Five papers that influenced my practice. Stephen Marks Consultant Paediatric Nephrologist
|
|
|
- Aubrie Susan Bradley
- 6 years ago
- Views:
Transcription
1 Five papers that influenced my practice Stephen Marks Consultant Paediatric Nephrologist Great Ormond Street Hospital for Children and UCL Institute of Child Health, London, UK. Nephrology for the General Paediatrician, Manchester Friday 21 June 2013
2 Introduction Basic scientific and laboratory research Translational research Aetiopathogenesis, investigations and management of renal disorders Influenced practice general paediatricians paediatric nephrologists
3 Antenatal hydronephrosis Urinary tract infections Nephrotic syndrome Renal genetics Prognosis and progression of renal disease Hypertension and obesity-related hypertension Renal replacement therapy Imaging in paediatric nephrology

4 First paper

5 Revised, evidence-based guidelines regarding diagnosis and management of initial urinary tract infections in febrile infants and young children 2m to 2y from AAP subcommittee on UTI
6 Why do we not need to know about VUR in all patients? 1. The number of infants with VUR might be higher then we have believed




7 VUR in 347 kids UTI?UTI Not
 Ped")
8 Occurrence of VUR in 1185 children Hannula et al (2010) Ped Nephrol;25:1463
9 Why do we not need to know about VUR in all patients? 1. The number of infants with VUR might be higher then we have believed 2. VUR has a high tendency to resolve

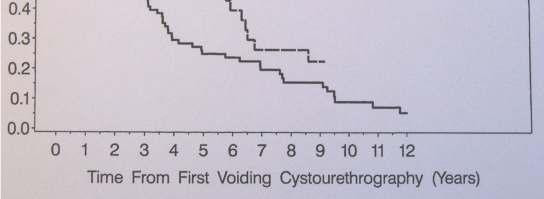
10 Natural history of VUR
11 Why do we not need to know about VUR in all patients? 1. The number of infants with VUR might be higher then we have believed 2. VUR has a high tendency to resolve 3. Surgical treatment of VUR does not help

J")
12 Importance of VUR for new scarring Olbing et al (1992)J Urol;148:1653-6

")
13 Medical vs surgical 5-year follow-up Smellie J et al (2001) Lancet;357:
14 Why do we not need to know about VUR in all patients? 1. The number of infants with VUR might be higher then we have believed 2. VUR has a high tendency to resolve 3. Surgical treatment of VUR does not help 4. Prophylactic antibiotics do not help - few good studies until recently - NICE concluded that prophylaxis should not be routinely recommended - AAP concluded should not be used

15 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age without VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics

16 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age with grade I VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics

17 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age with grade II VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics

18 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age with grade III VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics
19 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age with grade IV VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics

20 Estimate of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children 2 to 24 months of age with grade V VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics
21 Combined estimates of the effect of antimicrobial prophylaxis on prevention of pyelonephritis in children with VUR, from random-effects modeling. Pediatrics 2011;128:e749-e by American Academy of Pediatrics




22
23 Background Childhood-onset SLE variable clinical manifestations unpredictable natural history Epidemiological studies progressive clinical course of SLE significant morbidity and mortality rates 10-17% of proven cases present in childhood with more severe organ involvement than adults
24 Features Renal disease is a major determinant of the long-term outcome of SLE influence management with immunosuppressive agents 66% of childhood SLE have nephritis Haematological and renal disease more severe in patients with childhoodonset (compared to adult-onset) SLE
25 Introduction Conventional therapies steroid-sparing agents AZATHIOPRINE INTRAVENOUS CYCLOPHOSPHAMIDE MMF OTHER IMMUNOSUPPRESSION Different management strategies should be considered in problematic patients
26 Autoantibodies and B cells in SLE ANA and anti-dsdna important diagnostic / prognostic markers related to disease severity / renal damage Foster MH et al (1999):Semin Nephrol 19(2): Adults and children with active disease have profound B cell abnormalities Tangye SG et al (1998) J Exp Med 188: Odendahl M et al (2003) Ann Rheum Dis 62: 851-8

27 Rituximab Monoclonal antibody binds to CD20 Ag located on pre-b and mature B lymphocytes mediates B-cell lysis clinical use prophylaxis and treatment of lymphoma and EBVdriven LPD autoimmune diseases dose of 375mg/m 2 as slow iv infusion in PTLD once weekly for 4 weeks
28 Reasons for treatment Multi-systemic presentation of SLE with life or organ-threatening disease without response to iv methylprednisolone and/or plasma exchange no time to wait for iv cyclophosphamide Active disease after previous treatment with iv cyclophosphamide severe and continuous symptoms eg. ACTIVE SKIN / KIDNEY, POOR GROWTH
29 Six adult female patients with active SLE resistant to standard immunosuppressive therapy treated on an open-label basis during a 2-week period, each patient received two 500mg infusions of rituximab, two 750mg infusions of cyclophosphamide, and high-dose oral corticosteroids
30
31 All patients improve
32
33
34
35
36
37
38
39 Treatment protocol Day 1 and 15 premedicate with chlorphenamine and paracetamol one hour prior to rituximab infusion in addition a dose of iv methylprednisolone 100mg is given immediately prior to rituximab infusion Day 2 and 16 cyclophosphamide infusion 750mg (500mg if less than 50kg)
40 Rituximab infusion Dilute required dose with 0.9% NaCl or 5% dextrose to a final concentration of 1-4mg/ml Initial infusion rate is 25mg/hour can be increased by increments of 25mg/h q30m maximum of 200mg/h as tolerated Doctor should be present on the ward during the administration of rituximab Resuscitation facilities should be available
41 Steroid doses Post-rituximab therapy oral prednisolone is given for 3 days after the infusion at doses of 30mg, 20mg, 10mg (i.e. days 2, 3 & 4 & days 16, 17 & 18) and then continue with the patient s previous maintenance prednisolone dose
42
43


