RENINE Annual Report 2015
|
|
|
- Gilbert Weaver
- 6 years ago
- Views:
Transcription
 of the Nederlandse Federatie voor Nefrologie (NfN; Dutch federation for Nephrology): prof.dr. F.J.")

1 RENINE Annual Report 2015 T. Hoekstra, M.H. Hemmelder, F.J. van Ittersum In cooperation with the sectie Registratie (Registration division) of the Nederlandse Federatie voor Nefrologie (NfN; Dutch federation for Nephrology): prof.dr. F.J. van Ittersum, internist-nephrologist, epidemiologist chair sectie Registratie NfN dr. H. van Hamersvelt, internist-nephrologist, representative Guidelines division NfN dr. B. van Dam, internist-nephrologist, representative Guidelines division NfN dr. M.H. Hemmelder, internist-nephrologist, director Nefrovisie prof.dr. A. Hoitsma, emeritus internist-nephrologist, representative NOTR/NTS dr. V.S. Stel, epidemiologist, ERA-EDTA registry prof.dr. F.W. Dekker, epidemiologist dr. G. Laverman, internist-nephrologist dr. M. van Buren, internist-nephrologist dr. K. Cransberg, pediatric nephrologist P. v.d. Vlist, representative V&VN drs. H. Bart, director Nierpatiëntenvereniging Nederland (Dutch Association of Kidney Patients) drs. K. Prantl, Nierpatiënten Vereniging Nederland (Dutch Association of Kidney Patients) 2
2 CONTENTS Contents... 3 Introduction Prevalence and Incidence of renal replacement therapy Prevalence and Incidence of dialysis and renal transplants Prevalence and Incidence of dialysis Modalities Prevalence and Incidence of home dialysis Prevalence and Incidence of renal transplantations Pre-emptive renal transplantations and transplantation after dialysis Deceased donor and living donor renal transplantations Mortality Clinical data Phosphate and parathyroid hormone (PTH) Vascular access Discussion Appendix A. Definitions and methods Appendix B. Categorization of primary renal diseases Appendix C. Categorization Causes of death
3 INTRODUCTION The Nefrovisie foundation collects data from patients on renal replacement treatment in a national database (RENINE) since All Dutch dialysis centres 1. collaborate with this data collection to provide a nationwide overview of indicators of renal replacement treatment in the Netherlands. RENINE data are available on the webportal Nefrodata, both aggregated yearly data for the general public as well as actual centre specific data for the participating centres ( Nefrovisie has published annual reports since The annual report 2015 which we now present contains additional analyses in comparison to the 2014 report. The 2015 report has additional information on a number of clinical indicators, such as vascular access and PTH, as well as a more detailed analysis of mortality and causes of death. Dialysis centres provided data on clinical indicators in 2015 on a voluntary basis. Since 2016 the clinical indicators are an obligatory component of the RENINE data collection. We therefore expect to perform more complete analyses in future reports. In addition to general results for most topics, information is provided for different age categories as well as categories for primary renal disease. In addition to the 2014 report, data of children on renal replacement treatment are also included (age category 0-19 years). To enable international comparisons we use the same age and primary renal disease categories as the ERA-EDTA. We firstly present the 2015 report in English to enable international comparisons with registries of other countries. We also will provide a RENINE report 2015 in Dutch language which is suitable for patients. This report provides the main figures. Additional results will be provided on the website of Nefrovisie ( This will be indicated in the report if applicable. It should be noted that the numbers presented in this annual report might differ from the numbers on Nefrodata due to different definitions. 1 In Appendix D. an overview of the dialysis centres is given. 4
.")

4 1. PREVALENCE AND INCIDENCE OF RENAL REPLACEMENT THERAPY Renal replacement therapy (RRT) includes both renal transplantation as well as dialysis. At the end of 2015, 16,724 patients were on RRT in the Netherlands. The number of prevalent RRT patients shows a steady increase over the years (Figure 1.1). However, the number of patients starting RRT in a year, i.e. the incidence, has remained quite stable during the last seven years. In 2015, 1,996 patients started for the first time with renal replacement therapy with either renal transplantation or dialysis. The same pattern is observed when the prevalence and incidence are expressed as patients per million of the population (ppm) (Figure 1.2): in 2015, about 119 patients per million population started renal replacement therapy. Figure 1.1. Prevalence and incidence of renal replacement therapy Figure 1.2. Prevalence and incidence of renal replacement therapy expressed per million population. 5
.")


5 Age categories The patients were categorized into five age categories 2. Figure 1.3 shows age specific prevalences and incidences of renal replacement therapy per million age related population (pmarp). 3 These figures indicate that the overall rise in prevalence of RRT is caused by steady increases in the older age categories. In 2015, the prevalence per million population was with 2,354 patients per million the highest in the age category of 75 years and older. Incidence was also the highest in this age category (393 patients per million population). However, the prevalence in patients over 75 years seems to stabilize during the last years and the incidence is showing a decrease during the last years. Figure 1.3. Prevalence and incidence of renal replacement therapy in age categories expressed per million age related population. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 2 Age categories are in accordance to the age categories used by the ERA-EDTA registry 3 Figures with overall numbers per age category are shown in the online appendix. 6

6 Primary kidney disease and renal replacement therapy Primary kidney diseases were categorized in nine categories according to the ERA-EDTA categorization (see Appendix B). Figure 1.4 shows prevalences and incidences in the different categories. The primary kidney disease categories with the largest contribution to the prevalence of RRT are the categories miscellaneous and unknown. Prevalences of hypertension, diabetes type 2 and miscellaneous categories are all rising, although the incidence in these categories is rather stable. There is a remarkable rise in the category with unknown primary kidney disease. This is the only category with not only an increase over the years in the number of prevalent patients but also with a clear increase in incidence. 7


7 Figure 1.4. Prevalence and incidence of renal replacement therapy in primary kidney disease categories. 8
 Figure 2.1 also shows the incidence of both treatment modalities.")

8 2. PREVALENCE AND INCIDENCE OF DIALYSIS AND RENAL TRANSPLANTS The prevalence of patients with dialysis has been quite stable since 2009, whilst the number of patients living with a functioning renal transplant has shown a steady increase over time (Figure 2.1) Figure 2.1 also shows the incidence of both treatment modalities. Incidence has been defined by patients who received a renal transplant or started dialysis as their first renal replacement therapy. Figure 2.2 shows prevalences and incidences expressed per million of the population. In 2015, 1,749 patients started dialysis as the first renal replacement therapy and 247 patients received a renal transplant as first therapy (i.e. first pre-emptive transplant). Figure 2.1. Prevalence and incidence of dialysis and renal transplants. Incidence only includes patients without previous renal replacement therapy. Figure 2.2. Prevalence and incidence of dialysis and renal transplants expressed per million population. Incidence only includes patients without previous renal replacement therapy. When we change the definition of incidence to all patients who start with dialysis or receive a renal transplant, irrespective of earlier RRT treatment, 980 patients had a renal transplant and 1,998 patients started with dialysis in 2015 (Figure 2.3 and 2.4 (ppm)). Figure 2.3. Prevalence and incidence of dialysis and renal transplants. Incidence includes all patients starting dialysis or receiving a renal transplant irrespective of previous renal replacement therapy. Figure 2.4. Prevalence and incidence of dialysis and renal transplants expressed per million population. Incidence includes all patients starting dialysis or receiving a renal transplant irrespective of previous renal replacement therapy. 9




9 Figure 2.5 shows the prevalences and incidences of dialysis and renal transplants in different age categories. The numbers are shown per million age related population. Incidences includes only patients starting therapy as first RRT treatment 4. In young prevalent patients renal transplantation is the dominant therapy. In the age category years more patients were treated with dialysis than with renal transplantation until From 2011 more patients are living with a functioning renal transplant than being treated with dialysis in this age category. In the patients over 75 years of age dialysis remains the prevailing therapy. Figure 2.5. Prevalence and incidence of dialysis and renal transplants in age categories expressed per million age related population. Incidence includes only patients without previous renal replacement therapy. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 4 Figures showing incidence irrespective of previous renal replacement therapy for the age categories are presented in the online appendix. 10


10 Figure 2.6 shows prevalences and incidences for primary kidney disease categories 5. Noteworthy is the steep increase in both the prevalence and incidence of patients with renal transplantation in the category with unknown primary disease. A gradual increase of prevalence and incidence of patients with type 2 diabetes mellitus and dialysis persists, just as a gradual decrease of patients with pyelonephritis and dialysis. 5 Figures showing incidence irrespective of previous renal replacement therapy for the primary kidney disease categories are presented in the online appendix. 11


11 Figure 2.6. Prevalence and incidence of dialysis and renal transplants in primary kidney disease categories. Incidence includes only patients without previous renal replacement therapy. The mean age of prevalent dialysis and renal transplant patients has increased over time. In 2015 the mean age of dialysis patients was 67.4 years compared to 55.6 years for patients living with a renal transplant. In addition, the age at which patients started renal replacement therapy with either a transplantation or with dialysis has increased over time (Figure 2.7 and 2.8). Figure 2.7. Mean age of incident and prevalent dialysis patients. Incident dialysis patients are patients starting dialysis as first RRT. Figure 2.8. Mean age of incident and prevalent patients with renal transplant. Incident transplant patients are the patients that received a renal transplant as first RRT. 12
.")

