Gastrointestinal Emergencies. Candice M. Quillin BSN CGRN September 27, 2014
|
|
|
- Bethany Golden
- 6 years ago
- Views:
Transcription
1 Gastrointestinal Emergencies Candice M. Quillin BSN CGRN September 27, 2014
2 Objectives List four gastrointestinal emergencies and complications. Identify signs and symptoms of a variety of gastrointestinal emergencies.
3 What s coming up Perforations Obstructions Pancreatitis GI Bleed Variceal Bleed Adverse Drug Reaction Respiratory arrest Cardiac Arrest Shock
4 Perforations..
5 Perforation Upper GI tract Cervical Esophagus Crycopharyngeal Thoracic Esophagus Distal Esophagus Boerhaave s Syndrome Gastric Duodenal

6 Crycopharyngeal tear

7 Boerhaave s

8 Boerhaave s
9 Treatment algorithm for Boerhaave s Syndrome Early Diagnosis <48 hrs Late Diagnosis >48 hrs Sepsis Pleural cavity involved No Sepsis or pleural cavity involvement Thoracotomy with resection of tear. Hemifundoplication and pleura/mediastinal drainage. Laparotomy if intraabdominal leakage Endoscopic treatment without pleural drainage. Sepsis Conservative Treatment No Sepsis
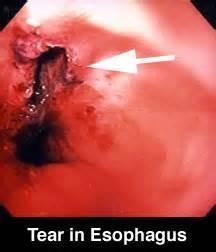
10 Esophageal Tear

11 Tear/Fistula

12


13 Gastric Ulcer to Perforation
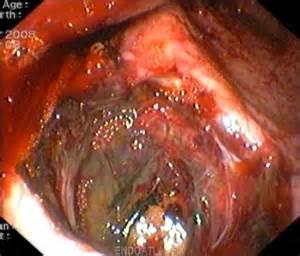
14 Gastric perforation

15 Small Bowel perforation

16 Colon Perforation with Ischemic Bowel
17 Obstructions
18 Esophageal Obstruction Causes of Obstructions of Esophagus: Strictures Cancer Bacterial/viral infections Foreign body Anatomy anomalies
19 Esophageal Obstruction due to Achalasia Achalasia ( peristalsis is absent with increased LES pressures and incomplete esophageal relaxation) Eventually esophagus dilates above LES storing large volumes of food and liquids. Occurs 1 in 100,000 Americans most often between the ages of 20 and 60.
20 Achalasia Symptoms include dysphagia, painful swallowing, substernal chest pain, bad breath, difficulty burping, weight loss and malnutrition Patient will swallow by stretching neck back and lifting shoulders to help get food down.
21 Achalasia Diagnosis: Chest Xray can reveal dilated esophagus and empty stomach, but does not confirm Barium swallow good screening tool Esophageal manometry confirms diagnosis Endoscopy allows physician to see.
22 Achalasia Treatment : Aim is to weaken LES. Drugs: Nitrates and calcium channel blockers Balloon Dilation of LES Surgery: Myotomy good success Botox: paralyzes the nerves

23 Achalasia
24 Gastric Outlet Obstruction Obstruction of the pyloric sphincter at the outlet of the stomach blocks the flow of gastric contents into the duodenum Symptoms: Vomiting partially digested food Gastric pain especially with eating Satiety relieved by vomiting Metabolic alkalosis as a result of frequent vomiting
25 Gastric Outlet Obstruction Treatment: Restoration of fluid and electrolytes Decompression of the stomach Pyloric dilatation Surgery if necessary
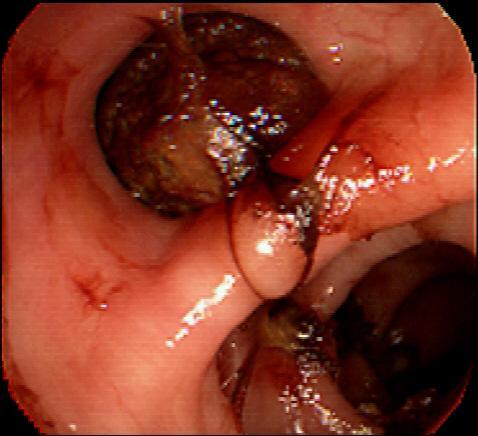
26 Bezoars Compositions of foreign materials found in the stomach that may cause gastric outlet obstruction and abdominal pain. Composed of vegetable or plant material or hair. Treatment is EGD or surgery with removal of the matter.

27 Bezoar
28 Pancreatitis
29 Acute Pancreatitis Autodigestion of pancreas due to inappropriate activation of pancreatic enzymes causing a severe inflammation of the pancreas Causes: ETOH Obstruction of ducts Biliary disease Mumps, scarlet fever Endocrine disorders
30 Pancreatitis Initial management of a patient with acute pancreatitis consists of supportive care with fluid resuscitation, pain control, and nutritional support.
31 Pancreatitis Patients with moderately severe or severe acute pancreatitis, signs of sepsis, or clinical deterioration 72 hours after initial presentation be assessed for presence of pancreatic or extrapancreatic necrosis and local complications
32 Pancreatitis Serum amylase rises within 6 to 12 hours of the onset of acute pancreatitis. Amylase has a short half-life of approximately 10 hours and in uncomplicated attacks returns to normal within three to five days. Serum amylase elevation of greater than three times the upper limit of normal has a sensitivity for the diagnosis of acute pancreatitis
33 Pancreatitis Serum lipase has a sensitivity and specificity for acute pancreatitis ranging from 82 to 100 percent Serum lipase rises within four to eight hours of the onset of symptoms, peaks at 24 hours, and returns to normal within 8 to 14 days
34 Pancreatitis Trypsinogen activation peptide (TAP), a five amino-acid peptide that is cleaved from trypsinogen to produce active trypsin, is elevated in acute pancreatitis Activation of trypsin is likely an early event in the pathogenesis of acute pancreatitis TAP may be useful in detection of early acute pancreatitis and as a predictor of the severity of acute pancreatitis
35 Pancreatitis Patients with pancreatitis May have leukocytosis May have elevated hematocrit from hemoconcentration due to extravasation of intravascular fluid into third spaces May have metabolic abnormalities including elevated blood urea nitrogen (BUN), hypocalcemia, hyperglycemia, and hypoglycemia
36 Pancreatitis S&S: Acute onset of a persistent, severe, epigastric pain with tenderness on palpation on physical examination. Acutely ill with severe pain, guarding, rigidity of abdomen, hypotension, respiratory distress, and symptoms of shock.

