Prof. Richard Češka, MD, PhD
|
|
|
- Sandra Hensley
- 6 years ago
- Views:
Transcription


1 Prof. Richard Češka, MD, PhD Head of the Center of Preventive Cardiology President of the Czech Society of Internal Medicine President of the Czech Atherosclerosis Society, member of EAS, IAS chair IAS Federation for Europe Focuses on internal medicine, preventive cardiology, lipidology and metabolism
2 ANTIHYPERTENSIVES & STATINS IN CV RISK PREVENTION: from guidelines to clinical practice Richard CESKA Centre for Preventive Cardiology University Hospital, Prague, Czech Republic
3 HLP Others HT CVD Smo king DM2T
4 How to influence it??? What is the priority???

5 Lifestyle changes, Lifestyle changes, Lifestyle changes, Lifestyle changes, Lifestyle changes, Lifestyle changes, Lifestyle changes, Lifestyle changes, lifestyle changes,

6 BUT!!!???

7

8
9
10 Complex treatment of the patient with CARDIOMETABOLIC RISK ACE-I ARBs CCBs Metformin Sulfonylurea Inzulin Statins Resins,eze,niacin CMR Glitazones Gliptines.. Niacin Fenofibrate Anti-Thrombotic Agents??? Diet & Physical Activity
11 Dyslipidemia Management Part of the complex approach to decrease CV RISK Influence all lipid parameters LDL-C The first target HDL-C,TGs, apob To lower MACROvascular risk To lower MICROvascular risk To lower CV morbidity and mortality
12 Treatment of Hyperlipidemia LDL-C Therapeutic Lifestyle Change Drug Therapy Therapy of Choice: Statin Alternative/combo: Ezetimibe,resin or niacin Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001;285:
13 Statins for everyone!!! Should we add statins to drinking water?
14 Association between preadmission statin use and death within 30 and 90 days /pneumonie/ Risk factor 0 30 d after hospital admission Patients (n) Deaths (n) Mortality (%) Odds ratio (95% CI) No statin use Reference Statin use ( ) 0 90 d after hospital admission No statin use Reference Statin use ( ) Thomsen R et al. Arch Intern Med 2008; 168:
15 Odds ratio (95% CI) for in-hospital onset of shock in patients with ACS without cardiogenic shock on admission Parameter OR (95% CI)* p ST-segment-elevation ACS 2.89 ( ) <0.001 Age (per-y increase) 1.03 ( ) <0.001 Primary PCI 0.59 ( ) <0.012 Lipid-lowering drugs 0.52 ( ) <0.001 *Adjusted for age, sex, cardiovascular diagnoses, diabetes, smoking status, electrocardiographic type of ACS, symptom-to-admission interval, whether cardioversion or cardiopulmonary resuscitation was administered, atrial fibrillation, heart rate, blood pressure, body-mass index, comorbidities, cardiovascular medications, and whether PCI, CABG, or intra-aortic balloon pump was used Jeger RV et al. Ann Intern Med 2008; 149:618-
16 Statin therapy postdischarge on stroke recurrence and mortality risk Statin therapy postdischarge Hazard ratio (95% CI) 1-y stroke recurrence 0.61 ( ) Mortality 0.22 ( ) Milionis HJ et al. Neurology 2009; 72:
17 Sattar N et al. Lancet 2010; available at: Association between statins and development of diabetes Statin Odds ratio (95% CI) Overall (n=91 140) 1.09 ( ) Atorvastatin only (n=7773) 1.14 ( ) Simvastatin only (n=18 815) 1.11 ( ) Rosuvastatin only (n=24 714) 1.18 ( ) Pravastatin (n=33 627) 1.03 ( ) Lovastatin (n=6211) 0.98 ( )