12 3. PREVALENCE AND INCIDENCE OF DIALYSIS MODALITIES The majority of patients on dialysis has been treated with haemodialysis. The number of patients treated with peritoneal dialysis shows a steady decrease over the years (Figure 3.1). However, the incidence of peritoneal dialysis is not further decreasing. Figure 3.1. Prevalence and incidence of haemodialysis and peritoneal dialysis. Incidence of dialysis only includes patients without previous renal replacement therapy. Figure 3.2. Prevalence and incidence of haemodialysis and peritoneal dialysis per million population. Incidence of dialysis only includes patients without previous renal replacement therapy. 13


13 The number of patients in the different age categories (per million age related population) and primary kidney disease categories are shown in Figure 3.3. and 3.4. The increase in prevalence of HD is primarily seen in the category of patients 75 years and older. However, since 2010 the incidence in this age category has been decreasing again and the number of prevalent patients seems to stabilize. The decrease in number of prevalent PD patients is most apparent in the age category years, even though the incidence is rather stable in this age category. Figure 3.3. Prevalence and incidence of haemodialysis and peritoneal dialysis in age categories expressed per million age related population. Incidence includes only patients without previous renal replacement therapy. Incidence only includes patients without previous renal replacement therapy. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 14
14 15



15 Figure 3.4. Prevalence and incidence of haemodialysis and peritoneal dialysis in primary kidney disease categories. Incidence only includes patients without previous renal replacement therapy. 16
16 Switches between modalities RENINE documents changes between dialysis modalities. For the current analyses only switches between dialysis modalities lasting longer than 30 days were included. In 2015, 175 switches of HD to PD were recorded and 239 switches of PD to HD. In Figure 3.5 and Figure 3.6. trends over time in modality changes are shown. For completeness transplantations are also reported. To make comparisons between the calendar years easier, the number of switches are expressed as percentage of the prevalent number of patients on either HD and PD at the beginning of the calendar year. Over time switches from PD to HD became more common. In addition, the time a patient is being treated by PD before switching to HD became shorter over time (See Figure 3.7.). In contrast, switching from HD to PD has happened less often in recent years. Figure 3.5. Modality changes in haemodialysis patients expressed as percentage of prevalent haemodialysis patients at the start of the calendar year. Figure 3.6. Modality changes in peritoneal dialysis patients expressed as percentage of prevalent peritoneal dialysis patients at the start of the calendar year. Figure 3.7. Time on dialysis modality at the moment of a switch to another dialysis modality 17
.")

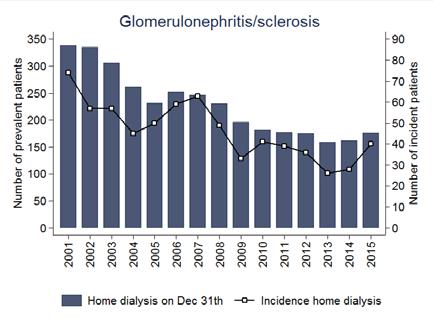
17 4. PREVALENCE AND INCIDENCE OF HOME DIALYSIS Home dialysis includes home haemodialysis and peritoneal dialysis. The number of prevalent patients treated with home dialysis is decreasing over the years (Figure 4.1 and 4.2). On December 31th ,140 patients were treated with home dialysis, which is 18% of the total patient population on dialysis. The incidence of home dialysis tends to rise. It should be noted that the incidence of home dialysis almost exclusively consists of peritoneal dialysis, because home haemodialysis is generally being performed after a start with in-centre haemodialysis. Figure 4.1. Prevalence and incidence of home dialysis (home haemodialysis and peritoneal dialysis). Incidence only includes patients without previous renal replacement therapy. Figure 4.2. Prevalence and incidence per million population of home dialysis (home haemodialysis and peritoneal dialysis). Incidence only includes patients without previous renal replacement therapy. 18
 and primary kidney disease categories are shown in Figure 4.3 and 4.")



18 The prevalences and incidences in different age categories (per million age related population) and primary kidney disease categories are shown in Figure 4.3 and 4.4, respectively. The age category 75 years and above is the only age category in which the number of patients on home dialysis is increasing. Figure 4.3. Prevalence and incidence of home dialysis (home haemodialysis and peritoneal dialysis) in age categories expressed per million age related population. Incidence only includes patients without previous renal replacement therapy. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 19
19 20

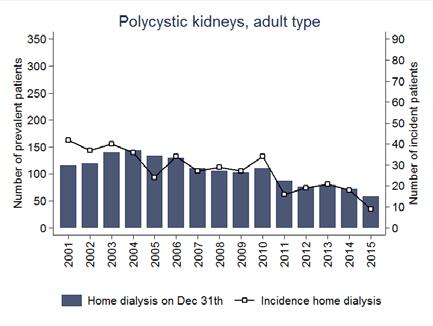
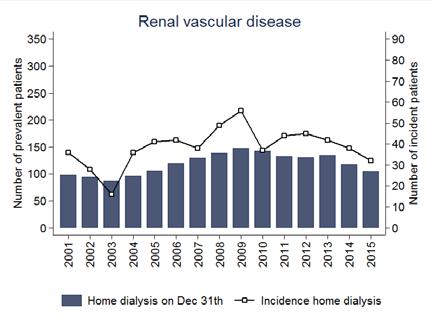
20 Figure 4.4. Prevalence and incidence of home dialysis (home haemodialysis and peritoneal dialysis) in categories of primary kidney disease. Incidence only includes patients without previous renal replacement therapy. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 21

.")
21 Peritoneal dialysis remains the primary modality in home dialysis as shown in Figure 4.5. In this figure home dialysis is presented as percentage of total dialysis. The fraction home haemodialysis has been slightly increased in In the online Appendix similar figures are shown for age and primary kidney disease categories. Figure 4.5. Prevalence of peritoneal dialysis and home haemodialysis on December 31th. Prevalence is expressed as percentage of total dialysis. The proportion of patients that is being treated with home dialysis shows a substantial variation among centres. A funnel plot analysis shows the percentage of home dialysis of the total patients on dialysis against the total number of dialysis patients (Figure 4.6). It should be noted that some centres only offer in-centre haemodialysis, but may refer patients for home haemodialysis to other centres. Therefore, it would be more informative to also include information on the number of patients that are being referred to another centre for home dialysis. More detailed analyses on this issue are planned for future reports. Figure 4.6. Funnel plot of the variation in home dialysis over centres. The percentage home dialysis is calculated based on the number of prevalent patients on December Dashed lines show the 95% confidence limits. 22

22 5. PREVALENCE AND INCIDENCE OF RENAL TRANSPLANTATIONS PRE-EMPTIVE RENAL TRANSPLANTATIONS AND TRANSPLANTATION AFTER DIALYSIS Prevalence and incidence of renal transplantation, separately for pre-emptive and transplants after dialysis are shown in Figure 5.1. and 5.2. Both types of renal transplantation are increasing over time. However, the incidence of renal transplantation after dialysis decreased in 2015 compared to Figure 5.1. Prevalence and incidence of pre-emptive transplantations and transplantations after dialysis. Figure 5.2. Prevalence and incidence per million population of preemptive transplantations and transplantations after dialysis. 23


23 Prevalences and incidences of renal transplantation for age categories and categories of primary kidney disease are shown in Figure 5.3 and 5.4. Prevalence and incidence per million population is highest in the age category years. Pre-emptive renal transplantations are overrepresented in the category unknown primary kidney disease. Figure 5.3. Prevalence and incidence of pre-emptive transplantations and transplantations after dialysis per million age related population in age categories. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 24
24 25
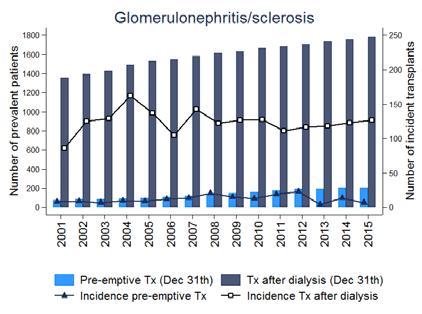
25 Figure 5.4. Prevalence and incidence of pre-emptive transplantations and transplantations after dialysis in primary kidney disease categories. 26
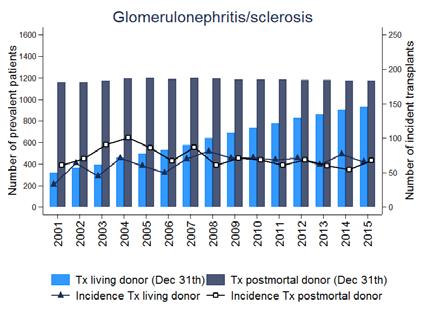
26 DECEASED DONOR AND LIVING DONOR RENAL TRANSPLANTATIONS The number of renal transplantations performed with kidneys from deceased and living donors are shown in figure 5.5 and 5.6. A steep increase in living donor transplantations is being observed. In 2015, 515 living donor transplantations were performed which is 63% of the total number of renal transplantations. Figure 5.5. Prevalence and incidence of transplantations with living and deceased (post mortal) donors. Figure 5.6. Prevalence and incidence of transplantations with living and deceased (post mortal) donors per million population. 27

 donors per million")
27 The number of living donor and deceased donor transplantations for different age categories and primary kidney disease categories are shown in Figures 5.7 and 5.8. Figure 5.7. Prevalence and incidence of transplantations with living and deceased (post mortal) donors per million population in age categories. To improve readability of the graph the scale of the youngest age category was adjusted to 10% of the scale in the other categories. 28
28 29

29 Figure 5.8. Prevalence and incidence of transplantations with living and post mortal donors in primary kidney disease categories. 30
.")

30 6. MORTALITY In 2015, 1426 patients died on renal replacement therapy. The majority (n=1,154; 81%) were patients on dialysis (Figure 6.1.). Figure 6.1. Number of patients who died on renal replacement therapy per calendar year. Causes of death were categorized into seven categories in accordance with the categorization used by the UK Renal Registry (see Appendix C). The most common cause of death in dialysis patients was stopping with treatment. The category Uncertain is the dominant category in patients with renal transplantation with a gradual increase. Figure 6.2. Causes of death in patients on dialysis Figure 6.3. Causes of death in patients with a renal transplant 31
31 Survival of patients starting renal replacement therapy in different cohorts are shown in Figures 6.4 and 6.5. In the crude Kaplan-Meier curves it can be seen that survival improved over time (Figure 6.4). After adjustments for fixed values of age, gender and primary kidney disease the improvement of survival during time became more apparent. Survival of patients starting dialysis is shown in Figure 6.6 and 6.7. In the crude Kaplan-Meier analysis, survival of the and cohorts overlap, but in the adjusted analysis, an improvement could be observed. It should be noted that firm conclusions cannot be drawn because we could not perform a complete case mix correction because important data on co-morbidity are not available. Figure 6.4. Unadjusted Kaplan- Meier survival curves for patients starting renal replacement therapy in different cohorts. Figure 6.5. Survival curves for patients starting renal replacement therapy in different cohorts. Analyses were adjusted for age, gender and using fixed values (age 60, 60% men, primary kidney disease distribution: 20% diabetes, 17% hypertension/renal vascular disease, 15% glomerulonephritis and 48% other causes). Figure 6.6. Unadjusted Kaplan-Meier survival curves for patients starting dialysis in different cohorts.only patients starting dialysis as first renal replacement therapy are included. Figure 6.7. Survival curves for patients starting dialysis in different cohorts. Analyses were adjusted for age, gender and using fixed values (age 60, 60% men). Only patients starting dialysis as first renal replacement therapy are included. Analyses were adjusted for age, gender and using fixed values (age 60, 60% men, primary kidney disease distribution: 20% diabetes, 17% hypertension/renal vascular disease, 15% glomerulonephritis and 48% other causes). 32
32 Survival of patients starting peritoneal dialysis is higher than survival on haemodialysis in the crude Kaplan-Meier analysis (Figure 6.8.). After adjustment for fixed values of age, gender and primary kidney disease a much smaller difference between these two modalities was present (Figure 6.9.) More extensive adjustments are necessary to draw firm conclusions on differences in survival between these treatment modalities. Figure 6.8. Unadjusted Kaplan-Meier survival curves for haemodialysis and peritoneal dialysis patients (cohort ). Figure6.9. Survival curves for haemodialysis and peritoneal dialysis patients (Cohort ). Analyses were adjusted for age and gender using fixed values (age 60, 60% men, primary kidney disease distribution: 20% diabetes, 17% hypertension/renal vascular disease, 15% glomerulonephritis and 48% other causes). 33

33 7. CLINICAL DATA A limited number of clinical indicators has been provided to RENINE on a voluntary basis. For the available data individual patient records are provided every three months. For this analyses only the first available measurement for a patient per calendar year was used. The number of centres that provided data on PTH and phosphate levels decreased from 45 centres in 2012 to only 25 in 2015 (Figure 7.1). PTH and phosphate data were available for about one third of all dialysis patients In We report on these data in the next figures. It should be noted that the observations might be biased by the fact that different centres provided data over the years. Figure 7.1. Number of centres that provided phosphate data and number of patients with at least one phosphate measurement available in a calendar year. PHOSPHATE AND PARATHYROID HORMONE (PTH) Mean phosphate levels decreased in 2015 compared to the previous years (Figure 7.2.) with a mean (SD) phosphate of 1.51(0.46) mmol/l. In addition, the percentage of patients with high phosphate levels also decreased over time (Figure 7.3). Mean parathyroid levels are reported in Figure 7.4. Figure 7.2. Mean phosphate levels with 95%-confidence intervals Figure 7.3. Percentage of patients in categories of phosphate levels. 34
 for each dialysis centre in a funnel plot.")

34 Figure 7.4. Mean PTH levels with 95% confidence intervals Figure 7.5. Percentage of patients in categories of PTH levels Figure 7.6 shows the percentage patients with high serum phosphate (i.e. > 1.8 mmol/l) for each dialysis centre in a funnel plot. Considerable variation exists with one centre above and one centre below the 95-% confidence interval. Figure 7.6. Funnel plot of the percentage patients with serum phosphate levels >1.8 mmol/l per centre. Dashed lines show the 95% confidence limits. 35
 in 2015.")
35 VASCULAR ACCESS Data on vascular access have also been registered at 3 months intervals. Figure 7.7. and 7.8 report on patients that started with haemodialysis. Like for PTH and phosphate, data availability on vascular access decreased over time. Vascular access data were available in 246 incident haemodialysis patients (15%) in Most of these patients (42%) started with a central venous catheter. After inclusion of all available data after start of haemodialysis the distribution of the vascular access is very different with approximately 15% central venous catheters (Figure 7.9). Figure 7.7. Number of patients that started haemodialysis and for whom data is available on vascular access Figure 7.8. Distribution of vascular access at start of haemodialysis Figure 7.9. Overall distribution of vascular access categories. 36
36 8. DISCUSSION In this RENINE 2015 annual report, Nefrovisie in collaboration with NfN provide more insight into a number of indicators of renal replacement therapy in the Netherlands. The information in this report is more extensive than in the previous RENINE 2014 annual report. We provide survival curves for patients on different renal replacement therapies and data on causes of death. These are the most important observations from the RENINE 2015 annual report: The incidence of patients seems to stabilize, although the number of prevalent renal replacement therapy patients is continuously growing. This trend is also observed in the primary kidney disease categories diabetes and hypertension. The cause of this development cannot be derived from our registry data. Possibly, the improvement of preventive renal care and the ensuing publication of new guidelines has gained effect over the last years. An already known decrease in incidence of home dialysis was confirmed, although there seems to be a trend to an increase of home dialysis in When we consider renal transplantation as a home treatment modality, the number of patients treated at home has increased tremendously over the last 15 years. There is a strong increase in the proportion of patients with unknown primary kidney disease. This trend was most apparent in renal transplantation patients. Similarly, in these patients, cause of death is more often unknown. Possibly, this is due to information bias in our database. We will investigate this issue in collaboration with the NOTR,. Survival analysis tends to show an improvement of survival in time, both for patients starting with renal replacement therapy as for patients starting with dialysis. I In this report, we firstly present data on phosphate, PTH and vascular access that were registered voluntarily by a part of the dialysis centres. The mean phosphate levels decreased over time as well as the proportion of patients in the highest phosphate categories. About 42% of the patients start with haemodialysis using a central venous catheter. We don t know the proportion of these patients that were prepared in a predialysis program. It is impossible to draw conclusions because we cannot exclude selection bias over the years, whereas centres stopped and started providing non-obligatory data to RENINE. Since dialysis centres provide obligatory clinical data from 2016, we expect to be able to extend information in our next annual report. Furthermore, we intend to collect data of patients in the predialysis period and data on comorbidity. This is necessary to draw firm conclusions after appropriate case-mix analysis on the quality of renal replacement treatment in the Netherlands. In conclusion, the incidence of patients on renal replacement therapy has been stabilized. The prevalence is still increasing, mainly due to patients with a functioning renal transplant. The next years Nefrovisie and NfN will continue to modify the information presented in the report to accommodate the needs of the different stake holders in a more optimal way. 37
37 APPENDIX A. DEFINITIONS AND METHODS Prevalence The number of people in a given population with a particular disease at a given time. In this report prevalence is the number of patients on a (specific) renal replacement therapy on December 31th of a calendar year. Incidence The number of new cases during a specific time period. In this report incidences per calendar years are reported. Throughout the report we use two definitions for incidence. 1. Incidence including only patients without previous renal replacement therapy. This means that patients who start dialysis after renal transplant failure are not included in the incidence number, as well as patients who have a second or third renal transplant after a previous transplant failure with or without a period with dialysis. Thus only patients who received a renal transplant or started dialysis as their first renal replacement therapy are counted. 2. Incidence including all patients who start with dialysis or receive a renal transplant, irrespective of earlier RRT. In this case, patients who start dialysis after renal transplant failure are thus included, as well as patients who have a second or third renal transplant after a previous transplant failure with or without a period with dialysis. Throughout the report we explicitly state which definition for incidence was used for the various analyses. Per million (age-related) population The incidence or prevalence per million population (pmp) is the observed incident or prevalent count divided by the general population in that year and multiplied by one million. The incidence or prevalence per age-related population (pmarp) is the observed incident or prevalent count for a specific age group divided by the general population of that age group and multiplied by one million. Information on the (age-specific) population in the calendar years is provided by Statistics Netherlands (Centraal Bureau voor de Statistiek). Survival analyses Survival was analysed from start of renal replacement therapy. Survival time was censored in case of recovery of kidney function of at least 30 days or when patients were lost to follow-up. Crude survival curves are being presented using the Kaplan-Meier method. Cox regression analysis was used to calculate adjusted survival curves. Survival was adjusted to age 60 years, 60% men and primary kidney disease distribution of 20% diabetes, 17% hypertension/renal vascular disease, 15% glomerulonephritis and 48% other causes. These fixed values were are in accordance to the fixed values applies in the ERA-EDTA Annual Report Funnel plots Variation across centres is shown in funnel plots. In these plots centre specific data is plotted against the sample size of that centre. A horizontal line represents the group average. The 95%-confidence intervals were estimated using a binomial distribution. 38
38 APPENDIX B. CATEGORIZATION OF PRIMARY RENAL DISEASES ERA- EDTA code Primary renal disease Glomerulonephritis/sclerosis 10 Glomerulonephritis, histologically NOT examined 11 Severe nephrotic syndrome with focal sclerosis (paediatric patients only) 12 IgA nephropathy (proven by immunofluorescence, not code 85) 13 Dense deposit disease membrano-proliferative GN, type II (proven by immunofluorescence and/or electron microscopy) 14 Membranous nephropathy 15 Membrano-proliferative GN, type I (proven by immunofluorescence and/orelectron microscopy - not code 84 or 89) 16 Rapidly progressive GN without systemic disease (crescentic, histologically confirmed, not coded elsewhere) 19 Glomerulonephritis, histologically examined 17 Focal segmental glomerusclerosis with nephrotic syndrome in adults Pyelonephritis 20 Pyelonephritis/Interstitial nephritis-cause not specified 21 Pyelonephritis/Interstitial nephritis associated with neurogenic bladder 22 Pyelonephritis/Interstitial nephritis due to congenital obstructive uropathy with or without vesico-ureteric reflux 23 Pyelonephritis/Interstitial nephritis due to acquired obstructive uropathy 24 Pyelonephritis/Interstitial nephritis due to vesicoureteric reflux without obstruction 25 Pyelonephritis/Interstitial nephritis due to urolithiasis 29 Pyelonephritis/Interstitial nephritis due to other cause Polycystic kidneys, adult type 41 Polycystic kidneys, adult type (dominant) Hypertension 71 Renal vascular disease due to malignant hypertension (NO primary renal disease) 72 Renal vascular disease due to hypertension (NO primary renal disease) 39
39 ERA- EDTA code Primary renal disease Renal vascular disease 70 Renal vascular disease-type unspecified 79 Renal vascular disease-classified Diabetes, type 1 80 Diabetes glomerulosclerosis or diabetic nephropathy Type 1 Diabetes, type 2 81 Diabetes glomerulosclerosis or diabetic nephropathy Type II Miscellaneous 30 Tubulo interstitial nephritis (not pyelonephritis) 31 Nephropathy due to analgesic drugs 32 Nephropathy due to cis-platinum 33 Nephropathy due to cyclosporin A 39 Nephropathy caused by other specific drug 40 Cystic kidney disease-type unspecified 42 Polycystic kidneys, infantile (recessive) 43 Medullary cystic disease, including nephronophthisis 49 Cystic kidney disease-other specified type 50 Hereditary/Familial nephropathy-type unspecified 51 Hereditary nephritis with nerve deafness (Alport's Syndrome) 52 Cystinosis 53 Primary oxalosis 54 Fabry s disease 59 Hereditary nephropathy-other 60 Congenital renal hypoplasia-type unspecified 61 Oligomeganephronic hypoplasia 63 Congenital renal dysplasia with or without urinary tract malformation 66 Syndrome of agenesis of abdominal muscles (Prune Belly Syndrome) 73 Renal vascular disease due to polyarteritis 74 Wegener s granulomatosis 82 Myelomatosis/light chain deposit disease 83 Amyloid 84 Lupus erythematosus 85 Henoch-Schoenlein purpura 86 Goodpasture s Syndrome 87 Systemic sclerosis (scleroderma) 40
40 ERA- EDTA code Primary renal disease Miscellaneous 88 Haemolytic Uraemic Syndrome including Moschcowitz Syndrome 89 Multi-system disease-other 90 Cortical or tubular necrosis 91 Tuberculosis 92 Gout 93 Nephrocalcinosis and hypercalcaemic nephropathy 94 Balkan nephropathy 95 Kidney tumour 96 Traumatic or surgical loss of kidney 99 Other identified renal disorders 34 Lead induced interstitial nephropathy 75 Ischaemic renal disease / cholesterol embolisation 76 Glomerulonephritis related to liver cirrhosis 78 Cryglobulinaemic glomerulonephritis Unknown 0 Chronic renal failure, aetiology uncertain 41
41 APPENDIX C. CATEGORIZATION CAUSES OF DEATH EDTA code Cause Category 0 Cause of death uncertain/not determined Uncertain 11 Myocardial ischaemia and infarction Heart 12 Hyperkalaemia Other 13 Haemorrhagic pericarditis Other 14 Other causes of cardiac failure Heart 15 Cardiac arrest/sudden death; other cause or unknown Heart 16 Hypertensive cardiac failure Heart 17 Hypokalaemia Other 18 Fluid overload/pulmonary oedema Heart 21 Pulmonary embolus Other 22 Cerebro-vascular accident, other cause or unspecified CVA 23 Gastro-intestinal haemorrhage Other 24 Haemorrhage from graft site Other 25 Haemorrhage from vascular access or dialysis circuit Other 26 Haemorrhage from ruptured vascular aneurysm (not code 22 or 23) Other 27 Haemorrhage from surgery (not code 23, 24 or 26) Other 28 Other haemorrhage (not codes 23-27) Other 29 Mesenteric infarction Other 30 Infection Infection 31 Pulmonary infection (bacterial - not code 73) Infection 32 Pulmonary infection (viral) Infection 33 Pulmonary infection (fungal or protozoal) Infection 34 Infections elsewhere (except viral hepatitis see codes 41-42) Infection 35 Septicaemia Infection 36 Tuberculosis (lung) Infection 37 Tuberculosis (elsewhere) Infection 38 Generalised viral infection Infection 39 Peritonitis (all causes except for Peritoneal Dialysis) Infection 41 Liver disease due to hepatitis B virus Other 42 Liver disease due to other viral hepatitis Other 43 Liver disease due to drug toxicity Other 44 Cirrhosis - not viral Other 45 Cystic liver disease Other 46 Liver failure - cause unknown Other 51 Patient refused further treatment Treatment stop 52 Suicide Other 53 ESRF treatment ceased for any other reason Treatment stop 54 ESRF treatment ceased for medical reasons Treatment stop 61 Uraemia caused by graft failure Treatment stop 62 Pancreatitis Other 63 Bone marrow depression Other 42
42 EDTA code Cause Category 64 Cachexia Other 66 Malignant disease possibly induced by immunosuppressive therapy Malignancies 67 Malignant disease: solid tumors except those of 66 Malignancies 68 Malignant disease: lymphoproliferative disorders except those of 66 Malignancies 69 Dementia Other 70 Peritonitis (sclerosing, with peritoneal dialysis) Other 71 Perforation of peptic ulcer Other 72 Perforation of colon Other 73 Chronic obstructive airways (lung) disease Other 80 Accident (all causes, specify) Other 81 Accident related to ESRF treatment (not code 25) Other 82 Accident unrelated to treatment Other 90 Gastro-intestinal - other (specify) Other 99 Other identified cause of death Other 100 Peritonitis (bacterial, with peritoneal dialysis) Infection 101 Peritonitis (fungal, with peritoneal dialysis) Infection 102 Peritonitis (due to other cause, with peritoneal dialysis Infection 43
RENINE year report 2016
 RENINE year report 216 T. Hoekstra, F.J. van Ittersum and M.H. Hemmelder In cooperation with the sectie Registratie (Registration division) of the Nederlandse Federatie voor Nefrologie (NfN; Dutch federation
RENINE year report 216 T. Hoekstra, F.J. van Ittersum and M.H. Hemmelder In cooperation with the sectie Registratie (Registration division) of the Nederlandse Federatie voor Nefrologie (NfN; Dutch federation
Appendix G Coding: Ethnicity, EDTA Primary Renal Diagnoses, EDTA Causes of Death and Treatment Timeline Modality Codes
 Coding: Ethnicity, EDTA Primary Renal Diagnoses, EDTA Causes of Death and Treatment Timeline Modality Codes G1: Ethnicity coding Ethnicity data is recorded in the clinical information systems in the individual
Coding: Ethnicity, EDTA Primary Renal Diagnoses, EDTA Causes of Death and Treatment Timeline Modality Codes G1: Ethnicity coding Ethnicity data is recorded in the clinical information systems in the individual
ESRD Dialysis Prevalence - One Year Statistics
 Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Age Group IL Other Total 00-04 12 1 13 05-09 5 2 7 10-14 15 1 16 15-19 55 2 57 20-24 170 10 180 25-29 269 14 283 30-34 381 9 390 35-39 583 14 597 40-44 871 20 891 45-49 1,119 20 1,139 50-54 1,505 35 1,540
Chapter 15: Causes of Death on Renal Replacement Therapy
 Chapter 15: Causes of Death on Renal Replacement Therapy Summary Cardiovascular disease is the most common cause of death in the renal population and is most evident in diabetics. Patients on renal replacement
Chapter 15: Causes of Death on Renal Replacement Therapy Summary Cardiovascular disease is the most common cause of death in the renal population and is most evident in diabetics. Patients on renal replacement
USRDS UNITED STATES RENAL DATA SYSTEM
 USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
USRDS UNITED STATES RENAL DATA SYSTEM Chapter 8: Pediatric ESRD 1,462 children in the United States began end-stage renal disease (ESRD) care in 2013. 9,921 children were being treated for ESRD on December
Chapter 8: ESRD Among Children, Adolescents, and Young Adults
 Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
Chapter 8: ESRD Among Children, Adolescents, and Young Adults The number of children beginning end-stage renal disease (ESRD) care decreased by 6% in 2014, totaling 1,398 (Figure 8.1.a). 9,721 children
CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 2007
 CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 27 Stephen McDonald Leonie Excell Hannah Dent NEW PATIENTS ANZDATA Registry 28 Report Figure 2.1 Annual Intake of New Patients 23-27 (Number Per Million Population)
CHAPTER 2 NEW PATIENTS COMMENCING TREATMENT IN 27 Stephen McDonald Leonie Excell Hannah Dent NEW PATIENTS ANZDATA Registry 28 Report Figure 2.1 Annual Intake of New Patients 23-27 (Number Per Million Population)
ERA-EDTA Registry Annual Report 2001
 ERA-EDTA Registry Annual Report 2001 Suggested citation ERA-EDTA Registry: ERA-EDTA Registry 2001 Annual Report. Academic Medical Center, Amsterdam, The Netherlands, June 2003. i ERA-EDTA Registry Dept.
ERA-EDTA Registry Annual Report 2001 Suggested citation ERA-EDTA Registry: ERA-EDTA Registry 2001 Annual Report. Academic Medical Center, Amsterdam, The Netherlands, June 2003. i ERA-EDTA Registry Dept.
Chapter 1. Incidence of End Stage Kidney Disease. Contents:
 Chapter 1 Incidence of End Stage Kidney Disease Contents: Incidence of End Stage Kidney Disease 1-1 Stock and Flow 1-2 Incident patients 1-3 Incident Rates 1-3 Late Referral 1-7 Co-Morbidities 1-9 Primary
Chapter 1 Incidence of End Stage Kidney Disease Contents: Incidence of End Stage Kidney Disease 1-1 Stock and Flow 1-2 Incident patients 1-3 Incident Rates 1-3 Late Referral 1-7 Co-Morbidities 1-9 Primary
CHAPTER 3 DEATHS. Stephen McDonald Leonie Excell Brian Livingston
 CHAPTER 3 DEATHS Stephen McDonald Leonie Excell Brian Livingston DEATHS ANZDATA Registry 2008 Report INTRODUCTION AUSTRALIA NEW ZEALAND The total number of deaths was 1,452 (15.4 deaths per 100 patient
CHAPTER 3 DEATHS Stephen McDonald Leonie Excell Brian Livingston DEATHS ANZDATA Registry 2008 Report INTRODUCTION AUSTRALIA NEW ZEALAND The total number of deaths was 1,452 (15.4 deaths per 100 patient
Chapter 7: ESRD among Children, Adolescents, and Young Adults
 Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
Chapter 7: ESRD among Children, Adolescents, and Young Adults The one-year end-stage renal disease (ESRD) patient mortality among the 0-4 year age group has declined approximately 41.6% over the past decade.
2014 /2018 ERA-EDTA PRD Code ERA-EDTA PRD code 1996 ERA-EDTA. SNOMED CT concept identifier Convert ERA-EDTA Primary Renal Diagnosis (PRD) Term
 Term") Convert Primary Renal Diagnosis (PRD) Term ERA_EDTA diagnosis 3380 901.1.C 90 Acute kidney injury Acute Renal Failure 14669001 Miscellaneous renal disorders 3398 901.2.C 90 Acute kidney injury due to hypovolaemia
Convert Primary Renal Diagnosis (PRD) Term ERA_EDTA diagnosis 3380 901.1.C 90 Acute kidney injury Acute Renal Failure 14669001 Miscellaneous renal disorders 3398 901.2.C 90 Acute kidney injury due to hypovolaemia
Chapter 15: Report of the Paediatric Renal Registry 1999
 Chapter 15: Report of the Paediatric Renal Registry 1999 Prepared by Dr M Lewis Introduction In parallel with the creation of the National Renal Registry, the British Association for Paediatric Nephrology
Chapter 15: Report of the Paediatric Renal Registry 1999 Prepared by Dr M Lewis Introduction In parallel with the creation of the National Renal Registry, the British Association for Paediatric Nephrology
ERA-EDTA ERA-EDTA Primary Renal Diagnosis (PRD) Term ERA-EDTA PRD classification SNOMED CT PRD Code 1/1/2015
 Term ERA-EDTA PRD classification SNOMED CT PRD Code 1/1/2015") 1003 Adult nephrotic syndrome - no histology Immunological Glomerulopathy 52254009 1019 Nephrotic syndrome of childhood - steroid sensitive - no histology Immunological Glomerulopathy 445119005 1026 Congenital
1003 Adult nephrotic syndrome - no histology Immunological Glomerulopathy 52254009 1019 Nephrotic syndrome of childhood - steroid sensitive - no histology Immunological Glomerulopathy 445119005 1026 Congenital
. Time to transplant listing is dependent on. . In 2003, 9.1% of all prevalent transplant. . Patients with diabetes mellitus are less
 Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
Chapter 5: Joint Analyses with UK Transplant in England and Wales; Access to the Renal Transplant Waiting List, Time to Listing, Diabetic Access to Transplantation and the Influence of Social Deprivation
SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND 2015
 Scottish Renal Registry Report SECTION N SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND All centres in Scotland were able to provide date of birth, sex (except centre), indication
Scottish Renal Registry Report SECTION N SCOTTISH REAL BIOPSY REGISTRY: SURVEY OF NATIVE KIDNEY BIOPSY IN SCOTLAND All centres in Scotland were able to provide date of birth, sex (except centre), indication
Chapter IX. Pediatric End Stage Renal Disease. Incidence of Reported Pediatric ESRD
 Annual Data Report Chapter IX T his chapter examines the incidence, prevalence, modalities of treatment, and survival outcomes specific to the national pediatric ESRD population. Children with advanced
Annual Data Report Chapter IX T his chapter examines the incidence, prevalence, modalities of treatment, and survival outcomes specific to the national pediatric ESRD population. Children with advanced
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
New perspec)ves on withdrawal from dialysis. Jennifer Chan, Phil Clayton, Stephen McDonald, John Agar, Ma?hew Jose
ves on withdrawal from dialysis. Jennifer Chan, Phil Clayton, Stephen McDonald, John Agar, Ma?hew Jose") New perspec)ves on withdrawal from dialysis Jennifer Chan, Phil Clayton, Stephen McDonald, John Agar, Ma?hew Jose Figure 3.8 Cause of Death by RRT Modality Cause of Death 1-Jan-2009 to 31-Dec-2009 Australia
New perspec)ves on withdrawal from dialysis Jennifer Chan, Phil Clayton, Stephen McDonald, John Agar, Ma?hew Jose Figure 3.8 Cause of Death by RRT Modality Cause of Death 1-Jan-2009 to 31-Dec-2009 Australia
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2010 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE I INTRODUCTION 1 II
NAPRTCS Annual Transplant Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2014 Annual Transplant Report This is a privileged communication not for publication. TABLE OF CONTENTS PAGE II TRANSPLANTATION Section
End Stage Kidney Disease Among Indigenous Peoples of Australia and New Zealand
 Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
Chapter 12 End Stage Kidney Disease Among Indigenous Peoples of and New Zealand 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, rates of end-stage kidney disease
The new ERA-EDTA PRDs UK Renal SNOMED CT subset TheProject
 The new ERA-EDTA PRDs UK Renal SNOMED CT subset TheProject Keith Simpson UKRR Advisor keith.simpson@nhs.net Thanks to ERA-EDTA Registry: Kitty Jager Managing Dir and members of the Coding and Terminology
The new ERA-EDTA PRDs UK Renal SNOMED CT subset TheProject Keith Simpson UKRR Advisor keith.simpson@nhs.net Thanks to ERA-EDTA Registry: Kitty Jager Managing Dir and members of the Coding and Terminology
TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA
 & TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
& TRENDS IN RENAL REPLACEMENT THERAPY IN BOSNIA AND HERZEGOVINA 2002-2008 Halima Resić* 1, Enisa Mešić 2 1 Clinic for Hemodialysis, University of Sarajevo Clinics Centre, Bolnička 25, 71000 Sarajevo, Bosnia
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Renal Transplant Registry Report 2008
 Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Renal Transplant Registry Report 28 Contents:. Introduction Page 2. Summary of transplant activity 27-28 Page 2 3. Graft and Patient Survival analysis 989-28 Page 3 4. Acute rejection 989-28 Page 24. Comparison
Chapter 12. End Stage Kidney Disease in Indigenous Peoples of Australia and Aotearoa/New Zealand. ANZDATA Registry 39th Annual Report
 Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Chapter 12 End Stage Kidney Disease in Indigenous Peoples of and Aotearoa/ 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Introduction In this chapter, the rates and practice patterns for end-stage
Epidemiology of CKD in Children
 Epidemiology of CKD in Children Ali Düzova, M.D. Hacettepe University Faculty of Medicine Pediatric Nephrology and Rheumatology Unit Ankara CKD Course 03 June 2011, İstanbul Aim & Plan Causes of CKD in
Epidemiology of CKD in Children Ali Düzova, M.D. Hacettepe University Faculty of Medicine Pediatric Nephrology and Rheumatology Unit Ankara CKD Course 03 June 2011, İstanbul Aim & Plan Causes of CKD in
Dialysis Mortality Regional Clinical Audit Report 2011
 Dialysis Mortality Regional Clinical Audit Report 2011 Clinical Audit Lead: Authors: Dr Iren Szeki Consultant Nephrologist, Manchester Royal Infirmary Dr Iren Szeki, Consultant Nephrologist Dr Helen Alderson,
Dialysis Mortality Regional Clinical Audit Report 2011 Clinical Audit Lead: Authors: Dr Iren Szeki Consultant Nephrologist, Manchester Royal Infirmary Dr Iren Szeki, Consultant Nephrologist Dr Helen Alderson,
CHAPTER 5. Paediatric Renal Replacement Therapy
 24th Report of the CHAPTER 5 Paediatric Renal Replacement Therapy Lee Ming Lee Lim Yam Ngo Lynster Liaw Chiew Tung Susan Pee Yap Yok Chin Wan Jazilah Wan Ismail 24th Report of the SECTION A: RRT PROVISION
24th Report of the CHAPTER 5 Paediatric Renal Replacement Therapy Lee Ming Lee Lim Yam Ngo Lynster Liaw Chiew Tung Susan Pee Yap Yok Chin Wan Jazilah Wan Ismail 24th Report of the SECTION A: RRT PROVISION
CHRONIC KIDNEY DISEASE (CKD)
") CHRONIC KIDNEY DISEASE (CKD) CKD implies longstanding (more than 3 months), and usually progressive, impairment in renal function. In many instances, no effective means are available to reverse the primary
CHRONIC KIDNEY DISEASE (CKD) CKD implies longstanding (more than 3 months), and usually progressive, impairment in renal function. In many instances, no effective means are available to reverse the primary
UK Renal Registry 20th Annual Report: Chapter 4 Demography of the UK Paediatric Renal Replacement Therapy Population in 2016
 Nephron 2018;139(suppl1):105 116 DOI: 10.1159/000490962 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Chapter 4 Demography of the UK Paediatric Renal Replacement Therapy Population
Nephron 2018;139(suppl1):105 116 DOI: 10.1159/000490962 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Chapter 4 Demography of the UK Paediatric Renal Replacement Therapy Population
Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY. Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin
 Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin SECTION A: RRT PROVISION FOR PAEDIATRIC PATIENTS This chapter presents
Chapter 5 PAEDIATRIC RENAL REPLACEMENT THERAPY Lee Ming Lee Lim Yam Ngo Lynster Liaw Susan Pee Wan Jazilah Wan Ismail Yap Yok Chin SECTION A: RRT PROVISION FOR PAEDIATRIC PATIENTS This chapter presents
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES OMB No
 CENTERS FOR MEDICARE & MEDICAID SERVICES OMB No. 0938-0046 END STAGE RENAL DISEASE MEDICAL EVIDENCE REPORT MEDICARE ENTITLEMENT AND/OR PATIENT REGISTRATION A. COMPLETE FOR ALL ESRD PATIENTS Check one:
CENTERS FOR MEDICARE & MEDICAID SERVICES OMB No. 0938-0046 END STAGE RENAL DISEASE MEDICAL EVIDENCE REPORT MEDICARE ENTITLEMENT AND/OR PATIENT REGISTRATION A. COMPLETE FOR ALL ESRD PATIENTS Check one:
CHAPTER 6 PERITONEAL DIALYSIS
 CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Hannah Dent Kylie Hurst Stephen McDonald PERITONEAL DIALYSIS ANZDATA Registry 11 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to
CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Hannah Dent Kylie Hurst Stephen McDonald PERITONEAL DIALYSIS ANZDATA Registry 11 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to
2015 Children's Mercy Hospitals and Clinics. All Rights Reserved.
 Growth van Stralen KJ, et al., Kidney Int, 2014 Blood Pressure Management van Stralen KJ, et al., Kidney Int, 2014 Sodium Losses on PD Infants might need higher UF rate per BSA as compared to adults to
Growth van Stralen KJ, et al., Kidney Int, 2014 Blood Pressure Management van Stralen KJ, et al., Kidney Int, 2014 Sodium Losses on PD Infants might need higher UF rate per BSA as compared to adults to
CHAPTER 9. End Stage Kidney Disease in Aotearoa/New Zealand
 CHAPTER 9 End Stage Kidney Disease in Aotearoa/New Zealand ANZDATA gratefully acknowledges the patients and their families and the clinicians who provided data, and the contributions of the Aotearoa/New
CHAPTER 9 End Stage Kidney Disease in Aotearoa/New Zealand ANZDATA gratefully acknowledges the patients and their families and the clinicians who provided data, and the contributions of the Aotearoa/New
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2006 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 2006 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 27 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
SPECIALISED SERVICES NATIONAL DEFINITIONS SET (THIRD EDITION 2008) Specialised Renal Services (adult) - Definition No. 11
 Specialised Renal Services (adult) - Definition No. 11") SPECIALISED SERVICES NATIONAL DEFINITIONS SET (THIRD EDITION 2008) Specialised Renal Services (adult) - Definition No. 11 Preface This definition is part of the third edition of the Specialised Services
SPECIALISED SERVICES NATIONAL DEFINITIONS SET (THIRD EDITION 2008) Specialised Renal Services (adult) - Definition No. 11 Preface This definition is part of the third edition of the Specialised Services
Chapter IV. Incidence and Causes of Treated ESRD. Methods
 Annual Data Report Chapter IV Incidence and Causes of Treated ESRD T he statistics in this chapter show a continued increase in the annual incidence rate of newly treated ESRD in the United States. The
Annual Data Report Chapter IV Incidence and Causes of Treated ESRD T he statistics in this chapter show a continued increase in the annual incidence rate of newly treated ESRD in the United States. The
CHAPTER 6 PERITONEAL DIALYSIS. Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst Annual Report 35th Edition
 CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst 212 Annual Report 35th Edition PERITONEAL DIALYSIS ANZDATA Registry 212 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis
CHAPTER 6 PERITONEAL DIALYSIS Fiona Brown Aarti Gulyani Stephen McDonald Kylie Hurst 212 Annual Report 35th Edition PERITONEAL DIALYSIS ANZDATA Registry 212 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis
Kidney Transplant. Description
 Section: Surgery Effective Date: October 15, 2015 Subject: Kidney Transplant Page: 1 of 9 Last Review Status/Date: September 2015 Kidney Transplant Description A kidney transplant involves the surgical
Section: Surgery Effective Date: October 15, 2015 Subject: Kidney Transplant Page: 1 of 9 Last Review Status/Date: September 2015 Kidney Transplant Description A kidney transplant involves the surgical
CHAPTER 6 PERITONEAL DIALYSIS. Neil Boudville. Hannah Dent. Stephen McDonald. Kylie Hurst. Philip Clayton Annual Report - 36th Edition
 CHAPTER 6 Neil Boudville Hannah Dent Stephen McDonald Kylie Hurst Philip Clayton 213 Annual Report - 36th Edition ANZDATA Registry 213 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to treat
CHAPTER 6 Neil Boudville Hannah Dent Stephen McDonald Kylie Hurst Philip Clayton 213 Annual Report - 36th Edition ANZDATA Registry 213 Report STOCK AND FLOW AUSTRALIA Peritoneal dialysis was used to treat
Protocol. Kidney Transplant
 Protocol Kidney Transplant (70301) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/18 Preauthorization Yes Review Dates: 05/09, 05/10, 05/11, 05/12, 05/13, 05/14, 11/14, 11/15, 11/16, 03/17
Protocol Kidney Transplant (70301) Medical Benefit Effective Date: 01/01/15 Next Review Date: 03/18 Preauthorization Yes Review Dates: 05/09, 05/10, 05/11, 05/12, 05/13, 05/14, 11/14, 11/15, 11/16, 03/17
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report. Renal Transplantation. Chronic Renal Insufficiency
 2005 Annual Report. Renal Transplantation. Chronic Renal Insufficiency") North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) 2005 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
VASCULAR ACCESS FOR HAEMODIALYSIS
 Scottish Renal Association Section H VASCULAR ACCESS FOR HAEMODIALYSIS Details of vascular access used for haemodialysis for all hospital and home haemodialysis were collected during the annual SRR census
Scottish Renal Association Section H VASCULAR ACCESS FOR HAEMODIALYSIS Details of vascular access used for haemodialysis for all hospital and home haemodialysis were collected during the annual SRR census
NAPRTCS Annual Report
 North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 28 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
North American Pediatric Renal Trials and Collaborative Studies NAPRTCS 28 Annual Report Renal Transplantation Dialysis Chronic Renal Insufficiency This is a privileged communication not for publication.
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Goh Bak Leong
 CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr Zaki Morad Mohd Zaher Dato Dr (Mr) Rohan Malek Dr Fan Kin Sing Dr Lily Mushahar Dr Lim Soo Kun Dr
CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr Zaki Morad Mohd Zaher Dato Dr (Mr) Rohan Malek Dr Fan Kin Sing Dr Lily Mushahar Dr Lim Soo Kun Dr
3/5/18. Background. Registry Reports. Dialysis Registry Update and Future Directions
 Dialysis Registry Update and Future Directions Annabelle N. Chua, MD March 4, 2018 Background Founded in 1987 as a transplant registry Expanded registry to include dialysis (1992) and CKD (1994) Patient
Dialysis Registry Update and Future Directions Annabelle N. Chua, MD March 4, 2018 Background Founded in 1987 as a transplant registry Expanded registry to include dialysis (1992) and CKD (1994) Patient
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Protocol: CRI Registry (CRIPR) Targeted Adverse Event(ADV)
 Targeted Adverse Event(ADV)") Page 1 of 19 Targeted Adverse Event(ADV) Version: 1.1; 02-03 Adverse Event: 1-Malignancy 2-Avascular necrosis 3-Slipped capital femoral epiphyses 4-Intracranial hypertension 5-Other serious adverse event
Page 1 of 19 Targeted Adverse Event(ADV) Version: 1.1; 02-03 Adverse Event: 1-Malignancy 2-Avascular necrosis 3-Slipped capital femoral epiphyses 4-Intracranial hypertension 5-Other serious adverse event
Paediatric Nephrology
 RCPCH Progress Paediatric curriculum for excellence Paediatric Nephrology Level 3 Paediatrics Sub-specialty Syllabus Version 1 Approved by the GMC for implementation from 1st August 2018 The Royal College
RCPCH Progress Paediatric curriculum for excellence Paediatric Nephrology Level 3 Paediatrics Sub-specialty Syllabus Version 1 Approved by the GMC for implementation from 1st August 2018 The Royal College
THIS chapter presents basic information about
 II. Incidence and Prevalence of ESRD INDEX WORDS: Cause of ESRD; diabetic ESRD; dialysis patient counts; ESRD growth rates; ESRD incidence; ESRD Medical Evidence Form 2728; ESRD Medicare; ESRD prevalence;
II. Incidence and Prevalence of ESRD INDEX WORDS: Cause of ESRD; diabetic ESRD; dialysis patient counts; ESRD growth rates; ESRD incidence; ESRD Medical Evidence Form 2728; ESRD Medicare; ESRD prevalence;
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Rosnawati Yahya
 CHAPTER 5 Editor: Dr Rosnawati Yahya Expert Panels: Dr Rosnawati Yahya Dr Ng Kok Peng Dr Suryati Binti Yakaob Dr Mohd Zaimi Abd Wahab Dr Yee Seow Ying Dr Wong Hin Seng Contents 5. Stock and Flow of Renal
CHAPTER 5 Editor: Dr Rosnawati Yahya Expert Panels: Dr Rosnawati Yahya Dr Ng Kok Peng Dr Suryati Binti Yakaob Dr Mohd Zaimi Abd Wahab Dr Yee Seow Ying Dr Wong Hin Seng Contents 5. Stock and Flow of Renal
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Dr Goh Bak Leong
 CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr (Mr) Rohan Malek Dr Wong Hin Seng Dr Fan Kin Sing Dr Rosnawati Yahya Dr S Prasad Menon Dr Tan Si
CHAPTER 5 RENAL TRANSPLANTATION Editor: Dr Goh Bak Leong Expert Panel: Dr Goh Bak Leong (Chair) Dato Dr (Mr) Rohan Malek Dr Wong Hin Seng Dr Fan Kin Sing Dr Rosnawati Yahya Dr S Prasad Menon Dr Tan Si
Final Report: Update on Prior Living Donors Who Were Subsequently Placed on the Waiting List
 OPTN/UNOS Minority Affairs Committee Descriptive Data Request Final Report: Update on Prior Living Donors Who Were Subsequently Placed on the Waiting List Prepared for: Minority Affairs Committee Meeting
OPTN/UNOS Minority Affairs Committee Descriptive Data Request Final Report: Update on Prior Living Donors Who Were Subsequently Placed on the Waiting List Prepared for: Minority Affairs Committee Meeting
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Matthew Jose Stephen McDonald Leonie Excell
 CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG PEOPLES OF AUSTRALIA AND NEW ZEALAND Matthew Jose Stephen McDonald Leonie Excell INTRODUCTION Rates of end-stage kidney disease among the Peoples of and are substantially
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG PEOPLES OF AUSTRALIA AND NEW ZEALAND Matthew Jose Stephen McDonald Leonie Excell INTRODUCTION Rates of end-stage kidney disease among the Peoples of and are substantially
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
CHAPTER 12 END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND. Stephen McDonald. Matthew Jose. Kylie Hurst INDIGENOUS 12-1
 ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
ANZDATA Registry 213 Report INDIGENOUS END-STAGE KIDNEY DISEASE AMONG INDIGENOUS PEOPLES OF AUSTRALIA AND NEW ZEALAND CHAPTER 12 Stephen McDonald Matthew Jose Kylie Hurst 213 Annual Report - 36th Edition
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room
 QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room msix PEDIATrIC ESrD 18 ž 21 ATLAS OF ESRD IN THE UNITED STATES Incident rates of ESRD in children have risen two
QQuickly take me up into the bright child of your mind. E.E. CUMMINGS, The Enormous Room msix PEDIATrIC ESrD 18 ž 21 ATLAS OF ESRD IN THE UNITED STATES Incident rates of ESRD in children have risen two
Analgesic and NSAID-induced Kidney Disease
 Analgesic and NSAID-induced Kidney Disease Edited by J.H.STEWART Associate Dean, Western Clinical School University of Sydney, Australia Oxford New York Tokyo Melbourne OXFORD UNIVERSITY PRESS 1993 CONTENTS
Analgesic and NSAID-induced Kidney Disease Edited by J.H.STEWART Associate Dean, Western Clinical School University of Sydney, Australia Oxford New York Tokyo Melbourne OXFORD UNIVERSITY PRESS 1993 CONTENTS
S2 File. Clinical Classifications Software (CCS). The CCS is a
. The CCS is a") S2 File. Clinical Classifications Software (CCS). The CCS is a diagnosis categorization scheme based on the ICD-9-CM that aggregates all diagnosis codes into 262 mutually exclusive, clinically homogeneous
S2 File. Clinical Classifications Software (CCS). The CCS is a diagnosis categorization scheme based on the ICD-9-CM that aggregates all diagnosis codes into 262 mutually exclusive, clinically homogeneous
Targeted Adverse Event (ADV)
") North American Pediatric Renal Trials Collaborative Studies Production Release 14.0 [$sitecode] User: Adverse Event: Adverse Event Date: Targeted Adverse Event (ADV) Web Version: 1.0; 2.0; 06-20-13 1.
North American Pediatric Renal Trials Collaborative Studies Production Release 14.0 [$sitecode] User: Adverse Event: Adverse Event Date: Targeted Adverse Event (ADV) Web Version: 1.0; 2.0; 06-20-13 1.
Renal Disease. Please refer to the assignment page Three online modules TBLs
 Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Renal Disease Please refer to the assignment page Three online modules TBLs 1 Renal Embryology 2 Lab Tests UA CBC Enzymes Creatinine Creatinine clearance Ammonia Abs C Bx 3 BUN Creatinine Creatinine Clearance
Proposed Scope of Work for KDIGO Clinical Practice Guideline for the Evaluation and Management of Candidates for Kidney Transplantation
 Proposed Scope of Work for KDIGO Clinical Practice Guideline for the Evaluation and Management of Candidates for Kidney Transplantation Introduction Transplantation is the renal replacement therapy of
Proposed Scope of Work for KDIGO Clinical Practice Guideline for the Evaluation and Management of Candidates for Kidney Transplantation Introduction Transplantation is the renal replacement therapy of
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS
 CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
CHAPTER 3 SECONDARY GLOMERULONEPHRITIS Leong Chong Men Kok Lai Sun Rosnawati Yahya 53 5th Report of the 3.1: Introduction This chapter covers the main secondary glomerulonephritis that were reported to
Finland and Sweden and UK GP-HOSP datasets
 Web appendix: Supplementary material Table 1 Specific diagnosis codes used to identify bladder cancer cases in each dataset Finland and Sweden and UK GP-HOSP datasets Netherlands hospital and cancer registry
Web appendix: Supplementary material Table 1 Specific diagnosis codes used to identify bladder cancer cases in each dataset Finland and Sweden and UK GP-HOSP datasets Netherlands hospital and cancer registry
Paediatric nephrology patients moving to adult age: a difficult transition to manage. The experience of a paediatric-to-adult out-patient clinic
 ORIGINAL ARTICLE Port J Nephrol Hypert 2007; 21 (3): 211-217 Paediatric nephrology patients moving to adult age: a difficult transition to manage. The experience of a paediatric-to-adult out-patient clinic
ORIGINAL ARTICLE Port J Nephrol Hypert 2007; 21 (3): 211-217 Paediatric nephrology patients moving to adult age: a difficult transition to manage. The experience of a paediatric-to-adult out-patient clinic
Mr PA. Clinical assessment of hydration. Poor urine output Sunken eyes Moistness of mucosa Cool peripheries Reduction in weight Postural hypotension
 X Anthony Warrens Mr PA 54 years old Previously well Went to Thailand Developed serious diarrhoea and vomiting two days before coming home 24 hours after return, still unwell GP found: urea 24 mmol/l creatinine
X Anthony Warrens Mr PA 54 years old Previously well Went to Thailand Developed serious diarrhoea and vomiting two days before coming home 24 hours after return, still unwell GP found: urea 24 mmol/l creatinine
Incidence of new patients starting RRT
 SECTION A INCIDENCE A1 Incidence of new patients starting RRT A1.1 Incidence of new patients starting RRT 196-213 3 25 2 Number of 15 patients 1 5 367 425 749 119 169 2319 Year starting RRT 2799 2924 2635
SECTION A INCIDENCE A1 Incidence of new patients starting RRT A1.1 Incidence of new patients starting RRT 196-213 3 25 2 Number of 15 patients 1 5 367 425 749 119 169 2319 Year starting RRT 2799 2924 2635
PATTERNS OF RENAL INJURY
 PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
PATTERNS OF RENAL INJURY Normal glomerulus podocyte Glomerular capillaries electron micrograph THE CLINICAL SYNDROMES 1. The Nephrotic Syndrome 2. The Acute Nephritic Syndrome 3. Rapidly Progressive Glomerulonephritis
Nephrology Dialysis Transplantation
 Nephrol Dial Transplant (993) 8-684-689 Original Article Nephrology Dialysis Transplantation Chronic renal failure in India M. K. Mani Renal Unit, Apollo Hospital, Madras, India Abstract. In a series of
Nephrol Dial Transplant (993) 8-684-689 Original Article Nephrology Dialysis Transplantation Chronic renal failure in India M. K. Mani Renal Unit, Apollo Hospital, Madras, India Abstract. In a series of
Anul de studiu 5 Semestrul * I Tipul de evaluare finală (E / V / C) E
 E") Denumirea disciplinei FIŞA DISCIPLINEI (english series) Numărul total de ore (pe semestru) din planul de învăţământ (84) NEPHROLOGY Anul de studiu 5 Semestrul * I Tipul de evaluare finală (E / V / C) E
Denumirea disciplinei FIŞA DISCIPLINEI (english series) Numărul total de ore (pe semestru) din planul de învăţământ (84) NEPHROLOGY Anul de studiu 5 Semestrul * I Tipul de evaluare finală (E / V / C) E
RaDaR Inclusion and Exclusion Criteria
 Cohort Inclusion Criteria Exclusion Criteria Adenine Phosphoribosyltransferase Deficiency (APRT-D) APRT Deficiency APRT Deficiency confirmed Abolished APRT enzyme activity or confirmed disease-causing
Cohort Inclusion Criteria Exclusion Criteria Adenine Phosphoribosyltransferase Deficiency (APRT-D) APRT Deficiency APRT Deficiency confirmed Abolished APRT enzyme activity or confirmed disease-causing
CHAPTER 5. Haemodialysis. Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald
 CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
CHAPTER Haemodialysis Kevan Polkinghorne Hannah Dent Aarti Gulyani Kylie Hurst Stephen McDonald STOCK AND FLOW AUSTRALIA The annual stock and flow of HD patients during the period - is shown in Figures.,.
CHAPTER 5 RENAL TRANSPLANTATION. Editor: Rosnawati Yahya. Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng.
 CHAPTER 5 Editor: Roswati Yahya Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng Contents 5. Stock and Flow of Rel Transplantation Stock and Flow Transplant Rates 5.2 Recipients
CHAPTER 5 Editor: Roswati Yahya Expert Panels: Hooi Lai Seong Ng Kok Peng Suryati Binti Yakaob Wong Hin Seng Contents 5. Stock and Flow of Rel Transplantation Stock and Flow Transplant Rates 5.2 Recipients
Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2003 to 2012
 Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2003 to 2012 Types of Care Our Vision Better data. Better decisions. Healthier Canadians. Our Mandate
Canadian Organ Replacement Register Annual Report: Treatment of End-Stage Organ Failure in Canada, 2003 to 2012 Types of Care Our Vision Better data. Better decisions. Healthier Canadians. Our Mandate
1. Normal and pathological embryology of the urinary and genital tract 2. Nephrology 3. Infection
 1 1. Normal and pathological embryology of the urinary and genital tract 1.1. Development of the kidney and ureter 1.2. Development of the bladder and the urethra 1.3. Development of the female genital
1 1. Normal and pathological embryology of the urinary and genital tract 1.1. Development of the kidney and ureter 1.2. Development of the bladder and the urethra 1.3. Development of the female genital
ANNUAL REPORT The Norwegian Renal Registry. (Norsk Nefrologiregister)
") ANNUAL REPORT 21 The Norwegian Renal Registry (Norsk Nefrologiregister) This report will also be available on: http://152.94.12.23/nyreforening/uremiregisteret/esdr.html Correspondence to: Overlege dr.med
ANNUAL REPORT 21 The Norwegian Renal Registry (Norsk Nefrologiregister) This report will also be available on: http://152.94.12.23/nyreforening/uremiregisteret/esdr.html Correspondence to: Overlege dr.med
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
BETA-2 MICROGLOBULIN Test Code Test Name CPT
 BETA-2 MICROGLOBULIN Test Code Test Name CPT BE2MC Beta-2 Microglobulin 82232 Narrative Description ICD9 ACUTE IN DISEASES CLASSIFIED ELSEWHERE 580.81 ACUTE WITH LESION OF PROLIFERATIVE 580.0 ACUTE WITH
BETA-2 MICROGLOBULIN Test Code Test Name CPT BE2MC Beta-2 Microglobulin 82232 Narrative Description ICD9 ACUTE IN DISEASES CLASSIFIED ELSEWHERE 580.81 ACUTE WITH LESION OF PROLIFERATIVE 580.0 ACUTE WITH
CHAPTER 14. Renal Transplantation
 15th Report of the Malaysian RENAL TRANSPLANTATION CHAPTER 14 Renal Transplantation Editor: Dr. Goh Bak Leong Expert Panel: : Dato Dr. Dato Zaki Dr. Morad Zaik Morad Mohd (Chair) Zaher (Chair) Dr. Goh
15th Report of the Malaysian RENAL TRANSPLANTATION CHAPTER 14 Renal Transplantation Editor: Dr. Goh Bak Leong Expert Panel: : Dato Dr. Dato Zaki Dr. Morad Zaik Morad Mohd (Chair) Zaher (Chair) Dr. Goh
532.6 (chronic or unspecified duodenal
 Supplementary table 1: ICD-9 and ICD-10 codes used for the identification of major bleeding and endoscopy Bleeding episode type ICD-9 codes ICD-10 codes Intracranial 430 (Subarachnoid), 431 (intracerebral),
Supplementary table 1: ICD-9 and ICD-10 codes used for the identification of major bleeding and endoscopy Bleeding episode type ICD-9 codes ICD-10 codes Intracranial 430 (Subarachnoid), 431 (intracerebral),
FOLLOW-UP AFTER EMERGENCY DEPARTMENT VISIT FOR PEOPLE WITH HIGH-RISK MULTIPLE CHRONIC CONDITIONS (FMC) HEDIS (Administrative)
 HEDIS (Administrative)") FOLLOW-UP AFTER EMERGENCY DEPARTMENT VISIT FOR PEOPLE WITH HIGH-RISK MULTIPLE CHRONIC CONDITIONS (FMC) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD
FOLLOW-UP AFTER EMERGENCY DEPARTMENT VISIT FOR PEOPLE WITH HIGH-RISK MULTIPLE CHRONIC CONDITIONS (FMC) APPLICATIONS OBJECTIVE Purpose of Measure: ELIGIBLE POPULATION Which members are included? STANDARD
Canadian Organ Replacement Register Annual Report. Treatment of End-Stage Organ Failure in Canada, 2000 to 2009
 Canadian Organ Replacement Register Annual Report Treatment of End-Stage Organ Failure in Canada, 2000 to 2009 January 2011 Who We Are Established in 1994, CIHI is an independent, not-for-profit corporation
Canadian Organ Replacement Register Annual Report Treatment of End-Stage Organ Failure in Canada, 2000 to 2009 January 2011 Who We Are Established in 1994, CIHI is an independent, not-for-profit corporation
Chapter 10. Cancer. ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong.
 Chapter Cancer ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong Contents: Cancer -1 Incidence of Cancer on Renal Replacement Therapy -2 Kidney Cancer
Chapter Cancer ANZDATA gratefully acknowledges the contributions of the Cancer Working Group convened by Germaine Wong Contents: Cancer -1 Incidence of Cancer on Renal Replacement Therapy -2 Kidney Cancer
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review
 Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Clinical and pathological characteristics of patients with glomerular diseases at a university teaching hospital: 5-year prospective review KW Chan, TM Chan, IKP Cheng Objective. To examine the prevalence
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Chapter 10. Cancer. ANZDATA Registry 39th Annual Report. Data to 31-Dec-2015
 Chapter Cancer 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Incidence of Cancer on Renal Replacement Therapy Figures.1-.6 and table.1 show the cumulative incidence of non-skin cancer in patients
Chapter Cancer 216 ANZDATA Registry 39th Annual Report Data to 31-Dec-215 Incidence of Cancer on Renal Replacement Therapy Figures.1-.6 and table.1 show the cumulative incidence of non-skin cancer in patients
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
ANNUAL REPORT The Norwegian Renal Registry. (Norsk Nefrologiregister)
") ANNUAL REPORT 1997 The Norwegian Renal Registry (Norsk Nefrologiregister) Correspondence to: Overlege dr.med Torbjørn Leivestad ITI, Rikshospitalet, 27 Oslo, Norway. Fax: 47-2223693 Tel: 47-22868559 Preface
ANNUAL REPORT 1997 The Norwegian Renal Registry (Norsk Nefrologiregister) Correspondence to: Overlege dr.med Torbjørn Leivestad ITI, Rikshospitalet, 27 Oslo, Norway. Fax: 47-2223693 Tel: 47-22868559 Preface
BK virus infection in renal transplant recipients: single centre experience. Dr Wong Lok Yan Ivy
 BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
BK virus infection in renal transplant recipients: single centre experience Dr Wong Lok Yan Ivy Background BK virus nephropathy (BKVN) has emerged as an important cause of renal graft dysfunction in recent
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Research Article End-Stage Kidney Failure in Oman: An Analysis of Registry Data with an Emphasis on Congenital and Inherited Renal Diseases
 Hindawi International Nephrology Volume 2017, Article ID 6403985, 7 pages https://doi.org/10.1155/2017/6403985 Research Article End-Stage Kidney Failure in Oman: An Analysis of Registry Data with an Emphasis
Hindawi International Nephrology Volume 2017, Article ID 6403985, 7 pages https://doi.org/10.1155/2017/6403985 Research Article End-Stage Kidney Failure in Oman: An Analysis of Registry Data with an Emphasis
The role of the Nephrologist in Acute Kidney Injury. Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital
 The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
The role of the Nephrologist in Acute Kidney Injury Rebecca Brown Consultant Nephrologist Royal Liverpool University Hospital Overview Impact of AKI Need for change Who needs a Nephrologist Are we making
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory