Multi-factor approach to reduce cardiovascular risk in diabetes
|
|
|
- Darren Mason
- 6 years ago
- Views:
Transcription



1 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
2 Type 2 diabetes progression: vascular changes and tissue damage Adapted from DeFronzo et al. International Textbook of Diabetes. 3rd edn. New York, NY: John Wiley & Sons; 2004:1141

3 Tissue damage leads to serious long-term complications in type 2 diabetes CHF, congestive heart failure; ESRD, end-stage renal disease; MI, myocardial infarction; TIA, transient ischaemic attack Adapted from Diabetes Atlas 4th edn. International Diabetes Federation. 2009
4 Micro- and macrovascular complications are associated with type 2 diabetes Adapted from Brown et al. Diabetes Obes Metab 2000;2(Suppl. 2):S11 18
5 Microvascular complications of type 2 diabetes
6 UKPDS: glycaemic control effects on microvascular endpoints* HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglycerides Adapted from Stratton et al. BMJ 2000;321:405 12
7 Modifiable CV risk factors are common in patients with T2D 1,2 Hyperglycaemia Hypertension Dyslipidaemia Obesity Almost a third of diabetes patients were current smokers 2 1. Svensson et al. Diab Vasc Dis Res 2013;10: Das et al. Am Heart J 2006;151:
8 ABCs of Type 2 Diabetes: AACE/ACE 2011 and ADA 2011 Target Treatment Goals AACE/ACE 2011 ADA 2011 A1C 6.5% < 7.0% Blood pressure Cholesterol (lipids) <130/80 mm Hg <130/80 mm Hg LDL-C < 100 mg/dl (< 70 mg/dl for patients with diabetes and coronary artery disease) HDL-C > 40 mg/dl in men; > 50 mg/dl in women Triglycerides <150 mg/dl LDL-C < 100 mg/dl (< 70 mg/dl for patients with diabetes and coronary artery disease) HDL-C > 40 mg/dl in men; > 50 mg/dl in women; Triglycerides < 150 mg/dl *In individuals with overt cardiovascluar disease, a lower LDL-cholesterol goal of <70 mg/dl (1.8 mmol/l), using high-dose of a statin, is an option. Handelsman Y, et al. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for AACE Developing Diabetes Mellitus a Diabetes Clinical Mellitus Practice Guidelines Comprehensive Task Force. Care Endocr Plan. Pract. Endocr 2007;13(suppl Pract. 2011;17(Suppl 1): ):1-53. "Standards of Medical of Medical Care in Care Diabetes 2011." in Diabetes Diabetes Care 34(Supplement Care. 34(Supplement 1): S11-S61. 1): S11-S61.
9 Glycemic Control Recommendations for Type 2 Diabetes: AACE/ACE 2011 and ADA 2011 Target Treatment Goals AACE/ACE 2011 ADA 2011 A1C 6.5% < 7.0% Fasting glucose Postprandial glucose Fasting plasma glucose: < 110 mg/dl 2-hr postprandial glucose: < 140 mg/dl Preprandial capillary plasma glucose: mg/dl Peak postprandial capillary plasma glucose: < 180 mg/dl *In Handelsman individuals with Y, overt et al. cardiovascluar American Association disease, a lower of Clinical LDL-cholesterol Endocrinologists goal of <70 Medical mg/dl (1.8 Guidelines mmol/l), using for Clinical high-dose Practice of a statin, for is an option. Developing a Diabetes Mellitus Comprehensive Care Plan. Endocr Pract. 2011;17(Suppl 2):1-53. AACE Diabetes Mellitus Clinical Practice Guidelines Task Force. Endocr Pract. 2007;13(suppl 1):1-68. Standards of Medical Care in Diabetes Diabetes Care. 34(Supplement 1): S11-S61. "Standards of Medical Care in Diabetes 2011." Diabetes Care 34(Supplement 1): S11-S61.