18 STATIN VS CONTROL Proportional effects on MAJOR VASCULAR EVENTS per mmol/l LDL-C No. of events reduction (% pa) Statin Control Relative risk (CI) per mmol/l LDL-C reduction Nonfatal MI CHD death Any major coronary event 2310 (0.9%) 1242 (0.5%) 3380 (1.3%) 3213 (1.2%) 1587 (0.6%) 4539 (1.7%) 0.74 ( ) 0.80 ( ) 0.76 ( ) CABG PTCA Unspecified 816 (0.3%) 601 (0.2%) 1686 (0.6%) 1126 (0.4%) 775 (0.3%) 2165 (0.8%) 0.76 ( ) 0.78 ( ) 0.76 ( ) Any coronary revascularisation 3103 (1.2%) 4066 (1.6%) 0.76 ( ) Ischaemic stroke Haemorrhagic stroke 987 (0.4%) 188 (0.1%) 1225 (0.5%) 163 (0.1%) 0.80 ( ) 1.10 ( ) Unknown stroke Any stroke 555 (0.2%) 1730 (0.7%) 629 (0.2%) 2017 (0.8%) 0.88 ( ) 0.85 ( ) Any major vascular event 7136 (2.8%) 8934 (3.6%) 0.79 ( ) 99% or 95% CI Statin better Control better 18
19 MORE VS LESS STATIN Proportional effects on MAJOR VASCULAR EVENTS per mmol/l LDL-C reduction No. of events (% pa) More statin Less statin Relative risk (CI) per mmol/l LDL-C reduction Nonfatal MI 1175 (1.3%) 1380 (1.5%) 0.71 ( ) CHD death Any major coronary event 645 (0.7%) 1725 (1.9%) 694 (0.7%) 1973 (2.2%) 0.85 ( ) 0.74 ( ) CABG 637 (0.7%) 731 (0.9%) 0.72 ( ) PTCA Unspecified 1166 (1.3%) 447 (0.5%) 1508 (1.8%) 502 (0.6%) 0.60 ( ) 0.78 ( ) Any coronary revascularisation 2250 (2.6%) 2741 (3.2%) 0.66 ( ) Ischaemic stroke Haemorrhagic stroke 440 (0.5%) 69 (0.1%) 526 (0.6%) 57 (0.1%) 0.69 ( ) 1.39 ( ) Unknown stroke Any stroke 63 (0.1%) 572 (0.6%) 80 (0.1%) 663 (0.7%) 0.63 ( ) 0.74 ( ) Any major vascular event 3837 (4.5%) 4416 (5.3%) 0.72 ( ) 99% or 95% CI More statin better Less statin better 19
20 Cochrane review: CVD risk in low risk population treated with statins Risk ratio (95% CI) Total mortality 0.83 ( ) Fatal and non-fatal CHD 0.72 ( ) Fatal and non-fatal stroke 0.78 ( )
 Study.")
21 GREACE study Treatment with atorvastatin to the National Cholesterol Educational Program goal versus usual care in secondary coronary heart disease prevention: the GREek Atorvastatin and Coronary- heart-disease Evaluation (GREACE) Study. The Lower The Better
22 Be carefull!!! Statins and increased risk of DM2T
23 Statins and increased risk of DM2T Increased risk of DM2T by 9% In patients over 60 years only Risk/benefit ratio 1 : 9 Risk of DM2T is dependent on LDL lowering potency
24 Effects on MAJOR VASCULAR EVENTS, per mmol/l reduction in LDL cholesterol, among participants with diabetes Major vascular event and prior diabetes Events (%) Treatment Control RR (CI) Major coronary event Diabetes 776 (8 3) 979 (10 5) No diabetes 2561 (7 2) 3441 (9 6) Any major coronary event 3337 (7 4) 4420 (9 8) 0 78 ( ) 0 77 ( ) 0 77 ( ) Coronary revascularization Diabetes 491 (5 2) 627 (6 7) No diabetes 2129 (6 0) 2807 (7 9) Any coronary revascularization 2620 (5 8) 3434 (7 6) Stroke Diabetes 407 (4 4) 501 (5 4) No diabetes 933 (2 7) 1116 (3 2) Any stroke 1340 (3 0) 1617 (3 7) Major vascular event Diabetes 1465 (15 6) 1782 (19 2) No diabetes 4889 (13 7) 6212 (17 4) Any major vascular event 6354 (14 1) 7994 (17 8) ( ) 0 76 ( ) 0 76 ( ) 0 79 ( ) 0 84 ( ) 0 83 ( ) 0 79 ( ) 0 79 ( ) 0 79 ( ) RR (99% CI) RR (95% CI)