37 Pancreatitis Turner s sign
38 Acute Pancreatitis Interventions: hemodynamic monitoring, antibiotics, pain management, body positioning sidelying, knees flexed, HOB up. Treatment: Remove potential causes necrotic pancreatic tissue, gallstones (cholecystectomy, ERCP), repair problems within biliary system with stents, drain abscesses, etc.
39 G I Bleed
40 How do you recognize bleeding in GI tract? Bright red blood coating stool Dark blood mixed with stool Black or tarry stool Bright red blood in vomit Coffee ground emesis
41 What are the sx s of acute bleed? Visually seeing bright red blood in stool and emesis Sudden weakness Shortness of breath Dizziness Crampy abdomen Faintness Diarrhea
42 What are sx s of Chronic bleeding Black tarry stools Coffee ground emesis Weakness Fatique Shortness of breath Lethargy Faintness Pale lips and nailbeds
43 Acute vs Chronic Some differences between acute and chronic low Hgb and Hct: Acute Symptoms of shock may be present Sudden pallor Obvious bleed Chronic History of weakness over weeks History of gradual increase in SOB History of dark stools
44 Emergency GI Bleed Nurses Role Review assessment made Review labs. 2 large bore IV sites are preferable. Type and Cross match completed or being done. Blood ordered or hanging if severe anemia Platelets, other blood products, etc
45 Emergency GI Bleed Nurses Role Be prepared to Lavage Stomach Be prepared to Suction patient orally. Keep patient on right lateral position if at all possible. Get additional support from other nurses to help with blood transfusions and additional fluids, etc.
46 Lab Values with Suspected GI Bleed Anemia A condition in which RBC s are below normal Hemoglobin Serves as a vehicle for transport of Oxygen and Carbon Dioxide within the RBC s Hematocrit measures the RBC mass by measuring space occupied by Packed RBC s; the % of RBC s in volume of whole blood
47 Lab Values with suspected GI Bleed Things to keep in mind when looking at H&H: Hematocrit may or may not be reliable immediately after an acute GI Bleed. Patients with COPD & CHF may have an abnormally high Hemoglobin before bleed. If erythrocytes are normal, Hematocrit is roughly 3 times higher than Hemoglobin. If Hgb is low keep in mind when sedating that patient has a decreased O2/CO2 carrying capacity
48 Lab Values if suspected GI Bleed BUN/ Creatinine BUN measures the amount of urea nitrogen in blood GI Bleed increases BUN therefore affects ratio If BUN is 100 or over patient has had a severe GI bleed
49 Summary Evaluation of the GI Bleed Laboratory studies should include CBC and platelets, PT/PTT, electrolytes, BUN/creatinine (GI bleeders will frequently have elevated BUN secondary to the increased ingestion of nitrogen from digested blood). Physical examination often reveals hyperactive bowel sounds secondary to intraluminal blood. Endoscopy may be done acutely for upper GI bleeding to help define the source and treat endoscopically if able. Angiography or nuclear medicine studies can be useful to localize lower GI bleeding.
50 Mallory Weis Tear History : Prolong forceful vomiting Increased esophageal intraluminal pressure Due to: Seizures, Childbirth, Coughing, straining at defecation, weighlifting Pathology: Submucosal and mucosal without perforation Imaging: Chest Radiograph: normal Diagnosis is almost always made by endoscopy Rarely does esophagram show if incomplete tear Rarely does angiography show bleeding site
51 Mallory-Weiss Tears Esophageal tear occurring most often at the esophagogastric junction. Occurs in 8% of all upper GI bleeds. Treatment: Cautery or injection of bleeding area. Liquid or soft diet Avoidance of sharp foods Carafate to heal and protect the esophagus Surgery if perforated through esophagus.
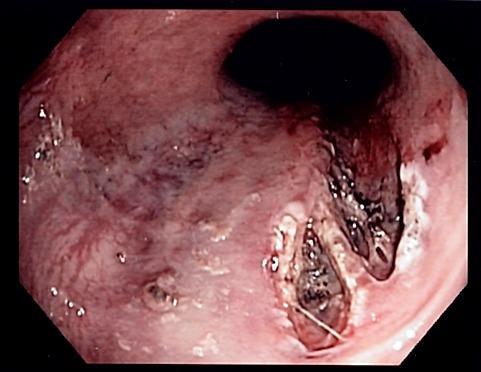
52 Mallory-Weiss Tear
53 Esophageal Varices Engorged vessels in the submucosa of the esophagus and may be caused by portal hypertension as a result of chronic hepatitis; alcoholic cirrhosis; portal vein thrombosis; or congenital anomalies such as biliary atresia Diagnosis made most often as an upper GI bleed (12% of all upper GI Bleeds) and subsequent EGD
54 Esophageal Varicies - Grading When esophageal varices are discovered, they are graded according to their size, as follows: Grade 1 Small, straight esophageal varices Grade 2 Enlarged, tortuous esophageal varices occupying less than one third of the lumen Grade 3 Large, coil-shaped esophageal varices occupying more than one third of the lumen
55 Variceal Bleed Phases Acute phase -Starts with onset of active hemorrhage Later phase -Period of 6wks following cessation of active bleeding -Greatest risk within 48-72hr -50% of rebleeds occur within first 10 days
56 Variceal Bleed Variceal Hemorrhage -1/23 of all deaths related to cirrhosis -Four major issues 1) Prediction of pts at risk 2) Therapy against a first bleed 3) Treatment of an active bleed 4) Prevention of rebleeding
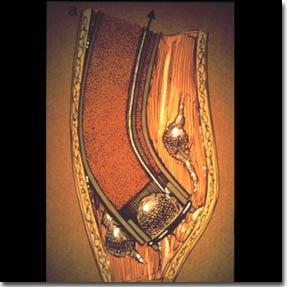
57 Variceal Bleed Therapies Endoscopic Treatment -Sclerotherapy -Variceal band ligation Other Therapies -Balloon tamponade -Transjugular intrahepatic portosystemic shunt (TIPS) -Surgical therapy
58 Therapy for Variceal Bleed Somatostatin and Octreotide Theoretical benefit due to: -Reduced splanchnic blood flow -Inhibition of gastric acid secretion -Gastric cytoprotective effects Purpose - Decrease release of GI hormones and hepatic blood flow and portal HTN Stabilization until definitive therapy can be performed
59 Nurses Role - Varices Esophageal Varices Vasopressin has been shown to be no more effective than placebo in controlling bleeding from esophageal varices or other upper GI sources. The combination of sclerotherapy and octreotide (a synthetic somatostatin analog, 25 μg/hour) is superior to sclerotherapy alone in controlling acute variceal bleeding in patients with cirrhosis. Transjugular intrahepatic portosystemic shunt (TIPS). This is regarded as a safe and established means of treating variceal hemorrhage in patients with portal hypertension who fail sclerotherapy. The combined use of a beta-blocker and nitrate has been shown to reduce portal pressure
60 Esophageal varices

61 Esophageal Varicies
62

63

64 Esophageal varcies
65 GI Bleed
66 Assessment leads you to believe patient is an Upper GI Bleed possible Peptic Ulcer Epigastric pain Pale Skin cool to touch Patient tachycardic c/o Lightheadedness Melena
67 Complications of Peptic Ulcer Disease (PUD) Hemorrhage 15% of all ulcer patients, hematemesis and/or black stools Perforation 5-7% occurrence; ulcer has eroded through stomach wall and has spilled into the peritoneum Penetration ulcer has eroded into another organ Obstruction Pylorus becomes edematous and does not allow chyme to pass
68 PUD Treatment: Control bleeding Fluid and electrolyte replacement Presence of perforation or penetration antibiotics and surgery Presence of obstruction NG tube for decompression, Dilation, surgery.
69 PUD continued Nursing interventions : patient education regarding medications and importance of adhering to dosing schedules; elimination of coffee, caffeine, spicy foods, carbonation, alcohol, chocolate and any other food that has caused pain and discomfort; small meals; smoking cessation; avoidance of aspirin and NSAIDS (if aspirin use is necessary then enteric coated is best)
70 Emergency Endoscopy Nurses Role Equipment setup Try to be aware of what performing physician likes to use and be prepared to use them. BICAP Endo Clips Epinephrine therapy Saline injection APC

71 Peptic Ulcer

72 Large Ulcer

73 Bleeding Ulcer

74 Ulcer post BICAP
75 Surgery Surgery is required if an ulcer fails to heal from medical therapies or is complicated by uncontrolled bleeding, perforation or obstruction. Types Vagotomy Cutting one or more nerves to stomach Pylorplasty Widening the opening of the pylorus Partial Gastric Resection. Removing part of stomach or duodenum affected by ulcer

76 Surgical ulcer removal
77 Other Causes of Gastric Bleed Gastric Varicies Gastric Carcinoma Dieulafoys lesion Arterial-Venous Malformations Gastritis

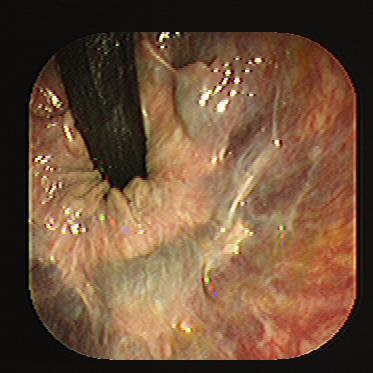
78 Dieulafoy s Lesion
79 Nurses role UGI Bleed Upper GI bleeding. Start IV fluid resuscitation and manage shock An NG tube should be placed to document the source and relative rate of bleeding (blood is usually present in the NG aspirate during an upper GI bleed). H2-antagonist therapy with either cimetidine (300 mg) or ranitidine (50 mg) can be given IV but will not act to slow current bleeding. Transfusions--whole blood, platelets, other blood products. Endoscopy and endoscopic therapy is the treatment of choice if possible.
80 Nurses role LGI BLeed Lower GI Bleeding Start IV fluid resuscitation and manageshock Work-up may include colonoscopy, barium enema, selective angiography, and radionuclide bleeding studies. Surgical consultation should be obtained in case operative intervention is needed.
81 Meckel s Diverticulum Diagnosis: Meckel s scan a radiology contrast study Treatment: Surgical removal of the diverticulum or resection of the ileum

82 Mekel s DIverticulum
83 Meckel s Diverticulum A congenital anomaly outpouching of the ileum which contains normal tissues as well as gastric and pancreatic tissue. These abnormal tissues for the ileum secrete acid and pepsin and can cause ulcerations of the ileum. Symptoms: Abdominal pain Bilious vomiting Red currant jelly like stools
84 Overview of GI Bleed Because GI bleeding is internal, it is possible for a person to have GI bleeding without symptoms. Important to recognize those symptoms which may accompany GI bleeding. Basically, the symptoms of possible GI bleeding vary, depending upon whether the source of the bleeding is in the upper part of the digestive tract (the esophagus, stomach or the beginning of the small intestine) or in the lower part (small intestine, colon or rectum
85 Various types of GI Bleed Possible reason(s) Esophagus Vomiting bright red (blood) or coffee ground material, Black stools Ulcer, varices Liver disease Stomach Vomiting bright red (blood) or coffee ground material, Black stools Ulcer, gastritis, varices Small Intestine Bright red/maroon bleeding Ulcer,Tumor Large Intestine (Colon) Blood in the stool Colon, polyps, colitis, diverticulas Rectum Bright red bleeding Hemorrhoids, Diverticulosis, Tumor
86 Critical Thinking Bleeding-GI Tract Ulcers: Muscles of the stomach or duodenal wall, blood vessels may be damaged, which causes bleeding. If the affected blood vessels are small, the blood may slowly seep into the digestive tract. Over a long period of time, a person may become anemic and feel weak,dizzy, or tired. If a damaged blood vessel is large, bleeding is dangerous and requires prompt medical attention. Symptoms include feeling weak and dizzy when standing, vomiting blood, or fainting. The stool may become a tarry black color from the blood.
87 Critical Thinking UGI Bleed Hematemesis-Vomiting of blood. May be bright red blood or coffee grounds-like material. Usually from bleeding proximal to the ligament of Treitz. Sources. Peptic ulcer disease may be asymptomatic until first bleed especially in patients taking NSAID. Gastritis, especially from alcohol. Mallory-Weiss tear occurs after prolonged vomiting or retching and is generally a self-limited bleed. Look for mediastinal air on CXR. Esophageal varices from portal hypertension especially secondary to chronic alcohol consumption. Swallowed blood from epistaxis or other source of bleeding.
88 Critical thinking Melena Passage of black, tarry stools secondary to GI bleeding with intestinal transit time allowing for the digestion of hemoglobin. May be of upper or lower GI origin Black, tarry stools can be the result of ingested iron, licorice, or bismuth, but the stool will be guaiac negative
89 Critical thinking Hematochezia - Bright red blood per rectum. Can be secondary to anal disease (hemorrhoids, rectal fissure). May be secondary to bleeding diverticulum, other colonic disease such as Crohn's disease, ulcerative colitis, carcinoma (very rarely causes gross bleeding), dysentery (especially amebiasis, Campylobacter, Shigella, or other invasive organisms).
90 Critical Thinking Clinical Predictors for Failure ->65yo -Shock -Poor overall health -Comorbid illnesses -Low initial Hgb -Melena -Transfusion requirement -Fresh red blood -Elevated BUN, SCr, or AST/ALT
91 Critical Thinking Endoscopic Predictors for Failure -Active bleeding -Non-bleeding visible variceal or adherent -Ulcer size -Ulcer location -Lesion type
92 Therapies for GI Bleed Treatment (Acute) Endoscopic Therapy -Thermal coagulation -Injection therapy -Hemostatic clips -Fibrin sealant -Combo therapy Acid suppression therapy
93 Therapies for GI Bleed Thermal Coagulation -Achieves acute hemostasis and prevents rebreeding -Coagulation of the underlying artery in the ulcer base -Multipolar probes and heater probe
94 Therapies for GI Bleed Injection Therapy -Absolute alcohol -Epinephrine (1:100,000 dilution) most common -Saline injection
95 Therapies for GI BLeed Hemostatic Clips -Alternative to other methods -Safe to use - Can be expensive -May serve as radiologic marker for subsequent interventional radiology
96 Therapies for GI Bleed Fibrin Sealant -Role remains to be defined -Single application vs daily repeated dose - Hard on scopes, expensive
97 Therapies for GI Bleed Combo Therapy BETTER OUTCOMES -Epi injection -Mechanical methods: thermal coag, hemoclip

98 Nuc med bleeding scan

99 Celiac arterigram showing duodenal bleed

100 Watermelon stomach

101 Crohn s Disease

102 AVM

103 AVM

104 Colon Cancer
105 Diverticular bleed

106 Ischemic Bowel
107 Hemorrhoids

108 Hemmorhoids
109 Other Gastrointestinal Emergencies
110 Shock Shock is a condition of acute peripheral circulatory failure caused by derangement of circulatory control or loss of circulating fluid. Can be endocrine, neurogenic, bacterial, cardiogenic, or hypovolemic.
111 Hypovolemic Shock Bodies response to perceived blood volume loss.
112 Septic Shock/Bacterimia From direct invasion of the bloodstream by microorganisms or their toxins.
113 Adverse Drug reactions Know side effects Know toxic reactions Know allergic responses Know how to treat anaphylaxis Know look alike sound alike drugs Know drug interactions
114 Respiratory Depression Highest risk factor from anesthesia, sedation and narcotics.
115 Cardiac Complications/Arrest Cardiac stress is most common complication of Endoscopy outside of medication reactions.
116 Vasovagal Syncope Transient vascular and neurogenic reaction marked by pallor, nausea, diaphoresis, bradycardia, rapid fall in B/P, to loss of consciousness(fainting).
117 Postural Hypotension Occurs when patient suddenly assumes an upright position. There is a fall in systolic and diastolic B/P.
118 Aspiration Occurs when liquids or solids mistakenly enter the pulmonary system.
119 Pediatric Complications and Emergencies Complications due to Endoscopy in pediatrics Oral trauma Loose baby teeth Orthodontics Wrong scope size O2 saturations Hypoxemia Over distension Arrhythmias

120 The End, but only the beginning.
GASTROINESTINAL BLEEDING. Dr.Ammar I. Abdul-Latif
 GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
GASTROINESTINAL BLEEDING Dr.Ammar I. Abdul-Latif CLASSIFICATION OF G.I.BLEEDING GIB Appearance Acuity Site Apparent Acute Upper Obscure Chronic Lower UPPER&LOWER G.I.BLEEDING CAUSES OF UPPER G.I. BLEEDING
Bleeding in the Digestive Tract
 Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
Bleeding in the Digestive Tract National Digestive Diseases Information Clearinghouse National Institute of Diabetes and Digestive and Kidney Diseases NATIONAL INSTITUTES OF HEALTH U.S. Department of Health
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds
 McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
McHenry Western Lake County EMS System Paramedic, EMT-B and PHRN Optional Continuing Education 2018 #10 Acute GI Bleeds Gastrointestinal bleeding is a very common problem in emergency medicine. Between
Outline. GI-Bleeding. Initial intervention
 Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Internal Medicine Board Review 2016: GI-Bleeding Stephan Goebel, M.D. Assistant Professor Division of Digestive Diseases Management UGI-Bleeding (80%) Ulcers Varices others LGI-Bleeding (20%) Outline Initial
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Chapter 14: Training in Radiology. DDSEP Chapter 1: Question 12
 DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
DDSEP Chapter 1: Question 12 A 52-year-old white male presents for evaluation of sudden onset of abdominal pain and shoulder pain. His past medical history is notable for a history of coronary artery disease,
COPYRIGHTED MATERIAL. 1 Approach to the patient with gross gastrointestinal bleeding. Grace H. Elta, Mimi Takami
 1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
1 Approach to the patient with gross gastrointestinal bleeding Grace H. Elta, Mimi Takami Gastrointestinal (GI) bleeding is a common clinical problem that requires more than 300 000 hospitalizations annually
Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased
 1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
1 2 3 4 5 6 7 Chapter 32 Gastroenterology General Pathophysiology General Risk Factors for GI emergencies: Excessive Consumption Excessive Smoking Increased Ingestion of Caustic Substances Poor Bowel Habits
GASTROINTESTINAL BLEEDING. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
GASTROINTESTINAL BLEEDING Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Gastrointestinal Bleeding Hematemesis- Vomiting of bright red blood
Historical perspective
 Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
Raj Santharam, MD GI Associates, LLC Clinical Assistant Professor of Medicine Medical College of Wisconsin Historical perspective FFS first widespread use in the early 1970 s Expansion of therapeutic techniques
INVESTIGATIONS OF GASTROINTESTINAL DISEAS
 INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
INVESTIGATIONS OF GASTROINTESTINAL DISEAS Lecture 1 and 2 دز اسماعيل داود فرع الطب كلية طب الموصل Radiological tests of structure (imaging) Plain X-ray: May shows soft tissue outlines like liver, spleen,
Perforated peptic ulcer
 Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Perforated peptic ulcer - Despite the widespread use of gastric anti-secretory agents and eradication therapy, the incidence of perforated peptic ulcer has changed little, age limits increase NSAIDs elderly
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective. Dr.J.H.Barnard Dept. of Surgery PAH
 Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
Acute Upper Gastrointestinal Hemorrhage Surgical Perspective Dr.J.H.Barnard Dept. of Surgery PAH Introduction: AGH is a leading cause of admissions into ICU. Overall mortality 5-12%, but increases to 40%
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE
 MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
MANAGING GI BLEEDING IN A COMMUNITY HOSPITAL SETTING DR M. F. M. BRULE DISCLOSURES Presenter: Dr Michele Brule Relationships with commercial interests: None OBJECTIVES Assess the severity of GI bleeding
UPPER AND LOWER GASTROINTESTINAL BLEEDING. Prof. G. Zuliani
 UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
UPPER AND LOWER GASTROINTESTINAL BLEEDING Prof. G. Zuliani Gastrointestinal Bleeding Hematemesis: vomiting of bright red blood usually represents bleeding proximal to the ligament of Treitz Hematochezia:
F A M N O P R S ! D !
 A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
A B C D E F A M N O P Q G H I J R S T U V 595 W http://www.encognitive.com/images/digestive-system-2.jpg K L M A N B C O P D E F G D Q R H S I J K http://apbrwww5.apsu.edu/thompsonj/anatomy%20&%20physiology/2020/2020%20exam%20reviews/exam%203/colon%20diagram.jpgd
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Peptic ulcer disease Disorders of the esophagus
 Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
Peptic ulcer disease Disorders of the esophagus Peptic ulcer disease Burning epigastric pain Exacerbated by fasting Improved with meals Ulcer: disruption of mucosal integrity >5 mm in size, with depth
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Emergency Surgery Course Graz, March UPPER GI BLEEDING. Carlos Mesquita Coimbra
 UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
UPPER GI BLEEDING Carlos Mesquita Coimbra Aim Causes Management Problem Above angle of Treitz Common emergency 1-2/1000 pts 10% rebleeed 1% angioembolization 20% over 60
A bleeding ulcer: What can the GP do? Gastrointestinal bleeding is a relatively common. How is UGI bleeding manifested? Who is at risk?
 Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
Focus on CME at the University of British Columbia A bleeding ulcer: What can the GP do? By Robert Enns, MD, FRCP Gastrointestinal bleeding is a relatively common disorder affecting thousands of Canadians
CrackCast Episode 30 GI Bleeding
 CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
CrackCast Episode 30 GI Bleeding Episode overview: 1) List 5 causes of UGIB in adults and pediatrics 2) List 5 causes of LGIB in adults and pediatrics 3) Describe your management approach for severe UGIB
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
58 year old male complaining of 3-week history of increasing epigastric pain
 Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
Peptic Ulcer Disease 58 year old male complaining of 3-week history of increasing epigastric pain Has had dyspepsia in the past for which he took Tums, but this is much worse and only partially relieved
SMALL GROUP DISCUSSION
 MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
MHD II, Session 1 Student Copy Page 1 SMALL GROUP DISCUSSION MHD II Session 1 Gastroinestinal Monday, January 9, 2017 STUDENT COPY MHD II, Session 1 Student Copy Page 2 CASE 1 CHIEF CONCERN: "I'm passing
HCPCS Codes (Alphanumeric, CPT AMA) ICD-9-CM Codes Covered by Medicare Program
 ICD-9-CM Codes Covered by Medicare Program") HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
HCPCS s (Alphanumeric, CPT AMA) 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal neoplasm screening ICD-9-CM
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Esophageal injuries. Pre-test /11/10. 新光急診張志華醫師 Facebook.com/jack119. O What is the most common cause of esophageal injuries?
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 O What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic 1 Pre-test 2 O Which contrast
ACUTE ABDOMEN. Dr. M Asadi. Surgical Oncology Research Center MUMS. Assistant Professor of General Surgery
 ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
ACUTE ABDOMEN Dr. M Asadi Assistant Professor of General Surgery Surgical Oncology Research Center MUMS Definition I. The term Acute Abdomen refers to signs & symptoms of abdominal pain and tenderness,
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
An Approach to Abdominal Pain
 An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
An Approach to Abdominal Pain objectives Should know the different types of abd pain Is acute or chronic? Hx taking skills with knowing the key questions Important abdominal pain signs A good differential
NCD for Fecal Occult Blood Test
 NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
NCD for Fecal Occult Blood Test Applicable CPT Code(s): 82272 Blood, occult, by peroxidase activity (e.g., guaiac), qualitative, feces, 1-3 simultaneous determinations, performed for other than colorectal
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC
 Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastrointestinal Emergencies CEN REVIEW 2017 MARY RALEY, BSN, RN, CEN, TCRN, TNSCC Gastrointestinal Emergencies is 7% of the CEN A. Acute abdomen B. Bleeding C. Cholecystitis D. Cirrhosis E. Diverticulitis
Gastroenterology. Certification Examination Blueprint. Purpose of the exam
 Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastroenterology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified gastroenterologist
Gastrointestinal bleeding and life threating conditions in surgery
 CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
CM w Bydgoszczy UMK w Toruniu Włodzimierz Gniłka Gastrointestinal bleeding and life threating conditions in surgery Gastrointestinal hemorrhage Upper GI hemorrhage proximal to the Treitz ligament (accounts
Oesophageal Disorders
 Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Oesophageal Disorders Anatomy Upper sphincter Oesophageal body Diaphragm Lower sphincter Gastric Cardia Symptoms Of Oesophageal Disorders Dysphagia Odynophagia Heartburn Atypical Chest Pain Regurgitation
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Suspected Foreign Body Ingestion
 Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Teresa Liang Suspected Foreign Body Ingestion 1. General Presentation Background: Of more than 100,000 cases of foreign body ingestion reported each year in the United States, 80% occur in children, with
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina
 Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
Back to Basics: What Imaging Test should I order? Jeanne G. Hill, M.D. Pediatric Radiology Medical University of South Carolina Disclosure Neither I nor any member of my immediate family has a relevant
The Usefulness of Capsule Endoscopy
 The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
The Usefulness of Capsule Endoscopy David J. Hass, MD, FACG Assistant Clinical Professor of Medicine Yale University School of Medicine Gastroenterology Center of Connecticut Obscure Gastrointestinal Bleeding
Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See
 Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Don t Waste Time with No Chance to See Kathy P. Bull-Henry, MD, FACG Dr. Bull-Henry has indicated no relevant financial relationships. Don t Waste Time With No Chance to See Kathy Bull-Henry, MD, FACG
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
9/10/2012. Chapter 44. Learning Objectives. Learning Objectives (Cont d) Bleeding
 Bleeding") Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Chapter 44 Bleeding 1 Learning Objectives Describe the etiology, history, and physical findings of external bleeding Predict hemorrhage on the basis of the patient s mechanism of injury Distinguish between
Occult GI Bleed. July 2015
 Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Occult GI Bleed July 2015 Occult GI Bleed Occult vs Obscure Occult positive FOB and/or IDA, but no evidence of visible blood loss to pt or physician Obscure GI bleed that persist/ recurs without obvious
Chapter Goal. Learning Objectives 9/12/2012. Chapter 29. Nontraumatic Abdominal Injuries
 Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Chapter 29 Nontraumatic Abdominal Injuries Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with nontraumatic abdominal pain Learning Objectives
Why Choose Wudassie Diagnostic Center for GI service? Ease of Use: One Location: Reduced Cross-Infection: Focus on the Patient: Reduced Cost:
 Why Choose Wudassie Diagnostic Center for GI service? In our center, patients find that the process much more convenient, as well as more personal. Our center offers a relaxed environment with medical
Why Choose Wudassie Diagnostic Center for GI service? In our center, patients find that the process much more convenient, as well as more personal. Our center offers a relaxed environment with medical
GIT RADIOLOGY. Water-soluble contrast media (e.g. gastrograffin) are the other available agents.which doesn t cause inflammatory peritonitis..
 are the other available agents.which doesn t cause inflammatory peritonitis..") GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
GIT RADIOLOGY Imaging techniques-general principles: Contrast examinations: Barium sulphate is the best contrast for GIT (with good mucosal coating & excellent opacification & being inert); but is contraindicated
Management of Lower Gastrointestinal Bleeding. Patrick Lau Department of Surgery Kwong Wah Hospital
 Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Management of Lower Gastrointestinal Bleeding Patrick Lau Department of Surgery Kwong Wah Hospital Lower Gastrointestinal bleeding The challenge Account for 20% of gastrointestinal bleeding 80% stopped
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
EGD Data Collection Form
 Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Sociodemographic Information Type Zip Code Gender Height (in inches) Race Ethnicity Inpatient Outpatient Male Female Birth Date Weight (in pounds) American Indian (Native American) or Alaska Native Asian
Colon Cancer , The Patient Education Institute, Inc. oc Last reviewed: 05/17/2017 1
 Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
Colon Cancer Introduction Colon cancer is fairly common. About 1 in 15 people develop colon cancer. Colon cancer can be a life threatening condition that affects the large intestine. However, if it is
Esophageal injuries. 新光急診張志華醫師 Facebook.com/jack119
 Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Esophageal injuries 新光急診張志華醫師 Facebook.com/jack119 Pre-test 1 What is the most common cause of esophageal injuries? A. Traffic accidents B. Gunshot wounds C. Iatrogenic Pre-test 2 Which contrast agent
Spleen indications of splenectomy complications OPSI
 Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Intestinal obstruction Differences between adynamic ileus and mechanical obstruction Aetiology Pathophysiology (Cluster contractions- bowel proximal to the obstruction dilate- wall of obstructed gut is
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
- Digestion occurs during periods of low activity - Produces more energy than it uses. - Mucosa
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Michele Bettinelli RN CCRN Lahey Health and Medical Center
 Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
Michele Bettinelli RN CCRN Lahey Health and Medical Center Differentiate the types of varices Identify glue preparations utilized when treating gastric varices Review the process of glue administration
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Departement of Surgery Faculty of Medicine University Sumatera Utara
 SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
SSS EESOPHAGEAL HPOSAGEAL DISORDERS IN SURGICAL PERSPECTIVE Departement of Surgery Faculty of Medicine University Sumatera Utara CONTENT 1. Esophageal Atresia 2. Achalasia 3. Esophageal Rupture 4. Tumor
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Anticoagulants are a contributing factor. Other causes are Mallory-Weiss tears, AV malformations, and malignancy and aorto-enteric fistula.
 Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Upper GI Bleeding EMU2018 Dr. Walter Himmel MD Incidence: In non-cirrhotics, the commonest causes are peptic ulcer disease (50%) followed by erosive gastritis. In cirrhotic patients, variceal bleeding
Objectives: Resources:
 Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Objectives: Realize the impact of Age : - Where/who are the history sources Recognize and interpret the : - Important symptoms - Important signs Resources: Davidson s. Slides Surgical recall. Raslan s
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment)
") Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Surgery for Complications of Peptic Ulcer Disease (Definitive Treatment) Amid Keshavarzi, MD UCHSC Grand Round 3/20/2006 Department of Surgery Introduction Epidemiology Pathophysiology Clinical manifestation
Upper gastrointestinal bleeding in children. Nguyễn Diệu Vinh, MD Department of Gastroenterology
 Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
Upper gastrointestinal bleeding in children Nguyễn Diệu Vinh, MD Department of Gastroenterology INTRODUCTION Upper gastrointestinal (UGI) bleeding : arising proximal to the ligament of Treitz in the distal
INTRODUCTION TO DIAGNOSTIC ENDOSCOPY
 INTRODUCTION TO DIAGNOSTIC ENDOSCOPY EGD & Colonoscopy Procedure Kolegium Ilmu Bedah Indonesia B. Parish Budiono Sub Bagian Bedah Digestif FK UNDIP/RSUP Dr. Kariadi Semarang GI Endoscopy GI Endoscopy is
INTRODUCTION TO DIAGNOSTIC ENDOSCOPY EGD & Colonoscopy Procedure Kolegium Ilmu Bedah Indonesia B. Parish Budiono Sub Bagian Bedah Digestif FK UNDIP/RSUP Dr. Kariadi Semarang GI Endoscopy GI Endoscopy is
INTRODUCTION TO UPPER ENDOSCOPY
 INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
INTRODUCTION TO UPPER ENDOSCOPY Satish Nagula, MD Associate Professor of Medicine Icahn School of Medicine at Mount Sinai NYSGE First Year Fellows Course July 14, 2018 Early endoscopes 1805: Bozzini Lichtleiter
GASTROINTESTINAL HEMORRHAGE
 Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
Anatomy GASTROINTESTINAL HEMORRHAGE Bleeding can occur anywhere along the gastrointestinal (GI) tract from the oropharynx to the anus. Bleeding is the initial presentation in 1/3 of patients with gastrointestinal
On-Call Upper GI Bleeding. Upper Gastrointestinal Bleeding
 On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
On-Call Upper GI Bleeding John R Saltzman MD, FACG Director of Endoscopy Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Upper Gastrointestinal Bleeding 300,000000 hospitalizations/year
Diarrhea may be: Acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections.
, which is usually related to bacterial or viral infections.") Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
Pediatric Gastroenterology Conditions Evaluated and Treated Having a child suffer with abdominal pain, chronic eating problems, or other gastrointestinal disorders can be a very trying time for a parent.
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Esophageal Disorders. Gastrointestinal Diseases. Peptic Ulcer Disease. Wireless capsule endoscopy. Diseases of the Small Intestine 7/24/2010
 Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
Esophageal Disorders Gastrointestinal Diseases Fernando Vega, MD HIHIM 409 Dysphagia Difficulty Swallowing and passing food from mouth via the esophagus Diagnostic aids: Endoscopy, Barium x ray, Cineradiology,
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING
 WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
WASSIM ABI JAOUDE, MD SUNY DOWNSTATE MEDICAL CENTER MAY 20 TH, 2010 MANAGEMENT OF ACUTE UPPER GI BLEEDING CASE PRESENTATION 74 YO female JEHOVAH S WITNESS admitted for CHEST PAIN to telemetry on 4/26/2010
Chapter 24 - Abdominal_Emergencies
 Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
Introduction to Emergency Medical Care 1 OBJECTIVES 24.1 Define key terms introduced in this chapter. 13, 15, 18, 20 22 24.2 Describe the location, structure, and function of the organs in the abdominal
But.. Capsule Endoscopy. Guidelines (OMED ECCO) Why is Enteroscopy so Important? 4/19/2017
 Why is Enteroscopy so Important? 4/19/2017") Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Dr. Elizabeth Odstrcil Digestive Health Associates of Texas April 22, 2017 But.. Capsules fail to reach the cecum in as many as 25% of patients Patients with known CD have a risk of capsule retention of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Fecal incontinence causes 196 epidemiology 8 treatment 196
 Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Subject Index Achalasia course 93 differential diagnosis 93 esophageal dysphagia 92 95 etiology 92, 93 treatment 93 95 work-up 93 Aminosalicylates, pharmacokinetics and aging effects 36 Antibiotics diarrhea
Gastric ulcer Duodenal ulcer Pancreatitis Ileus. Barbora Konečná
 Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
Gastric ulcer Duodenal ulcer Pancreatitis Ileus Barbora Konečná basa.konecna@gmail.com Peptic ulcers of stomach and duodenum (PUD) Ulcers are chronic, often solitary lesions, that occur in any part of
UGI BLEED. Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore
 UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
UGI BLEED Dr. KPP Abhilash Associate Professor Department of Emergency Medicine Christian Medical College, Vellore Outline UGI bleed: etiology and presentation Management: Non variceal / variceal bleed
Causes of abdominal pain Doctors in the ED spend lots of time and money diagnosing abdominal pain. They still often do not know the exact cause
 1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
1 2 3 What's Going On in There? EMS and Abdominal Pain Kevin McFarlane BSN,RN,CEN,CPEN,EMT Southwest Emergency Education and Consulting What is going on in there Acute Abdomen Sudden onset of pain within
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies
 Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Pearson's Comprehensive Medical Assisting Administrative and Clinical Competencies THIRD EDITION CHAPTER 30 The Digestive System Lesson 2: Pathology of the Digestive System Lesson Objectives Upon completion
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N
 Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Chapter 23 Endoscopic Diagnostic Procedures and Tests B Y L Y N N E L S L O O R N C G R N Objectives 1. Describe the different types of endoscopes and their components. 2. Discuss the indications for EGD,
Definitive Surgical Treatment When Endoscopy Fails. Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept.
 Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
Nonvariceal Gastrointestinal Hemorrhage: Definitive Surgical Treatment When Endoscopy Fails Erik Peltz D.O. Resident Debate February 26 th 2007 University of Colorado Dept. Surgery Non-Variceal Upper GI
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
- Digestion occurs during periods of low activity - Produces more energy than it uses. 3 Copyright 2016 by Elsevier Inc. All rights reserved.
 Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
Introduction Digestive System Chapter 29 Provides processes to break down molecules into a state easily used by cells - A disassembly line: Starts at the mouth and ends at the anus Digestive functions
DIGESTIVE SYSTEM CLASS NOTES. tube along with several
 DIGESTIVE SYSTEM CLASS NOTES Digestion Breakdown of food and the of nutrients in the bloodstream. Metabolism Production of for and cellular activities. The digestive system is composed of the canal which
DIGESTIVE SYSTEM CLASS NOTES Digestion Breakdown of food and the of nutrients in the bloodstream. Metabolism Production of for and cellular activities. The digestive system is composed of the canal which
Module 2 Heartburn Glossary
 Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
Absorption Antacids Antibiotic Module 2 Heartburn Glossary Barrett s oesophagus Bloating Body mass index Burping Chief cells Colon Digestion Endoscopy Enteroendocrine cells Epiglottis Epithelium Absorption
34th Annual Toronto Thoracic Surgery Refresher Course
 34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
34th Annual Toronto Thoracic Surgery Refresher Course TREATMENT OPTIONS FOR ACHALASIA Dr. Carmine Simone Director, Intensive Care Unit Head, Division of Critical Care Departments of Medicine and Surgery
Deep Enteroscopy Methods to Diagnose Small Bowel IBD
 Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
Deep Enteroscopy Methods to Diagnose Small Bowel IBD Name: Institution: Peter Draganov University of Florida, Gainesville, FL Overview Types of enteroscopy Enteroscopy equipment Enetoscopy do and don'ts
KK College of Nursing Peptic Ulcer Badil D ass Dass, Lecturer 25th July, 2011
 KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
KK College of Nursing Peptic Ulcer Badil Dass, Lecturer 25 th July, 2011 Objectives: By the end of this lecture, the students t will be able to: Define peptic pp ulcer Describe the etiology and pathology
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
SOD (Sphincter of Oddi Dysfunction)
") SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
Gastroesophageal Reflux Disease, Paraesophageal Hernias &
 530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
530.81 553.3 & 530.00 43289, 43659 1043432842, MD Assistant Clinical Professor of Surgery, UH JABSOM Associate General Surgery Program Director Director of Minimally Invasive & Bariatric Surgery Programs
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain
 Flexbook by Brian Lindshield is in the public domain") Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
Chapter 5: Common Digestive Problems from The Kansas State University Human Nutrition (HN 400) Flexbook by Brian Lindshield is in the public domain in the United States. 5 Common Digestive Problems Before
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology
 Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
Lahey Clinic Internal Medicine Residency Program: Curriculum for Gastroenterology Faculty representative: David L. Burns, MD, CNSP Resident representative: Tom Castiglione, MD Revision date: March 6, 2006
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint
 Examination Blueprint") GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
GASTROENTEROLOGY Maintenance of Certification (MOC) Examination Blueprint ABIM invites diplomates to help develop the Gastroenterology MOC exam blueprint Based on feedback from physicians that MOC assessments
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology
 Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
Management of Gastroenterology Emergencies Tim Gardner, MD Director, Pancreatic Disorders Section of Gastroenterology and Hepatology DHMC CREST Symposium November 7, 2008 There are no financial disclosures
The Aging Digestive System
 The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces
The Aging Digestive System shows significant senescence in old age: less saliva food less flavorful, harder swallowing ~half of those over 65 yrs wear dentures gastric mucosa secretes less acid reduces