Introduction. Peripheral arterial disease. Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone
|
|
|
- Moris Nichols
- 6 years ago
- Views:
Transcription
1 1
2 Introduction 2
3 Introduction Peripheral arterial disease Affects 20% adults in Europe and North America In the UK /million PAD, 1-2% require amputation LLA 8-15% in people with diabetes with up to 70% dying <5 years of surgery Hospital inpatient data - 5,498 FCE (2009/10), & 530 deaths in England alone Previous reports indicate mortality is high reflecting age and comorbidites 3
4 Introduction Wide geographic variation in the number of amputations carried out Peri-operative cardiac complications are the leading cause of morbidity & mortality following surgery Previous guidelines VSGBI Diabetes UK BACPAR 4
5 Aim To explore remediable factors in the process of care of patients undergoing major lower limb amputation 5
6 Objectives Pre-operative care Access to multidisciplinary teams and a multiprofessional pathway of care Pain management Clinical care of the patient Optimisation of comorbidities, including diabetic control Peri-operative care The scheduling of surgery, including priority and cancellations Seniority of clinicians (surgery and anaesthesia) Operation undertaken Antibiotic prophylaxis, venous thromboembolism prophylaxis Diabetes control Anaesthetic care 6
7 Objectives Post operative care Access to critical care Diabetes control Pain management Wound care Rehabilitation Organisational factors Hub & spoke arrangements Management of diabetic foot sepsis including multidisciplinary care Access to surgery Availability of rehabilitation and prosthetic services Submission of data to the NVD (NVR) 7
8 Objectives Hospital participation Organisational data Clinical data Study population 6 month data collection period OPCS codes amputation of leg or operations on amputation stump ICD10 codes diseases of the circulatory system or diabetes Case identification Local reporters identified all cases 7 cases per hospital/3 per clinician 8
9 Method Questionnaires Organisational Clinical Advisor assessment form Therapy assessment form Case notes Medical notes from admission to discharge MDT notes Imaging reports Consent forms Operation notes (including anaesthetic records) Nursing notes Rehabilitation (including physiotherapy) notes Drug charts 9

10 Data returns 10
11 Patient overview 11

12 Reason for admission 12

13 Admission category 13
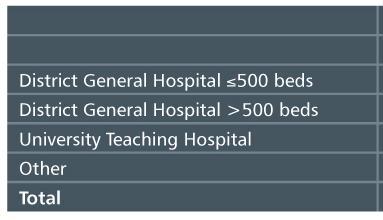
14 Organisation of care 14
15 Pre-operative care 15

16 Pathway for admission 16

17 Admitting ward 17
18 First consultant review 18
19 First consultant review 19
20 Co-morbidities 20
21 Co-morbidities In 123/138 patients an adequate attempt to control co-morbidities was made 21

22 Pre-operative medical review 22
23 Peri-operative care 23
24 Consultant vascular surgeon review 24
25 Consultant vascular surgeon review 25
26 Vascular surgeon review 1:4 emergency admissions not seen within 72h 26
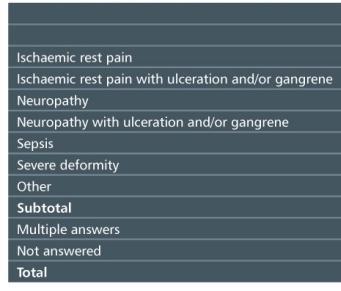

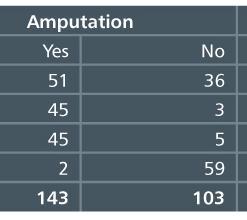
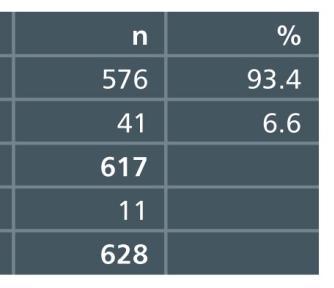
27 Indication for amputation 27

28 Angiography and duplex ultrasound 28

29 Inadequate assessment of limb 29
30 Time from assessment to operation 30

31 Delay between assessment and surgery 31

32 Limb salvage prior to amputation Advisors: appropriate in a further 22 (7.7%) patients 32
 had no MDT for amputees 33")
33 MDT (Organisational data) 58/140 (41%) had no MDT for amputees 33

34 MDT discussion 40% discussed: Centralisation should = dedicated MDT 34

35 Pre-operative support services 349 diabetics Potential impact on post-op recovery, rehab & discharge 35
36 Overall assessment of pre-operative care 36

37 Overall assessment of pre-operative care 37


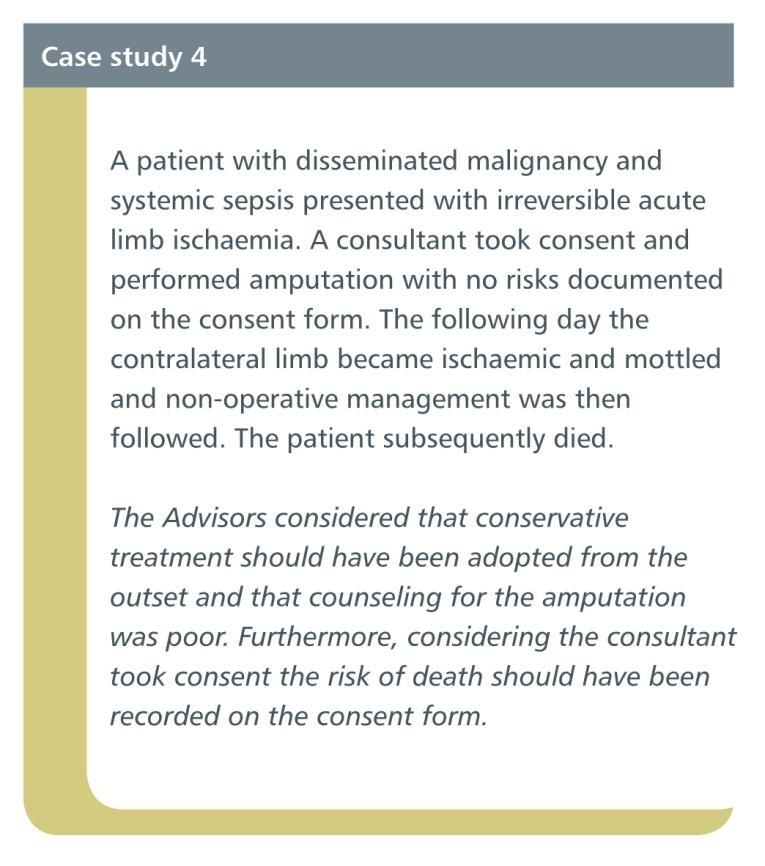
38 Consent 38
39 Consent 39

40 Consent: Poor or unacceptable information 40
41 41
42 42
43 Pre-operative investigations Advisors considered work-up adequate in 92.6% 43
 had a protocol for prophylaxis")
44 Prophylactic antibiotics Organisational data: 131/137 (96%) had a protocol for prophylaxis 44
")
45 MRSA screening 85% screened: 96% units screen routinely (Organisational data) 45