25 Case No: Familial hypercholesterolemia 12 years 2005
26 Statins in clinical studies in childern Study statin year No Weeks TC % LDL % HDL % De Jongh simva Wiegman prava Knipscheer prava Lambert lova Stein lova Clauss lova Mc Crindle atorva Avis rosuva TG %
27 LDL-C Killer No.1 The most important risk factor for CVD The first target for lipid lowering treatment

28 The Lower = The Better for LDL-C lowering For clinical outcomes reduction
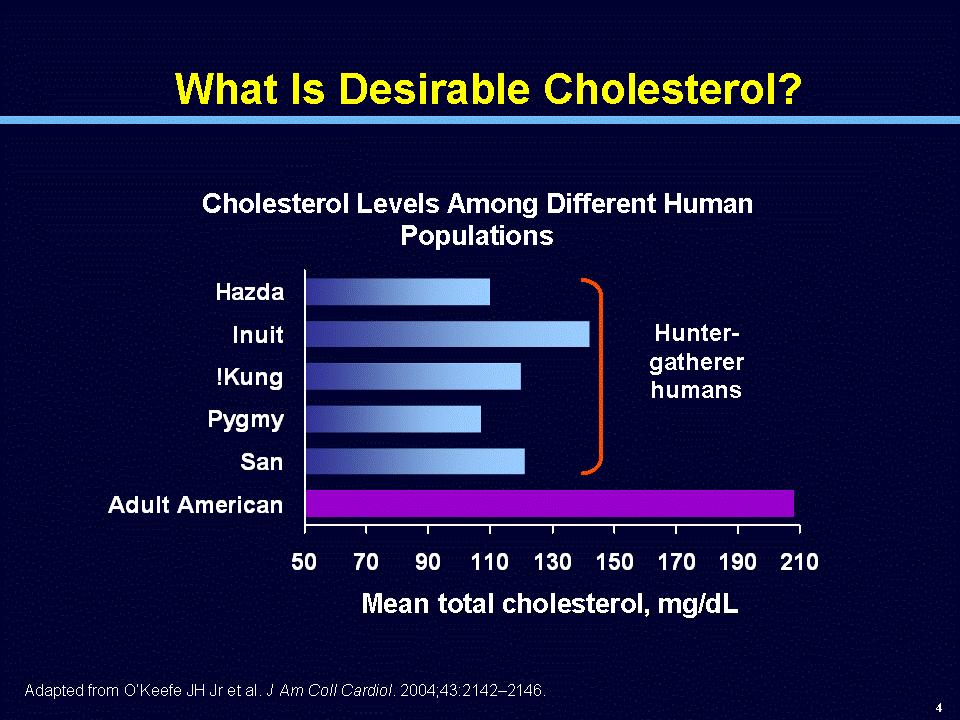
29 What is an appropriate therapeutic target for LDL-C?

30 The human evolution What was the LDL-C of our ancestry?
31
32 What is desirable LDL- C? Hunter-Gatherer humans Newborn Primates Domestic animals 1,3-1, ,8-1, ,0-2, > 2,1 >80 Adult Euro/American (probable physiologic level) 1,3-1, Desirable
33 TNT: The Lower the Better -22% Intensive lipid-lowering therapy with atorvastatin 80 mg/day in patie CHD provides significant clinical benefit beyond that provided by at J. C. LaRosa et al. Intensive Lipid Lowering with Atorvastatin in Patients with Stable Coronary Disease. // N Engl J Med 2005;352:
34 TNT pts after CABG n = 4,654 MACE -27%
35 High dose atorvastatin after stroke or transient ischaemic attack SPARCL -16% P. Amarenco et al. High-Dose Atorvastatin after Stroke or Transient Ischemic Attack.// N Engl J Med 2006;355:

