Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
|
|
|
- Grant Ellis
- 6 years ago
- Views:
Transcription
1 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center
2 Disclosures No conflicts of interest to disclose
3 Objectives 1. Describe the pathophysiology of critical illness-related corticosteroid insufficiency (CIRCI) 2. Recommend appropriate diagnostic tests for CIRCI 3. Discuss the literature regarding corticosteroid use in various critical care conditions 4. Determine appropriate utilization of corticosteroids in the ICU
4 Pathophysiology Cortisol is essential for: Gluconeogenesis Anti-inflammatory effects on the immune system Maintenance of vascular tone Endothelial integrity Increased sensitivity to catecholamines Reduction in nitric oxide vasodilation Modulation of angiotensinogen synthesis Increased cortisol production with severe infection, trauma, burns, illness, or surgery Cooper MS et al. NEJM. 2003;348:727-34
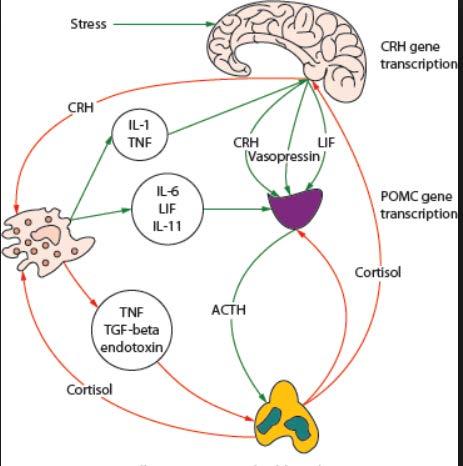
5 Pathophysiology
6 Critical Illness-Related Corticosteroid Insufficiency (CIRCI) Inadequate corticosteroid activity for the severity of illness of a patient During severe illness, many factors can impair the normal corticosteroid response Adrenal cortisol synthesis can be impaired High levels of inflammatory cytokines in patients with sepsis can directly inhibit cortisol synthesis Decreased production of CRH, ACTH, and cortisol Increased systemic or tissue specific corticosteroid resistance Excessive production of inflammatory cytokines during sepsis can lead to resistance Cooper MS et al. NEJM. 2003;348:727-34
7 Cooper MS et al. NEJM. 2003;348:727-34
8 Consequences of CIRCI Exaggerated pro-inflammatory response and have relative corticosteroid insufficiency Elevated levels of inflammation Decreased corticosteroid response leads to an increase in: Morbidity Mortality ICU length of stay
9 Diagnosis
10 Diagnosis 1. Random cortisol level A random cortisol level of less than 10 mcg/dl can be used to diagnose CIRCI 2. Cosyntropin stimulation test A delta serum cortisol level of less than 9 mcg/dl following an IV dose of 250 mcg of cosyntropin can be used to diagnose CIRCI 1. Obtain a baseline cortisol 2. Give IV cosyntropin 3. Obtain 30 minute cortisol 4. Obtain 60 minute cortisol
11 Cosyntropin Stimulation Test Annane et al. completed a prospective cohort study looking at risk factors associated with 28 day mortality (n=189) Factors associated with increased mortality APACHE II score > 55 MAP < 60 mmhg Arterial lactate > 2.8 mmol/l PaO 2 :FiO 2 < 160 mmhg Random cortisol level < 34 mcg/dl Delta cortisol level < 9 mcg/dl Annane et al. Am J Respir Crit Care Med.2006;174:
12 Adrenal Insufficiency During Septic Shock Marik et al. conducted a study that gave patients admitted to the MICU low dose (1 mcg) ACTH stimulation test followed by high dose (249 mcg) 60 minutes later (n=59) Hydrocortisone 100mg IV q8h was started after the test Steroids were discontinued if baseline cortisol was > 25 mcg/dl or delta cortisol > 18 mcg/dl Steroid responsiveness: discontinuing norepinephrine for MAP > 65 mmhg within 24 hours of steroid use Results Patients who were steroid responsive: 95% had a cortisol < 25 mcg/ml 54% had a diagnostic low dose ACTH test 22% had a diagnostic high dose ACTH test Marik PE et al. Crit Care Med. 2003;31 (1):
13 Total vs. Free Cortisol Levels 90% of circulating cortisol is bound to protein (i.e. corticosteroid-binding globulin and albumin) During critical illness elastase secreted from neutrophils at the site of inflammation cleave corticosteroid-binding globulin contributing to higher cortisol levels In a study looking at critically ill patients it was noted that patients had elevated glucocorticoid secretion that was not detectable when measuring serum cortisol but free cortisol was increased 7 to 10 fold Need to be careful interpreting total cortisol levels in patients with hypoproteinemia Arafah et al. J Clin Endocrinol Metab. 2006;91(10):