46 Urgency of surgery and type of theatre 57% emergency theatre QIF >75% elective n = 333 n =
47 Time to operation 47
48 Time to operation 48

49 Impact of the delay 49
50 Duration of the delay Significant delay in 118/617 (19%) patients 50

51 Reasons for delay in surgery 64 beyond surgeon s control 52 organisational or because using CEPOD theatre *Transfer, W/E Critical care bed 51

52 Pre-operative anaesthetic review 52


53 Pre-operative anaesthetic review Surgery: consultant present for 85% cases 53

54 Anaesthetic care 54

55 Methods of anaesthesia 55
56 The operation 56

57 Type of amputation performed 57

58 Seniority of surgeon operating and in theatre 58

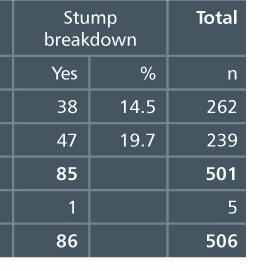
59 Grade of surgeon 48/533 patients booked & cancelled at least once 59

60 Appropriate procedure undertaken 60

61 Reason for inappropriate surgery 61
62 Intra- and post operative monitoring 42 immediate post-op complications 10 = bleeding 10 = cardiac 6 = hypotension 62
63 Post operative surgical care 63

64 Post operative destination and outcome 64
65 Escalation of care 2 delayed, 5 not transferred 65

66 Escalation of care 66
67 Escalation of care 67
 had a complication 68")
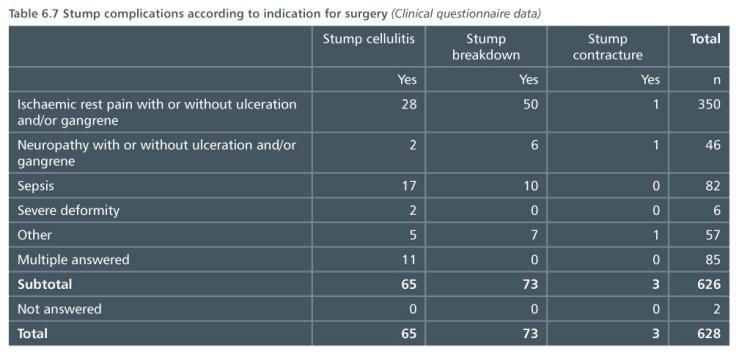
68 Stump complications 164/437 (37%) had a complication 68
69 Stump complications 69
70 Stump complications 70
71 Post operative medical care 71

72 Post operative complications 72
73 Post operative complications Frequent occurrence: 249/529 (47.1%) Advisor reviewed cases 290/628 (46.2%) Clinical questionnaire Medical twice as common as stump related complications 73
 patients reviewed by at least one non-surgical specialist")
74 Post operative physician review 319/529 (59.2%) patients reviewed by at least one non-surgical specialist (excludes microbiology) 74

75 Post operative physician review No relationship between: Complications and physician review Kidney failure and renal medicine review Myocardial infarction/arrhythmia and cardiology review 75
76 76
77 77
78 Physician involvement Pre operative 39.7% Post operative 59.2% Whole pathway 66.1% Recommendation: Model of medical care that includes regular review by physician and surgeon throughout the in-patient stay. 78
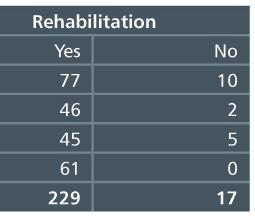
79 Rehabilitation and discharge 79

80 Co-ordination of care Complex patients Mobility changes admission to discharge Planning and care co-ordination important 80

81 Early planning of rehabilitation 81
82 Early planning of rehabilitation 82

83 Pre-operative discharge planning 83
84 Named individual available 84
 cases additional review appropriate Most common omissions: Psychology")
85 Rehabilitation 91/409 (22.2%) cases additional review appropriate Most common omissions: Psychology 38 Amputee rehabilitation 33 Foot care team 21 85

86 Post-operative physiotherapy 86
87 Physiotherapy 78/126 (62.4%) not suitable for early walking aids 36 cases where use delayed inappropriately 87

88 Falls risk assessment 88

89 Falls Adverse consequences (Advisors): Eleven stump complications 3 required further surgery One fracture 89
 Referral generally by combination of medical staff and physiotherapists")
90 Prosthetic services 124/169 hospitals formal arrangements for referral to prosthetics When prosthetics not available on site average distance 21 miles (<1 100) Referral generally by combination of medical staff and physiotherapists 90
91 Prosthetics 91
92 92
93 93
94 Overall quality of rehabilitation 94
95 Discharge planning 95
96 Discharge planning 96

97 Care beyond the acute hospital 97
98 Discharge from hospital 57.3% 5% 12.4% 25.3% 98
99 Delayed discharge 99

100 Delayed discharge Overall 75 cases of delay for non-medical reasons 100
101 101
102 102
103 Diabetes care 103
104 Diabetes care 349/628 patients diabetes (55.6%) Age 68 (no diabetes, 71) Complex diabetes 75/349 (21.5%) type 1 diabetes Population 10% type 1 diabetes 183/313 (58.5%) on insulin Population 40% diabetic patients on insulin 104
105 Pre-operative review 73/132 (55.3%) hospitals performing amputations, policy of routine review by diabetes specialist nurse (DNS) 160/274 (58.4%) pre-op review by DNS 123/217 (56.7%) peer reviewed cases advice given by diabetes team on blood sugar control 105
 had surgery on day of")
106 Insulin use and DNS review Advisors view All patients would benefit from DNS review pre-op Review by diabetologist would potentially improve care and optimise co-morbidity Only 31 cases (9%) had surgery on day of admission 106
107 Insulin infusions - hypoglycaemia 173/278 (62.2%) patients received insulin infusion 107
108 Insulin infusions - management 108
109 Glycaemic control Poor or unacceptable at some point in pathway in at least 26.7% of cases 109

110 Diabetes treatments 110

111 Diabetes prescribing 111

112 Diabetes prescribing 112
113 Outcomes and diabetes Complications: (Clinical Questionnaire) No differences: Individual complications Infections Cardiovascular 30 day mortality: Diabetes 11.6% No diabetes 13.3% 113
114 114
115 115
116 Diabetes care 116
117 Outcomes 117
118 Outcomes at 30 days 2009 VSGBI AGM: mortality 17% HES, 9% NVD 407/ % 2010 VSGBI QIF: mortality <5% by / % 77/ % 118

119 Outcome by mode of admission > 119

120 Morbidity & mortality meetings 120
121 VSGBI QIF Pre-operative aspects of care Implemented The decision with the patient to perform amputation should be timed and recorded in the notes Controllable risk factors should be optimised Antithrombotic prophylaxis should be prescribed and continued at least until discharge from hospital 121
122 VSGBI QIF Pre-operative aspects of care Implemented The decision with the patient to perform amputation should be timed and recorded in the notes Controllable risk factors should be optimised Antithrombotic prophylaxis should be prescribed and continued at least until discharge from hospital Not implemented Pain should be controlled, and the pain team involved if needed Patients should be assessed and managed by specialist MDT A named individual (identified pre-op) should be responsible for each patient (co-ordinate care, rehab and discharge planning) All patients should have formal risk assessment by, or in consultation with a consultant anaesthetist Discharge planning and rehabilitation should be considered preoperatively, and review by the rehabilitation team encouraged 122
123 VSGBI QIF Peri-operative aspects of care Implemented Anaesthesia should be given by a senior anaesthetist (post FRCA); a trainee should have consultant supervision available Amputation should only be undertaken in a facility with ready access to blood products and access to level III critical care All patients to have antibiotic prophylaxis, type of antibiotic according to local policy 123
124 VSGBI QIF Peri-operative aspects of care Implemented Anaesthesia should be given by a senior anaesthetist (post FRCA); a trainee should have consultant supervision available Amputation should only be undertaken in a facility with ready access to blood products and access to level III critical care All patients to have antibiotic prophylaxis, type of antibiotic according to local policy Not implemented Operation should be undertaken on a planned operating list in normal working hours (target 75% of all major amputations) Patients not on a planned list should have surgery within 48h of decision to operate and no patient should be deferred more than once (unless new medical contraindications) Aim to undertake below knee amputation (BKA) wherever appropriate and have below knee: above knee ratio > 1 124
125 VSGBI QIF Post-operative aspects of care Implemented Amputation should be undertaken in a unit with 24/7 network or local vascular cover, with access to multi-professional support (cardiac, renal, respiratory, diabetes) 125
126 VSGBI QIF Post-operative aspects of care Implemented Amputation should be undertaken in a unit with 24/7 network or local vascular cover, with access to multi-professional support (cardiac, renal, respiratory, diabetes) Not implemented There should be a formal pain management protocol, and access to an acute pain team There should be prompt access to a local amputee rehab team including early mobilisation and physiotherapy There should be continued discharge planning home, or to an appropriate facility There should be formal referral to a specialist rehabilitation team (prosthetics) Optimal medical management and health education should be completed before discharge 126
127 Overall assessment of care 127
128 Principal recommendations Best practice clinical care pathway to support QIF A best practice clinical care pathway, supporting the aims of the Vascular Society s Quality Improvement Framework for Major Amputation Surgery, and covering all aspects of the management of patients requiring amputation should be developed. This should include protocols for transfer, the development of a dedicated multidisciplinary team (MDT) for care planning of amputees and access to other medical specialists and health professionals both pre- and post operatively to reflect the standards of the Vascular Society of Great Britain and Ireland, the British Association of Chartered Physiotherapists in Amputee Rehabilitation and the British Society of Rehabilitation Medicine. It should promote greater use of dedicated vascular lists for surgery and the use of multidisciplinary records. 128
129 Principal recommendations Diabetics should be reviewed by specialist diabetes team both pre- and post-operatively All patients with diabetes undergoing lower limb amputation should be reviewed both pre- and post operatively by the specialist diabetes team to optimise control of diabetes and management of co-morbidities. The pre-operative review should not delay the operation in patients requiring emergency surgery. 129
130 Principal recommendations Vascular review within 24 hours if admitted under another specialty When patients are admitted to hospital as an emergency with limbthreatening ischaemia, including acute diabetic foot problems, they should be assessed by a relevant consultant within 12 hours of the decision to admit or a maximum of 14 hours from the time of arrival at the hospital, in line with current guidance. If this is not a consultant vascular surgeon then one should be asked to review the patient within 24 hours of admission. 130
131 Principal recommendations Commence planning for rehabilitation and discharge as early as possible For patients undergoing major limb amputation, planning for rehabilitation and subsequent discharge should commence as soon as the requirement for amputation is identified. All patients should have access to a suitably qualified amputation/discharge co-ordinator. 131
132 Principal recommendations Surgery on planned operating lists within 48 hours As recommended in the Quality Improvement Framework for Major Amputation Surgery (VSGBI), amputations should be done on a planned operating list during normal working hours and within 48 hours of the decision to operate. Any case waiting longer than this should be the subject of local case review to identify reasons for delay and improve subsequent organisation of care. 132
133 133
A Best Practice Clinical Care Pathway for Major Amputation Surgery
 A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
A Best Practice Clinical Care Pathway for Major Amputation Surgery April 2016 Introduction The perioperative mortality rate after major lower limb amputation in the UK is unacceptably high in modern medical
9 Diabetes care. Back to contents
 Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
Back to contents Diabetes is a major risk factor for the development of peripheral vascular disease and 349/628 (55.6%) of the patients in this study had diabetes. Hospital inpatients with diabetes are
SUMMARY Full report available to download at Lower Limb Amputation: Working Together
 Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator SUMMARY Full report available to download at www.ncepod.org.uk Lower Limb Amputation: Working
Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator SUMMARY Full report available to download at www.ncepod.org.uk Lower Limb Amputation: Working
Self- Assessment. Self- assessment checklist
 Self- Assessment Peer Review Self- assessment checklist (Based on RCA guidelines for the provision of anaesthetic services 2004, RCA/AA Guide for Departments of Anaesthesia 2002, NSF for children Standard
Self- Assessment Peer Review Self- assessment checklist (Based on RCA guidelines for the provision of anaesthetic services 2004, RCA/AA Guide for Departments of Anaesthesia 2002, NSF for children Standard
Hip Fracture (HFR) Measures Document
 Measures Document") Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Hip Fracture (HFR) Measures Document HFR Version: 2 - covering patients discharged between 01/10/2017 and present. Programme Lead: Sam Doddridge Clinical Leads: Ms Phil Thorpe Dr John Tsang Number of Measures
Diabetes (DIA) Measures Document
 Measures Document") Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Diabetes (DIA) Measures Document DIA Version: 2.1 - covering patients discharged between 01/07/2016 and present. Programme Lead: Liz Kanwar Clinical Lead: Dr Aftab Ahmad Number of Measures In Clinical
Wales Abdominal Aortic Aneurysm Screening Programme Proposal Paper: The Implementation and Development of Elective Vascular Networks
 Wales Abdominal Aortic Aneurysm Screening Programme Proposal Paper: The Implementation and Development of Elective Vascular Networks Authors: Mr Rhys Blake; Mrs Llywela Wilson; Dr Rosemary Fox; Dr Gareth
Wales Abdominal Aortic Aneurysm Screening Programme Proposal Paper: The Implementation and Development of Elective Vascular Networks Authors: Mr Rhys Blake; Mrs Llywela Wilson; Dr Rosemary Fox; Dr Gareth
Audit of perioperative management of patients with fracture neck of femur
 Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Audit of perioperative management of patients with fracture neck of femur *M Dissanayake 1, N Wijesuriya 2 Registrar in Anaesthesia 1, Consultant Anaesthetist 2, North Colombo Teaching Hospital, Ragama,
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
Lower Limb Amputation: Working Together
 Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator Lower Limb Amputation: Working Together A review of the care received by patients who underwent
Physiotherapists Interventional Radiologists Psychologists herapists TOccupational amputation co0ordinator Lower Limb Amputation: Working Together A review of the care received by patients who underwent
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
*Corresponding Author:
 Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
Audit of venous thromboembolism prophylaxis administered to general surgical patients undergoing elective and emergency operations at National Hospital, Sri Lanka *Migara Seneviratne 1, Asanka Hemachandra
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Scottish Standards of Care for Hip Fracture Patients
 Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Scottish Standards of Care for Hip Fracture Patients This document has been prepared in collaboration with Healthcare Improvement Scotland to align with the forthcoming updated Older People in Hospitals
Audit and Implementation Guide: Clinical guidelines for the pre and post operative physiotherapy management of adults with lower limb amputations
 2nd Edition- 2016 Audit and Implementation Guide: Clinical guidelines for the pre and post operative physiotherapy British Association of Chartered Physiotherapists in Amputee Rehabilitation NICE has accredited
2nd Edition- 2016 Audit and Implementation Guide: Clinical guidelines for the pre and post operative physiotherapy British Association of Chartered Physiotherapists in Amputee Rehabilitation NICE has accredited
NATIONAL VASCULAR REGISTRY Annual report
 NATIONAL VASCULAR REGISTRY 2015 Annual report November 2015 This report was prepared by Clinical Effectiveness Unit, The Royal College of Surgeons of England Mr Sam Waton, NVR Project Manager Dr Amundeep
NATIONAL VASCULAR REGISTRY 2015 Annual report November 2015 This report was prepared by Clinical Effectiveness Unit, The Royal College of Surgeons of England Mr Sam Waton, NVR Project Manager Dr Amundeep
Formation of Vascular Network and Centralised Intervention Centres
 Cardiac and Stroke Networks in Lancashire & Cumbria Formation of Vascular Network and Centralised Intervention Centres Vascular Services SERVICE SPECIFICATION The provision of vascular surgery needs to
Cardiac and Stroke Networks in Lancashire & Cumbria Formation of Vascular Network and Centralised Intervention Centres Vascular Services SERVICE SPECIFICATION The provision of vascular surgery needs to
Rehabilitation - Reducing costs and hospital stay. Dr Elizabeth Aitken Consultant Physician
 Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
Rehabilitation - Reducing costs and hospital stay Dr Elizabeth Aitken Consultant Physician What factors affect outcome? Comorbidities Cardiac Respiratory Neurological Nutritional issues Diabetes Anaemia
IMPROVING INSULIN SAFETY IN HOSPITAL
 FEATURE IMPROVING IN HOSPITAL PHOTO: DIABETES UK Medication errors are not uncommon among people with diabetes admitted to hospital and the consequences for their health can be very serious. However, hospitals
FEATURE IMPROVING IN HOSPITAL PHOTO: DIABETES UK Medication errors are not uncommon among people with diabetes admitted to hospital and the consequences for their health can be very serious. However, hospitals
Making Foot Surgery Safer for Patients with Diabetes
 Making Foot Surgery Safer for Patients with Diabetes Building a New Trust Pathway Patient Safety Briefing The Newcastle Peri-operative Diabetes Pathway Launched 9 May 2016 Aims to join up peri-operative
Making Foot Surgery Safer for Patients with Diabetes Building a New Trust Pathway Patient Safety Briefing The Newcastle Peri-operative Diabetes Pathway Launched 9 May 2016 Aims to join up peri-operative
Developing a pathway of. and care planning for people with diabetes
 Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
Developing a pathway of preoperative assessment and care planning for people with diabetes Louise Hilton, Marie Digner Diabetes is a common endocrine condition affecting 1.4 million people in the UK, with
Implementing the updated NICE Guidance on the Diabetic Foot
 Implementing the updated NICE Guidance on the Diabetic Foot Rachel Berrington Senior Diabetes Specialist Nurse Foot Lead University Hospitals of Leicester NHS Trust Key Priorities for Implementation NG19
Implementing the updated NICE Guidance on the Diabetic Foot Rachel Berrington Senior Diabetes Specialist Nurse Foot Lead University Hospitals of Leicester NHS Trust Key Priorities for Implementation NG19
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence!
 Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
Implementing a new Orthogeriatric model to improve patient care and outcomes Aiming for Excellence! Introduction Hip fractures effect 70,000 people in UK Central challenge for UK Trauma services- 560 in
SAFE HIP FRACTURES. Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust
 SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
SAFE HIP FRACTURES Dr Karthik Kayan MD FRCP Consultant Physician and Orthogeriatrician Stockport NHS Foundation Trust Why hip fracture? Common in older adult (~84 years) UK current incidence : 70000 (Stockport
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry
 National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
National Vascular Registry AAA Repair Patient Details Patient Consent* 0 No 1 Yes 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s)
Fixing footcare in Sheffield: Improving the pathway
 FOOTCARE CASE STUDY 1: FEBRUARY 2015 Fixing footcare in Sheffield: Improving the pathway SUMMARY The Sheffield Teaching Hospitals NHS Foundation Trust diabetes team transformed local footcare services
FOOTCARE CASE STUDY 1: FEBRUARY 2015 Fixing footcare in Sheffield: Improving the pathway SUMMARY The Sheffield Teaching Hospitals NHS Foundation Trust diabetes team transformed local footcare services
NATIONAL VASCULAR C REGISTRY Annual Report
 NATIONAL VASCULAR C REGISTRY 2017 Annual Report November 2017 This report was prepared by Clinical Effectiveness Unit, The Royal College of Surgeons of England Mr Sam Waton, NVR Project Manager Dr Amundeep
NATIONAL VASCULAR C REGISTRY 2017 Annual Report November 2017 This report was prepared by Clinical Effectiveness Unit, The Royal College of Surgeons of England Mr Sam Waton, NVR Project Manager Dr Amundeep
SCHEDULE 2 THE SERVICES. A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Clinical Lead Period Date of Review 170004/S Specialised Vascular Services (Adults) 12 months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service Commissioner Lead Clinical Lead Period Date of Review 170004/S Specialised Vascular Services (Adults) 12 months 1. Population
The Perioperative Care Chain is Only as Strong as its weakest link
 The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
The Perioperative Care Chain is Only as Strong as its weakest link Associate Professor Kerin Fielding The University of Notre Dame, Australia School of Medicine, Sydney Outline The perioperative chain
High Tibial Osteotomy surgery
 Golden Jubilee National Hospital NHS National Waiting Times Centre High Tibial Osteotomy surgery Patient information guide Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
Golden Jubilee National Hospital NHS National Waiting Times Centre High Tibial Osteotomy surgery Patient information guide Agamemnon Street Clydebank, G81 4DY (: 0141 951 5000 www.nhsgoldenjubilee.co.uk
FOOT AND ANKLE ARTHROSCOPY
 FOOT AND ANKLE ARTHROSCOPY Information for Patients WHAT IS FOOT AND ANKLE ARTHROSCOPY? The foot and the ankle are crucial for human movement. The balanced action of many bones, joints, muscles and tendons
FOOT AND ANKLE ARTHROSCOPY Information for Patients WHAT IS FOOT AND ANKLE ARTHROSCOPY? The foot and the ankle are crucial for human movement. The balanced action of many bones, joints, muscles and tendons
Commissioning for Better Outcomes in COPD
 Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
Commissioning for Better Outcomes in COPD Dr Matt Kearney Primary Care & Public Health Advisor Respiratory Programme, Department of Health General Practitioner, Runcorn November 2011 What are the Commissioning
Information for Patients having Total Knee Replacement Surgery
 Information for Patients having Total Knee Replacement Surgery Hello You will be coming into hospital for your surgery and we hope your stay will be pleasant. We have written this booklet to give you information
Information for Patients having Total Knee Replacement Surgery Hello You will be coming into hospital for your surgery and we hope your stay will be pleasant. We have written this booklet to give you information
Shaping Diabetes Services in Southern Derbyshire. A vision for Diabetes Services For Southern Derbyshire CCG
 Shaping Diabetes Services in Southern Derbyshire A vision for Diabetes Services For Southern Derbyshire CCG Vanessa Vale Commissioning Manager September 2013 Contents 1. Introduction 3 2. National Guidance
Shaping Diabetes Services in Southern Derbyshire A vision for Diabetes Services For Southern Derbyshire CCG Vanessa Vale Commissioning Manager September 2013 Contents 1. Introduction 3 2. National Guidance
DOCUMENT CONTROL PAGE
 DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
DOCUMENT CONTROL PAGE Title Title: UNDERGOING SPINAL DEFORMITY SURGERY Version: 2 Reference Number: Supersedes Supersedes: all other versions Description of Amendment(s): Revision of analgesia requirements
Insights on Diabetic Foot Management in UK
 Insights on Diabetic Foot Management in UK Presented by Helen CHU KEC POD I / TKOH POD i/c 2015/16 Overseas Corporate Scholarship Program for podiatrists in Diabetic Foot Management London / Leicester,
Insights on Diabetic Foot Management in UK Presented by Helen CHU KEC POD I / TKOH POD i/c 2015/16 Overseas Corporate Scholarship Program for podiatrists in Diabetic Foot Management London / Leicester,
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
19 Date clinically ready for DD/MM/YYYY Record date patient was clinically ready for discharge after delay 2
 Australian Rehabilitation Outcomes Centre (AROC) Amputation Impairment specific adjunct module to the AROC dataset Please use this excel workbook to record additional data on your amputatee patients. Collection
Australian Rehabilitation Outcomes Centre (AROC) Amputation Impairment specific adjunct module to the AROC dataset Please use this excel workbook to record additional data on your amputatee patients. Collection
6. Endovascular aneurysm repair
 Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Introduction The standard treatment for aortic aneurysm, open repair, involves a large abdominal incision and cross-clamping of the aorta. In recent years, a minimally invasive technique, endovascular
Frequently Asked Questions: Riverview Rehabilitation Center
 Frequently Asked Questions: Riverview Rehabilitation Center WHAT SERVICES ARE PROVIDED? Riverview Rehabilitation Center provides a comprehensive, interdisciplinary and functionally based treatment program
Frequently Asked Questions: Riverview Rehabilitation Center WHAT SERVICES ARE PROVIDED? Riverview Rehabilitation Center provides a comprehensive, interdisciplinary and functionally based treatment program
These are guidelines only and can be deviated from if it is thought to be in the patient s best interest.
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics Venous thromboembolism (VTE) is a recognised complication associated with inactivity and surgical procedures. Therefore, all
Venothromboembolism prophylaxis: Trauma and Orthopaedics Clinical guideline, V2
 Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
Clinical Guideline Venothromboembolism prophylaxis: Trauma and Orthopaedics 11/11/11 TEMPORARY GUIDANCE There is no prophylactic tinzaparin available in the Trust currently. Please substitute enoxaparin
UNICOMPARTMENTAL KNEE REPLACEMENT (UKR) PATIENT INFORMATION
 PATIENT INFORMATION") UNICOMPARTMENTAL KNEE REPLACEMENT (UKR) PATIENT INFORMATION The following information is to help you understand what is going to happen when you have a UKR. It is only a guide and some aspects will vary
UNICOMPARTMENTAL KNEE REPLACEMENT (UKR) PATIENT INFORMATION The following information is to help you understand what is going to happen when you have a UKR. It is only a guide and some aspects will vary
Acutely Ischaemic Arm Spoke Sites (RWHT + WMH)
") Ward In patients/medical ward Acutely Ischaemic Arm Spoke Sites (RWHT + WMH) Sudden onset of painful, pale and cold arm. Worrying features: -loss of sensation In patients/medical ward On call surgical
Ward In patients/medical ward Acutely Ischaemic Arm Spoke Sites (RWHT + WMH) Sudden onset of painful, pale and cold arm. Worrying features: -loss of sensation In patients/medical ward On call surgical
Foot and ankle fractures
 Foot and ankle fractures Some fractures can be managed without surgery, but others require surgery to achieve the best possible outcome. Fractures and injuries to joints have a high risk of developing
Foot and ankle fractures Some fractures can be managed without surgery, but others require surgery to achieve the best possible outcome. Fractures and injuries to joints have a high risk of developing
Rehabilitation/Geriatrics ADMISSION CRITERIA. Coordinated Entry System
 Rehabilitation/Geriatrics ADMISSION CRITERIA Coordinated Entry System Table of Contents Rehabilitation and Geriatric Service Sites 3 Overview of Coordinated Entry System...4 Geriatric Rehabilitation Service
Rehabilitation/Geriatrics ADMISSION CRITERIA Coordinated Entry System Table of Contents Rehabilitation and Geriatric Service Sites 3 Overview of Coordinated Entry System...4 Geriatric Rehabilitation Service
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015
 What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
What is Acute Oncology? Kay McCallum Acute Oncology Advanced Nurse Practitioner John Radcliffe Hospital Oxford September 2015 What is Acute Oncology? Outline of Talk Concept of Acute Oncology Service (AOS)
Joint Working Group to produce guidance on delivering an Endovascular Aneurysm Repair (EVAR) Service.
 Service.") Joint Working Group to produce guidance on delivering an Endovascular Aneurysm Repair (EVAR) Service. Royal College of Radiologists British Society of Interventional Radiology The Vascular Society of Great
Joint Working Group to produce guidance on delivering an Endovascular Aneurysm Repair (EVAR) Service. Royal College of Radiologists British Society of Interventional Radiology The Vascular Society of Great
National Emergency Laparotomy Audit. Help Box Text
 National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
National Emergency Laparotomy Audit Help Box Text Version Control Version 1.1 06/12/13 1.2 13/12/13 1.3 20/12/13 1.4 20/01/14 1.5 30/01/14 1.6 13/03/14 1.7 07/04/14 1.8 01/12/14 1.9 05/05/15 1.10 02/07/15
South East Coast Operational Delivery Network. Critical Care Rehabilitation
 South East Coast Operational Delivery Networks Hosted by Medway Foundation Trust South East Coast Operational Delivery Network Background Critical Care Rehabilitation The optimisation of recovery from
South East Coast Operational Delivery Networks Hosted by Medway Foundation Trust South East Coast Operational Delivery Network Background Critical Care Rehabilitation The optimisation of recovery from
Putting feet first: national minimum skills framework
 In partnership with Putting feet first: national minimum skills framework The national minimum skills framework for commissioning of footcare services for people with diabetes Revised March 2011 This report
In partnership with Putting feet first: national minimum skills framework The national minimum skills framework for commissioning of footcare services for people with diabetes Revised March 2011 This report
Striving to improve hip fracture care
 Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
Striving to improve hip fracture care The UHL experience 2008-2015 Mr F. Condon, Consultant Orthopaedic Surgeon Ms Jude Ryan, Consultant Ortho-Geriatrician (Mat Leave) & A. Butler Orthopaedic CNS (Mat
This is one of four summary leaflets covering each of the particularly high volume areas of ophthalmic care:
 The Way Forward Options to help meet demand for the current and future care of patients with eye disease Cataract This summary leaflet provides a quick reference guide to the options and practical steps
The Way Forward Options to help meet demand for the current and future care of patients with eye disease Cataract This summary leaflet provides a quick reference guide to the options and practical steps
Bariatric Surgery Questionnaire
 Bariatric Surgery Questionnaire This guidance applies to N.H.S. England only. This sheet is to assist you in researching your weight loss surgery options. The National Health Service uses a Tier system
Bariatric Surgery Questionnaire This guidance applies to N.H.S. England only. This sheet is to assist you in researching your weight loss surgery options. The National Health Service uses a Tier system
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents
 Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
Appendix E : Evidence table 9 Rehabilitation: Other Key Documents 1. Cameron et al. Geriatric rehabilitation following following fractures in older people: a systematic review. Health Technology Assessment
Susan Ward and Jason Clark Vascular Nurse Specialists
 Susan Ward and Jason Clark Vascular Nurse Specialists Sussex Vascular Network Population of 1,6million AAA screening in West Sussex since the 1980 s, East Sussex and Brighton and Hove since 2012 NAAASP
Susan Ward and Jason Clark Vascular Nurse Specialists Sussex Vascular Network Population of 1,6million AAA screening in West Sussex since the 1980 s, East Sussex and Brighton and Hove since 2012 NAAASP
Root Cause Analysis for nontraumatic
 Root Cause Analysis for nontraumatic amputations 2016 (Full Data) Date Richard Leigh and Stella Vig, Co-Chairs London SCN Footcare Network October 2015 Outline of London RCA 2016 London Hospitals invited
Root Cause Analysis for nontraumatic amputations 2016 (Full Data) Date Richard Leigh and Stella Vig, Co-Chairs London SCN Footcare Network October 2015 Outline of London RCA 2016 London Hospitals invited
UK Audit of Vascular Surgical Services & Carotid Endarterectomy July 2010 Public Report
 UK Audit of Vascular Surgical Services & Carotid Endarterectomy July 2010 Public Report Prepared on behalf of the Steering Group by The Clinical Standards Department Royal College of Physicians of London
UK Audit of Vascular Surgical Services & Carotid Endarterectomy July 2010 Public Report Prepared on behalf of the Steering Group by The Clinical Standards Department Royal College of Physicians of London
A. Service Specifications
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No: 170050S Service Primary Ciliary Dyskinesia Management Service (adults) Commissioner Lead Provider Lead 1. Scope 1.1 Prescribed
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Medical technology guidance SCOPE Debrisoft for the debridement of acute and chronic wounds 1 Technology 1.1 Description of the technology The Debrisoft
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Medical technology guidance SCOPE Debrisoft for the debridement of acute and chronic wounds 1 Technology 1.1 Description of the technology The Debrisoft
ANAESTHESIA & PAIN MANAGEMENT FOR KNEE REPLACEMENT
 BEFORE SURGERY ANAESTHESIA & PAIN MANAGEMENT FOR KNEE REPLACEMENT FASTING INSTRUCTIONS No food for 6 hours before your operation. It is okay to drink clear fluids up to 2 hours before surgery (water, clear
BEFORE SURGERY ANAESTHESIA & PAIN MANAGEMENT FOR KNEE REPLACEMENT FASTING INSTRUCTIONS No food for 6 hours before your operation. It is okay to drink clear fluids up to 2 hours before surgery (water, clear
Number of records submitted: 14,750 Number of participants: Part 1 = 146 hospitals (120 trusts); Part 2 = 140 hospitals (119 trusts)
; Part 2 = 140 hospitals (119 trusts)") British Thoracic Society Smoking Cessation Audit Report Smoking cessation policy and practice in NHS hospitals National Audit Period: 1 April 31 May 2016 Dr Sanjay Agrawal and Dr Zaheer Mangera Number
British Thoracic Society Smoking Cessation Audit Report Smoking cessation policy and practice in NHS hospitals National Audit Period: 1 April 31 May 2016 Dr Sanjay Agrawal and Dr Zaheer Mangera Number
Peri-operative management of pacemakers and implantable cardiac defibrillators
 Guideline Title: Peri-operative management of patients fitted with Permanent Pacemakers (PPMs) and Implantable Cardioverter Defibrillators (ICDs). Author(s): Jessica Osman (Chief Pacing Physiologist),
Guideline Title: Peri-operative management of patients fitted with Permanent Pacemakers (PPMs) and Implantable Cardioverter Defibrillators (ICDs). Author(s): Jessica Osman (Chief Pacing Physiologist),
Chapter 15 Guidelines for the Provision of Anaesthesia Services (GPAS) Guidance on the provision of vascular anaesthesia services 2017
 Guidance on the provision of vascular anaesthesia services 2017") Guidelines for the Provision of Anaesthesia Services (GPAS) Guidance on the provision of vascular anaesthesia services 2017 Authors Dr J P Thompson, Leicester Royal Infirmary Professor G R Danjoux, James
Guidelines for the Provision of Anaesthesia Services (GPAS) Guidance on the provision of vascular anaesthesia services 2017 Authors Dr J P Thompson, Leicester Royal Infirmary Professor G R Danjoux, James
Map 6: Percentage of people in the National Diabetes Audit (NDA) with Type 1 diabetes receiving all nine key care processes by PCT
 with Type 1 diabetes receiving all nine key care processes by PCT") 78 NHS ATLAS OF VARIATION ENDOCRINE, NUTRITIONAL AND METABOLIC PROBLEMS Map 6: Percentage of people in the National Diabetes Audit (NDA) with Type 1 diabetes receiving all nine key care processes by PCT
78 NHS ATLAS OF VARIATION ENDOCRINE, NUTRITIONAL AND METABOLIC PROBLEMS Map 6: Percentage of people in the National Diabetes Audit (NDA) with Type 1 diabetes receiving all nine key care processes by PCT
LUMBAR DECOMPRESSION / DISCECTOMY SURGERY INFORMATION
 LUMBAR DECOMPRESSION / DISCECTOMY SURGERY INFORMATION WHAT IS LUMBAR DECOMPRESSION / DISCECTOMY SURGERY? During lumbar decompression/ discectomy back surgery, a small portion of the bone over the nerve
LUMBAR DECOMPRESSION / DISCECTOMY SURGERY INFORMATION WHAT IS LUMBAR DECOMPRESSION / DISCECTOMY SURGERY? During lumbar decompression/ discectomy back surgery, a small portion of the bone over the nerve
All about your anaesthetic
 Patient information leaflet All about your anaesthetic 1 Introduction to anaesthesia and preparation for your surgery For patients having a surgical procedure at a Care UK independent diagnostic and treatment
Patient information leaflet All about your anaesthetic 1 Introduction to anaesthesia and preparation for your surgery For patients having a surgical procedure at a Care UK independent diagnostic and treatment
NICE Guidance: Venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital 1
 in patients admitted to hospital 1") The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
The College of Emergency Medicine Patron: HRH The Princess Royal Churchill House Tel +44 (0)207 404 1999 35 Red Lion Square Fax +44 (0)207 067 1267 London WC1R 4SG www.collemergencymed.ac.uk CLINICAL EFFECTIVENESS
Guidance on competencies for Spinal Cord Stimulation Reviewed
 Guidance on competencies for Spinal Cord Stimulation Reviewed 2016 Endorsed by: Contents Introduction A: Core competencies for practitioners in Pain Medicine Page 2 4 Appendix A: Curriculum 5 B: Competencies
Guidance on competencies for Spinal Cord Stimulation Reviewed 2016 Endorsed by: Contents Introduction A: Core competencies for practitioners in Pain Medicine Page 2 4 Appendix A: Curriculum 5 B: Competencies
The most recent estimates suggest that. A study of inpatient diabetes care on medical wards. Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal
 A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
A study of inpatient diabetes care on medical wards Saqib Javed, Yaser Javed, Kate Barnabas, Kalpana Kaushal Article points 1. It is well established that poor glycaemic control is associated with increased
Prevention and Management of Hip Fracture in Older People
 Scottish Intercollegiate Guidelines Network 56 Prevention and Management of Hip Fracture in Older People A national clinical guideline 1 Introduction 1 2 Prevention of hip fracture 4 3 Pre-hospital management
Scottish Intercollegiate Guidelines Network 56 Prevention and Management of Hip Fracture in Older People A national clinical guideline 1 Introduction 1 2 Prevention of hip fracture 4 3 Pre-hospital management
Selective Dorsal Rhizotomy (SDR) Scotland Service Pathway
 Scotland Service Pathway") Selective Dorsal Rhizotomy (SDR) Scotland Service Pathway This pathway should to be read in conjunction with the attached notes. The number in each text box refers to the note that relates to the specific
Selective Dorsal Rhizotomy (SDR) Scotland Service Pathway This pathway should to be read in conjunction with the attached notes. The number in each text box refers to the note that relates to the specific
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals
 Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Dr Ben Edwards Consultant Anaesthetist Sheffield Teaching Hospitals 70-75,000 #NOF per annum (costs 2 billion) 10% die within 1 month 33% die within 1 year Operative delays >48hs more than doubles risk
Intro Who should read this document 2 Key practice points 2 What is new in this version 3 Background 3 Guideline Subsection headings
 Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
Enhanced Recovery for Major Urology and Gynaecological Classification: Clinical Guideline Lead Author: Dr Dominic O Connor Additional author(s): Jane Kingham Authors Division: Anaesthesia Unique ID: DDCAna3(12)
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab
 MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
MSK Rehab Definitions Framework - hip fractures Self assessment Survey Outpatient Rehab In response to a changing rehab landscape in which rehabilitation is offered in many different settings with variations
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff
 National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
National Hip Fracture Database North West Regional Meeting 13th March 2013 Planning patient care and achieving Best Practice Tariff Dr John Tsang MB ChB, FRCP Consultant Orthogeriatrician Lead clinician
Toe and forefoot amputation. Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England.
 Toe and forefoot amputation Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information
Toe and forefoot amputation Brought to you in association with EIDO Healthcare and endorsed by the Royal College of Surgeons England. Discovery has made every effort to ensure that we obtained the information
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January December 2009
 Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2009 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Contents
Surveillance of Surgical Site Infection Annual Report For procedures carried out from: January 2003 - December 2009 Scottish Surveillance of Healthcare Associated Infection Programme (SSHAIP) Contents
The Experience in Exeter with. hip fracture care. Data For Change
 The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
The Experience in Exeter with hip fracture care Data For Change John Charity Associate Specialist in T&O, Lead NHFD Clinician, Royal Devon and Exeter NHS Foundation Trust Respond Deliver & Enable People
A06/S(HSS)b Ex-vivo partial nephrectomy service (Adult)
b Ex-vivo partial nephrectomy service (Adult)") A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
A06/S(HSS)b 2013/14 NHS STANDARD CONTRACT FOR EX-VIVO PARTIAL NEPHRECTOMY SERVICE (ADULT) PARTICULARS, SCHEDULE 2 THE SERVICES, A - SERVICE SPECIFICATION Service Specification No. Service Commissioner
Prioritasing services in hospital
 Prioritasing services in hospital Admission to, utilisation of and discharge from services Capacity in services can be created through the active management of admissions and discharges in conjunction
Prioritasing services in hospital Admission to, utilisation of and discharge from services Capacity in services can be created through the active management of admissions and discharges in conjunction
Diabetes is a lifelong, chronic. Survey on the quality of diabetes care in prison settings across the UK. Keith Booles
 Survey on the quality of diabetes care in prison settings across the UK Article points 1. The Royal College of Nursing Diabetes Forum conducted an audit of prisons within the UK to determine the level
Survey on the quality of diabetes care in prison settings across the UK Article points 1. The Royal College of Nursing Diabetes Forum conducted an audit of prisons within the UK to determine the level
Laparoscopic partial removal of the kidney
 Laparoscopic partial removal of the kidney Department of Urology 2 Patient Information What evidence is this information based on? This booklet includes advice from consensus panels, the British Association
Laparoscopic partial removal of the kidney Department of Urology 2 Patient Information What evidence is this information based on? This booklet includes advice from consensus panels, the British Association
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE
 THE CHRISTIE, GREATER MANCHESTER & CHESHIRE") PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
PATHWAY MANAGEMENT OF METASTATIC SPINAL CORD COMPRESSION (MSCC) THE CHRISTIE, GREATER MANCHESTER & CHESHIRE Procedure Reference: Document Owner: Dr V. Misra Version: Accountable Committee: V3 MSCC Network
Diagnostic laparoscopy: procedure-specific information
 PATIENT INFORMATION Diagnostic laparoscopy: procedure-specific information What is the evidence base for this information? This leaflet includes advice from consensus panels, the British Association of
PATIENT INFORMATION Diagnostic laparoscopy: procedure-specific information What is the evidence base for this information? This leaflet includes advice from consensus panels, the British Association of
Integrated cardiac services from an internationally renowned hospital
 cardiac Services Integrated cardiac services from an internationally renowned hospital Cardiac Services At London Bridge Hospital we provide a wide range of diagnostic services and treatments for cardiac
cardiac Services Integrated cardiac services from an internationally renowned hospital Cardiac Services At London Bridge Hospital we provide a wide range of diagnostic services and treatments for cardiac
Ratified by: Care and Clinical Policies Date: 17 th February 2016
 Clinical Guideline Reference Number: 0803 Version 5 Title: Physiotherapy guidelines for the Management of People with Multiple Sclerosis Document Author: Henrieke Dimmendaal / Laura Shenton Date February
Clinical Guideline Reference Number: 0803 Version 5 Title: Physiotherapy guidelines for the Management of People with Multiple Sclerosis Document Author: Henrieke Dimmendaal / Laura Shenton Date February
Enhanced Recovery After Surgery (ERAS) Diary
 Diary") Cardiac Surgery Enhanced Recovery After Surgery (ERAS) Diary Patient s Name: Options available If you d like a large print, audio, Braille or a translated version of this leaflet then please call: 01253
Cardiac Surgery Enhanced Recovery After Surgery (ERAS) Diary Patient s Name: Options available If you d like a large print, audio, Braille or a translated version of this leaflet then please call: 01253
How to make changes in the NHS
 How to make changes in the NHS Keith Willett Prof of Orthopaedic Trauma Surgery University of Oxford prev. National Clinical Director for Trauma Care ATOCP Conference Oxford 2016 Medical Director for Acute
How to make changes in the NHS Keith Willett Prof of Orthopaedic Trauma Surgery University of Oxford prev. National Clinical Director for Trauma Care ATOCP Conference Oxford 2016 Medical Director for Acute
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Total knee replacement: The enhanced recovery programme
 INFORMATION FOR PATIENTS Total knee replacement: The enhanced recovery programme This leaflet aims to explain the enhanced recovery programme after total knee replacement surgery, to outline certain common
INFORMATION FOR PATIENTS Total knee replacement: The enhanced recovery programme This leaflet aims to explain the enhanced recovery programme after total knee replacement surgery, to outline certain common
A Whole Pathway Integrated Approach to Improving Foot Care
 A Whole Pathway Integrated Approach to Improving Foot Care Excellence in Action London Foot Care Network 4 th Feb 2016 Georgina Cunningham, Commissioning Manager LTC, Southampton City Integrated Commissioning
A Whole Pathway Integrated Approach to Improving Foot Care Excellence in Action London Foot Care Network 4 th Feb 2016 Georgina Cunningham, Commissioning Manager LTC, Southampton City Integrated Commissioning
Aortobifemoral bypass graft Vascular Surgery Patient Information Leaflet
 Aortobifemoral bypass graft Vascular Surgery Patient Information Leaflet This information sheet includes extracts reproduced with permission from the Circulation Foundation. www.circulationfoundation.org.uk
Aortobifemoral bypass graft Vascular Surgery Patient Information Leaflet This information sheet includes extracts reproduced with permission from the Circulation Foundation. www.circulationfoundation.org.uk
Femoral endarterectomy
 Femoral endarterectomy The femoral arteries run from the groin to the thigh delivering blood to your legs. When there is a narrowing or blockage in these arteries, the blood supply to the legs is reduced,
Femoral endarterectomy The femoral arteries run from the groin to the thigh delivering blood to your legs. When there is a narrowing or blockage in these arteries, the blood supply to the legs is reduced,
Patient information. Total Ankle Replacement Trauma and Orthopaedic Directorate PIF 1335 V2
 Patient information Total Ankle Replacement Trauma and Orthopaedic Directorate PIF 1335 V2 Your Consultant has advised you that you are suitable to have a total ankle replacement. The aim of surgery is
Patient information Total Ankle Replacement Trauma and Orthopaedic Directorate PIF 1335 V2 Your Consultant has advised you that you are suitable to have a total ankle replacement. The aim of surgery is
PERCUTANEOUS NEPHROLITHOTOMY
 PERCUTANEOUS NEPHROLITHOTOMY AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport Tel: 0161 419 5698 Website: www.stockport.nhs.uk Tameside Tel: 0161 922 6696/6698 Website: www.tameside.nhs.uk
PERCUTANEOUS NEPHROLITHOTOMY AN INFORMATION LEAFLET Written by: Department of Urology May 2011 Stockport Tel: 0161 419 5698 Website: www.stockport.nhs.uk Tameside Tel: 0161 922 6696/6698 Website: www.tameside.nhs.uk
National Diabetes Treatment and Care Programme
 National Diabetes Treatment and Care Programme Introduction to and supporting documentation for VALUE BASED TRANSFORMATION FUNDING SITE SELECTION December 2016 1 Introduction and Contents The Planning
National Diabetes Treatment and Care Programme Introduction to and supporting documentation for VALUE BASED TRANSFORMATION FUNDING SITE SELECTION December 2016 1 Introduction and Contents The Planning
NATIONAL REHABILITATION HOSPITAL PROSTHETIC, ORTHOTIC & LIMB ABSENCE REHABILITATION PROGRAMME
 NATIONAL REHABILITATION HOSPITAL PROSTHETIC, ORTHOTIC & LIMB ABSENCE REHABILITATION PROGRAMME SCOPE OF SERVICE 1 Introduction: The Prosthetic, Orthotic & Limb Absence Rehabilitation Programme (POLAR) at
NATIONAL REHABILITATION HOSPITAL PROSTHETIC, ORTHOTIC & LIMB ABSENCE REHABILITATION PROGRAMME SCOPE OF SERVICE 1 Introduction: The Prosthetic, Orthotic & Limb Absence Rehabilitation Programme (POLAR) at