36 The Longer The Better for appropriate treatment duration for longer life (without MI,ACS, stroke )
37 PCSK9 (proprotein convertase subtilisin/kexin type 9) Enzyme - associated with plasma levels of LDL C (expressed in the liver, intestine and kidney) Overexpression of gene for PCSK9 more PCSK9 enzyme LDL receptors reduction (LDL-Receptor enable removal of LDL-C from the plasma) increase in circulating LDL-C High levels of PCSK9 = high LDL-C levels Conversely, lacking Pcsk9 leads to increased levels of hepatic LDL receptors,and they remove LDL from the plasma at an accelerated rate) Low levels of PCSK9 = low LDL- C levels 1.Brown, M.S.,Science, Vol 311, March 24, Cohen J.C. et al.,new England Journal of Medicine, Volume 354, 2006 Number 12
38 Cohen et al. studied patients with lifelong low LDL-C levels, due to loss of- function mutations in the gene encoding PCSK9 = they have low level of PCSK9 = low level of LDL-C Severe mutation: LDL-C was reduced by 1 mmol/l (38 mg/dl) 88%. prevalence of CHD declined by a remarkable Less severe mut.:ldl-c was reduced by only 0,52 mmol/l (21 mg/dl) CHD incidence declined by 47%. The Longer The Better Cohen et al., N Engl J Med 2006;354: Brown, M.S.,Science, Vol 311, March 24, 2006
39 Cohen s study The Longer The Better Why does lowering of LDL-C concentration by 40 mg/dl by a PCSK9 mutation reduce CHD incidence by 88% whereas a 40-mg/dl lowering with a statin reduces CHD prevalence by only 23% on average??? Cohen et al., N Engl J Med 2006;354: Brown, M.S.,Science, Vol 311, March 24, 2006
40 Cohens study The Longer The Better The most likely explanation is: DURATION Cohen et al., N Engl J Med 2006;354: Brown, M.S.,Science, Vol 311, March 24, 2006
41 Cohens study The Longer The Better People with mutations in PCSK9 likely have maintained relatively low LDL levels throughout their lives. People in statin trials have had their LDL levels lowered for only 5 years. Atherosclerosis is a chronic disease that begins in the teenage years Cohen et al., N Engl J Med 2006;354: Brown, M.S.,Science, Vol 311, March 24, 2006
42 Cohens et al. study The lesson of PCSK9 case is clear: The longer The better These data indicate that moderate lifelong reduction in the plasma level of LDL-C is associated with a substantial reduction in the incidence of coronary events Cohen et al., N Engl J Med 2006;354: Brown, M.S.,Science, Vol 311, March 24, 2006

43 % reduction in CHD risk Reduction of CHD treatment duration (trial results are standardised to a LDL-C reduction of 1 mmol/l) According Years of treatment Statins life long treatment 2 need to encourage patients treatment persistence 2 2. Mantel:Heart 2004,90:

44 What is the reason?
45 30% of adults in CZ: Metabolic Syndrome
46
47
 Patients with abdominal obesity (high waist circumference) often present with one or")
48 RFs in abdominal obesity (104 cm) (1.8 mmol/l) (0.9 mmol/l) Patients with abdominal obesity (high waist circumference) often present with one or more additional CV risk factors (6.0 mmol/l)

49 Intra-abdominal (visceral) fat examination The dangerous inner fat! Front Visceral AT Subcutaneous AT Back
50 Intra-abdominal fat examination

51 Cardiometabolic risk in MS patient Hypertriglyceridemia Low HDL-C Elevated apolipoprotein B Small, dense LDL particles Postprandial hyperlipidaemia Hyperinsulinemia Glucose intolerance Insulin resistance Impaired fibrinolysis Endothelial dysfunction Hypertension Central obesity Smoking, Depression
52 TGs, (HDL-C) Fibrates (niacin) Statin + Fibrate (niacin) COMBO
53 HDL-C (LDL,TG) Niacin Statin + Niacin (laropiprant)
54 Complex approach to the patients ACE-inhibitors ARBs Ca antagonists Metformin Sulfonylurea Statins ezetimibe Fibrate Niacin KV Risk Anti-Thrombotic Agents Pioglitazon, Insulin Anti-obesity, Stop smoking drugs


55
56 RR reduction (%) HOPE - Heart Outcomes Prevention Evaluation n = Yusuf et al., N Engl J Med 2000
57 Treatment of hypertension (RAS infl.drugs,bb,diuretics,ca antagonists) 70% combination!!! What antihypertensive drugs should we use? What combinations should be used?
58 Risk reduction (%) Atorva + AMLO/PERINDO lowers CV risk more than Atorva + BB/diuretics 0% -16% -20% (NS) -40% -36% (p=0,0005) -53% -60% ASCOT-LLA celkem (p<0,0001) Amlodipin+At vs Amlodipin Atenolol+At vs Atenolol Primary endpoint (fatal CHD, nonfatal MI) Sever PS, Dahlof B, Poulter NP, Wedel H. Anglo-Scandinavian Cardiac Outcomes Trial: Lipid Lowering Arm (ASCOT LLA) revisited: interaction of antihypertensive and lipid lowering therapy. Circulation. 2005;112(17 Suppl):II-134. Abstract 730.
59 ACCOMPLISH: Primary and secondary end points End point Hazard ratio (95% CI) Cardiovascular morbidity/mortality* 0.80 ( ) Individual components Cardiovascular mortality 0.80 ( ) Fatal and nonfatal MI 0.78 ( ) Fatal and nonfatal stroke 0.84 ( ) Hospitalization for unstable angina 0.75 ( ) Coronary revascularization 0.86 ( ) Resuscitation after sudden cardiac arrest 1.75 ( ) *Primary end point Jamerson K et al. N Engl J Med 2008; 359:
60
61
62 Primary outcome (%) Adjusted HR J-Curve in TNT Trial in Patients with CAD (n = 10,001) 35 Nadir = 79.2 mmhg > 100 Diastolic blood pressure (mmhg) 0 Bangalore et al., 2009
63 Play with the scale What a game!!!
64 Úmrtí na IM (na 1000 osoboroků) DTK (mmhg) Lancet 1987; i(8533):
 DTK")
65 Úmrtí na IM (na 1000 osoboroků) DTK (mmhg)
66 Úmrtí na IM (na 1000 osoboroků) DTK (mmhg)
 Total patients (n) 45 234 196 1709 493 6859 596 7216 437 3737 253 1663 248 1 157 Mean DBP (mm Hg) Patients with primary outcome Patients without primary outcome 65.7 67.9 70.8 73.5 74.")
67 Incidence (%) of Primary Outcome Incidence of Primary Outcome by SBP Strata >110 to 120 >120 to 130 >130 to 140 >140 to 150 >150 to 160 >160 SBP (mm Hg) Patients with primary outcome (n) Total patients (n) Mean DBP (mm Hg) Patients with primary outcome Patients without primary outcome Messerli FH, et al. Ann Int Med. 2006;144:
68 Incidence (%) of Primary Outcome Incidence of Primary Outcome by DBP Strata >60 to 70 >70 to 80 >80 to 90 >90 to 100 >100 to 110 >110 DBP (mm Hg) Patients with primary outcome (n) Total patients (n) Mean SBP (mm Hg) Patients with primary outcome Patients without primary outcome Messerli FH, et al. Ann Int Med. 2006;144:
69 Complex treatment of the patient with CARDIOMETABOLIC RISK ACE-I ARBs CCBs Metformin Sulfonylurea Inzulin Statins Resins,eze,niacin CMR Glitazones Gliptines.. Niacin Fenofibrate Anti-Thrombotic Agents??? Diet & Physical Activity
70 Experience from ATRACTIV project
71 ATRACTIV project 1. Identification of CVD risk factors 2. Evaluation of the effects of implementation of new guidelines and results of new clinical trials into everyday practice 3. Evaluation of possibilites of CVD risk reduction using combination of modern, evidence based treatment strategies in everyday practice in the Czech Republic
72 Duration ATRACTIV - Design 12 months Participating physicians: All 464 General Practice 453 Specialized Centers 11 Patients: All 4427 Men 2372 / Women 2055 Intervention: lifestyle counseling + pharmacotherapy: DLP: atorvastatin HT: amlodipin +/- ramipril or perindopril or losartan DM2T: metformin
 153 DBP (mmhg) 90 HR (bpm) 77 Men (%) 47,2 Women (%)")
73 Average ATRACTIV participant Age (years) 63 BMI (kg/m 2 ) 29,9 SBP (mmhg) 153 DBP (mmhg) 90 HR (bpm) 77 Men (%) 47,2 Women (%) 52,8
 6,6 LDL cholesterol 4,0 (mmol/l) HDL cholesterol (mmol/l) 1,4 Triglycerides 2,5")
74 Average ATRACTIV participant Variable Value Glycemia 6,3 (mmol/l) Total cholesterol (mmol/l) 6,6 LDL cholesterol 4,0 (mmol/l) HDL cholesterol (mmol/l) 1,4 Triglycerides 2,5 (mmol/l)
: 1131-9.")
75 Sever P et al. Lancet 2003; 361: Vrablík M et al. Vnitr Lek 2008; 54 (12): ATRACTIV and ASCOT Basic characteristics of participants
: 1131-9.")
76 Sever P et al. Lancet 2003; 361: Vrablík M et al. Vnitr Lek 2008; 54 (12): ATRACTIV and ASCOT Selected biochemical variables

77 mmhg ATRACTIV - results Blood pressure 132,5 152,5 80,2 90,5 P < 0,001

78 ATRACTIV - results Total and LDL cholesterol 23% 24% 28% 29% P < 0,001

79 ATRACTIV - results HDL cholesterol and triglycerides 26% 21% P < 0,001

80 ATRACTIV - results BMI.55 kg/m 2.65 kg/m 2 P < 0,001
81 ATRACTIV - results Waist circumference 3 cm 2 cm P < 0,001
82 ATRACTIV - results Glycaemia P < 0,001

83 ATRACTIV: change of the calculated CVD risk -48% P < 0,001
84 Results of ATRACTIV project Intesified treatment combining lifestyle changes, antihypertensive and lipid lowering therapy results in: Significant BP lowering Significant improvement of dyslipidemia Weigt loss and significant reduction of waist circumference Decreased glycaemia Minimum side effects Reduction of global risk of cardiovascular events
85 Do NOT treat LIPIDS!
86 Do NOT treat BP!!!
87 Do NOT treat Blood sugar!!!
88 TREAT THE PATIENT!!!
89 Stroke risk according to the number of RFs controlled n Hazard ratio 95% CI Amarenco P. American Academy of Neurology 2009 Annual Meeting; April 29, 2009; Seattle WA.