44



45
46 18-month old boy ahus developed 8 days after birth 3 further clinical presentations (3, 9 and 11 months of age); last treated with PE weekly for 20 weeks Normal ADAMTS13 activity, complement C2 - C9, factor H, factor I No mutation of factor H, factor I, and MCP genes Presentation at 18 months of age persistent progressive TMA; severe thrombocytopenia and worsening renal function, raised LDH despite 32 consecutive days PE Eculizumab treatment ongoing for 2.5+ years sustained normalisation haematological parameters sustained stabilisation and near normalisation of renal function including proteinuria
47
48 Typical and atypical forms of HUS Typical HUS most common form (90% of cases) triggered by shiga-toxin- (Stx-) producing E. coli (0157:H7) most often associated with diarrheal prodrome renal failure in 55-70% of cases (mostly recovers) Atypical HUS (ahus) represents ~ 10% of cases but poorer outcomes heterogenous group without evidence of Stx can be associated with triggers - infections, viruses, drugs, malignancies, pregnancy, transplantation Noris, J Am Soc Nephrol, 2005
49 What is ahus? ahus is rare, progressive, life-threatening disease characterised by chronic uncontrolled complement activation identifiable complement gene mutation in 60-70% Thrombotic microangiopathy (TMA) microvasculature thrombosis, inflammation and occlusion with renal and systemic manifestations ongoing subclinical disease Clinical triad of: thrombocytopenia (consumptive) microangiopathic haemolytic anaemia renal impairment (± systemic / CNS symptoms) Noris Stahl, Blood, 2008
50 ahus demographics Incidence approx 2/million population prevalence estimates Age at disease onset 59% 18 years of age 41% >18 years of age oldest presentation 83 years Gender 51% male 49% female Noris et al. Semin Nephrol 2010 Jul;30:
51 ahus outcomes Registry of 273 patients at 1 year after diagnosis up to 60% patients die or ESRD at 3 years, up to 70% die or at ESKD All patients at 1 year after diagnosis ~ 40% die or at ESKD at 3 years 56% die or at ESKD Systemic symptoms common Long-term outcomes not well documented Noris, J Am Soc Nephrol, 2010
52 Systemic clinical ahus manifestations Case series report ahus systemic manifestations in up to 48% patients CNS - coma, stroke, seizure, fluctuating focal signs Cardiovascular - cardiomyopathy, diffuse arterial stenosis, atherosclerosis Gastrointestinal - pancreatitis, colitis, hepatic impairment Other cases - pulmonary hemorrhage, pulmonary oedema, ophthalmological ischaemia 1. Noris M, Remuzzi G. N Engl J Med. 2009;361: Noris M, et al. Clin J Am Soc Nephrol. 2010;5: Neuhaus TJ, Arch Dis Child 1997; 76: Hirt-Minkowski P, Nephron Clin Pract 2010;114:c219 c Lee B, Pediatric Research 2009; 66:
53 Current ahus management Plasmapheresis / exchange / infusion no prospective controlled trials Antihypertensives Corticosteroids IVIg Anticoagulation (as applicable) Immunosuppressive therapy Dialysis Nephrectomy Renal transplantation up to 90% recurrence Liver-kidney transplantation
54 Eculizumab blocks terminal complement activation D + B Proximal Weak Anaphylatoxin C3a C3 C3b C5-convertase C3bi C3bBb CR3 Ba C3b Microbial Opsonization Immune Complex Clearance Terminal C5a C5 C5b C6 C7 C8 C9 Eculizumab binds with high affinity to C5 Proximal functions of complement remain intact Terminal complement activity is blocked C5b-9 Terminal Complement Complex
55 Tolerability of eculizumab Well tolerated in PNH but common side-effects headache nausea nasopharyngitis No HAHA Meningococcal infection eculizumab increases susceptibility to meningococal infection all patients must be vaccinated 14 days prior to treatment patient / parent education


56
57 What is the gold standard therapy for a child with end-stage kidney disease?
58 What is the gold standard therapy for a child with end-stage kidney disease? Pre-emptive living related renal transplantation
59 End-stage renal failure management Renal transplant ESRF management Peritoneal dialysis Haemo -dialysis
60 End-stage renal failure management Renal transplant ESRF management HOSPITAL or HOME Peritoneal dialysis Haemo -dialysis
61 End-stage renal failure management Renal transplant ESRF management HOSPITAL or HOME Peritoneal dialysis Haemo -dialysis HOSPITAL or HOME
62 End-stage renal failure management PRE-EMPTIVE vs ON DIALYSIS Renal transplant ESRF management DECEASED DONOR - en bloc; DBD and DCD kidneys LIVING RELATED / UNRELATED - altruistic - antibody removal - paired / pooled exchange HOSPITAL or HOME Peritoneal dialysis Haemo -dialysis HOSPITAL or HOME


63
64 Nocturnal haemodialysis (NHD) an intensive dialysis modality 6-8 HOURS/SESSION, 3-7 SESSIONS/WEEK associated with a significant improvement of clinical and biochemical parameters compared to conventional dialysis

65
66 Nocturnal haemodialysis Two regional adult NHD programmes USRDS data matched cohort study comparing survival between NHD and deceased and living donor kidney transplantation (DTX and LTX) by matching NHD patients to transplant recipients in a 1:3:3 ratio 177 NHD patients matched to 1062 DTX and LTX recipients (1239 patients) followed for a maximum of 12.4y proportion of deaths among NHD, DTX and LTX patients was 14.7%, 14.3% and 8.5%, respectively (p = 0.006) no difference in adjusted survival between NHD and DTX (HR 0.87, 95% CI ; NHD reference group), while LTX survival was better (HR 0.51, 95% CI )
67
68
69 GOSH patient experience Feels empowered and in control Recovery time minutes rather than hours Urine output did not change in the first year then gradual decline No real diet or fluid restrictions More energy Reduced phosphate binders on nocturnal increased/same for evening dialysis as appetite improved
70 Home haemodialysis Home HD is an option for children Increased dialysis time improve uraemic toxins clearance and patient well-being Possibility that nocturnal offers additional advantages Clear requirement for further research specifically in children

71
72 Number of UK deceased donor kidney Tx April March 2010 Adults Paediatrics Number Year
73 Number of UK living donor kidney Tx 1 April March 2010 Adults Paediatrics Number Year
74 Number of UK deceased & living RTx 1 April March 2010 Adults Paediatrics Number Year
75 First living donor kidney transplants Adult recipients Paediatric recipients % Graft survival % Graft survival Year of transplant (Number at risk on day 0) 30 Year of transplant (Number at risk on day 0) (448) (745) (1000) (2308) (64) (85) (119) (199) Years since transplant Years since transplant
76 Graft survival: First paediatric kidney only transplants in the UK, % Graft survival Cadaveric/Living 10 Cadaveric living Years since transplant



77 UK LKDT activity


78


79
80 ABOi RTx single centre paediatric & adult RTR from 2001 short-term results comparable with those of ABO-compatible (ABOc) living donor kidney transplantation 20 ABOi RTx > 12m (mean 3y) follow-up included all adult crossmatch negative ABOi kidney recipients (n=15) were compared with an adult ABOc living donor recipient control group (n=30), and all paediatric ABOi kidney recipients (<16 years of age) (n=5) were compared with a group of pediatric ABOc kidney recipients (n=18) No significant difference in patient survival, nor in graft survival or in the incidence of acute rejection in any of the groups
81 ABOi renal transplantation Adult RTR mean GFR equivalent at all time points (79-83 ml/min), as was Deltas-creatinine For paediatric RTR, Deltas-creatinine was similar but GFR lower among the ABOi kidney recipients significant reduction (p < ) without rebound in A/B antibody titres after transplantation (median IgG 1:2 and median IgM 1:1>1 year posttransplant) compared with pretransplant levels (median IgG 1:32 and IgM 1:16) ABOi RTx using Ag-specific immunoadsorption and rituximab is equivalent to ABOc living donor kidney transplantation ABOi transplantation after this protocol does not have a negative impact on long-term graft function
82


83
84 Antibody incompatibility ABOi transplantation transplants where the recipient has a blood group incompatibility with the donor eg. A into O, B into O, A into B, B into A eg. AB into A, AB into B, AB into O HLAi transplantation positive crossmatch positive baseline flow cytometric crossmatch or positive complement dependent cytotoxic crossmatch transplants where the recipient has donor specific antibody, but a negative crossmatch, do not fall into this category
85 Options for patients An antibody compatible living donor is preferred so, 1. Remain on the deceased donor list and avoid a living donor transplant 2. Enter KPD (Kidney Paired Donation) scheme - the National Living Donor Kidney Sharing Scheme (NLDKSS) in the UK 3. Undergo a direct antibody incompatible transplant Recommendations: 1. Ensure no alternative antibody compatible living donor is available 2. The recipient should be counselled about all available options
86 ABO and HLA incompatibility 24% of potential LRD are ABOi (GOSH) 14% of waiting list patients are very highly sensitised PRA / crf > 80%; UNOS Expertise in adult and paediatric units is highly specialised clinical experience, protocols, funding Recommendations: 1. centres not performing ABOi/HLAi transplantation should be formally linked to centres which are 2. all recipients with a blood group incompatible donor should be offered the option of referral to a centre performing ABOi/HLAi transplantation
87 Long term results of ABOi RTx Percent allograft survival Years Tanabe et al (1998); Transplantation
88 ABO incompatibility Excellent results from ABOi transplantation patient and renal allograft survival and AMR outcomes similar to compatible transplants Anti-A and anti-b titres vary significantly typically titres of 1 in 8 are used as a threshold to allow transplantation to proceed important to check baseline antibody titres, since these may be low enough to allow transplantation with little or no additional immunosuppressive therapy Recommendation 1. all patients with a blood group incompatible donor should have baseline haemagglutinin titres measured
89 ABO incompatible Tx protocol T-1m: Intravenous rituximab T - 1w: Oral mycophenolate mofetil Oral tacrolimus +/- PX / DFPP / IA D0: D4: Intravenous methylprednisolone Intravenous basiliximab Intravenous basiliximab
90 Tacrolimus/MMF/prednisolone Rituximab 375 mg/kg IVIG (0.5 g/kg) Anti-A1 IgG titre 1:128 1:64 1:32 1:16 1:8 1:4 1:2 1:1 <1:1 Glycosorb Tx Time (days) Am J Transplant. (2005) 5:
91
92 NLDKSS;UK A INTO O 15% B INTO A 36% >85% ABOi match within 4 runs NOT 1 IN 2056 BUT FEW DATA ABOVE 1 IN 256 IN KIDS? URGENCY
93 What are my chances of obtaining a kidney by national Recipient blood group sharing schemes? Recipient blood group O A B AB Donor blood group O 15/114 (13%) 21/42 (50%) 6/22 (27%) 0/1 (0%) A 23/152 (15%) 12/54 (22%) 11/33 (33%) 0/3 (0%) B 6/47 (13%) 10/28 (36%) 0/18 (0%) 1/3 (33%) AB 0/7 (0%) 0/4 (0%) 0/6 (0%) 0/1 (0%)
94 40% Oag anti A Ab anti B Ab 45% 10% Aag (A 1 ~36%, A 2 ~9%) Bag anti A ab anti B Ab AagBag no Ab 5% The likelihood that two unrelated individuals are: - identical is 37.5% - compatible is 26.75% - incompatible is 35.75%
95 No match for kidney paired donation Recommendation: 1. if an ABOi pair are entered into the KPD, the decision should be reviewed if no match has been obtained after 3 or 4 matching runs, and consideration given to direct ABOi transplantation 2. Recipients with low baseline ABO titres can proceed directly to ABOi transplantation - titres of 1 in under 512, 256 or 128
96 Take home messages The future is bright biomarkers Further research RCT in paediatric nephrology RCT in paediatric renal transplantation
97 Any questions?
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Blood Group Incompatible Renal Transplantation and Apheresis. Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT
 Blood Group Incompatible Renal Transplantation and Apheresis Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT Background There is growing interest in transplantation across the
Blood Group Incompatible Renal Transplantation and Apheresis Liz Wright Clinical Nurse Specialist Great Ormond Street Hospital NHS FT Background There is growing interest in transplantation across the
ABO mismatched Renal Transplants
 ABO mismatched Renal Transplants Nicos Kessaris Renal Transplant Surgeon St George s Hospital, London 7 th March 2012 Why? Protocol Risks Experience abroad Experience in UK Experience at St George s Conclusions
ABO mismatched Renal Transplants Nicos Kessaris Renal Transplant Surgeon St George s Hospital, London 7 th March 2012 Why? Protocol Risks Experience abroad Experience in UK Experience at St George s Conclusions
So why have CKD stages I and II at all?!
 So why have CKD stages I and II at all?! Structural / genetic abnormalities e.g. APKD Significant proteinuria Nephrotic range Microscopic haematoproteinuria in the absence of infection e.g. vasculitis?!!
So why have CKD stages I and II at all?! Structural / genetic abnormalities e.g. APKD Significant proteinuria Nephrotic range Microscopic haematoproteinuria in the absence of infection e.g. vasculitis?!!
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Strategies for Desensitization
 Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
Strategies for Desensitization Olwyn Johnston MB, MRCPI, MD, MHSc BC Nephrology Day October 8 th 2010 Pre-transplant crossmatch (CMX) with donor lymphocytes has been standard of practice Positive CDC CXM
ABO. ABO ABO ABO ABO ABO ABO ABO ABO. Key words ABO. Alexandre ABO ABO. double filtration plasmapheresis, DFPP. antibody-mediated rejection, AMR
 ABO ABO ABO ABO ABO ABO ABO ABO ABO ABO.. ABO ABO. ABO. ABO ABO Key words ABO ABO A B antibody-mediated rejection, AMR Alexandre ABO double filtration plasmapheresis, DFPP ABO ABO n ABO n p-value R.....
ABO ABO ABO ABO ABO ABO ABO ABO ABO ABO.. ABO ABO. ABO. ABO ABO Key words ABO ABO A B antibody-mediated rejection, AMR Alexandre ABO double filtration plasmapheresis, DFPP ABO ABO n ABO n p-value R.....
Paired Donation. Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle. Cambridge University NHS Hospitals NHS Foundation trust
 Paired Donation Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle Cambridge University NHS Hospitals NHS Foundation trust Showing a preference 1860 John Calcott Horsley UK Living Donor kidney transplant
Paired Donation Andrew Bradley Rachel Johnson Joanne Allen Susan V Fuggle Cambridge University NHS Hospitals NHS Foundation trust Showing a preference 1860 John Calcott Horsley UK Living Donor kidney transplant
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
M.Weitz has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Prophylactic eculizumab prior to kidney transplantation for atypical hemolytic uremic
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Recent advances in pathogenesis & treatment of ahus
 Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Recent advances in pathogenesis & treatment of ahus Miquel Blasco Pelicano Nephrology and Kidney Transplant Unit Hospital Clínic, Barcelona Atypical Hemolytic Uremic Syndrome (ahus) Ultra-rare disease:
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation
 Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
Spectrum of complement-mediated thrombotic microangiopathies after kidney transplantation Marius Miglinas Vilnius university hospital: Nephrology center, Center of Rare Kidney Diseases Vilnius university
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 7% from 5686 to 5275 The number of deceased kidney donors increased by 7%
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist
 UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
UTI and VUR Practical points and management Kjell Tullus Consultant Paediatric Nephrologist Discussion points Diagnosis VUR Radiological investigations 1. Contamination Problems 2. Bacterial numbers 3.
Desensitization in Kidney Transplant. James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver
 Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Desensitization in Kidney Transplant James Cooper, MD Assistant Professor, Kidney and Pancreas Transplant Program, Renal Division, UC Denver Organ Shortage Currently there are >90,000 patients on the kidney
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique. Mark D. Stegall Mayo Clinic, Rochester, MN
 Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Eculizumab chez les receveurs de greffe rénal à haut risque immunologique Mark D. Stegall Mayo Clinic, Rochester, MN Disclosure. Dr Mark Stegall. Institution : Mayo Clinic, Rochester. Research contracts
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
SA-PO546 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid,
The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033
 5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
5 Kidney Activity Kidney Activity Key messages The number of patients registered on the kidney transplant list this year fell by 4% from 5,233 to 5,033 The number of deceased kidney donors increased by
Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Dialysis
 SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
SP281 Safety and Efficacy of Eculizumab in Pediatric Patients With ahus, With or Without Baseline Johan Vande Walle, 1 Larry A. Greenbaum, 2 Camille L. Bedrosian, 3 Masayo Ogawa, 3 John F. Kincaid, 3 Chantal
Transplantation in Australia and New Zealand
 Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Transplantation in Australia and New Zealand Matthew D. Jose MBBS (Adel), FRACP, FASN, PhD (Monash), AFRACMA Professor of Medicine, UTAS Renal Physician, Royal Hobart Hospital Overview CKD in Australia
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014
 Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
Appendix to Notification Letter for rituximab and eltrombopag dated 20 February 2014 The notification letter which contains details of the decision to widen the restriction criteria for rituximab and eltrombopag
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation
 Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Why so Sensitive? Desensitizing Protocols for Living Donor Kidney Transplantation Stephen J Tomlanovich MD Objectives of this Talk Define the sensitized patient Describe the scope of the problem for a
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist
 Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Why is the management of UTI so controversial? Kjell Tullus Consultant Paediatric Nephrologist Diagnosing a UTI More difficult then most people realise Contaminating culture Bacterial numbers Confusion
Transfusion support in Transplantation
 Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Transfusion support in Transplantation Patricia Campbell University of Alberta Hospitals University of Alberta Objectives UofA transplant programs What we do and why? HLA and ABO incompatible transplants
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Oxford Transplant Centre. Live donor kidney transplantation what if we are not a match?
 Oxford Transplant Centre Live donor kidney transplantation what if we are not a match? page 2 You will already have been provided with information about different types of kidney transplant and the tests
Oxford Transplant Centre Live donor kidney transplantation what if we are not a match? page 2 You will already have been provided with information about different types of kidney transplant and the tests
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant
 SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
SDC, Patients and Methods Complement-dependent lymphocytotoxic crossmatch test () Serum samples from recipients were obtained within 48 hours before transplantation. Pre-transplant donor-specific CXM was
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions. Jonathan Evans Paediatric Nephrologist
 The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
The evidence base for interventions to slow the progression of chronic kidney disease: Medical interventions Jonathan Evans Paediatric Nephrologist CKD in adults Often unrecognised Preventable Major cardiovascular
Progress in Pediatric Kidney Transplantation
 Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
Send Orders for Reprints to reprints@benthamscience.net The Open Urology & Nephrology Journal, 214, 7, (Suppl 2: M2) 115-122 115 Progress in Pediatric Kidney Transplantation Jodi M. Smith *,1 and Vikas
ABO-incompatible kidney transplantation in elderly patients over 60 years of age
 Int Urol Nephrol (2012) 44:1563 1570 DOI 10.1007/s11255-012-0231-z NEPHROLOGY - ORIGINAL PAPER ABO-incompatible kidney transplantation in elderly patients over 60 years of age Junji Uchida Tomoaki Iwai
Int Urol Nephrol (2012) 44:1563 1570 DOI 10.1007/s11255-012-0231-z NEPHROLOGY - ORIGINAL PAPER ABO-incompatible kidney transplantation in elderly patients over 60 years of age Junji Uchida Tomoaki Iwai
For more information about how to cite these materials visit
 Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Should red cells be matched for transfusions to patients listed for renal transplantation?
 Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
Should red cells be matched for transfusions to patients listed for renal transplantation? Dr M.Willicombe Imperial College Renal and Transplant Centre, Hammersmith Hospital Should red cells be matched
ahus A PATIENT S GUIDE To learn more about ahus, visit Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved.
 To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
To learn more about ahus, visit www.ahussource.com ahus A PATIENT S GUIDE Copyright 2011, Alexion Pharmaceuticals, Inc. All rights reserved. SOL 1169 BECOME EMPOWERED By learning more and taking control
THE KIDNEY AND SLE LUPUS NEPHRITIS
 THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
THE KIDNEY AND SLE LUPUS NEPHRITIS JACK WATERMAN DO FACOI 2013 NEPHROLOGY SIR RICHARD BRIGHT TERMINOLOGY RENAL INSUFFICIENCY CKD (CHRONIC KIDNEY DISEASE) ESRD (ENDSTAGE RENAL DISEASE) GLOMERULONEPHRITIS
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk
 R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
R. Coward has documented that he has received cooperative grants from Takeda and Novo Nordisk Advances in our understanding of the pathogenesis of glomerular thrombotic microangiopathy Lindsay Keir Richard
The New Kidney Allocation System: What You Need to Know. Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health
 The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
The New Kidney Allocation System: What You Need to Know Anup Patel, MD Clinical Director Renal and Pancreas Transplant Division Barnabas Health ~6% of patients die each year on the deceased donor waiting
Updates on Paediatric clinical research activities
 Updates on Paediatric clinical research activities Shivaram Hegde Consultant paediatric nephrologist Children Kidney centre UHW, Cardiff Aim to Brief introduction Research updates Improve contribution
Updates on Paediatric clinical research activities Shivaram Hegde Consultant paediatric nephrologist Children Kidney centre UHW, Cardiff Aim to Brief introduction Research updates Improve contribution
Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab
 ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
ORIGINAL ARTICLE Advance Access publication 1 February 2010 Transplantation in highly sensitised patients treated with intravenous immunoglobulin and Rituximab Ana Carina Ferreira 1, Sandra Brum 1, Vasco
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Patient Education Transplant Services. Glossary of Terms. For a kidney/pancreas transplant
 Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Transplant Options for Patients: Choices and Consequences. Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital
 Transplant Options for Patients: Choices and Consequences Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital BC Kidney Days October 6 th 2017 Non contributory Conflict of
Transplant Options for Patients: Choices and Consequences Olwyn Johnston Medical Director Kidney Transplantation Vancouver General Hospital BC Kidney Days October 6 th 2017 Non contributory Conflict of
Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome. September 2013 Reference: E03/PS(HSS)/a.
/a.") Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome September 2013 Reference: E03/PS(HSS)/a England 1 NHS England INFORMATION READER BOX Directorate Medical Operations
Clinical Commissioning Policy Statement: Eculizumab for atypical haemolytic uraemic syndrome September 2013 Reference: E03/PS(HSS)/a England 1 NHS England INFORMATION READER BOX Directorate Medical Operations
PRODUCT INFORMATION. SOLIRIS Concentrated Solution for Intravenous Infusion
 PRODUCT INFORMATION SOLIRIS Concentrated Solution for Intravenous Infusion WARNING: SERIOUS MENINGOCOCCAL INFECTION SOLIRIS increases the risk of meningococcal infections Vaccinate patients with a meningococcal
PRODUCT INFORMATION SOLIRIS Concentrated Solution for Intravenous Infusion WARNING: SERIOUS MENINGOCOCCAL INFECTION SOLIRIS increases the risk of meningococcal infections Vaccinate patients with a meningococcal
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus)
") Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
Specialised Services Policy: CP98 Eculizumab for Atypical Haemolytic Uraemic Syndrome (ahus) Document Author: Assistant Director for Evidence, Evaluation and Effectiveness Executive Lead: Medical Director
H.Jalanko has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve.
 H.Jalanko has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Management dilemmas in infants with congenital nephrotic syndrome (CNS) Hannu Jalanko
H.Jalanko has documented that he has no relevant financial relationships to disclose or conflict of interest to resolve. Management dilemmas in infants with congenital nephrotic syndrome (CNS) Hannu Jalanko
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Recent advances in management of Pulmonary Vasculitis. Dr Nita MB
 Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
Recent advances in management of Pulmonary Vasculitis Dr Nita MB 23-01-2015 Overview of the seminar Recent classification of Vasculitis What is new in present classification? Trials on remission induction
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 30 November 2011
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 30 November 2011 NULOJIX 250 mg, powder for concentrate for solution for infusion B/1 (CIP code: 580 415-7) B/2 (CIP
The CARI Guidelines Caring for Australasians with Renal Impairment. Idiopathic membranous nephropathy: use of other therapies GUIDELINES
 Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
Idiopathic membranous nephropathy: use of other therapies Date written: July 2005 Final submission: September 2005 Author: Merlin Thomas GUIDELINES No recommendations possible based on Level I or II evidence
Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies
 Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies Professor Nick Webb DM FRCP
Clinical Research Facility Central Manchester University Hospitals NHS Foundation Trust Clinical trials in childhood steroid sensitive nephrotic syndrome: the PREDNOS studies Professor Nick Webb DM FRCP
Solid Organ Transplant
 Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
SELECTED ABSTRACTS. All (n) % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%
 % 3-year GS 88% 82% 86% 85% 88% 80% % 3-year DC-GS 95% 87% 94% 89% 96% 80%") SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
SELECTED ABSTRACTS The following are summaries of selected posters presented at the American Transplant Congress on May 5 9, 2007, in San Humar A, Gillingham KJ, Payne WD, et al. Review of >1000 kidney
Hemolytic Uremic Syndrome
 Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Hemolytic Uremic Syndrome Francesco Emma Division of Nephrology and Dialysis Bambino Gesù Children s Hospital, IRCCS Rome, Italy Hemolytic Uremic Syndrome (HUS) microangiopathic hemolytic anemia thrombocytopenia
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
TMA CASE STUDY. Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit
 TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
TMA CASE STUDY Pamela Harmon, RN & Keturah Tomlin, RN Toronto General Hospital Apheresis Unit Cumulative fraction of patients free of events ahus is a catastrophic disease that can result in sudden & progressive
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
New insights in thrombotic microangiopathies : TTP and ahus
 New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
New insights in thrombotic microangiopathies : TTP and ahus Dr Catherine LAMBERT Hematology Cliniques universitaires Saint-Luc Catherine.lambert@uclouvain.be New insights in thrombotic microangiopathies
Epidemiology of kidney diseases in children
 Epidemiology of kidney diseases in children Dr Lesley Rees Gt Ormond St Hospital for Children, London, UK September 2015 Definition of Epidemiology The patterns, causes, and effects of health and diseases
Epidemiology of kidney diseases in children Dr Lesley Rees Gt Ormond St Hospital for Children, London, UK September 2015 Definition of Epidemiology The patterns, causes, and effects of health and diseases
LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE
 & LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
& LONG-TERM OUTCOME OF PATIENTS WITH LUPUS NEPHRITIS: A SINGLE CENTER EXPERIENCE Senija Rašić 1 *, Amira Srna 1, Snežana Unčanin 1, Jasminka Džemidžić 1, Damir Rebić 1, Alma Muslimović 1, Maida Rakanović-Todić
Overview of New Approaches to Immunosuppression in Renal Transplantation
 Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
Overview of New Approaches to Immunosuppression in Renal Transplantation Ron Shapiro, M.D. Professor of Surgery Surgical Director, Kidney/Pancreas Transplant Program Recanati/Miller Transplantation Institute
ABO INCOMPATILIBITY AND TRANSPLANTATION
 ABO INCOMPATILIBITY AND TRANSPLANTATION Aleksandar Mijovic Consultant Haematologist/Senior Lecturer King s College Hospital/NHS Blood and Transplant London, UK RTC Edu Meeting May 2017 ABO antigens Expressed
ABO INCOMPATILIBITY AND TRANSPLANTATION Aleksandar Mijovic Consultant Haematologist/Senior Lecturer King s College Hospital/NHS Blood and Transplant London, UK RTC Edu Meeting May 2017 ABO antigens Expressed
Paediatric Nephrology
 RCPCH Progress Paediatric curriculum for excellence Paediatric Nephrology Level 3 Paediatrics Sub-specialty Syllabus Version 1 Approved by the GMC for implementation from 1st August 2018 The Royal College
RCPCH Progress Paediatric curriculum for excellence Paediatric Nephrology Level 3 Paediatrics Sub-specialty Syllabus Version 1 Approved by the GMC for implementation from 1st August 2018 The Royal College
Chapter 22: Hematological Complications
 Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Chapter 22: Hematological Complications 22.1: Perform a complete blood count at least (Not Graded): daily for 7 days, or until hospital discharge, whichever is earlier; two to three times per week for
Renal Transplant Registry Report 2008
 Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Supporting solid organ transplants: Challenges for Blood Transfusion Labs
 Supporting solid organ transplants: Challenges for Blood Transfusion Labs Dora Foukaneli Consultant in Haematology and Transfusion Medicine NHSBT Cambridge and Addenbrooke s Hospital Addenbrooke s Blood
Supporting solid organ transplants: Challenges for Blood Transfusion Labs Dora Foukaneli Consultant in Haematology and Transfusion Medicine NHSBT Cambridge and Addenbrooke s Hospital Addenbrooke s Blood
Kidney Transplantation in the Elderly. Kristian Heldal, MD, PhD Telemark Hospital Trust, Skien, Norway and University of Oslo
 Kidney Transplantation in the Elderly Kristian Heldal, MD, PhD Telemark Hospital Trust, Skien, Norway and University of Oslo Agenda Background: Age and chronic kidney disease End stage kidney disease:
Kidney Transplantation in the Elderly Kristian Heldal, MD, PhD Telemark Hospital Trust, Skien, Norway and University of Oslo Agenda Background: Age and chronic kidney disease End stage kidney disease:
16.1 Risk of UTI recurrence in children
 16. UTI prognosis 16.1 Risk of UTI recurrence in children Key question: What is the risk of recurrent UTI in children with no known structural or functional abnormalities of the urinary tract with a first
16. UTI prognosis 16.1 Risk of UTI recurrence in children Key question: What is the risk of recurrent UTI in children with no known structural or functional abnormalities of the urinary tract with a first
THERAPEUTIC PLASMA EXCHANGE
 THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
THERAPEUTIC PLASMA EXCHANGE DIRECTORATE OF NEPHROLOGY AND TRANSPLANTATION Background and Indications Therapeutic plasma exchange (TPE) is an extracorporeal blood purification technique in which plasma
SOLIRIS is a Complement Inhibitor Indicated for the Treatment of Patients With PNH to Reduce Hemolysis
 SOLIRIS (eculizumab) SOLIRIS is a Complement Inhibitor Indicated for the Treatment of Patients With PNH to Reduce Hemolysis SOLIRIS is the First and Only Approved Therapy for PNH SOLIRIS (eculizumab) [package
SOLIRIS (eculizumab) SOLIRIS is a Complement Inhibitor Indicated for the Treatment of Patients With PNH to Reduce Hemolysis SOLIRIS is the First and Only Approved Therapy for PNH SOLIRIS (eculizumab) [package
Transplantation: Year in Review
 Transplantation: Year in Review Alexander Wiseman, MD Medical Director, Kidney and Pancreas Transplant Program Associate Professor, Division of Renal Diseases and Hypertension University of Colorado Outline:
Transplantation: Year in Review Alexander Wiseman, MD Medical Director, Kidney and Pancreas Transplant Program Associate Professor, Division of Renal Diseases and Hypertension University of Colorado Outline:
Soliris (eculizumab, rmc) Section 100 Restriction Criteria
 Section 100 Restriction Criteria") Soliris (eculizumab, rmc) Section 100 Restriction Criteria A guide to initiation and ongoing access to (Section 100) funded Soliris for the treatment of patients with atypical Haemolytic Uraemic Syndrome
Soliris (eculizumab, rmc) Section 100 Restriction Criteria A guide to initiation and ongoing access to (Section 100) funded Soliris for the treatment of patients with atypical Haemolytic Uraemic Syndrome
Transplant in Pediatric Heart Failure
 Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS
 APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
APHERESIS FOR DESENSITIZATION OF NON-RENAL TRANSPLANTS GOW AREPALLY, MD MEDICAL DIRECTOR DUKE THERAPEUTIC APHERESIS SERVICE ASSOCIATE PROFESSOR, MEDICINE AMERICAN SOCIETY FOR APHERESIS MAY 25 TH 2013 OVERVIEW
LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD
 LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD Outline: PART 1 : Update on safety of nephrectomy for living donor candidate PART 2 : Latest guideline recommendation
LIVE KIDNEY DONOR RISK PREDICTION ; NEW PARADIGM, NEW CALCULATORS PEDRAM AHMADPOOR MD Outline: PART 1 : Update on safety of nephrectomy for living donor candidate PART 2 : Latest guideline recommendation
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES ALDO E CELE DACCO
 ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
ISTITUTO DI RICERCHE FARMACOLOGICHE MARIO NEGRI CENTRO MARIO DI NEGRI RICERCHE INSTITUTE CLINICHE FOR PHARMACOLOGICAL PER LE MALATTIE RESEARCH RARE CLINICAL RESEARCH CENTER ALDO E FOR CELE RARE DACCO DISEASES
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
Literature Review Transplantation
 Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Literature Review 2010- Transplantation Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of
Barriers to Transplantation
 Barriers to Transplantation Ruth McCarrell RN BSN CNeph(C) Clinical Nurse Leader Kidney transplant Program St. Paul s Hospital Email: rmccarrell@providencehealth.bc.ca Overview Transplant Basics Living
Barriers to Transplantation Ruth McCarrell RN BSN CNeph(C) Clinical Nurse Leader Kidney transplant Program St. Paul s Hospital Email: rmccarrell@providencehealth.bc.ca Overview Transplant Basics Living
7/14/2014. SOLIRIS (eculizumab) SOLIRIS PNH Clinical Studies. SOLIRIS Blocks Terminal Complement. 86% Reduction in LDH: TRIUMPH and SHEPHERD
 SOLIRIS PNH Clinical Studies. SOLIRIS Blocks Terminal Complement. 86% Reduction in LDH: TRIUMPH and SHEPHERD") Proximal Terminal Lactate Dehydrogenase (U/L) 7/1/1 SOLIRIS (eculizumab) Humanized First in Class Anti - C5 Antibody SOLIRIS (eculizumab) Human Framework Regions No mutations Germline SOLIRIS is a Complement
Proximal Terminal Lactate Dehydrogenase (U/L) 7/1/1 SOLIRIS (eculizumab) Humanized First in Class Anti - C5 Antibody SOLIRIS (eculizumab) Human Framework Regions No mutations Germline SOLIRIS is a Complement
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE. Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham
 SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
Lupus and Your Kidneys. Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia
 Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Lupus and Your Kidneys Michael P. Madaio, MD Professor of Medicine Chairman of Medicine Medical College of Georgia Augusta, Georgia Kidney Inflammation and Abnormal Function as a Result of Lupus (Lupus
Clinical and laboratory indices of severe renal lesions in children with febrile urinary tract infection
 Clinical and laboratory indices of severe renal lesions in children with febrile urinary tract infection Constantinos J. Stefanidis Head of Pediatric Nephrology P. & A. Kyriakou Children s Hospital, Athens,
Clinical and laboratory indices of severe renal lesions in children with febrile urinary tract infection Constantinos J. Stefanidis Head of Pediatric Nephrology P. & A. Kyriakou Children s Hospital, Athens,
PNH ahus. Dosing and Administration. For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients
 and atypical Hemolytic Uremic Syndrome (ahus) patients") For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
For Paroxysmal Nocturnal Hemoglobinuria (PNH) and atypical Hemolytic Uremic Syndrome (ahus) patients PNH ahus Dosing and Administration Soliris is indicated for the treatment of patients with paroxysmal
Kidney disease associated with autoimmune disease
 Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as