10 Physical exercise: recommendations Adults with diabetes should be advised to perform at least 150 min/week of moderate-intensity aerobic physical activity (50 70% of maximum heart rate), spread over at least 3 days/week with no more than 2 consecutive days without exercise. Class A In the absence of contraindications, adults with type 2 diabetes should be encouraged to perform resistance training at least twice per week. Class A 10

11 ØCaloric restriction is a drastic intervention on eating habits aimed to reduce the caloric intake of about 25%. ü Energy intake of about 1800 kcal/die, rich in fruit, vegetable, nuts, soy and meat Caloric restriction ü Reduced intake of carbohydrates and hydrogenated oils 11 Fontana L et al. JAMA 2009
12 Recent trials of newer glucose-lowering agents on the primary CV outcome HR: 1.0 (95% CI: 0.89, 1.12) SAVOR-TIMI 53 HR: 0.98 (95% CI: 0.88, 1.09) TECOS HR: 0.87 (95% CI: 0.78, 0,97) LEADER HR: 0.96 (95% CI: UL 1.16) EXAMINE DPP-4 inhibitors* GLP-1 analogues Empagliflozin HR: 1.02 (95% CI: 0.89, 1.17) HR: 0.86 (95% CI: 0.74, 0.99) ELIXA EMPA-REG OUTCOME CV, cardiovascular; HR, hazard ratio; DPP-4, dipeptidyl peptidase-4 *Saxagliptin, alogliptin, sitagliptin Adapted From: from Johansen OE. World J Diabetes 2015;6:

13 Primary Composite Cardiovascular Outcome* PP Analysis for Non-inferiority * CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina Green JB et al. NEJM 2015; DOI: /NEJMoa
14 Alogliptin and MACE Hazard ratio, 0.96 (* one-sided repeated CI bound, 1.16) Cumulative Incidence of the Primary End Point (%) Events, No. (%) Placebo: 316 (11.8) Alogliptin: 305 (11.3) Months Placebo (n): Alogliptin (n): * Using alpha=0.01.







15 Urinary glucose excretion via SGLT2 inhibition Filtered glucose load 180 g/day SGLT2 Inhibitor SGLT1 SGLT2 inhibitors reduce glucose re-absorption in the proximal tubule, leading to urinary glucose excretion* and osmotic diuresis *Loss of ~80 g of glucose/day (~240 cal/per day). Gerich JE. Diabet Med. 2010;27:
16 Phase III pooled efficacy and cardiovascular risk factor analysis Placebo-corrected change* from baseline in HbA 1c Adjusted mean (SE) difference versus placebo in change from baseline in HbA1c (%) Pooled data Empagliflozin 10 mg QD Pooled Monotherapy MET PIO MET+SU Insulin 78 week -0, ,6 Empagliflozin 25 mg QD Mild RI Patients, n BL HbA 1c, % BL, baseline; MET, metformin; PIO, pioglitazone; QD, once daily; RI, renal impairment; SE, standard error; SU, sulphonylurea. *All statistically significant unless otherwise marked. Hach T, et al., Häring H-U, et al., Rosenstock J, et al., Barnett A, et al. Diabetes. 2013;(Suppl 1) (P69-LB, P1092, P1102, P1104, respectively); Kovacs C, et al. Diabetes Obes Metab Aug 1. doi: /dom.12188; Häring H-U, et al. Diabetes Care doi: /dc Barnett A, et al. Lancet Diabetes Endocrinol May;2(5): doi: /S (13) Rosenstock J, et al Poster: 931, 49th Annual Meeting of the European Association for the Study of Diabetes, September 2013 Pooled data from 4 pivotal Phase III trials 16
17 Phase III pooled efficacy and cardiovascular risk factor analysis Placebo-corrected change* from baseline in SBP Adjusted mean (SE) difference versus placebo in change from baseline in SBP (mmhg) Pooled data Empagliflozin 10 mg QD Pooled Monotherapy MET PIO MET+SU Insulin 78 week Empagliflozin 25 mg QD Mild RI Patients, n BL SBP (mmhg) Pooled data from 4 pivotal Phase III trials BL, baseline ; MET, metformin; PIO, pioglitazone; QD, once daily; RI, renal impairment; SBP, systolic blood pressure; SE, standard error; SU, sulphonylurea. *All statistically significant unless otherwise marked. Not statistically significant. Hach T, et al., Häring H-U, et al., Rosenstock J, et al., Barnett A, et al. Diabetes. 2013;(Suppl 1) (P69-LB, P1092, P1102, P1104, respectively); Kovacs C, et al. Diabetes Obes Metab Aug 1. doi: /dom.12188; Häring H-U, et al. Diabetes Care doi: /dc Barnett A, et al. Lancet Diabetes Endocrinol May;2(5): doi: /S (13) Rosenstock J, et al Poster: 931, 49th Annual Meeting of the European Association for the Study of Diabetes, September
18 Phase III pooled efficacy and cardiovascular risk factor analysis Placebo-corrected change* from baseline in body weight Adjusted mean (SE) difference versus placebo in change from baseline in body weight (kg) Pooled data Empagliflozin 10 mg QD Pooled Monotherapy MET PIO MET+SU Insulin 78 week Empagliflozin 25 mg QD Mild RI Patients, n BL BW (kg) Pooled data from 4 pivotal Phase III trials BL, baseline; BW, body weight; MET, metformin; PIO, pioglitazone; QD, once daily; RI, renal impairment; SE, standard error; SU, sulphonylurea. *All statistically significant unless otherwise marked. Hach T, et al., Häring H-U, et al., Rosenstock J, et al., Barnett A, et al. Diabetes. 2013;(Suppl 1) (P69-LB, P1092, P1102, P1104, respectively); Kovacs C, et al. Diabetes Obes Metab Aug 1. doi: /dom.12188; Häring H-U, et al. Diabetes Care doi: /dc Barnett A, et al. Lancet Diabetes Endocrinol May;2(5): doi: /S (13) Rosenstock J, et al Poster: 931, 49th Annual Meeting of the European Association for the Study of Diabetes, September
19 104-week study with empagliflozin H2H versus glimepiride Change from baseline in visceral and subcutaneous fat at Week 104* Mean (95% CI) change from baseline in abdominal visceral adipose tissue (cm 3 ) Glimepiride (n = 34) 11.2 Empagliflozin (n = 39) cm 3 (95% CI: -37.1, -7.4) p = Mean (95% CI) change from baseline in subcutaneous adipose tissue (cm 3 ) Glimepiride (n = 34) 17.7 Empagliflozin (n = 39) cm 3 (95% CI: -58.9, -21.1) p < EMPA-REG H2H-SU Glimepiride EMPA 25 mg QD Glimepiride EMPA 25 mg QD Mean baseline (95% CI) (142.4, 207.9) (137.1, 175.3) Mean baseline (95% CI) (297.9, 381.1) 346. (310.6, 381.3) CI, confidence interval; EMPA, empagliflozin; H2H, head-to-head; QD, once daily. *Dedicated sub-study using magnetic resonance imaging; patient participation was optional. Ridderstråle M, et al. Lancet Diabetes Endocrinol. 2014;2:
20 Phase III pooled efficacy and cardiovascular risk factor analysis Change from baseline in uric acid Adjusted mean (SE) change from baseline in uric acid (μmol/l) Empagliflozin Placebo (n = 825) 10 mg QD (n = 830)25 mg QD (n = 822) Mean baseline (95% CI: , ) p < (95% CI: , ) p < Pooled data from 4 pivotal Phase III trials CI, confidence interval; QD, once daily; NS, not significant; SE, standard error. ANCOVA. TS. Adapted from: Hach T, et al. Diabetes. 2013;(Suppl 1) (P69-LB). 21
21 Primary Results of EMPA-REG OUTCOME Summary of primary results. Please refer to manuscript for full details 22

22 42 countries 11,531 pts screened >97 % completed trial >99 % vital status available Patients with T2D at high CV risk 590 sites 7020 pts randomized Placebo Randomisation Target: 691 CV events CV, cardiovascular. Empagliflozin 10 mg Empagliflozin 25 mg On top of standard of care
23 Pre-specified primary and key secondary outcomes Primary outcome 3-point MACE: Time to first occurrence of CV death, non-fatal MI or non-fatal stroke Key secondary outcome 4-point MACE: Time to first occurrence of CV death, non-fatal MI, non-fatal stroke or hospitalisation for unstable angina CV, cardiovascular; MI, myocardial infarction; MACE, Major Adverse Cardiovascular Event 24
24 Baseline characteristics: CV complications Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) Any CV risk factor 2307 (98.9%) 2333 (99.5%) 2324 (99.2%) Coronary artery disease 1763 (75.6%) 1782 (76.0%) 1763 (75.3%) Multi-vessel coronary artery disease 1100 (47.1%) 1078 (46.0%) 1101 (47.0%) History of MI 1083 (46.4%) 1107 (47.2%) 1083 (46.2%) Coronary artery bypass graft 563 (24.1%) 594 (25.3%) 581 (24.8%) History of stroke 553 (23.7%) 535 (22.8%) 549 (23.4%) Peripheral artery disease 479 (20.5%) 465 (19.8%) 517 (22.1%) Single vessel coronary artery disease 238 (10.2%) 258 (11.0%) 240 (10.2%) Cardiac failure* 244 (10.5%) 240 (10.2%) 222 (9.5%) Data are n (%) in patients treated with 1 dose of study drug *Based on narrow standardised MedDRA query cardiac failure 28
25 Cardiovascular outcomes 32
26 Cardiovascular outcomes -14% -38% -32% -35% 33
27 Safety and tolerability 34
28 EMPA-REG OUTCOME : conclusions Empagliflozin reduced risk for 3-point MACE by 14% Empagliflozin reduced hospitalisation for heart failure by 35% Empagliflozin reduced CV death by 38% Empagliflozin improved survival by reducing all-cause mortality by 32% CV, cardiovascular 35
29 EMPA-REG OUTCOME : Summary Empagliflozin was associated with a reduction in HbA1c without an increase in hypoglycaemia, reductions in weight and blood pressure, and small increases in LDL cholesterol and HDL cholesterol Empagliflozin was associated with an increase in genital infections but was otherwise well tolerated MACE, Major Adverse Cardiovascular Event; HDL, high density lipoprotein; LDL, low density lipoprotein 36
30 Number needed to treat (NNT) to prevent one death across landmark trials in patients with high CV risk Simvastatin 1 for 5.4 years Ramipril 2 for 5 years Empagliflozin for 3 years High CV risk 5% diabetes, 26% hypertension Pre-statin era High CV risk 38% diabetes, 46% hypertension Pre-ACEi/ARB era <29% statin T2DM with high CV risk 92% hypertension >80% ACEi/ARB >75% statin S investigator. Lancet 1994; 344: , 2. HOPE investigator N Engl J Med 2000;342:145-53, 37
31
32 Characterization of various GLP1-RA Half-life Dosing Titration injection meal related Duration of Action Reconstitution required? Extra action for device Lixisenatide 1,2 3 hours Once daily yes yes Short no Exenatide BID hours Twice daily yes yes Short no Liraglutide 3 13 hours Once daily Yes no Intermed. no Exenatide QW 5,6 2 weeks Once weekly no no Long yes Albiglutide 7,8 6 8 days Once weekly yes no Long yes Dulaglutide 4-5 days Once weekly No?/ tbd no Long No (invisible needle) 1 Lyxumia Summary of product characteristics. Accessed 14 May Fineman et al. Diabetes Obno/ tbdes Metab 2012;14: Victoza Summary of product characteristics. Accessed 14 May BYETTA Summary of product characteristics. Accessed 14 May BYDUREON Summary of product characteristics. Accessed 14 May Murphy CE. Ann Pharmacother 2012;46: Eperzan Summary of Opinion (EMA). Accessed 14 Feb Meier JJ. Nat Rev Endocrinol 2012;8: Barrington P et al. Obes Metab 2011;13:
33 Change in HbA1c: Once weekly GLP-1RA vs other Injectable therapies
34 LEADER: Study design 9340 patients Double blinded 2-week placebo run-in Placebo run-in Liraglutide mg OD + standard of care Placebo + standard of care Safety follow-up Safety follow-up 2 weeks Duration years 30 days Screening Randomisation (1:1) End of treatment Key inclusion criteria T2DM, HbA 1c 7.0% Antidiabetic drug naïve; OADs and/or basal/premix insulin Age 50 years and established CV disease or chronic renal failure or Age 60 years and risk factors for CV disease Key exclusion criteria T1DM Use of GLP-1RAs, DPP-4i, pramlintide, or rapid-acting insulin Familial or personal history of MEN-2 or MTC CV, cardiovascular; HbA 1c, glycosylated haemoglobin; OAD, oral antidiabetic drug; OD, once daily; T2DM, type 2 diabetes mellitus. Marso SP et al. N Engl J Med DOI: /NEJMoa
35 CV death Patients with an event (%) HR= % CI (0.66 ; 0.93) p=0.007 Patients at risk Time from randomisation (months) Liraglutide Placebo The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; CV, cardiovascular; HR, hazard ratio. Marso SP et al. N Engl J Med DOI: /NEJMoa
36 Non-fatal myocardial infarction Patients with an event (%) HR= % CI (0.75 ; 1.03) p=0.11 Patients at risk Time from randomisation (months) Liraglutide Placebo The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; HR, hazard ratio. Marso SP et al. N Engl J Med DOI: /NEJMoa
37 Non-fatal stroke Patients with an event (%) HR= % CI (0.72 ; 1.11) p=0.30 Patients at risk Time from randomisation (months) Liraglutide Placebo The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; HR, hazard ratio. Marso SP et al. N Engl J Med DOI: /NEJMoa
38 Expanded MACE All-cause death Hospitalisation for HF
39 Expanded MACE CV death, non-fatal MI, non-fatal stroke, coronary revascularisation, or hospitalisation for unstable angina pectoris or heart failure Patients with an event (%) HR= % CI (0.81 ; 0.96) p=0.005 Patients at risk Time from randomisation (months) Liraglutide Placebo The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiovascular event. Marso SP et al. N Engl J Med DOI: /NEJMoa
40 All-cause death Patients with an event (%) Liraglutide Placebo HR= % CI (0.74 ; 0.97) p= Patients at risk Time from randomisation (months) The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; HR, hazard ratio. Marso SP et al. N Engl J Med DOI: /NEJMoa
41 Hospitalisation for heart failure Patients with an event (%) HR= % CI (0.73 ; 1.05) p=0.14 Patients at risk Time from randomisation (months) Liraglutide Placebo The cumulative incidences were estimated with the use of the Kaplan Meier method, and the hazard ratios with the use of the Cox proportional-hazard regression model. The data analyses are truncated at 54 months, because less than 10% of the patients had an observation time beyond 54 months. CI, confidence interval; HR, hazard ratio. Marso SP et al. N Engl J Med DOI: /NEJMoa
42 Conclusion In patients with type 2 diabetes at high risk of cardiovascular events on standard therapy, liraglutide- as compared to placebo-treated patients had lower rates of cardiovascular events and all-cause death Marso SP et al. N Engl J Med DOI: /NEJMoa

43 50 ADA/EASD position statement 2012 Towards the personalization of glycaemic targets Inzucchi S. et al, Diabetes Care. Vol 35 (2012)
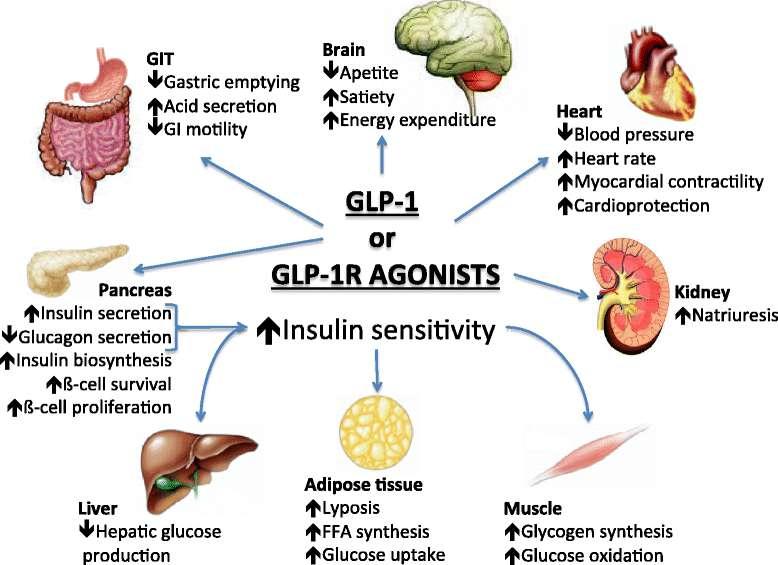
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
Current principles of diabetes management
 Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Current principles of diabetes management Prof. Martin Haluzík, MD, DSc. 3 Department of Medicine, General University Hospital and 1st Faculty of Medicine, Charles University in Prague, Czech Republic
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes
 LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
LEADER Liraglutide and cardiovascular outcomes in type 2 diabetes Presented at DSBS seminar on mediation analysis August 18 th Søren Rasmussen, Novo Nordisk. LEADER CV outcome study To determine the effect
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
CV outcomes Studies and Implications for diabetes management. Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH
 CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
CV outcomes Studies and Implications for diabetes management Seraj Abualnaja, MD, FRCPC Consultant Interventional cardiologist DSFH Case 49 y female with the following medical problems DM typ2 Hypertension
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists
 Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Can We Reduce Heart Failure by Treating Diabetes? CVOT Data on SGLT2 Inhibitors and GLP-1Receptor Agonists Robert R. Henry, MD Professor of Medicine University of California, San Diego Relevant Conflict
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Help the Heart. An Update on GLP-1 Agonists and SGLT2 Inhibitors. Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire
 Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Help the Heart An Update on GLP-1 Agonists and SGLT2 Inhibitors Tara Hawley, PharmD PGY1 Pharmacy Resident Mayo Clinic Health System Eau Claire Mayo Clinic Grand Rounds May 16, 2017 2017 MFMER slide-1
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Management of Type 2 Diabetes Cardiovascular Outcomes Trials Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas
 Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
Management of Type 2 Diabetes Cardiovascular Outcomes Trials 2018 Tom Blevins MD Texas Diabetes and Endocrinology Austin, Texas Speaker Disclosure Dr. Blevins has disclosed that he has received grant support
New Approaches for Treating Challenging Patients with Diabetes
 New Approaches for Treating Challenging Patients with Diabetes Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest
New Approaches for Treating Challenging Patients with Diabetes Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest
Update on Diabetes Cardiovascular Outcome Trials
 Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
Update on Diabetes Cardiovascular Outcome Trials Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of Miami Miller School of Medicine
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials
 Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
Cardiovascular Outcomes With Newer Diabetes Drugs: Results From The EMPA-REG and LEADER Trials Rajiv Roy, MD Endocrinology Sharp Rees-Stealy Medical Group Background Between 1990 and 2010: Incidence of
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Cardiovascular Management of a Patient with Diabetes
 Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Cardiovascular Management of a Patient with Diabetes Dr Jeremy Krebs Clinical Leader Endocrinology and Diabetes Wellington Hospital Summary People with diabetes take a lot of medication Compliance and
Diabetes new challenges, new agents, new order
 Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
Diabetes new challenges, new agents, new order Ken Earle St Georges University Hospitals NHS Foundation Trust Overview Cardiovascular disease unmet needs Treating evident and residual risk Integrating
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
, 2013 and Diabetes Atlas -sixth Edition: IDF 2013") IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013 Diabetes Atlas -sixth Edition: IDF 2013 Chronic complications
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd
 SMC No. (1083/15) Merck Sharp and Dohme UK Ltd") sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
sitagliptin, 25mg, 50mg and 100mg film-coated tablets (Januvia ) SMC No. (1083/15) Merck Sharp and Dohme UK Ltd 07 August 2015 The Scottish Medicines Consortium (SMC) has completed its assessment of the
Type 2 diabetes and cardiovascular risk: the role of GLP-1
 Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
Type 2 diabetes and cardiovascular risk: the role of GLP-1 Dr Isidora Kitsou-Mylona, PhD Novo Nordisk Regional Medical Advisor Business Area Africa, Gulf & India Disclaimer I am an employee of Novo Nordisk
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP
 Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Update on Cardiovascular Outcome Trials in Diabetes Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research InsAtute University of Miami Miller School of Medicine
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
Faculty. Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY
 Faculty Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY 2 Disclosures Robert S. Busch, MD, FACE serves as a speaker for Astra Zeneca,
Faculty Robert S. Busch, MD, FACE Director of Clinical Research Albany Medical Faculty: Community Endocrine Group Albany, NY 2 Disclosures Robert S. Busch, MD, FACE serves as a speaker for Astra Zeneca,
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE
 CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
CARDIOVASCULAR RISK FACTOR CONTROL IN TYPE 2 DIABETES MELLITUS AND NEW TRIAL EVIDENCE *Peter M. Nilsson Department of Clinical Sciences, Lund University, Skåne University Hospital, Malmö, Sweden *Correspondence
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
T2 Diabetes in Sep-16. Stephen Leow Disclosures. Why do we treat diabetes? Agenda. Targets
 Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Stephen Leow Disclosures I have received honoraria, sat on the advisory boards or received grants from Novo Nordisk, Sanofi Aventis, Eli Lilly, Boehringer Ingleheim, Jansenn Cilag, Mundipharma, BioCSL,
Type 2 Diabetes Management: Case 1: Reducing Hypoglycemic Risk Case 2: Reducing Cardiovascular Risk
 Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Type 2 Diabetes Management M. Susan Burke, MD, FACP Clinical Associate Professor of Medicine Sidney Kimmel Medical College at Thomas Jefferson University Senior Advisor, Lankenau Medical Associates Lankenau
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link?
 Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Updates in Diabetes and Cardiovascular Disease Management: Are You Making the Link? Denise Kolanczyk, PharmD, BCPS AQ Cardiology 1 Erika Hellenbart, PharmD, BCPS 2 Jennifer D Souza, PharmD, CDE, BC ADM
Safety profile of Liraglutide: Recent Updates. Mohammadreza Rostamzadeh,M.D.
 Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
Safety profile of Liraglutide: Recent Updates Mohammadreza Rostamzadeh,M.D. Pancreatitis: Victoza post-marketing experience: spontaneous reports of pancreatitis For the majority of the cases, there is
PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL
 Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Dr Aurora Alcantara Endocrinology PHARMACOLOGIC APPROACH TO ACHIEVE GLYCEMIC GOAL SPED Convention and Diabetes Postgraduate Course May26-29 Wyndham Grand Rio Mar, PR DISCLOSURES Speaker for the following
Diabetes and Heart Failure: The Role of SGLT2 Inhibitors
 22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
22 nd Annual Heart Failure 2018 Symposium Diabetes and Heart Failure: The Role of SGLT2 Inhibitors Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Update on Cardiovascular Outcome Trials in Diabetes. Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013
 Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Update on Cardiovascular Outcome Trials in Diabetes Rury R. Holman, FMedSci NIHR Senior Investigator 11 th February 2013 Residual Vascular Risk in People with Diabetes 2 Analyses based on 530,083 participants
Newer Therapies for Type 2 Diabetes
 Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
Newer Therapies for Type 2 Diabetes Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and Metabolism
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes
 Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2018 Cardiologists and HbA1c: Novel Diabetes Drugs and Cardiovascular Disease Outcomes Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI. Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
Terapia con agonisti GLP1 e outcome cardiovascolare. Edoardo Mannucci
 Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Terapia con agonisti GLP e outcome cardiovascolare Edoardo Mannucci Conflitti di interessi Negli ultimi due anni, E. Mannucci ha ricevuto compensi per relazioni e/o consulenze da: Abbott, AstraZeneca,
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus
 Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Diabetes Ther (2017) 8:33 53 DOI 10.1007/s13300-016-0211-x REVIEW Empagliflozin: Role in Treatment Options for Patients with Type 2 Diabetes Mellitus John E. Anderson. Eugene E. Wright Jr.. Charles F.
Newer Diabetes Treatments Drug Class Update with New Drug Evaluation: Semaglutide and Ertugliflozin
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Diabetes Management in CAD Patients. Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts
 Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes Management in CAD Patients Stuart R. Chipkin, MD Research Professor School of Public Health and Health Sciences University of Massachusetts Disclosure Stuart R. Chipkin, MD, FACE Nothing to disclose
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Cardiovascular Impact of Medications for Treating Type 2 Diabetes
 Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
Friday CME Breakfast Lecture Cardiovascular Impact of Medications for Treating Type 2 Diabetes Thomas Blevins, MD Endocrinologist, Private Practice Texas Diabetes and Endocrinology Austin, Texas Educational
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
Drug Class Update with New Drug Evaluation: Non-insulin Diabetes Treatments (SGLT-2 Inhibitors and GLP-1 Receptor Agonists)
") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Dr Tahseen A. Chowdhury Royal London Hospital. New Guidelines in Diabetes: NICE or Nasty?
 Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
Dr Tahseen A. Chowdhury Royal London Hospital New Guidelines in Diabetes: NICE or Nasty? I have no conflicts of interest I do not undertake talks / advisory bodies / research for any pharma company Consultant
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study
 for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study") Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Empagliflozin (Jardiance ) for the treatment of type 2 diabetes mellitus, the EMPA REG OUTCOME study POSITION STATEMENT: Clinicians should continue to follow MHRA advice and NICE technology appraisal guidance
Update Diabetes Therapie. Marc Y Donath
 Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Update Diabetes Therapie Marc Y Donath Recent CV outcome studies in Diabetes N Engl J Med. 2015 373:2117-28 (Empa-Reg outcome study) N Engl J Med. 2016 June 13 (LEADER trial) N Engl J Med. 2017 June 12
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician
 Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Biomarkers 2019 Cardiologists and HbA1c: Novel Diabetes Drugs and the Cardiologist as Diabetician Gregg C. Fonarow, MD, FACC, FAHA, FHFSA Elliot Corday Professor of Cardiovascular Medicine UCLA Division
Metformin should be considered in all patients with type 2 diabetes unless contra-indicated
 November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
November 2001 N P S National Prescribing Service Limited PPR fifteen Prescribing Practice Review PPR Managing type 2 diabetes For General Practice Key messages Metformin should be considered in all patients
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly
 SMC No. (993/14) Boehringer Ingelheim / Eli Lilly") empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly 05 September 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
empagliflozin 10mg and 25mg tablet (Jardiance ) SMC No. (993/14) Boehringer Ingelheim / Eli Lilly 05 September 2014 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants:
 In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
In compliance with the accrediting board policies, the American Diabetes Association requires the following disclosure to the participants: Entity Activity Financial Consideration Comments Novo Nordisk
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know. Hani Sabbour MD FACC FHRS
 Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Cardiovascular risk in diabetes: What the Cardiologist Needs to Know Hani Sabbour MD FACC FHRS Years of life lost Hazard ratio (95% CI) (diabetes vs. no diabetes) CVD is the leading cause of death among
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
What s New in Type 2 Diabetes? 2018 Diabetes Updates Jessica Conklin, PharmD, PhC, BCACP, CDE, AAHIP Associate Professor, UNM College of Phar macy jeconklin@salud.unm.edu Luis Gonzales, PharmD, PhC UNM
New Strategies for Cardiovascular Risk reduction in Diabetes
 New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
New Strategies for Cardiovascular Risk reduction in Diabetes Dr. Godwin LEUNG Tat Chi MB ChB(HK), MRCP (UK), FHKCP, FHKAM (Medicine) FRCP (Glasg), FACC Specialist in Cardiology % event as first CV event
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Dr Brandon Orr-Walker
 Dr Brandon Orr-Walker Endocrinologist Clinical Head of Endocrinology and Diabetes Middlemore Auckland 17:45-18:10 What Can New Agents Offer Us? Diabetes Management What do the new agents offer us? Brandon
Dr Brandon Orr-Walker Endocrinologist Clinical Head of Endocrinology and Diabetes Middlemore Auckland 17:45-18:10 What Can New Agents Offer Us? Diabetes Management What do the new agents offer us? Brandon
The Flozins Quest for Clarity?
 The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
The Flozins Quest for Clarity? Choosing Wisely with Academic Detailing 2018 ARE THEY THE REAL DEAL Disclosure statements The Academic Detailing Service is operated by Dalhousie Continuing Professional
Class Update: Sodium-glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Class Update: Sodium glucose Cotransporter 2 (SGLT2) Inhibitors
 Inhibitors") Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Making Sense of New DM Therapies and Technologies
 Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Making Sense of New DM Therapies and Technologies Sandra Indacochea Sobel, MD Clinical Assistant Professor of Medicine Clinical Chief of Endocrinology, UPMC Mercy Division of Endocrinology, Diabetes, and
Welcome and Introduction
 Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Welcome and Introduction This presentation will: Define obesity, prediabetes, and diabetes Discuss the diagnoses and management of obesity, prediabetes, and diabetes Explain the early risk factors for
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University
 Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Managing Perioperative Diabetes What s new? Kathryn A. Myers MD FRCPC Chair Chief Division of GIM Professor of Medicine Western University Objectives: By the end of this session, you will be able to: Identify
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit?
 Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
Intensifying Treatment Beyond Monotherapy in T2DM: Where Do Newer Therapies Fit? Vanita R. Aroda, MD Scientific Director & Physician Investigator MedStar Community Clinical Research Center MedStar Health
TRANSPARENCY COMMITTEE
 The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 17 December 2014 JARDIANCE 10 mg, film-coated tablet B/30 tablets (CIP: 34009 278 928 5 1) JARDIANCE 25 mg, film-coated
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM
 Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Let s not sugarcoat it! Update on Pharmacologic Management of Type II DM Gregory Castelli, PharmD, BCPS, BC-ADM Clinical Pharmacist UPMC St. Margaret Objectives By the end of this presentation, participants
Why is Earlier and More Aggressive Treatment of T2 Diabetes Better?
 Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Blood glucose (mmol/l) Why is Earlier and More Aggressive Treatment of T2 Diabetes Better? Disclosures Dr Kennedy has provided CME, been on advisory boards or received travel or conference support from:
Where are we with Incretin Based Therapies for the Treatment of Diabetes?
 Where are we with Incretin Based Therapies for the Treatment of Diabetes? Jens Juul Holst, NNF Center for Basic Metabolic Research Department of Biomedical Sciences Panum Institute, University of Copenhagen,
Where are we with Incretin Based Therapies for the Treatment of Diabetes? Jens Juul Holst, NNF Center for Basic Metabolic Research Department of Biomedical Sciences Panum Institute, University of Copenhagen,
Management of Type 2 Diabetes Mellitus. Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism
 Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Management of Type 2 Diabetes Mellitus Heather Corn, MD, MS Endocrinology, Diabetes, and Metabolism Disclosures Working for Intermountain Healthcare Some of the views represented are the opinion of ABIM-certified
Preventing Serious Health Consequences of Type 2 Diabetes
 Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton
Preventing Serious Health Consequences of Type 2 Diabetes The Evidence Hertzel C. Gerstein MD MSc FRCPC Professor and Population Health Institute Chair in Diabetes Research McMaster University and Hamilton