatment of kidney transplant bone disease ; doi:10.1038/ki.2009.193 Grade for strength of recommendation a Strength Wording
La relation dialyse et nutrition
 Nutrition en dialyse : controverses La relation dialyse et nutrition Charles Chazot, MD NephroCare Tassin-Charcot Sainte Foy Les Lyon, France HEMO study lessons (1) Dose Body weight flux Rocco, Kidney
Nutrition en dialyse : controverses La relation dialyse et nutrition Charles Chazot, MD NephroCare Tassin-Charcot Sainte Foy Les Lyon, France HEMO study lessons (1) Dose Body weight flux Rocco, Kidney
Effects of Diabetes Mellitus, Age, and Duration of Dialysis on Parathormone in Chronic Hemodialysis Patients. Hamid Nasri 1, Soleiman Kheiri 2
 Saudi J Kidney Dis Transplant 2008;19(4):608-613 2008 Saudi Center for Organ Transplantation Saudi Journal of Kidney Diseases and Transplantation Original Article Effects of Diabetes Mellitus, Age, and
Saudi J Kidney Dis Transplant 2008;19(4):608-613 2008 Saudi Center for Organ Transplantation Saudi Journal of Kidney Diseases and Transplantation Original Article Effects of Diabetes Mellitus, Age, and
chapter 1 & 2009 KDIGO
 http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
http://www.kidney-international.org chapter 1 & 2009 DIGO Chapter 1: Introduction and definition of CD MBD and the development of the guideline statements idney International (2009) 76 (Suppl 113), S3
Bone Disorders in CKD
 Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Osteoporosis in Dialysis Patients Challenges in Management David M. Klachko MD FACP Professor Emeritus of Medicine University of Missouri-Columbia Bone Disorders in CKD PTH-mediated high-turnover (osteitis
Sensipar. Sensipar (cinacalcet) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.46 Subject: Sensipar Page: 1 of 5 Last Review Date: June 22, 2018 Sensipar Description Sensipar (cinacalcet)
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet:
 Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Clinical benefits of an adherence monitoring program in the management of secondary hyperparathyroidism with cinacalcet: Results of a prospective randomized controlled study Forni Valentina¹, Pruijm Menno¹,
Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients with secondary hyperparathyroidism
 Ho et al. BMC Nephrology (2017) 18:12 DOI 10.1186/s12882-016-0421-5 RESEARCH ARTICLE Open Access Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients
Ho et al. BMC Nephrology (2017) 18:12 DOI 10.1186/s12882-016-0421-5 RESEARCH ARTICLE Open Access Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients
Prevalence of malnutrition in dialysis
 ESPEN Congress Cannes 2003 Organised by the Israel Society for Clinical Nutrition Education and Clinical Practice Programme Session: Nutrition and the Kidney Malnutrition and Haemodialysis Doctor Noël
ESPEN Congress Cannes 2003 Organised by the Israel Society for Clinical Nutrition Education and Clinical Practice Programme Session: Nutrition and the Kidney Malnutrition and Haemodialysis Doctor Noël
Chapter 3.1: Diagnosis of CKD MBD: biochemical abnormalities Kidney International (2009) 76 (Suppl 113), S22 S49. doi: /ki.2009.
 76 (Suppl 113), S22 S49. doi: /ki.2009.") chapter 3.1 http://www.kidney-international.org & 2009 KDIGO Chapter 3.1: Diagnosis of CKD MBD: biochemical abnormalities. doi:10.1038/ki.2009.191 Grade for strength of recommendation a Strength Wording
chapter 3.1 http://www.kidney-international.org & 2009 KDIGO Chapter 3.1: Diagnosis of CKD MBD: biochemical abnormalities. doi:10.1038/ki.2009.191 Grade for strength of recommendation a Strength Wording
Drugs for the treatment of secondary hyperparathyroidism and hyperphosphataemia
 NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
NSW Therapeutic Advisory Group Level 5, 376 Victoria Street PO Box 766 Darlinghurst NSW 2010 Phone: 61 2 8382 2852 Fax: 61 2 8382 3529 Email: nswtag@stvincents.com.au www.nswtag.org.au Drugs for the treatment
Level 1 Strong We recommendyshould A High Moderate Level 2 Weak We suggestymight C Low Very low. K Hyperphosphatemia has been associated with poor
 chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
chapter 4.1 http://www.kidney-international.org & 2009 KDIGO Chapter 4.1: Treatment of CKD MBD targeted at lowering high serum phosphorus and maintaining serum calcium ; doi:10.1038/ki.2009.192 Grade for
Velphoro (sucroferric oxyhydroxide)
") STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
STRENGTH DOSAGE FORM ROUTE GPID 500mg chewable tablet oral 36003 MANUFACTURER Fresenius Medical Care North America INDICATION(S) For the control of serum phosphorus levels in patients with chronic kidney
BONE AND MINERAL METABOLISM in the PD PATIENT
 BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
BONE AND MINERAL METABOLISM in the PD PATIENT John Burkart, MD Professor of Medicine/Nephrology Wake Forest University Baptist Medical Center Chief Medical Officer Health Systems Management Maria V. DeVita,
Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study
 Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study Fernstrom, Anders; Giaever, Jan; Granroth, Barbara; Hylander,
Achievement of recommended treatment targets for bone and mineral metabolism in haemodialysis patients using paricalcitol: An observational study Fernstrom, Anders; Giaever, Jan; Granroth, Barbara; Hylander,
Should cinacalcet be used in patients who are not on dialysis?
 Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
Should cinacalcet be used in patients who are not on dialysis? Jorge B Cannata-Andía and José Luis Fernández-Martín Affiliations: Bone and Mineral Research Unit. Hospital Universitario Central de Asturias.
NDT Advance Access published February 3, 2007
 NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
NDT Advance Access published February 3, 2007 Nephrol Dial Transplant (2007) 1 of 6 doi:10.1093/ndt/gfl840 Original Article Implementation of K/DOQI Clinical Practice Guidelines for Bone Metabolism and
Calcium x phosphate product
 Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Calcium x phosphate product GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL
Date written: August 2005 Final submission: October 2005 Author: Carmel Hawley Calcium x phosphate product GUIDELINES No recommendations possible based on Level I or II evidence SUGGESTIONS FOR CLINICAL
Clinical practice recommendations for treatment with active vitamin D analogues in children with chronic kidney disease Stages 2 5 and on dialysis
 Nephrol Dial Transplant (2017) 32: 1114 1127 doi: 10.1093/ndt/gfx080 Advance Access publication 1 June 2017 Clinical practice recommendations for treatment with active vitamin D analogues in children with
Nephrol Dial Transplant (2017) 32: 1114 1127 doi: 10.1093/ndt/gfx080 Advance Access publication 1 June 2017 Clinical practice recommendations for treatment with active vitamin D analogues in children with
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi
 Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
Attivazione selettiva dei VDR nella CKD-MBD: dalla conservativa alla dialisi Mario Cozzolino, MD, PhD, FERA Dipartimento di Scienze della Salute Università di Milano UO Nefrologia e Dialisi Laboratorio
TO EAT OR NOT TO EAT DURING HEMODIALYSIS TREATMENT?
 TO EAT OR NOT TO EAT DURING HEMODIALYSIS TREATMENT? Rana G. Rizk, PhD, MPH, LD Maastricht University, The Netherlands November, 2017 Learning objectives Review the evidence behind benefits and concerns
TO EAT OR NOT TO EAT DURING HEMODIALYSIS TREATMENT? Rana G. Rizk, PhD, MPH, LD Maastricht University, The Netherlands November, 2017 Learning objectives Review the evidence behind benefits and concerns
The Parsabiv Beginner s Book
 The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
The Parsabiv Beginner s Book A quick guide to help you learn about your treatment with Parsabiv and what to expect Indication Parsabiv (etelcalcetide) is indicated for the treatment of secondary hyperparathyroidism
Nottingham Renal and Transplant Unit
 Nottingham Renal and Transplant Unit Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out
Nottingham Renal and Transplant Unit Full Title of Guideline: Author (include email and role): Division & Speciality: Scope (Target audience, state if Trust wide): Review date (when this version goes out
Key words: Vitamin D analogues, alfacalcidol, calcitriol, secondary hyperparathyroidism, renal dialysis
 Oral cal ORAL CALCITRIOL VERSUS ORAL ALFACALCIDOL FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS RECEIVING HEMODIALYSIS: A RANDOMIZED, CROSSOVER TR IAL Samantha Moe 1, Lori D Wazny 2, Janet
Oral cal ORAL CALCITRIOL VERSUS ORAL ALFACALCIDOL FOR THE TREATMENT OF SECONDARY HYPERPARATHYROIDISM IN PATIENTS RECEIVING HEMODIALYSIS: A RANDOMIZED, CROSSOVER TR IAL Samantha Moe 1, Lori D Wazny 2, Janet
Clinical practice recommendations for treatment with active vitamin D analogues in children with chronic kidney disease stages 2 5 and on dialysis
 Nephrol Dial Transplant (2017) 1 14 doi: 10.1093/ndt/gfx080 Special Report Clinical practice recommendations for treatment with active vitamin D analogues in children with chronic kidney disease stages
Nephrol Dial Transplant (2017) 1 14 doi: 10.1093/ndt/gfx080 Special Report Clinical practice recommendations for treatment with active vitamin D analogues in children with chronic kidney disease stages
KDOQI COMMENTARY VOL 55, NO 5, MAY 2010
 VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
VOL 55, NO 5, MAY 2010 KDOQI COMMENTARY KDOQI US Commentary on the 2009 KDIGO Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of CKD Mineral and Bone Disorder (CKD-MBD) Katrin
What Are the Targets in CKD-MBD?
 Knowledge Exchange 2016 Paris, France, September 30, 2016 Date of preparation: Nov 2016 Item job code: INTSP/C-ANPROM/FOS/16/0025 Cristina Ortiz Jorge B Cannata-Andía Bone and Mineral Research Unit Hospital
Knowledge Exchange 2016 Paris, France, September 30, 2016 Date of preparation: Nov 2016 Item job code: INTSP/C-ANPROM/FOS/16/0025 Cristina Ortiz Jorge B Cannata-Andía Bone and Mineral Research Unit Hospital
Metabolic Bone Disease (Past, Present and Future Challenges in the Management)
") Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Metabolic Bone Disease 871 151 Metabolic Bone Disease (Past, Present and Future Challenges in the Management) SNA RIZVI INTRODUCTION The past 40 years have seen some important historical events leading
Opinion 23 April 2014
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 23 April 2014 MIMPARA 30 mg, film-coated tablet B/14 (CIP: 365 154 8) B/28 (CIP: 365 155 4) B/30 (CIP: 365 157 7)
TABLE OF CONTENTS T-1. A-1 Acronyms and Abbreviations. S-1 Stages of Chronic Kidney Disease (CKD)
") A-1 Acronyms and Abbreviations TABLE OF CONTENTS S-1 Stages of Chronic Kidney Disease (CKD) Chapter 1: Nutrition Assessment Charts, Tables and Formulas 1-2 Practical Steps to Nutrition Assessment Adult
A-1 Acronyms and Abbreviations TABLE OF CONTENTS S-1 Stages of Chronic Kidney Disease (CKD) Chapter 1: Nutrition Assessment Charts, Tables and Formulas 1-2 Practical Steps to Nutrition Assessment Adult
End stage renal disease and Protein Energy wasting
 End stage renal disease and Protein Energy wasting Dr Goh Heong Keong MBBS,MRCP(UK) www.passpaces.com/kidney.htm Introduction Chronic kidney disease- increasing health burden in many countries. The estimated
End stage renal disease and Protein Energy wasting Dr Goh Heong Keong MBBS,MRCP(UK) www.passpaces.com/kidney.htm Introduction Chronic kidney disease- increasing health burden in many countries. The estimated
Calcium Management for Patients Receiving Extended Duration Hemodialysis
 Calcium Management for Patients Receiving Extended Duration Hemodialysis Created November 2017; Updated March 2018 Approved by the BCPRA Home Hemodialysis Committee Table of Contents 1.0 Practice Standard...1
Calcium Management for Patients Receiving Extended Duration Hemodialysis Created November 2017; Updated March 2018 Approved by the BCPRA Home Hemodialysis Committee Table of Contents 1.0 Practice Standard...1
Malnutrition and Role of Nutrition in BMD:CKD
 Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Malnutrition and Role of Nutrition in BMD:CKD PNDS Continuing Nutrition Education Seminar Saturday, 30 th November 2013 Fayza Khan MSC (Foods and Nutrition) R.D President,PNDS Outline Objective Malnutrition
Management of mineral and bone disorders in renal transplant recipients
 Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Nephrology 22, Suppl. 2 (2017) 65 69 Management of mineral and bone disorders in renal transplant recipients MATTHEW J DAMASIEWICZ 1,3 and PETER R EBELING 2,3,4 Departments of 1 Nephrology, and 2 Endocrinology,
Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD
pth: ein neuer Marker für CKD-MBD") Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Biomarker der kardio-renalen Achse Mannheim, 20. Januar 2017 Nicht-oxidiertes (nox-)pth: ein neuer Marker für CKD-MBD Prof. Dr. med. Thomas Bernd Dschietzig Immundiagnostik AG, Bensheim Med. Klinik m.
Pediatric Nutrition and Kidney Disease
 Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
Pediatric Nutrition and Kidney Disease Loai Eid, MD, MSHS, FAAP Consultant Pediatric Nephrologist Pediatric Nephrology & Hypertension Division Chief Dubai Hospital - DHA 26 th October, 2017 Objectives
Effects of Lowering Dialysate Calcium Concentration on Mineral Metabolism and Hemodynamic Parameters in Hemodialysis Patients
 DIALYSIS Effects of Lowering Dialysate Calcium Concentration on Mineral Metabolism and Hemodynamic Parameters in Hemodialysis Patients Ahmed Alayoud, 1 Driss El Kabbaj, 2 Mohammed Benyahia, 2 Mohammed
DIALYSIS Effects of Lowering Dialysate Calcium Concentration on Mineral Metabolism and Hemodynamic Parameters in Hemodialysis Patients Ahmed Alayoud, 1 Driss El Kabbaj, 2 Mohammed Benyahia, 2 Mohammed
ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world
 ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world Nutrition in Kidney Disease: How to Apply Guidelines to Clinical Practice? T. Alp
ISN Mission: Advancing the diagnosis, treatment and prevention of kidney diseases in the developing and developed world Nutrition in Kidney Disease: How to Apply Guidelines to Clinical Practice? T. Alp
Original Article. Introduction
 Nephrol Dial Transplant (2006) 21: 1663 1668 doi:10.1093/ndt/gfl006 Advance Access publication 6 February 2006 Original Article Application of NKF-K/DOQI Clinical Practice Guidelines for Bone Metabolism
Nephrol Dial Transplant (2006) 21: 1663 1668 doi:10.1093/ndt/gfl006 Advance Access publication 6 February 2006 Original Article Application of NKF-K/DOQI Clinical Practice Guidelines for Bone Metabolism
Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol
 Dietetic Management Protocol") Nutrition and Dietetic Service Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol Authors Hilary Mathieson, Renal Dietitian Paul McKeveney, Consultant Nephrologist
Nutrition and Dietetic Service Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Dietetic Management Protocol Authors Hilary Mathieson, Renal Dietitian Paul McKeveney, Consultant Nephrologist
Clinical Policy: Cinacalcet (Sensipar) Reference Number: CP.PHAR.61 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.61 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Sensipar) Reference Number: CP.PHAR.61 Effective Date: 05.01.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Sensipar) Reference Number: CP.PHAR.61 Effective Date: 05.01.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
CG1339. Version: Renal Services Group. Approving forum (QIPS or equivalent):
:") University Hospitals Coventry & Warwickshire NHS Trust Clinical Guideline (full) CHRONIC KIDNEY DISEASE (CKD) NUTRITIONAL RECOMMENDATIONS FOR PERITONEAL DIALYSIS E-Library Reference CG1339 Version: Approving
University Hospitals Coventry & Warwickshire NHS Trust Clinical Guideline (full) CHRONIC KIDNEY DISEASE (CKD) NUTRITIONAL RECOMMENDATIONS FOR PERITONEAL DIALYSIS E-Library Reference CG1339 Version: Approving
Normal kidneys filter large amounts of organic
 ORIGINAL ARTICLE - NEPHROLOGY Effect Of Lanthanum Carbonate vs Calcium Acetate As A Phosphate Binder In Stage 3-4 CKD- Treat To Goal Study K.S. Sajeev Kumar (1), M K Mohandas (1), Ramdas Pisharody (1),
ORIGINAL ARTICLE - NEPHROLOGY Effect Of Lanthanum Carbonate vs Calcium Acetate As A Phosphate Binder In Stage 3-4 CKD- Treat To Goal Study K.S. Sajeev Kumar (1), M K Mohandas (1), Ramdas Pisharody (1),
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment
 Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Secondary hyperparathyroidism an Update on Pathophysiology and Treatment Klaus Olgaard Copenhagen Budapest Nephrology School August 2007 HPT IN CRF Renal mass Ca 2+ 1,25(OH) 2 D 3 CaR Hyperparathyroidism
Ying-Ping Sun, Wen-Jun Yang, Su-Hua Li, Yuan-yuan Han, and Jian Liu
 Hindawi BioMed Research International Volume 2017, Article ID 2516934, 5 pages https://doi.org/10.1155/2017/2516934 Research Article Clinical Epidemiology of Mineral Bone Disorder Markers in Prevalent
Hindawi BioMed Research International Volume 2017, Article ID 2516934, 5 pages https://doi.org/10.1155/2017/2516934 Research Article Clinical Epidemiology of Mineral Bone Disorder Markers in Prevalent
Pediatric CKD-MBD: pathophysiology and management
 Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Pediatric CKD-MBD: pathophysiology and management Justine Bacchetta, MD, PhD Reference Center for Rare Renal Diseases Reference Center for Rare Diseases of Calcium and Phosphate Bron, France Overview of
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls
 O. Mehls") Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
Actual Problems in Chronic Kidney Disease - Mineral and Bone Disorder (CKD MBD) O. Mehls Division of Pediatric Nephrology University Hospital for Children and Adolescents Heidelberg, Germany Definition
Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis patients
 original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
original article http://www.kidney-international.org & 2007 International Society of Nephrology Cost of applying the K/DOQI guidelines for bone metabolism and disease to a cohort of chronic hemodialysis
Use of magnesium as a drug in chronic kidney disease
 Clin Kidney J (2012) 5[Suppl 1]: i62 i70 doi: 10.1093/ndtplus/sfr168 Use of magnesium as a drug in chronic kidney disease Alastair J. Hutchison 1 and Martin Wilkie 2 1 University of Manchester and Manchester
Clin Kidney J (2012) 5[Suppl 1]: i62 i70 doi: 10.1093/ndtplus/sfr168 Use of magnesium as a drug in chronic kidney disease Alastair J. Hutchison 1 and Martin Wilkie 2 1 University of Manchester and Manchester
Hemodialysis: slightly beyond basics Dialysate calcium and magnesium concentrations
 Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
Dialysate calcium and magnesium concentrations Stefan Farese Department of Nephrology Bürgerspital Solothurn 04.12.2013 Dialysate calcium and magnesium concentrations Do we know the optimal concentrations?
The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure
 Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
Nephrol Dial Transplant (2002) 17: 340 345 The impact of improved phosphorus control: use of sevelamer hydrochloride in patients with chronic renal failure Naseem Amin Genzyme Corporation, Cambridge, MA,
International Journal of PharmTech Research CODEN (USA): IJPRIF, ISSN: Vol.7, No.4, pp ,
: IJPRIF, ISSN: Vol.7, No.4, pp ,") International Journal of PharmTech Research CODEN (USA): IJPRIF, ISSN: 0974-4304 Vol.7, No.4, pp 560-565, 2014-2015 Comparison of Calcium, Phosphate and Intact Parathyroid Hormone Levels Pre- and Post-Parathyroidectomy
International Journal of PharmTech Research CODEN (USA): IJPRIF, ISSN: 0974-4304 Vol.7, No.4, pp 560-565, 2014-2015 Comparison of Calcium, Phosphate and Intact Parathyroid Hormone Levels Pre- and Post-Parathyroidectomy
Metabolic Bone Disease Related to Chronic Kidney Disease
 Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab
Metabolic Bone Disease Related to Chronic Kidney Disease Deborah Sellmeyer, MD Director, Johns Hopkins Metabolic Bone Center Dept of Medicine, Division of Endocrinology Disclosure DSMB member for denosumab