Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
|
|
|
- Zoe Sparks
- 6 years ago
- Views:
Transcription
1 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018

2 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP When to consider enteral feeding How to manage fluid collections Endoscopic necrosectomy

3 Acute Pancreatitis An acute inflammatory process of the pancreas Accounts for 210, 000 admissions yearly in the US Mortality ranges 3% with interstitial edematous pancreatitis 17% with pancreatic necrosis
 T: trauma S: steroids M: mumps (and other infections)")
 E: ERCP D:")
4 Etiology - I GET SMASHED I: idiopathic G: gallstones E: ethanol (alcohol) T: trauma S: steroids M: mumps (and other infections) / malignancy A: autoimmnue S: scorpion sting/spider bites H: hyperlipidemia/hypercalcemia (metabolic disorders) E: ERCP D: drugs
5 Diagnosis Requires the presence of 2 of the following 3 criteria: Acute onset of persistent, severe, epigastric pain often radiating to the back Serum lipase and/or amylase > 3 ULN Classic CT or MRI findings
6 Clinical Features Most have acute onset of persistent, severe epigastric pain In 50%, the pain radiates to the back and may be partially relieved by sitting up or bending forward 90% have associated n/v which may persist for several hours With gallstone pancreatitis, the pain is well localized and the onset is rapid, reaching max intensity in minutes With alcohol, hereditary, or metabolic causes, the onset may be less abrupt and poorly localized Patients with severe pancreatitis may have dyspnea due to diaphragmatic inflammation, pleural effusions, or RDS
7 Laboratory Findings There is a breakdown in the synthesissecretion coupling of pancreatic digestive enzymes Synthesis continues while there is a blockade of secretion As a result, digestive enzymes leak out of acinar cells through the basolateral membrane to the interstitial space and enter circulation.
8 Serum Amylase Rises within 6-12 hours Has a short half-life of approximately 10 hours In uncomplicated attacks, returns to normal within 3-5d Elevation of greater than 3 times the upper limit of normal has a sensitivity of & specificity of 85-98% May not be seen 20% with alcoholic pancreatitis due to the inability of the parenchyma to produce amylase and 50% due to hypertriglyceridemia as TGs interfere with the amylase assay Given the short half-life, the diagnosis may be missed in patients who present >24 hours after the onset
9 Serum Lipase Rises within 4-8 hours, peaks at 24 hours, and returns to normal within 8-14 days Lipase elevations occur earlier and last longer as compared to amylase More useful in patients who present >24 hours after the onset of pain Serum lipase is also more sensitive than amylase in patients with pancreatitis secondary to alcohol


10 Revised Atlanta Classification 2012 Interstitial edematous pancreatitis: acute inflammation of the pancreatic parenchyma and peripancreatic tissues Necrotizing pancreatitis: inflammation with pancreatic or peri-pancreatic necrosis Banks et al. Gut 2013
11 Initial Assessment and Risk Stratification Revised Atlanta Classification 2012 Mild acute pancreatitis Absence of organ failure Absence of local complications Moderately severe acute pancreatitis Local complications and/or Transient organ failure (<48 hrs) Severe acute pancreatitis Persistent organ failure (>48 hrs) Banks PA. Gut 2013
12 Severe Acute Pancreatitis (15-20%) Two distinct phases: Early (within 1 week) Systemic Inflammatory Response Syndrome (SIRS) and/or organ failure Late (>1 week) Local complications Peri-pancreatic fluid collections Pancreatic and peri-pancreatic necrosis (sterile or infected) Pseudocysts Walled-off necrosis (sterile or infected) Banks PA. Gut 2013
13 Ranson's criteria One of the earliest scoring systems for severity that consists of 11 parameters Five of the factors are assessed at admission and six are assessed during the next 48 hours A later modification for biliary pancreatitis included only 10 points Mortality increases with an increasing score. Using the 11 component score, mortality was 0-3% when the score was < % when the score was 3 40% when the score was 6 Although the system continues to be used, a meta-analysis of 110 studies found the Ranson score to be a poor predictor of severity
14 APACHE II Score Score was originally developed for critically ill patients in the ICU It has 12 physiologic measures and extra points based upon age and presence of chronic disease Most widely studied severity scoring system in acute pancreatitis The AGA recommends using the APACHE II for prediction of severe disease, using a cutoff of 8
15 Bedside Index of Severity in Acute Pancreatitis The presence of three or more criteria in the first 24 hrs has been associated with an increased in hospital mortality BUN >25 Impaired mental status Systemic inflammatory response (SIRS) Age >60 Pleural effusion Wu BU. Gut 2008
16 CT severity index (Balthazar) Pancreatic inflammation Normal pancreas 0 Focal or diffuse enlargement of the pancreas 1 Pancreatic or peri-pancreatic fat inflammatory changes 2 Single, ill-defined fluid collection 3 Two or more collections or presence of gas 4 Pancreatic necrosis None 0 30% 2 >30% and 50% 4 >50% 6 Balthazar EJ. Rad 1990



17 Diagnosis of Acute Pancreatitis
18 Nutrition Patients with mild pancreatitis can often be managed with IV hydration alone since recovery occurs rapidly The time to reinitiate oral feedings depends on the severity of the pancreatitis In the absence of ileus, nausea or vomiting, oral feeds can be initiated as soon as the pain is decreasing and inflammatory markers are improving
19 Enteral Feedings Often required in patients with moderately severe pancreatitis and almost invariably with severe pancreatitis as they are unlikely to resume oral intake within 5-7d Nasojejunal tube feeding is preferred to TPN

20 Parenteral Nutrition Advantages Practical Mathematical Standardized solution for specific conditions Disadvantages The gut is not used Cost issues Complications related to IV access Metabolic issues Sepsis
21 Enteral vs Parenteral Nutrition Less hyperglycemia Fewer septic complications Decreased morbidity in groups receiving enteral nutrition Decreased rates of organ failure Faster return of bowel motility Lower hospital costs Macik BE. BMJ 2005
 <4 weeks Morgan DE: CGH")
22 Acute Fluid Collection Associated with interstitial pancreatitis Homogenous collection with fluid density confined by normal peri-pancreatic fascial planes with no definable wall Adjacent to pancreas (no intrapancreatic invasion) <4 weeks Morgan DE: CGH 2008

23 Acute Necrotic Collection Fluid and necrotic collection of the pancreatic parenchyma or peripancreatic tissue No definable wall Higher intervention rates and increased morbidity and mortality Morgan DE: CGH 2008

24 Pancreatic Pseudocyst Well circumscribed, encapsulated fluid collection with a well defined inflammatory wall Usually outside the pancreas Little or no necrosis Maturation requires > 4 weeks after onset of AP Banks PA. Gut 2013

25 Walled off Necrosis (WON) Matured, encapsulated collection of pancreatic or peri-pancreatic necrosis Well-defined inflammatory wall Maturation typically requires 4 weeks after onset of acute necrotizing pancreatitis Morgan DE: CGH 2008
26
27 Endoscopic Retrograde Cholangiopancreatography (ERCP) Should be performed within 24 hours for patients with gallstone pancreatitis and cholangitis Other indications for ERCP Common bile duct obstruction (visible stone on imaging) Dilated common bile duct Increasing liver tests without cholangitis When in doubt an MRCP could be performed to determine if there are stones in the CBD
28 Issues to Consider Prior to EUS Cyst Gastrostomy Alternative diagnoses No history or risk factors for pancreatitis Cystic pancreatic neoplasms Possible presence of a pseudoaneurysm Type of collection Bulging? Intervening vessels Role of conservative management Some studies showed about 60% resolution or stable PFC Is there a pancreatic duct disruption
29 Drainage Prerequisites Cross sectional imaging: road map Skills in interventional endoscopy/eus Multidisciplinary approach: backup General anesthesia: complexity Carbon dioxide only


30 EUS Cyst Gastrostomy Confirm diagnosis Routine EUS before drainage leads to change in management in 5-37% cases Identify vascular structures Measure lumen to cyst distance Characterize cyst contents Localize non-bulging pseudocysts
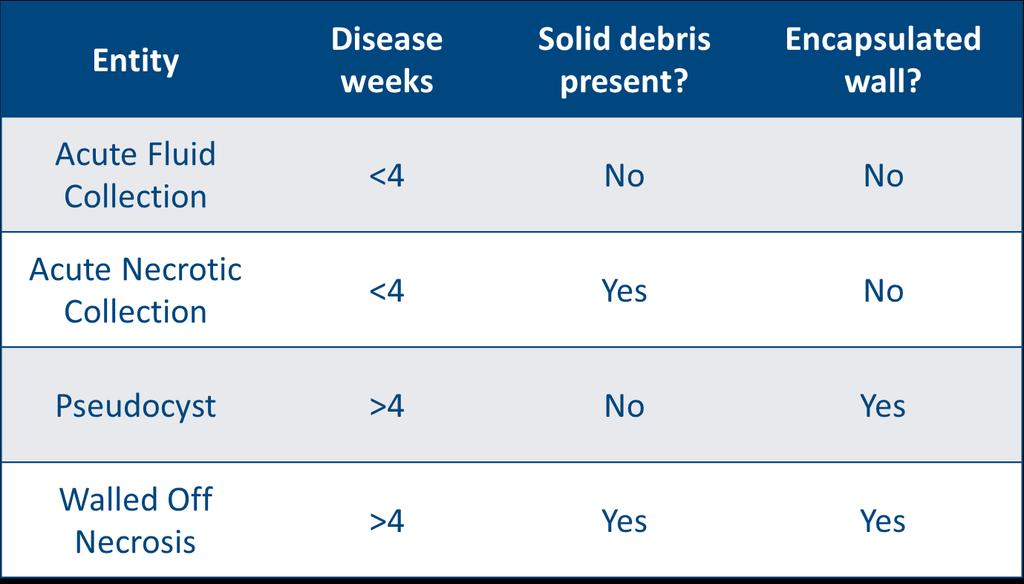
31 EUS Cyst Gastrostomy Techniques Prophylactic antibiotics Linear array echoendoscope (3 mm channel) Puncture with 19 gauge needle Placement of a inch wire Dilation with creation of a fistula Soehendra (6 Fr) Balloon (4-6 mm) Stent placement: FC SEMS, double pigtails Consider if ERCP needed to seal PD leak



32 EUS Cyst Gastrostomy -Needle passed and contrast is injected -Wire insertion under fluoro -Tract balloon dilation -Stent deployment under both views


33 EUS Cyst Gastrostomy
34 EUS Cyst Gastrostomy Talreja JP GIE 2008
 Pneumonperitoneum (1) 31/33 94% Kruger 2006 35 None 33/35 94% Kahaleh 2006 46 Bleeding (2), Stent Migration (1), Superinfection (4), Pneumonperitoneum (2) 43/46 96% Barthet 2008 28")
35 Author Year # Complications Success % Success Binmoeller Bleeding (2) 21/27 78% Giovannini Pneumoperitoneum (1) 31/35 89% Azar Pneumoperitoneum (1) 21/23 91% Antillon Bleeding (4) Pneumonperitoneum (1) 31/33 94% Kruger None 33/35 94% Kahaleh Bleeding (2), Stent Migration (1), Superinfection (4), Pneumonperitoneum (2) 43/46 96% Barthet Superinfection (5) 25/28 89% Hookey Pneumonperitoneum (2), Bleeding (1) Lopes Pneumonperitoneum (1), migration (1) 29/32 91% 48/51 94% Varadarajulu None 21/21 100% Total (9%) %

36 Axios Stent Therapeutic EUS scope Axios stent



37 *Gornals, et al. Surg Endosc Axios Stent




38 Axios Metal Stent Deployment 1. Advance the Stent Catheter Lock catheter lock once on place 2. Deploy Distal Anchor Move stent hub up to #2 on handle 3. Retract & Align Stent Unlock catheter, retract until 2-3mm of black marker visible, lock catheter lock 4. Deploy Proximal Anchor Unlock stent and move stent hub up to #4 on handle
39 Axios Stent Data
40 Pancreatic Duct Disruption Common in persistent smoldering pancreatitis, pancreatic trauma, pancreatic necrosis, and in acute pancreatic fluid collections Leakage of pancreatic secretions through these disruptions can result in the development of chronic fistulas Closure of fistulas depends upon Site and size of duct disruption There is superinfection downstream of the obstruction Disruption is a consequence of a stricture or stone Ductal disruption is partial or complete
41 Pancreatic Duct Disruption Findings on ERCP include extravasation of contrast during injection of the pancreatic duct the presence of fluid collections or pseudocysts that communicate directly with the main pancreatic duct Resolution of fluid collections and patient symptoms determine efficacy Stents are usually retrieved after four to six weeks.

42 Management of PD Disruption Transpapillary stenting leads to successful resolution of PD disruptions, particularly when the stent bridges the disruption Varadarajulu S. GIE 2005
43 Pancreatic Duct Stenting Indications pancreatic duct stones pancreatic duct strictures pseudocysts pancreatic duct disruptions pancreas divisum pancreatic sphincterotomy prevention of post-ercp pancreatitis
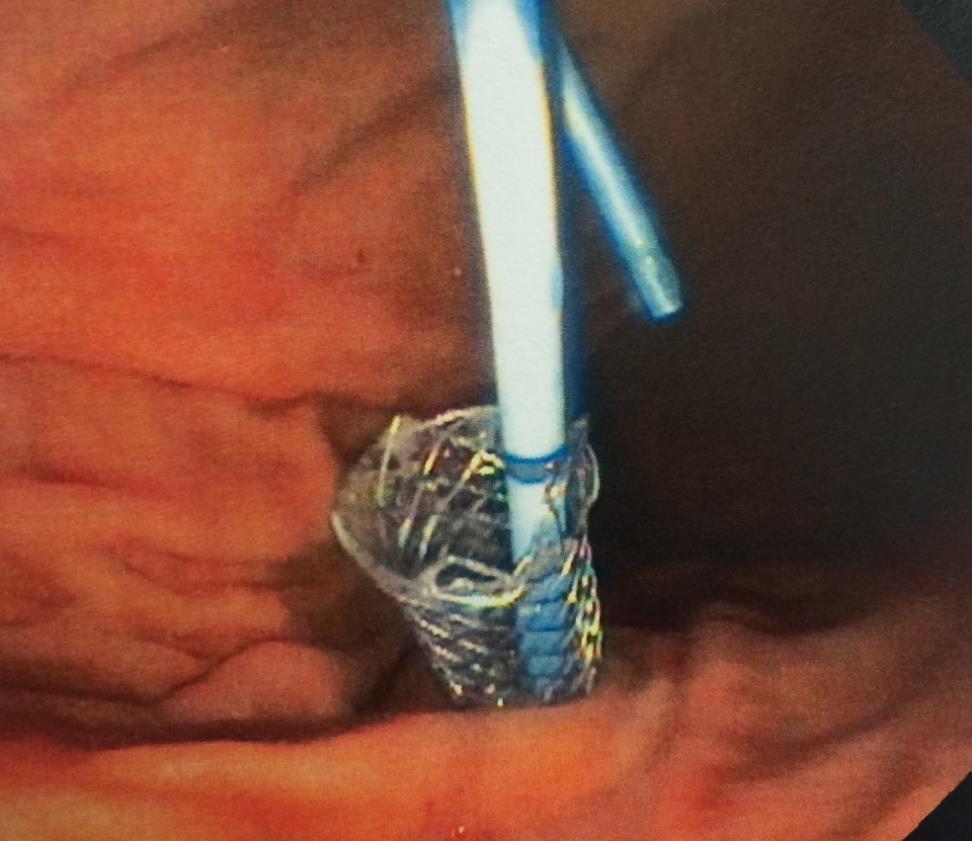
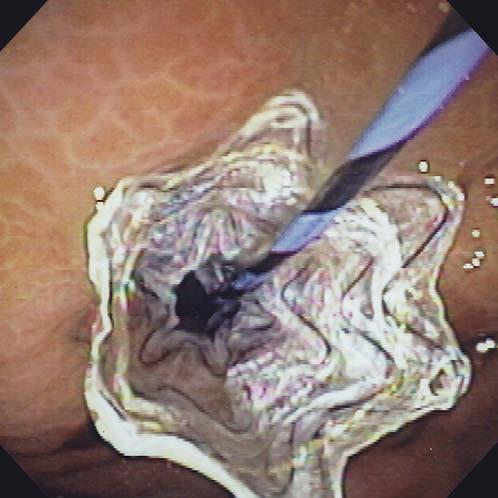
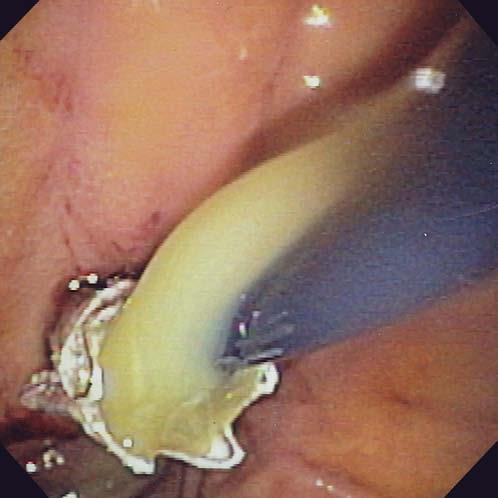
44 Pancreatic Necrosectomy Both infected pancreatic necrosis and symptomatic sterile necrosis are accepted indications for debridement Goal Excise all dead and devitalized pancreatic and peripancreatic tissue Preserve viable functioning pancreas and limit extraneous organ damage Optimal time is approximately 4 weeks after the onset Vascular inflammation has decreased Organization of the process has occurred Delineation of live from dead tissue is complete
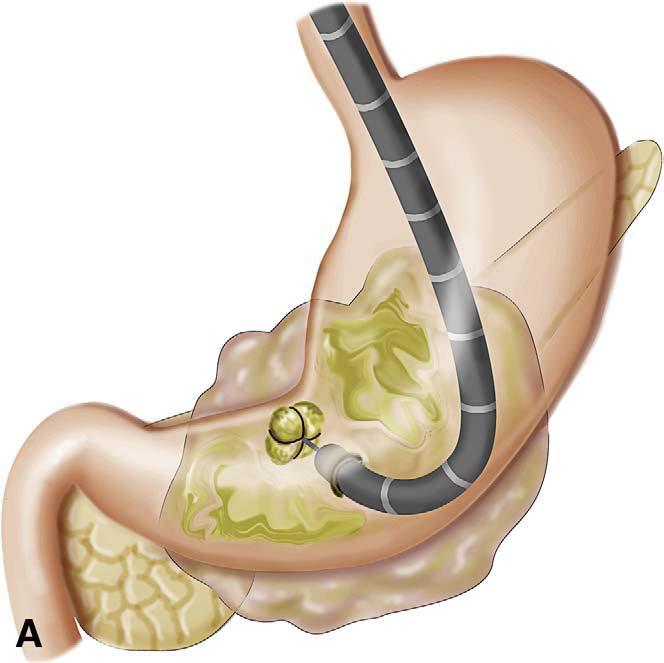
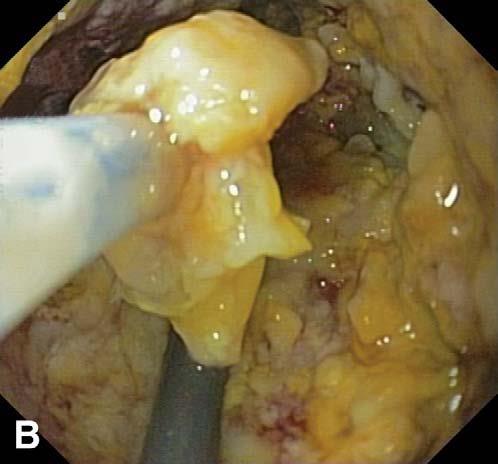
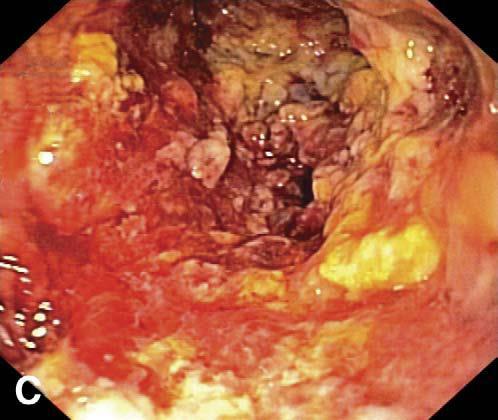
45 Pancreatic Necrosectomy Seewald GIE 2005
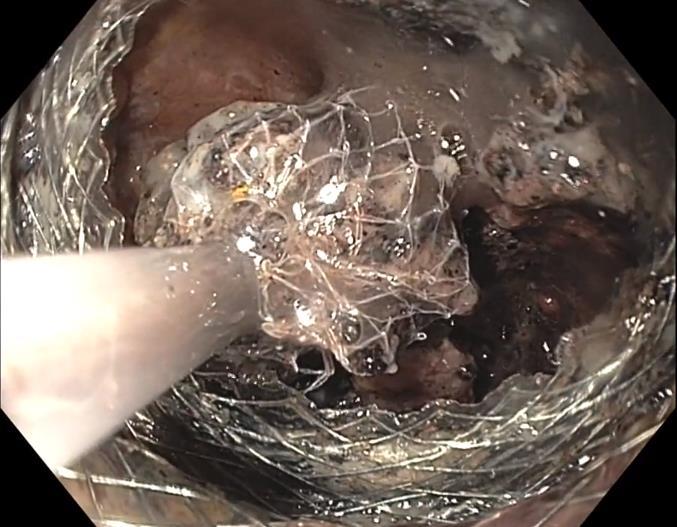
46 Pancreatic Necrosectomy

47 Not for the Uncommitted! May require nasocystic drain Multiple sessions Inpatient management Antibiotics Complications Multidisciplinary approach Baron TH. GIE 2002
48 Complications Overall complication 5-35% Occlusion Infection Antibiotics before and after?antifungal Hemorrhage Stent migration
49 Algorithm For Treatment of Pancreatic Necrosis Kozarek GIE 2005
50 Questions
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Endoscopic pancreatic necrosectomy in 2017
 Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Severe necrotizing pancreatitis. ICU Fellowship Training Radboudumc
 Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Severe necrotizing pancreatitis ICU Fellowship Training Radboudumc Acute pancreatitis Patients with acute pancreatitis van Dijk SM. Gut 2017;66:2024-2032 Diagnosis Revised Atlanta classification Abdominal
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Disclosures. Extra-hepatic Biliary Disease and the Pancreas. Objectives. Pancreatitis 10/3/2018. No relevant financial disclosures to report
 Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
Extra-hepatic Biliary Disease and the Pancreas Disclosures No relevant financial disclosures to report Jeffrey Coughenour MD FACS Clinical Associate Professor of Surgery and Emergency Medicine Division
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies. Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels
 PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
Does it matter what we drain?
 Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
U Nordic Forum - Trauma & Emergency Radiology. Lecture Objectives. MDCT in Acute Pancreatitis. Acute Pancreatitis: Etiologies
 Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Nordic Forum - Trauma & Emergency Radiology Lecture Objectives MDCT in Acute Pancreatitis Borut Marincek Institute of Diagnostic Radiology niversity Hospital Zurich, Switzerland To describe the role of
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Nothing to declare. Probable causes for the change
 acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
acute pancreatitis March 25, 2017 C. S PITCHUMONI. MD,MACP,MACG,MPH.FRCP (c) Adjunct Professor of Medicine New York Medical College Professor of Medicine Rutgers university Nothing to declare Lesser sac?
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
ESPEN Congress Brussels 2005
 ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Original Article INTRODUCTION
 Original Article A retrospective study evaluating endoscopic ultrasound guided drainage of pancreatic fluid collections using a novel lumen apposing metal stent on an electrocautery enhanced delivery system
Original Article A retrospective study evaluating endoscopic ultrasound guided drainage of pancreatic fluid collections using a novel lumen apposing metal stent on an electrocautery enhanced delivery system
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD
 Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Management of Acute Pancreatitis and its Complications Aspirus Grand Rounds June 6, 2017 Eric A. Johnson MD Disclosure: None In accordance with the Standards of the Wisconsin Medical Society, all those
Acute Pancreatitis. Encourage You to Read!
 Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Acute Pancreatitis Laith H. Jamil, MD, FACG Associate Director of Interventional Endoscopy Cedars Sinai Medical Center Los Angeles, CA Encourage You to Read! Copyright 2015 American College of Gastroenterology
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Mild. Moderate. Severe
 2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
AXIOS Stent and Delivery System
 PRESCRIPTIVE INFORMATION AXIOS Stent and Delivery System Warning REFER TO THE DEVICE DIRECTIONS FOR USE FOR COMPLETE INSTRUCTIONS ON DEVICE USE. RX ONLY. CAUTION: FEDERAL LAW (USA) RESTRICTS THIS DEVICE
PRESCRIPTIVE INFORMATION AXIOS Stent and Delivery System Warning REFER TO THE DEVICE DIRECTIONS FOR USE FOR COMPLETE INSTRUCTIONS ON DEVICE USE. RX ONLY. CAUTION: FEDERAL LAW (USA) RESTRICTS THIS DEVICE
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Exocrine functions: secretion of digestive enzymes (eg. lipase, amylase,
 Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
Chapter 91 Pancreas Episode Overview: 1. List 10 differential diagnoses for acute pancreatitis 2. List 10 causes of pancreatitis. Which are most common in adults? Which one is most common in pediatrics?
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS. Raed Abu Sham a, M.D
 CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
CLINICAL MANIFESTATIONS AND DIAGNOSIS OF ACUTE PANCREATITIS Raed Abu Sham a, M.D ACUTE PANCREATITIS Acute inflammatory process of the pancreas that resolves both clinically and histologically. It is usually
Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection
 Original Article Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection Shuntaro Mukai, Takao Itoi, Atsushi Sofuni,
Original Article Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection Shuntaro Mukai, Takao Itoi, Atsushi Sofuni,
Best of UEG week 2017 (Pancreas-biliary)
") Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Acute Pancreatitis. Falk Symposium 161 Dresden
 Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Acute Pancreatitis Falk Symposium 161 Dresden 12.10.2007 Incidence of Acute Pancreatitis (Malmö) Lindkvist B, et al Clin Gastroenterol Hepatol 2004;2:831-837 Gallstones Alcohol AGA Medical Position Statement
Emergency Surgery Course Graz, March ACUTE PANCREATITIS. Carlos Mesquita Coimbra
 ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
ACUTE PANCREATITIS Carlos Mesquita Coimbra ESSENTIALS (1) AP occurs when digestive enzymes become activated while still in the pancreas, causing inflammation repeated bouts of AP can lead to chronic pancreatitis
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION
 IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
IMAGING OF ACUTE AND CHRONIC PANCREATITIS, INCLUDING EXOCRINE FUNCTION Andrew T. Trout, MD @AndrewTroutMD Disclosures Grant support National Pancreas Foundation In-kind support - ChiRhoClin modified from:
Management of Acute Pancreatitis
 Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Management of Acute Pancreatitis A Clinical Practice Guideline developed by the University of Toronto s Best Practice in Surgery JA Greenberg, M Bawazeer, J Hsu, J Marshall, JO Friedrich, A Nathens, N
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
Therapeutic EUS: today & tomorrow Pietro Fusaroli
 Therapeutic EUS: today & tomorrow Pietro Fusaroli Gastroenterologia Università di Bologna AUSL di Imola, Castel S. Pietro Terme (BO) Direttore Prof. G. Caletti EUS FNA: CONVEX ARRAY Olympus, Pentax, Toshiba
Therapeutic EUS: today & tomorrow Pietro Fusaroli Gastroenterologia Università di Bologna AUSL di Imola, Castel S. Pietro Terme (BO) Direttore Prof. G. Caletti EUS FNA: CONVEX ARRAY Olympus, Pentax, Toshiba
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Pancreatic Disease. Chapter. Overview. Diagnosis of the Disease. Francisco Igor B. Macedo and Danny Sleeman. Laboratory Testing
 Chapter 128 Pancreatic Disease Francisco Igor B. Macedo and Danny Sleeman Overview Acute pancreatitis has an annual incidence of 5 to 40 per 100,000 with an overall mortality of 1.5 per 100,000 (1). The
Chapter 128 Pancreatic Disease Francisco Igor B. Macedo and Danny Sleeman Overview Acute pancreatitis has an annual incidence of 5 to 40 per 100,000 with an overall mortality of 1.5 per 100,000 (1). The
Surgical Management of Acute Pancreatitis
 Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
Surgical Management of Acute Pancreatitis Steven J. Hughes, MD, FACS Cracchiolo Family Professor of Surgery and Chief, General Surgery Overview Biliary pancreatitis a cost effective algorithm Key concepts
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Role of Imaging Methods in Diagnosis of Acute Pancreatitis. Válek V. Radiologická klinika, FN Brno a LF MU v Brně
 Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
Role of Imaging Methods in Diagnosis of Acute Pancreatitis Válek V. Radiologická klinika, FN Brno a LF MU v Brně New Classification: Acute Pancreatitis 2007 revision of Atlanta classification and definitions
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
Sepsis in Acute Pancreatitis. MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital
 Sepsis in Acute Pancreatitis MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital Introduction Self limiting disease in 85% Minority develop
Sepsis in Acute Pancreatitis MD Smith Department of Surgery University of the Witwatersrand, Johannesburg Chris Hani Baragwanath Academic Hospital Introduction Self limiting disease in 85% Minority develop
Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance of Gillian Lieberman, MD
 Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
Under the guidance of Gillian Lieberman, MD March 2016 RADIOLOGICAL HALLMARKS OF NECROTIZING PANCREATITIS Siddharth Gosavi, Vydehi Institute of Medical Sciences & Research Centre, India Under the guidance
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
and Transmural Drainage
 HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Joint Trust Management of Acute Severe Pancreatitis in Adults
 A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
A clinical guideline recommended for use For Use in: By: For: Division responsible for document: All clinical areas (as a reference for screening) ITU/HDU (for definitive care) All medical staff likely
EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice
 CASE REPORT EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice Tiing Leong Ang, Eng Kiong Teo, Kwong Ming Fock Division of Gastroenterology, Department
CASE REPORT EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice Tiing Leong Ang, Eng Kiong Teo, Kwong Ming Fock Division of Gastroenterology, Department
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis. William H. Nealon M.D.
 The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis William H. Nealon M.D. Students and Trainees: Guide to Creativity, Productivity and Innovation in a Clinical Career Choose
The Influence of Pancreatic Ductal Anatomy on the Complications of Pancreatitis William H. Nealon M.D. Students and Trainees: Guide to Creativity, Productivity and Innovation in a Clinical Career Choose
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
Multi modality Imaging in Acute Pancreatitis. Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009
 Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Multi modality Imaging in Acute Pancreatitis Marsha Lynch, HMS III Gillian Lieberman, MD BIDMC Core Clerkship in Radiology March 2009 Our Patient R: Introduction 52M with 10d history of nausea, vomiting
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
AXIOS Stent and Electrocautery Enhanced Delivery System. Quick Reference Guide
 AXIOS Stent and Electrocautery Enhanced Delivery System Quick Reference Guide AXIOS Stent (front and side views) UPN Codes Flange Diameter (mm) Lumen Diamter (mm) Saddle Length (mm) Catheter OD (Fr) Catheter
AXIOS Stent and Electrocautery Enhanced Delivery System Quick Reference Guide AXIOS Stent (front and side views) UPN Codes Flange Diameter (mm) Lumen Diamter (mm) Saddle Length (mm) Catheter OD (Fr) Catheter
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Endoscopic Retrograde Cholangiopancreatography (ERCP)
") Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Safety and Efficacy of Endoscopic Ultrasound-Guided Drainage of Pancreatic Fluid Collections With Lumen-Apposing Covered Self-Expanding Metal Stents
 All studies published in Clinical Gastroenterology and Hepatology are embargoed until 3PM ET of the day they are published as corrected proofs on-line. Studies cannot be publicized as accepted manuscripts
All studies published in Clinical Gastroenterology and Hepatology are embargoed until 3PM ET of the day they are published as corrected proofs on-line. Studies cannot be publicized as accepted manuscripts
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Evaluation and Management of Refractory Biliary Stricture. J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc.
 Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Evaluation and Management of Refractory Biliary Stricture J. David Horwhat, MD, FACG Director of Endoscopy Lancaster Gastroenterology, Inc Outline What defines a refractory biliary stricture Endoscopic
Acute Pancreatitis:
 American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
American College of Gastroenterology 2014 Acute Pancreatitis Scott Tenner, MD, MPH, FACG Clinical Professor of Medicine State University of New York Health Sciences Center Director, Brooklyn Gastroenterology
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Endoscopic Resolution of Pseudocyst Infection and Necrosis as a Complication of Endoscopic Pseudocyst Drainage. A Case Report
 CASE REPORT Endoscopic Resolution of Pseudocyst Infection and Necrosis as a Complication of Endoscopic Pseudocyst Drainage. A Case Report Rodrigo Azevedo Rodrigues, Lucianna Pereira da Motta Pires Correia,
CASE REPORT Endoscopic Resolution of Pseudocyst Infection and Necrosis as a Complication of Endoscopic Pseudocyst Drainage. A Case Report Rodrigo Azevedo Rodrigues, Lucianna Pereira da Motta Pires Correia,
Does Sphincter of Oddi Dysfunction Even Exist Anymore?
 Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Frank Burton Memorial Update on Pancreato-biliary Cancers
 Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Frank Burton Memorial Update on Pancreato-biliary Cancers Diagnosis and management of pancreatic cancer: common dilemmas Moderators: Banke Agarwal, MD Paul Buse, MD Evaluation of patients with obstructive
Endoscopic ultrasound-guided placement of AXIOS stent for drainage of pancreatic fluid collections
 REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 1-6 Endoscopic ultrasound-guided placement of AXIOS stent for drainage of pancreatic fluid collections Rashmee Patil a, Mel A. Ona b, Charilaos Papafragkakis
REVIEW ARTICLE Annals of Gastroenterology (2016) 29, 1-6 Endoscopic ultrasound-guided placement of AXIOS stent for drainage of pancreatic fluid collections Rashmee Patil a, Mel A. Ona b, Charilaos Papafragkakis
The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
Morning Report. Allison Haden, MD October 1, 2002
 Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Morning Report Allison Haden, MD October 1, 2002 68 yo WM with N/V and abdominal pain Became ill about 2 weeks ago, per pt. intermittent nausea: worse w/eating vomiting within 30min of eating, nonbilious,
Y A L E S C H O O L O F M E D I C I N E. This is a CME accredited activity. The presenters and there are no conflicts of interest.
 This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
This is a CME accredited activity. The presenters and there are no conflicts of interest. Pain in Pancreatic Cancer More than 50% of patients with pancreatic cancer suffer from abdominal and back pain
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Douglas G. Adler MD. ACG Regional Postgraduate Course - Nashville, TN Copyright 2013 American College of Gastroenterology
 Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
Enteral Stents 2013: State of the Art Douglas G. Adler MD Associate Professor of Medicine Director of Therapeutic Endoscopy University of Utah School of Medicine Huntsman Cancer Center Esophageal Stents
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction
 A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis
 ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 162-166 Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis Surinder
ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 162-166 Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis Surinder
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
A Guide for Patients Living with a Biliary Metal Stent
 A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
A Guide for Patients Living with a Biliary Metal Stent What is a biliary metal stent? A biliary metal stent (also known as a bile duct stent ) is a flexible metallic tube specially designed to hold your
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol
 Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Prof. (DR.) MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet
 MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet") Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
American College of Gastroenterology Guideline: Management of Acute Pancreatitis
 PRACTICE GUIDELINES nature publishing group 1 American College of Gastroenterology Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG1, John Baillie, MB, ChB, FRCP, FACG 2, Joh n D
PRACTICE GUIDELINES nature publishing group 1 American College of Gastroenterology Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG1, John Baillie, MB, ChB, FRCP, FACG 2, Joh n D
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
EUS- Gallbladder Drainage: is it time to replace percutaneous drainage?
 EUS- Gallbladder Drainage: is it time to replace percutaneous drainage? Jessica Widmer, DO 1, Juveria Abdullah 1, Michel Kahaleh, MD. 1 Division of Gastroenterology and Hepatology, Department of Medicine,
EUS- Gallbladder Drainage: is it time to replace percutaneous drainage? Jessica Widmer, DO 1, Juveria Abdullah 1, Michel Kahaleh, MD. 1 Division of Gastroenterology and Hepatology, Department of Medicine,
Pancreatic Lesions. Valerie Jefford Pediatric Surgery Rounds June 6, 2003
 Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Pancreatic Lesions Valerie Jefford Pediatric Surgery Rounds June 6, 2003 Embryology 4 th week 2 buds of endodermal origin from caudal foregut Dorsal and ventral bud Ventral migrates dorsally with CBD (below/behind
Intra-channel stent release technique for fluoroless endoscopic ultrasound-guided lumen-apposing metal stent placement: changing the paradigm
 Intra-channel stent release technique for fluoroless endoscopic ultrasound-guided lumen-apposing metal stent placement: changing the paradigm Authors Andrea Anderloni 1,FabiaAttili 2, Silvia Carrara 1,
Intra-channel stent release technique for fluoroless endoscopic ultrasound-guided lumen-apposing metal stent placement: changing the paradigm Authors Andrea Anderloni 1,FabiaAttili 2, Silvia Carrara 1,