90 What is the beauty? An indeal is changing. What is the best treatment of CV risk? Yesterday, today and tomorrow
Aggressive Lipid Lowering Treatment
 Aggressive Lipid Lowering Treatment Richard CESKA Centre of Preventive Cardiology University Hospital, Prague, Czech Republic International Atherosclerosis Society Chair: Federation for EUROPE Dyslipidemia
Aggressive Lipid Lowering Treatment Richard CESKA Centre of Preventive Cardiology University Hospital, Prague, Czech Republic International Atherosclerosis Society Chair: Federation for EUROPE Dyslipidemia
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology
 Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Diabetes and Cardiovascular Risk Management Denise M. Kolanczyk, PharmD, BCPS-AQ Cardiology Disclosures In compliance with the accrediting board policies, the American Diabetes Association requires the
Supplementary Online Content
 Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
Supplementary Online Content Navarese EP, Robinson JG, Kowalewski M, et al. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: a systematic review and
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Supplementary Online Content
 Supplementary Online Content Leibowitz M, Karpati T, Cohen-Stavi CJ, et al. Association between achieved low-density lipoprotein levels and major adverse cardiac events in patients with stable ischemic
Supplementary Online Content Leibowitz M, Karpati T, Cohen-Stavi CJ, et al. Association between achieved low-density lipoprotein levels and major adverse cardiac events in patients with stable ischemic
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
The role of statins in patients with arterial hypertension
 Invited review The role of statins in patients with arterial hypertension Trygve B. Tjugen 1, Sigrun Halvorsen 1, Reidar Bjørnerheim 1, Sverre E. Kjeldsen 1, 2 1University of Oslo, Department of Cardiology,
Invited review The role of statins in patients with arterial hypertension Trygve B. Tjugen 1, Sigrun Halvorsen 1, Reidar Bjørnerheim 1, Sverre E. Kjeldsen 1, 2 1University of Oslo, Department of Cardiology,
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
The Metabolic Syndrome
 The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
The Metabolic Syndrome Advances in Internal Medicine David D. Waters, MD May 21, 27 UCSF Metabolic Syndrome: Definition abdominal obesity increased waist circumference atherogenic dyslipidemia low HDL-C,
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Causes of death in Diabetes
 Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
Rates of CV events in Diabetes patients Respiratory4.2 Cancer 7.6 Diabetes 1.3 CV disease 17.3 Causes of death in Diabetes 250 200 150 100 50 0 per 10,000 person-years 97 151 243 Framingham 5 X increase
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
How to Reduce CVD Complications in Diabetes?
 How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
How to Reduce CVD Complications in Diabetes? Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Framingham Heart Study 30-Year
Macrovascular Residual Risk. What risk remains after LDL-C management and intensive therapy?
 Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Macrovascular Residual Risk What risk remains after LDL-C management and intensive therapy? Defining Residual Vascular Risk The risk of macrovascular events and microvascular complications which persists
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Statins in the elderly : Is there a rationale?
 Statins in the elderly : Is there a rationale? Pr B Boland After a communication by Dr. Manfred Gogol EAMA, Sion, June, 2006 1 RCTs with Statins Meta-Analysis, 1999 182 abstracts or research papers 29
Statins in the elderly : Is there a rationale? Pr B Boland After a communication by Dr. Manfred Gogol EAMA, Sion, June, 2006 1 RCTs with Statins Meta-Analysis, 1999 182 abstracts or research papers 29
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Update on Atherosclerosis Treatment and Prevention
 Update on Atherosclerosis Treatment and Prevention Ronald D. Scott, MD Lipidology and Family Medicine West LA Med Center Regional CVD Colead Overview Lipids and CAD risk CVD is major killer and impacts
Update on Atherosclerosis Treatment and Prevention Ronald D. Scott, MD Lipidology and Family Medicine West LA Med Center Regional CVD Colead Overview Lipids and CAD risk CVD is major killer and impacts
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Dr G R Letchuman. Clogged by Cholesterol
 Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Dr G R Letchuman Clogged by Cholesterol Main message Cholesterol management is all about reducing risk of CV events vs the side effects, hassle and cost of drugs News that it is no longer important to
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS
 BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
The updated guidelines from the National
 BEYOND NCEP ATP III: LESSONS LEARNED AND FUTURE DIRECTIONS * Benjamin J. Ansell, MD, FACP ABSTRACT The National Cholesterol Education Program (NCEP) Third Adult Treatment Panel (ATP III) guidelines provide
BEYOND NCEP ATP III: LESSONS LEARNED AND FUTURE DIRECTIONS * Benjamin J. Ansell, MD, FACP ABSTRACT The National Cholesterol Education Program (NCEP) Third Adult Treatment Panel (ATP III) guidelines provide
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital
 Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Soo LIM, MD, PHD Internal Medicine Seoul National University Bundang Hospital 1. Importance of Lowering LDL-Cholesterol in Diabetes Patients & Lipid Guidelines Prevalence of dyslipidemia in Korea Prevalence
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
APPENDIX B: LIST OF THE SELECTED SECONDARY STUDIES
 APPENDIX B: LIST OF THE SELECTED SECONDARY STUDIES Main systematic reviews secondary studies on the general effectiveness of statins in secondary cardiovascular prevention (search date: 2003-2006) NICE.
APPENDIX B: LIST OF THE SELECTED SECONDARY STUDIES Main systematic reviews secondary studies on the general effectiveness of statins in secondary cardiovascular prevention (search date: 2003-2006) NICE.
Treatment to reduce cardiovascular risk: multifactorial management
 Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Treatment to reduce cardiovascular risk: multifactorial management Matteo Anselmino, MD PhD Assistant Professor San Giovanni Battista Hospital Division of Cardiology, Department of Internal Medicine University
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Traitements associés chez l hypertendu: Statines, Aspirine
 Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
Traitements associés chez l hypertendu: Statines, Aspirine Pr Jean-Jacques Mourad CHU Avicenne, Université Paris 13, Bobigny DU HTA, Mars 2012 jean-jacques.mourad@avc.aphp.fr Global Mortality 2000: Impact
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA