Acute and Chronic Pancreatitis
|
|
|
- Chrystal Adams
- 6 years ago
- Views:
Transcription



1 Acute and Chronic Pancreatitis Diagnosis of Acute Pancreatitis Two of the following three features: Darwin L. Conwell, MD,MS Associate Director BWH Center for Pancreatic Disease Brigham and Women s Hospital Harvard Medical School Characteristic abdominal pain Amylase and/or lipase > 3 times upper limit of normal CT scan showing characteristic findings of AP No Disclosures Acute Pancreatitis: Pathophysiology Acute Pancreatitis Clinical Presentation Epigastric pain, nausea, vomiting Diagnosis Clinical evaluation Serology (amylase,lipase, LFTs) Imaging ULTRASOUND (early), CT (later) Prognosis Ranson criteria < 48 h APACHE II > 48 h BISAP Score BUN Trajectory Acute Pancreatitis: Differential Diagnosis Acute Pancreatitis: Red Flags Mesenteric ischemia Perforated gastric or duodenal ulcer Biliary colic Dissecting aortic aneurysm Intestinal obstruction Inferior wall myocardial infarction



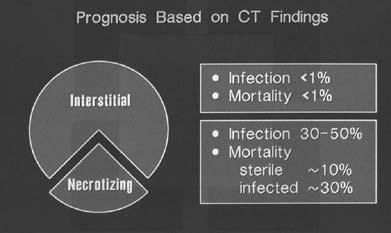
2 Acute Pancreatitis: Ranson Criteria Acute Pancreatitis: Mortality Acute Pancreatitis: Etiology Acute Pancreatitis Reasonable attempts etiology Affecting acute management Historical clues Alcohol, cholecystectomy, medications, weight loss, age Blood tests Abdominal ultrasound Contrast enhanced CT MRI / MRCP Acute Pancreatitis: CT Scan Definitions Acute Pancreatitis: CT Scan Interstitial Pancreatitis Focal or diffuse enlargement of the pancreas with enhancement of the parenchyma in response to IV contrast Blood supply maintained Necrotizing Pancreatitis Diffuse or focal areas of nonviable pancreatic parenchyma Blood supply lost



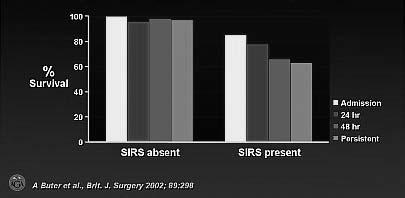
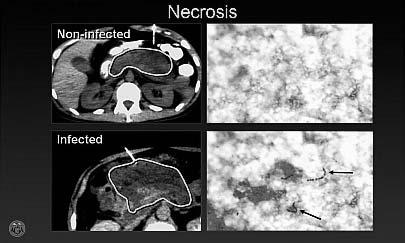
3 Acute Pancreatitis: Systemic effects Acute Pancreatitis: Systemic effects Acute Pancreatitis: Organ Failure Acute Pancreatitis: SIRS and Survival Acute Pancreatitis: CT implications Acute Pancreatitis: CT Guided Percutaneous Aspiration
4 Acute Pancreatitis Treatment Mild: Supportive care, IVFs, analgesics Severe: CT Scan, Necrosis vs. Interstitial Aggressive hydration, pain management Percutaneous aspiration / gram stain Surgical debridement Antibiotics Nutrition support Gallstones Emergent ERCP Case 1: Acute Pancreatitis On Hospital Day 3: 65 year old with persistent abd pain, fever, nausea, vomiting Exam: febrile 101.5, stable vital signs, tenderness, flank echymosis, rebound and absent bowel sounds Labs: Serology amylase lipase >2,000 Liver chemistries normal Imaging: Ultrasound: Normal gallbladder, bile ducts and pancreas head CT scan: edematous pancreas with 30% non-enhanced area Complications ARDS, ARF, SIRS Pseudocyst (symptomatic), abscess (E coli) Should we start prophylactic antibiotics? Acute Pancreatitis: Pharmacologic Issues Antimicrobial Use Prophylactic Antibiotics: Meta-analysis Infection Feeding Enteral versus parenteral nutrition Mortality Hughes S, et al. Gastroenterol Clin N Am. 2007;36: Pederzoli P, et al. Surg Gynecol Obstet. 1993;176: Bai Yu, et al. Am J Gastroenterol 2008;103: Prophylactic Antibiotics: Meta-analysis 329 patients 6 RCTs No reduction in infected necrosis No reduction in mortality No reduction in nonpancreatic infections No reduction in surgical intervention No reduction in hospital stay Mazaki, et al. BJS 2006;93: Case 1: Acute Pancreatitis On Hospital Day 3: 65 year old with persistent abd pain, fever, nausea, vomiting Exam: febrile 101.5, stable vital signs, tenderness, flank echymosis, rebound and absent bowel sounds Labs: Serology amylase lipase >2,000 Liver chemistries normal Imaging: Ultrasound: Normal gallbladder, bile ducts and pancreas head CT scan: edematous pancreas with 30% non-enhanced area Should we start prophylactic antibiotics? NO