14 Limitations of Tests Critically-ill patients have high baseline and cosyntropin stimulated cortisol levels Variable data on diagnostic values used in studies Due to this the incidence of adrenal dysfunction ranges from 0 to 60% Diagnostic tests can over diagnosis the occurrence of adrenal insufficiency ~40% of patients would not respond to consyntropin stimulation test and still recover from there illness without glucocorticoid therapy Reproducibility of the tests ~50% of patients may have a positive cosyntropin test one day and a negative test the next Effects of hypoproteinemia Arafah et al. J Clin Endocrinol Metab. 2006;91(10):
15 SCCM and ESICM Recommendations-2017 No recommendation regarding whether to use delta cortisol or a random plasma cortisol for the diagnosis of CIRCI Suggest against using plasma free cortisol level rather than plasm total cortisol level for diagnosis Conditional recommendation, very low quality of evidence Suggest that the high dose cosyntropin (250 mcg) rather than the low-dose (1 mcg) be used for diagnosis of CIRCI Conditional recommendation, low quality of evidence Suggest the use of the ACTH stimulation test rather than the hemodynamic response to hydrocortisone for the diagnosis of CIRCI Conditional recommendation, very low quality of evidence
16 Sepsis and Septic Shock
17 Sepsis and Septic Shock Sepsis Life-threatening organ dysfunction caused by a dysregulated host response to infection Septic shock Vasopressor requirement to maintain a mean arterial pressure of 65 mmhg or greater and serum lactate level greater than 2 mmol/l in the absence of hypovolemia Treatment Antibiotics Fluids Vasopressors Steroids
18 Role of Steroids in Septic Shock Glucocorticoids in sepsis play a beneficial role by: Inhibiting of cytokine production Preventing of migration of circulating inflammatory cells into tissues Enhancing vasoactive tone Increasing catecholamine responsiveness
19 Preventing Septic Shock The HYPRESS trial was conducted to compare hydrocortisone to placebo in the prevention of septic shock (n=353) Hydrocortisone 200 mg IV as a continuous infusion followed by a taper Endpoints: Development of septic shock within 14 days Time until development of septic shock ICU and hospital mortality Need for mechanical ventilation Need for renal replacement therapy Keh D et al. JAMA. 2016;316 (17):
20 Results Development of septic shock, n (%) Placebo (n=170) Hydrocortisone (n=170) p-value 39 (22.9) 36 (21.2) 0.70 ICU mortality, n (%) 14 (8.1) 13 (7.6) 0.85 Hospital mortality, n (%) 22 (12.8) 23 (13.5) 0.86 Mechanical ventilation, n (%) 103 (59.9) 91 (53.2) 0.21 RRT, n (%) 21 (12.2) 21 (12.3) 0.98 Annane D et al. JAMA. 2002;288 (7):
21 Results Cosyntropin stimulation test was performed on 206 patients in the HYPRESS trial Diagnosed with CIRCI: 69/206 (33.5%) Septic shock in placebo group With CIRCI: 27% Without CIRCI: 13.6%, p=0.09 There was no significant difference in any endpoint when comparing patients with or without CIRCI who received hydrocortisone or placebo Annane D et al. JAMA. 2002;288 (7):
22 SCCM and ESICM Recommendations-2017 Suggest against corticosteroid administration in adult patients with sepsis without shock Conditional recommendation, moderate quality of evidence
23 Low Dose Hydrocortisone and Fludrocortisone in Septic Shock Annane et al. completed a randomized, placebo controlled, double blinded study comparing the combination of hydrocortisone with fludrocortisone to placebo in patients with septic shock (n=299) Hydrocortisone 50 mg IV q6h + Fludrocortisone 50 mcg PO daily Treatment was continued for 7 days All patients in the study received the cosyntropin stimulation test Endpoints 28-day survival ICU, hospital, and 1-year mortality Time until vasopressor therapy withdrawal Annane D et al. JAMA. 2002;288 (7):
24 Annane D et al. JAMA. 2002;288 (7):
25 ICU mortality, n (%) Hospital mortality, n (%) 1-year mortality, n (%) Time-tovasopressor withdrawal, d *p<0.05 Non-responders Responders Total Placebo (n=115) Corticosteroid s (n=114) Placebo (n=34) Corticosteroid s (n=36) Placebo (n=149) Corticosteroid s (n=150) 81 (70) 66 (58)* 20 (59) 24 (67) 101 (68) 90 (60) 83 (72) 70 (61)* 20 (59) 25 (69) 103 (69) 95 (63) 88 (77) 77 (68)* 24 (71) 25 (69) 112 (75) 102 (68) 10 7* * Annane D et al. JAMA. 2002;288 (7):
26 CORTICUS Trial Sprung et al. conducted a multicenter, randomized, double-blind, placebocontrolled trial comparing hydrocortisone to placebo in patients with septic shock (n=499) Hydrocortisone 50mg IV q6h x 5 days, then tapered off for a total of 11 days of steroids All patients underwent a cosyntropin stimulation test Endpoints 28 day mortality ICU, hospital, and 1-year mortality rates Reversal of organ system failure ICU and hospital LOS Sprung CL et al. NEJM, 2008;358:111-24
27 Sprung CL et al. NEJM, 2008;358:111-24
28 ICU mortality, n (%) Hospital mortality, n (%) 1-year mortality, n (%) Time to shock reversal, d *p < 0.05 Non-responders Responders Total Placebo (n=108) Hydrocortison e (n=125) Placebo (n=136) Hydrocortisone (n=118) Placebo (n=248) Hydrocortisone (n=251) 44 (40.7) 58 (46.4) 45 (33.3) 41 (34.7) 89 (36) 102 (40.6) 50 (46.3) 60 (48) 50 (37.6) 48 (40.7) 100 (40.8) 111 (44.2) 60 (57.1) 73 (58.9) 67 (53.2) 61 (55) 127 (54) 137 (56.6) 6 3.9* * * Sprung CL et al. NEJM, 2008;358:111-24
29 Comparing Trials SAPS II (placebo/treatment) Annane CORTICUS 57/60 49/50 Received etomidate Excluded* 96 Control group mortality 61% 31.5% Cosyntropin nonresponders Admission category: medical Hospital acquired infection 77% 47% 60% 35% 16% 61% Study powered Yes No
30 Corticosteroids for Treating Sepsis A meta-analysis was completed in 2015 that included 33 studies looking at the use of steroids in sepsis (n=4268) The analysis showed that corticosteroids resulted in: Reduced 28 day mortality (RR=0.87, p=0.05) Reduced ICU mortality (RR=0.82, p=0.04) and in-hospital mortality (RR=0.85, p=0.03) Increased the proportion of shock reversal by day 7 (RR=1.31, p=0.0001) Decreased survivors length of stay in the ICU by 2.19 days Had no effect on gastroduodenal bleeding (RR=1.24, p=0.15) or superinfections (RR=1.02, p=0.81) Increased the risk of hyperglycemia (RR=1.26, p< ) Annane D et al. Cochrane Database Syst Rev. 2015;12
31 SCCM and ESICM Recommendations-2017 Suggest using corticosteroids in patients with septic shock that is not responsive to fluid and moderate- to high-dose vasopressor therapy Conditional recommendation, low quality of evidence If using corticosteroids for septic shock, they suggest using long course and low dose (IV hydrocortisone < 400 mg/day for at least 3 days at full dose) rather than high dose and short course Conditional recommendation, low quality of evidence
32 Acute Respiratory Distress Syndrome (ARDS)
33 Acute Respiratory Distress Syndrome (ARDS) Inflammatory injury to the lung that is characterized by acute hypoxemic respiratory failure Early exudative phase followed by proliferative and fibrotic phase Diagnosis Onset within 7 days of a defined event Bilateral opacities on chest x-ray Respiratory failure not fully explained by cardiac failure or fluid overload Classifications PaO 2 :FiO 2 ratio Mortality Mild % Moderate % Severe < % Fanelli V et al. J Thorac Dis. 2013;5 (3):
34 ARDS Treatment Options Protective mechanical ventilation Prone positioning High frequency oscillatory ventilation Extracorporeal membrane oxygenation Neuromuscular blocking agents Steroids Fanelli V et al. J Thorac Dis. 2013;5 (3):
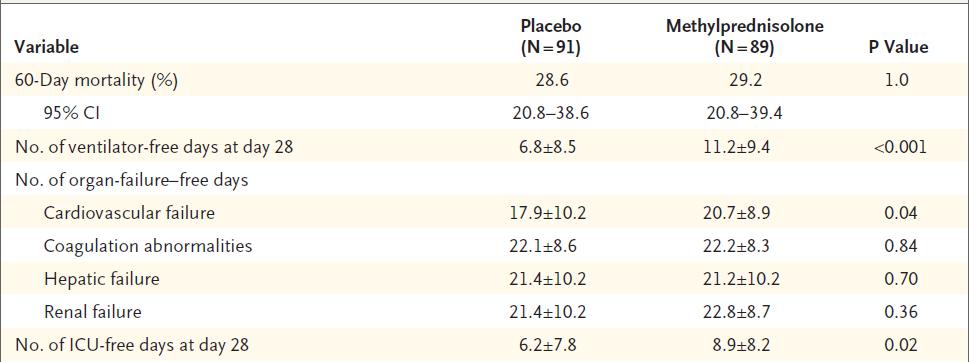
35 Corticosteroids for Persistent ARDS ARDS net group conducted a multicenter randomized controlled trial to determine the efficacy and safety of corticosteroids in ARDS (n=180) Methylprednisolone vs. placebo 2 mg/kg x 1, followed by 0.5 mg/kg q6h for 14 days, followed by 0.5 mg/kg q12h for 7 days Endpoints 60 day mortality Ventilator free days Days without organ failure Infectious complications Steinber KP et al. NEJM. 2006;354:

36 Results
37 Results Resuming ventilator assistance Methylprednisolone: 20 patients Placebo: 6 patients (p=0.008) Significant improvement in the PaO 2 :FiO 2 with the use of methylprednisolone Significant decrease in plateau pressures with methylprednisolone No difference in the development of infection between the groups Conclusion Methylprednisolone had no beneficial effect on survival and when initiated more than 2 weeks after onset of ARDS was associated with increased mortality Steinber KP et al. NEJM. 2006;354:
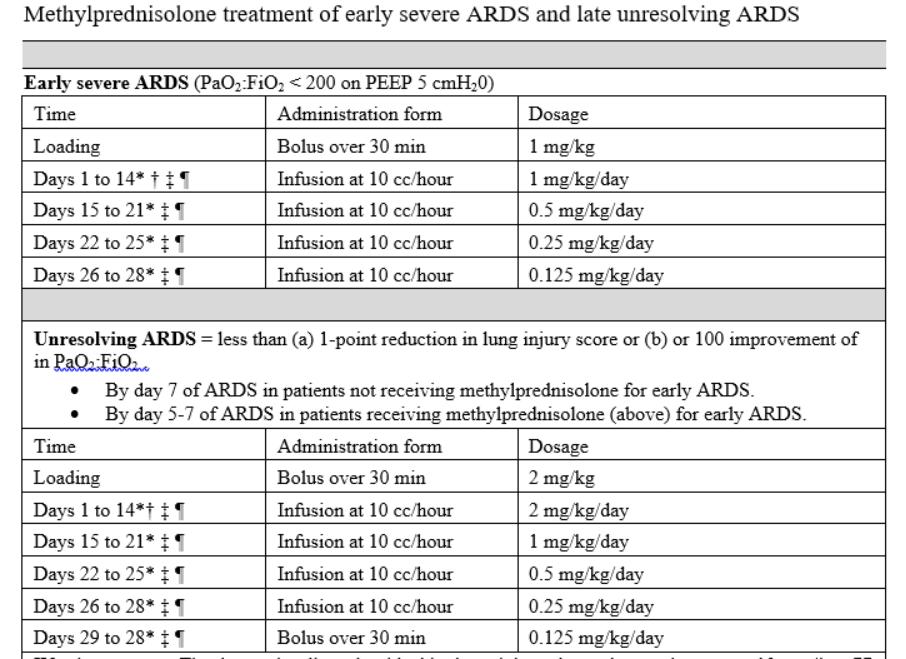
38 Methylprednisolone in Early Severe ARDS A randomized controlled trial conducted by Meduri et al. looked at the use of methylprednisolone within the first 72 hours of ARDS (n=91) All patients underwent a cosyntropin stimulation test Methylprednisolone 1 mg/kg/day for 14 days followed by taper until day 28 Endpoints Improvement in lung injury score (LIS) Improvement in PaO 2 :FiO 2 ratio Duration of mechanical ventilation ICU length of stay ICU mortality Hospital mortality Meduri GU et al. CHEST. 2007;131:
39 Results Meduri GU et al. CHEST. 2007;131:
40 Results Conclusion: Glucocorticoid treatment induced down-regulation of systemic inflammation in ARDS resulting in an improvement in pulmonary dysfunction and reduction in duration of mechanical ventilation and ICU length of stay Meduri GU et al. CHEST. 2007;131:
41 Corticosteroids in Septic Shock with or without ARDS Annane et al. conducted a post-hoc analysis of their previous study that compared hydrocortisone combined with fludrocortisone to placebo in patients with septic shock (n=177) 177 of the initial 299 patients met the criteria for ARDS Endpoints 28 day, ICU, and hospital mortality Days alive and off the ventilator Evolution of PaO 2 :FiO 2 Circulating cytokine levels Annane D et al. Crit Care Med 2006;34 (1):22-30
42 Results for patients with ARDS 28-day mortality, n (%) ICU mortality, n (%) Hospital mortality, n (%) Ventilator free days *p<0.05 Non-responders Responders Total Placebo (n=67) Corticosteroid s (n=62) Placebo (n=25) Corticosteroid s (n=23) Placebo (n=92) Corticosteroids (n=85) 50 (75) 33 (53)* 12 (48) 16 (70) 62 (67) 49 (58) 53 (79) 36 (58)* 14 (56) 17 (74) 67 (73) 53 (62) 53 (79) 37 (60)* 14 (56) 17 (74) 67 (73) 54 (64) 2.6 ± ± 8.6* 4.6 ± ± ± ± 8.4 Annane D et al. Crit Care Med 2006;34 (1):22-30
43 Annane D et al. Crit Care Med 2006;34 (1):22-30
44 Results Cytokine levels IL-6 plasma levels were significantly higher in non-responders IL-6 levels decreased over 7 days in non-responders and values were significantly lower in the steroid group Conclusion The use of hydrocortisone combined with fludrocortisone for 7 days improves 28-day, ICU, and hospital mortality as well as reducing duration of mechanical ventilation in patients with septic shock associated early ARDS who fail to respond to cosyntropin stimulation test Annane D et al. Crit Care Med 2006;34 (1):22-30
45 Prolonged Glucocorticoid Treatment in Patients with ARDS Meduri et al. conducted an individual patient data analysis of four RCT s that used methylprednisolone for the treatment of ARDS (n=322) Early vs. late initiation of steroids Slow vs. rapid taper of steroids Endpoints Time to successful removal of assisted breathing Mechanical ventilation free days ICU free days Hospital mortality Meduri GU et al. Intensive Care Med. 2016;42:
46 Results Time until extubation, d Methylprednisolone (n=186) Placebo (n=136) p-value 12.9 ± ± 13.9 <0.001 MV free days 13.3 ± ± 5.7 <0.001 Achieved extubation by day 28, n (%) 149 (80) 68 (50) <0.001 ICU free days 10.8 ± ± 6.4 <0.001 Hospital mortality 37 (20) 45 (33) Mortality prior to extubation, n (%) 23 (12) 39 (29) <0.001 Meduri GU et al. Intensive Care Med. 2016;42:
47 Prolonged Glucocorticoid Treatment in Patients with ARDS Meduri et al. additionally completed a meta-analysis of the first four RCT s in addition to an additional four RCT s that used hydrocortisone for the treatment of ARDS (n=619) Glucocorticoid treatment was associated with: Increase in mechanical ventilation free and ICU free days Reduced risk of in-hospital mortality (29 vs. 45%, RR=0.56, p=0.009) Reduced risk of mortality when randomized within 14 days (20 vs 48%, RR=0.52, p=0.006) No increased risk of nosocomial infections Meduri GU et al. Intensive Care Med. 2016;42:
48 Results
49 SCCM and ESICM Recommendations-2017 Suggest the use of corticosteroids in patients with early moderate to severe acute respiratory distress syndrome (PaO 2 :FiO 2 < 200 and within 14 days of onset) Conditional recommendation, moderate quality of evidence
50
51 Comparing Guidelines Diagnosis SCCM/ESICM 2008 Surviving Sepsis 2016 SCCM/ESICM 2017 Not recommended to perform ACTH stim test No recommendation ACTH stim test Steroids in Sepsis Septic shock not responsive to fluids or vasopressor therapy Septic shock not responsive to fluids or vasopressor therapy Septic shock not responsive to fluids or vasopressor therapy Steroid Dose Steroids in ARDS 50 mg q6h or 10 mg/h for at least 7 days Early severe ARDS within the first 14 days 200 mg/day <400 mg/day for > 3 days No comment Early moderate to severe ARDS
52 Conclusion Recommended to use ACTH stimulation test rather than the hemodynamic response to hydrocortisone for the diagnosis of CIRCI Corticosteroids should be used in patients with septic shock that is not responsive to fluid and moderate to high-vasopressor therapy A low dose and long duration of steroids are recommended if they are to be used in septic shock Corticosteroids can be used in patients with early moderate to severe ARDS
53 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE
 CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
CORTICOSTEROID USE IN SEPTIC SHOCK THE ONGOING DEBATE DIEM HO, PHARMD PGY1 PHARMACY RESIDENT VALLEY BAPTIST MEDICAL CENTER BROWNSVILLE 1 ABBREVIATIONS ACCP = American College of Chest Physicians ARF =
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX
 Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Should Roids Be the Rage in Septic Shock? Lauren Powell, MSN, RN, CCRN, AGACNP-BC CHI Baylor St. Luke s Medical Center, Houston, TX Learning Objectives 1. Review the mechanism of action for the use of
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Assessing Adrenal Function in Ill, Hospitalized Patients. Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism
 Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Assessing Adrenal Function in Ill, Hospitalized Patients Bruce Redmon, MD Division of Endocrinology, Diabetes and Metabolism Disclosures Very surprised when I received an email two weeks ago disclosing
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA
 DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
DIAGNOSING AND TREATING CORTISOL INSUFFICIENCY IN ICU MOHD BASRI MAT NOR, IIUM, KUANTAN, MALAYSIA Content Glucocorticoid physiology and effects of critical illness on HPA axis Assessment of tissue cortisol
Should we use steroids in sepsis? J.G. van der Hoeven
 Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
Should we use steroids in sepsis? J.G. van der Hoeven Why I don t like it It is boring.. It usually results in emotional outcries in the audience If any, the effects on outcome are very small You are not
Inflammation. Sepsis Ladder
 Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
Maureen Maloney-Poldek MSN, RN Chamberlain College of Nursing Pathophysiology of sepsis and septic shock How sepsis affects the endocrine system Pathophysiology of adrenal insufficiency Clinical manifestations
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK. Alexandria Rydz
 EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
EFFECT OF EARLY VASOPRESSIN VS NOREPINEPHRINE ON KIDNEY FAILURE IN PATIENTS WITH SEPTIC SHOCK Alexandria Rydz BACKGROUND- SEPSIS Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
INVESTIGATIONAL TREATMENTS FOR SEPSIS AN OVERVIEW
 INVESTIGATIONAL TREATMENTS FOR SEPSIS AN OVERVIEW THE GLOBAL BURDEN OF SEPSIS Mortality rate estimated to be 30-50% Rates estimated to be as high as 80% in developing nations One third to one half of all
INVESTIGATIONAL TREATMENTS FOR SEPSIS AN OVERVIEW THE GLOBAL BURDEN OF SEPSIS Mortality rate estimated to be 30-50% Rates estimated to be as high as 80% in developing nations One third to one half of all
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Corticosteroids in Severe CAP. Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand
 Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Top Sepsis Studies
 A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
A75M233/A75M529 Monday 08:00-09:15 Wednesday 14:45-16:00 Maureen A Seckel APRN, ACNS-BC, CCRN, CCNS, FCCM Critical Care CNS and Sepsis Leader Christiana Care Health Services, Newark, DE Top Sepsis Studies
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Polmoniti: Steroidi sì, no, quando. Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma
 Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU
 Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Stressed Out: Evaluating the Need for Stress Ulcer Prophylaxis in the ICU Josh Arnold, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds November 8, 2016 2016 MFMER slide-1 Objectives Identify the significance
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
HYDROCORTISONE SEPSIS: WHY AND WHEN? Eduardo Juan Troster,MD, Cristiane Freitas Pizarro, MD
 HYDROCORTISONE SEPSIS: WHY AND WHEN? Eduardo Juan Troster,MD, PhD Cristiane Freitas Pizarro, MD USE OF CORTICOSTEROID THERAPY IN SEPSIS/SEPTIC SHOCK IS BASED IN SEVERAL ASPECTS: Current epidemiology of
HYDROCORTISONE SEPSIS: WHY AND WHEN? Eduardo Juan Troster,MD, PhD Cristiane Freitas Pizarro, MD USE OF CORTICOSTEROID THERAPY IN SEPSIS/SEPTIC SHOCK IS BASED IN SEVERAL ASPECTS: Current epidemiology of
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Sepsis: Update on Diagnosis, Evaluation and Management
 Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Sepsis: Epidemiology Sepsis: Update on Diagnosis, Evaluation and Management Michael J. Apostolakos, MD Professor of Medicine Director of Adult Critical Care University of Rochester ~ 750,000 cases per
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
A Clinico-pharmacological Study on Effect of Methylprednisolone in Acute Respiratory Distress Syndrome Patients
 Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/135 A Clinico-pharmacological Study on Effect of Methylprednisolone in Acute Respiratory Distress Syndrome Patients
Original Article Print ISSN: 2321-6379 Online ISSN: 2321-595X DOI: 10.17354/ijss/2018/135 A Clinico-pharmacological Study on Effect of Methylprednisolone in Acute Respiratory Distress Syndrome Patients
Should we abandon corticosteroids during septic shock? No Arie Bastiaan Johan Groeneveld, Nienke Molenaar and Bert Beishuizen
 Should we abandon corticosteroids during septic shock? No Arie Bastiaan Johan Groeneveld, Nienke Molenaar and Bert Beishuizen Department of Intensive Care and Institute for Cardiovascular Research, Vrije
Should we abandon corticosteroids during septic shock? No Arie Bastiaan Johan Groeneveld, Nienke Molenaar and Bert Beishuizen Department of Intensive Care and Institute for Cardiovascular Research, Vrije
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
CONFERENCE REPORTS AND EXPERT PANEL
 Intensive Care Med (2017) 43:1751 1763 DOI 10.1007/s00134-017-4919-5 CONFERENCE REPORTS AND EXPERT PANEL Guidelines for the diagnosis and management of critical illness related corticosteroid insufficiency
Intensive Care Med (2017) 43:1751 1763 DOI 10.1007/s00134-017-4919-5 CONFERENCE REPORTS AND EXPERT PANEL Guidelines for the diagnosis and management of critical illness related corticosteroid insufficiency
Relative adrenocorticoid insufficiency exists and should be treated
 Relative adrenocorticoid insufficiency exists and should be treated Steven A R Webb The issue of relative adrenocortical insufficiency (RAI) in septic shock is confused and uncertain. This is a consequence
Relative adrenocorticoid insufficiency exists and should be treated Steven A R Webb The issue of relative adrenocortical insufficiency (RAI) in septic shock is confused and uncertain. This is a consequence
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
SEVERE SEPSIS PLACES A LARGE BURden
 CARING FOR THE CRITICALLY ILL PATIENT CLINICIAN S CORNER Corticosteroids in the Treatment of Severe Sepsis and Septic Shock in Adults A Systematic Review Djillali Annane, MD Eric Bellissant, MD Pierre-Edouard
CARING FOR THE CRITICALLY ILL PATIENT CLINICIAN S CORNER Corticosteroids in the Treatment of Severe Sepsis and Septic Shock in Adults A Systematic Review Djillali Annane, MD Eric Bellissant, MD Pierre-Edouard
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
The Egyptian Journal of Hospital Medicine (January 2018) Vol. 70 (4), Page
 Vol. 70 (4), Page") The Egyptian Journal of Hospital Medicine (January 2018) Vol. 70 (4), Page 708-712 Role of Systematic Steroids in Sepsis and Septic Shock Treatment Outcome: A Systematic Review Jumana Sahal Malibari College
The Egyptian Journal of Hospital Medicine (January 2018) Vol. 70 (4), Page 708-712 Role of Systematic Steroids in Sepsis and Septic Shock Treatment Outcome: A Systematic Review Jumana Sahal Malibari College
Sajeev Menon MD ADRENAL INSUFFICIENCY? FATIGUE? OUTLINE OBJECTIVES PATIENT 1 PATIENT 1 : CLINICAL COURSE
 ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
ADRENAL INSUFFICIENCY? FATIGUE? Sajeev Menon MD Endocrinologist KCIM OBJECTIVES OUTLINE Review primary and adrenal insufficiency including clinical and laboratory findings To appropriately interpret the
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK
 THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK Older people carry the burden of sepsis Older people carry the burden of sepsis Immunosenescence Co-morbidity Endothelial / mucosal atrophy Dependence
THE CRITICALLY ILL OLDER PERSON WITH: SEPTIC SHOCK Older people carry the burden of sepsis Older people carry the burden of sepsis Immunosenescence Co-morbidity Endothelial / mucosal atrophy Dependence
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Special Article. Crit Care Med 2008 Vol. 36, No. 6
 Special Article Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American
Special Article Recommendations for the diagnosis and management of corticosteroid insufficiency in critically ill adult patients: Consensus statements from an international task force by the American
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Identification & Treatment of Sepsis for the Pediatric Population
 Identification & Treatment of Sepsis for the Pediatric Population Priya Narang, PharmD, MS PGY-1 Pharmacy Practice Resident A presentation for HealthTrust Members March 13, 2018 Disclosures This program
Identification & Treatment of Sepsis for the Pediatric Population Priya Narang, PharmD, MS PGY-1 Pharmacy Practice Resident A presentation for HealthTrust Members March 13, 2018 Disclosures This program
Vasopressors in Septic Shock. Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada
 Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
Vasopressors in Septic Shock Keith R. Walley, MD St. Paul s Hospital University of British Columbia Vancouver, Canada Echocardiogram: EF=25% 57 y.o. female, pneumonia, shock Echocardiogram: EF=25% 57 y.o.
The syndrome formerly known as. Severe Sepsis. James Rooks MD. Coordinator of critical care education OU College of Medicine, Tulsa
 The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
The syndrome formerly known as Severe Sepsis James Rooks MD Coordinator of critical care education OU College of Medicine, Tulsa Disclosures I have no actual or practical conflicts of interest in relation
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia. Jess Hwang 11/8/12
 58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Canadian Trauma Trials Collaborative. Occult Pneumothorax in Critical Care (OPTICC): Standardized Data Collection Sheet
: Standardized Data Collection Sheet") Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
Canadian Trauma Trials Collaborative STUDY CENTRE: Institution: City / Province: / Occult Pneumothorax in Critical Care (OPTICC): Standardized Sheet PATIENT DEMOGRAPHICS: First Name: Health record number
CELLULAR IMMUNOTHERAPY FOR SEPTIC SHOCK: CISS Phase I Trial
 CELLULAR IMMUNOTHERAPY FOR SEPTIC SHOCK: CISS Phase I Trial Lauralyn McIntyre, MD, FRCPC, MHSc Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute CCCF MEETING,
CELLULAR IMMUNOTHERAPY FOR SEPTIC SHOCK: CISS Phase I Trial Lauralyn McIntyre, MD, FRCPC, MHSc Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute CCCF MEETING,
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Sprung CL, Annane D, Keh D, et al. Hydrocortisone therapy for
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Diagnosis and Management of Sepsis and Septic Shock. Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire
 Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Diagnosis and Management of Sepsis and Septic Shock Martin D. Black MD Concord Pulmonary Medicine Concord, New Hampshire Financial: none Disclosures Objectives: Identify physiologic principles of septic
Interactive Clinical Forum
 Interactive Clinical Forum The rules for this session Avery Tung, M.D, FCCM Department of Anesthesia and Critical Care University of Chicago 5 decisions embedded in a Clinical Scenario All are clinically
Interactive Clinical Forum The rules for this session Avery Tung, M.D, FCCM Department of Anesthesia and Critical Care University of Chicago 5 decisions embedded in a Clinical Scenario All are clinically
Indications and practical use of replacement dose of corticosteroids in critical illness Josef Briegel, Erich Kilger and Gustav Schelling
 Indications and practical use of replacement dose of corticosteroids in critical illness Josef Briegel, Erich Kilger and Gustav Schelling Purpose of review Ongoing and severe systemic inflammation affecting
Indications and practical use of replacement dose of corticosteroids in critical illness Josef Briegel, Erich Kilger and Gustav Schelling Purpose of review Ongoing and severe systemic inflammation affecting
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: A systematic review and meta-analysis*
 Continuing Medical Education Article Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: A systematic review and meta-analysis* Benjamin M. P. Tang, PhD; Jonathan C. Craig,
Continuing Medical Education Article Use of corticosteroids in acute lung injury and acute respiratory distress syndrome: A systematic review and meta-analysis* Benjamin M. P. Tang, PhD; Jonathan C. Craig,
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Lawrence S. Kirschner, MD, PhD Professor of Medicine
 Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Adrenal Insufficiency: Current Practice 2012 Lawrence S. Kirschner, MD, PhD Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism The Ohio State University s Wexner Medical Center Overview
Etomidate is a short-acting, sedative hypnotic
 Hosp Pharm 2014;49(2):177 183 2014 Thomas Land Publishers, Inc. www.hospital-pharmacy.com doi: 10.1310/hpj4902-177 Original Article Effects of Etomidate on Adrenal Suppression: A Review of Intubated Septic
Hosp Pharm 2014;49(2):177 183 2014 Thomas Land Publishers, Inc. www.hospital-pharmacy.com doi: 10.1310/hpj4902-177 Original Article Effects of Etomidate on Adrenal Suppression: A Review of Intubated Septic
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Intravenous Vitamin C. Severe Sepsis Acute Lung Injury
 Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Objectives. Outline. Sepsis Incidence and Outcomes. Definitions
 Objectives Evaluate recent literature on the management of sepsis Apply new and potentially controversial recommendations from the Surviving Sepsis Guidelines to patient cases. Surviving Sepsis Campaign
Objectives Evaluate recent literature on the management of sepsis Apply new and potentially controversial recommendations from the Surviving Sepsis Guidelines to patient cases. Surviving Sepsis Campaign