Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies. Module D
|
|
|
- Conrad Cox
- 6 years ago
- Views:
Transcription

1 Advances in Outpatient Diabetes Care: Algorithms for Care and the Role of Injectable Therapies Module D 1
2 Learning Objectives Apply the principles of the comprehensive diabetes algorithms to patients with type 2 diabetes Design therapeutic options to dual therapy in patients not well-controlled by metformin alone that are associated with a low risk of hypoglycemia and weight gain Identify therapeutic options for prandial control in basal insulin treated patients other than prandial insulin when intensification of therapy is required 2
 Only modestly active Family history: brother treated for T2DM Hypertension Lisinopril 20 mg daily BMI = body mass index; DM = diabetes mellitus; T2DM = type 2 diabetes mellitus. 3")
3 Case Study: Philip 65-year-old African- American man Retired executive, lives with wife Hospital admission for motor vehicle accident medical history No prior history of DM Polyuria, fatigue BMI = 30 kg/m 2 (overweight) Only modestly active Family history: brother treated for T2DM Hypertension Lisinopril 20 mg daily BMI = body mass index; DM = diabetes mellitus; T2DM = type 2 diabetes mellitus. 3
4 Admission Orders Consider obtaining an A1C level in patients with Diabetes admitted to the hospital if the result of testing in the previous 2 3 months is not immediately available Risk factors for undiagnosed diabetes who exhibit hyperglycemia in the hospital A1C = glycated hemoglobin. Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1): American Diabetes Association. Diabetes Care. 2014;37(suppl 1):S





5 Diagnosis and Recognition of Hyperglycemia and Diabetes in the Hospital Setting Admission Assess all patients for a history of diabetes Obtain laboratory BG testing on admission No history of diabetes BG <140 mg/dl No history of diabetes but BG >140 mg/dl History of diabetes Initiate POC BG monitoring according to clinical status Start POC BG monitoring x 24-48h Check A1C level Glucose management and monitoring A1C 6.5% POC BG = point-of-care blood glucose testing. Adapted from Umpierrez GE et al; Endocrine Society. J Clin Endocrinol Metab. 2012;97(1):
6 Percent Hyperglycemia in the Hospital and Status Post-Discharge Sample of a managed care outpatient database (8547 patients) with linkage to inpatient data from June 1, 2003, to June 30, Nearly 60% of patients either had DM or manifested hyperglycemia (defined here as BG >130 mg/dl) Established diabetes Newly diagnosed diabetes Returned to normoglycemia, but had stress hyperglycemia Waddell M et al. Postgrad Med. 2009;121(3):
7 Philip Workup and Diagnosis Admission A1C = 9.1% FPG = 195 mg/dl Normal sensory exam BP = 135/80 mm Hg BMI = 30 kg/m 2 Diagnosis: newly diagnosed uncontrolled T2DM Philip is treated with basal-bolus insulin in the hospital to a BG <140 mg/dl BP = blood pressure; FPG = fasting plasma glucose. 7
8 Discharge Considerations What are your discharge plans for this patient? Will he be discharged on insulin therapy? When and where will follow-up take place? What education does he need prior to discharge?

; if it is 35>")
9 Guideline Approach to Therapy in Patients With Newly Diagnosed Type 2 Diabetes Applying It to Philip Lifestyle intervention ± metformin Will we implement with this patient? Yes or No Lifestyle intervention is cornerstone therapy for all patients and most patients will receive metformin unless they have contraindications or can t tolerate it Depending on his A1C level, consider combination therapy or insulin If A1C level not at target (3 6 months), we ll add more therapy eg, If A1C 7.5%: consider combination therapy. If A1C 9: consider insulin This will depend on his BMI Let s come back and talk about where Philip is For example, if his BMI <30, DPP-4 inhibitor (consider GLP-1 RA, SGLT-2 inhibitor); if it is 35> BMI >30, GLP-1 RA, SGLT-2 inhibitors DPP-4 inhibitor and if BMI >35, GLP-1 RA, SGLT-2 inhibitors Consider bariatric surgery in nonresponders Raz I. Diabetes Care. 2013;36(suppl 2):S139 S144. 9
10 Setting Glycemic Goals for Philip Age 64 years BMI 28.6 kg/m 2 (overweight) A1C level Elevated on admission at 9.1% Lifestyle Only moderately active Cardiovascular Well-controlled hypertension (135/80 mm Hg) History of myocardial infarction Lipid profile not optimal (LDL <70 mg/dl but HDL not at goal) What glycemic goal would you set for Philip? What other treatment goals should he have? 10


11 Reducing the Risk of T2DM Complications: Comprehensive Diabetes Management American Diabetes Association. Diabetes Care. 2014;37(suppl 1):S14 S80. 11
:1364 1379. Ismail-Beigi F et al. Ann Intern Med. 2011;154(8):554 559. 12")
12 Setting Individualized Glycemic Goals in T2DM 2012 ADA/EASD Position Statement ADA = American Diabetes Association; EASD = European Association for the Study of Diabetes. Inzucchi S et al. Diabetes Care. 2012;35(6): Ismail-Beigi F et al. Ann Intern Med. 2011;154(8):
13 Philip Target A1C level: 7.0% Physician begins discussing pharmacotherapy for Philip Diabetes educator consult Patient education Detailed dietary and exercise recommendations Weight-loss strategies 13
14 Weight Reduction in T2DM Calorie restriction Key factor for weight loss Moderate calorie restriction recommended kcal/day fewer than baseline intake Dietary changes Reduce saturated and trans fatty acids, cholesterol, and sodium Behavioral modification Self-monitoring of food intake with daily log Stimulus control Cognitive restructuring Stress management Physical activity At least 150 minutes/week of moderate activity Aerobic, resistance, flexibility training In patients with T2DM, weight loss and exercise can reduce insulin resistance and hepatic glucose production. Bantle JP et al. Diabetes Care. 2008;31(suppl 1):S61 S78; Brown A et al. Postgrad Med. 2010;122(1): ; Inzucchi SE et al. Diabetologia. 2012;55(6): ; Ismail-Beigi F. N Engl J Med. 2012;366(14): ; National Institutes of Health. Obes Res. 1998;6(suppl 2):51S 209S. 14
15 LOOK AHEAD Study Intensive Lifestyle Intervention and Risk Reduction Primary objective To examine, in overweight volunteers with T2DM, the longterm effects of an intensive lifestyle intervention program designed to achieve and maintain weight loss by decreased caloric intake and increased physical activity Comparison Control condition involving a program of diabetes support and education Look AHEAD Research Group. Arch Intern Med. 2010;170(17):
16 LOOK AHEAD Study Intensive Lifestyle Intervention and Risk Reduction Diet modification, exercise, behavioral training Group support with in-person and telephone follow-ups Parameter Lifestyle Intervention (n = 2570) Support and Education (n = 2575) Weight loss, % a Treadmill fitness, % METS a A1C level a Systolic BP, mm Hg a Diastolic BP, mm Hg b HDL-C, mg/dl a Triglycerides, mg/dl b a P <0.001; b P = HDL-C = high-density lipoprotein cholesterol; MET = metabolic equivalent. Look AHEAD Research Group. Arch Intern Med. 2010;170(17):
17 Effect of Antihyperglycemic Drugs on A1C Level, Hypoglycemia, Weight (Injectable Therapies Are Highlighted) Drug A1C Reduction (%) Hypoglycemia Incidence (%) a Weight Effects (kg) Sulfonylureas Pioglitazone a +0.9 to +2.6 Linagliptin a No change Saxagliptin a 0.1 to 1.2 Sitagliptin <3-5 a 0.2 to 0.8 Exenatide twice daily to 3.1 Liraglutide to 2.26 Exenatide once weekly SGLT-2 inhibitors to 2.2 Basal insulin b c to +4 a Similar to placebo. b Includes NPH, insulin glargine, and insulin detemir. c No dose or A1C-lowering limit. Exenatide once weekly not approved for use with basal insulin. Adapted from Boland CL et al. Ann Pharmacother. 2013;47(4): ; and Monami M et al. Diabetes Obes Metab. 2014;16(5):
18 Philip Discharge Planning Discuss with the patient the need for basal insulin in addition to oral agents Educator to provide hands-on instruction on administration techniques Provide education to caregiver/family if possible Comprehensive outpatient education should be scheduled Philip is discharged on oral metformin 1000 mg bid and a basal insulin pen device, 0.2 u/kg in the evening with instructions to self-titrate to an FPG level of mg/dl Some might suggest lower boundary of 80 mg/dl as in algorithm, given that Philip is new to insulin and has a prior history of myocardial infarction 18
19 Predischarge Checklist Diet information Monitor/strips & Rx Rx for/supplies of medications, insulin, needles Treatment goals Contact phone numbers Medi-Alert bracelet Survival Skills training Meal planning Sick day planning Involve nursing, dietitian, diabetes educator 19
20 Survival Skills to Be Taught Before Discharge Basic understanding of what diabetes is How and when to take diabetes medications Basic knowledge of effect of carbohydrates on glucose levels Recognition, treatment, and prevention of hypoglycemia Self-monitoring of BG and implication of results What to do during illness How to dispose of lancets and insulin syringes Moghissi ES et al; American Association of Clinical Endocrinologists; American Diabetes Association. Endocr Pract. 2009;15(4):
21 Transition to Discharge Does patient have a glucose monitor for home use? Is patient clear about the diabetes therapy after discharge? Does patient have appropriate outpatient follow-up appointment with primary care, specialist, diabetes specialist clinic? Additional attention to difficulties with insurance, transportation, etc Divide material up throughout course of hospital stay; support and reinforce with written material; ensure that follow-up connection is made with outpatient provider 21
22 Specific Advantages of Main Drug Classes Metformin First-line therapy in most consensus algorithms Large safety margin Can be used by most patients Decreases hepatic glucose production, has a mild effect on peripheral resistance, and increases both total and active endogenous GLP-1 in response to food Might also be cardioprotective in obese T2DM patients Reduction in mortality in UKPDS Lowers risk of cancer in T2DM patients Insulin Most powerful agent to lower glucose; no dose limit to efficacy; indicated when A1C levels above 9% Garber AJ et al. Endocr Pract. 2013;19(3): Inzucchi SE et al. Diabetes Care. 2012;35(6): Raz I. Diabetes Care. 2013;36(suppl 2):S139 S




23 Guideline Approach to Therapy in Patients With Newly Diagnosed Type 2 Diabetes Philip Set A1C goal 7% Lifestyle intervention ± metformin If A1C 7.5%: consider combination therapy Diet, exercise program set up Metformin 1 g bid prescribed Yes, metformin + insulin If A1C 9%: consider insulin Yes, Basal insulin started, titrated against FPG Raz I. Diabetes Care. 2013;36(suppl 2):S139 S




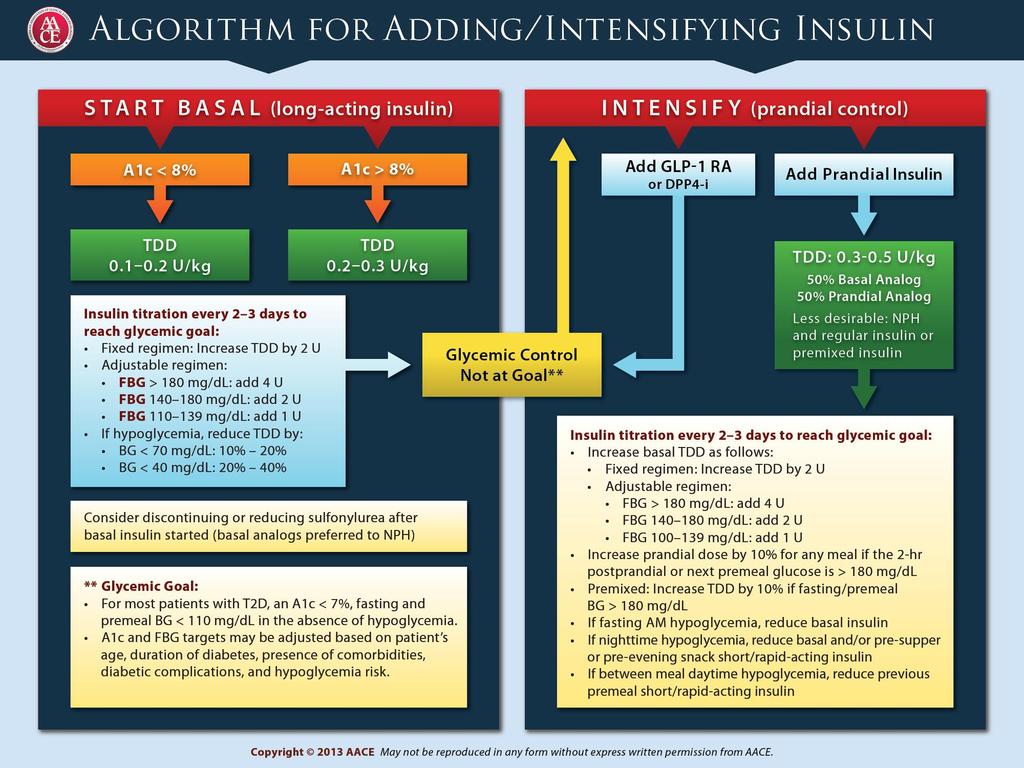
24 Initiation and Adjustment of Insulin Regimens Start once-a-day long-acting insulin analog or NPH bedtime or morning Starting dose 10 units or 0.2 units/kg Titrate against FPG until in target range ( mg/dl) Increase dose typically by 2 units q 3 days Can increase dose by 4 units q 3 days if BG >180 mg/dl If hypoglycemia occurs or if BG <70 mg/dl Reduce dose by 4 U, or by 10% if dose is >60 U Adapted from Nathan DM et al. Diabetes Care. 2009;32(1):
25 Philip Sees Primary Care Physician at 6 Months Basal insulin dose is 30 units, FPG is between 80 and 110 mg/dl most days PPG is between 180 and 220 mg/dl BMI = 30 kg/m 2 He denies any symptoms of hypoglycemia How would you modify his injectable therapy? Continue to titrate basal insulin therapy? Add prandial insulin? Add a GLP-1 RA? PPG = postprandial glucose. 25
26 26

27 Guideline Approach to Therapy in Patients With Newly Diagnosed Type 2 Diabetes Step Action in Philip Set A1C goal 7% Lifestyle intervention ± metformin If A1C 7.5%: consider combination therapy If A1C 9%: consider insulin Metformin 1 mg bid Set up with dietitian, exercise trainer Yes, metformin + basal insulin Basal insulin started, titrated against FPG (conservative dosing discontinuation of nutritional and correction dosing used in hospital) With SMBG 1 4 times/day orders for test strips, lancets, syringes, needles (unless a pen ordered), and a glucagon kit If A1C not at target (3 6 months), add an agent, depending on BMI BMI <30 kg/m 2 35> BMI >30 kg/m 2 BMI >35 kg/m 2 DPP-4 inhibitor (Consider GLP-1 RA, SGLT-2 inhibitor) GLP-1 RA, SGLT-2 inhibitors DPP-4 inhibitors GLP-1 RA, SGLT-2 inhibitors Consider bariatric surgery in nonresponders Raz I. Diabetes Care. 2013;36(suppl 2):S139 S

28 Role of Incretin-based Therapies in Reducing Hyperglycemia Ussher JR, Drucker DJ. Endocr Rev. 2012;33(2):
29 GLP-1 Receptor Agonists Place in Therapy: ADA/EASD Recommendations Second-line in addition to metformin In 3-drug combinations With basal insulin Among preferred agents in specific situations When goal is to avoid hypoglycemia When goal is to avoid weight gain Actions complement those of commonly used antihyperglycemic agents Class Effectiveness Cellular Mechanism Primary Physiologic Actions Insulin Highest Activate insulin receptors GLP-1 RA High Activate GLP-1 receptors Inzucchi SE et al. Diabetes Care. 2012;35(6): Glucose disposal Hepatic glucose production Insulin secretion (glucose dependent) Glucagon secretion (glucose dependent) Satiety 29
30 GLP-1 Receptor Agonists Place in Therapy in the AACE 2013 Algorithm Recommended for treatment-naïve patients at every A1C level as Monotherapy or Part of combination-therapy regimens Both oral or with insulin Based on multifactorial mechanism of action, glucose-dependent mechanism of action (low risk of hypoglycemia), and potential for weigh loss/no risk of weight gain Garber AJ et al. Endocr Pract. 2013;19(3):
31 Marketed GLP-1 Receptor Agonists Characteristic Exenatide bid Liraglutide Exenatide ER Albiglutide Dulaglutide Initial US approval Trade name Byetta Victoza Bydureon Tanzeum Trulicity Description Synthetic exendin-4, a peptide identified in H. suspectum; activates GLP-1 receptors and is resistant to DPP-4 degradation GLP-1 modified to be resistant to DPP-4 degradation Exenatide contained in hydrolyzable polymer microspheres for extended release GLP-1 modified to be resistant to DPP-4 degradation GLP-1 modified to be resistant to DPP-4 degradation Administration Subcutaneous injection Half-life 2.4 hours 13 hours >1 week 5 days 5 days Dosing 2 daily, before meals 1 daily, anytime 1 weekly 1 weekly 1 weekly 1. Byetta (exenatide) [prescribing information]. 2. Victoza (liraglutide) [prescribing information]. 3. Bydureon (exenatide extendedrelease for injectable suspension) [prescribing information]. 4. Tanzeum (albiglutide) [prescribing information]. 5. Trulicity (dulaglutide) [prescribing information].
32 GLP-1 Receptor Agonists FDA-Approved Agents Liraglutide Albiglutide Dulaglutide Exenatide Exenatide ER Key Features Injectable administration Mimic action of native GLP-1 Increase glucose-dependent insulin secretion Suppress glucagon production in glucosedependent manner Slow gastric emptying Increase satiety (reducing appetite/food intake) ER = extended release; GLP-1 = glucagon-like peptide 1. Garber AJ et al. Endocr Pract. 2013;19(suppl 2):
33 Placebo-adjusted A1C (%) Glucose Control With GLP-1 Receptor Agonists Placebo-adjusted Change From Baseline (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alb 1 Dul 2 Exe 3 Exe ER 4 Lir 5 Alb 6 Dul 7 Exe 8 Exe ER 9 Lir 10 Alb 11, * Exe 12 Exe ER 13, Lir 14 Baseline A1C (%) *Metformin with or without SU or TZD. Metformin with or without SU. Absolute change from baseline (active-controlled trial). 1. Tanzeum (albiglutide) injection [prescribing information]. Research Triangle Park, NC: GlaxoSmithKline; Umpierrez G et al. Diabetes Care. 2014;37: Moretto TJ et al. Clin Ther. 2008;30: Russell-Jones D et al. Diabetes Care. 2012;35: Garber A et al. Lancet. 2009;373: Ahrén B et al. Diabetes Care. 2014;37: Dungan KM et al. Lancet. 2014;384: DeFronzo RA et al. Diabetes Care. 2005;28: Bergenstal RM et al. Lancet. 2010;376: Pratley RE et al. Lancet. 2010;375: Pratley RE et al. Lancet Diabetes Endocrinol. 2014;2: Buse JB et al. Diabetes Care. 2004;27: Diamant M et al. Lancet. 2010;375: Marre M et al. Diabet Med. 2009;26:
34 Weight (kg) Weight Change With GLP-1 Receptor Agonists Absolute Change From Baseline (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alb 1 Dul 2 Exe 3 Exe ER 4 Lir 5 Alb 6 Dul 7 Exe 8 Exe ER 9 Lir 10 Alb 11, * Exe 12 Exe ER 13, Lir *Metformin with or without SU or TZD. Metformin with or without SU. 1. Tanzeum (albiglutide) injection [prescribing information]. Research Triangle Park, NC: GlaxoSmithKline; Umpierrez G et al. Diabetes Care. 2014;37: Moretto TJ et al. Clin Ther. 2008;30: Russell-Jones D et al. Diabetes Care. 2012;35: Garber A et al. Lancet. 2009;373: Ahrén B et al. Diabetes Care. 2014;37: Dungan KM et al. Lancet. 2014;384: DeFronzo RA et al. Diabetes Care. 2005;28: Bergenstal RM et al. Lancet. 2010;376: Pratley RE et al. Lancet. 2010;375: Pratley RE et al. Lancet Diabetes Endocrinol. 2014;2: Buse JB et al. Diabetes Care. 2004;27: Diamant M et al. Lancet. 2010;375: Marre M et al. Diabet Med. 2009;26:
35 Patients (%) Hypoglycemia With GLP-1 Receptor Agonists Percentage of Patients Reporting Hypoglycemia (Not Head-to-Head Trials) Monotherapy Add-on to Metformin Add-on to SU Alb 1 Dul 2 Exe 3 Exe ER 4 Lir 5 Alb 6 Dul 7 Exe 8 Exe ER 9 Lir 10 Alb 11, * Exe 12 Exe ER 13, Lir *Metformin with or without SU or TZD. Metformin with or without SU. 1. Nauck M et al. Diabetes. 2013;62(suppl 2): Abstr. 55-LB. 2. Umpierrez G et al. Diabetes Care. 2014;37: Moretto TJ et al. Clin Ther. 2008;30: Russell-Jones D et al. Diabetes Care. 2012;35: Garber A et al. Lancet. 2009;373: Ahrén B et al. Diabetes Care. 2014;37: Dungan KM et al. Lancet. 2014;384: DeFronzo RA et al. Diabetes Care. 2005;28: Bergenstal RM et al. Lancet. 2010;376: Pratley RE et al. Lancet. 2010;375: Pratley RE et al. Lancet Diabetes Endocrinol. 2014;2: Buse JB et al. Diabetes Care. 2004;27: Diamant M et al. Lancet. 2010;375: Marre M et al. Diabet Med. 2009;26:

36 Weight* (kg) GLP-1 Receptor Agonist Weight Effects in Patients With T2DM Meta-analysis of Published Studies Exenatide Liraglutide Exenatide ER % of patients lost weight With exenatide bid or exenatide ER: ~10% lost >10 kg ~20% lost 5 10 kg ~48% lost 0 5 kg ~20% 23% gained 0 5 kg ~1% 2% gained 5 10 kg -3.0 * Weight changes in patients treated for 12 weeks. Aroda VR et al. Clin Ther. 2012;34: ; Buse JB et al. Lancet. 2009;374:39 47; Drucker DJ et al. Lancet. 2008;372: ; Blevins T et al. J Clin Endocrinol Metab. 2011;96: ; Rosenstock J et al. Presented at: 47 th EASD Annual Meeting. 2011; Abstract 786; Buse J et al. Lancet. 2013;381: ; Pratley RE et al. Presented at: 72 nd ADA Scientific Sessions. 2012; Abstract 945-P. 36
37 Safety Considerations With GLP-1 Receptor Agonists GI adverse events Pancreatitis Renal impairment CV Common Usually dose-dependent and transient Usually reduced with dose titration Pancreatitis has been reported with postmarketing use of some of incretin agents, although no causal relationship has been established Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs. other agents Labeling for all incretins states these agents should be immediately discontinued if pancreatitis is suspected Labeling for GLP-1 receptor agonists suggests consideration of other therapies for patients with a history of pancreatitis Renal Impairment has been reported postmarketing, usually in association with nausea, vomiting, diarrhea, or dehydration. Use caution when initiating or escalating doses in patients with renal impairment. Exenatide is contraindicated in patients with severe renal insufficiency or ESRD Small increase in pulse rate with these agents, although the clinical significance is not known ER = extended release; MTC = medullary thyroid carcinoma. Garber AJ et al. Endocr Pract. 2013;19(suppl 2):1 48. ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28,
38 Safety Considerations With GLP-1 Receptor Agonists Pancreatic cancer Medullary thyroid cancer Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs. other agents Further assessments required from long-duration controlled studies or epidemiologic databases Animal data showed an increased incidence of C-cell tumors with liraglutide and exenatide ER treatment, but confirmatory population studies are lacking Labeling for albiglutide, dulaglutide, exenatide ER, and liraglutide: Patients should be counseled regarding MTC and the signs/symptoms of thyroid tumors Contraindicated in patients with personal/family history of MTC or multiple endocrine neoplasia syndrome type 2 ER = extended release; MTC = medullary thyroid carcinoma. Garber AJ et al. Endocr Pract. 2013;19(suppl 2):1 48. ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28,
GLP-1 (glucagon-like peptide-1) Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary
 Agonists (Byetta, Bydureon, Tanzeum, Trulicity, Victoza ) Step Therapy and Quantity Limit Criteria Program Summary") OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) s (Byetta/exenatide, Bydureon/ exenatide extended-release, Tanzeum/albiglutide, Trulicity/dulaglutide, and Victoza/liraglutide) Step Therapy
Initiating Injectable Therapy in Type 2 Diabetes
 Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Initiating Injectable Therapy in Type 2 Diabetes David Doriguzzi, PA C Learning Objectives To understand current Diabetes treatment guidelines To understand how injectable medications fit into current
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol
 Agonists Drug Class Prior Authorization Protocol") Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Glucagon-like peptide-1 (GLP-1) Agonists Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Multiple Factors Should Be Considered When Setting a Glycemic Goal
 Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Multiple Facts Should Be Considered When Setting a Glycemic Goal Patient attitude and expected treatment effts Risks potentially associated with hypoglycemia, other adverse events Disease duration Me stringent
Injectable Agents for Type 2 Diabetes. Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017
 Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Injectable Agents for Type 2 Diabetes Richard Christensen, MD AACE Diabetes Day, Boise, ID September 2017 Financial Disclosures Sanofi speaker honoraria No other relevant financial disclosures Injectable
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE. CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010
 Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Practical Strategies for the Clinical Use of Incretin Mimetics CME/CE Robert R. Henry, MD Authors and Disclosures CME/CE Released: 09/15/2009; Valid for credit through 09/15/2010 Introduction Type 2 diabetes
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
A Practical Approach to the Use of Diabetes Medications
 A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
A Practical Approach to the Use of Diabetes Medications Juan Pablo Frias, M.D., FACE President, National Research Institute, Los Angles, CA Clinical Faculty, University of California, San Diego, CA OUTLINE
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES
 INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
INJECTABLE THERAPY FOR THE TREATMENT OF DIABETES ARSHNA SANGHRAJKA DIABETES SPECIALIST PRESCRIBING PHARMACIST OBJECTIVES EXPLORE THE TYPES OF INSULIN AND INJECTABLE DIABETES TREATMENTS AND DEVICES AVAILABLE
Presented By: Creative Educational Concepts, Inc. Lexington, KY
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of April 2015. The content and views presented in this educational activity are those of the
Insulin Initiation and Intensification. Disclosure. Objectives
 Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Insulin Initiation and Intensification Neil Skolnik, M.D. Associate Director Family Medicine Residency Program Abington Memorial Hospital Professor of Family and Community Medicine Temple University School
Diabetes: Three Core Deficits
 Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
Diabetes: Three Core Deficits Fat Cell Dysfunction Impaired Incretin Function Impaired Appetite Suppression Obesity and Insulin Resistance in Muscle and Liver Hyperglycemia Impaired Insulin Secretion Islet
This program applies to Commercial, GenPlus and Health Insurance Marketplace formularies.
 OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
OBJECTIVE The intent of the GLP-1 (glucagon-like peptide-1) Agonists [Adlyxin (lixisenatide), Byetta (exenatide), Bydureon (exenatide extended-release), Tanzeum (albiglutide), Trulicity (dulaglutide),
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.
 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION.") GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
GLUCAGON LIKE PEPTIDE (GLP) 1 AGONISTS FOR THE TREATMENT OF TYPE 2 DIABETES, WEIGHT CONTROL AND CARDIOVASCULAR PROTECTION. Patricia Garnica MS, ANP-BC, CDE, CDTC Inpatient Diabetes Nurse Practitioner North
The first stop for professional medicines advice
 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1 receptor analogues The first stop for professional medicines advice 1 London Medicines Evaluation Network Overview: Glucagon-Like Peptide-1
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My!
 DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
DM-2 Therapy Update: GLP-1, SGLT-2 Inhibitors, and Inhaled Insulin, Oh My! Kevin M. Pantalone, DO, ECNU, CCD Associate Staff Director of Clinical Research Department of Endocrinology Endocrinology and
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items
 Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
Diabetes Update: Intensifying Insulin Therapy Nuts, Bolts and Other Items Hayley A. Miller, MD Physician, Internal Medicine, Diabetes and Metabolism, Sandy Clinic, Intermountain Healthcare Objectives:
New Drug Evaluation: Dulaglutide
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Speaker Disclosures 6/17/ :07 AM. Management of Type 2 Diabetes: From Pathophysiology to Pharmacology
 Speaker Disclosures Management of Type 2 Diabetes: From Pathophysiology to Pharmacology Barry S. Horowitz, MD, FACE, FACP Clinical Research: Eli Lilly, NovoNordisk, Amgen, Pfizer, Sanofi, GSK, Lexicon,
Speaker Disclosures Management of Type 2 Diabetes: From Pathophysiology to Pharmacology Barry S. Horowitz, MD, FACE, FACP Clinical Research: Eli Lilly, NovoNordisk, Amgen, Pfizer, Sanofi, GSK, Lexicon,
Achieving and maintaining good glycemic control is an
 Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Glycemic Efficacy, Weight Effects, and Safety of Once-Weekly Glucagon-Like Peptide-1 Receptor Agonists Yehuda Handelsman, MD, FACP, FNLA, FASPC, MACE; Kathleen Wyne, MD, PhD, FACE, FNLA; Anthony Cannon,
Application of the Diabetes Algorithm to a Patient
 Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to a Patient Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Update on Insulin-based Agents for T2D
 Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Update on Insulin-based Agents for T2D Injectable Therapies for Type 2 Diabetes Mellitus (T2DM) and Obesity This presentation will: Describe established and newly available insulin therapies for treatment
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Metformin although effective has become obsolete
 Metformin although effective has become obsolete Does not address core needs as well as other agents (ominous octet) Does not address metabolic parameters (blood pressure, Hgb A1C) as well as other agents
Metformin although effective has become obsolete Does not address core needs as well as other agents (ominous octet) Does not address metabolic parameters (blood pressure, Hgb A1C) as well as other agents
Reviewing Diabetes Guidelines. Newsletter compiled by Danny Jaek, Pharm.D. Candidate
 Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Reviewing Diabetes Guidelines Newsletter compiled by Danny Jaek, Pharm.D. Candidate AL AS KA N AT IV E DI AB ET ES TE A M Volume 6, Issue 1 Spring 2011 Dia bet es Dis pat ch There are nearly 24 million
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol
 Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
Brigham and Women s Hospital Type 2 Diabetes Management Program Physician Pharmacist Collaborative Drug Therapy Management Protocol *Please note that this guideline may not be appropriate for all patients
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
GLP-1-based therapies in the management of type 2 diabetes
 GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
GLP-1-based therapies in the management of type 2 diabetes Makbul Aman Mansyur Division Endocrine & Metabolism Department of Internal Medicine Faculty of Medicine Hasanuddin University/ RSUP Dr. Wahidin
What s New in Diabetes Treatment. Disclosures
 What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
What s New in Diabetes Treatment Shiri Levy M.D. Henry Ford Hospital Senior Staff Physician Service Chief, West Bloomfield Hospital Endocrinology, Metabolism, Bone and Mineral Disorders Disclosures None
Progressive Loss of β-cell Function in T2DM
 Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
Disclaimer This slide deck in its original and unaltered format is for educational purposes and is current as of November 2015. The content and views presented in this educational activity are those of
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors
 Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Incretin-based Therapies for Type 2 Diabetes Comparisons Between Glucagon-like Peptide-1 Receptor Agonists and Dipeptidyl Peptidase-4 Inhibitors Timothy Bailey, MD, FACE, CPI Director, AMCR Institute,
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Incredible Incretins Abby Frye, PharmD, BCACP
 Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Incredible Incretins Abby Frye, PharmD, BCACP Objectives & Disclosures Review the pathophysiology of T2DM and the impact of the incretin system Describe the defining characteristics of the available glucagonlike
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
What to Do After Basal Insulin
 BasalINSULIN What to Do After Basal Insulin 3 Treatment Strategies for Type 2 Diabetes These strategies can help you optimize glucose control in your patient with type 2 diabetes when basal insulin alone
BasalINSULIN What to Do After Basal Insulin 3 Treatment Strategies for Type 2 Diabetes These strategies can help you optimize glucose control in your patient with type 2 diabetes when basal insulin alone
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Glucagon-Like Peptide-1 (GLP-1) Agonists
 Agonists") Glucagon-Like Peptide-1 (GLP-1) Agonists Policy Number: 5.01.565 Last Review: 07/2018 Origination: 06/2014 Next Review: 07/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Glucagon-Like Peptide-1 (GLP-1) Agonists Policy Number: 5.01.565 Last Review: 07/2018 Origination: 06/2014 Next Review: 07/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
UKPDS: Over Time, Need for Exogenous Insulin Increases
 UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
UKPDS: Over Time, Need for Exogenous Insulin Increases Patients Requiring Additional Insulin (%) 60 40 20 Oral agents By 6 Chlorpropamide years, Glyburide more than 50% of UKPDS patients required insulin
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes
 Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Optimizing Treatment Strategies to Improve Patient Outcomes in the Management of Type 2 Diabetes Philip Raskin, MD Professor of Medicine The University of Texas, Southwestern Medical Center NAMCP Spring
Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes
 St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
St. Onge et al. Medical Research Archives, vol. 5, issue 11, November 2017 issue Page 1 of 10 REVIEW ARTICLE Albiglutide, a Once-Weekly GLP-1RA, for the Treatment of Type 2 Diabetes Erin St. Onge 1*, Shannon
Ertugliflozin (Steglatro ) 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy
 5 mg daily. May increase to 15 mg daily. Take in the morning +/- food. < 60: Do not initiate; discontinue therapy") Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
Sodium-glucose Cotransporter-2 (SGLT2) s Inhibit SGLT in proximal renal tubules, reducing reabsorption of filtered glucose from tubular lumen Lowers renal threshold for glucose à increase urinary excretion
MOA: Long acting glucagon-like peptide 1 receptor agonist
 Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Alexandria Rydz MOA: Long acting glucagon-like peptide 1 receptor agonist Increases glucose dependent insulin secretion Decreases inappropriate glucagon secretion Increases β- cell growth and replication
Timely!Insulinization In!Type!2! Diabetes,!When!and!How
 Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Timely!Insulinization In!Type!2! Diabetes,!When!and!How, FACP, FACE, CDE Professor of Internal Medicine UT Southwestern Medical Center Dallas, Texas Current Control and Targets 1 Treatment Guidelines for
Diabetes Mellitus II CPG
 1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
1 Diabetes Mellitus II CPG Candidates for Screening Integrated Complex Care Patients: Check Yearly Prediabetes: Check Yearly No Diabetes Mellitus (DM) Risk Factors: Check at Age 45, Repeat Every 3 Years
Pathogenesis of Type 2 Diabetes
 9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
9/23/215 Multiple, Complex Pathophysiological Abnmalities in T2DM incretin effect gut carbohydrate delivery & absption pancreatic insulin secretion pancreatic glucagon secretion HYPERGLYCEMIA? Pathogenesis
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM
 Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
Beyond Basal Insulin: Intensification of Therapy Jennifer D Souza, PharmD, CDE, BC-ADM Disclosures Jennifer D Souza has no conflicts of interest to disclose. 2 When Basal Insulin Is Not Enough Learning
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S.
 GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
GLP-1 receptor agonists for type 2 diabetes currently available in the U.S. GLP-1 agonists are a class of antidiabetic agents that mimic the actions of the glucagon-like peptide. GLP-1 is one of several
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy
 New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy New Treatment Options for Type 2 Diabetes: Incretin-Based Therapy is supported by an educational grant from Novo Nordisk Inc. This program
Agenda. Indications Different insulin preparations Insulin initiation Insulin intensification
 Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Insulin Therapy F. Hosseinpanah Obesity Research Center Research Institute for Endocrine sciences Shahid Beheshti University of Medical Sciences November 11, 2017 Agenda Indications Different insulin preparations
Basal & GLP-1 Fixed Combination Use
 Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Basal & GLP-1 Fixed Combination Use Michelle M. Mangual, MD Diplomate of the American board of Internal Medicine and Endocrinology, Diabetes and Metabolism San Juan City hospital Learning Objectives o
Selecting GLP-1 RA Treatment
 Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Selecting GLP-1 RA Treatment Dr Felicity Kaplan March 2017 Objectives Review the progressive nature of type 2 diabetes Understand the need for timely treatment intensification Examine the place of GLP-1
Intensification of Diabetic Therapy. Case studies
 Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Intensification of Diabetic Therapy Case studies Patient #1 1 st visit: 64 year old male, H/O prediabetes, lost weight 280 lbs. to 240 lbs. ER for dental abscess, glucose >300 A1C 11.4%, no diabetic medication,
Diabesity. Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs
 Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
Diabesity Metabolic dysfunction that ranges from mild blood glucose imbalance to full fledged Type 2 DM Signs Abdominal obesity Low HDL, high LDL, and high triglycerides HTN High blood glucose (F>100l,
9/29/ Disclosure. Learning Objectives. Diabetes Update: Guidelines, Treatment Options & Trends
 + Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
+ Diabetes Update: Guidelines, Treatment Options & Trends Melissa Max, PharmD, BC-ADM, CDE Assistant Professor of Pharmacy Practice Harding University College of Pharmacy + Disclosure Conflicts Of Interest
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
Update on Therapies for Type 2 Diabetes: Angela D. Mazza, DO July 31, 2015
 Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
Update on Therapies for Type 2 Diabetes: 2015 Angela D. Mazza, DO July 31, 2015 Objectives To present the newer available therapies for the management of T2D To discuss the advantages and disadvantages
All the New Medications: What Should I. Lauren LaBryer, MD Endocrinologist Oklahoma Heart Institute
 All the New Medications: What Should I Choose for NIDDM Lauren LaBryer, MD Endocrinologist Oklahoma Heart Institute None Disclosures Objectives To become familiar with the new medication classes for the
All the New Medications: What Should I Choose for NIDDM Lauren LaBryer, MD Endocrinologist Oklahoma Heart Institute None Disclosures Objectives To become familiar with the new medication classes for the
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace See Important
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace See Important
Newer and Expensive treatment of diabetes. Endocrinology Visiting Associate Professor Institute of Medicine TUTH
 Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Newer and Expensive treatment of diabetes Jyoti Bhattarai MD Endocrinology Visiting Associate Professor Institute of Medicine TUTH Four out of every five people with diabetes now live in developing countries.
Comprehensive Diabetes Treatment
 Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
Comprehensive Diabetes Treatment Joshua L. Cohen, M.D., F.A.C.P. Professor of Medicine Interim Director, Division of Endocrinology & Metabolism The George Washington University School of Medicine Diabetes
What s New in Diabetes Medications. Jena Torpin, PharmD
 What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
What s New in Diabetes Medications Jena Torpin, PharmD 1 Objectives Discuss new medications in the management of diabetes Understand the mechanism of the medications discussed Understand the side effects
Soliqua (insulin glargine and lixisenatide), Xultophy (insulin degludec and liraglutide)
, Xultophy (insulin degludec and liraglutide)") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.48 Subject: Insulin GLP-1 Combinations Page: 1 of 5 Last Review Date: September 15, 2017 Insulin GLP-1
OBESITY IN TYPE 2 DIABETES
 OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
OBESITY IN TYPE 2 DIABETES Ashley Crowl, PharmD, BCACP Assistant Professor University of Kansas Objectives Review how to manage obesity in patients with type-2 diabetes mellitus Compare antiobesity agents
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes
 Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
Breaking the Cycle: Using Incretin-Based Therapies to Overcome Clinical Inertia in Type 2 Diabetes Taking It to the Next Level: Pearls for Your Clinical Practice Thursday, April 23, 2009 6:00 AM - 8:00
3/8/2011. Julie M. Sease, Pharm D, BCPS, CDE Associate Professor of Pharmacy Practice Presbyterian College School of Pharmacy
 Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Summarize revisions to the 2011 American Diabetes Association clinical practice guidelines. Evaluate bromocriptine as a therapeutic option in the management of type 2 diabetes. Compare and contrast the
Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American
 Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American Association of Diabetes Educators (AADE) for nurses, dietitians,
Update on GLP-1 Agonists in Type 2 Diabetes is supported by an educational grant from Novo Nordisk Inc. It has been accredited by the American Association of Diabetes Educators (AADE) for nurses, dietitians,
Vipul Lakhani, MD Oregon Medical Group Endocrinology
 Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Vipul Lakhani, MD Oregon Medical Group Endocrinology Disclosures None Objectives Be able to diagnose diabetes and assess control Be able to identify appropriate classes of medications for diabetes treatment
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: Last Review Date: 02.
 Receptor Agonists Reference Number: HIM.PA.53 Effective Date: Last Review Date: 02.") Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.19 Line of Business: HIM Revision Log See Important Reminder
Clinical Policy: Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists Reference Number: HIM.PA.53 Effective Date: 03.01.18 Last Review Date: 02.19 Line of Business: HIM Revision Log See Important Reminder
4/10/2015. Foundations to Managing Inpatient Hyperglycemia. Learning Objectives
 Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
Foundations to Managing Inpatient Hyperglycemia Module A 1 Learning Objectives Develop strategies to identify patients with hyperglycemia or diabetes in the inpatient setting Establish glycemic goals to
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE
 INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
INSULIN IN THE OBESE PATIENT JACQUELINE THOMPSON RN, MAS, CDE SYSTEM DIRECTOR, DIABETES SERVICE LINE SHARP HEALTHCARE OBJECTIVES DESCRIBE INSULIN, INCLUDING WHERE IT COMES FROM AND WHAT IT DOES STATE THAT
Update on Insulin-based Agents for T2D. Harry Jiménez MD, FACE
 Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Update on Insulin-based Agents for T2D Harry Jiménez MD, FACE Harry Jiménez MD, FACE Has received honorarium as Speaker and/or Consultant for the following pharmaceutical companies: Eli Lilly Merck Boehringer
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
Glucagon-like polypeptide agonists in type 2 diabetes mellitus: efficacy and tolerability, a balance
 580257TAE0010.1177/2042018815580257Therapeutic Advances in Endocrinology and MetabolismSH Tella and MS Rendell research-article2015 Therapeutic Advances in Endocrinology and Metabolism Review Glucagon-like
580257TAE0010.1177/2042018815580257Therapeutic Advances in Endocrinology and MetabolismSH Tella and MS Rendell research-article2015 Therapeutic Advances in Endocrinology and Metabolism Review Glucagon-like
Approaches to Addressing Incretin Deficiency. Non-Insulin Injectable Agents. Incretin Mimetics. Exendin-4 in the Gila Monster
 Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
Non-Insulin Injectable Agents Approaches to Addressing Incretin Deficiency Longer-acting analogs? (Incretin mimetics) GLP-1 Analogs Inhibition of inactivation? (Incretin enhancers) DPP-4 Inhibitors Drucker
Type 2 DM in Adolescents: Use of GLP-1 RA. Objectives. Scope of Problem: Obesity. Background. Pathophysiology of T2DM
 Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
Type 2 DM in Adolescents: Use of GLP-1 RA Objectives Identify patients in the pediatric population with T2DM that would potentially benefit from the use of GLP-1 RA Discuss changes in glycemic outcomes
The Death of Sulfonylureas? A Review of New Diabetes Medications
 The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
The Death of Sulfonylureas? A Review of New Diabetes Medications Kelly Hoenig, Pharm.D., BCPS Cedar Rapids Family Medicine Residency 2/4/17 Objectives Review GLP-1 Agonists, DPP-IV Inhibitors and SGLT-2
Application of the Diabetes Algorithm to Patients
 Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Application of the Diabetes Algorithm to Patients Apply knowledge gained from this activity to improve disease management and outcomes for patients with T2DM and obesity Note: The cases in this deck represent
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
 Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes Obesity (BMI 30 kg/m 2 ) 1994 2000 2009 No Data 26.0% Diabetes 1994 2000 2009
Learning Objectives. Impact of Diabetes II UPDATES IN TYPE 2 DIABETES. David Doriguzzi, PA-C
 UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
UPDATES IN TYPE 2 DIABETES David Doriguzzi, PA-C Learning Objectives Upon completion of this educational activity, the participant should be able to: Overcome barriers and attitudes that limit Clinician/Patient
Francesca Porcellati
 XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
XX Congresso Nazionale AMD Razionali e Benefici dell Aggiunta del GLP-1 RA Short-Acting all Insulina Basale Francesca Porcellati Dipartimento di Medicina Interna, Sezione di Medicina Interna, Endocrinologia
Beyond A1C. Non-glycemic Effects of GLP-1 Receptor Agonists. Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows
 Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
Beyond A1C Non-glycemic Effects of GLP-1 Receptor Agonists Olga Astapova MD, PhD Luis Chavez MD URMC Endocrinology Fellows Disclosures No conflicts of interest. Learning Objectives 1. Understand the physiological
New Drug Evaluation: lixisenatide injection, subcutaneous
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery
 Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia
ANGELA GINN-MEADOW RD LDN CDE
 DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
DIABETES DRUGS & TRENDS MADE SIMPLE PHARMD TO RD ANGELA GINN-MEADOW RD LDN CDE OBJECTIVES At the end of this presentation, participants should be able to: Evaluate the emerging role of GLP-1 Agonists for
Individualizing Care for Patients with Type 2 Diabetes
 Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
Individualizing Care for Patients with Type 2 Diabetes Disclosures Speaker: AstraZeneca, Novo Nordisk, BI/Lilly, Valeritas, Takeda Advisor: Tandem Diabetes, Sanofi Objectives Develop individualized approaches
DM Fundamentals Class 4 Meds for Type 2
 DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
DM Fundamentals Class 4 Meds for Type 2 Beverly Thomassian, RN, MPH, BC ADM, CDE President, Diabetes Education Services Copyright 1999 2015, Diabetes Education Services, All Rights Reserved. Diabetes Meds
What s New in Type 2 Diabetes? 2018 Diabetes Updates
 What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
What s New in Type 2 Diabetes? 2018 Diabetes Updates Gretchen Ray, PharmD, PhC, BCACP, CDE Associate Professor, UNM College of Pharmacy January 28, 2018 gray@salud.unm.edu OBJECTIVES Describe the most
Management of Diabetes
 Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships
Management of Diabetes Mellitus: Which Drugs for Which Patients? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu Disclosure No relevant financial relationships