5 Case 1: Acute Pancreatitis On Hospital Day 5: 65 year old with persistent abd pain, fever, nausea, vomiting Exam: febrile 101.5, stable vital signs, tenderness, flank echymosis, rebound and absent bowel sounds Labs: Serology amylase lipase >2,000 Liver chemistries normal Imaging: Ultrasound: Normal gallbladder, bile ducts and pancreas head CT scan: edematous pancreas with 30% non-enhanced area Should we feed patient? If so, what route delivery? Acute Pancreatitis: Nutrition Activation of intracellular proteolytic enzymes Food further stimulates production of trypsin Cornerstone of AP mgmt: pancreatic rest Long-term resting fasting the pancreas led to: High rates of body nitrogen and protein loss Increased mortality O Keefe SJ, et al. Gastroenterol Clin N Am. 2007(36): Acute Pancreatitis: Nutrition to Improve Outcomes 1) Tissue repair and recovery Meta-analysis: Nutritional Support and Infection Hypermetabolic and catabolic disease state Necrotizing disease: accelerated amino acid losses 2) Modulates inflammatory response Partially generated within the gut lumen and mucosa Prevention of intestinal ischemia Prevention of luminal stasis and bacterial overgrowth O Keefe SJ, et al. Gastroenterol Clin N Am. 2007(36): Sitzmann J, et al. Surg Gynecol Obstet. 1989;168: Marik PE, Zaloga GP. Br Med J. 2004;328(7453): Meta-analysis: Endpoints Case 1: Acute Pancreatitis On Hospital Day 5: 65 year old with persistent abd pain, fever, nausea, vomiting Exam: febrile 100.5, stable vital signs, tenderness, flank echymosis, rebound and absent bowel sounds Labs: Serology amylase lipase >2,000 Liver chemistries normal Imaging: Ultrasound: Normal gallbladder, bile ducts and pancreas head CT scan: edematous pancreas with 30% non-enhanced area Additional: Reduced hospital stay in enteral feeding groups (mean reduction 2.9days, p<0.001) Should we feed patient? YES If so, what route delivery? ENTERAL, jejunal preferred Marik PE, Zaloga GP. Br Med J. 2004;328(7453):


6 Drug-Induced Pancreatitis Pancreatic Necrosis (confirmed by CT scan) High suspicion of infected necrosis Obtain CT-guided FNA + Gram Stain (usually after 7-10 days) Negative culture Positive culture May repeat FNA q5-7 days if clinically indicated Clinically stable Targeted antimicrobial therapy Clinically unstable Prompt surgical debridement vs. delayed surgical or endoscopic debridement vs. no debridement Prompt surgical, percutaneous, or endoscopic debridement Badalov N, et al. Clin Gastroenterol Hepatol. 2007;5(6): Berzin, et al. Gastroenterol Clin N Am. 2006,35: Medical History 1700 s Chronic Pancreatitis: Overview 1788 Cawley reported a free living young man who died of emaciation and diabetes and whose postmortem examination revealed multiple pancreatic calculi Progressive, irreversible damage Exocrine and endocrine cells Exocrine insufficiency steatorrhea Endocrine insufficiency diabetes Incidence 3.5 to 10 per 100,000 population Marks IN, Bank S., Bockus Gastroenterology. 4th ed Pancreatic Steatorrhea Chronic Pancreatitis AGA, Gastroenterology Teaching Project A. Computed tomography B. Endoscopic retrograde pancreatography C. Endoscopic ultrasound D. Histology

7 TIGAR-O Toxic-metabolic Alcohol Tobacco Hypercalcemia Chronic renal failure Toxins Idiopathic Early onset Late onset Tropical Genetic Hereditary pancreatitis (cationic trypsinogen mutation) CFTR mutations SPINK 1 mutations Alpha-1 antitrypsin deficiency TIGAR-O Autoimmune Isolated autoimmune CP Syndromic autoimmune CP (PSC, Sjögren's-associated, etc.) Recurrent and severe AP Postnecrotic Recurrent acute pancreatitis Ischemic/vascular Obstructive Pancreas divisum Intrapapillary mucinous tumor Ductal adenocarcinoma Gastroenterology 2001, Vol. 120, Etemad B, Whitcomb DC Gastroenterology 2001, Vol. 120, Etemad B, Whitcomb DC SAPE Hypothesis (Sentinel AP Event) Chronic Pancreatitis A Step A: Acinar cell stimulation Alcohol, gallstone, TG, oxidative stress Pain Management C D B Step B: Sentinel Event Early: pro-inflammatory respone Late: Stellate cells, pro-fibrotic response Step C: Removal of stimulus Abstinence Cholecystectomy Lipid lowering agents Step D: Recurrent stimulation Stellate cell mediated periacinar fibrosis Malabsorption: exocrine dysfunction Pancreatic Diabetes: endocrine dysfunction Stevens T, Conwell DL. Am J Gastroenterol 2004;99:2256. Whitcomb D, Best Prac and Res in Clin Gastro 2002;16:347. Kozarek R, et al. Gastroenterology. 1998;115: CP Pain Neurobiology CP pain leads to changes in cortical projections of the nociceptive system Gastroenterology 2007;132: Probably the most important article in years on chronic pancreatic pain neurobiology. This publication has opened the door for further investigations in CP pain management CP pain includes activation and modulation of visceral afferents, descending pain pathways and central neuroplasticity. The degree of central sensitization was 17% in controls and 36% in CP patients. Pancreas 2007; 35(1): 22-9 Further evidence supporting neurobiology & central processing in CP pain Thorascopic splanchnicectomy reduces nociceptive visceral input as evidenced by a decreased narcotic requirement but appears to have no affect on central sensitization in CP patients by quantitative sensory testing. European J Pain 2007; 11: Case 2: Chronic Pancreatitis CE is a 58YOM presenting for evaluation of 1-yr hx of epigastric pain radiating to the back and 10lb wt loss. He describes the pain as constant, present on most days, often debilitating (10/10 pain scale), and oily bowel movements SH: alcohol consumption 5-6 beers/day for 25 years but reduced since onset pain Normal CBC, electrolytes, liver chemistries, amylase, and lipase Upper GI endoscopy: no signs PUD CT abdomen: scattered parenchymal calcifications, dilation of main pancreatic duct to 5 mm max diameter, no mass 1. What are the pharmacologic options for pain management?



8 Pain Management: Step-wise Management Low-fat diet, non-narcotic analgesics, no alcohol Therapeutic trial of enzyme 1-2 months, reassess pain Dose: 16,000-64,000 units lipase qac Narcotic analgesia Endoscopic, surgical management Case 2: Chronic Pancreatitis 1. What are the pharmacologic options for pain management? Reasonable to: Initiate a trial of pancreatic enzymes If failed response: Analgesics +/- pain modifying agents Endoscopic therapy Surgery American Gastroenterological Association. Gastroenterology. 1998;115: Chronic Pancreatitis Pain Management Malabsorption: exocrine dysfunction Pancreatic Diabetes: endocrine dysfunction Kozarek R, et al. Gastroenterology. 1998;115: Pancreatic Enzyme Replacement Therapy Mechanism for steatorrhea: Lipase synthesis Lipase denaturation Fat digestion by lipase: Healthy subjects: Gastric lipase activity ~10% total lipase activity CP: Gastric lipase activity ~90% of all lipase activity Unable to compensate for all lipid digestion required Lipase Activity Low [HCO3] CP High [HCO3] Healthy Subjects Duodenal ph Exogenous Enzymes Dutta SK, et al. Dig Dis Sci. 1979;23: Pancreatic Enzyme Replacement Therapy Vast array of formulations available Pharmacologic principles Goal of enzyme replacement: Achieve normal [enzyme] in duodenum Goal of disease state management: Eliminate malabsorption (reduce steatorrhea) Maintain adequate nutrition (prevent wt loss) Ferrone M, et al. Pharmacotherapy. 2007;27(6): Pezzilli R, et al. Dig Liver Dis. 2005;37: Pancreatic Enzyme Pharmacotherapy Commercially available pancrelipase preparations: Creon Zenprep Differences in efficacy? Ferrone M, et al. Pharmacotherapy. 2007;27(6):
9 Pancreatic Enzyme Pharmacotherapy 1. Conventional, uncoated: Susceptible to inactivation by acidity of stomach Increase dose Acid suppressive therapy 2. Enteric-coated microencapsulated: ph-sensitive coating Microspheres, minimicrospheres, microtablets Distribution in chyme throughout gastric emptying 3. Enteric-coated, high buffered Contain bicarbonate Ferrone M, et al. Pharmacotherapy. 2007;27(6): Kalnins D, et al. J Pediatr Gastroenterol Nutr. 2006;42: Treatment Regimens: Malabsorption Dose approximated by lipase content Mean duodenal lipase activity: units/ml Adults: ~25,000-40,000 units lipase/meal Children, adolescents: ~ units lipase/kg/meal (or units lipase/g fat) Goal: Reduce steatorrhea to <15g/day of fat Titrate dose based to effect Considerations if treatment failure: Check compliance Product integrity Acid suppression Ferrone M, et al. Pharmacotherapy. 2007;27(6): Layer PT, et al. Pancreas. 1992;7:745. Chronic Pancreatitis Pain Management Malabsorption: exocrine dysfunction Pancreatic Diabetes: endocrine dysfunction Pancreatic Diabetes Glucose intolerance Overt diabetes: late in the course of disease Pancreatic diabetes: Typically insulin-requiring Different from type 1 diabetes Pancreatic alpha cells also affected May lead to increased risk hypoglycemia Kozarek R, et al. Gastroenterology. 1998;115: Del Prato S, et al. Diabetes Reviews. 1993;1:260. Malka D, et al. Gastroenterology. 2000;119:1324. Treatment Options for CP Good Anatomy based Macroscopic Better Physiology based Microscopic Best Pathogenesis based Molecular Pathogenesis Based Therapy: Best Pancreatic stellate cells activation Molecular mediators TGF-B, PDGF Pro-inflammatory cytokines IL-1, IL-6, TNF-alpha Molecular pathways MAPK, PI3K Novel molecular targets Potential therapeutic agents Talukdar R., J Gastro and Hep 2008; 23(1):
10 Question 1 Enteric coated enzymes are preferable over uncoated enzymes in the management of steatorrhea? A.True B.False Question 1 Enteric coated enzymes are preferable over uncoated enzymes in the management of steatorrhea? A.True B.False Answer A: True Protection of lipase from low ph in stomach Question 2 Which of the following diagnostic tests has the highest accuracy at detecting early / mild chronic pancreatitis? A. ERCP B.MRCP C. Pancreas function test D.EUS Question 2 Answer: C, Pancreas Function Test Structural Changes Pancreas Function Early Late Sxs Abd Pain(10y) Dyspepsia Steatorrhea(29y) Diabetes(38y) Cancer (55y) PFT Normal Abnormal ERCP Normal Minimal Moderate Severe MRCP Normal T1 signal Ductal Duct/secretion EUS >5 Question 3 Which of the following is not part of the Ranson Criteria for assessment of Acute Pancreatitis Severity? WBC Gender Age Glucose LDH Question 3 Answer C: Gender Which of the following is not part of the Ranson Criteria for assessment of Acute Pancreatitis Severity? A. WBC B. Gender C. Age D. Glucose E. LDH
11 Pancreatitis Resources Harrisons and Cecil stextbooks of Medicine Practice Guidelines for Acute Pancreatitis: American College of Gastroenterology American Gastroenterological Association Practice guidelines for acute pancreatitis, pain management in chronic pancreatitis Gastroenterology Clinics of North America:
12
Diseases of pancreas - Chronic pancreatitis
 Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Chronic Pancreatitis
 Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
Falk Symposium 161 October 12, 2007 Chronic Pancreatitis David C Whitcomb MD PhD Giant Eagle Foundation Professor of Cancer Genetics. Professor of Medicine, Cell biology & Physiology, and Human Genetics
CLASSIFICATION OF CHRONIC PANCREATITIS
 CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
CLASSIFICATION OF CHRONIC PANCREATITIS EAGE, Podstgraduate Course, Prague, April 2010. Tomica Milosavljević School of Medicine, University of Belgrade Clinical Center of Serbia,Belgrade The phrase chronic
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Prof. (DR.) MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet
 MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet") Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Case 1. Intro to Gallbladder & Pancreas Pathology. Case 1 DIAGNOSIS??? Acute Cholecystitis. Acute Cholecystitis. Helen Remotti M.D.
 Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
Cholecystitis acute chronic Gallbladder tumors Adenomyoma (benign) Adenocarcinoma Pancreatitis acute chronic Pancreatic tumors Intro to Gallbladder & Pancreas Pathology Helen Remotti M.D. Case 1 70 year
LOKUN! I got stomach ache!
 LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
LOKUN! I got stomach ache! Mr L is a 67year old Chinese gentleman who is a non smoker, social drinker. He has a medical history significant for Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus, Chronic
CASE 01 LA Path Slide Seminar 13 March, 08. Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center
 CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
CASE 01 LA Path Slide Seminar 13 March, 08 Deepti Dhall, MD Department of Pathology and Laboratory Medicine Cedars-Sinai Medical Center Clinical History 60 year old male presented with obstructive jaundice
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Chronic Pancreatitis
 Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Supportive module 2: Basics of diagnosis, treatment and prevention of major gastroenterological diseases Chronic Pancreatitis LECTURE IN INTERNAL MEDICINE FOR IV COURSE STUDENTS M. Yabluchansky, L. Bogun,
Acute Pancreatitis. Falk Symposium 161 Dresden
 Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Chronic Pancreatitis. Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture
 Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Chronic Pancreatitis Ara Sahakian, M.D. Assistant Professor of Medicine USC core lecture What is Chronic Pancreatitis Progressive inflammatory disease Pancreatic parenchyma replaced w/fibrous tissue Destruction
Diseases of exocrine pancreas
 Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good. Karen Lo R 3 University of Colorado Oct 11, 2010
 Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
Prophylactic Antibiotics in Severe Acute Pancreatitis: Antibiotics are good Karen Lo R 3 University of Colorado Oct 11, 2010 Overview Pancreas: The History Pancreas: The Organ The Disease Pathogenesis
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
PANCREATITIS. By April McMurray. March 14, 2013 NDFS 356
 PANCREATITIS By April McMurray March 14, 2013 NDFS 356 INTRODUCTION The pancreas is a small gland that sits behind the stomach and plays an important role in digestion (1). Its head is situated within
PANCREATITIS By April McMurray March 14, 2013 NDFS 356 INTRODUCTION The pancreas is a small gland that sits behind the stomach and plays an important role in digestion (1). Its head is situated within
Acute Pancreatitis. Case: NG. Idiopathic Pancreatitis is Common. Investigation and Management of Idiopathic Acute Recurrent Pancreatitis (IARP)
") BRIGHAM AND WOMENS HOSPITAL Investigation and Management of (IARP) Acute Pancreatitis j Darwin L. Conwell MD, MS Associate Professor of Medicine Harvard Medical School Boston, MA Case: NG 54 year old female
BRIGHAM AND WOMENS HOSPITAL Investigation and Management of (IARP) Acute Pancreatitis j Darwin L. Conwell MD, MS Associate Professor of Medicine Harvard Medical School Boston, MA Case: NG 54 year old female
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
ESPEN Congress Brussels 2005
 ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
Surgical Management of Acute Pancreatitis
 Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD
 Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
6.2.1 Exocrine pancreatic insufficiency
 6.2.1 Exocrine pancreatic insufficiency Authors: Jean Louis Frossard, Alain Sauty 1. INTRODUCTION Exocrine pancreatic insufficiency is a biological and clinical condition that is characterized by a progressive
6.2.1 Exocrine pancreatic insufficiency Authors: Jean Louis Frossard, Alain Sauty 1. INTRODUCTION Exocrine pancreatic insufficiency is a biological and clinical condition that is characterized by a progressive
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION
 IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
Pancreatitis. Leigh Ann Mike, Pharm.D., BCPS, CGP Clinical Assistant Professor UW School of Pharmacy. Spring 2014
 Pancreatitis Leigh Ann Mike, Pharm.D., BCPS, CGP Clinical Assistant Professor UW School of Pharmacy laam@uw.edu Spring 2014 Case Study Tina is a 42 year old woman who presents to the Emergency Department
Pancreatitis Leigh Ann Mike, Pharm.D., BCPS, CGP Clinical Assistant Professor UW School of Pharmacy laam@uw.edu Spring 2014 Case Study Tina is a 42 year old woman who presents to the Emergency Department
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Perforation of a Duodenal Diverticulum. Elective Student S. C.
 Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Perforation of a Duodenal Diverticulum 2008 4 Elective Student S. C. Case History An elderly male presented to the Emergency Department with abdominal pain. Chief Complaint: Worsening, diffuse abdominal
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram
 Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
What Is Pancreatitis?
 What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018
 Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018 This document is only a SHORT PREVIEW of the Medifocus Guidebook on Chronic Pancreatitis. It is intended primarily to give
Preview of the Medifocus Guidebook on: Chronic Pancreatitis Updated July 4, 2018 This document is only a SHORT PREVIEW of the Medifocus Guidebook on Chronic Pancreatitis. It is intended primarily to give
Exocrine functions: secretion of digestive enzymes (eg. lipase, amylase,
 Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Causes of pancreatic insufficiency. Eugen Dumitru
 Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Bile composition. Pathophysiology of Gallstone Formation and Pancreatitis. Bile
 Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Bile composition Pathophysiology of Gallstone Formation and Pancreatitis Robert F. Schwabe rfs2102@columbia.edu Phospholipids Miscellaneous (Pigment, Protein) (Lecithin) Bile Salts 0.7% 4% H 2 0 1% 12%
Early chronic pancreatitis - Are you missing it?
 Early chronic pancreatitis - Are you missing it? Pancreatic diseases and Pancreatic Exocrine Insufficiency (PEI) What is the relevance to general practice? Darren A. Pavey MBBS FRACP Staff Specialist,
Early chronic pancreatitis - Are you missing it? Pancreatic diseases and Pancreatic Exocrine Insufficiency (PEI) What is the relevance to general practice? Darren A. Pavey MBBS FRACP Staff Specialist,
Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome
 PancreasFest 2017 Precision Medicine Approach For Benign Pancreatic Disease Friday, July 28, 2017 Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome David C Whitcomb MD PhD Director,
PancreasFest 2017 Precision Medicine Approach For Benign Pancreatic Disease Friday, July 28, 2017 Peering Into the Black Box of the Complex Chronic Pancreatitis Syndrome David C Whitcomb MD PhD Director,
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Malabsorption: etiology, pathogenesis and evaluation
 Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Malabsorption: etiology, pathogenesis and evaluation Peter HR Green NORMAL ABSORPTION Coordination of gastric, small intestinal, pancreatic and biliary function Multiple mechanisms Fat protein carbohydrate
Nutrition in Pancreatic Disease Topic 14
 Nutrition in Pancreatic Disease Topic 14 Module 14.2 Chronic Pancreatitis Learning objectives Johann Ockenga, MD, Prof. Dep. of Gastroenterology, Endocrinology & Nutrition, Klinikum Bremen Mitte, St. Juergensstrasse
Nutrition in Pancreatic Disease Topic 14 Module 14.2 Chronic Pancreatitis Learning objectives Johann Ockenga, MD, Prof. Dep. of Gastroenterology, Endocrinology & Nutrition, Klinikum Bremen Mitte, St. Juergensstrasse
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
SASKATCHEWAN REGISTERED NURSES ASSOCIATION. RNs WITH ADDITIONAL AUTHORIZED PRACTICE CLINICAL DECISION TOOL AUGUST 2017
 DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
DEFINITION Cholelithiasis Presence of gall stones in the biliary tract. Biliary Colic Right upper quadrant pain due to obstruction of a bile duct by a gallstone. Cholecystitis Inflammation of the gallbladder
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter
 Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Resident Teaching Conference 10/16/09 Rondi Kauffmann Resident presenter William Nealon Faculty presenter KC 59 year old male Referred to Surgery clinic for incidentally discovered 5cm x 3cm pancreatic
Chronic Pancreatitis
 Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Gastro Foundation Fellows Weekend 2017 Chronic Pancreatitis Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Aetiology in SA Alcohol (up to 80%) Idiopathic Tropical Obstruction Autoimmune
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
Adv Pathophysiology Unit 9: GI Page 1 of 10
 Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Adv Pathophysiology Unit 9: GI Page 1 of 10 Learning objectives for this file: 1. Recognize positive physical and lab findings that point to the diagnosis 2. Appreciate the appearance of the affected organ
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Acute Abdomen. Nirav Patel MD, FACS Banner University Medical Center - Phoenix
 Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Acute Abdomen Nirav Patel MD, FACS Banner University Medical Center - Phoenix ? Diffuse periumbilical with localization to RLQ + Nausea, anorexia, fevers - Diarrhea, emesis Exacerbated by movement, bumps
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
Pediatric Pancreatic Lesions
 Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
Pediatric Pancreatic Lesions Pediatric Surgery Grand Rounds 9 October 2013 Tim Weatherall, PGY2 The University of Tennessee Health Science Center Memphis, TN Disclosures No financial interests to disclose
Acute Pancreatitis. What is the Pancreas? What does it do? What is acute pancreatitis? What causes acute pancreatitis? What symptoms do you get?
 In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute Pancreatitis www.corecharity.org.uk What is the Pancreas? What does it do? What is acute pancreatitis? What causes
In association with: Primary Care Society for Gastroenterology INFORMATION ABOUT Acute Pancreatitis www.corecharity.org.uk What is the Pancreas? What does it do? What is acute pancreatitis? What causes
Evidence Process for Abdominal Pain Guideline Research 11/16/2017. Guideline Review using ADAPTE method and AGREE II instrument 11/16/2017
 Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Evidence Process for Abdominal Pain Guideline Research Guideline Review using ADAPTE method and AGREE II instrument Approximately 139 Potentially relevant guidelines identified in various resources* 59
Acute pancreatitis Case reports. Clinical problems. Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4)
 Surgical treatment of AP? (P 3 & 4)") Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Case reports Clinical problems Use of antibiotics? (P 1 & 2) Surgical treatment of AP? (P 3 & 4) Case reports Case 1 Case 1 Patient KD History M, 63 y Obesity BMI 30.3 kg/m 2 Gallbladder stones No concomitant
Long Term Follow-up. 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown. Is the patient alive? Yes No
 Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Long Term Follow-up 6 Month 1 Year Annual enter year #: What is the assessment date: / / Unknown Is the patient alive? Yes No Was an exam performed by a bariatric physician or PA/NP? Yes No Was the patient
Joint Trust Management of Acute Severe Pancreatitis in Adults
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
5. Which component of the duodenal contents entering the stomach causes the most severe changes to gastric mucosa:
 Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
Gastro-intestinal disorders 1. Which are the most common causes of chronic gastritis? 1. Toxic substances 2. Chronic stress 3. Alimentary factors 4. Endogenous noxious stimuli 5. Genetic factors 2. Chronic
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis.
 Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
Page 1 of 6 Int. Med J Vol. 6 No 1 June 2007 Enteral Nutrition In Intensive Care: Tiger Tube For Small Bowel Feeding In Acute Pancreatitis. Case Report Mohd Basri bin Mat Nor. Department of Anaesthesiology
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
Appendix B: Scope NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE Post publication note: The title of this guideline changed during development. This scope was published before the guideline
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
Chronic pancreatitis an increasing Indian Problem
 Chronic pancreatitis an increasing Indian Problem Dr Ramesh Ardhanari M.S; MCh.(SGE); FRCS (Hon)(G) Medical Director, Sr. Consultant & Head Dept. of Surgical Gastroenterology Meenakshi Mission Hospital,Madurai
Chronic pancreatitis an increasing Indian Problem Dr Ramesh Ardhanari M.S; MCh.(SGE); FRCS (Hon)(G) Medical Director, Sr. Consultant & Head Dept. of Surgical Gastroenterology Meenakshi Mission Hospital,Madurai
9/21/15. Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015
 Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Unless they prove otherwise. ~Every ED attending ever Joshua Pruitt, MD, FAAEM Medical Director, LifeGuard Air Ambulance Iowa PA Society Fall CME Conference September 29, 2015 AAA with rupture Mesenteric
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 11
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 11 Contents 11. Chronic Pancreatitis 138 11.1. Overview of management
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 11 Contents 11. Chronic Pancreatitis 138 11.1. Overview of management
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Soft palate elevates, closing off the nasopharynx. Hard palate Tongue Bolus Epiglottis. Glottis Larynx moves up and forward.
 The Cephalic Phase Chemical and mechanical digestion begins in the mouth Saliva is an exocrine secretion Salivary secretion is under autonomic control Softens and lubricates food Chemical digestion: salivary
The Cephalic Phase Chemical and mechanical digestion begins in the mouth Saliva is an exocrine secretion Salivary secretion is under autonomic control Softens and lubricates food Chemical digestion: salivary
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected